Embed Size (px)
Citation preview

Publié par : Published by: Publicación de la:
Faculté des sciences de l’administration Université Laval Québec (Québec) Canada G1K 7P4 Tél. Ph. Tel. : (418) 656-3644 Télec. Fax : (418) 656-7047
Édition électronique : Electronic publishing: Edición electrónica:
Aline Guimont Vice-décanat - Recherche et affaires académiques Faculté des sciences de l’administration
Disponible sur Internet : Available on Internet Disponible por Internet :
http://www5.fsa.ulaval.ca/sgc/documentsdetravail [email protected]
DOCUMENT DE TRAVAIL 2009-007
MODELING THE INFORMATION ARCHITECTURE OF THE QUEBEC HEALTHCARE NETWORK Daniel PASCOT Faouzi BOUSLAMA Sehl MELLOULI
Version originale : Original manuscript: Version original:
ISBN – 978-2-89524-333-5
Série électronique mise à jour : On-line publication updated : Seria electrónica, puesta al dia
02-2009

Modeling the Information Architecture of the Quebec
Healthcare Network
Daniel Pascot∗, Faouzi Bouslama†and Sehl Mellouli‡
Management Information Systems Department, Université Laval
Abstract
This paper shows the implementation of the Corporate Conceptual Data Model (CCDM)-basedmethodology to create a stable and coherent information architecture of the Quebec informationhealthcare system. The CCDM-based approach shows how to build the stable pivot on the commonpart of the information architecture of this highly complex system. The information architecturewhich is built around the knowledge of the Quebec health domain is based on three core organisa-tional concepts: Field actions, the CCDM global model, and Views of sub-schemas of the CCDM.The �eld actions capture the essential data elements representing the persistent healthcare infor-mation of the reality on the ground. They are considered the key reusable components of theprocess architecture. The global data model provides a holistic view of information in the health-care knowledge domain. The sub-schemas are subsets of the CCDM that model information fordi�erent health stakeholders. The results of implementation using the Silverrun data and businessmodeling tool are provided. This information architecture allows the Quebec healthcare organi-zation to understand its complexities, contribute to the alignment of its business strategies andimplementations in order to better serve the citizens of Quebec, and monitor its transformationand evolution.
1 Introduction
The increasing use of information technologies to manage the many aspects of transformations inhealthcare organizations has resulted in the creation of a multitude of applications and informationsystems. Many of these applications and systems have been created in silos over the years where eachapplication had its own development life cycle. There was no common vision nor a common referentialor repository. Moreover, many of these applications were developed in the absence of standards andnorms, and shared technological orientations.
As implications to this historical development, there was a lack of interoperability between thehealthcare information systems. Healthcare providers and managers using those systems have wit-nessed a proliferation of data sources and technological infrastructures. The health knowledge was notcumulative as a result of this vertical transformation, and the processes of information sharing andsystems integration have been largely hindered. In addition to these implications, healthcare organi-zations have been witnessing an organizational development much slower than the technological pace
∗Faculty of Business Administration, Pavillon Palasis-Prince, 2325 rue de la Terasse, local 2507 Université Laval,Quebec (QC) G1V 0A6, Canada. [email protected]†[email protected]‡[email protected]
1

of changes. In fact, the lifespan of hardware or software to catalogue suppliers is just few years whilethe lifetime of critical healthcare applications is in the order of several tens of years. As a consequenceof these challenges, healthcare organizations are nowadays facing an ever increasing volume of com-plexity, ine�ciency, and rigidity. In fact, they are in search of solutions and best practices to modeland understand their transformations-related complexities. These solutions are expected to allow themanagement and evolution of healthcare applications, and the control over the organization's globalmodel of information and pace of changes.
In an earlier paper [1], the authors proposed a solution based on an enterprise architecture havinga Corporate Conceptual Data Model (CCDM) as its hub, and using a two-track information systemdevelopment cycle. The CCDM-based solution is able to create information architectures that areexpected to cope well with the above mentioned complexities and challenges. The solution provides aholistic view and a mechanism to design, develop, communicate and understand complex enterprisessuch as the Quebec healthcare organization. It is designed to organize all the created and communicatedinformation in order to secure progressively, in terms of information, consistency of all operational andmanagement information levels systems. The enterprise architecture framework was based on threecore organisational concepts: Field Actions (FAs) [2], a Corporate Conceptual Data Model (CCDM)[4], and Views as subsets of the global model[4].
This paper shows how to apply the CCDM-based methodology to create a common conceptualreferential and a stable information architecture for the Quebec healthcare network. The �rst step inbuilding this architecture is to identify the FAs that are used to capture the persistent information ofthe reality on the ground. This involves any action, decision or event involving one or several partiesor players in the Quebec healthcare organization. These FAs can be described independently of anyparticular business process and constitute the reusable elements in the process architecture. The secondstep in the solution consists of building a global data model that is called the CCDM for the entireQuebec health network. The CCDM [15] which has only the main entities and attributes commonto several health information systems is created to provide a holistic view of the information in thisorganization. To model the interest of the many stakeholders in this large and complex network, viewsor sub-schemas of the CCDM are used. To create the articfacts of the information architecture, theSilverrun and the Open ModelSphere data and business modeling tools are used. A coupling mechanismis developed in Silverrun and used to map logical data models with their conceptual counterparts. Thegraphical representation of the global data model can be very complex. To manage these complexities,a new concept called Rubrics is used to simplify this data model since details about entities in theCCDM can be expressed only in their particular context.
The rest of the paper is organized as follows. Section 2 recalls the main steps in the CCDM-based methodology used in the creation of the information architecture for the Quebec healthcarenetwork. Section 3 introduces the Quebec healthcare network. Section 4 presents the results of theimplementation with artifacts in each of the design steps including FAs, the CCDM, and the views.Finally, Section 5 is the conclusion.
2 The CCDM-based approach
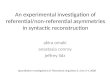
In [1], the authors proposed a methodology to create an information architecture that copes well withtransformations-related complexities of large and complex organizations, and which can guarantee theirpresent operation and future evolution. The methodology is data-driven approach that is based ona corporate conceptual data model (CCDM) that represents the hub of the information architecture.This information architecture is part of a proposed enterprise architecture shown in Figure 1 whichincludes a business and a system architecture respectively.
There are three core organizationnel concepts used to build this architecture. These are the FieldActions or FAs, a CCDM, and Views. The �eld actions are the key reusable components in thearchitecture and they serve as the building blocks for the various business processes in the organization.These �eld actions which capture the persistent information of the reality on the ground are used as
2

System Architecture(SA)
Business Architecture(BA)
Information Architecture(IA)
ServicesView
Services
Services
Services
Services (SOA)
HL7 v2 or v3
Messages
DB
DB
DB
Existing Systems
CCDM
Business Process Mapping
FieldActions
BusinessLayer
FunctionalLayer
System Layer(Software & Technology)
Process Diagrams
Field Actions
View
Process View
MessagesView
Systems View
many-to-many relationship iterative
Figure 1: The enterprise architecture framework for the Quebec health network.
generators of essential data that are being exchanged between the business processes in order to createthe required services and products.
The �rst step in the CCDM-based approach is to identify those �eld actions and then to extract allthe primary data that they represent. The primary data will make up the entities in the global concep-tual data model, or the CCDM, which represents the knowledge of the domain under consideration[4].In this paper, the �eld actions will represent any action, decision, or events involving parties such asPatient, Practitioners, Healthcaregiver, Parmacist, Nurse, Etc. In fact, these actions can be describedindependently of any particular business process. A catalogue of all the FAs is then established, andthese FAs within the corporate conceptual data model or CCDM give a coherent and global infor-mation model. The second step in the methodology consists of creating the CCDM [15] to providea holistic view of the healthcare information. The CCDM is a high level data model where only themain healthcare entities and attributes common to several healthcare information systems are de�ned.Finally, the third step consists of building subsets of the global model or views to represent the infor-mation that is of interest to a particular stakeholder in the network such as a business view, a systemview or a message view. In this framework, the CCDM is at the heart of the information architectureof an organization. It can be considered as a switching platform that connects the various models thatconstitute the information architecture.
The development process of the information systems then follows an iterative and incrementaltwo-track Y-model as was suggested by the authors in an earlier paper. This development processfollows a functional and a technical path, respectively, as shown in Figure 2. It stresses the initialnon-correlation between the two paths to ensure a certain degree of their mutual independance. Then,the two track merge for the design of the computer-based information system. The initial subdivision
3

allows both to capitalize on the business knowledge on the left arm and reuse the technical know-howon the right arm. The right part captures the functional requirements to produce a model focused onthe needs of business users. Based on the analysis of this part of the model, it is possible to assess in anearly stage the risk of producing a system unsuited for business users. Consequently, developers willbe able to consolidate the speci�cations and verify their coherence and completeness. This analysis isindependant of any particular technology.
Figure 2: The two-track Y-model development cycle for CBIS.
The right arm of the Y model, known as 'Engineering Tools and Technical Needs', is used to capturethe technical needs including the software architectures, frameworks, operating systems, programminglanguages, libraries, and utilities necessary for the design and implementation of the information sys-tems. This part of the Y model helps identify all the constraints and choices a�ecting the system'sdesign independently of the functional aspects. It aims at standardizing and reusing the same mecha-nisms for one system. The central arm of the Y model which is called 'CBIS Development' representsthe phases for the development of computer-based information systems. This part includes a prelimi-nary design phase which integrates the analysis model in the technical architecture in order to picturethe system components to develop, the detailed system design showing how to achieve each component,software coding, and �nally testing and validation.
The CCDM-based methodology and the two-track Y-model for system development are appliedto create the information architecture of the Quebec healthcare network as detailed in the followingsections.
3 The Quebec healthcare network
The Quebec health and social services ystem is a very complex network of eighteen regional authoritiesor agencies, 4000 community organisms such as private clinics, and 95 centres for health and socialservices (CSSS) such as hospitals and readaptation centres, and whose aim is to maintain, improve, andrestore the health and well-being of all citizens of the Quebec Province in Canada [20]. The Quebechealth and social services system has approximately 300 institutions providing a set of integrated health
4

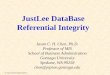
as well as social services in more than 1700 service points. The agencies are in charge of coordinatingand inplementing health and social services with regard to funding, human resources deployment, andthe access to specialized services in their respective regions. The CSSS centres are a merger of localcommunity centres (CLSCs), residential and long-term care centres (CHSLDs), and hospital centre(CHs) as depicted in Figure 3.
Physicians
(GMF, Medical Clinics)
Social Economy Entreprises
Private Resources
Community-Based
Pharmacies
Community Organizations
Non-Institutional Resources
Hospital Centres Youth Centres Rehabilitation Centres
Other Activity
Sectors: School,
Municipal, etc.
HEALTH AND SOCIAL
SERVICES CENTRE
Grouping of one or more
CLSC, CHSLD and CH
Figure 3: The Quebec network of health and social services (Source: MSSS).
A system of this complexity can not be rethought in a context of re-engineering. One has to knowhow to accompagny the evolution of this system and �nd the proper tools to accomplish that. Inorder to achieve this goal, the CCDM-based approach has been applied to the modeling of the Quebechealth care system where it is expected to provide a global view of information and a mean to manageits complexities and evolution, while urbanizing its complex network of services. The MSSS has beenworking for a few years now with a goal to develop and maintain a coherent vision of the digitizationof its network of health and social services. The proposed CCDM-based approach is implemented tocreate a proper and coherent information architecture of this organization.
In the domain of health informatics, the use electronic healthcare records facilitates the creation andsharing of information about patients. The elctronic records are used to help coordinate the storageand retrieval of individual patient's medical record among physician practices and other stakeholdersin any healthcare system. The computerization of health records' contents and their associated pro-cesses is expected to improve the management of patients' personal data with regard to their healthcondition[21] [22]. The information systems when used by physicians in the form of software plat-forms are expected to increase the physicians' e�ciency and reduce service costs while streamliningthe health delivery processes [23]. However, the implementation of this technology requires the carefulconsideration of many factors such as the transition and integration of the physical data into electronicform, and the ability of health information systems to consolidate geographically dispersed medicalrecords.
In the case of the healthcare in the Province of Quebec, the information systems are made upof electronic medical records that are distributed over many healthcare systems in many dispersedlocations over the province. To be able to share the enormous amount of generated data between thedi�erent healthcare systems, the electronic records are designed in a uniform and a consistent way.Having a proper and coherent information architecture is therefore important for the Quebec healthcaresystem. Moreover, electronic records are subject to data standards which are necessary to homogenizethe coding of concepts used to describe those records, especially for the sharing of patients' databetween di�erent systems and jurisdictions at the pan-Canadian level. Health standards, such as HL7
5

V3 messaging (Health Level 7) [24], SNOMED CT (Systematized Nomenclature of Medicine ClinicalTerms) [25]and LOINC (Logical Observation Identi�ers Names and Codes) vocabulary [26], and otherexternal information lay the foundation for interoperable healthcare information systems that de�nethe electronic data transaction and the healthcare set of standard codes. All of this information isneeded and is expected to be modeled and integrated in the overall data model.
4 Building the Quebec healthcare information systems archi-
tecture
The development of the information architecture for the Quebec healthcare system is initiated withthe identi�cation of the FAs which are later combined to form the overall conceptual data model orthe CCDM. To identify the FAs, business process mapping techniques can be used or an investigationof the reality on the ground can also lead to their identi�cation.
4.1 Identifying the �eld actions
In the information architecture of the Quebec healthcare system, an FA is an action, decision or anevent involving one or more caregivers which contributes signi�cantly to the achievement of a businessprocess but which can be described independently of this particular business process. This FA isuniform and takes place in a unit of time and place. Prescribing a drug, taking a blood sample, adiagnosis, an examination of a diagnostic imaging can all be considered as �eld actions.
There are three prerequisites for an activity to be considered an a FA:
• The activity must generate information relevant to the achievement of a clinical or social services;
• This information must be su�ciently persistent to be registered; and
• The activity must represent the reality on the ground of the action and not from an IT perspective.
The same FA can be found in several business processes, and each business process may have morethan one FA.
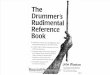
Each FA is associated with both a descriptive form and a view of the action or a data model.The description form [27] of the FA contains secondary information in support of the FAs. Theseare the metadata of the action. They include entries such as the name of the FA which should begeneric enough to be reusable and su�ciently precise to be recognized by people on the ground, astandard code of the FA, and the de�nition of the FA which identi�es the main actor as well as otherinformation. Figure 4 shows an example of a descriptive form and the corresponding conceptual datamodel. The data model is created using the Silverrun data and business process modeling tool. Thegraphical representation is an entity-relationship diagram.
A list of FAs in the information architecture is therefore formed, and this list is maintained alongwith the CCDM. This gives a coherent and global information model of the reality on the ground of theQuebec healthcare system. An FA is consequently a sub-schema of the CCDM where a sub-schemacan be de�ned as a subset of a parent schema. The sub-schema is therefore composed of relationsand connectors taken exclusively from the parent schema. For example, the Vaccination FA containsconcepts such as 'Caregiver', 'Contact', and 'Patient'. These concepts are also present in other FAs andare consequently constantly reused. However, some other concepts such as 'Vaccination Equipment'and 'Vaccination' are very speci�c to the Vaccination FA. In an FA, only entities and attributes speci�cto the context are available. As for the CCDM, it contains entities and attributes that are taken fromevery FA. Therefore, it is by integrating every FA in a common model that it is possible to manageand construct a global model for the Quebec healthcare system. The CCDM can actually be seen asthe aggregate of all the FAs.
6

Code de l'action terrain
(Field Action Code)RCAI_AT000002QC01
Nom de l'action terrain
(Field Action Name)Prescription médicament
Définition (Definition)
Une prescription est une recommandation écrite faite par le médecin, s'adressant à un usager afin que ce dernier puisse acquérir des médicaments. Le médecin peut prescrire soit un médicament ou une dénomination commune. Dan ce cas, le pharmacien choisit le médicament à délivrer en fonction de la dénomination commune identifiée.
Acteur principal (Main Actor) Médecin
Autres acteurs (Other Actors) Intervenant, Pharmacien, Usager
Intrants/Déclencheurs (Inputs/Initiators)
Rencontre médecin, Rencontre intervenant
Documents de référence (Reference Documents)
"Architecture préliminaire des systèmes d'information sur les médicaments-Livrable 5 version préliminaire", Régie de l'Assurance Maladie du Québec, 25 février 2005.
Aspect légal (Legal Aspect) Contraintes de la loi 83
Exemple (Example) À venir
1
USAGER
Identifiant usager
NAM usager
Nom usager
Prénom usager
Date expiration NAM usager
Sexe usager
Provenance NAM usager
Date naissance usager
Curatelle usager
Usager jumeau identique?
Initiale
Suffixe
Préfixe
Langue de communication
Assurabilité RAMQ
UNITÉ SERVICE
Identifiant unité service
Description unité service
Code comptabilité
FK Identifiant organisation dispensatrice service
MEDICAMENT
DIN médicament
Nom médicament
Forme médicament
Catégorie médicament
Médicament origine-générique ?
Voie normale administration médicament
Date expiration brevet médicament
VACCIN
INTERVENANT
Identifiant Intervenant
Numéro inscription RAMQ intervenant
Nom intervenant
Prénom intervenant
Coordonnées professionnelles intervenant
Numéro licence
Numéro interne médecin
Abréviation médecin
Droit de pratique ( à vérifier )
Numéro de résident (médecin)
MOLÉCULE
Code DCI
Nom dénomination commune
Dénomination scientifique
CONTACT
Identifiant contact
Date et heure début contact
Date et heure fin contact
Durée effective contact
Raison contact
Type contact
Lieu contact
FK Identifiant usager
FK Identifiant Intervenant
FK Identifiant unité service
FK Identifiant organisation dispensatrice service
ORGANISATION DISPENSATRICE SERVICE
Identifiant organisation dispensatrice service
Nom organisation dispensatrice service
Coordonnées principales organisation dispensatrice
service
COMPOSITION MÉDICAMENT
FK DIN médicament
FK Code DCI
Quantité composition médicament
Teneur médicamentPRESCRIPTION
Identifiant prescription
Type prescription
Date et heure prescription
Posologie prescription médicament
Montant prescription médicament
Prescription substituable ? médicament
Prescription renouvelable ? médicament
Durée prescription médicament
Indicateur PRN prescription médicament
Intention thérapeutique médicament
FK Code DCI
FK DIN médicament
FK Identifiant contact
1,1 0,N
1,10,N
0,1
0,N
0,1
Contexte organisationnel0,N
1,1
Rattachement
0,N
1,1
1,N
1,10,N
0,1
Molécule prescrite
0,N
1,1Contact origine de prescription
0,N
0,1Prescription médicament
0,NNom du schéma
Créateur Version
Créé le Modifié le
MCCD 6/RCAI_AT000002QC01
DAAOT MSSS Québec Prescriptio…
2002-07-17 2007-12-07
Figure 4: Descriptive form and data model of the Medication Prescription FA.
If there is a need to construct a data model for a particular information system within the Quebechealthcare system, it is possible to easily isolate only the FAs that are relevant to the system underinvestigation out of the overall list of all FAs included in the CCDM. Here, the corresponding businessprocesses can be used to identify which events are relevant to the project. For example, Figure 5 showsthe RSIPA project at the Quebec healthcare system with its seven business processes. RSIPA is aninformation system that will be used to manage integrated services given to autonomy loosing personsin Quebec.
What is important to understand is that for every identi�ed business process such as Evaluationand Inscription, there will be a corresponding FA, either taken from the CCDM or created speci�callyfor RSIPA, and eventually added to the CCDM. Therefore, during this procedure, business processesare �rst identi�ed independently of existing FAs. Afterwards, existing FAs are selected in the CCDM.If a corresponding FA does not exist in the CCDM, then there is a need to create it. To add the FAto the CCDM, the information architect can either use existing concepts from the CCDM or createnew ones as needed. The FA will then be integrated to the global model and can be reused and laterupdated and improved. When all the necessary FAs have been identi�ed, the analyst can integratethem altogether and create a sub-schema of the CCDM which will be speci�c to the project at hands.In the case of RSIPA, the sub-schema will contain every FA related to the business processes of Figure5. This helps guarantying a high degree of coherence between projects since every concept comes fromthe CCDM and is eventually integrated to it.
4.2 Creating the CCDM of the Quebec healthcare system
The second step in the approach is to build the global data model or CCDM. The CCDM providesa global view of information for the entire Quebec healthcare system. This model uniquely refers toprimary data that describe components such as Patients, Caregivers (physicians, nurses), Hospitals,and real life events such as a Diagnosis, a Prescription, and a Medical exam. The CCDM contains arepresentation of the main actors and actions that can generate data in the Quebec healthcare systemand shows how these components can interact with each other.
Figure 6 shows a graphical representation of CCDM of the Quebec healthcare system representedas entity-relationship in the the Silverrun modeling tool. The model is being developed at the DAAOT(Direction Adjointe à l'Architecture et aux Orientations Technologiques) at the Ministry of Health andSocial Services of Quebec (MSSS) [16]. This graphical representation shows the entities encountered inthe healthcare domain, their attributes and the semantic associations and their cardinalities between
7

Field Action
Field Action
Field Action
Field ActionCCDM
Graphical
CCDM
Bu
sin
ess
Layer
Fu
nc
tio
na
l L
ay
er
Access Profile Links Consent User Register DSEIQ
RSIPA
{FA}
SIRTF
SIGDU
SICDU
SICDP
ADT
SICHELD
I-CLSC
SICRA
INFO SANTÉ
INFO SANTÉ
SICRA
I-CLSC
SICHELD
ADT
SICDP
SICDU
SIGDU
SIRTF
SIRTF
Autonomy Evolutive Profile
Healthcare tableShort-term
Healthcare Autonomy Evaluation
Autonomy Multi-client Evaluation
Contact Set Up
Allocation and Intervention Service Plan
Locate Act
Inscription
Service Requirement
Assignment
Follow-up Management
Planification Evaluation
Co
nc
ep
tua
l
Da
ta M
od
els
Lo
gic
al D
ata
Mo
de
ls
CDM Project
Existing Systems’ CDM
CDM Processes
Logical ModelsCoupling
Figure 5: Business processes and IA for RSIPA project (Source: MSSS).
those entities [17].In this information architecture, the CCDM is used to select concepts which are relevant to a speci�c
project. When it is necessary to model a particular healthcare information system, only parts of theCCDM will be used. However, there are common subsets of entities found in nearly all healthcarecontexts such as a PATIENT (French: USAGER). This is shown in yellow color. Other commonconcepts such a CONTACT (shown in dark green color), a PRESCRIPTION (in purple color), andCLINICIAN (French: INTERVENANT) shown in light green color. All of these subsets constitute thereusable part in every system.
Figure 7 shows a subset of the CCDM representing a Conceptual Data Model (CDM) for the i-CLSCinformation system. The i-CLSC keeps track of the CLSC (Local Centre for Community Services)clients and the provided services, and supports the activities of physicians as well as managers of aCLSC.
The Quebec healthcare global model of information is therefore composed of two di�erent subsets:a common subset and a context-dependent subset. The common subset includes entities and relationswhich exist in almost any operational domain (e.g. CAREGIVER, PATIENT, CONTACT, etc.);and the context dependant subset has the entities which are speci�c to a particular context (e.g.VACCINATION, PUBLIC HEALTH, DRUG PRESCRIPTIONS, etc.). The CCDM, therefore, givesa view of the entire information domain while showing how di�erent the subparts are interrelated. ThisCCDM-based method allows to constantly reuse the common concepts while still having a satisfyinglevel of granularity to �t di�erent speci�c healthcare domains.
8

1
OBSERVATION
ASSIGNATIONINTERVENTION
ADMINISTRATION
PROTOCOLE
CODE DIAGNOSTIC (2/2)
INSCRIPTIONUNITÉ
NAISSANCE (1/2)
INSCRIPTIONINSTALLATION
OBSERVATIONNORMEE
DIAGNOSTIC (1/3)
AFFECTATION
SPECIALITÉMÉDECIN
INTERVENANT (4/7)
UNITE SERVICE (1/5)
USAGER (1/6)
TRANSFERT
REGROUPEMENTRENCONTRE
CONTACT GROUPÉ (2/4)
EQUIPEMENT (1/3)
FOURNITURE
STOCKFOURNITURE
CONSOMMATIONFOURNITURE
CONSOMMATION FOURNITURE RENCONTREGROUPÉE
NORME (2/4)
RÉFÉRENCEINSTITUTION
PERMIS
MISSION CLASSE TYPE
DÉTAIL PERMIS
PHARMACIE
DEMANDEREMBOURSEMENT
AIDETECHNIQUE
LIVRAISON AIDETECHNIQUE
ÉVÉNEMENT CARRIÈREMEDECIN
PLAN TRIENNALMINISTÉRIEL
PREM RÉGION
RÉPARTITIONPREM
MEDICAMENT (1/2)
FABRICANT (1/2)
MOLÉCULE
INTERACTION
LIT
RELATIONMÉDECIN
CODE DIAGNOSTIC (1/2)
INDICATION
CONTACT GROUPÉ (3/4)
COMPOSITION MÉDICAMENT(1/2)
HIÉRARCHIETERRITOIRE
TYPE ÉLÉMENTTERRITORIAL
ÉLÉMENT TERRITORIAL(2/3)
SUBSTITUTION MÉDICAMENT(1/2)
DÉLIVRANCE
SPECIMEN
CENTREACTIVITÉ
COMPTE
IMPUTATION
EMPLOI
LOCAL
INTERVENANT (5/7)
EQUIPECLINIQUE LOCALISATION ORGANISATION
(1/2)
TYPE STRUCTURECORRESPONDANCE CENTRE
ACTIVITÉ
CORRESPONDANCEINTERVENTION
MEMBREÉQUIPE
INSCRIPTIONGMF
ADOPTION
PARTICIPATION
PROGRAMME (1/2)
REALISATIONINTERVENTION
PRÉLÈVEMENT
RESULTAT ANALYSE LABORATOIRE
DRG
TRANSPORT
UNITÉRESSOURCE
AFFECTATIONPRÉHOSPITALIÈRE
ORGANISATION DISPENSATRICE SERVICE(3/5)
NORME (1/4)
ORDREPROFESSIONNEL
CODEINTERVENTION
TYPE HIERARCHIE(1/2)
USAGER (2/6)
DEMANDE SERVICE (1/2)
ÉVALUATION
PROBLÈME
SOURCE
TYPE SOURCE
OBJECTIF
PLANIFICATION INTERVENTION(1/2)
COORDINATION (1/2)
TRANSFERTDEMANDE
CONTACT (6/9)
INTERVENANT (3/7)
UNITE SERVICE (2/5)
CONTACT (5/9)
APPEL
CONTACT (4/9)
RENDEZ-VOUS (2/2)
SÉJOUR INSTALLATION
RAPPORT OBSERVATION
RAPPORT IMAGERIEDIAGNOSTIQUE
EXAMEN
IMAGERIEDIAGNOSTIQUE
CORRESPONDANCENORME
SOMMAIREINTERVENTION
CONTRE-INDICATIONUSAGER
CONTRE-INDICATION(1/2)
TYPE ALLERGIE
PERSONNE CONTACT(1/2)
ORGANISATION DISPENSATRICE SERVICE(4/5)
CATÉGORIE INTERVENANT(1/2)
SÉJOUR UNITÉ
SÉJOURURGENCE
CONTACT (7/9)
ACCIDENT
AGENT ALLERGÈNE (1/2)
ÉQUIPEMENT REQUIS RENCONTRE MÉDICALEGROUPÉE
ÉQUIPEMENT REQUISCONTACT
DON DE SANGPRODUIT SANGUIN
TRANSFUSION (1/2)
SÉJOUR ÉTRANGER
COMPOSITIONPROTOCOLE
ADRESSE TELECOMMUNICATIONUSAGER
CONTACT (8/9)
DEMANDEADMISSION
DEMANDE SÉJOUR
TYPE PRODUITSANGUIN
RENDEZ-VOUS (1/2)
ASSIGNATIONINTERVENANT
PLANIFICATION INTERVENTION(2/2)
TRANSFUSION (2/2)
CONSENTEMENT ACCÈS ÀL'INFORMATION
INTERVENANT (6/7)
STATUT INTERVENANT
CATÉGORIE INTERVENANT(2/2)
ADRESSE USAGER
PLAN D'INTERVENTIONS(1/2)
SERVICE
SERVICES DUPROGRAMME
USAGE TELECOMMUNICATIONUSAGER
EQUIPEMENT (2/3)
RAPPORTENQUETE
ORDONNANCECOUR
LOT VACCINS
LOCALISATION LOT VACCINS
FOURNISSEUR LOTVACCIN
FOURNISSEUREQUIPEMENT
ENQUETE SANTEPUBLIQUE
ELEMENT DESCRIPTIF ENQUETE SANTEPUBLIQUE
CORRESPONDANCEDIAGNOSTIC
ACTE VACCINATION (1/2)
FABRICANT (2/2)
CONTRE-INDICATION(2/2)
ORGANISATION DISPENSATRICE SERVICE(2/5)
REQUISITION
INTERACTIONVACCIN
INGREDIENTVACCIN
EVENEMENTSIGNALE
EVENEMENT SANTE PUBLIQUE(1/2)
USAGER (3/6)
MANIFESTATION CLINIQUEP.I.
PARTICIPATIONENTENTEENTENTE
DOSE VACCIN
DOSE SUIVANTE
DIAGNOSTIC (2/3)
DEMANDE SERVICE (2/2)
RESEAU ALERTAGE
INTOXICATION SANTEPUBLIQUE
EVENEMENT DEL'ECLOSION
ECLOSION
ALERTE MEDICALE
AGENTCHIMIQUE
EVENEMENT SANTE PUBLIQUE(2/2)
CONTACT (3/9)ÉLÉMENT TERRITORIAL
(1/3)
LOCALISATION ECOLE
FREQUENTATIONSCOLAIRE
ECOLE
INTERVENANT (2/7)
EQUIPEMENT (3/3)
PLAN TYPE VACCIN
MILIEU DE VIE
INFECTION SANTEPUBLIQUE
EQUIPEMENT REQUIS CLINIQUEVACCINATION
CATEGORIEINDUSTRIELLE
CATEGORIE AGENTCHIMIQUE
AGENTINFECTIEUX
TRANSPLANTATION
TYPE ORGANE OUTISSU
DON ORGANE TISSU
ACTE VACCINATION (2/2)
PARTICIPANTS CLINIQUEVACCINATION
CONVOCATION USAGER
CONVOCATIONINTERVENANT
GROUPE USAGERS
CLINIQUEVACCINATION
COORDINATION (2/2)
NAISSANCE (2/2)
USAGER (4/6)
INTERVENANT (1/7)
USAGER (5/6)
PROGRAMME (2/2)
UNITE SERVICE (3/5)
UNITE SERVICE (4/5)
ORGANISATION DISPENSATRICE SERVICE(1/5)
UNITE SERVICE (5/5)
AGENT ALLERGÈNE (2/2)
USAGER (6/6)
EQUIPEMENT REQUIS ACTEVACCINATION
PERSONNE CONTACT(2/2)
RAPPORT ANALYSE LABORATOIRE
EQUIPEMENT REQUIS ANALYSELABORATOIRE
ANALYSE LABORATOIRE
CODE RESULTAT ANALYSELABORATOIRE
NORME (3/4)
DIAGNOSTIC (3/3)
GROUPEMENT RESULTAT ANALYSELABORATOIRE
SPECIMEN DE L'ANALYSELABORATOIRE
CODE PRESCRIPTION ANALYSELABORATOIRE
PRELEVEMENTSFAITS
NORME (4/4) CODESPECIMEN
COMPOSITIONGROUPE
PRESCRIPTION(5/5)
PRESCRIPTION(4/5)
PRESCRIPTION(3/5)
PRESCRIPTION(2/5)
CONTACT (2/9)
CONTACT (1/9)
CONTACT GROUPÉ (1/4)
PRESCRIPTION(1/5)
ÉVÉNEMENT SOUSENQUÊTE
ADRESSE TELECOMMUNICATIONINTERVENANT
USAGE TÉLÉCOMMUNICATIONINTERVENANT
ADRESSEINTERVENANT
MEDICAMENT (2/2)SUBSTITUTION MÉDICAMENT(2/2)
COMPOSITION MÉDICAMENT(2/2)
MALADIE EFFETSECONDAIRE
TRAITEMENTMALADIES EFFETS SECONDAIRES
VACCIN
EVENEMENT DEVIE
ÉPISODE DE VIE
CONTACT GROUPÉ (4/4)
CONSTATATIONSNAISSANCE
CONSENTEMENT AUTRAITEMENT
AUTORISATION D'ACCÈS
ORGANISATION DISPENSATRICE SERVICE(5/5)
SIGNALEMENTMENACE
ÉVÉNEMENTDÉCLARÉ
CONTACT (9/9) INTERVENANT (7/7)
PLAN D'INTERVENTIONS(2/2)
PROBLÈMESADRESSÉS
DIAGNOSTICSADRESSÉS
PRESCRIPTIONSADRESSÉES
ADRESSE ODS
ADRESSE TELECOMMUNICATIONODS
USAGE TELECOMMUNICATIONODS ÉLÉMENT TERRITORIAL
(3/3)
LOCALISATION USAGER
LOCALISATIONINTERVENANT
LOCALISATION ORGANISATION(2/2)
COMPOSITIONHIÉRARCHIE
TYPE HIERARCHIE(2/2)
1,10,N
1,10,N
0,N 1,10,N1,1
1,1
0,N
1,1
0,N
<4> 1,1
0,N
0,10,1 0,1 0,N
0,10,N1,1
0,N
1,10,N1,10,N
1,10,N
0,1
0,N
1,10,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
0,10,N
0,10,11,10,N
0,10,N
1,1
0,N
1,1
0,N1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
1,10,N
1,1
0,N
0,1
0,N0,1 0,N
1,1 0,N
1,1
0,N
1,1
0,N
1,10,N
1,10,N
1,11,N
1,10,N
1,1
0,N
1,1
0,N
1,10,N
0,10,N
1,10,N
1,10,N
1,10,N
1,1
0,N
1,1
0,N
0,10,N
0,1
0,N
0,1 0,N
1,1
0,N
1,10,N
1,1
0,N
1,10,N
1,10,N
1,1
0,N
1,1
0,N0,1 0,N
1,1
0,N
1,10,N
1,10,N
1,10,N
1,10,N
0,10,N
1,1
0,N
0,1
0,N
1,10,N
1,10,N
1,10,N
0,10,N
1,10,N
1,10,N
0,1
0,N
1,10,N
1,1
0,N
1,1
0,N
0,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
0,10,N
0,10,1
1,1 0,N
1,10,N
1,1
0,N0,1 0,N
0,1
0,N
0,1
0,N
0,1
0,N
1,10,N
1,10,N1,10,N
1,1
0,N
0,1
0,N
1,1
0,N
0,1
0,N
1,10,1
1,10,N
0,1
0,N1,10,N
0,1
0,N
0,1
0,N
1,10,N
0,10,N
0,1
0,N
1,10,N
0,1
0,N
0,1
0,N
1,1
0,1
1,1
0,N
0,1
1,1
1,1
0,N
0,1
0,N
1,10,N
0,10,N
1,1
0,N
0,1
0,N
0,1 0,N
1,10,N0,1
0,1
1,1
0,N
0,1
0,N
0,1
0,N
0,10,N
0,1
0,N0,1
0,N
1,11,N
1,1
0,N
1,10,N
1,1
0,N
0,1
0,N
0,1
0,1
1,1
0,N
1,1
0,N
0,1
0,N
1,1
0,1
1,10,1
1,10,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
0,10,N
1,10,N
0,10,N
1,10,N1,10,N
1,1
0,10,N
0,1
1,1
0,N
1,10,N
0,10,N
1,1
0,N
1,10,N
0,1
0,N
1,10,N
1,1 0,N
0,1
0,N
1,10,N1,1
0,N
1,1
0,N1,1
0,N
0,10,N
1,10,N
0,1
0,N
1,1
0,N
1,10,N
0,11,1
0,1
0,N
1,10,N
1,1
0,N
1,1
0,N
0,1
0,N
0,1
0,1
0,10,1
1,1
0,1
1,1
0,N
1,1
0,N
1,1
0,N
0,1
0,N
1,10,N
1,10,N
1,10,N
1,10,N
1,1
0,N
1,1 0,N
1,10,N0,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
0,N1,1
0,10,N
1,10,N
1,1
0,N
1,10,N
1,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N1,1
0,N
1,10,N1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N1,1
0,N
1,1
0,N
0,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
1,10,N1,10,N0,11,1 1,1
0,N
1,1 0,1
1,1
0,N
1,1
0,1
1,1
0,N
1,10,N
1,10,N
0,N 0,1
0,1
0,N1,1
0,1
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N
0,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
0,1
0,N
1,10,N
0,1
0,N
1,1
0,1
0,1
0,N
0,1
0,N
0,1
0,N
1,1
0,1
0,10,N
0,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N1,1
0,N
0,1
0,N
0,10,N0,1
0,N
1,10,N
0,10,N
0,10,N
1,1
0,N
1,1
0,N
1,10,N
0,10,N
0,1
0,N
0,1
0,N
0,1
0,N
1,10,N1,1
0,N
1,10,N
0,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,10,N
1,10,N
1,1
0,N
1,10,N
0,1
0,N
1,10,N
1,1
0,N
0,1
0,N
0,10,N
0,10,N
1,10,N
1,10,N
1,10,N
1,10,N
1,10,N
1,10,N
1,1
0,1
1,10,N
1,1
0,N
1,1
0,N
1,10,N1,1
0,N1,1
0,1
0,1
0,N
1,10,N
1,10,N
1,10,N
1,1
0,1
1,1
0,1
1,1
0,1
1,10,N
1,10,N
0,1
0,N
0,1
0,N
1,1
0,10,1
0,N
1,10,N
1,10,N
0,11,1
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
0,1
0,10,1
0,1
1,10,N
1,10,N
1,1
0,N
0,1
0,N
1,1
0,1
1,N
0,1
0,1
0,N
0,10,N
1,1
0,N
1,1
0,N
0,1
0,N
1,1
0,N1,10,N
0,N
0,11,1
0,1
1,1 0,N
0,1
0,N
1,1
0,N
0,10,N0,1
0,1
1,10,N1,10,N
1,1
0,N
1,10,N
1,1
0,N1,10,N
1,10,N
1,10,N
1,1
0,N1,10,N
1,1 0,N1,1 0,N1,1
0,N1,1
0,N
0,10,N
1,1
0,N1,1
0,N1,10,N
1,10,N
1,10,N
1,10,N
1,1
0,N
1,10,N
0,1
0,N
0,1 0,N0,1
0,N
1,1
0,N
1,1
0,N 0,1
0,N
1,10,N
1,1
0,N
0,10,N
0,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,1
1,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
0,10,N
1,10,N 1,10,N
1,1
0,N
1,10,N
1,1
0,N
1,1
0,N0,1
0,1 0,1
0,N
1,10,N
1,10,N1,10,N
1,10,N
1,10,N
1,10,N1,1
0,N
1,1
0,N
1,10,N
1,10,N
1,10,N
1,10,N
1,10,N
1,1
0,N
1,10,N
1,10,N
Figure 6: The CCDM of the Quebec healthcare system.
4.3 Constructing views for the di�erent stakeholders
After constructing the global data model, the next step consists of creating subsets of this model toanswer the needs of information for di�erent stakeholders in the healthcare network. These subsets arecalled views and they constitute a core concept in the architecture with which the information architectis able to articulate the CCDM. In fact, the CCDM forms the hub of the information architectureputting in relation these di�erent models. Figure 8 shows four di�erent views that can be deducedfrom the MCCD: Field Action View, Business Process View, Messages View, and Systems/DB View.
The Field Action View is the sub-schema of the CCDM that groups all the relevant componentsthat make a particular FA such the Drug Prescription FA, Service Request Transfer FA, etc. As for theBusiness Process View, it contains all the relevant business processes that are speci�c to a particularproject. The System/DB View is a view of the databases and interfaces of existing systems. It can alsobe a view of systems that are currently being implemented. As for the Messages View, it representsthe relevant entities that compose an HL7 message.
4.3.1 The message view
The Quebec healthcare network is subject to Canada Health Infoway [29], a pan-Canadian not-for-pro�t organization that collaborates with the provinces and territories, healthcare providers and tech-nology solution providers for information integration, systems interoperability, and vocabulary andcommunications standards and norms.
In the Quebec healthcare system, a major leap forward had to be made to integrate the HL7 V3standard of communication between the di�erent healthcare information systems. HL7 speci�es anumber of �exible standards and guidelines by which various healthcare systems can communicatewith each other. These data standards and guidelines allow the information to be uniformly andconsistently shared and processed. The HL7 V3 [24] threfore provides a framework for the exchangeand sharing of electronic health information. The electronic messaging of HL7 is expected to supportthe Quebec healthcare applications through the speci�cation of message artifacts for the exchange ofhealth records within the province and with other jurisdictions across Canada. These records can beboth of clinical and administrative nature.
The CCDM-based information architecture can be very easily used to create views of messages. Infact, using the terminology coming from the CCDM and the development process represented by thetwo-track Y-model cycle, it is possible not only to understand how each of the HL7 messages relates
9

1
USAGER_1
UNITE SERVICE
ORGANISATION DISPENSATRICE SERVICE
NORME
COORDINATION
CONTACT
INTERVENANT_1
CATÉGORIE INTERVENANT
TRANSFERT DEMANDE
STATUT INTERVENANT
SPECIALITÉ MÉDECIN
SOMMAIRE INTERVENTION
SÉJOUR INSTALLATION
REALISATION INTERVENTION
NAISSANCE
GROUPE USAGERS
EVENEMENT DE VIE
ÉPISODE DE VIE
DEMANDE SERVICE
CORRESPONDANCE INTERVENTION
CONSTATATIONS NAISSANCE
COMPOSITION GROUPE
CODE INTERVENTION
CENTRE ACTIVITÉ_1
ÉLÉMENT TERRITORIAL (2/2)
ÉLÉMENT TERRITORIAL (1/2)
LOCALISATION ORGANISATION
LOCALISATION USAGER
ADRESSE USAGER
ADRESSE ODS
TYPE ÉLÉMENT TERRITORIAL
1,10,N
1,10,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
0,10,N
1,1
0,10,1
0,1
0,10,N
0,1
0,N
1,1
0,1
1,1
0,N
1,1
0,N
0,1
0,N 1,10,N
1,1
0,N0,1
0,N0,1
0,N
1,1
0,N
1,10,1
1,1
0,N1,1
0,N0,1
0,1
1,10,N
1,1
0,N
0,1
0,N0,1
0,N
1,1
0,N
0,1
0,N
0,1
0,N
0,1
0,N
0,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
1,10,N
1,10,N
1,1
0,N
1,1
0,N
1,1 0,N
1,10,N
0,10,N
1,1
0,N
0,1
0,N
Nom du schéma
Créateur Version
Créé le Modifié le
MCCD 6/RCAI_SCxxxxxxQC01
DAAOT MSSS Québec MCD iCLSC
2002-07-17 2008-07-31
Figure 7: The CDM of the i-CLSC information system.
to the reality on the ground through the �eld actions, but it becomes clear to see the overlap betweenthe functional requirements and technical needs as modeled and suggested by Canada Health Infoway.In Infoway, the messages are created based on two semantic foundations- a Reference InformationModel or RIM, and a set of terminology domains. To model HL7 messages, Canada Health Infowayuses software engineering tools to support the process. This includes OO concepts, Uni�ed ModelingLanguage (UML) diagrams, XML, and other graphic and documenting software tools such as theRMIM Designer, the RoseTree DB, and XML's schemas.
In the re�ned reference models for messages, one can notice that many object-oriented abstractconcepts that do not relate directly to the reality on the gorund but are there just for the programmerconvenience are used in those models. The message models which include the payloads, the wrap-pers, and the common message element types or CMETs are constrained models of the original RIM.Therefore, it becomes unclear to dissociates the functional requirements for an HL7 message from itstechnical and software needs. But using the CCDM-based information architecture, it is possible tocreate message views as sub-schemas of the CCDM which not only related directly to the �eld actionsand therefore the reality on the ground, but also can be very easily communicated to interested partiesand stakeholders in the health domain. Moreover, it is easy to analyze the business needs and followthe two-track Y-cycle in order to address the technical needs of the message.
For this purpose, an HL7 message is modeled at both the conceptual and logical levels of abstraction.The logical view of an HL7 message is built based on the business view of the message provided byCanada Health Infoway. A logical view is an LDM that represents an HL7 message content and itstechnical details. Figure 9 shows the logical view of the message 'Add Client Request' [29] for addinga new client in a source system that wants to request a client identi�er from a jurisdictional clientregistry system. This message, which is provided by Canada Health Infoway in the context of the HL7V3 pan-Canadian messaging standards, is used at the DAAOT [35] unit as part of the administrativedomain of Client Registry.
10

Field Action
View
Business
Process
View
Messages
View
Systems/DB
View
Sub-schema
Sub-schemaSub-schema
Sub-schema
Reality
Business Architecture
System Architecture
Figure 8: The views of the CCDM.
4.3.2 Creating the conceptual and logical system view
Besides constructing messages views in the context of HL7 standards, other views such as system viewcan also be created based on the CCDM. For the i-CLSC, the information system that keeps trackof the CLSC patients, a conceptual data model (CDM) view can be constructed as a subset of theCCDM. In the same time, a logical data model (LDM) can be drawn based on the terminology andconcepts used by the healthcare providers and other entities in the network such as patients.
To generate the conceptual and logical views, the authors developed in an earlier paper [] a dedicatedmechanism of mapping called the CCDM Coupling Method. This mechanism allows the transitionbetween the conceptual and logical modeling levels of abstraction. Figure 10 shows the coupling of thei-CLSC CDM with its counterpart the i-CLSC LDM in the Silverrun tool. The LDM is shown in thelower part of the Figure 10, and the CDM is depicted in the upper part. The coupling between thetwo models of the i-CLSC system is depicted by the red color connecting lines.
4.4 Using the concept of rubrics to simplify the CCDM
The Quebec healthcare systems uses a wealth of information external to its business architecture whichcan be in several forms such as the HL7 standards for messaging, the SNOMED CT and the LOINCvocabularies and code systems for terminology, etc. To keep the information architecture manageable,the explicit modeling of all of this information and other external information, and their inclusion inthe global model can be presented in a consice manner.
To avoid the overloading of the global data model, the concept of rubrics can be used in order tomanage the CCDM's graphical representation. Rubrics allow the addition of information to a datamodel without being explicitly represented in the global model. In fact, it was stated in [19] thatnarratives or rubrics allow health professionals to share complex ideas in an e�cient manner. Theyprovide easily understandable content while representing complex and disparate data. Compared tostructured data, such as web forms, narratives are much more �exible, easy to interpret, and closer tothe way caregivers are used to work with. Meaning can be lost when clinicians are forced to work withhighly structured data. However, structured documents are necessary when information systems need
11

1,1
has person (M)
1,1
1,1
has (R)
0,N
1,1
has (M10)
0,N1,1
has (R100)
0,N
1,1
Personal Relationship (R10)
0,N
1,1
IDENTIFIED CLIENTClient Healthcare Identification number (P40
Client Status Code (P)
Client Effective Time (R)
ø Client Masked Information (P)Clé primaire(Client Healthcare Identification number (P40)
IDENTIFICATION ASSIGNING ORGANIZATIONonHealthCare Organization Identifier (M)
ø NonHealthCare Organization Name (P)Primaire(NonHealthCare Organization Identifier (M))
LANGUAGE COMMUNICATIONLanguage of Communication Code (M)
ø Language of Communication Preference Indicator (RClé primaire(Language of Communication Code (M))
Other IDs Non Healthcare IdentifiersNon Health Care Identification (M)
ø Non Health Care Identification Code (P)Primaire(Non Health Care Identification (M))
PARENT PERSONNext of Kin Identifier (M)
Client Next of Kin (M)
ø Next of Kin Name (R)Primaire(Next of Kin Identifier (M))
FK1 CLIENT()
PERSONø Client Name (P20)
ø Client Gender (P)
ø Client Date of Birth (P)
ø Client Address (P10)
ø Client Telecom (P20)
ø Client Deceased Indicator (R)
ø Client Deceased Date (R)
ø Client Multiple Birth Order Number (R
ø Client Multiple Birth Indicator (R)Clé primaire()
Projet : projet
Modèle : RCAI_ML000000QC01 Version : Add Client Request
Auteur : DAAOT MSSS Québec
Description :
Figure 9: Logical view of the message Add Client.
to exchange data.The rubrics represent a block of text that can be shown to the user to obtain details about a certain
aspect of an entity. Rubrics are presented together with a set of Meta tags that can help the usersort di�erent rubrics. These Meta tags are directly taken from the CCDM and are attributes that arecommon to every possible representation format that the rubric can take. Rubrics contain plain textbut can be structured using XML to facilitate their presentation to the user using for example stylesheets. In the global model, a rubric is viewed as an entity. The main di�erence with other entitiesis that a rubric can be broken into di�erent sub-entities depending of the context. Therefore, in aparticular sub-schema of the CCDM, a rubric will have additional attributes although it will alwayskeep the attributes that were present in the CCDM (i.e. the Meta tags).
This method allows the simpli�cation of the global data model since details about entities can beexpressed only in their particular context. This also reduces the number of entities in the CCDMsince only rubrics in the global model are kept but their di�erent specializations in the sub-schemasare not. The use of rubrics in the CCDM model generates a simpli�ed global model easy to maintain,brings in reusability of entities, and �nally focuses on the use of attributes only in the appropriatecontext. Figure 11 shows an example of a rubric, the Prescription Rubric. This rubric has commonattributes, or Meta tags, which are Prescription ID, Prescription Type and Prescription Date andTime. The other elements written in capital letters (i.e. DRUG PRESCRIPTION, LABORATORYANALYSIS PRESCRIPTION, IN TERVENTION PRESCRIPTION, etc.) indicate the di�erent waysthat a rubric can be expanded. In the context of a drug prescription (Drug Prescription Field Action),the Prescription rubric still keeps the same Meta tags from the CCDM as shown in Figure 11. Otherattributes are added to comply with the drug prescription context. The process is repeated for theLaboratory Analysis Prescription context and for the forms that the Prescription rubric can take.
12

1
CLSC (2/2)
USAGERTYPE USAGER
TYPE
SERVICE SPÉCIFIQUE PÉRINATALITÉ
SERVICE DE PÉRINATALITÉ DEMANDÉ
POPULATION-CIBLE USAGER
INTERVENTION
INTERVENANT
DEMANDE SERVICES
DÉLIVRANCE SERVICEPÉRINATALITÉ
CLSC (1/2)
CENTRE ACTIVITÉ
CATÉGORIE USAGER
BÉBÉ
ACTIVITÉ PONCTUELLE
ACTE
ACCOUCHEMENT
USAGER_1UNITE SERVICE
TRANSFERT DEMANDE
STATUT INTERVENANT
SPECIALITÉ MÉDECIN
SOMMAIRE INTERVENTIONSÉJOUR INSTALLATION
REALISATION INTERVENTION
ORGANISATION DISPENSATRICESERVICE
NORME
NAISSANCE
INTERVENANT_1
GROUPE USAGERS
EVENEMENT DE VIE
ÉPISODE DE VIE
DEMANDE SERVICE
CORRESPONDANCE INTERVENTION
COORDINATION
CONTACT
CONSTATATIONS NAISSANCE
COMPOSITION GROUPE
CODE INTERVENTION
CATÉGORIE INTERVENANT
ÉLÉMENT TERRITORIAL (2/2)
LOCALISATION USAGER
LOCALISATIONORGANISATION
ÉLÉMENT TERRITORIAL (1/2)
ADRESSE USAGER
ADRESSE ODS
TYPE ÉLÉMENT TERRITORIAL
CENTRE ACTIVITÉ_1
RAISON INTERVENTION
RAISON
BÉNÉFICIAIRE INTERVENTION
ALLAITEMENT
ALIMENTATION EFFECTIVE NOURRISSON
ACTIVITÉ PRINCIPALECOMMUNAUTAIRE
ACTIVITÉCOMMUNAUTAIRE
ACTE INTERVENTION
RAISON ACTIVITÉ PONCTUELLE
ACTE ACTIVITÉ PONCTUELLE
1,1 0,1
0,1
0,N
1,1
0,N
1,10,N0,10,N
1,10,N
1,10,N
1,1
0,N
1,1
0,N
1,1 0,N
1,1
0,N
1,1
0,N
1,10,N
1,10,N 1,1
0,N
1,1
0,N
0,1
0,N
0,1 0,N
1,1
0,1
1,1
0,N
0,1
0,N
1,1
0,N
1,1
0,N1,10,N
1,10,N
1,10,N
1,1 0,1
1,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N0,1
0,N
1,1
0,10,1
0,1
0,10,N
0,1
0,N
1,1
0,1
1,1
0,N
1,1
0,N
0,10,N
1,1
0,N
1,1
0,N
0,1
0,N0,1
0,N
1,10,N
1,1
0,1
1,1
0,N
1,10,N0,1
0,1
1,1
0,N1,1
0,N
0,1
0,N0,10,N
1,1
0,N
0,1
0,N
0,10,N
0,1
0,N
0,1
0,N
1,1
0,N1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N1,10,N1,1
0,N
1,10,N
1,1
0,N1,1 0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
0,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,1
0,N
1,1
0,N
1,1
1,3
1,1
1,3
1,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N
1,10,N
1,1
0,N
0,10,N
1,1
0,N
1,1
0,N
1,1
0,N
1,10,N 1,1
0,N
1,1
0,N
0,1
0,N
1,1
0,N
1,1
0,N
Nom du schéma
Créateur Version
Créé le Modifié le
MCCD 6/RCAI_SCxxxxxxQC01 MCD iCLSC/…
DAAOT MSSS Québec Rac iCLSC
2002-07-17 2008-08-04
MCD
MLD
Figure 10: The LDM and the CDM of the i-CLSC, and their coupling.
4.5 Using the proper data modeling tool to manage the CCDM's graphical
complexities
The information architecture of the Quebec healthcare system is composed of a very large numberof sub-schemas and models which required the use of an appropriate modeling tool to manage thecomplexity of this environment. The only software with functionalities that suited the research project'sneeds was the Silverrun business process and data modeling tool [34] o�ered by Grandite.
The Silverrun tool while supporting the business process re-engineering projects, provide modelingcapabilities to model data based on traditional entity-relationship method and the development canbe made compatible with the Datarun framework [4] which are used in this research work. Thelatest version, the Silverrun ModelSphere5, can also be used to model business processes and to createbusiness process mapping in which one can identify the �eld actions. This tool provides a �exibleenvironment for business processes, systems views, and �eld action views' management which cangreatly help manage the complexities faced with when dealing with multiple schemas and sub-schemas.This software tool which is designed in Java and works on a standard virtual machine can be installedon di�erent platforms such as Linux and Windows. Users of this software tool can easily build theirdata models either from scratch or via reverse engineering from a variety of sources such as RelationalDatabase Management Systems (RDBMS).
Another important tool that was developed to support this research is the CCDM_Extract [15]tool used to generate CCDM mapping matrices. The CCDM_Extract is a simple web-based softwarethat allows the comparison of di�erent data models with the global data model of the CCDM. Itallows the identi�cation of common elements and attributes between the models under investigation.Figure 12 shows an example of model matrix generated using CCDM_Extract where the letter 'X'indicate that an element is present in a speci�c model. The CCDM_Extract tool helps identify anyredundancy with respect to entities presence in existing information systems and applications. With
13

Prescription
Prescription ID
Prescription Type
Prescription Date & Time
DRUG PRESCRIPTION
LABORATORY ANALYSIS
PRESCRITION
INTERVENTION
PRESCRIPTION
Entity X
Entity Y
Entity Z
Entity Z Entity W
Entity Y
Prescription ID
Prescription Type
Prescription Date &
Time
Status
Test encoding
...
Entity Y
Prescription ID
Prescription Type
Prescription Date &
Time
Posology
Renewable
prescription?
…
CCDM
Laboratory Analysis Prescription Field Action Drug Prescription Field Action
Figure 11: The Prescription rubric.
the help of CCDM_Extract, organizations can create e�cient new systems based on existing oneswhere the concept of re-utilization is exploited.
5 Conclusions
This paper presented the results of implementing the CCDM-based approach to the creation of theinformation architecture for the Quebec healthcare network. The information architecture was builtaround the knowledge of the Quebec health domain and was based on three core organisational con-cepts: Field actions, the CCDM global model, and Views of sub-schemas of the CCDM. The �eldactions were used to capture the essential data elements representing the persistent healthcare infor-mation of the reality on the ground. The global data model provided a holistic view of informationin the healthcare knowledge domain and represented the stable and coherent information hub of thiscomplex organization. The views were used to model any information needs for any healthcare stake-holder. All of the implementation artifacts were produced using the Silverrun data and businessmodeling tools. A MIGRATION TO Open ModelSphere is presently taking place. This informationarchitecture allowed the Quebec healthcare organization not only to understand its complexities butalso to align its business strategies and implementations in order to better serve the citizens of Que-bec. It is expected in the future that this information architecture within an CCDM-based enterprisearchiteture will help the Quebec healthcare organizationmonitor its transformation and better planand urbanize its evolution.
Acknowledgments- This research work is being conducted at the DAAOT (Direction Adjointe
14

Entities/Attributes CCDMUser
RegisterRODIS RSIPA OEMC
ADRESSE INTERVENANT X X
Date début validité adresse inetrvenant X X
Type adrese intervenant X X
Date fin validité adresse intervenant X X
Identifiant intervenant X X
MEDICAMENT (DRUGS) X X X
D IN médicament X X X
Nom médicament X X X
Forme médicament X X X
Catégorie médicament X X X
Médicament origine-générique? X X X
Date expiration brevet médicament X X X
Voie normale administration médicament X X X
ORGANISATION DISPENSATRICE SERVICE X X X
Identifiant ODS X X X
Nom légal ODS X X X
Nom abrégé ODS X X X
Numero de permis ODS X X X
Coordonnées principales ODS X X X
Période de disponibilité X X X
Type ODS X X X
Type financement ODS X X X
Mode Financement ODS X X X
USAGER (USER) X X X X
Identifiant usager X X X X
NAM usager X X X X
Nom usager X X X X
Autre nom X X
Autre prénom X X
Prénom usager X X X X
Date expiration NAM usager X X X X
Sexe usager X X X X
Provenance NAM usager X X X
Lieu de naissance X X X X
Curatelle usager X X X X
Usager jumeau identique? X X X
Prénom usuel usager X X X
Figure 12: An example of a CCDM_Extract matrix.
à l'Architecture et aux Orientations Technologiques) at the Ministry of Health and Social Services ofQuebec in Canada.
References
[1] Pascot, D., Bouslama, F., and Mellouli, S., An Enterpise Architecture Framework for LargeIntegrated Complex Information Systems, Submitted to:
[2] Le Moigne, J. L., Les systèmes d'information dans les organisations, PUF 1973.
[3] Tardieu, H., Rochfeld, A., Colletti, R., Panet, G., and Vahée G., (1985). La méthode Merise -Tome 2 Démarches et pratiques. Editions d'organisation (Paris) : 460 p. ISBN 2-7081-0703-8.
[4] D. Pascot, La méthode Datarun, Management Information Systems Department,Faculty of Business Administration, Laval University, Quebec, Canada, 1999.http://loli.fsa.ulaval.ca/�leadmin/Methodes/Analyse/pdf-datarun/DATARUN.pdf
[5] M. Lankhorst, Enterprise Architecture At Work: Modeling Communications and Analysis,Springer, 2005.
[6] Batini, C., Lenzerini, M., and Navathe, S. B., A comparative analysis of methodologies fordatabase schema integration, ACM Computing Surveys (CSUR), Vol. 18 , Issue 4, pp. 323- 364,1986.
15

[7] Doerr, M., Hunter, J., and Lagoze, C., Towards a Core Ontology for Information Integration,Journal of Digital Information, 4 (1), 2004 http://jodi.ecs.soton.ac.uk/Articles/v04/i01/Doerr/
[8] Calvanese, D., De Giacomo, G., Lenzerini, M., Nardi, D., and Rosati, R., Description LogicFramework for Information Integration, Proc. of the 6th Int. Conf. on the Principles of KnowledgeRepresentation and Reasoning (KR'98), Trento, IT, pp. 2-13, 1998.
[9] Jean, G., Urbanisation du business et des SI, Hermes 2000, Lavoisier 20002. ISBN: 2-7462-0135-6
[10] P. Roques and F. Vallée, UML en action, de l,analyse des besoins à la conception en java, Deuxièmeédition, Groupe Eyrolles, 2003. ISBN: 2-212-11213-0.
[11] Dupuy-Chessa, S., Godet-bar, G., Juras, D., and Rieu, D., Principes pour une méthode de concep-tion de systèmes mixtes, in Proceedings of 19th Conférence francophone sur l'Interaction Homme-Machine (IHM'2007)
[12] Kato, S., System Development Guide Book, NikkeiBP Publications, Printed in Japan, June 26,2000 ISBN4-8222-8073-X
[13] Pascot, D., and Ochimizu, K., C/S DataBase Sekkei Nyumon, A Japanese Translation ofDATARUN Concepts, Client/Server Power System Series, NikkeiBP Publications, Printed inJapan, 1996, ISBN4-8222-9015-8.
[14] PFU, The DATARUN Epoch-making Multi-Media teaching Materials, For Easy Understandingof the Business Process Reengineering methodology DATARUN, CD-ROM, PFU Limited, Tokyo,Japan, 1996.
[15] Pascot, D. Conception des SIO, Lecture Notes, Management Information Systems De-partment, Faculty of Business Administration, Laval University, Quebec, Canada (2007)http://loli.fsa.ulaval.ca/index.php?id=478
[16] The Quebec Health and Social Services System-Ministère de la Santé et des Services Sociaux,http://www.msss.gouv.qc.ca/en/index.php
[17] Cadre méthodologique, Direction adjointe à l'architecture et aux orientations technologiques(DAAOT), The Ministry of Health and Social Services (MSSS), Quebec, Canada, 2007.
[18] Silberzahn, N., Le dossier médical informatisé : Modélisation et consultation. Ph.D. Thesis, Fac-ulté de médecine, Université de Caen, France, December 1997.
[19] Shapiro, J. S., Bakken, S., Hyun, S., Melton, G. B., Schlegel, C., and Johnson, S. B., Documentontology: Supporting narrative documents in electronic health records, In Proceedings of AMIAAnnual Symposium, pp. 684-688, 2005.
[20] The Québec Health and Social Services System, http://publications.msss.gouv.qc.ca/acrobat/f/documentation/2007/07-731-01A.pdf
[21] Gans, D., Kralewski, J., Hammons, T., and Dowd, B., Medical groups' adoption of electronichealth records and information systems, in Health A�airs No. 24, Vol. 5, pp. 1323-1333, 2005.
[22] Miller, R. H., and Sim, I., Physicians' use of electronic medical records: barriers and solutions, inHealth A�airs, No. 23, Vol. 2, pp. 116-126, 2004.
[23] Wang, S. J., Middleton, B., Prosser, L. A., Bardon, C. G., Spurr, C. D., Carchidi, P. J., Kittler, A.F., Goldszer, R. C., Fairchild, D. G., Sussman, A. J., Kuperman, G. J., and Bates, D.W., A cost-bene�t analysis of electronic medical records in primary care, in American Journal of Medicine,No. 114, Vol. 5, pp. 397-403, 2003.
16

[24] Health Level Seven, 2008. http://www.hl7.org/
[25] Systematized Nomenclature of Medicine- Clinical Terms, The International Health TerminologyStandards Development Organization (IHTSDO), 2008. http://www.ihtsdo.org/
[26] Logical Observation Identi�ers Names and Codes, 2008. http://loinc.org/
[27] Gagon-Argion, L. and Vien, H., Typologie des documents des organisation : de la création à laconservation, Presses de l'Université du Québec, ISBN : 2-7605-0943-5.
[28] D. Pascot, Conception des SIO, Méthodes: du besoin du SIO à l'entretien du SI, August 2007.http://loli.fsa.ulaval.ca/index.php?id=567
[29] Canada Health Infoway- Inforoute Santé Canada, 2008. http://www.infoway-inforoute.ca/
[30] Tardieu, H., Nanci, D., and Pascat, D., Conception d'un système d'information : Constructionde la base de données, Edition d'organisation, 1979.
[31] Le Moigne, J. L., La modélisation des systèmes complexes, Dunod, 2002.
[32] Le Moigne, J. L., Les formalismes de la modélisation systémique,http://www.mcxapc.org/docs/ateliers/0505formalismesvfr.pdf
[33] Mougin, Y., La cartographie des processus: maîtriser les interfaces, La méthode de la voix duclient, 2ème édition, Éditions d'organisation, 2004. ISBN : 2-7081-3106-0.
[34] SILVERRUN Modeling Tools, Grandite, 2008. http://www.modelsphere.com/
[35] Logical View of Message Model PRPM_MT303010CA - Update Provider, Direction adjointe àl'architecture et aux orientations technologiques (DAAOT), The Ministry of Health and SocialServices (MSSS), Quebec, Canada, 2008.
[36] Bonnet, P., Detavernier, J.-M., and Vauquier, D., Le sytème d'information durable: la refonteprogressive du SI avec SOA, Editions Hermes-Science, ISBN:978-2-7462-1829-1.
[37] Pascot, D., and Pascot, I., La modélisation de l'information du système de santé : le dossiermédical minimal commun, In Forum sur les standards en santé, Terminologies et modélisationHL7, (2004).
[38] Pascot, D., Les cartes des processus, In Report of the Projet Architecture des données des RSSS(Phase IV), Quebec Ministry of Health (MSSS), February 22, 2006.
[39] Forrey, A. W., McDonald, C. J., DeMoor, G., Hu�, S. M., Leavelle, D., Leland, D., Fiers, T.,Charles, L., Gri�n, B., Stalling, F., Tullis, A., Hutchins, K., and Baenziger, J. Logical observationidenti�er names and codes (LOINC) database: a public use set of codes and names for electronicreporting of clinical laboratory test results, Clinical Chemistry 42, pp. 81-90, 1996.
[40] Tang A., Huan J., Chen P., A comparative analysis of architecture frameworks, 2004.http://www.it.swin.edu.au/centres/TechnicalReports/2004/SUTIT-TR2004.01.pdf
[41] Iyer B., Gottlieb R., The Four-Domain Architecture: An approach to support enterprise architec-ture design, IBM system Journal, Vol. 43, No. 3, 2004.
[42] Gérard, J., Urbanisation du business et des SI, Hermes Science, Lavoisier 2002.
[43] Refonte du système LPRG, Ministère de la santé et des services sociaux, MSSS, Quebec, Canada,2008.
17

[44] Siegel, J., Introduction to OMG's Uni�ed Modeling Language, The Object Management Group,2005. http://www.omg.org/gettingstarted/what_is_uml.htm
[45] Cadre de référence-Étude des cadres de références du marché, Report, Ministère des ServicesGouvernementaux du Québec, Architecture Entreprise Gouvernementale, October 17, 2007.
[46] Anderson, C. L., Mishra, A. N., Agarwal, R., and Angst, C., Digitizing healthcare: the abilityand motivation of physician practices and their adoption of electronic health record systems, inProceedings of 28th International Conference on Information Systems, Montreal, pp. 1-17, 2007
18