Embed Size (px)
Citation preview

Division of Workers’ Compensation
Wednesday, August 24, 2016

Regulatory and Legislative Update
Andrew Sabolic
Assistant Director

2016 Legislative Update
Highlights of House Bill 613 –effective 10/1/16:
•25 percent penalty credit for certain employers;
•Establishing a deadline for employers to file certain documentation to receive a penalty reduction;
•Reducing the imputed payroll multiplier from 2 times to 1.5 times the statewide average weekly wage;
•Relieving employers of the obligation to notify the DFS by telephone or telegraph within 24 hours of any work related death
3

2016 Legislative Update
Highlights of House Bill 613 –effective 10/1/16:
•Removing insurers and employers from the medical reimbursement dispute provision since they meet their adjustment, disallowance and provider violation reporting duties through other provisions of law;
•Eliminating fees collected by the DFS related to new insurer registrations and Special Disability Trust Fund notices of claim and proofs of claim;
•Revising the method for certifying an expert medical examiner;
•Eliminating the Preferred Worker Program
4

2016 Legislative Update
SB 1402 – 2015 Health Care Provider Reimbursement Manual
• Legislative ratification of the manual
• New maximum reimbursement allowances are based upon 2014 Medicare rates
• 1.8% increase in costs
• Became effective on July 1, 2016
5

What to expect during the 2017 Legislative Session?
• Legislation to ONLY address the unconstitutionality of the attorney fee cap and the duration temporary total disability benefit
OR
• Comprehensive legislation to address other system cost drivers and administrative efficiencies
OR
• Do nothing and wait until the 2018 session
6

Activities and Initiatives
• 2017 Three-Member Panel Biennial Report
• Insurer Regulatory Report
• WCATF & SDTF Assessment Rates
• Check Cashing Store Database Results
• Mini-MAP
• Investigator’s Observations for Underwriting (IOU)
7

Determine your performance among your peers

Audit Data

EAO Data

Financial Accountability Data

Data Quality & Collection


Activities and Initiatives
• 2017 Three-Member Panel Biennial Report
• Insurer Regulatory Report
• WCATF & SDTF Assessment Rates
• Check Cashing Store Database Results
• Mini-MAP
• Investigator’s Observations for Underwriting (IOU)
14

Emerging Issues
• Compound drugs
• Timeliness of medical authorization
• Proper application of contracts for health care provider payments
• Analysis of “outlier” health care provider bills
15

Questions

Policy in the Workers’ Compensation Medical Arena
Theresa Pugh
Program Administrator
Medical Services Section

Discussion Topics
69L-7 Rule Series: Workers’ Compensation Medical Reimbursement and Utilization Review (AKA the Billing Rule)
69L-8 Rule Series: Selected Materials Incorporated by Reference
69L-7.100: Reimbursement Manual for Ambulatory Surgical Centers
69L-7.020: Healthcare Provider Reimbursement Manual
69L-7.501: Reimbursement Manual for Hospitals
69L-30: Expert Medical Advisors
69L-31: Utilization and Reimbursement Dispute Rule
69L-34: Carrier Report of Health Care Provider Violations

Workers’ Compensation Medical Reimbursement and Utilization Review, 69L-7 Rule Series
Adopted and went into effect on February 18, 2016
Substantial rewrite and reorganization of existing Rule 69L-7.710, F.A.C. (aka the Billing Rule)
Five separate rules• 69L-7.710: Definitions
• 69L-7.720: Forms Incorporated by Reference
• 69L-7.730: Health Care Medical Billing and Reporting Responsibilities
• 69L-7.740: Insurer Authorization and Medical Bill Review Responsibilities
• 69L-7.750: Insurer Electronic Medical Report Filing to the Division

Rewrite of 69L-7.710, F.A.C. (aka the Billing Rule)
Effective February 18, 2016
69L-7.710: Definitions
69L-7.720: Forms Incorporated
by Reference
69L-7.730: Health Care Medical Billing
and Reporting Responsibilities
69L-7.740: Insurer Authorization
and Medical Bill Review Responsibilities
69L-7.750: Insurer Electronic Medical Report Filing to the Division
69L-7
7.710
7.720
7.7307.740
7.750

Workers’ Compensation Medical Reimbursement and Utilization Review, 69L-7 Rule Series
Summary of changes:
• Incorporates Revision F
• Allows for the use of revised national billing forms
• Establishes the use of ICD-10 Coding
• Contains billing instructions for dispensing repackaged medication
• Updates EOBR codes
• Updates definitions

Adopted and went into effect on February 18, 2016
Reorganizes incorporated reference materials used in conjunction with DWC medical reimbursement manuals and throughout the medical billing rule
Selected Materials Incorporated by Reference, 69L-8 Rule Series

Selected Materials Incorporated by Reference, 69L-8 Rule Series
Rule Chapter 69L-8 contains the following:
• 69L-8.071: Materials for use with the Florida Workers’ Compensation Health Care Provider Reimbursement Manual
• 69L-8.072: Materials for use with the Florida Workers’ Compensation Reimbursement Manual for Ambulatory Surgical Centers
• 69L-8.073: Materials for use with the Florida Workers’ Compensation Hospital Reimbursement Manual
• 69L-8.074: Materials for use throughout Rule Chapter 69L-7, F.A.C.

Reimbursement Manual for Ambulatory Surgical Centers, 2015 Edition,
Rule 69L-7.100, F.A.C. Effective 1/1/2016
Adopted September 28, 2015 & based on date of service
Increased the Number of MRAs to 90
Clarified surgical implant policy
Prohibited multiple surgery reduction
Reduced reimbursement from 70% of the billed charge to 60% of the billed charge if the procedure is not listed in the fee schedule and a contract does not apply

Workshop held July 28, 2016
• Will require legislative ratification
• Incorporates updated schedule of MRAs
• Includes 81 MRAs
• General reimbursement remains:
The MRA, or
60% of billed charge if procedure not listed in schedule, or
An agreed upon contract price
Reimbursement Manual for Ambulatory Surgical Centers, 2016 Edition ,
Rule 69L-7.100, F.A.C.

Healthcare Provider Reimbursement Manual, 2015 Edition, Rule 69L-7.020, F.A.C.
Adopted July 2015
Ratified during 2016 legislative session
Effective July 1, 2016
• (based on date of service)
Incorporated 2014 Medicare Relative Value Units (RVUs)

Healthcare Provider Reimbursement Manual, 2016 Edition, Rule 69L-7.020, F.A.C.
Workshop held July 28, 2016
Updates MRAs to incorporate 2016 Medicare Relative Value Units (RVUs)
Will not require ratification

Hospital Reimbursement Manual, 2014 Edition, Rule 69L-7.501, F.A.C.
Effective January 1, 2015
• (based on date of service or date of discharge for admissions)
Increased Stop-Loss Reimbursement threshold
Increased per-diem rates
Established Outpatient Base Rates
Established Geographic Modifiers

Hospital Reimbursement Manual, 2016 Edition, Rule 69L-7.501, F.A.C.
Workshop held July 28, 2016
Increases Stop-Loss Reimbursement threshold to $65,587.00
Increases per-diem rates• Inpatient trauma:
– Surgical - $4,216.00 Non-Surgical - $2,534.00
• Inpatient acute care:– Surgical - $4,215.00 Non-Surgical - $2,501.00
Updates Outpatient Base Rates
Updates Geographic Modifiers

Expert Medical Advisors, Rule 69L-30, F.A.C.
Effective March 1, 2016
Introduced the online certification and educational tutorial
Simplified the qualifications for becoming a certified Expert Medical Advisor
Increased reimbursement fees for EMA services
Established reimbursement fees for ancillary EMA services
Anticipate updating to reflect statutory change –effective 10/1/2016

Expert Medical Advisors
About 140 Expert Medical Advisors
We need EMAs in the following specialties• Internal Medicine
• Neurology and Psychiatry
• Pain Management
• Anesthesiology
Eligible for use by DWC or JCC to resolve disputed appropriateness of medical care and treatment issues
Florida DWC EMA Website: https://msuwebportal.fldfs.com/

Expert Medical Advisors Web Portal

Utilization and Reimbursement Dispute Rule, Rule 69L-31, F.A.C.
First workshop held January 12, 2016
Second workshop held June 10, 2016
Summary of changes:
• Relaxes requirements for notices of disallowance or adjustment of payment require to file a petition
• Notice of Deficiencies will remain
• Reflects the statutory change to 45 days for filing reimbursement dispute petitions and 30 days for filing carrier response to petitions
• Clarifies contract review in determination process

Carrier Report of Health Care Provider (HCP) Violations, Rule Chapter 69L-34, F.A.C.
General Violation types:• Improper Billing of Services
• Improper Reporting of Services
• Improper Form Completion
• Standard of Care Violation, including overutilization
Referral Submission Types• Manual- Form DFS-F6-DWC-2000 Health Care Provider
Violation Referral
• Health Care Provider Violations Website:https://apps8.fldfs.com/hcprov/default.aspx

Carrier Reports of HCP Violations Performance
Rule 69L-34, F.A.C.

Carrier Reports of HCP Provider ViolationsRule 69L-34, F.A.C.

Medical Services SectionBureau of Monitoring and Audit
Contact Information(850) 413-1613
Theresa Pugh, Program Administrator
Medical Services
Lavounia Bozman, Sr. Management Analyst I

Questions

Carrier Compliance and Industry Performance
Pam Macon
Bureau Chief
Compliance

Today’s Topics
• Bureau of Monitoring and Audit Data
• Explanation of Bill Reviews
• Medical Services Statistics
• Q & A

Bureau of Monitoring & Audit
The Bureau of Monitoring and Audit (M&A) is responsible for ensuring that the practices of insurers, claim administrators and providers meet the requirements of Chapter 440, Florida Statutes and the Florida Administrative Code.

Bureau of Monitoring & Audit
The responsibilities are handled through four programmatic areas:
– Audit Section
– Penalty Section
– Permanent Total Disability Section
– Medical Services Section

Audit Section
Pursuant to Sections 440.185, 440.20, and 440.525, Florida Statutes and the rules of the Florida Administrative Code, the Audit Section examines claims-handling practices of:
– Insurers
– Self-insurers
– Self-insurance funds
– Other claims-handling entities

AUDIT SECTION
During FY 2015-2016, the Audit Section:
50 on-site insurer audits
5,809 insurer claim files
Identified 749 files with underpayments
additional injured worker payments of $337,728 for indemnity benefits, penalties, and interest

AUDIT SECTION
FY 2014/2015Category Totals
Number of Audits 56
Total Files Reviewed 5,303
Files Reviewed for Indemnity Payments
3,597
Underpaid Files 491
Total amount of UP + P&I Identified
$310,845
Total Pattern & Practice Penalties Assessed
$202,500
FY 2015/2016Category Totals
Number of Audits 50
Total Files Reviewed 5,809
Files Reviewed for IndemnityPayments
4,274
Underpaid Files 749
Total amount of UP + P&I Identified
$337,728
Total Pattern & Practice Penalties Assessed
$392,500

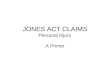
Untimely Indemnity Payment and FRoI Penalties by Fiscal Year
$64,200 $70,850
$83,300
$102,300
$27,500 $25,800
$60,300
$78,900
$0
$20,000
$40,000
$60,000
$80,000
$100,000
$120,000
FY12-13 (61 Audits) FY 13-14 (52 Audits) FY 14-15 (56 Audits) FY 15-16 (50 Audits)
Total Amount of Penalties Issued for Untimely Indemnity Payments
Total Amount of Penalties Issued for Untimely First Reports of Injury or Illness

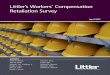
Total Non-Willful Pattern & Practice Penalties by Fiscal Year
41 64 81 157
$102,500
$160,000
$202,500
$392,500
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
$400,000
$450,000
0
20
40
60
80
100
120
140
160
180
FY12-13 (61 Audits) FY13-14 (52 Audits) FY14-15 (56 Audits) FY 15-16 (50 Audits)

PENALTY SECTION
The Penalty Section is responsible for evaluating and assessing insurer performance of timely payments of initial indemnity benefits and medical bills, and the untimely reporting of First Reports of Injury or Illness and medical bills.

CPS – First Reports Reviewed
Fiscal Year# of First Reports
Reviewed
FY 11-12 53,211
FY 12-13 51,690
FY 13-14 52,344
FY 14-15 53,929
FY 15-16 54,731

CPS Performance Statistics
Fiscal YearTimely Initial Benefit
Payments Timely Filing of First
Reports
FY 11-12 95% 95%
FY 12-13 95% 95%
FY 13-14 95% 95%
FY 14-15 95% 93%
FY 15-16 93% 95%

CPS Performance Statistics
Fiscal YearTimely Medical Bill
Payments Timely Medical
Bill Filing
FY 11-12 99% 99%
FY 12-13 98% 96%
FY 13-14 99% 98%
FY 14-15 99% 99%
FY 15-16 98% 98%

PERMANENT TOTAL DISABILITY SECTION
Division pays permanent total supplemental benefits on accidents prior to July 1, 1984 to eligible injured workers
FY 2015-2016 supplemental benefits for 987 claims totaling $14,624,125 were calculated, approved, and processed

EXPLANATIONS OF BILL REVIEW (EOBRs)
What is an EOBR?
An Explanation of Bill Review is the notice of payment or notice of adjustment, disallowance or denial sent by a carrier, service company/third party administrator or any entity acting on behalf of a carrier to a health care provider containing code(s) and code descriptor(s), in conformance with subsection 69L-7.740(13), Florida Administrative Code.

EXPLANATIONS OF BILL REVIEW (EOBRs)
What is the purpose of the EOBR?
The purpose is to communicate to the provider, the carrier’s decision to pay, disallow or adjust reimbursement. The carrier is required to explain the reimbursement for each billed line item by using the EOBR codes (listed in Rule within subsection 69L-7.740(13)(b), F.A.C.) that best describe the carrier’s reimbursement decision.

EXPLANATIONS OF BILL REVIEW• Explanations of Bill Review (EOBRs) must contain
the following elements per rule 69L-7.740, F.A.C.:
– Insurer’s name;
– Insurer’s mailing address;
– Division-issued insurer ID number
– EOBR Codes from the Billing Rule
– Compliant descriptors
– Name of the dispute copy designee
– Name of the dispute copy designee’s mailing address
– Disallowance language

MEDICAL SERVICES SECTION
• Responsibilities:
– Establishing rules and policy
– Implementing the Three-Member Panel’s uniform schedules for Maximum Reimbursement Allowances (MRAs)
– Resolving medical reimbursement disputes between providers and payers
– Certifying Expert Medical Advisors

MEDICAL SERVICES SECTION
• A Petition for Reimbursement Dispute must be filed within 45 days from receipt of the carrier’s notice of disallowance or adjustment of payment.
• The carrier must submit, within 30 days of receipt of the petition, its response and all documentation to the department to substantiate its disallowance or adjustment.

MEDICAL SERVICES SECTION
• Beginning Fiscal Year 15-16, there were 13,064 pending Petitions for Resolution of Reimbursement Disputes (Petitions)
• During Fiscal Year 15-16, the Medical Services Section:
– Received 5,533 Petitions
– Processed 18,133 Petitions

MEDICAL SERVICES SECTION
• The Medical Services Section issues Dismissals or Determinations for all Petitions received
• In Fiscal Year 2015-2016, the Section issued:
– 9,570 Determinations
– 8,546 Dismissals

Medical Services Data
Petitions Submitted by Provider Type
FY 12-13 FY 13-14 FY 14-15 FY 15-16
Practitioner 7,805 8,412 7,323 3,601
ASC 737 665 331 400
Hospital Inpatient
350 266 453 341
Hospital Outpatient
1,303 1,069 1,550 1,184
Total 10,209 10,483 9,659 5,533

Medical Services Data
Petitions Determination Outcomes by Provider Type
FY 12-13 FY 13-14 FY 14-15 FY 15-16
Practitioner 2,573 2.992 4,326 8,221
ASC 584 512 213 240
Hospital Inpatient 217 183 226 215
Hospital Outpatient 966 767 996 894
Total 4,340 5,454 5,761 9,570

Medical Services Data
Petitions Dismissal Outcomes by Provider Type
FY 12-13 FY 13-14 FY 14-15 FY 15-16
Practitioner 2,605 4,432 2,374 7,636
ASC 216 173 104 175
Hospital Inpatient 140 96 181 174
Hospital Outpatient
448 270 432 548
Other 0 0 2 13
Total 3,409 4,971 3,093 8,546

Charlene Miller, Bureau Chief
(850) 413-1738
Derrick Richardson,
Audit and PT Manager
(850) 413-1671

QUESTIONS

When a Notice of Action or Change is Required
Charlene Miller & Lawanna Morrow
Bureau of Monitoring and Audit

69L-56.304 & 69L-56.3045
Florida Administrative Code
Electronic Notice of Action or Change, Including Change in
Claims Administration

Notices of Action or ChangeTop 10 Sequencing Errors/Rejections
• Report RTW Info
• Report MMI Info
• Report a Change From TTD to TPD
• Report Adjustment to AWW/CR
• Report Annual Increase of PTD Supplemental Benefits
• Report Suspension of Benefits
• Report a Settlement
• Report Reinstatement of Benefits
• Report a Change From TPD to TTD
• Report an Acquired Claim

EDI Resourceshttp://www.myfloridacfo.com/division/WC/EDI/default.htm

EDI Resourceshttp://www.myfloridacfo.com/division/WC/EDI/default.htm

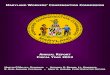
Auditing Notice of Action or Change Compliance
• Compliance percentages are documented in Audit Reports, and Pattern and Practice Penalties are assessed for compliance percentages below 90% per 440.525(4), Florida Statutes and Rule 69L-24.007, Florida Administrative Code.

4,318 4,1213,735
4,647
2,727
786521
982
734
1053
912
892 904
922
719
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
5,000
5,500
6,000
6,500
FY 11-12 FY 12-13 FY 13-14 FY 14-15 FY 15-16
Notices of Action or Change Compliance by Fiscal Year
Timely Not Sent Sent Late Compliance

Reason Notice of Change was Necessary
# of Late Forms
Report RTW Info 232
Report MMI Info 127
Report a Settlement 69
Report Suspension of Benefits 64
Report Reinstatement of Benefits 58
Report Adjustment to AWW/CR 53
Report a Change From TTD to TPD 53
Report Annual Increase of PTD Supps 33
Report a Change From TPD to TTD 18
FY 15/16 Notices of Action or Change Filed Late

Reason Notice of Change was Necessary
# of Not Filed Forms
Report RTW Info 268
Report MMI Info 236
Report a Change From TTD to TPD 121
Report a Settlement 112
Report Suspension of Benefits 72
Report Annual Increase of PTD Supps 69
Report a Change From TPD to TTD 63
Report Adjustment to AWW/CR 52
Report Reinstatement of Benefits 35
Report the Recoupment of Paid Benefits
12
FY 15/16 Notices of Action or Change Not Filed

Contacts:[email protected]
Bureau Chief, Bureau of Monitoring & Audit
(850) 413-1738
Operations Management Consultant Manager
(850) 413-1671
Workers’ Compensation Administrator-Tallahassee
(850) 413-1791
Workers’ Compensation Administrator-Orlando
(407) 835-4492

Division of Workers’ Compensation
Medical & Claims EDI
Update
August 2016
Michelle CarterBureau of Data Quality and Collection

Florida Medical EDI

Revision F Phase-In Schedule
Revision F Testing
Helpful Resources
Discussion Topics

Revision F Phase-In Schedule

All phase-in schedule dates are based on
the effective date of the Workers’
Compensation Medical Reimbursement
and Utilization Rule – which took effect on
February 18, 2016.
Revision F Phase-in Schedule

Group 1 (Submitter ID 001 – 199)
Testing began on July 18, 2016 (150 days
after the effective date of rule) and must be
completed by August 31, 2016 (195 days of
the effective date of the rule).
Revision F Phase-in Schedule

Group 2 (Submitter ID 200 – 899)
Testing begins on September 1, 2016 (195
days after the effective date of rule) and
must be complete within 240 days of the
effective date of the rule (October 15, 2016).
Revision F Phase-in Schedule

Group 3 (Submitter ID 900 and above)
Testing begins on October 16, 2016 (240
days after the effective date of rule) and
must be complete within 285 days of the
effective date of the rule (November 29,
2016).
Revision F Phase-in Schedule

Revision F Testing

Revision F Testing
Electronic files containing five (5) test bills
(for each form type tested) must be
transmitted to the Division by current batch
submitters.
Electronic files containing fifteen (15) test
bills (for each form type tested) must be
transmitted to the Division by new batch
submitters.

Revision F Testing
The ‘Test/Production Indicator’ in the file
name and ‘Transmission Header Record’
must be set to ‘T’.

Revision F Testing
Current web submitters must submit five
(5) test bills (for each form type tested) to
the Division.
New web submitters must submit fifteen
(15) test bills (for each form type tested)
to the Division.

There are several test scenarios that must
be completed. Pre-filled “dummy” bills and
information pertaining to the scenarios
have/will be sent to all submitters prior to
the test start date.
If any changes are made to the information
listed on any of the “dummy” bills provided,
a copy must be sent to the Division via fax
or email.
Revision F Testing

Revision F testing is not considered
complete until all bills have been accepted
by the Medical Data Management System,
passed visual comparison to paper bills
and all test scenarios have been
successfully completed.
Submitters will be notified via email upon
completion of testing.
Revision F Testing

Please direct any questions related to
Medical EDI submissions to:
Fax number for test bills: (850) 413-1986

Helpful Resources

There have been changes recently
made to the Division’s website.
http://www.myfloridacfo.com/Division/WC/
Helpful Resources

Helpful Resources

Helpful Resources

Helpful Resources

Florida Claims EDI

Triage & Training Team
TA-FL Errors (Non-Fatal)
Helpful Resources
Discussion Topics

Triage & Training Team
The Division has expanded its efforts to
assist Trading Partners with successfully
submitting claims transactions by creating
the Triage & Training Team.

Triage & Training Team
In an effort to help minimize rejections
and improve the quality of data submitted
to the Division, the Triage & Training
Team provides training on various Claims
EDI related issues by partnering with
individual claim administrators.

Triage assistance is provided via:
Webinars
Teleconferences
Onsite visits (claim administrator’s office
or at the Division)
Triage & Training Team

Triage assistance can be requested by
the claim administrator or identified and
initiated by the one of the Triage Team
members.
To request training assistance, please
send an email to:
Triage & Training Team

TA-FL Errors
(Non-Fatal)

The Division has re-evaluated the TA-FL
process to reduce the number of errors
received for which the industry and EDI
team have to respond.
As a result of this, all unresolved errors
prior to April 27, 2016 were mass closed.
TA-FL Errors (Non-Fatal)

As you are aware, automated email
notifications are sent (next day) regarding
the posting of non-fatal errors from the
previous night’s transactions. As outlined
in Division Rule 69L-56.300(1)(i), the
errors should be responded to on or
before 21 days after the date the error
was posted.
TA-FL Errors (Non-Fatal)

At this time, the Division has staff
dedicated to review and respond to all
TA-FL errors received in the Claims EDI
Warehouse. The team will only handle
errors on transactions where notes have
been entered into the Claims EDI
Warehouse by the claim administrator.
TA-FL Errors (Non-Fatal)

Helpful Resources

Helpful Resources

Helpful Resources

Helpful Resources

Thank You!
Slides will be made available on
the Division’s website
http://www.myfloridacfo.com/Division/wc/