Embed Size (px)
Citation preview
DizzinessandVer,go
InvernessCPD–August31,2018DrBlairWilliamsMDFRCSC
Otolaryngology–head&necksurgery

DisclosureSlide
• Thisspeakerhasbeenaskedtodisclosetotheaudienceanyinvolvementwithindustryorotherorganiza,onsthatmaypoten,allyinfluencethepresenta,onofanyeduca,onalmaterial.
• Receivingevalua,onsiscri,caltotheaccredita,onprocess.– ARertheprogram,pleaseprovidefeedbackathSps://surveys.dal.ca/opinio/s?s=44738
Abitaboutme…
• FromBarney’sRiverSta,on,NS
• Medical/surgicaltrainingatDalhousieUniversity
• Startedprac,ceinSydneyinJuly2017• IhaveaninterestandafellowshipinHeadandNeckOncology– Skincancer,thyroid,paro,d,throat,oral– AlsoofferBotox(medicalandcosme,c)

Objec,ves–DizzinessandVer,go
• Todifferen,atever,gofromothertypesofdizziness
• Todeterminewhetherver,goisofcentralorperipheralorigin
• Todescribethepresenta,onandtreatmentofperipheralves,bularcondi,ons

Dizziness
• Thisisanon-specificterm,oRenusedbypa,entsthatcouldmeananynumberofsymptoms– Lightheadedness– Presyncope– Ver,go– Ataxia– Unsteadiness– Dysequilibrium
• Amorespecificterm/descrip,onwillhelpguidetreatment,inves,ga,on,andappropriatereferrals

TrueSpinning
Ves$bulare$ology
Toandfrorocking
Lightheadedness Ataxia
Dizziness

Balance
Visual
Propriocept
Soma,csensa,on
Ves,bular
Sensory
Input
BrainstemCerebellumCortex
SensoryIntegra$on
Muscletone
BalanceOutput
Dizziness–Ves,bularornot?
Vesitbular• Ver,go• Episodic• Vomi,ng
• OtologicSymptoms• Worsewithheadmovement
Other• Lightheadedness• Chronicdisequilibrium• Cardiacsymptoms
• Neurologicsymptoms• LossofConsciousness

Ver,go
• Thesensa,onofmovementintheabsenceofmovement– Mostcommonlyspinning
• Typicallyves,bularinorigin–innerear,CNVIII,brainstemnuclei

SemicircularCanalPhysiology

Push/PullSystem

FiringRate
0
RightHC
LeRHC
Differen,alisDrivingVOR
Push/PullSystem
Ver,go
• Thesensa,onofmovementintheabsenceofmovement– Mostcommonlyspinning
• Typicallyves,bularinorigin–innerear,CNVIII,brainstemnuclei
• Historyisthekeytodiagnosis– Featuresofthesensa,on– Timingoftheepisodes– Associatedsymptoms– Triggers

Ver,goDifferen,al
Timing HearingPreserved HearingLoss
Seconds-Minutes BPPV
Minutes-Hours Ves,bularMigraine Meniere’sDisease
Days Ves,bularNeuri,s Labyrinthi,s

FeaturesSugges,ngCentralVer,go
• Five“D’s”– Dysarthria– Dysphagia– Dysmetria– Diplopia– Downbea,ngorDirec,onchangingnystagmus
• Hemifacialorhemibodysensoryormotordeficit
• DropaSacks,visualloss,confusion
Unlikelyperipheralwiththesefeatures!

AcuteVer,go–CentralvsPeripheral

HINTSStudyKaSahetal,2009.Stroke.
• AcuteVer,goPresenta,on– N=101,25ves,bularand76central
• Bedsideexamandimagingforeveryone
• AnormalHINTStestcorrectlyruledoutstrokeat96%,superiortoMRIwithDWI(12%falsenega,ve)

HINTSExam
AbsenceofALLofthesefeatures(IN-FA-RCT)essen,allyrulesoutacentrale,ology

PERIPHERALVESTIBULARCONDITIONS

SECONDSTOMINUTES-BPPV

BenignParoxysmalPosi,onalVer,go
• Mostcommoncauseofver,go(90%)– Alsothebest:oRencanbecuredintheoffice!• Nomeds,noscans
• Brief,intenseepisodes– Rollingover,,tlingheadback,etc

BPPV
• Looseotoconiainsemi-circularcanals– Con,nueds,mula,onaRerheadmovementstops
• Diagnosedbymovingtheotoconia
• Treatedbyguidingtheotoconiatotheutricle
BPPV–PosteriorCanal
! DixHallpike(Diagnosis)
BPPV–PosteriorCanal
! Epley(Reposi,oning)

BPPV–LateralCanal
! RollTest(Diagnos,c) ! BarbecueRoll(Reposi,oning)

BPPV–HomeExercises
• Thoughttoworkthroughhabitua,onratherthanreposi,oning– Repeat10-20xpersession– Upto3xperday
• Minimalevidencetosupport– Highrateofspontaneousresolu,oninBPPV
• Stopwhensymptomsresolve– Doesnotpreventrecurrence
hSps://www.uptodate.com/contents/images/NEURO/63738/Brandt_Daroff_maneuver.jpg
! Brandt-Daroff
hSps://www.uptodate.com/contents/images/NEURO/63738/Brandt_Daroff_maneuver.jpg

BPPVSummary
• Freepar,clesinthesemicircularcanals• Diagnosisandtreatmentatbedside– Noneedforimaging
– Noneedformeds
• Lowthresholdtotrythemaneuvers
• Physiotherapiststrainedinves,bularrehabarereallygoodatthis!

MINUTESTOHOURS:MENIERE’S&MIGRAINE
Meniere’sDisease
• Episodicver,go(20minutestohours)– Transienthearingloss,,nnitus,auralfullnesswiththever,go– Typicallyunilateral
• Thoughttoarisefromendolympha,chydrops– S,llpoorlyunderstooddespitebeingdescribed>150yearsago
• Treatmentaimstopreventdistensionoftheendolympha,csac

Meniere’sDisease
• HearinglossfluctuateswithepisodesBUTtheretendstobesomebaselinelossover,me

Meniere’sDisease
• Betahis,ne(betahis,ne)istypicallyfirstline:– Innerearvasodila,onwhichhelpsprevent/relievethehydrops– Notgivenrou,nelyforanythingbutMeniere’s– Worksbestasapreven,vemedica,on,notPRN– Startaslowas8mgTID,safeinhigherdosesifincompletesymptomscontrol
• Thiazidediure,cs,lowsodiumdiet,avoidtriggers
• Proceduraltreatments,iffailureofmedicalmanagement

Meniere’sDiseaseSummary
• Episodicver,golas,nghours• Prominent,transientunilateralauralsymptoms– Hearingloss,,nnitus,fullness
• Audiogramhelpfulindiagnosis
• Treatmentsaddressendolympha,chydrops
• Regularbetahis,nedosingfirstlinebutlimitedevidenceforanytreatment

Ves,bularMigraine
• Rela,velynewdiagnosis(~20years)• Truever,go,typicallylas,nghours– Imbalance,mo,onintol,boat-likerocking– Visualtriggers–movingscenes,traffic,etc
• Similartriggerstoothermigraine– Sleepdepriva,on,stress,hormonalchanges
– Canoccurseveral,mesperyearorasfrequentlyasdaily

Ves,bularMigraine
• Typicalmigraineheadache– Doesnothavetooccurwithver,goepisodes– Canprecedever,gobyyears
• 1+non-headachesymptom– Photophobia,phonophobia,aura– Auralsymptomsuncommon
• MorecommonthanMeniere’s– Someoverlapexists
– Canbedifficulttodifferen,ate
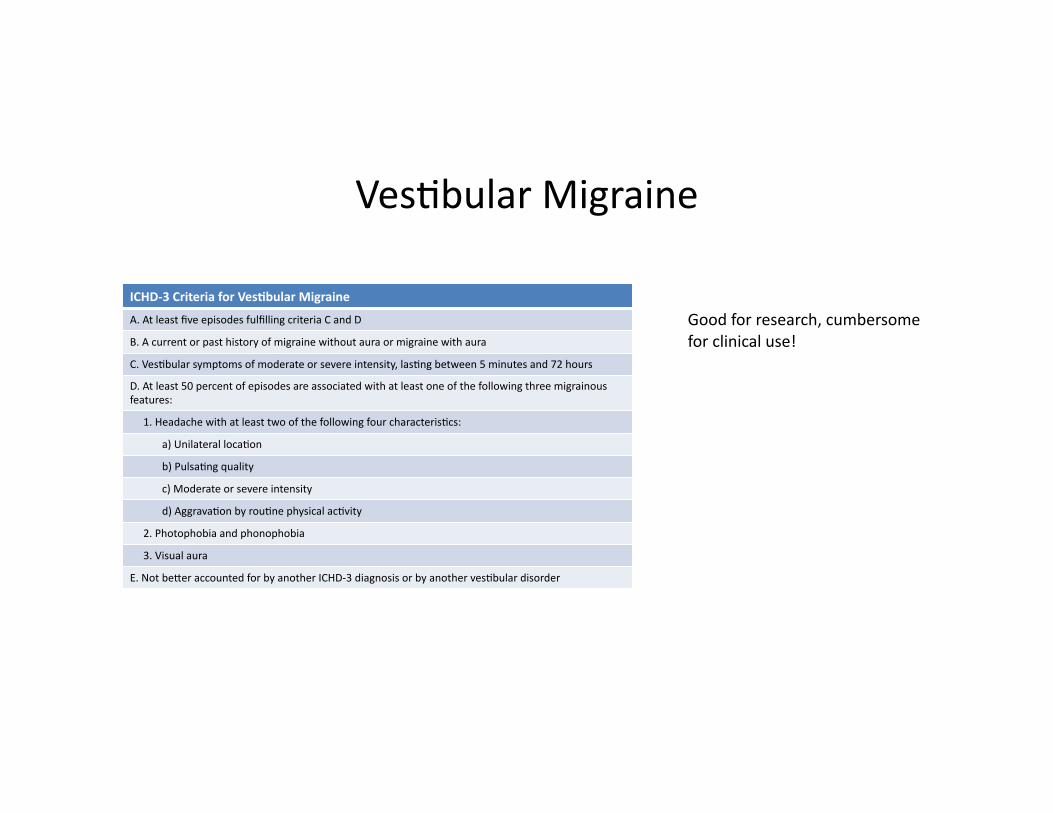
Ves,bularMigraine
ICHD-3CriteriaforVes$bularMigraine
A.AtleastfiveepisodesfulfillingcriteriaCandD
B.Acurrentorpasthistoryofmigrainewithoutauraormigrainewithaura
C.Ves,bularsymptomsofmoderateorsevereintensity,las,ngbetween5minutesand72hours
D.Atleast50percentofepisodesareassociatedwithatleastoneofthefollowingthreemigrainousfeatures:
1.Headachewithatleasttwoofthefollowingfourcharacteris,cs:
a)Unilateralloca,on
b)Pulsa,ngquality
c)Moderateorsevereintensity
d)Aggrava,onbyrou,nephysicalac,vity
2.Photophobiaandphonophobia
3.Visualaura
E.NotbeSeraccountedforbyanotherICHD-3diagnosisorbyanotherves,bulardisorder
Goodforresearch,cumbersomeforclinicaluse!

Ves,bularMigraine
• Treatment– LiSleavailabledata(caseseriesandretrospec,vestudies)
• Currentapproachbasedonothermigrainevariants
– Lifestyle• Adequaterest,exercise,diet• Avoidknowntriggers
– Triptansasanabor,vetherapy– Preven,on
• Considerfrequency,dura,on,severityofaSacks• Venlafaxine37.5mgdaily• TCAs,CCBs(flunarizine)
Ves,bularMigraineSummary
• Suspectifnoassociatedauralsymptoms• Historyofmigrainecommon
• Prominentvisualsymptoms
• ORenexhibitsaura,photo/phonophobia• Typicalmigrainetriggers–avoidance!
• Treatasmigraine–triptansifinfrequent,prophylacitcmedsiffrequentandsevere

LASTINGDAYS–VESTIBULARNEURITIS

Ves,bularNeuri,s
• Acuteonsetofsevere,unrelen,ngver,go– Nystagmus,ataxia,nausea/vomi,ng,intoleranceofheadmovement
• Uncleare,ology– Neurotrophicvirus– Inflammatory,microcirculatory
• +/-hearingloss(termed‘labyrinthi,s’ifunilateralSNHL)
Ves,bularNeuri,s
• Selflimi,ng– Ruleoutischemicevent
– Variablerecoveryinves,bularfunc,on• Suppor,vemeasuresforfirstfewdays– Steroids,an,-eme,cs,benzos
• Avoidlong-termbedrestandsuppressants– Delaysadapta,ontonewlevelofves,bularinput

AcuteTreatmentofVes,bularNeuri,s
• Shorttermuseonly– 3-5days
• Prolongedusewilldelaycompensa,on
• Noestablishedroleforbetahis,ne
hSps://www.uptodate.com/contents/ves,bular-neuri,s-and-labyrinthi,s?topicRef=5097&source=see_link#H9
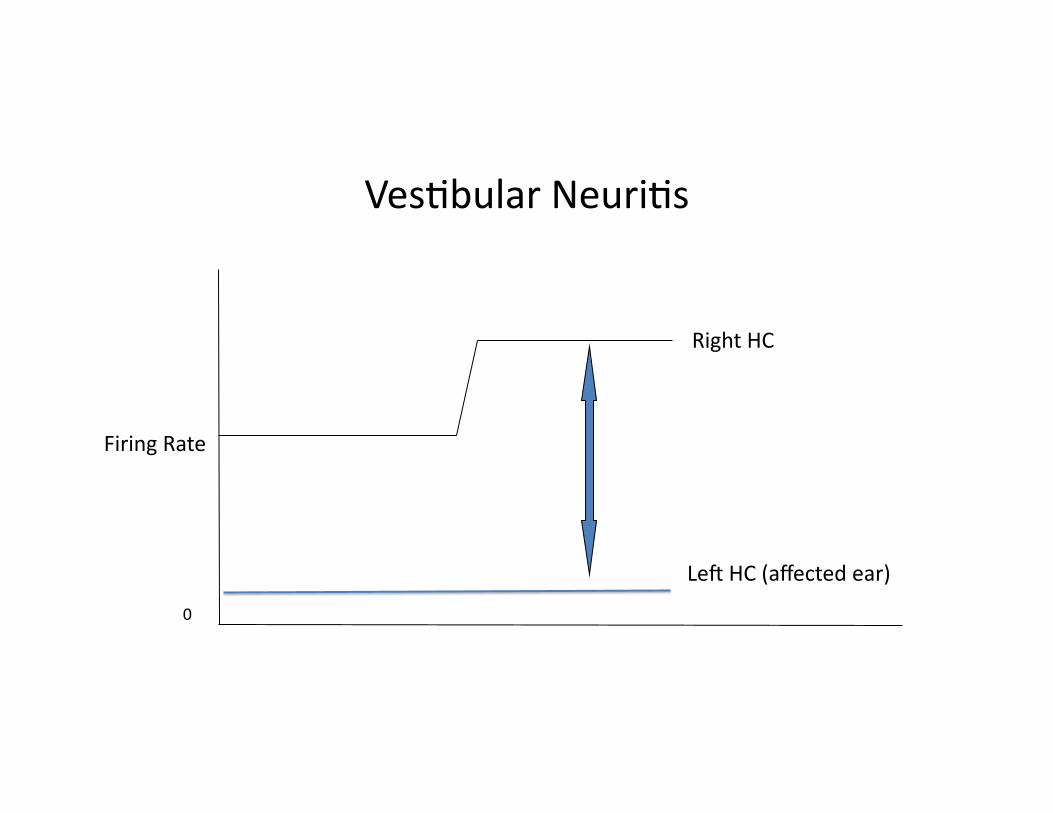
FiringRate
0
RightHC
LeRHC(affectedear)
Ves,bularNeuri,s

DizzinessSummary
• Ver,goversusothercause• Ifver,go,centralvsperipheral(innerear)• Ifperipheral,limitednumberofcauses– Timingiskey– Associatedsymptomshelp– Tailortreatmenttothemostlikelycause
– Ifineffec,ve,reassessdiagnosisandtrysomethingelse

RealityCheck
• Itsnicetohavelabelsbut…– SooRenpa,entdon’tfitnicelyintooneofthesecategories– Symptomsarevagueorthereareelementsofmul,plecondi,ons
• Videonystagmography(VNG)canhelp– Peripheralvscentrale,ology– AvailablethroughNSHearingandSpeech
• Ves,bularrehabilita,oncanhelpmostpeopleregardlessofe,ology– Visionstability,posturetraining,strengthening

KeyMessages
• Ruleoutcentralcause• BPPVismostcommon–noneedforRxorscan• Betahis,neshouldbereservedasfirstlinemedforsuspectedMeniere’sDisease
• Ves,bularmigraineismorecommonthanMeniere’ssosuspec,ngthisandtrea,ngasmigrainecandoalotofgood!
• Compensa,oniskeyinVes,bularneuri,s,solimitsuppressivemedica,ontoseveraldaysdura,on

Thankyou
• ThankyouforyouraSen,onandyourreferrals• Iwelcomeyourfeedback
• Manyimagesarecopyrightedandcannotbeposted–Icansendbyemailifyouwantthefullpresenta,on– [email protected]
Sources
• CummingsOtolaryngology–Head&NeckSurgery6thEdi,on
• UpToDate.com
• Dizziness-and-balance.com
• Evalua,onandTreatmentofDizzyPa,ent-HalifaxOtolaryngologyReviewCourse