Embed Size (px)
Citation preview

Page 1Diabetes Education Services© 1998-2017 www.DiabetesEd.net
DM Fundamentals – Class 3Insulin and Pattern Management
Beverly Thomassian, RN, MPH, BC‐ADM, CDEPresident, Diabetes Education Services
2017
Insulin – Ultimate Hormone Replacement Therapy – Class 3
Incorporating National Guidelines into practice
Using basal/bolus insulin therapy to improve glucose control from hospital to home
Glucose patterns and adjustment strategies
Insulin – the Ultimate Hormone Replacement Therapy
Objectives: •Discuss the actions of different insulins•Describe using pattern management as an insulin adjustment tool.

Page 2Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Poll question 1. A patient tells you she doesn't want to start on insulin. What is your best response?a. The needles are so small, you won't feel a thing.
b. You might die if you don't take insulin.
c. Tell me why.
d. There is a doctors' order to start insulin.
Psychological Insulin Resistance (PIR)
50% of providers in study threatened pts “with the needle”.
Less than 50% of providers realized insulins’ positive effect on type 2 dm
Most pts don’t believe that insulin would “better help them manage their diabetes”.
Solutions: Find the root of PIR and address it, use more insulin pens
Diabetes Attitudes, Wishes, Needs Study ‐ Rubin
Needle Size often a BarrierSize DoesMatter
Use more short needles – 4 mm
Effective for pts with BMI of 24‐ 49
Keeps it subq
If pt thin, inject at angle
To avoid leakage, count to 10 before withdrawing needle
½ the patients who could benefit from insulin are not using it due to needle phobias

Page 3Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Poll question 2. What best describes the role of bolus insulins?
a. cover carbs at meals and hyperglycemia
b. helps to lower fasting blood glucose
c. keeps overnight blood sugars under control
d. should be used during hypoglycemic episodes
Insulin(µU/mL)
Glucose(mg/dL)
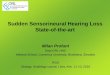
Physiologic Insulin Secretion: 24‐Hour Profile
150
100
50
07 8 9 10 11 12 1 2 3 4 5 6 7 8 9
A.M. P.M.
Basal Glucose
Time of Day
50
25
0 Basal Insulin
Breakfast Lunch Dinner
Bolus Insulin
Mealtime Glucose
Insulin Action Teams Bolus: lowers after meal glucose levels Rapid Acting Aspart, Lispro, Glulisine, Afrezza
Short Acting Regular
Basal: controls glucose between meals, hs Intermediate NPH
Long Acting Detemir (Levemir) Glargine (Lantus, Basaglar) Degludec (Tresiba)

Page 4Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Bolus Insulins(½ of total daily dose ÷ meals)
Name Onset Peak Action
Lispro (Humalog) 15‐30 min 1‐1.5 hrs
Aspart (NovoLog)
Glulisine (Apidra)
Afrezza (Inhaled)
Regular 30 mins 2‐4 hrs
Poll question
3. Which insulins are cheapest?a. Lantus, Levemir
b. Novolog, Humalog
c. Reg, NPH
d. Insulin pens
Cost Per Vial in Northern CA

Page 5Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Afrezza – Inhaled Insulin –Approved 2014 – Type 1 or 2
Only studied in adults over 18Not indicated for pregnancy, while breastfeeding
Steps, Cost, Terms Afrezza is regular human insulin in powder form using Technospheretechnology.
Pricing –similar pricing as pens ~ $300 a month
Referred to as TI in papers –“Technosphere Insulin”
Afrezza Dosing and Considerations Bolus regular insulin – inhaled before meals
Dosing: 4, 8 and 12 unit cartridges Convert with 1:1 ratio to existing insulin dose
Lung function test before start (FEV1) Not for pts w/ chronic lung issues
Asthma, COPD, history of lung cancer, smokers
Can cause acute bronchospasm – Black box warning
Side effects: Hypoglycemia, sore throat, cough
Less hypoglycemia than injected insulin

Page 6Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Afrezza Inhaler
Replace inhaler every 15 days –Do not wash
Bolus Insulin Summary
Regular, Novolog, Humalog, Apidra, Afrezza
Starts working fast (15‐30 mins)
Gets out fast (3‐6 hours)
Post meal BG reflects effectiveness
Should comprise about ½ total daily dose
Covers food or hyperglycemia.
1 unit Covers ≈ 10 ‐15 gms of carb
Lowers BG ≈ 30 – 50 points
Bolus Insulin Timing How is the effectiveness of bolus insulin determined? 2 hour post meal (if you can get it)
Before next meal blood glucose
Glucose goals (ADA) – may be modified by provider/pt 1‐2 hours post meal <180
Before next meal – 80 ‐ 130

Page 7Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Bolus – Insulin Sliding ScaleStarts at 150, 2 units for every 50 mg/dl >150
Basal Insulins(½ of total daily dose)
Intermediate Acting Peak Action Duration NPH 4‐12 hrs 12‐24
Long Acting Peak Action Duration Detemir (Levemir) No Peak 20 hrs Glargine (Lantus) 24 hrs Glargine (Basaglar) 24 hrs Degludec (Tresiba) 42 hrs
Fasting BG reflects efficacy of basal
Degludec and Basaglar Degludec (Tresiba) An ultra long acting insulin ‐ lasts
up to 42 hours
Takes 3‐4 days to reach steady state
Available in u‐100 and u‐200 pens
Seems to cause less hypo
Adjust dose every 3‐4 days
Wait at least 8 hours between doses
Good at room temp for 8 wks
Ryzodeg 70/30 mixture of insulin degludec and aspart

Page 8Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Basal Insulin Summary
NPH, Levemir, Glargine, Degludec
Covers in between meals, through night
Starts working slow (4 hours)
Stays in long (12‐24 hours) NPH 12 hrs
Levemir, Glargine 20‐24 hrs
Degludec – up to 42 hrs
Fasting blood glucose reflects effectiveness
Pattern Management
Poll Question 4. When looking at glucose patterns, which problem do you fix first?
a. hyperglycemia
b. hypoglycemia
c. non‐compliance
d. legible writing

Page 9Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Pattern Management Safety 1st!! ‐ Evaluate 3 day patterns
Hypo: eval 1st and fix: If possible, decrease medication dose
Timing of meals, exercise, medications
Hyperglycemia: evaluate 2nd Identify patterns
Before increase insulin, make sure not missing something (carbs, exercise, omission)
Type 2 – Amaryl 4mg AM, 10u Lantus pm
Case Study 70 yr old, avid walker
BMI 24, Weighs 60kg, creat 1.5
A1c – 9.8%, BG 250 – 300s during day
Insulin – 30 units Lantus (solostar pen)
Oral Meds: glipizide 20mg What medication changes?
What insulin changes?
Pt can’t afford insulin pen – what other option

Page 10Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Basal + 20 mg GlipizideType 2, 60kg – A1c 9.8%
Basal insulin key points – Type 2? ADA Standards of Care 2017 Start basal insulin at 10 units or 0.1 to 0.2 units/kg day
Keep metformin and sometimes one other oral agent
Consider NPH insulin at HS if cost is a factor
When is it too much basal insulin? If basal insulin is >0.5 units/kg day, advance to combination injectable therapy Add bolus, switch premixed 70/30 or to Basal + GLP‐RA
Maintain metformin therapy and stop other oral meds to decrease complexity.

Page 11Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Combo Sub‐Q Insulin
Case Study 70 yr old, avid walker
BMI 24, Weighs 60kg, creat 1.5
A1c – 9.8%, BG 300s for past weeks
30 units Lantus Pen (60kg x .5 = 30units max dose)
Oral Meds: glipizide 20mg What medication changes? Stop glipizide
What insulin changes? Try adding 1 bolus injection at largest meal, or switch to 70/30. 2/3s am, 1/3 pre dinner = 20units 70/30 am, 10 units 70/30 pre dinner
Pt can’t afford insulin pen – use vial and syringes

Page 12Diabetes Education Services© 1998-2017 www.DiabetesEd.net
20u 70/30 am, 10u 70/30 pmPatterns? Changes needed?
Basal Bolus – What Adjustments? Pt weighs 80kg
Poll Question
5. Which of the following are suggested insulin teaching keys? (multiple)
a. Test, inject, eat – TIE
b. abdomen is preferred injection site
c. use a sharps container to dispose of needles/lancets
d. always have treatment for hypo available

Page 13Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Intensive Diabetes Therapy
Insulin Dosing Strategy
50/50 Rule
0.5‐1.0 units/kg day
Basal = 50% of total Glargine QD
NPH or Detemir BID
Bolus = 50% of total
usually divided into 3 meals
Example
Wt 50kg x 0.5 = 25 units of insulin/day
Basal dose: 13 units
Glargine 13 units QD
Degludec 13 units QD
NPH/Detemir 6u BID
Bolus dose: 12 units
4 units NovoLog, ApidraHumalog, Regular each meal
Intensive Diabetes TherapyInsulin Dosing Strategy
50/50 Rule
0.5‐1.0 units/kg day
Basal = 50% of total Glargine QD
NPH or Detemir BID
Bolus = 50% of totalusually divided into 3 meals
Example – You Try Wt 60 kg x 0.5 = ___ units of insulin/day
Basal dose: ____ unitsGlargine ____ QDDeguldec ____ QDNPH/Detemir __ BID
Bolus dose: ____ units___units NovoLog, ApidraHumalog, Reg each meal
Intensive Diabetes TherapyInsulin Dosing Strategy
50/50 Rule
0.5‐1.0 units/kg day
Basal = 50% of total
Glargine QD
NPH or Detemir BID
Bolus = 50% of total
usually divided into 3 meals
Example – You Try Wt 60kg x 0.5 = 30 units of insulin/day
Basal dose: 15 unitsGlargine 15 QD orDegludec 15 QDNPH/Detemir 7u BID
Bolus dose: 15 units 5 NovoLog, Apidra, Humalog, Reg each meal

Page 14Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Basal Bolus – Using 50/50 Rule ‐ Ptweighs 80kg
Insulin Dosing Type 1 & 2
U-500 Insulin: When More With Less Yields Success: Diabetes Spectrum March 20, 2009 vol. 22 no. 2 116-122
More than 200 units a day?

Page 15Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Quick Question 6: What best describes U‐500 Regular Insulin?
a. Regular insulin delivered in 5xs the volume of U‐100
b. High potency inhaled insulin
c. Regular insulin that is 5xs the concentration of U‐100
d. Insulin that is given 5 times a day
Humulin Regular U‐500
Consider U‐500 High Potency Insulin
5 x’s the concentration of u100
500 units per mL vs 100 units per mL 20 mL a vial. 500 units per mL= 10,000 units/vial
Costs ~ $400 $1,200 per vial
Less volume

Page 16Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Dedicated U‐500 Insulin Syringe Manufactured by BD – Nov 2016
5 unit increments
No conversion required
If 85 units of U‐500 R Insulin is ordered…
Humulin R U‐500 Updated Package Insert
Patients using the U‐500 vial must be prescribed the U‐500 insulin syringe
Administer U‐500 two to three times daily 30 minutes before a meal
Don’t mix U‐500 with other insulins
Do not perform dose conversion when using U‐500 KwikPen or U‐500 Insulin syringe.
Do not transfer U‐500 from the KwikPen into any syringe.
All Concentrated InsulinsNo calculation required
All concentrated insulin pens and the U‐500 syringe automatically deliver the correct dose in less volume.
Pen comes in 5 unit increments
No conversion, calculations or adjustments required.For example, if order reads:“85 units Regular U-500 Insulin”Pull plunger to 85 units U-500 Insulin on the U-500 Syringe.Dial 85 units on the U-500 Pen

Page 17Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Dosing Strategies u‐500 Dosing – take total daily needs and split into 2‐3 doses
2 doses: 60% am / 40% pm or
3 doses: 40/30/30 or 40/40/20
No basal insulin needed, because U‐500 has bolus and basal action
Needs careful monitoring/ education
Example ‐ Pt on 240 units of insulin a day 140 units am / 100 units pm (2 doses)
100 / 70 / 70 or 100 / 100/ 40
Lispro (Humalog) U‐200 Kwik Pen 2 xs the concentration of U‐100
200 units per mL Humalog U‐200 Kwik Pen
Comes in 3mL pen/ 600 units (2 pack)
Once opened, keep at room temp. Toss after 28 days.
Not approved for use in insulin pump

Page 18Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Humalog 200 units/mL KwikPen
Toujeo U‐300 Solostar Pen
For example, if order reads:“30 units Toujeo U-300 Solostar Pen”
Dial the pen to 30 units.
Glargine (Toujeo) Solostar Pen U‐300 Glargine 300 units / mL Need 10‐14% higher dose than previous U‐100 dose
Start with 1:1 conversion and adjust based on FBG
Less nocturnal and hypoglycemia.
Similar weight gain to U‐100
Extend release of U‐300 results in smoother, stable more prolonged profile
More injection site reactions with U‐300
Max 80 units injection
Comes in 1.5mL pen/450 units (3 or 5 pack)
Once opened, keep at room temp. Toss after 42 days.

Page 19Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Degludec (Tresiba) FlexTouch U‐200 Pen
Concentration – 200 Units/mL
Max 160 units injection
Comes in 3mL pen/600 units (3 pack)
Dose increments – 2 units
Once opened, keep at room temp. Good for 8 weeks
For example, if order reads:“160 unitsTresiba U-200 FlexTouch Pen”
Dial the pen to 160 units.
Concentrated Insulin
Pros Cons
As pts are getting heavier, more insulin is needed
More insulin in less volume
Patients need less insulin ‐
Risk of incorrect administration
Cost
Making sure orders are written correctly
Quick Question 7: Which of the following is true about all concentrated insulins?
a. Need to convert to get correct dose
b. Delivers the same amount of insulin in more volume.
c. Delivers the correct dose in less volume
d. No calculation or conversion required
e. C & D

Page 20Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Key Teaching Points Never withdraw concentrated insulin from a pen into a syringe
All concentrated insulin pens and the U‐500 insulin syringe automatically deliver the correct dose in less volume.
No conversion, calculation or adjustment required.
When writing Rx include type of insulin, concentration, delivery device and dose.
Bolus insulin with meals
Basal 1‐2xs daily
Abdomen preferred injection site
Stay 1” away from previous site
Don’t re‐use ultra fine syringes
Keep unopened insulin in refrigerator
Toss opened insulin vial after 28 days
Proper disposal
Review patients ability to withdraw and inject.
Side effects include hypoglycemia/wt gain
Insulin pens – Prime needle to assure
accurate insulin dose given
Hold needle in for 5 seconds after injection
Roll 70/30 pens
Insulin Teaching Keys
Sharps Disposal: Product and Info Look in the Government section
white pages for a household hazardous waste listing for your city or county.
Call 1‐800‐CLEANUP (1‐800‐253‐2687)
Search for collection centers on the California Integrated Waste Management Board (CIWMB) Web site: http://www.ciwmb.ca.gov/HHW/HealthCare/Collection/

Page 21Diabetes Education Services© 1998-2017 www.DiabetesEd.net
Thank You Questions?
Email [email protected]
Web www.DiabetesEdUniversity.net







![Sequential Pattern Mining - DidaWiki [DidaWiki]didawiki.cli.di.unipi.it/.../dm/sequential_patterns_2018.pdf · 2018-02-22 · Generalized Sequential Pattern (GSP) Follows the same](https://img.pdfslide.us/doc/110x75/5f029f847e708231d4052fd3/sequential-pattern-mining-didawiki-didawiki-2018-02-22-generalized-sequential.jpg)



















