Embed Size (px)
Citation preview

Divisions of Critical Care Medicine*, Pulmonology¶, Department of Pediatrics#, and Department of Pathology§, Advocate Lutheran General Children’s Hospital. Pediatric Pulmonary Unit and Dept of Pediatrics, Massachusetts General Hospital. ∆
Department of Pediatrics, Harvard Medical School ǂ
Divisions of Critical Care Medicine*, Pulmonology¶, Department of Pediatrics#, and Department of Pathology§, Advocate Lutheran General Children’s Hospital. Pediatric Pulmonary Unit and Dept of Pediatrics, Massachusetts General Hospital. ∆
Department of Pediatrics, Harvard Medical School ǂ
References:
Discussion
Clinical Course
Patient Description
There is currently no specific treatment for CAP or any other pattern of ChILD caused by ABCA3 mutations. The only evidence-based treatment of CAP is lung transplantation.
This is the first report of successful use of hydroxychloroquine in a patient specifically with an ABCA3 mutation. Success with hydroxychloroquine has previously been reported in a closely-related pathology secondary to surfactant protein C mutation. 1
In the past, before the genetic bases of the gamut of ChILD had been elucidated, the use of hydroxychloroquine was also occasionally successful. It is possible that some of these diseases were secondary to ABCA3 mutations.
Further study is needed to assess the mechanism of action (which is unknown, but thought to be related to anti-inflammatory effects on toxic mediators released as a result of misfolded proteins), and usefulness of hydroxychloroquine in the treatment of surfactant protein disorders.
The patient was transferred to the pediatric ICU due to worsening respiratory distress, and ultimately required high-frequency oscillatory ventilation with FiO2 of 100%.
Her chest x-rays showed worsening infiltrates, and after chest CT raised suspicion for interstitial lung disease (figure 3), she underwent a lung biopsy which was consistent with CAP (figure 1), and genetic testing was positive for an ABCA3 mutation.
The family decided against lung transplantation; therefore, high-dose hydroxychloroquine was initiated empirically given anecdotal success in interstitial lung disease of childhood (ChILD). Within days of starting treatment, her pulmonary compliance significantly improved corresponding to airspace clearing on chest imaging (figures 2-3), and she was weaned to conventional ventilation at minimal settings.
Congenital alveolar proteinosis (CAP) is a rare condition characterized by accumulation of lipoproteinaceous material within alveoli (see figure 1), often resulting from genetic defects in surfactant metabolism. ATP-binding cassette transporter A3 (ABCA3) gene mutations are a usually fatal form of surfactant deficiency in infants for which treatment options are few and often futile. We report the first successful use of hydroxychloroquine in the treatment of an infant with CAP due to an ABCA3 mutation.
ABCA3 is a transmembrane protein, highly expressed in type II alveolar cells at the limiting membrane of lamellar bodies, and is thought to be involved in surfactant lipid transport into lamellar bodies.
Successful Treatment of ABCA3 Mutation Associated Congenital Pulmonary Alveolar Proteinosis with High-Dose Hydroxychloroquine
E Swanson, DO#; T Kinane, MD∆; L Yonkers, MDǂ; R Sirota, MD§; G Aljadeff, MD¶; M Tsifansky, MD*
Introduction
A 3 month old full term female with history of mild laryngomalacia, born to consanguineous parents, was hospitalized with persistent cough, respiratory distress, and failure to thrive.
An extensive initial workup was negative with the exception of bilateral infiltrates on repeat chest x-ray.
1. Rosen DM, Waltz DA. Hydroxychloroquine and surfactant protein c deficiency. NEJM 2005; 352 (2): 207-208
2. Nogee LM. Genetics of pediatric interstitial lung disease. Curr Opin Pediatr 2006;18: 287-292.
3. Clement A, Eber E. Interstitial lung disease in infants and children. Eur Respir J 2008; 31: 658-666.
4. Wert SE, Whitsett JA, Nogee LM. Genetic disorders of surfactant dysfunction. Pediatr Dev Pathol 2009; 12 (4): 253-274
5. Deterding R, Fn LL. Surfactant dysfunction mutations in children’s interstitial lung disease and beyond. Am J Respir Crit Care Med 2005; 172: 940-941.
6. Shulenin S, Nogee LM, Annilo T et. al. ABCA3 gene mutations in newborns with fatal sufactant defiiency. N Engl J Med 2004; 350: 1296-1303.
7. Bullard JE, Wert SE, et al. ABCA3 mutations associated with pediatric interstitial ung disease. Am J Respir Crit Care Med 2005; 172: 1026-1031.
8. Dinwiddie R. Treatment of interstitial lung disease in children Paediatr Respir Rev 2004; 5: 108-115.
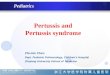
Figure 1: Congenital Alveolar Proteinosis. Panel A shows the milky white appearance of our patient’s BAL fluid, consistent with CAP. Panels B and C show the histopathology from thorascopic - assisted wedge lung biopsy with diffuse alveolar filling by PAS positive amorphous proteinaceous material and degenerating foamy macrophages.
Figure 3: Chest CT before (left) and one month after (right) initiation of hydroxychloroquine, showing improvement in diffuse opacity of lungs.
Figure 2: Chest radiographs before (left) and 3 days after (right) hydroxychloroquine initiation, showing diffuse clearing of airspace consolidation.
A B C
Her improvement was not sustained, however, and after 7 weeks of improvement on hydroxychloroquine, she had respiratory deterioration from which she could not recover.