Embed Size (px)
Citation preview

The Journal of Arthroplasty 29 (2014) 401–404
Contents lists available at ScienceDirect
The Journal of Arthroplasty
j ourna l homepage: www.arth rop lasty journa l .o rg
Do Larger Femoral Heads Improve the Functional Outcome in Total Hip Arthroplasty?
Charlotte L. Allen, MBCHB a, Gary J. Hooper, MBCHB, FRACS b, Christopher M.A. Frampton, PhD c
a Department of Orthopaedics, Christchurch Hospitalb Department of Orthopaedic Surgery and Musculoskeletal Medicine, University of Otago, Christchurchc Department of Medicine, Christchurch Hospital, University of Otago
a b s t r a c ta r t i c l e i n f o
There are no conflicts of interest.The Conflict of Interest statement associated with thi
dx.doi.org/10.1016/j.arth.2013.06.017.Reprint requests: Charlotte L. Allen, MBCHB, D
Christchurch Hospital.
0883-5403/2902-0032$36.00/0 – see front matter © 20http://dx.doi.org/10.1016/j.arth.2013.06.017
Article history:Received 22 April 2013Accepted 12 June 2013
Keywords:hip joint arthroplastylarge headsfunctional outcome
Use of larger diameter femoral heads has been popularised in total hip arthroplasty (THA). Recent studieshave implicated larger femoral heads in early failure. We evaluated what effect the size of the femoralhead had on the early functional outcome in order to determine the optimal head size for the maximalfunctional outcome. There were 726 patients who underwent elective THA and were divided into 3 groupsaccording to head size then compared with respect to functional outcome scores and dislocation rates. Thisstudy failed to show that increasing the size of the femoral head significantly improved the functionaloutcome at 1 year after total hip arthroplasty but that the use of a 36 mm or greater femoral head didreduce the dislocation rate.
s article can be found at http://
epartment of Orthopaedics,
14 Elsevier Inc. All rights reserved.
© 2014 Elsevier Inc. All rights reserved.
Increasing the femoral head size in total hip arthroplasty (THA)has been shown to improve both the range of motion (ROM) andstability of the hip [1]. Dislocation has been shown to be thecommonest cause for early revision in THA [2,3] with rates of up to14% [4], and the use of larger femoral heads has been reported toreduce this hip dislocation rate [1,4,5]. Most of the studiesinvestigating the effects of head size on ROM, revision rates anddislocation following THJR [1,3,4,6] have been conducted in vitro oron cadavers.
Larger femoral heads are associated with higher volumetric wearindependent of material [7–9] and with polyethylene couplings havebeen associated with excessive polyethylene wear and periprostheticosteolysis [1]. The recent development of highly cross-linked ultra-high molecular weight polyethylene has been reported to reduce thiswear rate significantly [10–12]. Larger femoral heads associated withhard-on-hard bearing surfaces may reduce the periprosthetic osteo-lysis but have been associated with metal ion debris, pseudotumour,trunion failure, squeaking and ceramic fracture [9,13–15].
The objective of this study is to review all patients who underwentTHJR in a dedicated elective hospital between 2009 and 2011 and toidentify the relationship between femoral head size and earlyfunctional outcome at 6 and 12 months in order to determine theoptimal head size which allowed the best functional outcome.
Our hypothesis was that larger femoral heads would be associatedwith better functional outcomes and a lower dislocation rate.
Materials and Methodology
This was a prospective observational study of all patients whounderwent THA at a single dedicated elective hospital betweenAugust 2009 and April 2011.
There were a total of 726 THJRs performed over the period by 17surgeons who individually chose the implants used, in particular thefemoral head size. The femoral head size was determined by thepatient’s age and acetabular size and was an individual decision basedon the surgeon’s preference. All procedures were performed by aposterior approach.
Patients were divided into three groups according to hip headsize — small head group (b36 mm), medium head group (36 mm)and one large head group (N36 mm). These groups were arbitrarilychosen to match the report of our National joint registry.
Parameters/Assessment of Functional Outcome
Patients completed modified questionnaires to assess the primaryoutcome of functional improvement. These questionnaires used werethe Oxford hip score (OHS) [16], the Western Ontario McMastersOsteoarthritis Index (WOMAC) [17,18], the High Activity ArthroplastyScore (HAAS) [19] and the University of California Los Angeles (UCLA)[20] activity scores to look for any subtle changes in more demandingactivities. We divided the HAAS score into 3 parts giving HAAS 1(walking), HAAS 2 (running) and HAAS 3 (overall).
Pain was assessed using a visual analogue scale with 0 being nopain and 10 the most severe pain imaginable.
Patients were asked to complete pre-operative questionnaires andthen repeat these at 6 months and 12 months post-operatively. Of the726 patients 84% returned a fully completed questionnaire at12 months.

Table 2Results Pre-Operatively, at 6 and 12 Months Post-Operatively.
HAAS 1 HAAS 2 HAAS 3 Oxford Pain UCLA WOMAC
Pre-OperativeSmall 3.6 13.9 3.1 17.9 3.9 3.7 35Medium 3.2 15.6 3.5 17.9 3.9 4.1 38.7Large 3.3 16.3 3.3 18.9 4 4.1 36.1P value 0.104 b0.001 0.061 0.551 0.762 0.073 0.021
6 monthsSmall 10.1 21.3 3.6 39.7 1.0 5.4 77.1Medium 9.9 23.5 4.0 40.0 0.9 6.1 80.1Large 10.2 25.1 4.6 41.3 0.8 6.7 83.8P value 0.425 0.078 0.008 0.502 0.657 0.004 0.033
12 monthsSmall 10.3 22.2 3.8 41.1 0.8 5.7 79.6Medium 10.5 24.8 4.2 42.1 0.8 6.3 83.8Large 10.9 25.8 4.3 43.5 0.6 6.9 88.0P value 0.07 0.543 0.536 0.529 0.261 0.445 0.164
402 C.L. Allen et al. / The Journal of Arthroplasty 29 (2014) 401–404
A secondary endpoint of dislocation, revision and infection withinthe first year was also reviewed. These were assessed through thequestionnaire by asking the patient directly. The New Zealand JointRegistry was used to check the revision data.
Statistical Analysis
Preoperative characteristics were compared between head sizegroups using Chi-square and 1-way ANOVA tests. Functional scoreswere compared between groups using 1-way ANOVA and wherethese were significant these differences were further explored usingFisher’s least significant difference tests.
Significance was set at P b 0.05.
Results
The patient demographics are shown in Table 1. There werestatistically significant differences between the groups pre-opera-tively in gender, age and BMI. There were more females in thesmall head group compared with a higher percentage of males inthe medium and large groups. Patients in the large head groupwere younger on average than the patients in the smaller headgroups and patients in the smallest head group tended to have alower BMI.
Pre-operative scores between the groups were generally similar.However there were statistically significant differences in the HAAS 2and the WOMAC scores with the small group having lower pre-operative scores compared to the medium or large in the HAAS 2 andthe medium in the WOMAC (Table 2).
The results from each group are shown at 6 and 12 months(Table 2). There was statistically significant change between the largeheads and the smaller heads in the HAAS 3, UCLA and WOMAC scoresat 6 months. No statistically significant differences were seen in thechanges to 12 months (Table 3).
There was a significant increase in the scores between the pre-opand the 12 month assessments in all the scoring systems. There was aslightly increased improvement in the group of large heads comparedwith the small and medium heads although this was not found to bestatistically significant.
Age Group and Gender Analysis
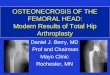
The data were then reassessed to control for age. Patients under60 years at the time of surgery were compared to those ≥ 60 years,and difference in results reached statistical significance for the Haas 2score (P b 0.001). The under 60 year group also showed slightlyhigher pre-operative (Fig. 1).
In patients b60 years, greater improvement over 12 months wasgenerally seen across all head sizes when compared to the N60 yearsgroup and this reached statistical significance for the UCLA scores(P = 0.021) (Table 4). Patients ≥60 years had the greatest func-
Table 1Characteristics of Head Sizes Within Each Group.
Small (b36) Medium (36) Large (N36) P Value
Number 399 254 73Gender Male 129 (32%) 160 (63%) 49 (67%) b0.001
Female 270 (68%) 94 (37%) 24 (33%)Side Left 187 (47%) 119 (47%) 36 (49%) 0.924
Right 212 (53%) 135 (53%) 37 (51%)Average Age(range)
Total 68 72 (22–94) 63 (31–86) 56 (33–76) b0.001
Average BMI(range)
Total 28.2 27.7 (13–44) 28.9 (19–52) 28.2 (20–44) 0.018
tional improvement in smaller heads which is the opposite effectthan predicted.
Scores were further analysed divided into two groups by gender.Males had 38% in the small head group, 47% medium and 14% in thelarge group. This compared to the female group which had 70%small, 24% medium and 6% large which reflect the different sizes ofthe patients.
The overall change in scores across the 12 month period wassmaller in females than males in the small and large ball groups inevery category except theWOMAC and pain scoreswhere females hadgreater improvement across all the sizes (Table 5). The difference inchange between the genders reached statistical significance for Haas 3(P = 0.044) and UCLA (P = 0.049) scores.
Secondary Outcomes
There were 5 dislocations, 7 infections and 1 revision over the12 month post-operative period. The majority of these were inthe small head size group. All of the dislocations, over half of theinfections and the only revision were in patients with a size 32 head.The cases of dislocations were further reviewed to ensure nodifferences in implant positioning or surgical approach. The noteswere also reviewed to determine cause of dislocation and none werefound to have had a significant trauma (Table 6).
When divided into age groups, two infections occurred in patientsyounger than 60, however all other complications occurred in theover 60 year old group including all the dislocations. The majority ofthe dislocations occurred in females with 5 dislocations comparedwith 1 in males.
Discussion
The aim of a total hip joint arthroplasty is to relieve joint pain andimprove function in patients with disabling arthritis with the lowestpossible complication rate [21,22]. Dislocation is a significanttraumatic event for patients and has an incidence of 0.5%–5% [5,23–25]. It is one of the most common causes of early revision followingtotal hip arthroplasty [2]. There are several causes for early dislocationincluding patient, surgeon and implant related factors. Reducing the
Table 3Change Over 12 Month Period Post-Operatively.
Total HAAS 1 HAAS 2 HAAS 3 Oxford Pain UCLA WOMAC
Small 6.8 8.3 0.6 23.1 −3.1 2.0 44.6Medium 7.3 9.2 0.7 24.2 −3.1 2.2 45.1Large 7.6 9.6 0.9 24.6 −3.4 2.8 51.8P value 0.07 0.543 0.536 0.529 0.261 0.445 0.164

Pre-op scores
0.05.0
10.015.020.025.030.035.040.0
Haas 1
Haas 2
Haas 3 Ox
Pain
UCLA
Wom
ac
<60
>60
Fig. 1. Comparison of preoperative scores for patients below 60 years and those≥60 years.
Table 5Change in Scores at 12 Months Post-Op in (A) Male Patients and (B) Female Patients
A. Male Patients
Male HAAS 1 HAAS 2 HAAS 3 Oxford Pain UCLA WOMAC
Small 7.0 9.0 0.8 23.8 −2.9 2.0 43.0Medium 7.2 8.9 0.8 24.1 −3.1 2.4 44.4Large 7.7 9.7 1.1 25.0 −3.3 3.2 50.2P value 0.25 0.55 0.45 0.66 0.19 0.52 0.13
B. Female Patients
Female HAAS 1 HAAS 2 HAAS 3 Oxford Pain UCLA WOMAC
Small 6.7 7.9 0.5 22.8 −3.1 1.9 45.3Medium 7.4 9.2 0.4 24.2 −3.1 1.9 45.7Large 7.4 9.1 0.7 23.9 −3.5 1.9 53.9P value 0.15 0.30 0.84 0.46 0.69 0.87 0.66
403C.L. Allen et al. / The Journal of Arthroplasty 29 (2014) 401–404
risk of this disabling complication has been focused on increasing thefemoral head to neck ratio, thereby enabling an extended ROM beforethe neck and cup impinge resulting in levering of the femoral head outof the socket. The introduction of hard on hard bearing surfaces, aswell as the success of highly cross-linked polyethylene, has encour-aged surgeons to use larger femoral heads with thinner acetabulararticulating surfaces in an attempt to reduce dislocation. The results ofthis study demonstrated that the use of a 36 mm femoral head doesreduce the risk of dislocation and support the results of other studies[1,4,5,26], however the number of dislocations was low (0.8%) and alarger study group will be required to reach statistical significance.
The approach used in all patients was a posterior approachwhich has been shown to lead to high dislocation rates [23,26]. The5 cases of dislocation were reviewed separately and no differenceswere found in approach, implant positioning or effects of trauma tocause dislocation.
A number of different patient-related outcome measure (PROMs)systems have been developed to try to accurately assess the clinicaloutcomes patients achieve following joint arthroplasty and specifi-cally, how successful the surgery has been from their point of view.Most of these scoring systems incorporate questions relating to painand everyday activities. Assessing functional status pre and postoperatively can also help us assess which patients benefit most andtherefore those who are the most appropriate to be offered theseprocedures [22]. The early functional status as demonstrated by the6 month Oxford hip score has been shown to be a predictor of therequirement for early revision [27] and therefore may be an essentialelement in determining the prognosis following THA. The Oxford hipscore however was shown to have no predictive accuracy in thesatisfaction of patients therefore may not be useful in patientprioritisation [21]. There has been a correlation however betweenhigher number of pre-operative expectations and greater improve-ment following surgery [21].
Table 4Change in Scores at 12 Months Post-Op in (A) Patients Under 60 Years and (B) PatientsOver 60 Years.
A. Patients Under 60 Years
b60 HAAS 1 HAAS 2 HAAS 3 Oxford Pain UCLA WOMAC
Small 7.3 8.2 0.2 24.5 −3.5 2.4 50.3Medium 7.3 8.8 0.8 24.5 −3.0 2.3 44.7Large 7.6 10.1 1.1 24.4 −3.4 3.5 54.6P value 0.70 0.84 0.13 0.89 0.25 0.40 0.084
B. Patients Over 60 Years
N60 HAAS 1 HAAS 2 HAAS 3 Oxford Pain UCLA WOMAC
Small 7.2 9.3 0.7 24.0 −3.2 2.2 46.8Medium 6.5 7.0 0.6 22.5 −3.0 1.6 40.4Large 6.1 6.7 0.7 20.9 −2.5 0.4 35.4P value 0.13 0.55 0.86 0.59 0.65 0.57 0.58
.
The extended ROM afforded by a larger femoral head should alsoenable increased activities and it intuitively would be expected thatthis patient group should score higher on hip outcome measures. Weshowed an overall improvement in all outcomes at 6 months and12 months post operatively, as expected, and the scores showed astatistically significant greater improvement with a larger head size at6 months. The difference was so small that it was unlikely todemonstrate a clinically significant improvement eg the differencein the OHS was 1.5 between the small and large head group and toachieve a clinically significant improvement 3–5-point (10%) differ-ence is required [28]. This early functional improvement with largerheads however was not continued at 12 months.
The difference between preoperative and postoperative scores wasincreasedwhen the groupswere assessedwith respect to age. Patientsb60 years had slightly higher pre-operative scores, which could beexpected, but they also performed better across all outcome scoresbetween head sizes when compared to those N60 years, with theUCLA activity score being significant (P b 0.021).
When assessed by gender, females had a higher percentage ofsmall heads compared to males which is likely to reflect smallerpatient size in this group. There was a statistically significant greaterimprovement in Haas 3 (P = 0.044) and UCLA (P = 0.049). In maleshowever there was no significant difference between head sizes ineither group.
We used 2 outcome measures that assess higher activities in orderto see whether the younger patients with larger femoral headsachieved better in ‘sporting activities’ but were unable to show anydifference at 12 months, although the results for all measures of theHAAS and the UCLA scorewere increased in patients b60 years as wellas in males with larger femoral heads.
Increased volumetric wear has been shown in metal-on-poly andmetal-on-metal articulations with increased head size and this maybe a cause for early failure [7–9]. This study only recorded the earlyresults of joint function and cannot comment on the long termoutcomewith respect to wear. The purpose of this study was to assessthe early functional results of various sized femoral heads in order togive a rational method for the choice of femoral head size. Currentlythere are several studies assessing the wear rate of larger femoralheads with highly cross linked polyethylene which are recording lowwear rates over 5 years and offer encouragement for the continueduse of these implants [10–12]. Increasing the size of the femoral headmay also cause increased metal debris from the articulation of thehead and Morse taper of the stemwhichmay result in early failure. Asthe primary aim of this study was to assess early function, nocomment can bemade on the long term outcome however, the resultsdo suggest that there is little functional improvement to be gained inusing a head size N36 mm.
The choice of femoral head size in total hip joint arthroplasty isoften determined by patient size, therefore the differences betweenthe groups in this study pre-operatively were expected, with females,

Table 6Details of Patients With Dislocations.
Gender Side BMIDislocationDirection Size
AcetabulumSize
Acetabular Inclination(Degrees)
Acetabular Anteversion(Degrees) Trauma Revision
F R 27 posterior 32 50 37 17 Twist in garden NoneM L 20 anterior 32 52 39 32 nil — post-op x-ray NoneF R 29 posterior 32 52 33 17 Standing NoneF R 31 anterior 32 52 55 46 Standing from toilet None
404 C.L. Allen et al. / The Journal of Arthroplasty 29 (2014) 401–404
lighter and older patients all being more likely to have a smaller headsize. The study was a retrospective review of cases done by multiplesurgeons in a single centre in which the surgeon chose the head sizedependent on the patient from pre-operative planning tools and intra-operative assessment. Although this is acknowledged as a limitation ofthis studywe believe that it also represents a clinical reality and henceadds more balance to the rationalisation of femoral head size.
Another limitation was that not all questionnaires were completedfully at the pre-operative stage and this incomplete information mayhave altered the baseline scores. There was a delay in return of12 month scores following a series of major earthquakes in our citywhere several thousand people were displaced from their homes andnot contactable. These patients were finally contacted by telephoneinterview in order to gain more complete information, however thequestionnaires were returned after the 12 month period which mayhave altered the scores. Despite this limitation the overall 12 monthfollow up was excellent at over 84%.
We acknowledge that this study does have a short follow-up butbelieve that it provides important information showing that themaximum functional advantage following total hip arthroplasty is notsignificantly improved by using a femoral head N36 mm.
Conclusion
In conclusion, this study failed to show a relationship betweenincreased functional outcome and increased size of femoral head atone year after total hip joint arthroplasty but the dislocation rate wasreduced with use of a 36 mm or greater femoral head. Based on theseresults there appears to be little advantage in using a femoral headN36 mm in all patients undergoing THA.
References
1. Burroughs BR, Hallstrom B, Golladay GJ, et al. Range of motion and stability in totalhip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J Arthroplasty2005;20(1):11.
2. Hooper GJ, Rothwell AG, Stringer M, et al. Revision following cemented anduncemented primary total hip replacement: a seven-year analysis from the NewZealand joint registry. J Bone Joint Surg Br 2009;91-B(4):451.
3. Matsushita A, Nakashima Y, Jingushi S, et al. Effects of the femoral offset and thehead size on the safe range of motion in total hip arthroplasty. J Arthroplasty 2009:646 Taylor and Francis.
4. Dudda M, Gueleryuez A, Gautier E, et al. Risk factors for early dislocation after totalhip arthroplasty: a matched case–control study. J Orthop Surg (Hong Kong)2010;18(2):179.
5. Jameson SS, Lees D, James P, et al. Lower rates of dislocation with increased femoralhead size after primary total hip replacement: a five-year analysis of NHS patientsin England. J Bone Joint Surg Br 2011;93-B(7):876.
6. Kluess D, Martin H, Mittelmeier W, et al. Influence of femoral head size onimpingement, dislocation and stress distribution in total hip replacement. Med EngPhys 2007;29(4):465.
7. Lachiewicz PF, Heckman DS, Soileau ES, et al. Femoral head size and wear ofhighly cross-linked polyethylene at 5 to 8 years. Clin Orthop Relat Res 2009;467(12):3290.
8. Leslie I, Williams S, Brown C, et al. Effect of bearing size on the long-term wear,wear debris, and ion levels of large diameter metal-on-metal hip replacements—anin vitro study. J Biomed Mater Res 2008;87B(1):163 Wiley Subscription Services,Inc., A Wiley Company.
9. Cross M, Nam D, Mayman D. Ideal femoral head size in total hip arthroplastybalances stability and volumetric wear. HSS Jrnl. Springer-Verlag; 2012;8(3):270–4.
10. Jibodh S, Bragdon C, Greene M, et al. Minimum five year outcome and wear analysisof large diameter femoral heads on highly cross-linked polyethylene liners. J BoneJoint Surg Br 2010;92-B(SUPP IV):520.
11. Bragdon CR, Kwon YM, Geller JA, et al. Minimum 6-year followup of highly cross-linked polyethylene in THA. Clin Orthop Relat Res 2007:465.
12. Muratoglu OK, Bragdon CR, O'Connor D, et al. Larger diameter femoral heads usedin conjunction with a highly cross-linked ultra–high molecular weight polyethyl-ene: a new concept. J Arthroplasty 2001:24 Taylor and Francis.
13. Hammerberg EM, Wan Z, Dastane M, et al. Wear and range of motion of differentfemoral head sizes. J Arthroplasty 2010:839 Taylor and Francis.
14. Callaghan JJ, Cuckler JM, Huddleston JI, et al. How have alternative bearings (such asmetal-on-metal, highly cross-linked polyethylene, and ceramic-on-ceramic)affected the prevention and treatment of osteolysis? J Am Acad Orthop Surg2008;16(Suppl 1):S33.
15. Garbuz D, Tanzer M, Greidanus N, et al. The John Charnley award: metal-on-metal hip resurfacing versus large-diameter head metal-on-metal total hiparthroplasty: a randomized clinical trial. Clin Orthop Relat Res 2010;468(2):318Springer-Verlag.
16. Dawson J, Fitzpatrick R, Murray D, et al. Questionnaire on the perceptions ofpatients about total knee replacement. J Bone Joint Surg Br 1998;80-B(1):63.
17. Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: ahealth status instrument for measuring clinically important patient relevantoutcomes to antirheumatic drug therapy in patients with osteoarthritis of the hipor knee. J Rheumatol 1988;15(12):1833.
18. Bellamy N. WOMAC osteoarthritis index: user guide IX. Nicholas Bellamy; 2008 .19. Talbot S, Hooper G, Stokes A, et al. Use of a new high-activity arthroplasty score to
assess function of young patients with total hip or knee arthroplasty. J Arthroplasty2010:268 Taylor and Francis.
20. Zahiri CA, Schmalzried TP, Szuszczewicz ES, et al. Assessing activity in jointreplacement patients. J Arthroplasty 1998:890 Taylor and Francis.
21. Judge A, Arden NK, Price A, et al. Assessing patients for joint replacement: can pre-operative Oxford hip and knee scores be used to predict patient satisfactionfollowing joint replacement surgery and to guide patient selection? J Bone JointSurg Br 2011;93-B(12):1660.
22. Quintana JM, Escobar A, Arostegui I, et al. HEalth-related quality of life andappropriateness of knee or hip joint replacement. Arch Intern Med 2006;166(2):220.
23. Kwon MS, Kuskowski M, Mulhall KJ, et al. Does surgical approach affect total hiparthroplasty dislocation rates? Clin Orthop Relat Res 2006:447.
24. Hedlundh U, Ahnfelt L, Hybbinette CH, et al. Surgical experience related todislocations after total hip arthroplasty. J Bone Joint Surg Br 1996;78-B(2):206.
25. Woo RY, Morrey BF. Dislocations after total hip arthroplasty. J Bone Joint Surg Am1982;64(9):1295.
26. Krenzel BA, Berend ME, Malinzak RA, et al. High preoperative range of motion isa significant risk factor for dislocation in primary total hip arthroplasty.J Arthroplasty 2010:31 Taylor and Francis.
27. Rothwell AG, Hooper GJ, Hobbs A, et al. An analysis of the Oxford hip and kneescores and their relationship to early joint revision in the New Zealand JointRegistry. J Bone Joint Surg Br 2010;92-B(3):413.
28. Murray DW, Fitzpatrick R, Rogers K, et al. The use of the Oxford hip and knee scores.J Bone Joint Surg Br 2007;89-B(8):1010.