Embed Size (px)
Citation preview
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 1
CLINICAL NOTESRehabilitation Clinical
Documentation
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 2
Clinical Notes
The goals aligned with the patients plan of care are based on the patient centered functional goals.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 3
Clinical Notes
Long Term Goal: The clinical goals are expected to be
achievable and realistic within the designated time frame and the treatments listed (referred to as the treatment plan) are necessary to achieve these goals within the designated time frame.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 4
Clinical Notes
The functional goals were created based on the reported patient’s prior level of function as compared to the assessed current level of function.
Goals are Identified by: Valid and Reliable functional test Objective measures Co-morbidities Therapist judgment
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 5
Validity Defined
Test is measuring what it is intended to measure Balance Dizziness Back Pain Neck Pain Leg function Arm function
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 6
Reliability Defined
Broadly defined: One is able to rely on the test scores being
accurate and reproducible

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 7
Objective Measures
Data that are measureable Impairments
Strength Pain Range of Motion Reflexes Circumference measures
Function Functional Tests
TGUG Berg
Questionnaires Oswestry Neck Disability Index
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 8
Comorbidities
Issue that affect the outcome of treatment Age Past Medical History Family participation Cognitive Issues Access to attend PT Equipment needs
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 9
Therapist Judgment
To determine functional status or level of disability the following must be considered Prior Level of Function Severity of Procedure/Pathology/Disease Objective Impairment Finding Functional Test(s) scores and the consideration
of the minimally detectable change and cut offs
Motivation of patient and family Experience of therapist
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 10
DOCUMENTING MEDICAL NECESSITY
THRU OUTCOMES ASSESSMENT
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 11
OUTCOMES
Outcomes Assessment Collection and recording of information
relative to health processes Outcomes Management
Using information in a way that enhances patient care
(Hansen DT, Mior S, Mootz RD in Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 12
The Era of Outcomes Assessment
Outcomes in clinical practice provide the mechanism by which the health care provider, the patient, the public, and the payer are able to assess the end results of care and its effect upon the health of the patient and society. (Anderson & Weinstein, 1994).
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 13
Survival
To survive, in fact to flourish, in this era of accountability health care providers must be prepared to maintain and be able to provide appropriate documentation and patient records in a clinically efficient and economical manner. (Hansen, 1994).

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 14
Health Policy
With the dawning, of the “era of accountability,” there are new social mandates directed toward health care providers and health-related facilities. Measurements of quality, satisfaction, efficacy, and effectiveness now serve as essential elements for health care decisions and matters of health policy. (Hansen DT, Mior S, Mootz RD in Yeomans SG:
The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 15
Outcome Meanings
Health Care Customer - Meaning of Outcomes Payers-purchasers Cost containment Regulators HCP compliance Administrators Efficiency-low
utilization Clinical Researchers Proof of a premise Outcomes Experts Patient’s benefit Health Care Providers Clinical-Health
Status
(Hansen DT, Mior S, Mootz RD in Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 16
Outcomes Criteria
Utility Is it useful? Reliability Is it dependable? Validity Does it do what it is
supposed to? Sensitivity Can it identify patients with
a condition? Specificity Can it identify those that do
not have the condition? Responsiveness Can it measure
differences over time?
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 17
Outcome Measures Appropriate for Clinical Use
Questionnaires General health status Pain Functional status Patient satisfaction
Physiological outcomes Utilization measures Cost measures
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 18
Outcomes Measures Appropriately Used
When outcome measures are appropriately used and integrated into an evidence-based, patient-centered model of practice, there is accountability and quality assurance.
(Hansen DT, Mior S, Mootz RD in Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 19
Subjective Questionnaires
Subjective outcomes assessment information is gathered by the patient in self-administered questionnaires and scored by either the: health care provider staff members or by a computer.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 20
Subjective Questionnaires
In spite of the definition associated with the term “subjective,” these “pen-and-paper tools” have been described as very valid and reliable – in many cases more so than many of the “objective’ tests that health care providers have relied upon for years.
(Chapman-Smith, 1992; Hansen, 1994; Mootz, 1994).
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 21
Subjective vs Objective
It must be emphasized that although the term “subjective” carries negative connotations, the reliability/validity data published regarding these methods of collecting outcomes is exceptional, typically out-performing the test-retest reliability and validity of most “objective” physical performance tests. (Chapman-Smith, 1992).

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 22
Classification of Outcome Assessment Tools
Subjective (Patient Driven)
General Health Pain Perception Condition or Disease Specific Psychometric Disability Prediction Patient Satisfaction Prior Level of function
Objective (HCP Driven)
Range of Motion Strength - Endurance Nonorganic Proprioception Cardiopulmonary Developmental Neurological Pain (VAS) Integumentary Special Test Functional Tests
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 23
Outcomes Assessment Tools
It is important to remember to utilize the same outcome assessment tool through the course of case management with each patient.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 24
Defining Terms
Progress Note Re-assessment Re-evaluation
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 25
Clinical Notes
The progress notes allows the therapist to determine the effectiveness of the allocated plan of care and to measure the clinical findings that are compared to the clinical goals that establish indicators of progress toward addressing functional limitations and achieving functional goals.
Falls hand and hand with the Re-assessment
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 26
Clinical Notes
A re-evaluation is performed when a significant changes has taken place and there is an alteration in the plan of care.
Be careful not to over-utilize this code in your billing methodology
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 27
Clinical Notes
The functional goals are based upon a correlation of functional assessment tools, clinical findings/tests, performance based tests, objective findings and the therapist judgment call.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 28
Nagi:Functional Levels
Impairment: Loss or abnormality of anatomical, physiological,
mental, or psychological structure or function. Organ specific
Functional Limitation Restriction of ability to perform, at the level of the
whole person, a physical action, task or activity in an efficient, typically expected, or competent manner. Person specific.
Disability: The inability to perform or a limitation in the
performance of actions, tasks, and activities usually expected in specific social roles.
(Nagi, S. Some conceptual issues in disability and rehabilitation. In : Sussman M, ed Sociology and Rehabilitation. Washington DC: American Sociology Society; 1965: 100-113)

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 29
APTA References to Proper Clinical Documentation
APTA has numerous publication that address components of clinical documentation. Below are a list of three publications that will be discussed. Guide to Physical Therapy Practice Peer Review/Utilization Review Task Force on Measurements APTA Standards of Tests and Measurements Primer on Measurement: An introductory guide to
measurement issues. (Rothstein, Echternach) WHO: International classification of functioning,
disability and health
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 30
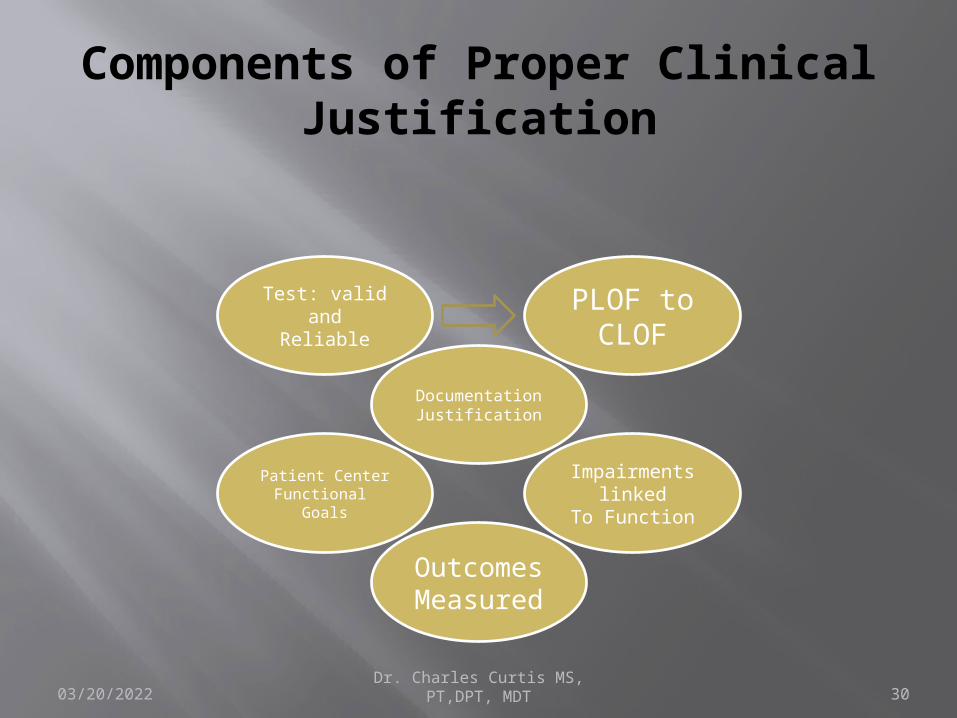
Components of Proper Clinical Justification
Documentation
Justification
PLOF to CLOF
Impairments linked
To Function
Outcomes Measured
Patient CenterFunctional
Goals
Test: valid and
Reliable
04/15/2023
MEASUREMENT AND UTILIZATION REVIEW
Dr. Charles Curtis MS, PT,DPT, MDT31
Validity and Reliability. Concurrent and Retrospective Reviews
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 32
Physical Therapy Scope of Practice
Provide services to patients/clients who have impairments, functional limitation, disabilities or changes in physical function and health status resulting from injury, disease or other causes.
(Guide to Physical Therapy Practice 2nd Edition. pg S31)
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 33
Utilization Review
What is needed for Review The inclusion of the patient in establishing goals:
Patient centered functional goals A statement of impairment related to functional
limitation Valid Function Tests with reliable scores
A statement on any changes in health status, wellness, and fitness needs to be identified Objective noted with impairment measures
Medicare signed plan of care Physician signature
MD script for most commercial products Direct access does not require us to have a script just
communication with patient’s physician

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 34
Medical and Scientific Evidence
To set criteria for the effectiveness and efficiency of a test Peer Review articles are defined: Peer-review scientific studies published in, or
in accepted for publication by, medical journals that meet nationally recognized requirements for scientific manuscripts and that submit most of their published articles for review by experts who are not part of the editorial staff.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 35
Summary of Section
Scope of practice is a key component to keep in mind as to what services a PT should provide.
Valid and Reliable Measure are an essential part of clinical documentation.
Scientific literature is the source of information regarding the application of tests and how to interpret the findings
Validity: is the test measuring what it claims to Reliability: is the test consistent and stable and
reproducible.
04/15/2023
INSURANCE COMPANIES AND UTILIZATION REVIEW
Dr. Charles Curtis MS, PT,DPT, MDT36
View on Documentation and Function
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 37
Utilization Review
Utilization Review Process Defined The review to determine whether health care
services that have been provided, are being provided or are proposed to be provided to a patient, whether undertaken prior to, concurrent with or subsequent to the delivery of such services are medically necessary.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 38
Utilization Review
Concurrent Review Defined: The review preformed at the time of
treatment. Review is performed to determine medical
necessity of the treatment performed and it effect on the consequence of disease , including
impairments, functional limitations, patient centered functional goals that justify
treatment, which lead to the foundation of medically necessary.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 39
Utilization Review
The fact that a provider and or physician (par or non par) has made a prescribed, recommended, or approved a service, supply or equipment, does not in itself, makes it medically necessary.
What is required: Justification through written documentation
utilizing measurement that are valid and reliable
These are the items that are required by a majority of Utilization review process
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 40
Summary of Documentation Requirements
What is required by parties interested in documentation? Proof that care is necessary, effective and
important to the patient. How do we do this?
At the core of proper documentation is the validity and reliability of the measurements. Linking these measurement changes, from an impairments view and the direct association to the functional limitation, of the patient.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 41
Authors Views on Documentation
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 42
Peat, et al. (1979) Analysis of Performance
According to Peat and Campbell (1979) “…the profession (physical therapy) has been
criticized for not objectively recording events” Why:
Primary tools in the assessment of motor performance are visual tools and gross motor test.
Visual test disadvantage is the absence of quantification of specific parameters of the event
The validity of the test is placed on the therapist personal observation a particular response.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 43
Peat (1979) Analysis of Performance
To improve our clinical documentation there must be: An emphasis on function we must be able to
analysis performance An analysis of performance is the quantification
of stipulated parameters, comparison of parameters with respect to a
normative data, comparison of the present and previous states of
results for the same set of parameters.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 44
How to improve recording of motor performance tasks?
In the analysis of motor performance look to two components: Product or outcome
Effectiveness Efficiency
Process Biomechanical efficiency Biomechanics is the science of accelerations,
forces, and displacements acting on the human body and the injuries caused by these forces
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 45
Product or outcome
Effectiveness: The degree of success attained in the
achievement of the goal Efficiency:
Ratio of mechanical work accomplished by the total work accomplished (How much effort to how much work). Directly related to time, distance, force and accuracy.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 46
ProcessBiomechanical efficiency
Biomechanical efficiency Skill of task.
Exhibited by patient when attempting to perform a movement
Gross measurement (ie. Gross gait pattern)
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 47
Biomechanics
The human body is subject to gravitational force and through the study of these force we can maintain or improve a humans overall quality of life.
Any injury to, or lesion in, any of the individual elements of the musculoskeletal system will change the mechanical interaction and cause degradation, instability or disability of movement.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 48
Biomechanics
In response to these negative adaptations: proper modification, manipulation and control
of the mechanical environment can help prevent injury, correct abnormality, and speed healing and rehabilitation.
To Accomplish this, an understanding the biomechanics and
loading of each element during movement using visual assessment and or motion analysis is helpful for studying disease etiology, making decisions about treatment, and evaluating treatment effects
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 49
Peat and Campbell Summary
Proper documentation should follow the same outline as analysis of movement: Effectiveness of a functional task should be
measured by the degree of success attained by the achievement of the task or activity
Efficiency of a functional task to measure time, distance, force or energy required and accuracy of the task. (RPE example of measuring this)
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 50
Randall and McEwen (2000)Patient-Centered Functional Goals
All areas including, research, health care policy reimbursement practices and the standards of accrediting bodies all support writing patient-centered functional goals.
Reason: It promotes a patient-centered approach in
which PT actively facilitate the participation of the patient/client, family, significant other and caregivers in the plan of care.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 51
Randall and McEwen (2000)Patient-Centered Functional Goals
Rational for such goals: Functional Goals are necessary to address
the fact that correction of impairment alone is not directly functional and may not necessarily lead to functional improvements or may not be meaningful to the patient.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 52
Randall and McEwen (2000)Patient-Centered Functional Goals
Function: those activities identified by individual as essential to support physical, social, and psychological well being and to create a personal sense of meaningful living.
Goals: remediation of impairment and uses the term “outcomes” for minimization of functional limitation, optimization of health status, prevention of disabilities, and optimization of patient/client satisfaction.
Primary goal is to maintain and improve the quality of life of an individual—
empowering independency

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 53
Functional Goals
Defined: as the individually meaningful activities that a person cannot perform as a result of an injury, illness or congenital or acquired condition, but want to be able to accomplish as a result of physical limitation.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 54
Steffen and Meyer (1995)
The shift in federal guidelines of cost reimbursement have alternatively benefited, bewildered and penalized the clinics.
The potential shift to a dependency of reimbursement on the evidence based practice will be required to utilize and document credible measures of outcomes.
Why? to safe guard our patients interest and to promote our own professional self interest
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 55
Steffen and Meyer (1995)
Appropriate question to identify patient centered functional goals. Determine the patients desired outcomes Rank outcomes in priority order. (Ask patient
which of their goals is the most important) Develop an understanding of patients self
care, work, and leisure activities and environment in which these activities occur (Life style, hobbies, activity levels, etc.)
Establish goals with the patient and if necessary with family that relate to desired outcomes.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 56
Rothstein and Echternach (2001)HOAC II
Hypothesis Orientated Algorithm for Clinicians II (HOAC II) A new decision making and documentation
guide in physical therapy. It is to serve as a template for documentation
and as a conceptual model for decision making and therefore, could link documentation and practice.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 57
Rothstein and Echternach (2001)HOAC II
Algorithm presented provide a problem solving approach to clinical decision
Divides patient problems into two categoriesPatient identified problems (PIP):Non patient identified problems
(NPIP):
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 58
Patient Identified problems
Consist of functional limitations and disabilities identified by patient, will often exist when therapist is performing initial evaluation, however these items can also be anticipated by the therapist.
Generated before examination, therefore driven by patient.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 59
Non Patient Identified Problems
Problems that may occur (Risk Factors) or existing problems not expressed by the patient, but found
by therapist.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 60
Rothstein and Echternach (2001)HOAC II
Testing Criteria Used to examine correctness of hypothesis related to
problems that currently exist. Informs us of the level of performance that a patient needs to achieve to eliminate a problem (impairment and functional limitation).
Predictive Criteria Measured for anticipated problems. How long
intervention for prevention should be carried out. A focus on risk factors that lead to corrective hypothesis, reduced risk factors. These are not goals because they are worth achieving only if sufficient evidence indicates that a problems might occur.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 61
Rothstein and Echternach (2001)HOAC II
HOAC II: prevention activities are goal driven and are
planned for specified period of time, therapists can, through use of the algorithm, identify to payers the resources they will need to achieve prevention.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 62
Hypothesis generation
With two types of problems two types of hypotheses are needed (Evidence-Based Preferred or Logic as to the need) Existing Problems Hypotheses: requires
hypotheses about the diagnosis that detail what needs to be changed to eliminate existing problems.
Anticipated Problems: Elimination of risk factors and a case as to what may happen with out intervention.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 63
Anticipated problems
Rational for the intervention to avoid a problem is difficult. Must look to the risk factors and the removal of such. Epidemiological base Augmentative / Logic base with some type of
scientific basis Justification is critical with this type of
problem.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 64
HOAC II Goals
Goals: To base a goal on the change in impairment is almost always inappropriate
Goals should represent meaningful accomplishments. Changes are functional
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 65
HOAC II Goals
The simplest way of checking whether a goal is appropriate Whether the payer would find therapy to be
worthwhile if this is all that is achieved Whether anyone would feel therapy was
worthwhile if this is all that was achieved Commit to a evaluation schedule,
identifiable time lines when status of patient will be checked
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 66
How to make these changes?
Provide measurement tools to clinical personnel and qualify existing documents, training and competencyMake all clinical personnel accountable to documentation requirementsQuality assurance preformed on documentation (Peer Review ¼’ly) with reports and action plans. Included in yearly review
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 67
What impact will be made by improved documentation
Improve the field of physical therapy Improve the quality of care to patients Improve efficiency and effectiveness of
care with closer monitoring Reduce denials for utilization review Add to evidence based practice data base
with published outcomes Provide data to potential clients

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 68
Points to remember
Points to Remember Document all objective data on evaluation
Compare prior level of function to current level Medicare looks at a 90-180 day as the time line.
Link all functional limitations with impairments Re-measure often to determine effectiveness Use measurements that are valid and reliable All goals should be patient centered, realistic and
functional. Good documentation leads to justification of treatments
that leads to improved quality of care to patients
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 69
Valid and Reliable Tests1) Six minute walk test (pulmonary/cardiac)
Olsson L, Swedberg K. Eur Heart J. 2005 Oct;26(20):2209. Epub 2005 Aug 16. 2) DASH (upper extremity)
Deshmukh, AV et al. Total shoulder arthroplasty: Long-term survivorship, functional outcome, and quality of life. J Shoulder Elbow Surg. 2005 Sep-Oct;14(5):471-9.
3) Oswastry (low back)Ostelo, RW, de Vet HC. Clinically important outcomes in low back pain.Best Pract Res Clin Rheumatol. 2005 Aug;19(4):593-607. Review
4) Neck index Wlodyka-Demaillle, S.The ability to change of three questionnaires for neck pain.Joint Bone Spine. 2004 Jul;71(4):317-26.
5) Lower Extremity Motor Coordination TestDesrosiers, J. et al. Validation of a new lower-extremity motor coordination test.Arch Phys Med Rehabil. 2005 May;86(5):993-8.
6) Berg balance (out patient) Paltamaa, J. et al Reliability of physical functioning measures in ambulatory subjects with MS.Physiother Res Int. 2005;10(2):93-109. PMID: 15895347
7) Tinnitte (snf, long term care)Mold, JW et al. The prevalence, predictors, and consequences of peripheral sensory neuropathy in older patients.J Am Board Fam Pract. 2004 Sep-Oct;17(5):309-18.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 70
CMS Documentation Overview

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 71
Triangle of Review
The ICD-9 and CPT code match up CCI edits with CPT codes Documentation:
Functional Objective Test
Valid Reliable

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT72
Medicare Triangle of Justification
ICD-9 CPT codeMatch-upMedical Necessity
CCI Edits
Functional Changes via Documentation of patients Centered Functional Goals

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 73
CMS Documentation Requirements
Documentation required to indicate objective, measurable beneficiary physical function including, e.g., Functional assessment individual item and summary
scores (and comparisons to prior assessment scores) from commercially available therapy outcomes instruments other than those listed above; or
Functional assessment scores (and comparisons to prior assessment scores) from tests and measurements validated in the professional literature that are appropriate for the condition/function being measured; or
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 74
CMS Documentation Requirements Continued
Other measurable progress towards identified goals for functioning in the home environment at the conclusion of this therapy episode of care.
Clinician’s clinical judgments or subjective impressions that describe the current functional status of the condition being evaluated, when they provide further information to supplement measurement tools; and
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 75
CMS Documentation Requirements Cont
A determination that treatment is not needed, or, if treatment is needed a prognosis for return to premorbid condition or maximum expected condition with expected time frame and a plan of care.
Clinician’s clinical judgments or subjective impressions that describe the current functional status of the condition being evaluated, when they provide further information to supplement measurement tools; and
A determination that treatment is not needed, or, if treatment is needed a prognosis for return to premorbid condition or maximum expected condition with expected time frame and a plan of care.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 76
CMS Supporting Documentation
Documentation supporting medical care prior to the current episode, if any, (or document none) including, e.g., Record of discharge from a Part A qualifying inpatient,
SNF, or home health episode within 30 days of the onset of this outpatient therapy episode, or
Identification of whether beneficiary was treated for this same condition previously by the same therapy discipline (regardless of where prior services were furnished; and
Record of a previous episode of therapy treatment from the same or different therapy discipline in the past year.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 77
CMS Supporting Documentation
Documentation required to indicate beneficiary health related to quality of life, specifically, The beneficiary’s response to the following
question of self-related health: “At the present time, would you say that your health is excellent, very good, fair, or poor?” If the beneficiary is unable to respond, indicate why; and
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 78
CMS Supporting Documentation
Documentation required to indicate beneficiary social support including, specifically, Where does the beneficiary live (or intend to live) at the
conclusion of this outpatient therapy episode? (e.g., private home, private apartment, rented room, group home, board and care apartment, assisted living, SNF), and
Who does beneficiary live with (or intend to live with) at the conclusion of this outpatient therapy episode? (e.g., lives alone, spouse/significant other, child/children, other relative, unrelated person(s), personal care attendant), and
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 79
CMS Supporting Documentation
Does the beneficiary require this outpatient therapy plan of care in order to return to a premorbid (or reside in a new) living environment, and
Does the beneficiary require this outpatient therapy plan of care in order to reduce Activities of Daily Living (ADL) or Instrumental Activities of Daily Living or (IADL) assistance to a premorbid level or to reside in a new level of living environment (document prior level of independence and current assistance needs); and
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 80
CMS Supporting Documentation
Progress Note: Timing. The minimum Progress Report Period shall be at least
once every 10 treatment days or at least once during each 30 calendar days, whichever is less.
The day beginning the first reporting period is the first day of the episode of treatment regardless of whether the service provided on that day is an evaluation, re-evaluation or treatment. Regardless of the date on which the report is actually written (and dated),
the end of the Progress Report Period is either a date chosen by the clinician, the 10th treatment day, or the 30th calendar day of the episode of treatment, whichever is shorter.
The next treatment day begins the next reporting period. The Progress Report Period requirements are complete when both the elements of the Progress Report and the clinician’s active participation in treatment have been documented.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 81
CMS Discharge Note
The Discharge Note or Discharge Summary:
is required for each episode of outpatient treatment. In provider settings where the physician/NPP writes a discharge summary and the discharge documentation meets the requirements of the provider setting, a separate discharge note written by a therapist is not required.
The Discharge Note shall be a Progress Report written by a clinician, and shall cover the reporting period from the last Progress Report to the date of discharge.
In the case of a discharge unanticipated in the plan or previous Progress Report, the clinician may base any judgments required to write the report on the Treatment Notes and verbal reports of the assistant or qualified personnel.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 82
Discharge Note
At the discretion of the clinician, the discharge note may include additional information; for example, it may summarize the entire episode of treatment, or justify services that may have extended beyond those usually expected for the patient’s condition.
Clinicians should consider the discharge note the last opportunity to justify the medical necessity of the entire treatment episode in case the record is reviewed. The record should be reviewed and organized so that the required documentation is ready for presentation to the contractor if requested.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 83
Treatment Note
The purpose of these notes is simply to create a record of all treatments and skilled interventions and to record the time of the services in order to justify the use of billing codes on the claim.
Documentation is required for every treatment day, and every therapy service.
The Treatment Note is not required to document the medical necessity or appropriateness of the ongoing therapy services.
Descriptions of skilled interventions should be included in the plan or the Progress Reports and are allowed, but not required daily.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 84
Treatment Note
Non-skilled interventions need not be recorded in the Treatment Notes as they are not billable.
However, notation of non-skilled treatment or report of activities performed by the patient or non-skilled staff may be reported voluntarily as additional information if they are relevant and not billed.
Specifics such as number of repetitions of an exercise and other details included in the plan of care need not be repeated in the Treatment Notes unless they are changed from the plan.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 85
Treatment NoteIntervention
Documentation of each Treatment shall include the following required elements:
Date of treatment; and
Identification of each specific intervention/modality provided and billed, for both timed and untimed codes, in language that can be compared with the billing on the claim to verify correct coding. Record each service provided that is represented by a timed code, regardless of whether or not it is billed, because the unbilled timed services may impact the billing; and

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 86
Treatment Note Time Codes
Total timed code treatment minutes and total treatment time in minutes. Total treatment time includes the minutes for timed code treatment and untimed code treatment.
Total treatment time does not include time for services that are not billable (e.g., rest periods). For Medicare purposes, it is not required that unbilled services that are not part of the total treatment minutes be recorded, although they may be included voluntarily to provide an accurate description of the treatment, show consistency with the plan, or comply with state or local policies.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 87
Treatment Notes and Timed Codes
The amount of time for each specific intervention/modality provided to the patient may also be recorded voluntarily, but contractors shall not require it, as it is indicated in the billing.
The billing and the total timed code treatment minutes must be consistent. See Pub. 100-04, chapter 5, section 20.2 for description of billing timed codes; and
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 88
Treatment NoteSignature
Signature and professional identification of the qualified professional who furnished or supervised the services and a list of each person who contributed to that treatment (i.e., the signature of Kathleen Smith, PTA, with notation of phone consultation with Judy Jones, PT, supervisor, when permitted by state and local law).
The signature and identification of the supervisor need not be on each Treatment Note, unless the supervisor actively participated in the treatment.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 89
Treatment Notes Signature
Since a clinician must be identified on the Plan of Care and the Progress Report, the name and professional identification of the supervisor responsible for the treatment is assumed to be the clinician who wrote the plan or report. When the treatment is supervised without active participation by the supervisor, the supervisor is not required to cosign the Treatment Note written by a qualified professional.
When the responsible supervisor is absent, the presence of a similarly qualified supervisor on the clinic roster for that day is sufficient documentation and it is not required that the substitute supervisor sign or be identified in the documentation.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 90
Treatment NoteModification to POC
If a treatment is added or changed under the direction of a clinician during the treatment days between the Progress Reports, the change must be recorded and justified on the medical record, either in the Treatment Note or the Progress Report, as determined by the policies of the provider/supplier.
New exercises added or changes made to the exercise program help justify that the services are skilled. For example: The original plan was for therapeutic activities, gait training and neuromuscular re-education. “On Feb. 1 clinician added electrical stim. to address shoulder pain.”
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 91
Treatment note Modification to POC
Documentation of each treatment may also include the following optional elements to be mentioned only if the qualified professional recording the note determines they are appropriate and relevant. If these are not recorded daily, any relevant information should be included in the progress report. Patient self-report; Adverse reaction to intervention; Communication/consultation with other
providers(e.g., supervising clinician, attending physician, nurse, another therapist, etc.);
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 92
Treatment Notes and Modification to POC
Significant, unusual or unexpected changes in clinical status;
services that are not part of the total treatment minutes be recorded, although they may be included voluntarily to provide an accurate description of the treatment, show consistency with the plan, or comply with state or local policies. The amount of time for each specific intervention/modality provided to the patient may also be recorded voluntarily, but contractors shall not require it, as it is indicated in the billing. The billing and the total timed code treatment minutes must be consistent. See Pub. 100-04, chapter 5, section 20.2 for description of billing timed codes
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 93
MODIFIERSNCCI #59 Modifier
Medicare Cap KX modifier
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 94
59 Modifier Use
Under certain circumstances, the physician may need to indicate that a procedure or service was distinct or independent from other services performed on the same day. Modifier 59 is used to identify procedures/services that are not normally reported together, but are appropriate under the circumstances.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 95
59 Modifier
NCCI edits define when two procedure HCPCS/CPT codes may not be reported together except under special circumstances.
For the NCCI its primary purpose is to indicate that two or more procedures are performed at different anatomic sites or different patient encounters.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 96
59 Modifier Use Example: Column 1 Code/Column 2 Code
97140/97530 CPT Code 97140 – Manual therapy techniques
(eg, mobilization/manipulation, manual lymphatic drainage, manual traction), one or more regions, each 15 minutes
CPT Code 97530 – Therapeutic activities, direct (one-on-one) patient
contact by the provider (use of dynamic activities to improve functional performance), each 15 minutes
Policy: Mutually exclusive procedures Modifier -59 is:
Only appropriate if the two procedures are performed in distinctly
different 15 minute intervals. The two codes cannot be reported together if
performed during the same 15 minute time interval.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 97
Medicare Cap KX
Use the KX modifier only in cases where the condition of the individual patient is such that services are APPROPRIATELY provided in an episode that exceeds the cap.
Routine use of the KX modifier for all patients with these conditions will likely show up on data analysis as aberrant and invite inquiry. Be sure that documentation is sufficiently detailed to support the use of the modifier.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 98
KX Modifier
COMPLEXITIES are complicating factors that may influence treatment, e.g., they may influence the type, frequency, intensity and/or duration of treatment.
Complexities may be represented by diagnoses (ICD-9 codes), by patient factors such as age, severity, acuity, multiple conditions, and motivation, or by the patient’s social circumstances such as the support of a significant other or the availability of transportation to therapy.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 99
KX Documentation of Complexity of patients status and rehabilitative potential
Documentation supporting illness severity or complexity including, e.g.,
Identification of other health services concurrently being provided for this condition (e.g., physician, PT, OT, SLP, chiropractic, nurse, respiratory therapy, social services, psychology, nutritional/dietetic services, radiation therapy, chemotherapy, etc.), and/ or
Identification of durable medical equipment needed for this condition, and/or Identification of the number of medications the beneficiary is talking (and type if known); and/or

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 100
KX Documentation of Complexity of patients status and rehabilitative potential
If complicating factors (complexities) affect treatment, describe why or how. For example: Cardiac dysrhythmia is not a condition for which a therapist would directly treat a patient, but in some patients such dysrhythmias may so directly and significantly affect the pace of progress in treatment for other conditions as to require an exception to caps for necessary services. Documentation should indicate how the progress was affected by the complexity. Or, the severity of the patient’s condition as reported on a functional measurement tool may be so great as to suggest extended treatment is anticipated; and/or
Generalized or multiple conditions. The beneficiary has, in addition to the primary condition being treated, another disease or condition being treated, or generalized musculoskeletal conditions, or conditions affecting multiple sites and these conditions will directly and significantly impact the rate of recovery; and/or.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 101
KX Documentation of Complexity of patients status and rehabilitative potential
Mental or cognitive disorder. The beneficiary has a mental or cognitive disorder in addition to the condition being treated that will directly and significantly impact the rate of recovery; and/or.
Identification of factors that impact severity including e.g., age, time since onset, cause of the condition, stability of symptoms, how typical/atypical are the symptoms of the diagnosed condition, availability of an intervention/treatment known to be effective, predictability of progress.

04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 102
KX Documentation of Complexity of patients status and rehabilitative potential
Mental or cognitive disorder. The beneficiary has a mental or cognitive disorder in addition to the condition being treated that will directly and significantly impact the rate of recovery; and/or.
Identification of factors that impact severity including e.g., age, time since onset, cause of the condition, stability of symptoms, how typical/atypical are the symptoms of the diagnosed condition, availability of an intervention/treatment known to be effective, predictability of progress.
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 103
References1) Nagi, S. Disability concepts revisited: implication for prevention. In: Pope AM, Tarlov
AR, eds. Disability in America: Toward a National Agenda for Prevention. Washington, DC: National Academy Press, 1991.
2) Guide to Physical Therapy Practice. 2nd ed. Physical Therapy. 2001;81:9-744.3) Jette AM. Physical disablement concepts for physical therapy research and practice.
Phys Ther. 1994;74:380-386.4) Ware JE Jr, Sherbourne CD. The MOS 36-item short form health survey (SF-36), I:
conceptual framework and item selection. Med Care. 1992:30:473-483.5) Roland M, Morris R. A study of the natural history of back pain, part 1: development
of a reliable and sensitive measure of disability in low back pain. Spine. 1983;8:141-144.
6) Stratford PW, Binkley JM, Solomon P, et al. Defining the minimum level of detectable change for the Roland-Morris questionnaire. Phys Ther. 1996;76:365.
7) International Classification of Impairments Disabilities and Handicaps. Geneva, Switzerland, World Health Organization, 1980.
8) Moorhead, JF, Clifford, J. Determining Medical Necessity of Outpatient Services. American College of Medical Quality. 1992;7(3);81-4.
9) Cyriax, J. The advantage of accurate treatment. Physiotherapy. 1952 Jan;38(1):3-810) Zitsmann, SL. Utilization Management of Worker’s Compensation: Out patient
Therapy. JHQ:1993;15(3):34-7. 11) http://www.rehabmeasures.org/default.aspx
04/15/2023 Dr. Charles Curtis MS, PT,DPT, MDT 104
Contact InformationDr. Charles Curtis MS, PT, DPT, MDT33 Orchard Place Little Silver, NJ [email protected]