Embed Size (px)
Citation preview

J AY I . S A N D L O W, M D
VOL. 2, NO. 4, DECEMBER 2004 Sexuality, Reproduction & Menopause
The varicocele is an enigma in thefield of male infertility. Despitemore than 30 years of evidence thatrepair of varicoceles results in im-
proved fertility, controversy continues to sur-round the utility of treatment. This is com-pounded by the fact that not all varicocelescause infertility and thus not all varicoceles re-quire treatment. Varicoceles, in fact, are pres-ent in approximately 15% of the general malepopulation.
Most authors recommend treatment ofvaricoceles in the event of male factor infer-tility.1 Varicoceles, in fact, are the most com-monly diagnosed cause of male infertility, ac-counting for up to 40% of cases. On the otherhand, nearly two-thirds of men with varico-celes remain fertile. The reason for thisdiscrepancy remains unknown, although thecause of infertility is believed to be related toboth temperature and time. Varicoceles donot represent a general health risk, but theycan lead to deterioration of fertility over time.2
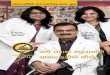
How varicoceles developVaricoceles are a dilation of the veins thatdrain the testis. These veins are found in thespermatic cord and are called the pampini-form plexus (Figure 1).
The main blood supply to the testis comesfrom the aorta. The internal spermatic (tes-ticular) artery is the major source, with collat-eral flow from the deferential artery, as well asthe cremasteric arteries. Venous drainage isvariable, with the pampiniform plexus drain-ing into the internal spermatic (testicular)veins. These veins insert into the renal vein onthe left and the inferior vena cava on the right.The veins surround the artery, thus providing
a mechanism for cooling the warm arterialblood via countercurrent heat exchange.3 Thisis one way that the intratesticular temperatureis maintained several degrees below bodytemperature. Disruption of this system can re-sult in hyperthermia of the testes.
Varicoceles typically develop after puber-ty, although many are not detected until thepatient is evaluated for fertility problems. Thedevelopment of varicoceles is controversial.Classically, it was thought that varicoceles de-veloped due to failure of the valves within theinternal spermatic vein(s). However, more re-cent studies have demonstrated intact valvesin men with clinical varicoceles, as well as ab-sent valves in men without varicoceles. Thus,it appears that the anatomy of the drainagesystem plays a major role in the developmentof varicoceles. Because the left side drains intoa system with higher resistance (the renalvein), small venules may persist or open dur-ing embyrogenesis. And because testicularblood flow remains low prior to puberty, theseveins do not become clinically apparent until
219
Do varicoceles really affect male fertility?Varicoceles account for up to 40% of male factor infertility, yet nearly two-thirds of men with varicoceles are fertile. What’s a clinician to do? Two things, really: Understand whatcauses varicoceles and appreciate the benefits of repair.
J AY I . S A N D L O W, M D
Jay I. Sandlow, MDDepartment of UrologyMedical College of WisconsinMilwaukee
✒ KEY POINTS
■ Although varicoceles are common, not all require treatment. Most authorsrecommend treatment of varicoceles in the event of male factor infertility.
■ Varicoceles are thought to cause spermatogenic defects by raising theintratesticular temperature in both the affected and contralateral testes.
■ Varicoceles may cause progressive, duration-dependent injury to theseminiferous epithelium. Repair is thought to halt this duration-dependentprocess.
■ The goals of varicocele repair are to relieve pain in symptomatic cases and to improve semen parameters, testicular function, and pregnancy ratesin couples with varicocele-associated male factor infertility.

Do varicoceles really affect male fertility?
Sexuality, Reproduction & Menopause VOL. 2, NO. 4, DECEMBER 2004
adolescence, when testicular blood flow in-creases, thus explaining the appearance ofmost varicoceles around puberty.4 Varicocelesare thought to cause spermatogenic defects byraising the intratesticular temperature in boththe affected and contralateral testes.
Endocrine dysfunction may also con-tribute to the effects of varicoceles on fertili-ty. Studies have demonstrated altered func-tion of Leydig, Sertoli, and germ cells in menwith significant varicoceles.5 Whether this is
due to increased intratesticular temperatureor other factors is unknown at present. Otherstudies have demonstrated subtle hormonalabnormalities, most notably an exaggeratedresponse to gonadotropin-releasing hormone(GnRH). The clinical utility of this informa-tion, however, is debatable. Repair of varico-cele may halt any further damage to testicularhormone function and, in a large percentageof men, result in improved spermatogenesisas well as enhanced Leydig cell function.
Making the diagnosisVaricoceles are typically diagnosed by physi-cal examination. They are most easily detect-ed when the patient has been standing in awarm room for several minutes. Often, theywill expand when the patient bears down (Val-salva maneuver), as the blood reverses flowback toward the testicle.
Most experts agree that only varicoceles
detected by physical examination are clinicallysignificant. Therefore, confirmatory testing is usually not necessary except under certaincircumstances.
Ultrasound can identify varicoceles assmall as 2–3 mm in diameter. However, ultra-sound will also identify “subclinical” varico-celes—those that are not clinically palpable.Because the original studies examining the ef-fects of varicocele ligation on seminal param-eters did not find a significant correlation be-tween size of the varicocele and response,some believe that correcting subclinical vari-coceles would lead to the same rate of im-provement as the correction of clinical vari-coceles. However, most studies report a lowerresponse rate following repair of subclinicalvaricoceles, and even lower pregnancy rates.6
Doppler studies are easily performed inthe office and identify the reversal of bloodflow during Valsalva maneuver. Doppler mayalso detect a subclinical varicocele, althoughit is also useful in examining men with tightscrotal skin or short spermatic cords, and inexploring the right side when the patient hasa palpable left varicocele.
Varicoceles are usually associated with ab-normalities in all of the seminal parameters.However, they can also cause isolated defectsin sperm count, motility, morphology, or func-tion. Therefore, the results of semen analysisare not a good predictor of the presence or ab-sence of a varicocele.
Goals of varicocele repairThe objectives of varicocele repair are to:• relieve pain in symptomatic cases;• improve semen parameters;• enhance testicular function; and• improve pregnancy rates in couples with
male factor infertility associated with varico-cele.
Studies have shown that varicocele repaircan result in a significant improvement insemen parameters in 60% to 70% of men.7
Men with large varicoceles tend to have poor-er preoperative semen quality than men withsmall varicoceles, but repair of large varico-celes results in greater improvement than repair of small ones.
Varicoceles are identified in 35% to 40%of men with primary infertility and 81% ofmen with secondary infertility.8 Studies haveshown that varicoceles cause progressive du-ration-dependent injury to the seminiferous
220
Bladder
External inguinal ring
Ductus deferens
Testicular arteryPampiniform plexusof testicular veins
Figure 1. How varico-celes develop. The majorsource of blood supply tothe testis is the testicularartery. Varcicoceles occurwhen the veins that drainthe testis, known as thepampiniform plexus, becomedilated. Small venules maypersist or open during embryogenesis but may notbecome clinically apparentuntil puberty, when testi-cular blood flow increases.
Testis Epididymis
Prostate
Internal pudendal artery
Internal pudendal vein
© KEVIN SOMERVILLE 2004

Do varicoceles really affect male fertility?
VOL. 2, NO. 4, DECEMBER 2004 Sexuality, Reproduction & Menopause
epithelium. Repair is thought to halt this du-ration-dependent process. The goal: A signi-ficant percentage of couples will go on toachieve pregnancy without assisted tech-niques, and those who do proceed to assistedreproductive technology will have optimizedthe sperm quality.
Methods of varicocele repair Treatment modalities for varicocele vary fromradiologic ablation to surgical ligation. Stud-ies have examined a variety of methods, at-tempting to demonstrate a difference in effi-cacy and outcomes. Although most methodsyield similar short-term results, open micro-surgery tends to have lower long-term com-plications, such as recurrences and hydro-celes. This is due to the ability to tie off allveins while sparing the arterial blood supplyand lymphatic vessels.
It also seems that the higher the ligation(e.g., in the retroperitoneum) the higher thepersistence/recurrence rate. Such complica-tions most likely occur because small venouschannels branch off or cross over from the testicular veins below the level of ligation. As a result, most experts in male infertilityprefer a low inguinal/subinguinal approach.Although laparoscopic varicocele ligation wasonce touted as a minimally invasive method ofrepair, several authors have demonstratedsimilar recovery rates with open microsurgi-cal methods9 along with equal efficacy, fewercomplications, and the advantage of not hav-ing to enter the abdomen.
Most men prefer general anesthesia,though the procedure may be performedunder local with intravenous sedation. Timeto recovery varies, but most men get back towork within 3–4 days and resume full activitywithin 7–10 days.
The most common complications fromvaricocelectomy are hydrocele, varicocele re-currence, and testicular artery injury. Use ofthe operating microscope allows for reliableidentification of spermatic cord lymphatics,internal spermatic veins and venous collater-als, and the testicular artery or arteries, so thatthe incidence of these complications can bereduced significantly. Thus, in a significantnumber of men, the microsurgical techniqueprovides a safe and effective approach tovaricocele repair that preserves testicularfunction, enhances semen quality, and im-proves partners’ pregnancy rates.
What the evidence showsAlthough there is a paucity of randomizedcontrolled trials determining the benefit oftreating varicocele-related infertility, manynon-randomized studies support this notion.10
Most of those studies are retrospective andsomewhat biased in their patient selection.Nevertheless, there is both direct and indirectevidence that varicocele repair improves seminal parameters in up to 60%–70% ofcases, with natural pregnancy rates up to 50%.However, a Cochrane review of several randomized controlled trials did not show sufficient evidence regarding the treatment of varicoceles to warrant their repair.11 Al-though some of the trials in this review suffered from significant problems in method-ology, the review once again raises the ques-tion of whether treating varicoceles improvesfertility.
Despite the lack of large randomized tri-als, the majority of available evidence favorsthe surgical treatment of clinical varicocelesin men with infertility. Current research, bothbasic and clinical, seeks to further character-ize this common, yet poorly understood, con-dition. Until more definitive results are re-ported, varicoceles will continue to stimulatecontroversy among reproductive experts. ■■
REFERENCES1. Dubin L, Amelar RD. Varicocele size and results of varicocelectomyin selected subfertile men with varicocele. Fertil Steril 1970;21:606-09.2. Chehval MJ, Purcell MH. Deterioration of semen parameters overtime in men with untreated varicocele: evidence of progressive testicu-lar damage. Fertil Steril 1992;57:174-77.3. Dahl EV, Herrick JF. A vascular mechanism for maintaining testic-ular temperature by counter-current exchange. Surg Gynecol Obstet1959;108:697-705.4. Braedel HU, Steffens J, Ziegler M, et al. A possible ontogenic etiol-ogy for idiopathic left varicocele. J Urol 1994;151:62-66.5. Fretz PC, Sandlow JI. Varicocele: current concepts in pathophysiol-ogy, diagnosis, and treatment. Urol Clin North Am 2002;29:921-37.6. Jarow JP, Ogle SR, Eskew LA. Seminal improvement following repairof ultrasound detected subclinical varicoceles. J Urol 1996;155:1287-90.7. Nagler HM, Luntz RK, Martinis FG. Varicocele. In Infertility in theMale, ed 3. Lipshultz LI, Howards SS, eds. St. Louis, Mosby Press, Ch.18, p 337, 1997.8. Gorelick JI, Goldstein M. Loss of fertility in men with varicocele. Fer-til Steril 1993;59:613-16.9. Enquist E, Stein BS, Sigman M. Laparoscopic versus subinguinalvaricocelectomy: a comparative study. Fertil Steril 1994;61:1092-96.10. Schlesinger MH, Wilets IF, Nagler HM. Treatment outcome aftervaricocelectomy. A critical analysis. Urol Clin North Am 1994;21:517-29.11. Evers JLH, Collins JA, Vandekerckhove P. Surgery or embolisationfor varicocele in subfertile men (Cochrane Review). In: The CochraneLibrary, Issue 1, 2003. Oxford: Update Software.
221
T here is evidence that varicocele repair improvesseminal parameters in up to 60%–70% of
cases, with natural pregnancy rates up to 50%.
Jay I. Sandlow, MDAssociate Professor and
Vice-ChairmanDepartment of UrologyMedical College of WisconsinMilwaukee, [email protected]