Embed Size (px)
Citation preview
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 1 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Document Control
Title
Management of Legal Claims Policy
Author Author’s job title Legal Claims Manager
Directorate Strategy & Transformation
Department Corporate Governance (Compliance)
Version Date
Issued Status Comment / Changes / Approval
4.0 Nov 2011
Final Approved by Quality Assurance Committee subject to minor amendments suggested by Investigations Lead
4.1 Nov 2011
Revision Minor amendments made following suggestions.
4.2 Feb 2012
Revision NHSLA Compliance audit form added, update to references and change of Quality Assurance Committee name.
5.0 Feb 2015
Final Approved by Quality Assurance Committee and Published on BOB.
5.1 Nov 15 Revision Reformatted for house style
Main Contact Legal Claims Manager Suite 1, Munro House North Devon District Hospital Raleigh Park Barnstaple, EX31 4JB
Lead Director Director of Strategy & Transformation
Superseded Documents NDHT Claims Handling Policy (v4.2)
Issue Date March 2015
Review Date March 2018
Review Cycle Three years
Consulted with the following stakeholders:
Director of Workforce Development Compliance Team Head of Corporate Governance Trust Secretariat Director of Finance Trust Solicitors Medical Director Audit & Assurance Committee Maternity Services Risk Lead
Approval and Review Process
Quality Assurance Committee
Local Archive Reference
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 2 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
G:/Corporate Governance/Compliance Team Local Path Policies Procedural Documents Filename Management of Legal Claims policy v5. 0 15Apr15
Policy categories for Trust’s internal website (Bob) Corporate Governance
Tags for Trust’s internal website (Bob) Complaints, incidents, investigate, legal, negligence, inquests, risk management, personal, injury, claim, indemnity
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 3 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
CONTENTS
Document Control........................................................................................................................ 1
1. Purpose ................................................................................................................................ 4
2. Definitions............................................................................................................................ 4
3. Responsibilities .................................................................................................................... 6
4. NHS Litigation Authority Schemes: ........................................................................................ 9
5. Third Party Claims – Non-Clinical ......................................................................................... 10
6. Fraud Awareness – Unjustified claims ................................................................................. 11
7. Who can make a claim? ...................................................................................................... 11
8. Limitation ........................................................................................................................... 11
9. Communication with Relevant Stakeholders ....................................................................... 12
10. Saying Sorry – Press Release – December 2013 .................................................................... 12
11. Duty of Candour ................................................................................................................. 13
12. Support for Staff ................................................................................................................. 13
13. Links with Corporate Governance processes ........................................................................ 14
14. Management of Personal Injury Claims – Non Clinical .......................................................... 15
15. Management of Clinical Negligence Claims .......................................................................... 15
16. Management of Inquests .................................................................................................... 18
17. Lessons Learned arising from Claims ................................................................................... 19
18. Monitoring and Reporting Claims Activity ........................................................................... 20
19. Training Requirements........................................................................................................ 21
20. Monitoring and Auditing Compliance with the Effectiveness of the Managing Legal Claims Policy......................................................................................................................................... 21
21. References ......................................................................................................................... 23
22. Associated Documentation ................................................................................................. 23
23. Quality Impact Assessment ................................................................................................. 23
Appendix A : CNST and RPST Reporting Guidelines ...................................................................... 25
Appendix B : NHS Indemnity....................................................................................................... 29
Appendix C : Limitation .............................................................................................................. 35
Appendix D : Saying Sorry Leaflet ............................................................................................... 37
Appendix E : Duty of Candour ..................................................................................................... 38
Appendix F: Facing Litigation leaflet ........................................................................................... 39
Appendix I - Standard Operating Procedure Managing Inquests .................................... 47
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 4 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
1. Purpose
The purpose of this document is to detail the process to ensure the handling of clinical negligence, personal injury and other liability claims are managed effectively, i.e. that the organisation learns from these claims. Implementation of the policy will:
1.1. Implementation of this policy will ensure that:
Ensure the Trust complies with the National Health Service Litigation Authority (NHS Litigation Authority) requirements.
Ensure the right payments are made to the right claimants.
Minimise the cost of litigation arising from clinical negligence, personal injury and other liability claims over time.
Initiate a series of improvements through effective claims handling arrangements and the risk management programme, to reduce the incidents which give rise to claims.
Provide assurance to the Trust Board though its Committees of the Governance Committee that appropriate systems are in place for the handling of claims and that any learning from the events giving rise to those claims is appropriately disseminated.
The Trust acknowledges that being involved in a case which is being investigated as a possible claim can be a stressful experience for all staff (see Supporting Staff involved in an incident, complaint or claim Policy ). The policy applies to all Trust staff.
2. Definitions
2.1. Claim
Allegations of clinical negligence and/or a demand for compensation made following an adverse incident resulting in personal injury or any clinical incident which carries significant litigation risk for the Trust.
2.2. Clinical Negligence Claims
Allegations of clinical negligence and/ or a demand for compensation made following and adverse clinical incident resulting in a personal injury, or any clinical incident, which carries significant litigation risk to the Trust.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 5 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Clinical negligence is defined as “a breach of duty of care by members of the health care professions employed by NHS bodies or by others consequent on decisions or judgements made by members of those professions acting in their professional capacity in the course of their employment, and which are admitted as negligent by the employer or are determined as such through the legal process”
2.3. Employers Liability Claims (non-clinical)
The Trust is under common law duty and a statutory duty to take reasonable care to provide competent staff, safe plant and equipment, safe premises and safe working systems. The Trust may be liable to pay compensation to an employee for an injury or loss suffered as a result of a breach of their responsibilities.
2.4. Public Liability Claims (non-clinical)
Formal allegations from a member of the public or third party who has suffered a wrong or injury deemed to be under the Trust’s liability as a direct result of the Trust’s actions and services.
2.5. The DATIX System
The DATIX system is a risk management system used by the Trust to record information on the following modules:
Incidents
Risks
Complaints
Claims
Patient Advice and Liaison Service
The Legal Claims Manager has sole access and management of the “Claims module within Datix.
2.6. Indemnity and Vicarious Liability
The Northern Devon Healthcare Trust as an NHS body is legally liable for the negligent acts and omissions of their employees in the course of their NHS employment. Under NHS indemnity, NHS bodies take direct responsibility for costs and damages arising from clinical negligence where they (as employers) are vicariously liable for the acts and omissions of their health care professional staff. For work not covered in this way health care professionals may have a civil, or even, in extreme circumstances, criminal liability for their actions. (see Appendix B)
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 6 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
3. Responsibilities
3.1. Role of the Chief Executive
The Chief Executive is ultimately responsible that all claims are dealt with responsibly and effectively.
3.2. Role of the Medical Director
The Medical Director has Executive responsibility for clinical negligence and personal injury issues and keeps the Trust Board informed of major developments.
In the event of a clinical negligence claim the Director of Nursing and/ or Medical Director may be required to comment on care provided.
3.3. Role of the Director of Finance and Performance
The Director of Finance and Performance is responsible for the effective handling of claims under the Property Expenses Scheme for damage, loss or destruction of the Trust property or estate in line with managing the Trust’s “insurance” matters and is responsible for keeping the Trust Board informed of major developments. Further responsibilities include:
Liaising with the NHSLA over the RPST and with any commercial companies.
Dealing with claims the Trust wishes to make against RPST and PES in respect of loss or damage to Trust property or estate.
Managing the Trust reserve in respect of Employer/Public liability claims.
Dealing with pure financial loss/compensation requests in line with the Trust’s Losses and Special Payments Policy and the NHSLA’s Guidelines for clinical and non-clinical claim (ex-gratia payments)
3.4. Role of the Legal Claims Manager
The Legal Claims Manager has management responsibility for the conduct and control of all claims in accordance with the Claims Management Policy and the reporting procedures by:
Monitoring progress and outcomes of claims and provide confidential reports and/or feedback to relevant committees and personnel.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 7 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Managing all personal injury claims in accordance with the Pre-action Protocol for Personal Injuries reporting guidelines for non-clinical claims (RPST) to the NHS Litigation Authority (See Appendix A).
Attending “site visits” to investigate all employer and public liability claims, gathering documentation relevant to these claims Management of the secure NHSLA Extranet system to download and upload claims documentation for action and progression
Providing help and support to all staff in relation to all claims management.
Alerting and liaising with Communications team for any potential risk of adverse Trust publicity.
Assisting the management of all clinical negligence claims against the Trust in liaison with Trust Solicitors in accordance with Pre-Action Protocol for the Resolution of Clinical Disputes (see Appendix A)
Assisting the support and management of all formal Trust Inquests in liaison with Trust Solicitors.
Ensuring that all risk management issues/remedial actions identified during the course of a claim are referred and reported appropriately for action. Formal identified risk issues are managed in line with the Trust’s risk management process through entry to the Corporate Risk Register.
Liase with Counter Fraud Specialist, refer potential cases for fraudulent activity and work closely with the Fraud team throughout their investigations.
Communication with relevant Stakeholders.
3.5. Role of the Clinical and Non-Clinical Specialist Advisors
Clinical Specialist Advisors will be used when a third party review is required or when an expert opinion is needed through robust and authorised procedures.
3.6. Role of the Line Managers
Line managers are responsible for:
Ensuring staff are supported appropriately during the claim process. Where staff have been adversely affected, Managers must follow the Trust’s policy for Supporting Staff involved in an incident, complaint or claim Policy.
Ensuring that untoward occurrences are reported in line with the Trust’s Incident Reporting Policy and the Investigations policy Ensuring all identified risk management issues pertaining to their service during the course of a claim are actioned appropriately and in accordance with the Trust’s risk management process/Policy.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 8 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
3.7. Role of All Staff involved in claims
All staff are required to:
Comply with relevant aspects of this policy as staff may, in the event of a claim, be called upon to make a statement. Occasionally they will be required to meet with Trust Solicitors and, on rare occasions, be required to attend court.
Report untoward occurrences in accordance with the Trust’s Incident Reporting Policy and Serious Incidents Requiring Investigation Policy thus facilitating an early investigation that may give rise to a claim or identification of risk management issues
Fully co-operate in the investigation of any claim by providing comments, statements as requested. This also applies to current and ex-employees. All NHS employees are covered by the NHS Indemnity where they were acting the course of their NHS employment at the time of the incident (see Appendix B).
Forward all documentation and/or alert any issues in a timely fashion to meet legal deadlines including requests for medical records where it is intimated there may be a possible claim against Trust, to the Legal Claims Manager.
Keep any privileged documents (those produced in contemplation of litigation) filed separately from the medical records.
Ensure safe keeping of any physical evidence which may be required for the investigation of a claim i.e. foetal scans, CTG traces, archived documents (i.e. Policies, protocols, file notes) and photographs.
Management of any highlighted risks in relation to a claim.
3.8. Role of the Trust Solicitors (North and East Devon Legal Services)
Solicitors, Legal Claims Handlers and Legal Support Team are responsible for managing all the Trust’s clinical negligence claims whether brought by Solicitors or by Litigants in Person (i.e. people acting without the representation of Solicitors).
The Trust Solicitors:
Adhere to legislative requirements and timescales. (Appendix A) outlines their responsibilities under the CNST Reporting Guidelines.
Comply with the Law Society’s Continuing Professional Development requirements to ensure the Legal Claims Handlers and rest of the legal team receive supervision, departmental training and advice.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 9 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Ensure any identified risk management issues are actioned during the course of the claim and any remaining issues are highlighted to the Trust for action.
Manage all clinical negligence claims up to a delegated authority of damages of up to £25,000 (or higher if approved). This includes an authority to settle.
Those claims with potential damages of over £25,000, approval to admit liability, negotiate settlements, proceed to trial, settle Claimant’s costs etc will be required from the NHSLA.
The NHSLA will instruct a panel firm of Solicitors for any claims that are likely to be higher than the £25,000 delegated authority.
3.9. Role of the Trust’s nominated Panel Solicitors
Once the preliminary analysis has been conducted, significant and high value claims which exceed the Trust’s Solicitors’ delegated authority will be handled by panel solicitors for further legal conduct, this will normally be in agreement with the Trust. If a claim forms part of a group action, this may require a dedicated team from a firm of panel solicitors not known to the Trust, as set out in the NHS Litigation Authority’s guidelines (See Appendix A).
3.10. Role of the Audit and Assurance Committee
The Audit and Assurance Committee has overarching responsibility for governing claims management and has discharged the analysis of claims and monitoring of organisational learning to the Learning from Patient Experience Group.
The Audit and Assurance Committee’s role is to review the establishment and maintenance of an effective system of internal control and risk management to receive reports and assurance to the Trust Board.
4. NHS Litigation Authority Schemes:
The NHS Litigation Authority are a not-for-profit part of the NHS. They handle negligence claims on behalf of the NHS under a number of different schemes.
4.1. Clinical Negligence Scheme for Trusts (CNST)
The Clinical Negligence Scheme for Trusts handles all clinical negligence claims against member NHS bodies where the incident in question took place on or after 1 April 1995 (or when the body joined the scheme, if that is later). Although membership of the scheme is voluntary, all NHS Trusts (including Foundation Trusts) and Primary Care Trusts (PCTs) in England currently belong to the scheme. The costs of the scheme are met by membership contributions.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 10 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
4.2. Existing Liability Scheme (ELS)
This covers clinical negligence claims arising out of incidents which occurred before April 1995.
4.3. Ex-RHAs Scheme
This is a relatively small scheme covering clinical claims made against the former Regional Health Authorities, which were abolished in 1996. Like the ELS it is centrally funded by the Department of Health. It differs from the NHSLA’s other schemes in that the NHSLA is the legal defendant in any action.
4.4. Risk Pooling Scheme for Trusts (RPST)
HSC (1999) 021 issued in February 1999 introduced a new non-clinical risk pooling scheme to be run by the NHS Litigation Authority – the main scheme comprises of two separate schemes.
Under this collective Pooling scheme are the following schemes:
4.4.1 Liabilities to Third Parties Scheme (LTPS)
Employer Liability Claims (see 2.3)
Public Liability Claims (see 2.4)
4.4.2 Property Expenses Scheme (PES)
A scheme relating to any expenses incurred from any loss or damage to property which the original loss occurred on or after 1 April 1999.
5. Third Party Claims – Non-Clinical
Claims may be made against the Trust which do not come within the NHS Litigation Authority Schemes e.g. third party claims for pure financial loss such as replacement or repair against third party insurance.
Where there is evidence of other Trusts, individuals or external agencies being involved in a claim then that divisional team should be involved in any investigation that may take place and any findings or recommendations be shared with the Trust/agency
The Legal Claims Manager is responsible for informing the NHS Litigation Authority of the possibility of additional parties/joint defendants when reporting the claim (if applicable) or as soon as they are identified and they are also responsible for informing all additional parties/joint defendants. The Legal Claims Manager and the Trust’s Finance Department are responsible for counter-claiming via third party any losses requiring reclaim of financial loss and/or costs involved.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 11 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
6. Fraud Awareness – Unjustified claims
Government concerns regarding the increase in the number of fraudulent and grossly exaggerated personal injury claims and the effect that this has on public authority resources has encouraged action to be taken to deter dishonesty behaviour and give greater incentive to defendants (the Trust) and their insurers (the NHSLA) to investigate and challenge dubious claims for compensation.
The Trust’s Legal Claims Manager regularly communicates and liaises with the Trust’s Counter Fraud Specialist to consider referring those claims which show indication of potential fraudulent activities.
7. Who can make a claim?
The Trust, as an employer is vicariously liable for any tort committed by an employee in the course of his or her employment. The Trust has a duty of care in law, and a claim can be made if that duty is breached and if the claimant has suffered an injury, provided that breach has caused the injury.
Any patient, member of staff or the public or their personal representative in the case of death, who has suffered an injury or loss in accordance with the above definition, has the right to make a claim for damages.
8. Limitation
A claim must be made within 3 years (called the limitation period). The limitation period starts either from the date of:
Treatment, OR
Knowledge, which is when a claimant has realised that they have suffered an injury.
It is always safer to assume that the 3 year time limit runs from the date of the treatment that caused injury unless a solicitor advises otherwise.
In the case of children, the 3 year limit does not start until their 18th birthday. This means that a child who was injured when they were born would have until they were 21 years old to take legal action, but they do not have to wait until then. Before they are 18 years old, a parent or other person to them can make a claim on their behalf, acting as their “Litigation Friend”.
When defending a claim the timescales and procedures for the exchange of information with other parties relating to the period within which a claim should be brought are known as the “limitation” period and described further in Appendix C.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 12 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
9. Communication with Relevant Stakeholders
The Legal Claims Manager ensures that there are relevant communications with the various stakeholders. This includes giving and receiving instructions, updates, direction and advice to and from the following bodies:
NHS Litigation Authority – clinical negligence and non-clinical claims.
Panel Solicitors (who are instructed by the NHS Litigation Authority)
Claimant and Defendant Solicitors
North and East Devon Legal Services – to include clinical negligence claims and inquests.
Care and Quality Commission.
Health and Safety Executive
HM Coroner for Exeter and Greater Devon which falls under Devon County Council.
Mental Health and Learning Disability Services which falls under the Devon Partnership NHS Trust (including wards and Units located on North Devon District Hospital site and Centres within the community).
10. Saying Sorry – Press Release – December 2013
Saying sorry when things go wrong is vital for the patient, their families and carers, as well as to support learning and improve safety. Of those that have suffered harm as a result of their healthcare, 50% wanted an apology and explanation. Patients, their families and carers should receive a meaningful apology – one that is a sincere expression of sorrow or regret for the harm that has occurred.
The NHSLA has always encouraged Trusts to issue a verbal apology to patients as soon as staff are aware that an incident has occurred. A written apology, which clearly states the healthcare organisation is sorry for the suffering and distress resulting from the incident, must also be given.
Saying sorry is not an admission of legal liability; it is the right thing to do. Healthcare professionals should explain that new information may emerge as an investigation is undertaken, and that patients, their families and carers will be kept up to date with the progress of an investigation.
It is important that all healthcare organisations create an environment in which members of staff are encouraged to report patient safety incidents. Staff should feel supported throughout the investigation process because they too may have been traumatised by being involved.
For more information Saying Sorry leaflet at (Appendix D)
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 13 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
11. Duty of Candour
The Duty of Candour is a legal duty on hospital, community and mental health trusts to inform and apologise to patients if there have been mistakes in their care that have led to significant harm.
Duty of Candour aims to help patients receive accurate, truthful information from health providers. Under Duty of Candour staff should apologise when an incident occurs For more information see Duty of Candour Guidance documented at Appendix E and within the Trust’s Duty of Candour Policy.
12. Support for Staff
The receipt of a claim can be an upsetting experience for any member of staff. As a Trust, we are committed to ensuring that all staff are supported during the claims process:
The Trust will seek to ensure fairness, openness and impartiality during claims investigations.
As a Trust we always seek to accept where something has gone wrong and apologise for it.
Equally, if it is felt that the claim is unfounded or incorrect, the Trust will fully support staff and the service or services questioned.
Managers should discuss with staff options for support (e.g. Ward/ Team Manager, clinical supervisor, manager, occupational health, defence unions). The Trust has a Supporting Staff involved in an incident, complaint or claim Policy which is available on the Trust’s Intranet site.
Trust Solicitors and the Legal Claims Manager are available over the telephone for advice and will attend individual meetings upon request from both parties.
The NHS Litigation Authority has produced a fact sheet for clinicians which is available from their website www.nhsla.com
The Legal Claims Manager has produced the following leaflets to promote staff support and awareness of claims. These are documented at Appendices I-L:
Facing litigation (seeAppendix F)
Legal Claims Awareness (see AppendixG)
Writing a Legal Report (see Appendix H)
Preparing for an Inquest (see Appendix I)
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 14 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
13. Links with Corporate Governance processes
The responsibilities for risk management and corporate governance are stated in the Risk Management and Clinical Governance Strategies. In these documents the Chief Executive Officer and the Executive Directors have overall accountability for leading the processes. Non Executive Directors are responsible for ensuring significant risks are being managed effectively by testing the level of assurance provided.
The Risk Management Strategy and Policy state that a risk assessment be considered on all accidents/incidents and complaints assessed as high priority. This will ensure the event is captured in the risk register and subject to internal control and assurance.
Prior to the notification of a claim a number of processes may have already been instigated following a serious incident in line with the following:
Investigations Policy
Raising Concerns and Complaints Policy
Health & Safety Policy
The primary or dominant purpose of this latter process, the Serious Investigations Requiring Investigations (SIRI) is to identify learning and improve patient safety and the quality of care. Trust Boards have a clear duty to investigate serious incidents and satisfy themselves that all reasonable steps have been manage risks and taken to prevent recurrence. This has to be done openly and within a culture that seeks to learn from the event. This philosophy runs directly counter to the adversarial principles which underpin the conduct of litigation. It is therefore vital to ensure that investigations and root cause analysis are factual, and that both the recommendations and further actions are based on evidence rather than supposition and anecdote. Where there are links with an NHS Complaint Investigation the modules are linked on DATIX and the complaint file is immediately made available to the Trust Solicitors. If there is intimation that a claim may be received or that risks to the Trust are identified during a complaint investigation, the Trust Solicitor is alerted who will liaise with the NHSLA. Additionally, the Trust Solicitor is also requested to scrutinise the Trust’s response prior to sending the final response letter to the complaint.
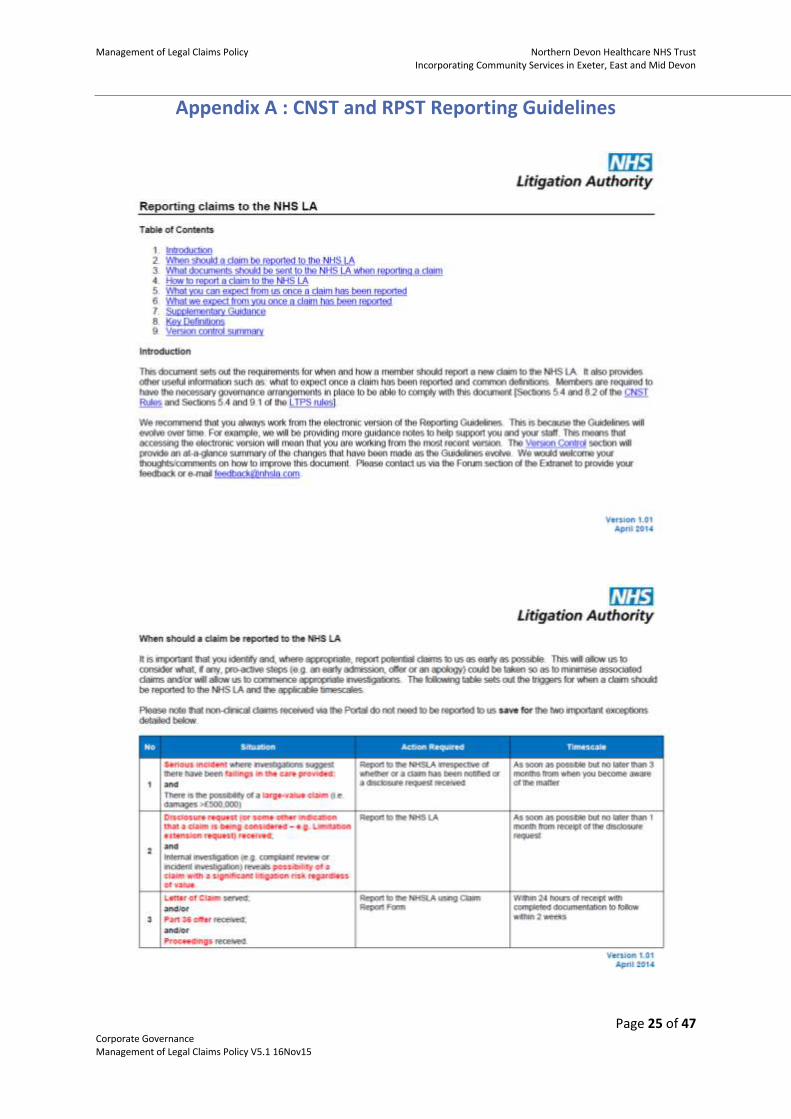
Where there are links with both internal investigations for example through Significant Event Audit (SEA), Significant Incident Requiring Investigation (SIRI) processes or external enquiries through the Care Quality Commission (CQC) that identify significant issues requiring indemnity these cases are required to be reported externally to the NHS Litigation Authority (see Appendix A detailing CNST and RPST reporting guidelines).
All significant SEA and SIRI investigation reports which are independent to, or directly related to a legal claim or Inquest are required to be scrutinised by Trust Solicitors prior to ratification.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 15 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
The Trust may consider in certain circumstances, to involve external agencies in a claims investigation. This could be when there is insufficient expertise within the Trust or if specialist skills are needed such as testing equipment. Occasionally, the Trust will need to eliminate bias and again involve a third party for an objective opinion.
In some circumstances external stake holders such as the Department of Health, Care Quality Commission, Clinical Commissioning Group, Ombudsman, Health & Safety Executive, Police or HM Coroner will need to be informed. This will be dependent on the particulars of the case and political sensitivity.
14. Management of Personal Injury Claims – Non Clinical
In 2013/14 the NHS Litigation Authority received 4,802 (including potential claims) in respect of its non-clinical schemes (RPST).
In 2012/13 the figure was 4,632.
Non-clinical (RPST) claims are received through a national centralised “Claims Portal” system only authorised and accessed by the Legal Claims Manager. Claimants issue their allegations within a “Claim Form” submitted through this Portal system which is issued against the Trust’s indemnifiers i.e. the NHS Litigation Authority. They automatically acknowledge the Claim and forward all documentation through the Portal system for the Legal Claims Manager to access and begin investigations.
Through the new Portal system the Trust has 30 days for Employer Liability claims and 40 days for Public Liability claims, to investigate the allegations, interview staff, conduct an “initial analysis claims investigation” supply a formal decision on Trust liability (either admit, in part of full, or deny), gather and supply documentary evidence for the NHS Litigation to respond with directly back to the Claimants via the Portal system.
Management of claims outside of the national centralised “Claims Portal” system attracts costs to the Trust therefore management of non-clinical (RPST) claims within the “Portal” system is both cost effective and reduces the lifespan of a claim.
The majority of non-clinical (LTPS) claims are linked to incidents which meet the Reporting of Incidents, Diseases and Dangerous Occurrences Regulations (RIDDOR) and will have been investigated in accordance with the Trust’s RIDDOR Policy. The Health & Safety Executive (HSE) Report will be submitted to the NHS Litigation Authority together with supporting evidence. (See Appendix A reporting guidelines)
15. Management of Clinical Negligence Claims
In 2013/14, the NHS Litigation Authority received 11,945 claims (including potential claims) under its clinical negligence schemes (CNST).
In 2012/13 the figures were 10,129.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 16 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
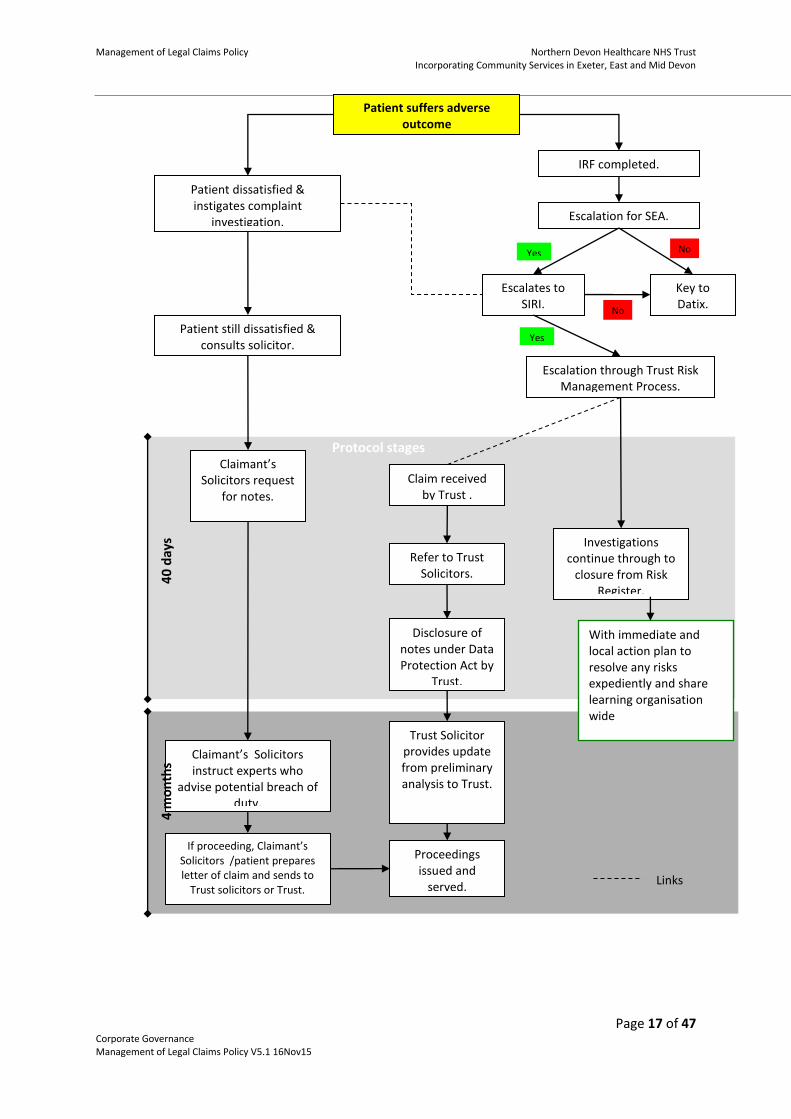
Since the Marsh review, claims in the NHS have increased significantly and the NHS Litigation Authority has welcomed the National Clinical Assessment Service (NCAS), which supports organisations and practitioners with performance concerns, as an operating division on 1st April 2013. The response to the Marsh report highlights how the NHS Litigation Authority has risen to the challenge of dealing with an increased number of claims, improved performance and ensured that costs are effectively managed.
Below outlines the management of an assumed negligence process.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 17 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Patient suffers adverse outcome
Patient dissatisfied & instigates complaint
investigation.
Patient still dissatisfied & consults solicitor.
Escalates to SIRI.
IRF completed.
Escalation for SEA.
Key to Datix.
Escalation through Trust Risk Management Process.
Claim received by Trust .
Refer to Trust Solicitors.
Disclosure of notes under Data Protection Act by
Trust.
Trust Solicitor provides update from preliminary analysis to Trust.
Proceedings issued and
served.
Investigations continue through to
closure from Risk Register.
Claimant’s Solicitors request
for notes.
Claimant’s Solicitors instruct experts who
advise potential breach of duty.
If proceeding, Claimant’s Solicitors /patient prepares letter of claim and sends to
Trust solicitors or Trust.
Yes
No
Yes
No
Links
Protocol stages
40
day
s 4
mo
nth
s
With immediate and local action plan to resolve any risks expediently and share learning organisation wide
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 18 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
16. Management of Inquests
Inquests are managed by Trust Solicitors with local support provided by the Legal Claims Manager. Please see attached Standing Operating Procedure for the management of Inquests and supporting staff information leaflet at Appendix J.
16.1. The HM Coroner for Exeter & Greater Devon District
The Coroner investigates all unexpected, accidental and/or suspicious deaths. She is assisted in this by officers from Devon and Cornwall Police as well as local pathologists. Part of her work includes conducting inquests into these deaths which are attended by interested parties and sometimes expert witnesses. Inquests are commonly held at venues which are conveniently close to the local communities or, in some circumstances, at County Hall in Exeter.
Her Majesty’s Coroner for the Exeter and Greater Devon District which includes North, West and East Devon is:
Dr Elizabeth Earland H.M. Coroner County Hall Topsham Road Exeter EX2 4QD Tel: 01392 383636 Fax: 01392 38363
16.2. Preparation for an Inquest Hearing
The HM Coroner will contact Trust Solicitors in the event that she requires further information to ascertain how the patient died. Statements will requested by Trust Solicitors to the staff involved in the patient’s care for the Coroner’s purposes.
Statements are disclosed to the HM Coroner she will call a Hearing which staff may or may not be required to attend. Trust Solicitors attend all Hearings where there are members of staff called as witnesses or whether there is an anticipated or potential risk of a Coroner’s Regulation 28 report.
Where necessary, press statements will be prepared in advance of the Hearing. Should staff be required to attend Trust Solicitors will meet with those staff providing guidance and support prior to the Hearing.
If staff are to be called to the Hearing they must ensure they are equipped with a copy of their signed statement, any other associated documentation i.e. copy medical records, reports. Trust Solicitors will meet with the staff at the Court prior to the Hearing to prepare the witness(es) with a chance to view the Court Room beforehand. Staff must attend if called and arrive promptly, suitably dressed.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 19 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
After the Hearing and the verdict is announced the Trust Solicitor will provide the Trust with an attendance note and advise the witnesses (whether they are required to attend or not) of the outcome with any issues or risk management recommendations from the HM Coroner.
16.3. Regulation 28 Reports
The HM Coroner has the power under Regulation 28 of the Coroners (investigations) Regulations 2013 to issue a report where the evidence at the Inquest gives rise to a concern that a similar death may occur in the future.
The Coroner may issue a regulation 28 report where she feels action should be taken to reduce the risk of future deaths. If a regulation 28 letter is sent, the Trust must respond to the Coroner within 56 days (or longer if agreed by the Coroner). Such letters may be received where, for example, it appears to the Coroner that Policies or Procedures have not been followed, or need amendment or review.
The Trust Solicitors will liaise with the Legal Claims Manager when regulation 28 reports are anticipated to ensure that an appropriate statement is forwarded to the Coroner dealing with issues likely to fall within the regulation 28 report. However the response to the Coroner must be from the Trust’s Chief Executive.
17. Lessons Learned arising from Claims
The Trust is committed to learn and make changes to practice and improve services and safety as a result of claims. The Trust’s systematic approach to encourage learning and promote improvements in practice based on individual and aggregated analysis of claims is a key aspect of the Risk Management Strategy and the Trust’s Clinical Risk Management Standards.
The identification of a risk following claims investigation will be considered for inclusion in the relevant local/divisional/corporate risk register with plans to manage, reduce the risk and thereby learn lessons.
The Risk Management Team provides support to clinical teams to produce and implement action plans to develop practice following an investigation. Monitoring of progress against any agreed action plans is undertaken by divisions in their consideration of risk management.
Lessons learned are disseminated by the Legal Claims Manager to all staff involved in the individual claims through risk management reports, bespoke teaching sessions or via divisional Governance days. Quarterly reports to the Trust’s Audit and Assurance Committee also detail lessons learned in general and for each claim whereby financial compensation has been awarded.

Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 20 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
The turnover of those lessons learned from non-clinical (RPST) claims are generally managed quicker due to their reactive nature and management of appropriate reasonably practicable control measures, robustly reducing likelihood of further risk of injury. The Health & Safety and Legal Claims Managers are within the same “Compliance” team which offers effective resilience and strong partnership involvement.
Where appropriate the Trust will also inform and share learning with external stakeholders such as commissioners and Trust/Panel Solicitors to inform any Solicitor Risk Management reports that may be shared with other organisations, The Legal Claims Manager has secured access to the NHS Litigation Authority web-based administration system which supplies case studies, pod casts, videos, guidance and best practice guidance to share with the Trust to enhance and promote learning from claims.
18. Monitoring and Reporting Claims Activity
18.1. Quarterly Reports
The Legal Claims Manager will produce quarterly claims reports for the confidential sections of the Audit and Assurance Committee.
This report includes details of:
New claims (clinical, non-clinical and Inquests) received within the quarter.
All settled and closed claims (clinical, non-clinical and Inquests) within the quarter including those non-clinical claims recorded on the losses register.
Links to other processes (Incidents, Serious Incident Requiring Investigation, Significant Event Audits, Complaints, Inquests, other Claims, Patient Advice and Liaison enquiries, Human Resources issues, and risks recorded on the Corporate Risk Register).
Financial reserves.
Trends
Benchmarking against regional numbers of claims received by the NHS Litigation Authority
On-going claims information.
Identified Risks.
Legal Updates.
Exception issues arising.
18.2. Key Performance Indicators (KPIs)
The Legal Claims Manager will produce monthly claims reports for the Senior Corporate Governance (Compliance) Manager for the Commercial Service Division for local compliance with measurable KPIs.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 21 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
19. Training Requirements
The Legal Claims Manager provides training on an ad-hoc basis for claims awareness sessions for attendances at Directorate Governance Days or individual teams.
Where staff are required to undertake claims training within specific policies the Trust’s training matrix will detail:
Staff groups requiring training.
Frequency of training.
Mode of delivery i.e. e-learning or taught.
Course titles.
Bookings for those staff required to undertake claims training within specific Policies will be undertaken through Workforce Development via the Electronic Staff Record. Signed records must be kept of all training undertaken in the Trust. These records will be held centrally and reported Trustwide through ESR records. Individuals are encouraged to keep a copy of this in their portfolio.
20. Monitoring and Auditing Compliance with the Effectiveness of the Managing Legal Claims Policy
20.1. Standards / Key Performance Indicators
Key Performance Indicators include:
Reduction in the number of claims and injury to NHS patients, staff and visitors of similar nature because of changes in practice as a result of organisational learning.
Improved patient experience measured through a reduction in Complaints and Claims.
Reduced financial compensation paid out due to changes and actions taken following organisational learning and management of identified risks.
100% compliance with timescales
20.2. Process for Monitoring Compliance and Effectiveness
The process to monitor the standard key performance indicators (above) include:
Collation and reporting full claims data to the Audit and Assurance Committee on a quarterly basis.
Collation and reporting of all linked processes in complaints and claims to Audit & Assurance Committee
Collation and reporting of all compensation payments with lessons learned and prevention of recurrences data.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 22 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Collation and reporting closed claims to Audit and Assurance Committee within these reports it will detail non-clinical claims links through the Trust’s losses register demonstrating those claims paid under the Trust’s non-clinical excesses.
Compliance to timescales is monitored through an audit form within each case file.
Corporate Governance (Compliance) key performance indicators (KPIs) feed into the Commercial Services division for compliance to the divisional KPIs through the Trust’s Performance Management team.
Periodically but no less than every four years, an audit of Trust compliance with NHS Litigation Authority standards will be conducted. This may be completed by Internal Audit or Corporate Governance staff. The outcome of the audit will be presented to the Quality Assurance Committee and/ or the Audit and Assurance Committee. Any deficits found will be subject to an action plan and monitored through the aforementioned committees.
Services provided by the Trust Solicitors are in accordance with a formal Service Legal Agreement which will be subject to annual review. The Service Level Agreement states monitoring arrangements and responsibilities for compliance.
20.3. Monitoring Arrangements Compliance of this policy against all minimum requirements in the Trust’s Clinical Risk Management Standards will be monitored on a case by case basis evidenced through quarterly reports.
20.4. Responsibility The Legal Claims Manager will be responsible for monitoring key performance indicators reporting to the Senior Corporate Governance (Compliance) Manager.
20.5. Methodology The Legal Claims Manager will use standard audit and spreadsheets using key performance indicators to monitor compliance with national guidance and legislation such as:
Pre-Action Protocol for the resolution of clinical disputes.
Pre-Action Protocol for Personal Injury Claims.
Trust Policies and Procedures.
20.6. Reporting Arrangements
The result of the audit will be reviewed by the Investigations Team as and when audits are undertaken or required.
The Corporate Governance (Compliance) team will develop an action plan to improve compliance and ensure improvements in performance occur. Action plans will be implemented by the Legal Claims Manager to ensure learning takes place.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 23 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
The Corporate Governance (Compliance) team will monitor progress of the action plan on a monthly basis and exceptions will be reported via this Team to the Audit and Assurance Committee. Identified risks related to non-compliance with this policy will be registered on the Trust Risk Register.
21. References
NHSLA website, www.nhsla.com “CNST reporting guidelines version 1.01 April 2014 [Publication-Claims publication]
NHSLA website www.nhsla.com “LTPS reporting guidelines version 1.01 April 2014” [Publications – Claims publications]
www.gov.uk website (2015) “factsheet – Unjustified Personal Injury Claims”
NHSLA website, www.nhsla.com
NPSA website www.npsa.nhs.uk.
22. Associated Documentation
Raising concerns and complaints policy
Risk Management Policy
Supporting staff involved in an incident, complaint or claim policy
Raising Concerns and Complaints Policy
Risk Management Policy
Supporting Staff involved in an incident, complaint or claim Policy
23. Quality Impact Assessment
Table 1: Equality impact Assessment
Group Positive Impact
Negative Impact
No Impact
Comment
Age X
Disability X
Gender X
Gender Reassignment X
Human Rights (rights to privacy, dignity, liberty and non-degrading treatment)
X
Marriage and civil X
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 24 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
partnership
Pregnancy X
Maternity and Breastfeeding
X
Race (ethnic origin) X
Religion (or belief) X
Sexual Orientation x
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 25 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
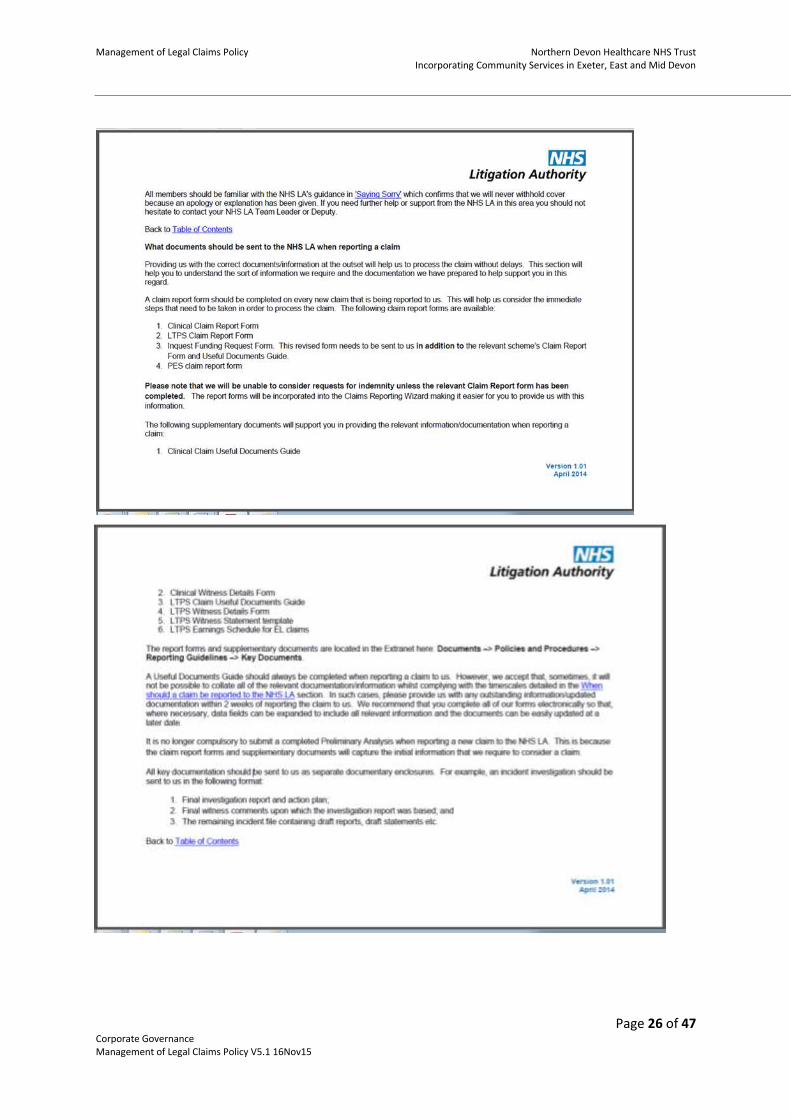
Appendix A : CNST and RPST Reporting Guidelines
Appendix A : CNST and RPST Reporting Guidelines
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 26 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 27 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
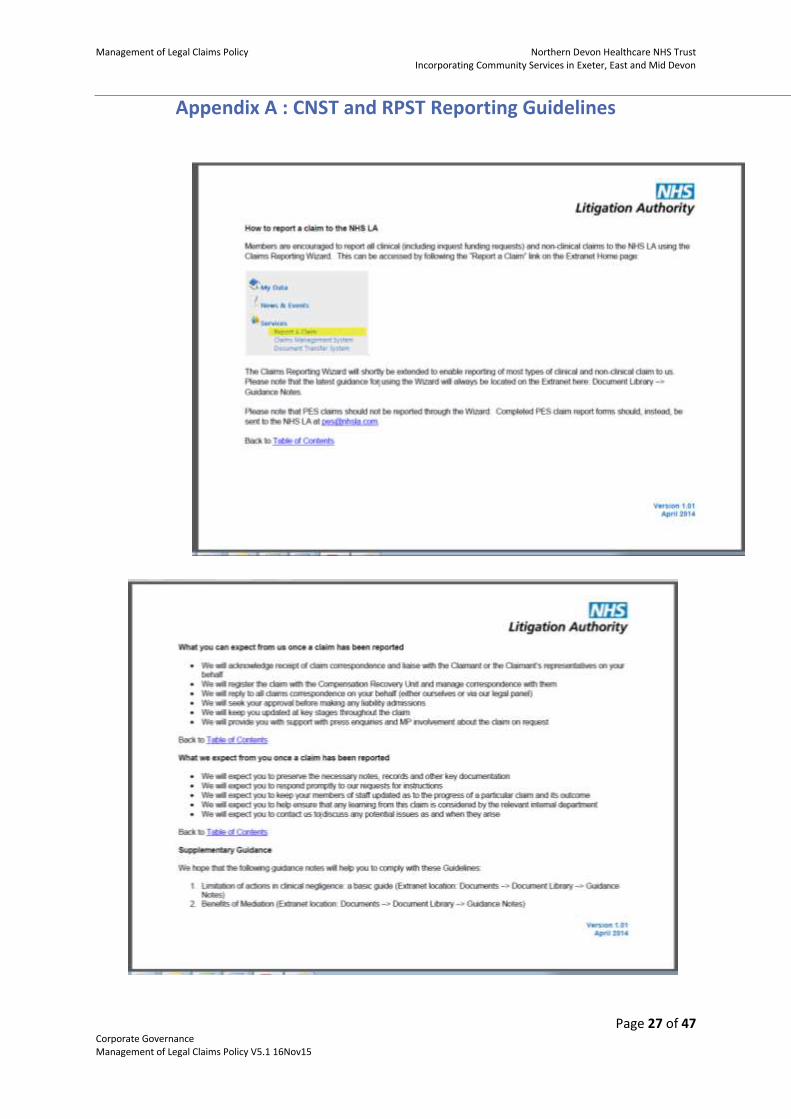
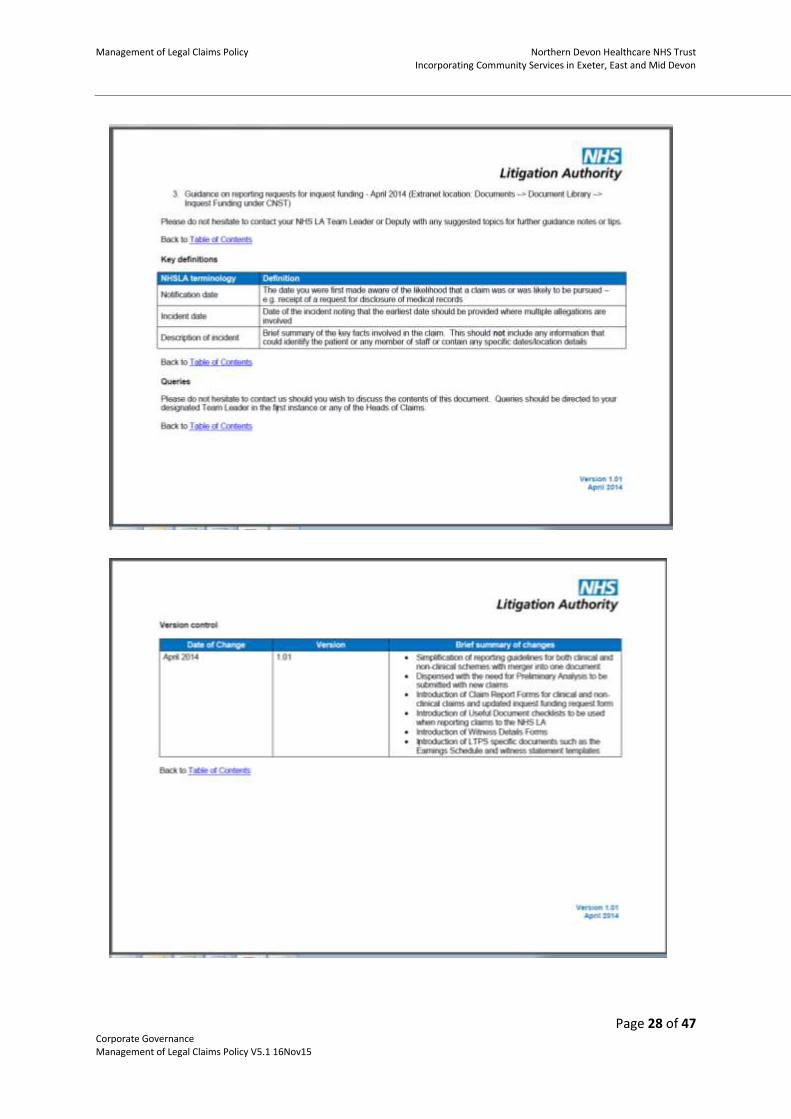
Appendix A : CNST and RPST Reporting Guidelines
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 28 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix B : NHS Indemnity
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 29 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix B : NHS Indemnity
The NHS Executive issued updated guidelines on ‘NHS Indemnity – arrangements for handling clinical negligence claims against NHS staff’ under HSG(96)48 on 8 November 1996. This guidance is still current and confirms that all NHS staff are covered under NHS indemnity for harm caused by any acts or omissions whilst carrying out their NHS work. The guidance states that for those covered under NHS Indemnity the NHS body (now the NHS Litigation Authority) should accept full financial liability where negligent harm has occurred and should not seek to recover their costs from the health care professional involved. If staff are to benefit from the protection offered by NHS Indemnity it is fair that in return they co-operate fully with the claims management process. A very useful document is included with the guidance which includes Questions and Answers on various indemnity issues. The full text is available on line in the Documents section of the NHS Litigation Authority website at www.nhsla.co.uk under publications/claims publications/NHS Indemnity. A snapshot of this guidance is detailed below.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 30 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix B : NHS Indemnity
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 31 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
24.
25.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 32 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix B : NHS Indemnity

Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 33 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix B : NHS Indemnity
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 34 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix B : NHS Indemnity
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 35 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix C : Limitation
LIMITATION
1. Currently the Limitation Act 1980 is the key legislation which applies. This legislation seeks to strike a balance between the competing interests of Claimants and Defendants. It seeks to avoid the litigation of claims which are too old and where the evidence may no longer be available whilst still allowing actions to proceed where the strict application of time limits would result in unfairness to the Claimant.
2. In practice the commencement of a claim means the ‘issue’ of the Claim Form by the Court. For personal injury and clinical negligence claims the Claimant should issue their Claim Form through the Court within a period of 3 years of the date of incident which allegedly caused them harm or within 3 years of their ‘date of knowledge’ if this can be proven to be later.
3. The exceptions to this are:
i) children – their 3 year period does not commence until they reach the age of majority at 18 years i.e. their primary limitation period expires at age 21.
ii) people under a ‘disability’, i.e. ‘of unsound mind’ who are incapable of managing
their own affairs. Such people may bring an action at any time whilst they remain under a disability. In view of their on-going disability the claim is usually brought on their behalf by a ‘Litigation Friend’.
4. For claims for deceased patients being brought by their Personal Representative under the Law Reform (miscellaneous provisions) Act 1934 or the Fatal Accidents Act 1976 – the following applies:
If the person injured dies before the expiration of the 3 year period, the period applicable, as respects the cause of action surviving for the benefit of his estate by virtue of S.1 of the Law Reform (Miscellaneous Provisions) Act 1934, shall be 3 years from the date of death or the date of the personal representative’s knowledge, whichever is the later. The time limit for bringing an action on behalf of dependants under the Fatal Accidents Act 1976 for bereavement damages or a dependency claim is 3 years from the date of death or from the date of knowledge of the person for whose benefit the action is brought, whichever is later. However, an action for bereavement/dependency under the Fatal Accidents Act 1976 shall not be brought if the death occurred when the person injured could no longer maintain an action to recover damages in respect of the injury (Limitation Act 1980 S.12 (1)).
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 36 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
5. Date of Knowledge
Date of knowledge is when the claimant first had knowledge that the damage was significant and attributable in whole or part to the act or omissions of the Defendant. Significant case law in recent years has led to the concepts of actual and constructive date of knowledge – i.e. when did the Claimant first obtain knowledge and when should they have first obtained knowledge.
6. The Court’s discretion to disapply the Limitation Period
Even though the Defendant may seek to put up a ‘limitation’ defence – the court has the discretion to disapply the limitation period under Section 33 of the Limitation Act.
Before doing so the Court will consider the facts of the case, the reasons for the delay etc and whether or not the Defendant will be prejudiced if the action goes ahead.
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 37 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix D : Saying Sorry Leaflet
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 38 of 47 Corporate Governance Management of Legal Claims Policy V5.1 16Nov15
Appendix E : Duty of Candour
Corporate Governance Page 39 of 47 Legal Claims Policy V5.1 16Nov15
Over the past few years, there has been a national increase in the number of complaints and compensation claims against the Health Service. Statistically, it now seems that you are likely to be involved in a litigation claim every five years throughout your professional life. These odds appear to be shortening…Why? Many reasons are given by the patients involved but the most common appear to be these:
To prevent the same thing happening to anyone else.
To try to establish the true facts. We are often told that a patient’s motive is to find out what really happened. Sadly, they also frequently add that they have never received a proper explanation from the health workers concerned and that the first time they were ever taken seriously was when they involved solicitors.
To get compensation. Coupled with that, we have seen a great increase in what patients expect from the Health Service. People are aware of huge advances in medical technology and are unwilling to accept anything less than a perfect outcome. Medicine is a victim of its own success in this respect. In addition, patients appear more aware of their “rights”. Part of this may be that health issues always attract media interest and wide publicity. The purpose of this leaflet is to inform you of the steps you should take if you are faced with a claim. It is also to assist and to guide you through the litigation process. WHO PAYS FOR LITIGATION? Until 1990, all doctors insured themselves through a Medical Defence Organisation. Although GPs and Consultants performing private work still do so, this is no longer the case with NHS employed doctors, who have been indemnified by the health service since 1990, in line with other NHS employees. A central funding
Appendix F: Facing Litigation leaflet
system has been set up – the NHS Litigation Authority, which oversees all compensation claims. BUT cost cannot be measured solely in financial terms. Issues such as professional reputation and public confidence must not be forgotten. The time spent by clinicians analysing medical records, attending meetings with solicitors, preparing witness statements and attending court is immeasurable. So too can be the human cost in terms of stress. WHEN LITIGATION IS THREATENED You may become aware that a patient is considering legal action in a number of ways:
The patient tells you.
The patient or a relative uses the Complaints Procedure to investigate their grievance but is not then satisfied with the result.
You may receive information from the Trust’s Legal Manager, or solicitor, informing you of a potential claim and asking for your comments. If the claim is being made against a hospital you no longer work in, notification almost always comes from the Trust’s solicitors – but make sure it is from them and not from the patient’s own solicitors.
You receive a (patient’s) solicitor’s letter, outlining the patient’s care which they claim was deficient and requesting copies of the medical records.
You receive a formal request under the Access to Health Records Act for the release of hospital records. This may not necessarily be because the patient is contemplating litigation but such a request, particularly if it is from a solicitor, should always prompt that suspicion.
Occasionally, the first intimation of legal action is the service of Court Proceedings. This is rare and usually arises where a patient has delayed instructing solicitors.
THE INITIAL RESPONSE When you are told of a potential claim, it is absolutely vital that you act promptly. Clinical negligence claims are now dealt with under the terms of the Pre-Action Protocol, introduced by Lord Woolf in the Civil Justice Reforms of 1999. Timetables are short and very strict. A failure to comply can result in heavy penalties, including fines, and in extreme cases the Court can even strike out the delaying party’s case, so a patient could win their claim by default. If you have been notified direct, for example, by a letter from the patient’s solicitor, it is very important that you bring it to the attention of the hospital’s litigation manager immediately. He or she will then take all necessary steps to comply with the protocol. WORKING THROUGH THE PROTOCOL
Disclosure of records – This is always the first formal step in the process. The patient’s request should now be made on standard form, along with sufficient information to let you know the nature of the claim. The patient is also required to be as specific as possible as to the records required. Copies MUST then be supplied by the hospital within 40 days of the request. Failure could result in the patient applying for Court Order, with costs penalty against the hospital. If disclosure within this time frame is not possible, for example, the patient is receiving outpatient treatment, perhaps in another department, then the problem should be explained quickly and details given of how it is being resolved. It is worth mentioning that the protocol envisages that this will only happen in rare circumstances.
The letter of claim – If the patient decides to proceed, he/she must
write a formal Letter of Claim. If solicitors have not been involved before this point, they will almost certainly become so now and this letter will usually come from them. It
Management of Legal Claims Policy Northern Devon Healthcare NHS Trust Incorporating Community Services in Exeter, East and Mid Devon
Page 40 of 47 Legal Claims Policy V5.1 16Nov15
should contain specific information, including a clear summary of the facts; the main allegations; details of the injuries and outline of the financial loss of the patient has suffered. More complicated cases should also include a chronology of events. Once this letter has been received, the litigation process gathers momentum. The patient becomes a “claimant” and investigation into their allegations MUST begin in earnest.
The acknowledgement – Generally, any letter of claim will be addressed to the hospital’s Legal Manager. If for some reason it comes to you, please pass it on to the Legal Claims Manager without delay. The Protocol requires that the hospital replies to the claimant or their solicitor within 14 days, acknowledging the Letter of Claim and identifying who is dealing with the matter.
The reasoned response – Within four months of the Letter of Claim, the hospital must provide a Reasoned Response to the allegations. This may be in the form of an admission of liability (either a full or a partial admission, in which case it is important to specify exactly which allegations are admitted and which are denied, giving reasons.) or a denial of liability. If this is the case, the hospital must deny the allegations specifically, providing an alternative explanation and chronology to account for the adverse outcome.
WHEN WILL YOU BE ASKED FOR INFORMATION? This depends very much on the nature of the claim and in what capacity you were involved. Increasingly however, investigations will begin promptly and your input will play a vital part. This subject is covered in detail in our leaflet
entitled “Writing A Legal Report”
which explains when you are likely to be involved and what information you will be asked to provide. A FINAL NOTE Please try not to feel concerned about the prospect of litigation. Help and advice is always available. Initially seek the help and support from your Line Manager who will provide guidance. If you would like to speak to someone, do contact the hospital’s Legal Claims Manager, who will then be able to call the Trust’s Solicitors if additional support is necessary. Please note that contained within “BOB” is the Claims Handling Policy and the Supporting Staff Policy which are also forms of support and guidance for anyone facing a legal claim. CONTACT The sources of support that will be beneficial to you personally are individual professional bodies and your Line Managers. If your Line Manager requires support they should contact: Legal Claims Manager Corporate Governance Suite 1, Munro House Northern Devon Healthcare NHS Trust Raleigh Park Barnstaple Devon EX31 4JB Direct Line: 01271 314082 (with voicemail) Email: [email protected] Trust Solicitor North & East Devon Legal Services Royal Devon & Exeter Hospital (Heavitree) Gladstone Road Exeter Direct Line: 01392 405286
FACING
LITIGATION
CORPORATE GOVERNANCE
Legal Claims Manager
Mrs Sharron Bates
June 2014 Produced by S Bates In Association with Bevan Brittan Solicitors
Management of Legal Claims Policy
Corporate Governance G:\Corporate Governance\Compliance Team\Policies Procedural Documents\Published Policy Database\Corporate Governance\claims policy\Legal Claims Policy V5.1 16Nov15.docx V2.0 10Jul15 Page 41 of 47
Appendix G: Legal Claims Awareness leaflet WHO AM I? Sharron Bates Legal Claims Manager Corporate Governance Directorate Based at: Suite 8, Munro House Northern Devon Healthcare NHS Trust Raleigh Park Barnstaple Devon EX31 4JB Tel: 01271 314082 Office hours: 08.30am – 16.30pm Monday – Thursday Email: [email protected] WHAT DO I DO? I have been with the Trust for 18 years, 16 of them working in Legal matters and now manage the Legal Claims Department. I manage all personal injury claims (claims brought by members of staff, contractors, visitors etc, anyone using our premises) across the Northern Devon Healthcare Trust including community services in Exeter, East and mid Devon I am the Trust liaison and contact point for all clinical negligence claims and Inquests. I manage all risk management issues arising from all legal claims and am here to support staff through this process. OUTLINE OF STAFF ROLE IN LEGAL CLAIMS What do you do if you receive legal documentation? Firstly, do not panic! Contact me either by phone or email if you are worried about what has been received. Send the documentation to me so I am able to investigate what is being requested. In any legal query, I am happy to help and advise. If further advice is needed I am able obtain this, communicating to you what action has been taken and provide you with a general update.
The key message is, please contact me, send me any legal documentation, I am here to help in anyway I can. The Claims Handling Policy and Supporting Staff policy is available on ‘BOB’ for your information, guidance and support. TRUST SOLICITORS This Trust has a Legal Team based in Exeter who manage our clinical negligence claims only. They are extremely approachable and are more than happy to receive queries or calls in relation to legal matters. They are a fantastic source of support for staff members and cases providing a professional legal service at a local level. They are: North & East Devon Legal Services Royal Devon & Exeter Hospital (Heavitree) Gladstone Road Exeter EX1 2ED Office Tel: 01392 405286 Emails: [email protected] The Team consists of: Sue Walsh -Trust Solicitor Claire Hyatt - Assistant Trust Solicitor Jennie Holvey - Legal Claims Handler Jo Cunningham - Legal Claims Handler Catherine Maunders - Senior Legal Secretary Dawn Lush - Legal Secretary Office hours: 9.00am – 5.00pm Monday-Friday
In a nutshell, the Trust Solicitors provide the following service:
Act as Trust Defence Solicitors
Work within a delegated authority
Provide Legal Advice
Update/feedback to Legal Claims Manager
Process & attend Trust Inquests
Obtain clinicians’ comments / liaisons with clinical staff
Commission Independent Experts
Liaison with NHS Litigation Authority & Panel Solicitors
Prepare & Serve Defences/Settlements
Attend Trials
PANEL SOLICITORS
When a clinical negligence claim reaches beyond the Trust Solicitors’ delegated authority the case is passed to our Panel Solicitors which are:
Messrs Bevan Brittan LLP Solicitors Kings Orchard 1 Queen Street Bristol BS2 0HQ Tel: 0844 736 1000 Fax: 0844 736 1001 They work closely with the Legal Team and myself in order to secure the Trust’s defence. All personal injury claims are managed by myself. However, if a personal injury claim is required by the NHS Litigation Authority to be managed by our Panel Solicitors they will refer the case to:
Brownejacobson LLP Solicitors 1 Manor Court Dix's Field Exeter EX1 1UP Tel (01392) 278381 Fax (01392) 410247 THE NHS LITIGATION AUTHORITY The NHSLA handles negligence claims and works to improve risk management practices in the NHS.
They are the Trust’s “Insurers”
They receive annual premiums to act
Their aim is to improve risk management within the NHS Litigation is increasing and costly to the NHS in financial terms. It must not be forgotten that there is also a human cost to both patients and staff. Improving patient experience is a non financial cost we can all play a part in. In order to reduce the risk of litigation the NHS Litigation Authority have put in place Risk Management processes which the Trust is obliged to report and act upon once their formal notification has been received by the Trust. RISK MANAGEMENT
Management of Legal Claims Policy
Corporate Governance G:\Corporate Governance\Compliance Team\Policies Procedural Documents\Published Policy Database\Corporate Governance\claims policy\Legal Claims Policy V5.1 16Nov15.docx V2.0 10Jul15 Page 42 of 47
A huge role in the Claims Department is managing risks. For claims exceeding a value of £50,000 the Trust’s Panel Solicitors will provide a formal risk management report to the
Trust and the NHS Litigation Authority. This will outline all recommended actions for the Trust to take following their investigations into the claim and allegations. These are managed through the Trust Risk management process, added to the Corporate Risk Register for assurance to the NHS Litigation Authority and Trust Board that lessons will be learned following recommendations from claims investigations. This sets a definitive programme of standards and assessments supported by education and learning No matter how big or small, all risks are identified throughout the entire life of a claim and those risks which may be unforeseen at the beginning can produce surprising trends for the Trust to act upon. All this is to ensure the Trust and staff are keeping patients safe, improving the quality of care and contributing to NHS risk management. WHAT HAPPENS DURING A NEGLIGENCE CLAIM? As a quick summary of what happens during a negligence claim here is a snapshot:
Trust receives the notification of an intended claim
Pre-Action Protocol is sent to the Trust for release of healthcare records
Disclosure of Healthcare records is undertaken in accordance with the Pre-Action Protocol and Data Protection Act 1988
Referral to Trust Solicitors is made upon receiving the notification and full disclosure once the notes are copied.
Trust Solicitors make initial Investigations into the allegations with staff members
Referral is made to the NHS Litigation Authority if appropriate.
A decision is made on liability.
Possible Trial and/or formal Conferences attended
Eventually settlement/closure
As an employee of the Health Service, there are several occasions in which you could be called upon to provide a report for use in a legal investigation.
Please remember that a negligence claim can be ‘live’ for many years, especially if the claim involves children or allegations from birth damages. If you are involved in a claim and you have not heard any updates, please don’t assume it has gone away. Please contact me or the Trust Solicitors if you wish to know any updates with regards to your involvement . WHAT HAPPENS DURING A PERSONAL INJURY CLAIM? A quick summary of what happens during a personal injury claim:
A formal Letter of Claim is received by the Trust
Time will be spent collating all the necessary evidence against the stated allegations.
The evidence and referral is made the NHS Litigation Authority within 3 weeks.
The claim continues to be managed by Desktop management (through me and the NHS Litigation Authority)
Decision on liability will be made upon the evidence provided.
If allegations are pursued despite a denial of liability the NHS Litigation will request one of their Claims Inspectors visits the Trust to further investigate.
Panel Solicitors (Brownejacobson) may be instructed at this stage.
Court proceedings if continuing to Trial.
If liability is accepted, negotiations will commence.
Settlement/Closure
Communications provided to the Trust with regards admissions, denial and risk management issues.
The turnaround of personal injury claims is relatively quick compared to clinical negligence. If you are involved in a personal injury claim it is important to keep accurate documentation such as risk assessments, incident report forms and updated entries to personnel files.
Appendix H: Writing a Legal Report leaflet
Primarily, that investigation is likely to be in relation to a civil claim for compensation, usually by a patient or one of
LEGAL CLAIMS
AWARENESS
CORPORATE GOVERNANCE
Sharron Bates
Legal Claims Manager
June 2014 Produced S Bates
their relatives in a clinical negligence action. There are other circumstances however, where you may be asked to make a report. If you have worked in Casualty, you may
Management of Legal Claims Policy
Corporate Governance G:\Corporate Governance\Compliance Team\Policies Procedural Documents\Published Policy Database\Corporate Governance\claims policy\Legal Claims Policy V5.1 16Nov15.docx V2.0 10Jul15 Page 43 of 47
already be familiar with Police Statements, which often require you to describe the injuries of an assault or road accident victim, whom you have treated. If you have been involved in the clinical care of a patient who has died, you may have been asked to provide a statement for the Coroner for use in an inquest hearing. This is particularly so if someone dies within 24 hours of being admitted to hospital; or shortly after an operation; or in circumstances where the cause of death is unidentifiable or suspicious. A “Statement” is a formal legal document, prepared by an individual who has been involved in some way in a situation that has become the subject of legal proceedings. It records the account of events an individual saw, heard or did. That individual is then a “Witness” in the proceedings. The statement records the “Evidence” the Witness will bring before the court and is of course prepared in contemplation of those proceedings. Before going further however, it is important to stress that if you are asked to provide a legal report, you will not be expected to produce it in the form of a legal document, ready for use as a witness statement. What is required initially is an informal but detailed report of your involvement. If it subsequently becomes necessary to produce a formal witness statement, the Trust’s Solicitors or the Legal Claims Manager will be on hand to help you do this and will usually draft the document for you. WHEN WILL YOU BE ASKED FOR INFORMATION? In Clinical Negligence actions, investigations may begin very soon after a patient makes a request for the release of their records – particularly if the claim is potentially very large or where there is evidence to suggest, even at an early stage, that it is indefensible. In other situations, investigations may not begin in earnest until after a formal “Letter of Claim” is received and it appears more likely that a claim is to be pursued. The hospital, or sometimes their Solicitors, will approach those involved in the care of the patient for their comments. If you are a Consultant or Ward Manager “nominally” in charge you may be approached quite frequently for an overview, even if you did not deal with the patient personally. In other cases, you are approached because your name appears in the medical records or the Letter of Claim.
If you no longer work at the hospital, you will be sent a copy of the records. Otherwise, it is best to get hold of the originals. WHAT INFORMATION WILL YOU BE ASKED FOR?
What happened? The first and most important step when investigating a claim is to establish as fully as possible what happened. The most effective testimony is the first hand evidence of those who were there – supported of course by contemporaneous clinical records. It may appear to clinicians that the notes give a full record. To the layperson, (such as a patient, a solicitor and a judge) however, they often contain abbreviations, assumptions and jargon, which make them less than clear. Try to consider the notes from a layperson’s view and consider what detail is missing. Try to identify five levels of information:-
What you know from your own knowledge and is substantiated by the notes.
What you remember but did not record at the time.
What you know was your normal practice at the time – perhaps substantiated by a protocol or guidelines – which you would have followed but where you can’t absolutely state was the treatment provided to this particular patient.
What you have forgotten.
What you know from others or from reading the records but you did not witness yourself.
What was the patient (or the family) told? There are two reasons to look at this. First, the issue of consent – was a patient given enough information about the nature and the risks of a treatment before they agreed to it? Secondly, particularly in cases where a claim seems unreasonable, this information may shed light on what it is that the patient is aggrieved about, which may in turn help with case management tactics. It is particularly important to consider what was said to a patient by senior staff, perhaps in outpatients, which may help with questions about consent.
Was anything less than perfect? In very many cases, when records are scrutinised in detail, departures from “best practice” become apparent. This reflects the fact that medicine is an imprecise science and clinicians are human. However, we should try to identify such areas of vulnerability at an early stage. Many will be wholly unimportant and irrelevant to the long term welfare of the patient. However, minor deficiencies can be used in court to embarrass the defence and to make the hospital look less capable than they are. There may also be more serious happenings. Again, these need to be identified as early as possible. They may even include unavoidable (non-negligent) complications of treatment, which the patient may have complained about and which the hospital can then explain in their “reasoned response”. It is for the claimant to prove negligence, by showing that the hospital staff failed in some way to provide acceptable care. The law states that you will be judged by clinicians in your own speciality. The claimant and the hospital’s solicitors will both take advice of appropriate clinicians from elsewhere. If it can be shown that “a responsible body of clinicians” would have acted the same way as you, there can be no finding of negligence.
Was the adverse outcome preventable? In order to succeed, the claimant must also show that any medical mistake or inappropriate treatment received has led to the adverse outcome they suffered. It is by no means always the case, just because a mishap occurs, that any damage the claimant suffers is as a direct consequence. However, if you consider that mishaps have indeed led to the adverse outcome, it is important to say so. It is in nobody’s interests to continue defending a claim that is indefensible. Your views on this are important. Remember, when considering whether mishaps have occurred, you should look at what was not done to the patient as well as what was done.
Why you did what you did In many cases, the notes record what you did but not why you did it. It is very helpful for the defence team to understand your treatment plan or strategy, particularly if decisions were made under time pressure or on clinical judgement. This information will also be vital to the experts who are looking at the records to determine whether treatment is negligent or not. Your comments may help to put the medical notes into perspective. Remember, an error of clinical judgement does not equate with negligence. It
Management of Legal Claims Policy
Corporate Governance G:\Corporate Governance\Compliance Team\Policies Procedural Documents\Published Policy Database\Corporate Governance\claims policy\Legal Claims Policy V5.1 16Nov15.docx V2.0 10Jul15 Page 44 of 47
is easy to see where decisions are wrong in retrospect but is helpful to have insight into the situation as it was at the time decisions were being made
What is your view of the patient’s prognosis? If liability is to be admitted by the hospital or if the case is lost in court, it is important to establish the degree of loss and damaged the patient has suffered, so that the level of compensation can be determined. You may no longer be looking after the patient, but you may still have a good idea of the severity of residual problems. If these are likely to improve, you should mention this. It is also important to try and distinguish between problems the patient now suffers as a result of a medical mishap and those which he/she would have suffered anyway as a result of unavoidable complications or illness.
What is your own background and experience? Information about your own level of experience and qualifications, particularly at the time of the alleged incident, is very important for the defence team’s investigation. Please do not feel reticent about giving these details. They are sought for genuine reasons. If the claim proceeds, the information you have provided will be drafted into a formal “witness statement” and placed before the court. These documents always contain information about the qualifications and experience of the individual concerned.
A FINAL NOTE Please try not to feel concerned about the prospect of litigation. Help and advice is always available. If you would like to speak to someone, contact the Trust’s Claims Legal Manager, who will then be able to contact the Trust Solicitors if additional support is necessary. CONTACTS The sources of support that will be beneficial to you personally are individual professional bodies and your Line Managers. If your Line Manager requires support they should contact us. Legal Claims Manager
Corporate Governance Suite 1, Munro House Northern Devon Healthcare NHS Trust Raleigh Park Barnstaple Devon EX31 4JB Direct Line: 01271 314082 (with voicemail) Email: [email protected]
Trust Solicitor North & East Devon Legal Services Royal Devon & Exeter Hospital (Heavitree) Gladstone Road Exeter Direct Line: 01392 405286
WRITING
A
LEGAL REPORT
CORPORATE GOVERNANCE
Legal Claims Manager Mrs Sharron Bates
June 2014 Produced by S Bates In Association with Bevan Brittan Solicitors
Management of Legal Claims Policy
Corporate Governance G:\Corporate Governance\Compliance Team\Policies Procedural Documents\Published Policy Database\Corporate Governance\claims policy\Legal Claims Policy V5.1 16Nov15.docx V2.0 10Jul15 Page 45 of 47
WHO IS THE CORONER? The Coroner may be a Lawyer or a Doctor (or hold both qualifications) and is an independent judicial officer who must investigate sudden death where the cause is unknown, violent or unnatural and decide:
who died how when where the medical cause of death
The Coroner must give a verdict. The Coroner investigates all unexpected, accidental and/or suspicious deaths. She is assisted in this by officers provided by the Devon and Cornwall Police (see Police) and local pathologists (see Health). Part of her work includes the conduct of Inquests into the death(s) and these are attended by interested parties and sometimes expert witnesses. Inquests are frequently held at venues which are conveniently close to the local communities or, in some circumstances, at County Hall, Exeter. Her Majesty's Coroner for the Exeter and Greater Devon District which includes North, West and East Devon is: Dr Elizabeth A Earland H.M. Coroner Room 226 County Hall Topsham Road Exeter Telephone: 01392 383636 Fax: 01392 383635 WHICH DEATHS SHOULD BE REPORTED? The Office for National Statistics (ONS) has in the past confirmed that in practice, doctors voluntarily report 60% of all deaths considered by a Coroner. If a doctor has not referred a relevant death to the Coroner, the Registrar has a statutory duty to do so. Common circumstances when the death will be reported are as follows:
when no doctor has treated the deceased during his or her last illness
when the doctor attending the patient did not see him or her within 14 days before death or after death;
when the death occurred during an operation or recovery from an anaesthetic;
Appendix I : Preparing for an Inquest
where the death was sudden and unexplained or attended by suspicious circumstances;
where the death might be due to an industrial injury or disease;
where the death may be due to an accident, violence, neglect or abortion or any kind of poisoning.
In the past there has been some doubt whether a death from AIDS should be reported to the Coroner. Legal advice confirms that a death from AIDS should normally be considered as a death from natural causes. Therefore, AIDS deaths should not usually need to be referred to the Coroner, unless there is some other separate ground for doing so. In any cases of doubt, the Coroner and his staff, the senior clinicians involved or the Trust’s Solicitors will help decide if a death should be reported. If the Coroner decides that the death is not due to a natural cause he must then hold an Inquest. THE INQUEST An Inquest is a fact finding exercise not a fault-finding exercise unlike a claim, civil or criminal court. There is no prosecution, no defence and no trial. It is not part of the Coroner’s role to probe into potential issues of medical negligence although sometimes an Inquest may be followed by a civil claim for damages, or a formal complaint and then a claim. Any report prepared for the Coroner will have to be shown to the patient’s relatives or their solicitors, if the patient’s relative subsequently begins a civil claim for damages. MUST REQUESTED WITNESSES ATTEND AN INQUEST? Yes. The polite invitation from the Coroner’s Court is really an
Order and the Coroner can subpoena personnel if necessary.
STATEMENTS Your statement should contain all or some of the following features:
State – what you know from your own knowledge and is substantiated by the notes.
What you remember but not supported by documentation.
What is normal practice at the time – perhaps
What you know from reading the records but you did not witness yourself.
The Trust’s solicitors will provide a detailed request letter for information and explain the key issues which will need to be covered. BEFORE THE INQUEST Almost invariably witnesses will be asked to submit a written statement before the Inquest through the Trust’s Solicitors based at the RD&E Hospital. After the drafted statement has been made, witnesses may need to meet with the Trust’s Solicitors to finalise the completed statement. Statements should contain a full but concise, factual account in chronological order of the doctor or nurse’s personal involvement in the case. The statement will need to be prepared with access to the contemporary clinical notes, although these should be available at the Inquest for reference. If staff are asked to attend the Inquest then the Trust’s solicitors will also attend to support and represent the member of staff. AT THE HEARING Witnesses will be told of the date, time and place of the Inquest through the Trust Solicitors and should ensure that they are punctual and appropriately dressed. The order in which witnesses are called is decided by the Coroner. Where important clinical commitments which cannot be changed, require a witness to be called out of sequence it may be possible to persuade a Coroner to accede to such a request, given sufficient notice. Each witness should take with them a copy of their statement. In cases where witnesses are attending the Trust Solicitor will meet with the individuals for advice, support, to go through statements and the procedure on the day. The degree of formality in Court depends largely on the Coroner, although each witness will begin by taking the oath or affirming and will then be asked questions by the Coroner. The Coroner, if she is the opinion that the evidence contained in a statement is unlikely to be controversial, will decide simply to read the statement and dispense with the need for the witness to attend. The proceedings in the Coroner’s Court are taped and it is important that the witnesses’ replies are audible and concise. It is important for a medical witness to have all the clinical facts at his fingertips: muddled thinking or speaking or the shuffling of papers always gives a bad impression. If it is necessary to refer to the original records, the witness should simply ask to
Management of Legal Claims Policy
Corporate Governance G:\Corporate Governance\Compliance Team\Policies Procedural Documents\Published Policy Database\Corporate Governance\claims policy\Legal Claims Policy V5.1 16Nov15.docx V2.0 10Jul15 Page 46 of 47
have an opportunity to do so before answering the question. When the Coroner has finished his examination of each witness the relatives or their Lawyer may ask relevant questions via the Coroner. Usually where a number of relatives have attended and there is no legal representation, one member will be appointed as spokesperson. A witness cannot be obliged to answer any questions which tend to incriminate him and should decline to do so. After the family have asked any questions the Trust is legally represented, the Trust’s representative will have an opportunity to ask further questions by way of re-examination. EVIDENCE FROM THE PATHOLOGIST Before the start of the Inquest, although the practice in each Coroner’s Court will differ, it is usually possible for the Trust’s Solicitors to obtain a copy of the Post Mortem report. POSSIBLE VERDICTS Typically when the evidence has been completed the Coroner will sum this up before giving her findings in the form of an inquisition. Her findings (with some notable exceptions) are made on the balance of probabilities. The Coroner’s Rules (1984) suggest a number of possible verdicts: e.g:
natural causes industrial disease dependence on drugs unlawful killing accident/misadventure
Where the evidence is inconclusive an open verdict will be recorded. No verdict shall be framed in such a way as to determine any question of civil liability and this is specifically precluded by the Coroner’s Rules. The Coroner does have power to make recommendations under the Rules, where she believes that action should be taken to prevent the recurrence of similar fatalities. A Neglect verdict means a gross failure to provide adequate nourishment or liquid, or provide or procure basic medical attention or shelter or warmth for someone in a dependent position (because of youth, age, illness or incarceration) who cannot provide it for himself. Failure to provide medical attention for a dependent person whose physical condition is such as to show that he obviously needs it may mount to neglect. PUBLICITY In most cases an Inquest will be held in public and the press may be present. If approached by a press officer, do not speak or comment on the Inquest after the hearing. Always
refer them to the Trust’s Communications team who is based at Trinity Suite, Level 5, NDDH. CONTACT AND SUPPORT Most Inquests are routine matters, though it should not be forgotten that they can be extremely worrying especially for junior doctors and nursing staff. Careful preparation is vital and will minimise difficulties on the day. The sources of support that will be beneficial to you personally are individual professional bodies and your Line Managers, the Trust Solicitors and/or Legal Claims Manager and reference to the Claims Handling and Support Staff Policies are available on “BOB”. Legal Claims Office Suite 1, Munro House Northern Devon Healthcare NHS Trust Barnstaple, Devon EX31 4JB Direct Line: 01271 31408 Email: [email protected] Trust Solicitor North & East Devon Legal Services Royal Devon & Exeter Hospital (Heavitree) Gladstone Road Exeter Direct Line: 01392 405286
PREPARING
FOR AN
INQUEST
CORPORATE GOVERNANCE
Sharron Bates Legal Claims Manager
June 2014 Produced S Bates

Management of Legal Claims Policy
Corporate Governance G:\Corporate Governance\Compliance Team\Policies Procedural Documents\Published Policy Database\Corporate Governance\claims policy\Legal Claims Policy V5.1 16Nov15.docx V2.0 10Jul15 Page 47 of 47
Appendix I - Standard Operating Procedure Managing Inquests