Embed Size (px)
Citation preview

Dizziness
“Coles Notes”
Dr. Rick Balys MD, FRCSC
Sue Ehler, BSC PT ; Steven MacNeil, BSC PT, RCA MPT

Faculty/Presenter Disclosure
Faculty: Dr. Rick Balys, FRCSC Otolaryngology
Relationships with commercial interests:
– Grants/Research Support: None
– Speakers Bureau/Honoraria: None
– Consulting Fees: None
– Other: None
CFPC CoI Templates: Slide 1

Disclosure of Commercial Support
None
Potential for conflict(s) of interest:
– None
CFPC CoI Templates: Slide 2

Objectives
Provide an approach to the dizzy patient
Help differentiate the most common forms
of dizziness and vertigo
Discuss when to refer and resources

Philosophy
Rule out the bad stuff
Treat the treatable stuff
Make patients feel better / compensate
Make sure patients don’t get worse (fall)

Method
1. Get them to describe it
2. Classify it
3. What is the timing and trajectory
4. Associated symptoms / signs

What do you mean…Dizzy?
Lightheaded
Faint
Off-Balance
Clumsy
Unable to concentrate
Weak
Leaning
Trouble focusing
Disorientated
Anxious
Floating
Confused
Shaky
Nauseous
Sweating
Fatigue/exhaustion
Spinning
Pulled to one side

The 4 Flavor’s of Dizzyness
1. Lightheaded / presyncopy
2. Disequilibrium (others notice)
A. Gait
B. Global
3. Vertigo
– The illusion of motion
4. Psychogenic / vague / disconnected /
floating (others don’t notice)

1. Presyncope “nearly blacking out”, “nearly fainting”
When you spin around, you might vomit but you never think you are about to pass out
lasts seconds to minutes – Medications
– Orthostatic hypotension
– Cardiac arrhythmias
– Vasovagal attacks
– Severe Anemia / Hypoglycemia
– Hyperventilation / Anxiety

2A. Gait Disequilibrium
Only when standing / walking
Fine when sitting - able to drive
Imbalance / Unsteady / Fall
Neurology / Neuromuscular Multisensory / Progressive disequilibrium of aging
Joints, spine
Cerebellar / movement disorders
Muscular disorders: PMR / MG / GBS / ALS

Progressive Dysequilibrium of
Aging - *** Fall Risk ***
Multisensory disorder:
1. peripheral neuropathy
2. visual impairment
3. musculoskeletal issues
4. vestibular disorder
5. central problems with integration
6. bunyons and improper footwear
7. general weakness
Medications, especially antidepressants,
benzo’s and anticholinergics

Progressive Dysequilibrium of
Aging - *** Fall Risk ***
Slowly get more rickety
Reach a tipping point:
– New drug
– New joint
– New injury
– New environment
– New illness, usually with weight loss
– BPPV

2B. Global Disequilibrium
Symptoms even when sitting
– Unable to drive
– May be central or peripheral vestibular
– Look for ataxia

3. Vertigo…The Illusion of Motion
Never “all the time”
Worse with head movement
Often associated with N/V, Sweating, Pale
There is usually nystagmus
Rotating, tilt, rock, bounce, floor drops

4. Psychogenic
Spacey / Disconnected / Watching world
on TV
Stress, Anxiety, Sleep issues, Medications
(including caffeine)
Possibly Migraine “a global distortion of
sensory perception”
Chronic Subjective Dizziness
– Persistent activation of the Threat State
– MOST COMMON FORM IN PTS < 40

Method
1. Get them to describe it
2. Classify it
3. What is the timing and trajectory
4. Associated symptoms / signs

Timing (of Vertigo) is Everything
Seconds – Minutes
– BPPV
Minutes to Hours
– Migraine or Meniere’s
– CNS (VBI, TIA brainstem or labyrinth)
Days
– Vestibular Neuronitis
– Cerebellar CVA, Lateral Medullary syndrome, MS
Chronic continuous…Psychogenic, Migraine,
CSD, Post-concussion, Chronic pain

Associated Symptoms “You can get to know a person by looking at
who their friends are”
CNS: PD3, Weak, Numb, Ataxia
Meniere’s: Single sided fullness/pressure, Tinnitus, Fluctuating hearing loss
Migraine: Aura, SS Pounding Headache, Photo/phonophobia – Motion sickness, Family History, Menstruation related H/S
Anxiety: SOB, Palpitations, Hyperventilation
With noise or exertion: PLF, SCDS, Meniere’s, Syphilis


BPPV
Episodes of true, often violent spinning
Brief <1min but often followed by N/V
When you think your dying, a minute is an eternity
No hearing change, no tinnitus, no pressure
Occurs in 10%, responsible for about 50% of
Vertigo in Elderly

BPPV – What is Provocative?
1. Rolling in bed (which side?)
2. Looking up and to one direction (grocery store, lightbulb)
3. Putting your head between your legs
Still feel ‘off’ between events
Can last for days to years
but you can take it away instantly!

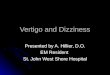
BPPV Pathophysiology
Otoconia (CaCO3) from the Utricle gets
loose and gets trapped in the posterior
canal (usually)
Where is the posterior
Canal???

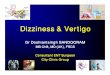
BPPV – the Dix Hallpike
The Provocative Position: Head slightly extended
and turned 45o
1. Usually a brief delay
2. Rotatory geotropic nystagmus with a vertical
component (in the plane of the PSSC)
3. Lasts 10 sec to 1 min
4. Vertigo returns but nystagmus less
pronounced on return to upright
5. Fatigable

BPPV – the Dix Hallpike
(Also the first position of Epley)

Meniere’s Disease
One Sided Ear Symptoms!
1. CONTINUOUS Vertigo lasting minutes to hours (can have a few days of fatigue)
2. Fluctuating Unilateral SNHL
3. Unilateral Tinnitus
– Usually low pitch
– Can intensify before an attack
4. Unilateral pressure / fullness

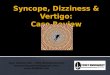
Meniere’s / Endolymphatic Hydrops

Meniere’s Treatment
Low salt diet (<1500mg/d)
Avoid caffeine, cola, nicotine, alcohol, chocolate
HCTZ
Serc (8-24mg TID)
Tympanostomy tube
Intratympanic steroids
Intratympanic gent

Migraine & Vertigo
15x more common than Meniere’s(Rauch)
Problem with brain chemistry – dysfunction of sensory signal processing
Migrainous vertigo: – 2 episodes of vertigo concurrent with migraine
features (H/A, PP, PP, Aura)
Migraine-associated vertigo: – Episodic vertigo in a pt with migraine disorder (HIS
criteria)
Mimics Meniere’s but no hearing loss
Motion Sensitivity

Migraine Associated Vertigo
Treatment
Avoid triggers
– Stress change, caffeine change, weather change, hormone change.
– Dietary triggers
TCA, B-Blocker, CCB, Topiramate,SSRI’s
Manage flare ups

Vestibular Neuronitis
Constant Vertigo x Days
– Usually with nausea, vomiting, and nystagmus
– Often a URTI within 2 wks before event
No other neurological or audiological symptoms
Horizontal and slight torsional nystagmus
COWS (fixed direction) and Alexander’s Law
Fixation suppression, worse with head
movement

Vestibular Neuronitis
Ensure hearing is not involved
Vertigo stops in days
– Use Vestibular suppressants for 5 days tops
Imbalance persists for weeks
Expect full recovery
Can be followed by BPPV
Rarely recurrent (recurrent vestibulopathy)

Central Nystagmus
Can be purely vertical, purely horizontal
Can change in direction with gaze change
(bidirectional)
No fixation suppression
No significant change with head motion
Doesn’t stop (BPPV)
Not fatigable
Other neurological findings

Red Flags - Image
Neck injuries / Head injuries
Hx of Significant Ear disease / surgery / trauma
Unexplained Neurolgical Findings
Exam findings – Vertical nystagmus, direction changing, not following the rules
– Horners
CVA RF – Advanced age
– Previous TIA / CVA / CAD
– Hypertension
– DM
– Hypercholesterolemia
– Smoking
– Atrial fibrillation

Exam
Otoscopy
Gait – Ataxic, Staggering, Wide based gait
Nystagmus
CN testing, Horner’s
Cerebellar testing – Finger nose
– RAM
– Toe tapping and Heel shin
Romberg testing – With distraction
Stepping Test – With distraction
Dix Hallpike

Cheat Sheet Describe it
Classify it:
1. Lightheaded
2. Vertigo
3. Gait vs Global dysequilibrium
4. ‘Spacey’
Timing
– Min: BPPV
– Hours: Migraine, Meniere’s (ss ear sx), VBI
– Days: Vestibular neuronitis, MS, VBI/CVA
– Weeks: ?anxiety
Associated symptoms
– Focal neurological
– Single side tinnitus, pressure and hearing loss
– Motion sickness, photophobia, phonophobia, headache
– SOB, palpitations, anxiety

When To Refer
Red Flags
Suspected Central Cause
Not responding / Symptoms progressing
Associated hearing loss
Deteriorating quality of life

Who to refer to?
Audiology (hearing assessment)
Radiology (head and temporal bones)
Physiotherapy “specialists”
– Atlantic Balance and Dizziness Centre
– Vest Rehab Adv Comp (Emmory)
ENT
Neurology

If all else fails….

Meniere’s Natural History
Exacerbations and remissions
Within 10 years most patients are in
remission
– Often with a 50dB hearing loss
10-50% can get bilateral disease