Embed Size (px)
Citation preview

HEALTH ECONOMICSHealth Econ. 19: 716–729 (2010)Published online 18 June 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hec.1509
DO REGIONAL PRIMARY-CARE ORGANISATIONSINFLUENCE PRIMARY-CARE PERFORMANCE? A DYNAMIC
PANEL ESTIMATION
ANTHONY SCOTTa,� and WILLIAM COOTEb
aMelbourne Institute of Applied Economic and Social Research, The University of Melbourne, AustraliabCoote Practice Pty. Ltd, Canberra, Australia
SUMMARY
The role of regional primary-care organizations (PCOs) in health-care systems is not well understood. This is the firststudy to attempt to isolate the effect of regional PCOs on primary-care performance. We examine Divisions of GeneralPractice in Australia, which were established in 1992. A unique Division-level panel data set is used to examine theeffect of Divisions, and their activities, on various aspects of primary-care performance. Dynamic panel estimation isused to account for state dependence and the endogeneity of Divisions’ activities. The results show that Divisions weremore likely to have influenced general practice infrastructure than clinical performance in diabetes, asthma and cervicalscreening. The effect of specific Division activities, such as providing support for practice nurses and IT support, wasnot directly related to changes in the level of general practice performance. Specific support in the areas of diabetes andasthma was associated with general practice performance, but this was due to reverse causality and the effect ofunobservable factors, rather than the direct effect of Divisions. Copyright r 2009 John Wiley & Sons, Ltd.
Received 31 January 2008; Revised 19 April 2009; Accepted 29 April 2009
KEY WORDS: primary care; dynamic panel estimation; performance; organization of healthcare
1. INTRODUCTION
A strong primary health-care system is regarded as a major part of any modern efficient and equitablehealth-care system (Starfield and Macinko, 2005). A number of countries have developed regionalprimary-care organizations PCOs, including Primary Care Trusts in the UK, Primary HealthOrganisations in the New Zealand and Divisions of General Practice in Australia (Smith and Mays,2007). PCOs have been defined as: ‘bodies that seek to increase the influence of primary careprofessionals, and in particular general practitioners (GPs), in health planning and resource allocation,and in the health system more generally’ (Smith and Goodwin, 2006).1 These organisations began as aform of network where GPs can choose to become involved and are the main influence on the nature,objectives and operation of the PCO. PCOs vary in how they have evolved, their roles, function, theextent to which they are horizontally or vertically integrated, and in the completeness and nature ofthe contracts between the PCO, government, secondary care and the providers and population within it.The relative efficiency of these different institutional structures, and their impact on the costs and qualityof primary-care services and the broader health-care system, remains an important policy question inhealth care. This paper fills an important gap in the literature by examining the effect of regional PCOs onperformance in primary care using a unique panel dataset on Divisions of General Practice in Australia.
*Correspondence to: Melbourne Institute of Applied Economic and Social Research, The University of Melbourne, Australia.E-mail: [email protected]
1Regional PCOs have a regional and population health focus and so are distinct from HMOs and managed care organisations.
Copyright r 2009 John Wiley & Sons, Ltd.

2. INSTITUTIONAL BACKGROUND
The Australian health-care system is dominated by the national universal insurance scheme, Medicare,which is funded through general taxation and is split into a number of separate funding streams.Medical services, including GPs services, are directly funded by the federal government throughuncapped fee-for-service, whilst public hospitals are managed by state governments who providearound half of their funding with the other half from the federal government. There is also a largeprivate health sector, supported in part through the public subsidy of private health insurancepremiums, with almost half of the population holding private health insurance.
In addition to the Medicare system of fee-for-service re-imbursement in Australia, blended paymentsfor GPs were introduced in 1999 through the Practice Incentive Program (PIP) (Scott et al., 2008).Accredited practices can join the programme and claim capitation payments for practice infrastructure,and are eligible to claim service incentive payments (SIPs) in the areas of asthma, diabetes, mentalhealth and cervical screening. These are additional fees for the completion of defined annual cycles ofcare in these disease areas based on clinical guidelines.
Divisions of General Practice were established in 1992 and emerged from local coalitions of GPswhich responded to funding from the federal government for demonstration sites to undertake specificlocal projects. Division boundaries emerged over 7 years between 1991 and 1998, by which time therewere 123 Divisions across Australia. Although the emergence of Divisions was determined by smallgroups of interested GPs and so are potentially endogenous in our analysis, the vast majority of GPshad little to do with their formation and it took some time for membership to increase. The federalgovernment provides around half of their funding through a contract with each Division, with theremainder of funding coming from state governments, specific federal government programmes andother sources. In 2006, there were 120 geographically based Divisions covering all of Australia.
Participation in Division activity by individual doctors is voluntary and in 2004/5 Divisions reporteda membership of 94.2% of all GPs in Australia (Hordacre, 2006). GPs can join more than one Division.Divisions had a median of 152 GPs (ranging from 15 to 747) practising within their boundaries and amedian of 53 general practices (ranging from 7 to 215) in 2004/5. The population covered by an averageDivision is 167 000 and ranges from 16 993 to 608 451 in 2004/5.
The activities in which Divisions have been involved are diverse. Divisions have evolved with littlecentral direction, leading to much variation in their scope and function within Australia. They have hadsubstantial discretion in defining their roles and the type of activities they undertake. In simple terms,the outputs of Divisions can be defined as the provision of advice, information (through training) andthe provision of ‘in-kind’ resources and assistance to GPs, such as supporting accreditation, the ITcapability of practices and the employment of practice nurses. Division inputs include their board andemployed staff who directly interact with GPs (an average of 10.6 FTE mainly non-GP staff perDivision, ranging from 1 to 46 FTEs (Hordacre et al., 2006)). Division outputs are then used as inputsin GPs’ production functions that help to lower the costs of GPs for undertaking certain activities.In addition, advice and information delivered by Divisions through educational activities are assumedto change GPs’ perceptions of the benefits of such activities to themselves and to patients, which in turninfluences GPs‘ behaviour and their performance.
3. METHODS
The objective is to examine the effect of Divisions on the performance of GPs and general practices.There are a number of econometric issues to be examined given the type of model and data. Since we donot have data on primary-care activity before and after the introduction of Divisions, it is not possibleto directly compare primary-care activity with and without Divisions or to construct a counterfactual.In the absence of being able to estimate a direct ‘treatment effect’ of Divisions, two types of model are
REGIONAL PRIMARY-CARE ORGANISATIONS INFLUENCE 717
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

therefore estimated. The first is to estimate the overall Division fixed effects. A basic panel data modelcan be used:
yit ¼aþ xitbþ eit
eit ¼ui þ vitð1Þ
where yit is the average level of performance of GP practices in Division i in time t, a is the average levelof performance, xit is a set of observable exogenous factors, vit is the usual IID error term, ui is aDivision-specific error term capturing unobserved Division-level influences on performance, b, areparameters to be estimated.
The Division effect ui contains a number of factors associated with general practice outputs that wedo not observe or measure directly but are specific to Divisions and their local areas and are timeinvariant. As well as the existence and activities of Divisions, other factors influencing performanceinclude rurality, population characteristics and other unobserved factors influencing performance (e.g.GPs selection into geographical areas). The direct effect of the existence and activities of Divisions (e.g.network effects, managerial style and culture) may have changed over time as the Divisions wereestablished, but are likely to be mostly time invariant in short time period we observe and whereDivisions have already been established for up to 8 years. To the extent that unobserved factors changeover time, we include quarterly time dummy variables.
If (1) is estimated using fixed effects, then the fixed effects could not be used as a measure of the effectof Divisions on general practice performance. Time-invariant variables that we can measure, such asrurality and population health needs, would drop out of the model and be subsumed into the fixed effect.However, Mundlak (1978) suggested an approach that allows these measurable area characteristics to beincluded as independent variables, whilst allowing for correlation between ui and x. This involvesincluding the time-averaged values all of the time-varying independent variables as independentvariables, and then estimating the model using random effects. Random effects estimation allows theinclusion of the time-invariant geographical area characteristics as independent variables, thus removingthem from the random effect. The random effect can then be interpreted as the overall effect ofDivisions. The proportion of the variance in yit explained by ui is, therefore, a measure of the effect ofDivisions, subject to the ability of the model to control for all other factors affecting general practiceperformance.
The second type of model estimated focuses on the influence of specific Division outputs onvariations in general practice performance, while controlling the population and practice characteristics.The model to be estimated is
yit ¼aþ xitbþ zitdþ qityþ eit
eit ¼ui þ vitð2Þ
Our central focus is the effect of Division outputs, qit, on general practice performance, yit. Divisionoutputs are likely to be endogenous. If zit represent unobserved variables that influence yit andcorr(qit, zit)6¼0, then qit will also be correlated with vit leading to a biased estimate of qit. The correlationbetween qit and vit may be the result of reverse causality and/or unobserved zit. The influence ofa Division’s GP members in one period can influence what activities Divisions undertake in thefollowing period. Instrumental variable approaches are, therefore, needed and this is possible byexploiting the dynamic properties of the data.
In addition to the endogeneity of Division outputs, general practice performance in the currentperiod is also likely be influenced by their past values. This suggests a dynamic specification andlong-term adjustment process for yit, such that
yit ¼ ayi;t�1 þ xitbþ qityþ ui þ vit ð3Þ
A. SCOTT AND W. COOTE718
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

Fixed effects estimation of (3) results in dynamic panel bias as yi;t�1 is endogenous to the fixed effectsbecause yi;t�1 is part of the fixed effect under the within groups transformation. The usual procedure inthis case is to apply a different transformation to remove the fixed effects, either by taking firstdifferences or forward orthogonal deviations2. This does not in itself remove the endogeneity of yi;t�1,but importantly allows the use of lags of yi;t�1 as valid instruments (Arellano and Bond, 1991; Arellanoand Bover, 1995; Baltagi, 2005). For example, if first differences are taken, then (3) becomes
Dyit ¼ aDyi;t�1 þ Dxitbþ Dqityþ Dvit; t ¼ 2; . . . ;T ð4Þ
Using lags as instruments for D yi;t�1, it becomes apparent that yi;t�2 are correlated with Dyi;t�1 ¼ yi;t�1 � yi;t�2, but not with the error term Dvit ¼ vit � vi;t�1, assuming vit are not seriallycorrelated. This latter assumption can be tested using an autocorrelation test developed by Arellano andBond for order �l serial correlation (Roodman, 2006). The same is true for deeper lags yi;t�s, wheresZ2. As the number of time periods increase, so do the number of valid instruments that can be used,although so does the risk of over-identification. Lags of qi;t�1 can also be used as instruments for q in asimilar way in addition to other instruments for q, such as Division inputs.
Equation (4) can, therefore, be estimated using the Arellano–Bond estimator based on GMM(‘difference’ GMM). Blundell and Bond (1998) suggested a more efficient estimator (‘system’ GMM)that combines the above first differences model with a model estimated in levels that uses laggeddifferences as instruments. It, therefore, combines instruments that capture the effect of lagged levels ofyit on growth in yit (the difference estimator) with the effect of lagged growth in yit on the level of yi;t�1(the levels estimator). System GMM is likely to perform better when a is large but less than 1, i.e. whenthere is persistence in yi;t�s, which is likely to be the case in our data. The validity of the additionalinstruments can be tested using the Sargan test, although this becomes unreliable as the number ofinstruments increases (Roodman, 2006).
4. DATA
A Division-level panel data set was constructed from a number of different sources. Data on theperformance of general practices in a Division area were taken from quarterly administrative fee claimsdata that were publicly available on the Medicare Australia web site. Four dependent variables and fourbasic models were estimated, including practice infrastructure defined as the percentage of generalpractices in the Division who were participating in the PIP and primary-care performance in diabetes,asthma and cervical screening. For each disease area, the variable used is the total value of SIPs in theDivision, divided by the total number of practices in the Division.
Independent variables include data on Division inputs and outputs from the Annual Survey ofDivisions between 1995/6 and 2004/5 (Table I). There is a 100% response rate to these self-reportsurveys and missing or inconsistent data are followed up by telephone. Common questions from eachsurvey were identified and linked over time.
General practice performance is also influenced by the characteristics of GPs and general practices,including inputs, the organisational capacity of general practices and the practice style of GPs (Beilbyet al., 2003; Productivity Commission, 2003; Proudfoot et al., 2004; Bensing et al., 1993; Charles et al.,2006; Choudhry et al., 2005). GP and practice characteristics measured at Division level are shown inTable I. In addition to remoteness and rurality, population need for health care is captured by ameasure of socio-economic disadvantage, mortality rates and the percentage of elderly and indigenousAustralians in each Division. A set of quarterly time dummies was also included to control for anytrends or seasonal effects in the data.
2The latter is more suitable where there are gaps in panels.
REGIONAL PRIMARY-CARE ORGANISATIONS INFLUENCE 719
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

5. RESULTS
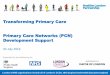
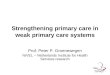
Figures 1 and 2 show trends in the four dependent variables. The sharp drop in the proportion of PIPpractices of almost 10 percentage points at the end of 2001 was due to the introduction of a formalaccreditation requirement to be eligible for the programme in 2002. Since 2004, around two-thirds ofgeneral practices in Australia are registered for the programme. In 2004, this varied between 18 and100% across Divisions. Figure 2 shows the growth in incentive payments for diabetes, asthma andcervical screening since they were first introduced. The value of diabetes and cervical screeningpayments grew over the period, whilst the value of asthma payments claims fell because of problems inbeing able to claim the incentives (Zwar et al., 2005). There was also substantial variation betweenDivisions at a given point in time. For example, in 2004 the average value of diabetes incentivepayments was very close to zero in some Divisions and as high as $698 per PIP practice per quarter inothers. Descriptive statistics of the independent variables used are shown in Table I. These aresummarised between the calendar years 2002 and 2004 to give an idea of variation over time.
The results of the first set of models (regression results are shown in the Appendix) estimate theproportion of the variation in general practice outputs that can be explained by Divisions (the Division
Table I. Descriptive statistics for independent variables (Division-level)
2002 2003 2004 2002–2004 sd min max
Area characteristicsProportion of Divisions inRemote areas 0.09 0.09 0.09 0.09 0.28 0 1Outer regional areas 0.20 0.20 0.20 0.20 0.40 0 1Inner regional areas 0.27 0.27 0.27 0.27 0.44 0 1Major cities 0.45 0.45 0.45 0.45 0.50 0 1Index of relative socio-economic disadvantagea 992.82 992.82 992.82 992.82 47.53 857 1129All cause mortality rate per 100 000 (o75 years old)b 301.18 301.18 301.18 301.18 50.64 198.08 580.6Indigenous population (5 1 if 410%) 0.09 0.10 0.10 0.10 0.30 0 1Proportion of population 465 years old 0.12 0.13 0.13 0.13 0.03 0.02 0.23GP characteristicsPatients per GPc 1031.63 1018.76 1008.9 1019.76 143.07 646.85 1637.6GPs per practiced 2.3 2.34 2.34 2.33 0.72 0.59 6.82Proportion of part time GPs 0.42 0.42 0.41 0.42 0.12 0.12 0.8Proportion of female GPs 0.31 0.32 0.32 0.32 0.1 0.05 0.71Proportion of GPs aged 455 years old 0.25 0.26 0.27 0.26 0.08 0.04 0.48Division inputsNumber of Division board members 8.78 8.6 8.49 8.62 2.15 3 18Number of Division staff (FTE) 10 10.41 10.51 10.3 5.96 1 52.28Proportion of Divisions with a governance manual 0.86 0.89 0.90 0.88 0.32 0 1Division outputsProportion of Divisions providingActivities with an Asthma focus (yes5 1)e 0.82 0.93 0.87 0.87 0.33 0 1Activities with a diabetes focus (yes5 1)e 0.97 0.98 0.97 0.98 0.16 0 1Activities with a cervical screening focus (yes5 1)e 0.68 0.76 0.7 0.71 0.45 0 1Practice nurse support (yes5 1) 0.74 0.80 0.82 0.78 0.41 0 1IT support (yes5 1)f 0.40 0.37 0.32 0.36 0.48 0 1
aThis is a continuous measure aggregated to Division level and is based on the 2001 census derived from attributes such as income,educational attainment, unemployment, and dwellings without motor vehicles. It focuses on low income earners, relatively lowereducational attainment and high unemployment (ABS, 2004). The value of this variable does not change over time.
bAverage between 2000 to 2002 based on ABS data and aggregated to Division level. The value of this variable does not changeover time.
cThe total Standardised Weighted Patient Equivalents (SWPEs) per Division was divided by the number of full-time workloadequivalent (FWE) GPs in each Division.dThe number of FWE GPs in a Division divided by the number of general practices in a Division.eIncludes GP education, practice support, community awareness, patient services or recall systems.fElectronic communication between GPs and others, electronic data transfer, and support in establishing age-sex registers and/orrecall systems. Further information of all variables are available in Scott and Coote (2007).
A. SCOTT AND W. COOTE720
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

random effect) for each type of general practice output. Division random effects were statisticallysignificant suggesting that the Divisions influenced practice infrastructure and performance. Divisionsexplained 45% of the variation for practice infrastructure (the proportion of PIP practices in aDivision), followed by 19% for asthma, 12% for diabetes and 11% for cervical screening.
These results tell us little, however, about what exactly Divisions did that influenced general practiceperformance. The random effects capture factors that were constant within Divisions over the timeperiod. Tables II–IV show the results from the analysis that included specific Division outputs asexplanatory variables, in addition to accounting for the dynamic nature of Division and general practiceactivities.
For each dependent variable, results are shown comparing OLS, fixed effects, system GMM withoutinstrumenting for q (but instrumenting for yit�1), and system GMM instrumenting for q. In systemGMM, all models used orthogonal deviations rather than first differences to control for fixed effects.This helps maximise sample size given the existence of an unbalanced panel.
An important issue in system GMM is that the number of instruments is quadratic in the number oftime periods. Too many instruments can result in over-identification and unreliability of the Sargan test.
1
51
101
151
201
251
301
351
401
451
Nov-0
1
Mar
-02
Jul-0
2
Nov-0
2
Mar
-03
Jul-0
3
Nov-0
3
Mar
-04
Jul-0
4
Nov-0
4
Mar
-05
Jul-0
5
Nov-0
5
$ B
enef
it p
er P
IP p
ract
ice
Asthma SIP
Diabetes SIP
Cervical SIP
Figure 2. Growth in Service Incentive Payments for Diabetes, Asthma, and Cervical screening
54%
56%
58%
60%
62%
64%
66%
68%
70%
72%
Aug
-00
Nov
-00
Feb
-01
May
-01
Aug
-01
Nov
-01
Feb
-02
May
-02
Aug
-02
Nov
-02
Feb
-03
May
-03
Aug
-03
Nov
-03
Feb
-04
May
-04
Aug
-04
Nov
-04
Feb
-05
May
-05
% o
f P
IP p
ract
ices
Figure 1. Proportion of practices in the Practice Incentive Program, 2000–2005
REGIONAL PRIMARY-CARE ORGANISATIONS INFLUENCE 721
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

Our data have up to 15 quarters depending on the model, potentially resulting in hundreds ofinstruments, many more than the number of Divisions per time period (around 120). The number ofinstruments was kept to a relatively low number in each model by collapsing the instrument matrix(Roodman, 2006) and limiting the number of lags that could be used as instruments. For yit�1, thepreceding four quarters were used as instruments to capture any seasonal effects. For Divisionoutputs q, the observation in the previous year (i.e. one instrument) was used, since the data for q wereannual (i.e. were repeated across quarters in the data set) and would, therefore, exhibit no variationwithin a given year. In addition, instruments for q also included Division inputs: the number of boardmembers, the number of FTE staff, the proportion of GPs on the board and whether the Division hada manual of operating procedures. These were all expected to be correlated with Division outputs, butnot general practice performance. The figures on the number of instruments in the table, therefore, referto the number of instruments over and above the exogenous variables already in the model. Includingmore or fewer instruments did not influence the results greatly.
The effect of specific Division activities on the proportion of PIP practices is shown in Table II.System GMM showed strong evidence of state dependence. The proportion of participating practices inquarter t is heavily influenced by the proportion in the previous quarter. This partially reflects that oncea practice becomes a PIP practice, it is highly likely to remain a PIP practice. In the two system GMMmodels, using the last four quarters (yit�2 to yit�5) as instruments for yit�l showed strong evidence ofover-identification with a statistically significant Hansen/Sargan test and difference in Sargan test forthe excluded instruments. This result remained after reducing the number of quarters used asinstruments. We then used deeper lags and found that yit�5 to yit�8 were a valid set of instruments.
Table II. The effect of Division activities on the proportion of practices in the Practice Incentive Program
Variable OLS Fixed effectsSystem GMM
(without instruments for q)System GMM
(with instruments for q)
Constant �0.0054 �0.2114�� �0.0172 0.0005yit�1 0.9279��� 0.6470��� 0.9521��� 0.9684���
Area characteristicsRemote area 0.0161�� — 0.014 0.0103Outer regional area 0.0099�� — 0.0092 0.0076Inner regional area 0.0051� — 0.0042 0.0043IRSD 1.45E�05 — 1.77E�05 9.35E�06Mortality rate �1.20E-05 — �7.24E�06 2.30E�05GP characteristicsPatients per GP �0.001 0.0265�� �0.0048 �0.0064Patients per GP squared 0.0001 �0.001 0.0002 0.0003GPs per practice 0.0299��� 0.1558��� 0.0297� 0.0283��
Practice size squared �0.0039��� �0.0158��� �0.0037� �0.0036��
Part time GPs 0.0018 �0.0195 0.0085 0.0103Female GPs �0.0096 �0.0354� �0.0051 �0.0022GPs aged 455 years old �0.0118 0.0889�� 0.0034 0.0052Division outputsIT support 0.0008 0.0009 0.0002 �0.004Practice nurse support 0.0065�� 0.003 0.0046� �0.0015Sample size 2168 2168 2168 2168Divisions 119 119 119Instruments 38 44Over-identifying restrictions 4 10Mean number of quarters 18.22 18.22 18.22Hansen/Sargan test w2(df ) 2.12 (4) 10.68 (10)AR1 test �5.97��� �6.32���
AR2 test �1.14 �1.15F-statistic (df ) 900 (33)��� 182 (146)��� 939 (33)��� 978 (33)���
Notes: po0.1; ��po0.05; ���po0.0001. Models also include quarterly dummies (not shown). Based on data from the quarterbegining 1st November 2000 to 1st May 2005.
A. SCOTT AND W. COOTE722
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

Specific Division activities included were the provision of IT support and support for practice nurses.IT support is not statistically significant in any of the models. Practice nurse support is significant in theOLS model, and weakly significant in the first system GMM model. However, it is not significant in thefinal model.
Other variables in the final model are of the expected signs. As the number of GPs per practiceincreases, so does the proportion of PIP practices in a Division up to around four GPs per practice, afterwhich the proportion of PIP practices starts to fall. This suggests that a key influence on the proportion ofPIP practices in a Division is the size of general practices. No other variables are statistically significant.
The effect of Division activities on diabetes SIP payments is shown in Table III. In the system GMMmodels, the use of lags as instruments relies on the assumption of no first-order serial correlation in theerror term, vit. However, there was strong evidence of second, third and fourth-order autocorrelationbetween the errors, and the model failed the Hansen test providing evidence that the instruments werenot valid. The use of deeper lags was, therefore, investigated (starting from lags of yit�5 to yit�8). Lags ofyit�6 to yit�9 were found to be valid instruments for yit�1 in both system GMM models. The modelsshowed strong evidence of persistence, in that the current period’s level of diabetes SIP claims wasdependent on the previous period.
In terms of specific Division activities, the first system GMM model shows a strong associationbetween Division activities in diabetes and diabetes SIP claims. However, this disappears onceunobserved factors and reverse causality are accounted for in the final model. The effect of practicenurse support on diabetes SIP claims is statistically significant, but negative and, therefore,
Table III. The effect of Division activities on the value of diabetes service incentive paymentsper particpating practice
Variable OLS Fixed effectsSystem GMM
(without instruments for q)System GMM
(with instruments for q)
Constant 1.4409��� 5.4439��� 2.3403�� 1.5222��
yit�1 0.6447��� 0.2264��� 0.5629��� 0.7445���
Area characteristicsRemote area �0.1838�� — �0.2336�� �0.1159�
Outer regional area �0.0696�� — �0.1093� �0.0539Inner regional area �0.0174 — �0.0282 �0.0146IRSD �0.0007�� — �0.0008� �0.0004Mortality rate 0.0004� — 0.0004 0.0002GP characteristicsPatients per GP 0.0856� �0.1005 0.1152� 0.0599Patients per GP squared �0.003 0.0017 �0.0043 �0.0017GPs per practice 0.2498��� �0.0625 0.2791�� 0.2065��
Practice size squared �0.0338��� 0.0125 �0.0385�� �0.0295��
Part time GPs �0.2144� 0.0542 �0.2551 �0.1949Female GPs 0.0066 0.1891 0.0062 �0.0266GPs aged 455 years old �0.0946 �0.2763 �0.2072 �0.1871Division outputsDiabetes activities 0.075 0.0321 0.0620�� �0.0363Practice nurse support 0.0114 �0.0195 0.0074 �0.0792��
Sample size 1552 1552 1552 1552Divisions 117 117 117Instruments 33 39Over-identifying restrictions 4 10Mean number of quarters 13.26 13.26 13.26Hansen/Sargan test w2(df) 3.49 (4) 8.96 (10)AR1 test �4.33��� �5.1���
AR2 test �1.43 �1.05F-statistic (df ) 123.11 (28)��� 50.35 (139)��� 97.02 (28)��� 209.19 (28)���
Notes: po0.1; ��po0.05; ���po0.0001. Models also include quarterly dummies (not shown). Based on data from the quarterbeginning 1st February 2002 to 1st May 2005.
REGIONAL PRIMARY-CARE ORGANISATIONS INFLUENCE 723
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

counterintuitive. Divisions providing practice nurse support had a lower level of diabetes SIP claims.This may be because practice nurses were focusing on other clinical areas that were substitutes fordiabetes SIP activity as the variable was based on a question that was not specific to diabetes.
Divisions in remote areas had a lower level of SIP claims compared with those in major cities. Thenumber of GPs per practice was also strongly related to diabetes SIP claims, with the effect peaking atfour GPs per practice and falling thereafter.
Cervical screening SIP payments were also assumed to be influenced by Division activities(Table IV). As with the other models, there was strong evidence of persistence in the dynamic models.The use of lags as instruments relies on the assumption of no first-order serial correlation amongst thevit. In a model using the four most recent quarters as instruments for yit�1, the test for autocorrelationshowed some second-order serial correlation between the errors, meaning that some of the instrumentswould not be valid. Deeper four-quarter lags were then explored, beginning with lags yit�4 to yit�7. Thisprovided evidence of over-identification and so the number of instruments was reduced with yit�7dropped from the instrument set, resulting in a valid set of instruments and an insignificant Hansen/Sargan test.
There were no statistically significant effects of either Division activities in cervical screening orpractice nurse support, once unobserved factors had been accounted for. Few other variables werestatistically significant. Outer regional areas had a lower level of SIP claims, as did Divisions with a high
Table IV. The effect of Division activities on the value of cervical screening service incentive paymentsper participating practice.
Variable OLS Fixed effectsSystem GMM
(without instruments for q)System GMM
(with instruments for q)
Constant 1.2470�� 3.8660��� 2.2792 2.0971�
yit�1 0.6371��� 0.2159��� 0.4611� 0.4939��
Area characteristicsRemote area �0.1793�� — �0.1993 �0.1658Outer regional area �0.1519��� — �0.1763 �0.1741�
Inner regional area �0.0439� — �0.0549 �0.046IRSD 0.0005� — 0.0005 0.0007Mortality rate 0.0003 — 0.0002 0.0003GP characteristicsPatients per GP �0.0685 �0.1221 �0.0777 �0.0921Patients per GP squared 0.0028 0.0049 0.0031 0.0038GPs per practice 0.1237�� �0.1 0.1627 0.1493Practice size squared �0.0081 0.0321�� �0.0094 �0.0089Part time GPs �0.2561�� 0.4397 �0.4337 �0.4387��
Female GPs 0.2952�� 0.0915 0.4406 0.4061GPs aged 455 years old 0.3168�� 0.9091�� 0.5389 0.5413Division outputsCervical screening activities 0.0195 0.0237 0.0265 �0.019Practice nurse support 0.032 0.0722�� 0.036 0.0195
Sample size 1467 1467 1467 1467Divisions 117 117 117Instruments 32 38Over-identifying restrictions 3 9Mean number of quarters 12.54 12.54 12.54Hansen/Sargan test w2(df ) 3.07 (3) 6.91(9)AR1 test �2.56�� �3.16���
AR2 test 1.12 1.48F-statistic (df ) 125.97 (28)��� 19.07 (139)��� 32.02 (28)��� 40.54 (28)���
Notes: po.1; ��po.05; ���po.0001. Models also include quarterly dummies (not shown). Based on data from the quarterbeginning 1st February 2002 to 1st May 2005.
A. SCOTT AND W. COOTE724
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

proportion of part time GPs. Unlike the other models, the number of GPs per practice did not influencethe level or growth of SIP claims for cervical screening.
The effect of Division outputs on asthma SIP claims per PIP practice is shown in Table V. Inaddition to a high level of persistence, Division activities with a focus on asthma were associated with ahigher level of asthma SIP claims in the first three models. However, once instruments were used andunobserved heterogeneity accounted for, asthma activities were no longer statistically significant.Whether Divisions provided practice nurse support was not related to the level or growth of asthma SIPclaims.
Divisions with a higher level of socio-economic disadvantage had higher asthma SIP claims, as didDivisions with larger practices. Divisions with more than four GPs per practice on average, however,had a lower level of asthma SIP claims. Divisions with a high proportion of part time GPs also had alower level of asthma SIP claims.
For all models, combinations of insignificant variables were excluded as a test of model stability, andthe results remained very similar.
6. DISCUSSION
Regional PCOs in different countries vary in their form and function and little is known of the effects ofthese different institutional arrangements on the quality and cost of primary health care. This study has
Table V. The effect of Division activities on the value of asthma service incentive paymentsper participating practice.
Variable OLS Fixed effectsSystem GMM
(without instruments for q)System GMM
(with instruments for q)
Constant 0.5141 2.6131 0.194 0.0271yit�1 0.6199��� 0.2765��� 0.5494��� 0.5581���
Area characteristicsRemote area 0.067 — 0.1092 0.0477Outer regional area 0.0006 — �0.0061 �0.0282Inner regional area 0.0613 — 0.0521 0.02IRSD 0.0010�� — 0.0014� 0.0015��
Mortality rate 0.0005 — 0.0004 0.0006GP characteristicsPatients per GP 0.0392 0.078 �0.0493 �0.0356Patients per GP squared �0.0021 �0.005 0.0022 0.0015GPs per practice 0.1921�� 0.1485 0.2282� 0.2548��
Practice size squared �0.0204 �0.0069 �0.0259 �0.0297�
Part time GPs �0.5995�� �0.9111 �0.7245� �0.7148�
Female GPs 0.1584 �0.0002 �0.0105 �0.0096GPs aged 455 years old 0.4469�� 0.4954 0.3534 0.3367Division outputsAsthma activities 0.1176�� 0.1629�� 0.1337�� �0.0037Practice nurse support 0.0043 0.052 0.0109 0.038Sample size 1388 1388 1388 1388Divisions 115 115 115Instruments 33 39Over-identifying restrictions 4 10Mean number of quarters 12.07 12.07 12.07Hansen/Sargan test w2(df) 5.06 (4) 11.32 (10)AR1 test �4.3��� �4.36���
AR2 test 0.55 0.59F-statistic (df) 73.09 (28)��� 55.73 (137)��� 63.11 (28)��� 72 (28)���
Notes: po0.1; ��po0.05; ���po0.0001. Models also include quarterly dummies (not shown). Based on data from the quarterbeginning 1st February 2002 to 1st May 2005.
REGIONAL PRIMARY-CARE ORGANISATIONS INFLUENCE 725
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

provided the first quantitative evidence about the effects of one particular model of PCO on primary-care performance using a unique longitudinal data set. The results show that Divisions of GeneralPractice in Australia are more likely to have influenced general practice infrastructure than clinicalperformance in diabetes, asthma or cervical screening. Evidence on the effect of specific Divisionactivities on performance was weak and suggested that there was an association between Divisionactivities in diabetes and asthma, but that this may have been due to reverse causality and unobservedfactors, rather than the effect of Divisions per se. Divisions that provided support for practice nurses didnot seem to influence any of the four measures of general practice performance. The results also showthat general practice performance in one period is heavily influenced by performance in previous timeperiods.
Although there have been a number of qualitative studies examining the development of PCOs, thereis very little quantitative evaluation of their impact on the costs and quality of primary-care services(Smith and Goodwin, 2006; Gravelle et al., 2000; Naccarella et al., 2006). Only two published studieshave attempted to examine the effect of Divisions. Georgiou et al. (2004) examined factors associatedwith the level of diabetes activity, using Division-level data and controlling for disease prevalenceand other factors. The study found that specific Division activities for diabetes were not associated withthe volume of diabetes activity. Morely et al. (2007) examined different models used by Divisionsin providing mental health services and found that Divisions which directly employed alliedhealth professionals or had a system of direct referral from GPs to allied health professionals wereassociated with higher health outcomes. Our results greatly improve on these studies by exploiting thedynamic nature of decision making by Divisions and general practices, and accounting for muchunobserved heterogeneity and the reverse causality between Division and general practice decisionmaking.
The data used were limited in that they covered a relatively narrow range of general practiceperformance. It was possible that Divisions were focusing on other clinical areas at the time of theanalysis and these are not captured in the data. This may underestimate their effects. Furthermore, thedata on specific Division outputs were limited to dummy variables of whether Divisions reported thatthey were undertaking these activities or not. There was no information that was common across timeperiods on what specific activities these were or their magnitude, and this information was self-reportedin a survey. Further research would ideally use a wider range of general practice-level data and wouldrequire more accurate and reliable data on Division activities.
Our interpretation of Division random effects as the effect of Divisions on performance relies on ourability to control for health-care needs, rurality and other characteristics of Divisions. We havecontrolled for many of the major sets of confounding factors that influence variations in performance,such as rurality, health needs, population, and GP and practice characteristics. The models included allcause mortality for the under 75’s as a general indicator of needs, along with variables reflectingsocioeconomic disadvantage, indigenous population and the proportion of over 65 year olds. Modelswere also estimated with disease-specific mortality rates for respiratory conditions in the asthma model,diabetes mortality in the diabetes model and cancer in the cervical screening model and the results didnot change.
Nevertheless, we cannot rule out that there are other unobserved factors that influence theproportion of explained variation in performance, and that these are not related to the existence oractivities of Divisions. This may include unobserved factors influencing GPs’ location decisions. To theextent that when some unobserved variables exist, then we are likely to overestimate the proportion ofvariation explained by Division effects. To the extent that these unobserved factors are the same foreach measure of performance, it is then differences in the proportion of variation explained that are themost interesting. Division effects are higher for general practice infrastructure (45% of explainedvariation) than for the clinical areas of performance, suggesting that Divisions have had a relativelystronger impact on infrastructure than in clinical areas.
A. SCOTT AND W. COOTE726
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

The data used covered 2000–2005 (depending on the model used). This was a period when the earlyeffect of Divisions had perhaps already been realised, and was a period of funding uncertainty forDivisions due to a major government review (Divisions Review Panel, 2003). There was also anemerging GP workforce shortage that led to rising prices charged to patients for GP services, and GPswere finding it difficult to comply with the administrative requirements of government programmes,including the PIP scheme (Proudfoot et al., 2003; Productivity Commission, 2003). These may bereasons why the measured impacts of Divisions in the study were weak.
A potential issue with the analysis is that the dependent variables used may be related to one anotherand a simultaneous estimation would have been appropriate (Hauck and Street, 2006; Martin et al.,2007). For example, Divisions with practices who claim a high level of SIP payments for asthma are alsolikely to contain practices with a high level of claims for SIP payments for diabetes. Alternatively thetwo may be substitutes, such that practices focus their effort on the more profitable activities. Thiswould be more of an issue if we had been using practice-level data, but since Division-level data arebeing used, issues of substitution of activity between practices (rather than within practices) are lessrelevant.
A further issue relates to the use of system GMM and the problem of weak instruments. Although weused the minimum number of over-identifying restrictions, the problem of weak instruments magnifiesitself in system GMM when the variance of the fixed effects is large relative to the variance of theidiosyncratic error and where the data series are highly persistent, some of which are evident in themodels estimated, with a particularly high level of persistence in the model explaining the proportion ofPIP practices in a Division (Bun and Windmeijer, 2007). A high level of persistence means that theinstrument set contains little information that can be used to identify the parameters. The issue of highpersistence is more likely to occur in aggregate data where little observed change from one period to thenext masks any positive or negative changes amongst individuals that are averaged out in the aggregate.This is another reason why the use of small area data is not ideal.
To conclude, the evolution of Divisions of General Practice in Australia is set to continue as theyincreasingly become providers and funders of health-care services, in addition to providing support togeneral practices. The lack of impact by Divisions on GPs’ clinical activity may reflect the findings fromthe literature on the use of educational strategies and other non-financial interventions (e.g. recall-reminder systems, opinion leaders) to change clinical practice, where evidence of their effects is mixed(O’Brien et al., 2001; Renders et al., 2000; Doumit et al., 2007). Divisions in Australia use a diverse setof strategies, and it would seem important that the mechanisms they use to attempt to change GPbehaviour and support GPs need to be re-examined in the light of this evidence.
The future role of Divisions of General Practice in Australia is uncertain, although they could evolveinto similar organisations as Primary Care Trusts in the UK or Primary Health Organisations inNew Zealand. However, this change will mean that there will be more pressure to act as agents forgovernment as well as agents for their GP members. Whether this would crowd out the network effects ofDivisions will be important to monitor. What is clear from this research is that Divisions, and regionalPCOs more generally, do have a role to play in influencing the efficiency of the primary-care sector.
ACKNOWLEDGEMENTS
This project was funded by the Australian General Practice Network (AGPN). The views are those ofthe authors and not AGPN. Thanks go to support from the project advisory group and Shirley Chanfor research assistance. Data were kindly provided by the Primary Health Care Research andInformation Service at Flinders University and the Department of Health and Ageing. Usefulcomments were provided from seminar participants at the University Technology Sydney and MonashUniversity.
REGIONAL PRIMARY-CARE ORGANISATIONS INFLUENCE 727
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

APPENDIX A
The random effects regression models used to calculate Division random effect its given in Table AI.
REFERENCES
Arellano M, Bond S. 1991. Some tests of specification for panel data: Monte Carlo evidence and an application toemployment equations. Review of Economic Studies 58: 277–297.
Arellano M, Bover O. 1995. Another look at the instrumental variables estimation of error-components models.Journal of Econometrics 68: 29–51.
Baltagi B. 2005. Econometric Analysis of Panel Data (3rd edn). Wiley: Chichester.Beilby J, Holton C, Bubner T, Harris M, Powell Davies G, Proudfoot J. 2003. Building Practice Capacity for
Chronic Disease Management in General Practice: Discussion Paper for General Practice Partnership AdvisoryCouncil. Department of Health & Ageing, Canberra.
Bensing JM, van den Brink-Muinen A, de Bakker DH. 1993. Gender differences in practice style: a Dutch study ofgeneral practitioners. Medical Care 31: 219–229.
Blundell R, Bond S. 1998. Initial conditions and moment restrictions in dynamic panel data models. Journal ofEconometrics 87: 11–143.
Charles J, Britt H, Valentini L. 2006. The independent effect of age of general practitioner on clinical practice.Medical Journal of Australia 185: 105–109.
Choudhry NK, Fletcher RH, Soumerai SB. 2005. Systematic review: the relationship between clinical experienceand quality of health care. Annals of Internal Medicine 142: 260–273.
Demange G, Wooders M. 2005. Group Formation in Economics. Networks, Clubs, and Coalitions. CambridgeUniversity Press: Cambridge.
Table AI. Random effects regression models used to calculate Division random effect.
Variable PIP practices Asthma SIP Diabetes SIP Cervical SIP
Remote area 0.097 0.7261� �0.3572 �0.4133Outer regional area 0.0089 �0.0172 �0.5550�� �0.6040���
Inner regional area 0.0046 0.148 �0.1039 �0.1421IRSD 0.0000 0.0055�� 0.0052��� 0.0060���
Mortality rate 0.0003 �0.0004 0.0017 �0.0010Indigenous population 0.0343 0.5487 �0.0879 0.0947Population 465 years old �0.0677 �4.7757�� �3.1404�� 1.2657Patients per GP 0.0007�� �0.0042 �0.0075�� �0.0087���
Patients per GP squared �0.0000� 0.0000 0.0000�� 0.0000���
GPs per practice 0.3866��� �0.1024 �0.3650�� �0.3754��
Practice size squared �0.0415��� 0.0506 0.0575�� 0.0676��
Part time GPs �0.1892�� �1.7723�� �1.9605�� �1.4874��
Female GPs �0.0513� 0.5251 0.6660� 0.499GPs aged 455 years old 0.0045 �0.958 1.0375� 2.5853���
Number of observations 1377 1271 1363 1361Number of Divisions 118 118 119 119Number of quarters 11.46 8.96 10.92 10.69Model w2 (df ) 1487 (41) 697 (41) 911 (41) 861 (41)R2 (within) 0.52 0.34 0.22 0.05R2 (between) 0.58 0.37 0.44 0.47R2 (overall) 0.6 0.45 0.65 0.73Rho (var u/(var u 1 var v)) 0.89 0.37 0.42 0.37Var(y) 0.0216 0.7846 0.6849 0.5554Var(u) 0.0097 0.1471 0.0850 0.0603Var (u)/Var (y) 0.45 0.19 0.12 0.11
Notes: 1: Based on data from the quarter beginning 1st February 2002 to 1st November 2004. All models include quarterlydummies, state dummies, and a time-averaged variable for each time-varying explanatory variable, as per Mundlak (1978).Coefficients are not shown but available from authors on request.�5 po0.1, ��5 po0.05, ���5 po0.0001.
A. SCOTT AND W. COOTE728
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec

Divisions Review Panel 2003. The future role of the Divisions network. Report of the Review of the Role of Divisionsof General Practice. Australian Government Department of Health and Ageing: Canberra.
Doumit G, Gattellari M, Grimshaw J, O’Brien MA. 2007. Local opinion leaders: effects on professional practiceand health care outcomes. Cochrane Database of Systematic Reviews (1).
Georgiou A, Burns J, Harris MF. 2004. GP claims for completing diabetes ‘cycle of care’. Australian FamilyPhysician 33: 755–757.
Hamilton K, Wyke S, Sullivan F, Scott A, Taylor R, Ikenwilo D. 2005. A managed clinical network for cardiacservices: set-up, operation and impact on patient care. International Journal of Integrated Care 5: 1–15.
Hordacre AL, Keane M, Kalucy E, Moretti C. 2006. Making the connections. Report of the 2004–2005 AnnualSurvey of Divisions of General Practice, Primary Health Care Research & Information Service, Department ofGeneral Practice, Flinders University, Adelaide and Australian Government Department of Health and Ageing.
Jackson MO. 2005. A survey of network formation models: stability and efficiency. In Group Formation inEconomics. Networks, Clubs, and Coalitions, Demange G, Wooders M (eds). Cambridge University Press:Cambridge.
Morely B, Pirkis J, Sanderson K, Burgess P, Kohn F, Naccarella L, Blashki G. 2007. Better outcomes in mentalhealth care: impact of different models of psychological service provision on patient outcomes. Australian andNew Zealand Journal of Psychiatry 41: 142–149.
Mundlak Y. 1978. On the pooling of time series and cross section data. Econometrica 46(1): 69–85.O’Brien MA, Freemantle N, Oxman AD, Wolf F, Davis DA, Herrin J. 2001. Continuing education meetings and
workshops: effects on professional practice and health care outcomes. Cochrane Database of Systematic Reviews (1).Productivity Commission 2003. General practice administrative and compliance costs. Research Report.
Productivity Commission, Canberra.Proudfoot J, Swan E, Amoroso C, Grimm J, Jayasinghe U, Powell Davies G, Bubner T, Holton C, Barton C,
Beilby J, Harris M. 2004. Measuring the capacity of Australian general practices to conduct quality chronicdisease care. Proceedings of 2nd Australasian Conference on Safety and Quality in Health Care, Canberra.
Renders CM, Valk GD, Griffin S, Wagner EH, van Eijk JThM, Assendelft WJJ. 2000. Interventions to improve themanagement of diabetes mellitus in primary care, outpatient and community settings. Cochrane Database ofSystematic Reviews (4).
Roodman D. 2008. How to do xtabond2: an introduction to ‘difference’ and ‘system’ GMM in Stata. WorkingPaper No. 103. Center for Global Development.
Scott A, Coote B. 2007. The value of the divisions network. An evaluation of the effect of divisions of generalpractice on primary care performance. Report No. 8, Melbourne Institute of Applied Economic and SocialResearch, The University of Melbourne, March.
Scott A, Schurer S, Jensen PH, Sivey P. 2008. The effects of financial incentives on quality of care: the case ofdiabetes. Working Paper No. 12/08, Melbourne Institute of Applied Economic and Social Research, TheUniversity of Melbourne.
Simeons S, Scott A. 2005a. Voluntary or compulsory health care reform? The case of primary care organisations inScotland. Health Policy 72: 351–358.
Simeons S, Scott A. 2005b. Integrated primary care organisations: to what extent is integration occurring and why?Health Services Management Research 18: 25–40.
Smith J, Goodwin N. 2006. Towards Managed Primary Care: The Role and Experience of Primary CareOrganisations. Ashgate Publishing: Aldershot.
Smith J, Mays N. 2007. Primary care organizations in New Zealand and England: tipping the balance of the healthsystem in favour of primary care? International Journal of Health Planning and Management 22(1): 3–19;discussion 21–4.
Starfield B, Macinko J. 2005. Contribution of primary care to health systems and health. Milbank Quarterly 83:457–502.
Zwar NA, Comino EJ, Hasan I et al. 2005. General practitioner views on barriers and facilitators toimplementation of the Asthma 31 visit plan. Medical Journal of Australia 183: 64–67.
REGIONAL PRIMARY-CARE ORGANISATIONS INFLUENCE 729
Copyright r 2009 John Wiley & Sons, Ltd. Health Econ. 19: 716–729 (2010)
DOI: 10.1002/hec