Embed Size (px)
Citation preview

Journal of Surgical Research 136, 179–181 (2006)
Association for Academic Surgery, 2006
Does Frozen Section Alter Surgical Management of MultinodularThyroid Disease?1
Sarah Olson, M.S.,* Yusra Cheema, B.S.,* Josephine Harter, M.D.,† James Starling, M.D., F.A.C.S.,*and Herbert Chen, M.D., F.A.C.S.*,2
*Department of Surgery, Section of Endocrine Surgery, and †Department of Pathology, University of Wisconsin, Madison, Wisconsin
Submitted for publication January 11, 2006
doi:10.1016/j.jss.2006.07.030
Background. Frozen section (FS) evaluation duringthyroid surgery is often used to guide intraoperativemanagement. We sought to determine the utility of FSin patients undergoing thyroidectomy for multinodu-lar thyroid disease.
Methods. From May 1994 through November 2004, 236patients with multinodular goiter underwent thyroidec-tomy at our institution. Patient data were retrospec-tively analyzed to see if a frozen section was performedduring the procedure and whether it changed the pa-tient’s outcome.
Results. Of the 236 patients, 135 (57%) had intra-operative FS. There were no differences between pa-tients who had FS analysis and those who did not withregard to age, gender, and the incidence of malignancy.Of the patients who had FS, 4/135 (3%) were subse-quently diagnosed with thyroid cancer on permanenthistology. Three of these FS were misread as benign.Therefore, the sensitivity of FS for the diagnosis of thy-roid cancer was only 25%. Importantly, in none of the 135patients did FS alter the intraoperative management.
Conclusion. While FS was commonly used in pa-tients undergoing thyroidectomy at our institution, inno patient over the last decade did FS correctly alterthe intraoperative management. Given the time re-quired to perform FS and the cost associated with it,we believe that routine FS should not be performed inthese patients. © 2006 Elsevier Inc. All rights reserved.
Key Words: thyroid goiter; thyroid surgery; frozensection; multinodular goiter.
1 Presented at the 1st Annual Academic Surgical Congress (Asso-ciation for Academic Surgery), San Diego, CA, February 7–11, 2006.
2 To whom correspondence and reprint requests should be ad-dressed at University of Wisconsin, Department of Surgery, H4/750CSC 600 Highland Avenue, Madison, WI 53792. E-mail: chen@
surgery.wisc.edu.179
INTRODUCTION
Multinodular goiter (MNG) is the most common formof benign thyroid disease both worldwide and in theUnited States. Worldwide, it affects 500 to 600 millionpeople and in the US prevalence is 4 to 7%, but may behigher in areas where goiter is endemic [1, 2]. In theinitial evaluation of patients with MNG, ultrasound isoften used to assess the character and size of the thy-roid gland. Furthermore, any suspicious nodules foundon examination can be assessed with fine needle aspi-ration biopsy to rule out malignancy [3–5]. Occasion-ally, the development of MNG can be because ofhypothyroidism. In patients with an elevated thyroidstimulated hormone (TSH), replacement with exoge-nous thyroid hormone can reduce the size of the thy-roid gland [1]. Patients with MNG can present withsymptoms including dysphagia, shortness of breath,compression of the large vessels of the neck and thorax.Cosmetic appearance is also a concern for many pa-tients. Thus, patients with MNG often require inter-vention to alleviate these symptoms and concerns.
While some investigators have attempted to treatMNG with other modalities including radioactive io-dine [1, 6], the most efficient and efficacious treatmentis thyroidectomy. The surgical options for treatment ofMNG include thyroid lobectomy, subtotal thyroidec-tomy, and total thyroidectomy. The extent of thyroid-ectomy is often determined by whether the nodulardisease is present unilaterally or bilaterally [2, 7, 8].
Frozen section evaluation is often used to guide in-traoperative decision-making during thyroid surgery.We have previously shown that frozen section analysiscan be useful in patients with lesions suspicious forpapillary thyroid cancer, but can also be misleadingin the setting of a follicular or Hurthle cell neoplasm[9, 10]. Because of the low incidence of malignancy inMNG and the fact that frozen section adds time and
expense to the operation, we sought to determine how0022-4804/06 $32.00© 2006 Elsevier Inc. All rights reserved.
180 JOURNAL OF SURGICAL RESEARCH: VOL. 136, NO. 2, DECEMBER 2006
often the results of the frozen section actually changethe operative outcome in patients with MNG.
METHODS
From May 1994 through November 2004, 236 patients with MNGunderwent thyroidectomy at the University of Wisconsin. Thesepatients were identified from an ongoing prospective endocrine da-tabase and data were retrospectively analyzed. Both the data collec-tion and analysis were approved by separate protocols through theUniversity of Wisconsin Human Subjects Institutional ReviewBoard. Statistical analysis was performed with SPSS software (SPSSInc.) Statistical significance was defined as a P � 0.05.
Of these patients, 135 (57%) had intraoperative frozen section; thedecision to perform frozen section was at the discretion of the indi-vidual surgeon. After receipt of tissue in the pathology laboratory,one slice was made through the largest dimension of the specimen. Asection from the dominant or most suspicious nodule was snap frozenin an isopentane bath, sectioned at approximately 5 �m thickness,stained with hematoxylin and eosin and microscopically examined.
After frozen section analysis, standard formalin-fixed, paraffin sec-tion slides of the frozen tissue were prepared. The remaining tissue wassampled with at least one tissue block per centimeter of the greatestdimension of the dominant nodule. Paraffin section slides were pre-pared and examined for definitive pathologic diagnosis. These resultswere then compared to the results of the frozen section.
RESULTS
Demographically, the two groups were similar. Themean age of patients undergoing frozen section was50 � 14 years while the mean age of those not receivingfrozen section was 53 � 16 years. The gender of thoseundergoing frozen section compared to the others was85% and 80%, respectively. 3% of patients undergoingfrozen section were diagnosed with cancer versus 8% ofthose undergoing only permanent section were foundto have cancer (P � 0.086) (Table 1).
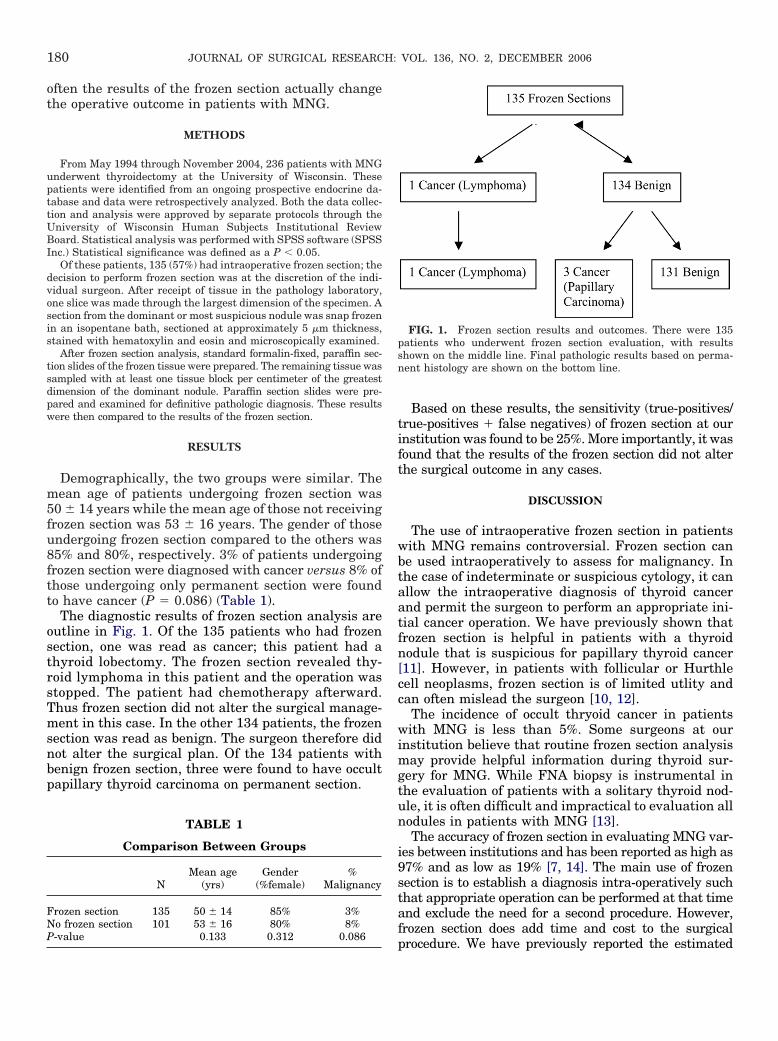
The diagnostic results of frozen section analysis areoutline in Fig. 1. Of the 135 patients who had frozensection, one was read as cancer; this patient had athyroid lobectomy. The frozen section revealed thy-roid lymphoma in this patient and the operation wasstopped. The patient had chemotherapy afterward.Thus frozen section did not alter the surgical manage-ment in this case. In the other 134 patients, the frozensection was read as benign. The surgeon therefore didnot alter the surgical plan. Of the 134 patients withbenign frozen section, three were found to have occultpapillary thyroid carcinoma on permanent section.
TABLE 1
Comparison Between Groups
NMean age
(yrs)Gender
(%female)%
Malignancy
Frozen section 135 50 � 14 85% 3%No frozen section 101 53 � 16 80% 8%
P-value 0.133 0.312 0.086Based on these results, the sensitivity (true-positives/true-positives � false negatives) of frozen section at ourinstitution was found to be 25%. More importantly, it wasfound that the results of the frozen section did not alterthe surgical outcome in any cases.
DISCUSSION
The use of intraoperative frozen section in patientswith MNG remains controversial. Frozen section canbe used intraoperatively to assess for malignancy. Inthe case of indeterminate or suspicious cytology, it canallow the intraoperative diagnosis of thyroid cancerand permit the surgeon to perform an appropriate ini-tial cancer operation. We have previously shown thatfrozen section is helpful in patients with a thyroidnodule that is suspicious for papillary thyroid cancer[11]. However, in patients with follicular or Hurthlecell neoplasms, frozen section is of limited utlity andcan often mislead the surgeon [10, 12].
The incidence of occult thryoid cancer in patientswith MNG is less than 5%. Some surgeons at ourinstitution believe that routine frozen section analysismay provide helpful information during thyroid sur-gery for MNG. While FNA biopsy is instrumental inthe evaluation of patients with a solitary thyroid nod-ule, it is often difficult and impractical to evaluation allnodules in patients with MNG [13].
The accuracy of frozen section in evaluating MNG var-ies between institutions and has been reported as high as97% and as low as 19% [7, 14]. The main use of frozensection is to establish a diagnosis intra-operatively suchthat appropriate operation can be performed at that timeand exclude the need for a second procedure. However,frozen section does add time and cost to the surgical
FIG. 1. Frozen section results and outcomes. There were 135patients who underwent frozen section evaluation, with resultsshown on the middle line. Final pathologic results based on perma-nent histology are shown on the bottom line.
procedure. We have previously reported the estimated

181OLSON ET AL.: FROZEN SECTION IN GOITERS
cost per useful frozen section to be between $15,000 to$24,000 [10]. There are few studies that looked at the useof frozen section in surgery for MNG. Rios et al. reportthat frozen section had a sensitivity of 19% in detectingcancer in patients with MNG and recommend not usingfrozen section in the evaluation of MNG [14].
In summary, MNG is the most common form of be-nign thyroid disease both worldwide and in the UnitedStates. Thyroidectomy is often perform to alleviatesymptoms. We found that frozen section analysis wascommonly utlized at our institution for intra-operativeevaluation of the thyroid. Despite its common use, fro-zen section did not alter the operative procedure in anycase. Therefore, given the cost and time involved inperforming intra-operative frozen section, we recom-mend that routine frozen section not be performed inpatients with MNG undergoing surgical resection.
REFERENCES
1. Day TA, Chu A, Hoang KG. Multinodular Goiter. OtolaryngolClin North Am 2003;36:35.
2. Lang BH, Lo CY. Total thyroidectomy for multinodular goiter inthe elderly. Am J Surg 2005;190:418.
3. Bonnema SJ, Bennedbaek FN, Ladenson PW, Hegedus L. Man-agement of the nontoxic multinodular goiter: A north Americansurvey. J Clin Endocrinol Metab 2002;87:112.
4. Chen H, Dudley NE, Westra WH, Sadler GP, Udelsman R. The
utilization of fine-needle aspiration in patients undergoing thy-roidectomy at two academic centers across the Atlantic. WorldJ Surg 2003;27:208.
5. Chen H, Nicol TL, Rosenthal DL, Udelsman R. The role offine needle aspiration in the evaluation of thyroid nodules.In: Norton JA, ed. Problems in general surgery: Surgery ofthe thyroid gland. New York, NY: Lippincott-Raven Publish-ers; 1997.
6. Nygaard B, Hegedus L, Gervil M, Hjalgrim H, Soe-Jensen P,Hansen JM. Radioiodine treatment of multinodular non-toxicgoitre. Br Med J 1993;307:828.
7. Clark OH. Total thyroidectomy: The preferred option for multi-nodular goiter. Ann Surg 1988;208:244.
8. Liu Q, Djuricin G, Prinz RA. Total thyroidectomy for benignthyroid disease. Surgery 1998;123:2.
9. Udelsman R, Chen H. The current management of thyroidcancer. In: Cameron JL, ed. Advances in surgery. St. Louis, MO:Mosby, Inc.; 1999.
10. Chen H, Nicol T, Udelsman R. Follicular lesions of the thyroid:Does frozen section evaluation alter operative management?Ann Surg 1995;222:101.
11. Chen H, Zeiger MA, Clark DP, Westra WH, Udelsman R.Papillary carcinoma of the thyroid: Can operative managementbe based solely on fine needle aspiration? J Am Coll Surg1997;184:605.
12. Chen H, Nicol TL, Zeiger MA, et al. Hurthle cell neoplasm of thethyroid: Are there factors predictive of malignancy? Ann Surg1998;227:542.
13. Greenblatt DY, Woltman T, Harter J, Starling J, Mack E, ChenH. Fine needle aspiration optimizes surgical management inpatients with thyroid cancer. Ann Surg Oncol 2006;13:859.
14. Rios Zambudio A, Rodriguez Gonzalez JM, Sola Perez J, SoriaCogollos T, Galindo Fernandez PJ, Parrilla Paricio P. Utility offrozen-section examination for diagnosis of malignancy associ-
ated with multinodular goiter. Thyroid 2004;14:600.




























