Embed Size (px)
Citation preview
OUTCOMES OF ANAL FISTULA SURGERY IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE
Division of General Surgery, St Paul's Hospital
Z. Rahimi
M. Hoorzad
American journal of surgery, May 2010
Background:
Anal fistulas in patients with Crohn's disease are especially difficult to manage because of nonhealing and incontinence. We reviewed our outcomes for the newer sphincter-preserving techniques of anal fistula plug and fibrin glue compared with standard treatments of advancement flap closure and seton drain insertion.
Methods:
This was a retrospective study of patients with inflammatory bowel disease treated for high transsphincteric anal fistulas. The primary outcome was healing and continence at 12 weeks postoperatively.
Results:
Between 1997 and 2009, 51 patients with anal fistulas and inflammatory bowel disease were identified in the St Paul's Hospital Anal Fistula Database.
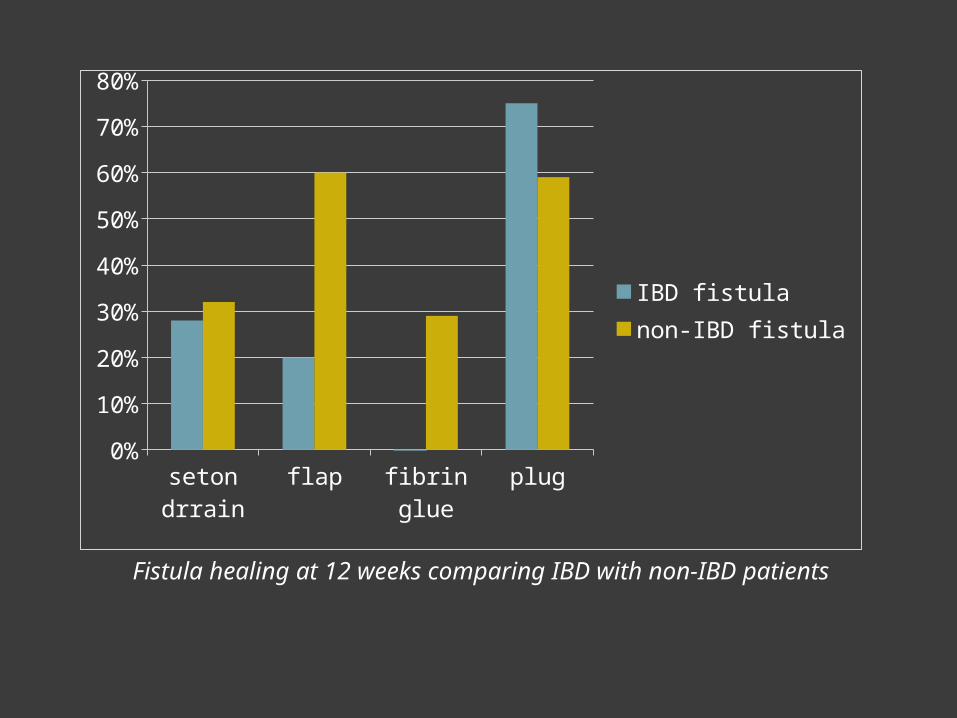
Postoperative healing rates at 12 weeks for the fistula plug, fibrin glue, flap advancement, and seton drain groups were 75%, 0%, 20%, and 28%, respectively. Continence scores were not altered by these procedures.
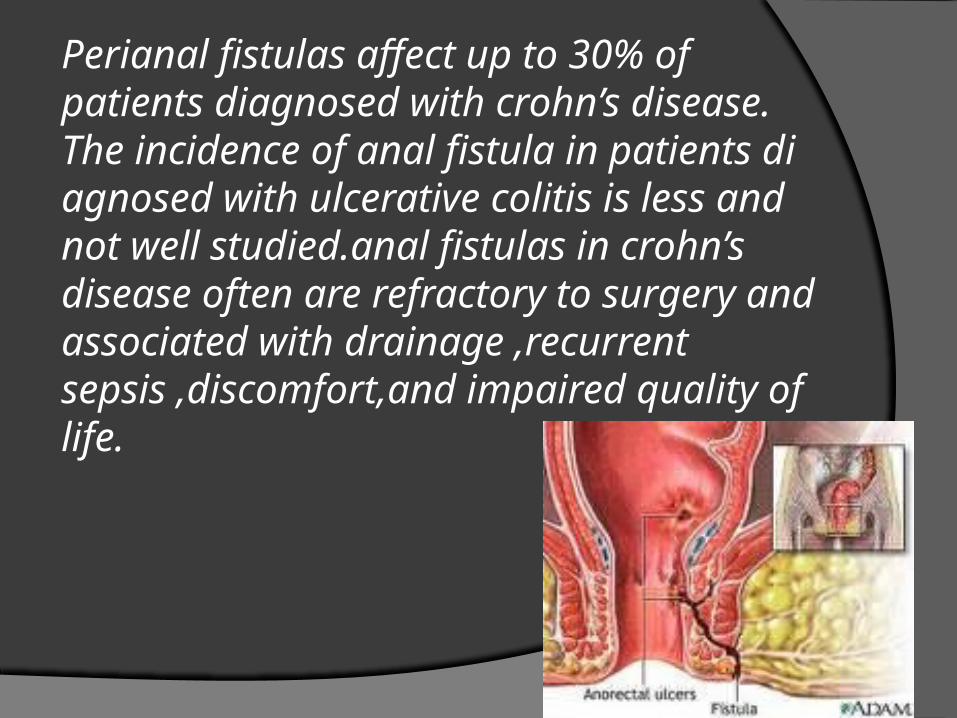
Perianal fistulas affect up to 30% of patients diagnosed with crohn’s disease. The incidence of anal fistula in patients di agnosed with ulcerative colitis is less and not well studied.anal fistulas in crohn’s disease often are refractory to surgery and associated with drainage ,recurrent sepsis ,discomfort,and impaired quality of life.
The goal of fistula surgery for patients with inflammatry bowel disease (IBD) is to relieve symptoms and achieve closure in selected cases. conventional fistulotomy generally is avoided because of the potential for impaired continence secondary to division of any sphincter muscle.
Some patients are manage successfully by placement of a long-term draining and noncutting seton. other sphincter-sparing approaches for anal fistula management in crohn’s disease include rectal advancement flaps, fibrin glue injection, and collagen plug insertion.
In this study , we reviewed outcomes for high transsphincteric fistula repair in our patients affected with IBD,especially with respect to the newer sphincter-preserving techniques of plug and glue,and compare them with our previously reported outcomes in non-IBDpatient. We also assessed whether there was any change in continence resulting from the surgery.
Methods:
All IBD patients treated for anal fistulas by a single colorectal at St paul,s Hospital.university of British Colombia.from january 1997 to january2009,were identified from a database.
Simple fistulas were defined as low fistulas including subcutaneous,intersphincteric,and low transsphincteric fistulas. Low transsphincteric fistulas involved the lower third of the external anal sphincter mechanism. Conversely,complex anal fistulas were defined as crohn,s fistulas,low compromised fistulas,and high transsphincteric fistulas.
Low compromised fistulas occurred in the lower thirrd of the external anal sphincter in patients who had pre-existing tendency for incontinence. high transsphincteric fistulas involved the upper two thirds of the external sphincter and were subclassified further as direct transsphincteric,horse-shoe,and supralevator fistulas.
Surgical procedures:
All procedures were performed under general anesthesia. Fibrin glue Bioprosthetic plug Seton drain
placement Advancement flap
closure
Fibrin glue:
Fibrin glue was instilled into the fistula tract by way of the external opening.a nonadherent dressing was placed,and the patient was instructed to avoid lifting and vigorous physical activity for the next 7 days.
Data collection and follow-up evaluation:
All patient were evaluated in the outpatient clinic.
Patient incontinence was evaluated preoperatively and postoperatively using the vaizey et al incontinence grading system.the validated vaizey et al scale consists of items concering the type and frequency of incontinence and changes in lifestyle,with a score ranging from 0%(complete continence)to 24%(complete incontinence).
our secondary objective was comparison of fistula healing rates for our IBD versus non-IBD patients
Result:
Fifty-one patient with high transsphincteric fistulas concomitant with IBD were included.
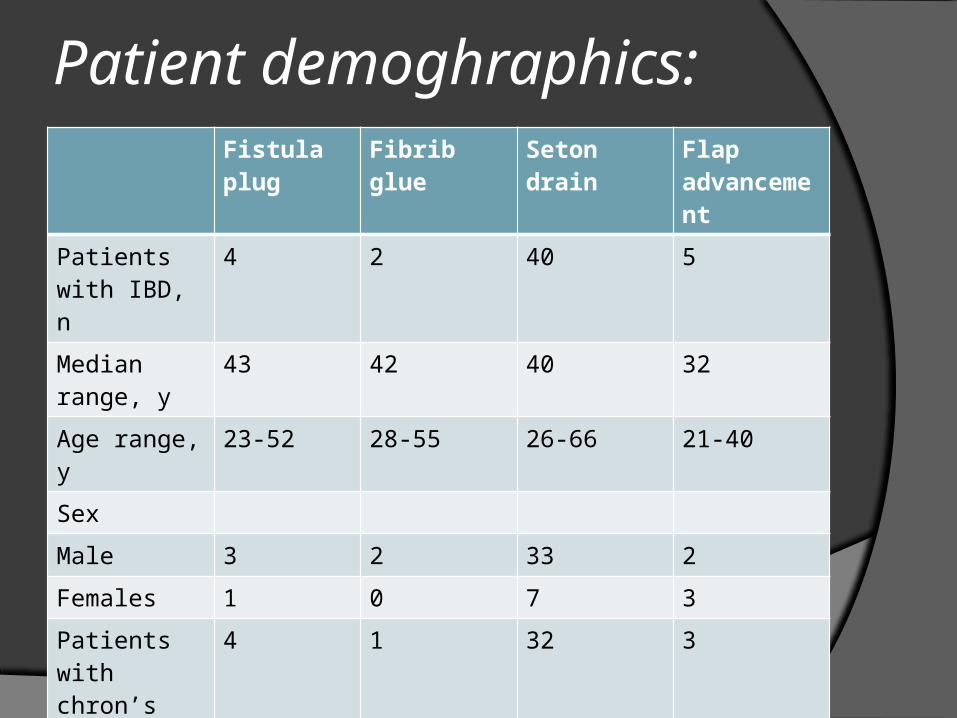
Patient demoghraphics:Fistula plug
Fibrib glue Seton drain Flap advancement
Patients with IBD, n
4 2 40 5
Median range, y
43 42 40 32
Age range, y 23-52 28-55 26-66 21-40
Sex
Male 3 2 33 2
Females 1 0 7 3
Patients with chron’s disease
4 1 32 3
Patient’n with ulcerative colitis
0 1 8 2
IBD patients treated using the fistula plug showed a healing compared with 59.3% in the non-IBD group.all other procedures showed a reduction in healing rates at 12 weeks for IBD patients compared with non-IBD patients.
seton dr-rain
flap fibrin glue plug0%
10%
20%
30%
40%
50%
60%
70%
80%
IBD fistulanon-IBD fistula
Fistula healing at 12 weeks comparing IBD with non-IBD patients
Risk factors assessed for possible association with treatment failure were age fistula classification,and comorbidities(diabetes,human immunodeficiency virus,and perioperative infliximab).none of these factors were associated significantly with healing at 12 weeks using multivariate analysis.
Comments:
Complex fistulas are notoriously difficult to manage and particulary so in patients with crohn,s disease.
We found that healing rates at 12 weeks were highest for the anal plug procedure and lower for the other procedure compared with non-IBD patients.
Healing rates for the fistula plug group was 75% in IBD patients and 59% in non-IBD patients.
Twenty-five percent of plug failures were secondary to extrusion within the first week postoperatively . Our healing rate for the fistula pluge in IBD patients is similar to previouly reported small series that have shown success rate of 80% to 86%.
Both fibrin glue and fistula plug treatments have minimal risk of incontinence. Failure of these newer treatment does not compromise subsequent surgical options. Lower healing rate seen with fibrin glue treatment may be secondary to the liquid consistency of the glue in a short fistula tract causing early extrusion.
Conversely, the higher healing rate seen with the fistula plug likely is owing to a more secure fixation than glue in the fistula tract, resulting in less early extrusion.
Discussion:
Anal fistula of Chron’s disease have been notoriously difficult to treat. Fistulotomy would lead to incontinence.
THEN:
Healing rates after anal fistula plug were better in Chron’s patients than in non-Chron’s patients: 75% vs. 59%

THANK YOU FOR YOUR ATTENTION!





























