Embed Size (px)
Citation preview

DIVERTICULITIS
Nancy Edith Aguilar O.Septiembre 2009 1
INTRODUCCIÓN
2

www.uptodate.comHarrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
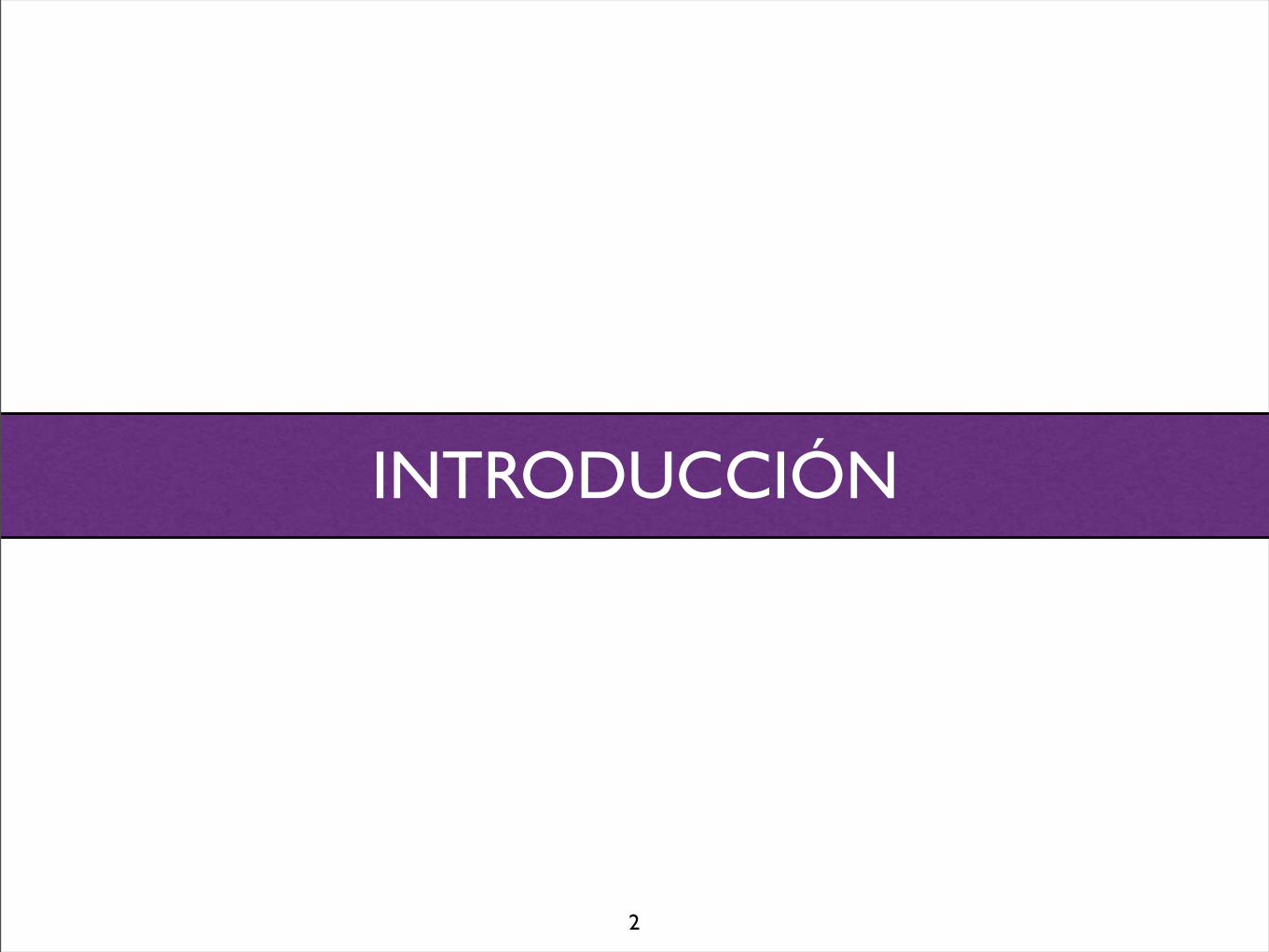
Divertículo(pseudodivertículo)

www.uptodate.comHarrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
Divertículo(pseudodivertículo)
Diverticulosis

www.uptodate.comHarrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
Divertículo(pseudodivertículo)
Diverticulosis
Diverticulitis
www.uptodate.comHarrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
Enfermedad Diverticular
Divertículo(pseudodivertículo)
Diverticulosis
Diverticulitis
EPIDEMIOLOGÍA

• PREVALENCIA DIVERTICULOSIS
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.Rege, RV, Nahrwold, DL. Diverticular disease. Curr Probl Surg 1989; 26:133.
• PREVALENCIA DIVERTICULOSIS
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.Rege, RV, Nahrwold, DL. Diverticular disease. Curr Probl Surg 1989; 26:133.
Occidente: 5 a 45%
Lado izquierdo
Diverticulosis 20%

• PREVALENCIA DIVERTICULOSIS
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.Rege, RV, Nahrwold, DL. Diverticular disease. Curr Probl Surg 1989; 26:133.
Occidente: 5 a 45%
Lado izquierdo
Diverticulosis 20%
Lado derecho en 5%
Diverticulosis 1.5% (Dx en 4 -16%)

• PREVALENCIA DIVERTICULOSIS
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.Rege, RV, Nahrwold, DL. Diverticular disease. Curr Probl Surg 1989; 26:133.
Occidente: 5 a 45%
Lado izquierdo
Diverticulosis 20%
Asia y Africa: < 0.2 %
Usualmente derecha 75%
Lado derecho en 5%
Diverticulosis 1.5% (Dx en 4 -16%)

• La prevalencia depende de la edad
• 40 años..................5-10%
• 60 años..................30%
• >85 años................65%
Parks, TG. Natural history of diverticular disease of the colon. Clin Gastroenterol 1975; 4:53.Painter, NS, Burkitt, DP. Diverticular disease of the colon, a 20th century problem. Clin Gastroenterol 1975; 4:3.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
• La prevalencia depende de la edad
• 40 años..................5-10%
• 60 años..................30%
• >85 años................65%
Parks, TG. Natural history of diverticular disease of the colon. Clin Gastroenterol 1975; 4:53.Painter, NS, Burkitt, DP. Diverticular disease of the colon, a 20th century problem. Clin Gastroenterol 1975; 4:3.
Edad media de presentación: 59 años
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
• EPIDEMIOLOGIA
• Prevalencia similar entre homdres y mujeres
Hombres mujeresEdad
Rodkey, GV, Welch, CE. Changing patterns in the surgical treatment of diverticular disease. Ann Surg 1984; 200:466.

• EPIDEMIOLOGIA
• Prevalencia similar entre homdres y mujeres
Hombres mujeresEdad
Rodkey, GV, Welch, CE. Changing patterns in the surgical treatment of diverticular disease. Ann Surg 1984; 200:466.

ETIOLOGÍA Y FISIOPATOLOGÍA

Aldoori, WH, Giovannucci, EL, Rimm, EB, et al. A prospective study of diet and the risk of symptomatic diverticular disease in men. Am J Clin Nutr 1994; 60:757.Aldoori, WH, Giovannucci, EL, Rimm, EB, et al. A prospective study of alcohol, smoking, caffeine, and the risk of symptomatic diverticular disease in men. Ann Epidemiol 1995; 5:221.Strate, LL, Liu, YL, Aldoori, WH, et al. Obesity increases the risks of diverticulitis and diverticular bleeding. Gastroenterology 2009; 136:115.
Obesidad (RR 1.56)
Dieta baja en fibra
Dieta rica en grasa y carne (RR 2.35 a 3.32)

• El riesgo no se incrementa con el tabaco, el alcohol ni cafeína
• El riesgo es inverso a la actividad física
Aldoori, WH, Giovannucci, EL, Rimm, EB, et al. A prospective study of diet and the risk of symptomatic diverticular disease in men. Am J Clin Nutr 1994; 60:757.Aldoori, WH, Giovannucci, EL, Rimm, EB, et al. A prospective study of alcohol, smoking, caffeine, and the risk of symptomatic diverticular disease in men. Ann Epidemiol 1995; 5:221.Strate, LL, Liu, YL, Aldoori, WH, et al. Obesity increases the risks of diverticulitis and diverticular bleeding. Gastroenterology 2009; 136:115.
Obesidad (RR 1.56)
Dieta baja en fibra
Dieta rica en grasa y carne (RR 2.35 a 3.32)

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072058
The pathogenesis of diverticulitis is uncertain. However, stasis or obstruction in the narrow-necked pseudodiverticulum may lead to bacterial overgrowth and local tissue ischemia, findings that are similar to those described in appendici-tis. Anaerobes (including bacteroides, pepto-streptococcus, clostridium, and fusobacterium species) are the most commonly isolated organ-isms. Gram-negative aerobes, especially Escherichia coli, and facultative gram-positive bacteria, such as streptococci, are often cultured as well.12
“Complicated” diverticulitis is present when there is an abscess or phlegmon, fistula forma-tion, stricture disease, bowel obstruction, or peri-tonitis. Generalized peritonitis may result from
rupture of a peridiverticular abscess or from free rupture of an uninflamed diverticulum. Only 1 to 2% of patients who present for urgent evaluation have free perforation. High-grade colonic obstruc-tion, though relatively uncommon, may result from abscess formation or edema or from stric-ture formation after recurrent attacks of diverticu-litis.13 Small-bowel obstruction may occur some-what more frequently, especially in the presence of a large peridiverticular abscess.
The consequences of diverticulitis may be more severe in immunocompromised patients, includ-ing those who have undergone organ transplan-tation, have human immunodeficiency virus infec-tion, or are taking corticosteroids. These patients
Figure!1.!Colonic!Diverticula.
Colonic diverticula have narrow necks that can be easily obstructed by fecal matter. Obstruction of the neck sets a cascade of events in motion that may include distention of the sac, bacterial overgrowth, vascular compromise, and perforation. When perforations occur, they are often contiguous with other tissues or organs, such as the omentum, mesocolon, bladder, or small bowel. Some perforations are localized and contained, whereas others may invade the skin or erode into adjacent viscera, causing fistulas. Fistulization most frequently involves the colon and bladder (in up to 65% of cases), although the bladder is a less frequent site in women if the uterus is present.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
• 95% ocupan el sigmoides
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072058
The pathogenesis of diverticulitis is uncertain. However, stasis or obstruction in the narrow-necked pseudodiverticulum may lead to bacterial overgrowth and local tissue ischemia, findings that are similar to those described in appendici-tis. Anaerobes (including bacteroides, pepto-streptococcus, clostridium, and fusobacterium species) are the most commonly isolated organ-isms. Gram-negative aerobes, especially Escherichia coli, and facultative gram-positive bacteria, such as streptococci, are often cultured as well.12
“Complicated” diverticulitis is present when there is an abscess or phlegmon, fistula forma-tion, stricture disease, bowel obstruction, or peri-tonitis. Generalized peritonitis may result from
rupture of a peridiverticular abscess or from free rupture of an uninflamed diverticulum. Only 1 to 2% of patients who present for urgent evaluation have free perforation. High-grade colonic obstruc-tion, though relatively uncommon, may result from abscess formation or edema or from stric-ture formation after recurrent attacks of diverticu-litis.13 Small-bowel obstruction may occur some-what more frequently, especially in the presence of a large peridiverticular abscess.
The consequences of diverticulitis may be more severe in immunocompromised patients, includ-ing those who have undergone organ transplan-tation, have human immunodeficiency virus infec-tion, or are taking corticosteroids. These patients
Figure!1.!Colonic!Diverticula.
Colonic diverticula have narrow necks that can be easily obstructed by fecal matter. Obstruction of the neck sets a cascade of events in motion that may include distention of the sac, bacterial overgrowth, vascular compromise, and perforation. When perforations occur, they are often contiguous with other tissues or organs, such as the omentum, mesocolon, bladder, or small bowel. Some perforations are localized and contained, whereas others may invade the skin or erode into adjacent viscera, causing fistulas. Fistulization most frequently involves the colon and bladder (in up to 65% of cases), although the bladder is a less frequent site in women if the uterus is present.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
• 95% ocupan el sigmoides
Se desarrolla en 4 puntos bien definidos
Sitios de perforación de la vasa recta
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072058
The pathogenesis of diverticulitis is uncertain. However, stasis or obstruction in the narrow-necked pseudodiverticulum may lead to bacterial overgrowth and local tissue ischemia, findings that are similar to those described in appendici-tis. Anaerobes (including bacteroides, pepto-streptococcus, clostridium, and fusobacterium species) are the most commonly isolated organ-isms. Gram-negative aerobes, especially Escherichia coli, and facultative gram-positive bacteria, such as streptococci, are often cultured as well.12
“Complicated” diverticulitis is present when there is an abscess or phlegmon, fistula forma-tion, stricture disease, bowel obstruction, or peri-tonitis. Generalized peritonitis may result from
rupture of a peridiverticular abscess or from free rupture of an uninflamed diverticulum. Only 1 to 2% of patients who present for urgent evaluation have free perforation. High-grade colonic obstruc-tion, though relatively uncommon, may result from abscess formation or edema or from stric-ture formation after recurrent attacks of diverticu-litis.13 Small-bowel obstruction may occur some-what more frequently, especially in the presence of a large peridiverticular abscess.
The consequences of diverticulitis may be more severe in immunocompromised patients, includ-ing those who have undergone organ transplan-tation, have human immunodeficiency virus infec-tion, or are taking corticosteroids. These patients
Figure!1.!Colonic!Diverticula.
Colonic diverticula have narrow necks that can be easily obstructed by fecal matter. Obstruction of the neck sets a cascade of events in motion that may include distention of the sac, bacterial overgrowth, vascular compromise, and perforation. When perforations occur, they are often contiguous with other tissues or organs, such as the omentum, mesocolon, bladder, or small bowel. Some perforations are localized and contained, whereas others may invade the skin or erode into adjacent viscera, causing fistulas. Fistulization most frequently involves the colon and bladder (in up to 65% of cases), although the bladder is a less frequent site in women if the uterus is present.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
• 95% ocupan el sigmoides
Se desarrolla en 4 puntos bien definidos
Sitios de perforación de la vasa recta
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.
• FISIOPATOLOGIA
Wess, L, Eastwood, MA, Wess, TJ, et al. Cross linking of collagen is increased in colonic diverticulosis. Gut 1995; 37:91
P = kT ÷ R
Áreas débiles
Miocosis (elastina)
Inicio temprano en enfermedades del tejido conectivo
Ley de Laplace

MANIFESTACIONES CLÍNICAS

DIVERTICULOSIS
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
absceso fístula obstrucción perforación
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
absceso fístula obstrucción perforación
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
absceso fístula obstrucción perforación
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
absceso fístula obstrucción perforación
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
absceso fístula obstrucción perforación
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
absceso fístula obstrucción perforación
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
HAS Aterosclerosis
AINES

DIVERTICULOSIS
70%asintomático
15-25%diverticulitis
5-20%sangrado
absceso fístula obstrucción perforación
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
HAS Aterosclerosis
AINES
Riesgo de resangrado de 25%

DIVERTICULOSIS DIVERTICULITIS
Hallazgo
Dolor cólico Distensión FlatulenciaAlteraciones en la defecación
SIMPLE 75%Dolor por varios díasEpisodios de dolor similarObstipaciónAnorexiaNáusea y vómito (20-62%)Constipación (50%)Diarrea (25-35%)Síntomas urinarios (10-15%)Fiebre y leucocitosis en bajo grado
COMPLICADA 25%
www.uptodate.comHarrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

Diverticulitis Complicada
AbscesoPerforaciónObstrucción/EstenosisFístula
16%10%5%2%
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
• Diagnóstico diferencial:
• Apendicitis
• Enfermedad inflamatoria intestinal
• Enfermedad pélvica inflamatoria
• Cáncer en etapa avanzada
• Colitis infecciosa
• Síndrome de colon irritable
• Quistes ováricos
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

DIAGNÓSTICO

• Placas: excluye otras causas
Rao, PM, Rhea, JT, Novelline, RA, et al. Helical CT with only colonic contrast materialfor diagnosing diverticulitis: Prospective evaluation of 150 patients. AJR Am J Roentgenol 1998; 170:1445

• Placas: excluye otras causas
Rao, PM, Rhea, JT, Novelline, RA, et al. Helical CT with only colonic contrast materialfor diagnosing diverticulitis: Prospective evaluation of 150 patients. AJR Am J Roentgenol 1998; 170:1445
TAC:

• Placas: excluye otras causas
DiagnósticoEvaluación de la severidad
ComplicacionesIntervención terapéutica
Evaluación de la resolución
Rao, PM, Rhea, JT, Novelline, RA, et al. Helical CT with only colonic contrast materialfor diagnosing diverticulitis: Prospective evaluation of 150 patients. AJR Am J Roentgenol 1998; 170:1445
TAC:

• TAC con contraste
• Sensibilidad: 97%
• Especificidad: 100%
• VPP: 100%
• VPN: 98%
www.uptodate.com
• 98% - Incremento de la densidad de la grasa pericolónica
• 84% - Diverticulos
• 70% - Engrosamiento de la pared intestinal >4 cm
• En 10% no se puede distinguir de carcinoma
• 35% - Masas, colecciones y abscesos
www.uptodate.com
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.
Clasificación de Hinchey
Predice evolución después del tratamiento quirúrgico de la enfermedad diverticular complicada
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

clinical pr actice
n engl j med 357;20 www.nejm.org november 15, 2007 2059
may have atypical signs and symptoms, are more likely to have free perforation, are less likely to have a response to conservative management, and have higher postoperative risks of complications and death than immunocompetent patients.2,14
Di agnosis a nd E va luation
The clinical manifestations of acute colonic diver-ticulitis vary with the extent of the disease process. In classic cases, patients report obstipation and ab-dominal pain that localizes to the left lower quad-rant. An abdominal or perirectal fullness, or “mass effect,” may be apparent. Stool guaiac testing may be trace-positive. A low-grade fever is common, as is leukocytosis.
Alternative diagnoses for lower abdominal pain must be considered. Sigmoid diverticulitis may mimic acute appendicitis if the colon is redundant or otherwise configured such that the inflamed portion resides in the suprapubic region of the right lower quadrant. Inflammatory bowel disease (especially Crohn’s disease), pelvic inflammatory disease, tubal pregnancy, cystitis, advanced colonic cancer, and infectious colitis may also have pre-sentations similar to that of diverticulitis.
Patients with free perforation have peritoneal irritation, including marked abdominal tenderness that begins suddenly and spreads rapidly to involve the entire abdomen with guarding and involun-tary rigidity. Peritonitis is an indication for emer-gency surgical exploration.
StagingThe severity of diverticulitis is often graded with the use of Hinchey’s criteria (Fig. 2), although this classification system does not take into account the effects of coexisting conditions on disease sever-ity or outcome. The risk of death is less than 5% for most patients with stage 1 or 2 diverticulitis, ap-proximately 13% for those with stage 3, and 43% for those with stage 4.15
Imaging and EndoscopyComputed tomography (CT) is recommended as the initial radiologic examination (Fig. 3). It has high sensitivity (approximately 93 to 97%) and specificity approaching 100% for the diagno-sis,16,17 and it allows delineation of the extent of the disease process.18,19 In occasional cases, when
it is difficult to distinguish between diverticulitis and carcinoma, limited contrast studies of the de-scending colon and rectum with the use of water-soluble contrast material may be helpful. The pres-ence of diverticula, inflammation of the pericolic fat or other tissues, bowel-wall thickness of more than 4 mm, or a peridiverticular abscess strongly suggests diverticulitis.2 CT may also reveal other disease processes accounting for lower abdominal pain, such as appendicitis, tubo-ovarian abscess, or Crohn’s disease.
Colonoscopy and sigmoidoscopy are typically
Figure!2.!Hinchey!Classification!Scheme.
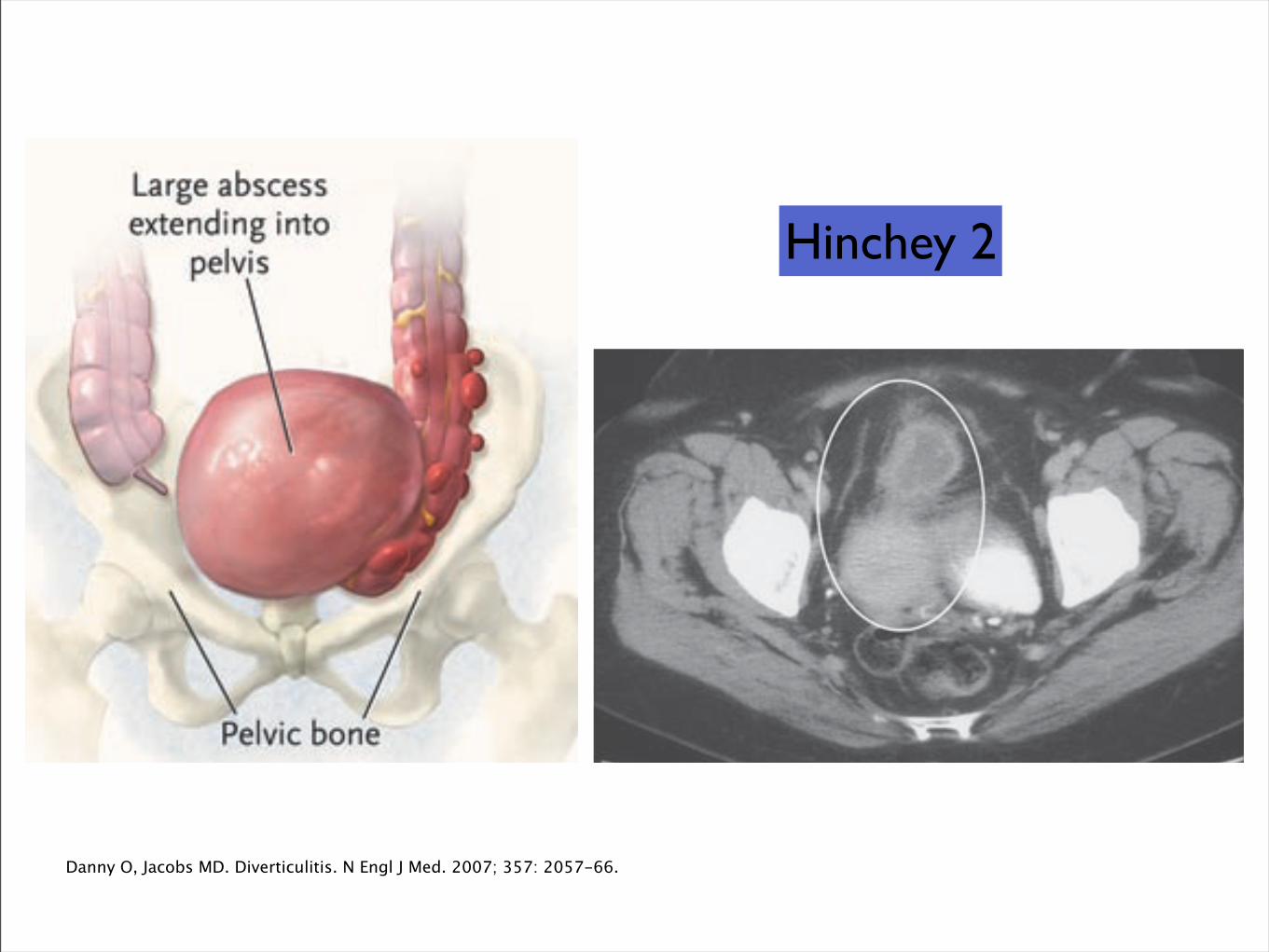
Patients with stage 1 disease have small, confined pericolic or mesenteric abscesses, whereas those with stage 2 disease have larger abscesses, often confined to the pelvis. Stage 3 disease, or perforated diverticulitis, is pres-ent when a peridiverticular abscess has ruptured and caused purulent peritonitis. Rupture of an uninflamed and unobstructed diverticulum into the free peritoneal cavity with fecal contamination, the so-called free rup-ture, signifies stage 4 disease and carries the highest risk of an adverse outcome.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072060
avoided when acute diverticulitis is suspected be-cause of the risk of perforation or other exacerba-tion of the disease process. Expert opinion is in favor of performing these tests when the acute process has resolved, usually after approximately 6 weeks, to rule out the presence of other diseases, such as cancer and inflammatory bowel disease.
HospitalizationThe decision to hospitalize a patient for diverticu-litis depends on the patient’s clinical status. For most patients (i.e., immunocompetent patients who have a mild attack and can tolerate oral intake), outpatient therapy is reasonable. This involves 7 to 10 days of oral broad-spectrum antimicrobial ther-apy, including coverage against anaerobic micro-organisms. A combination of ciprofloxacin and metronidazole is often used, but other regimens are also effective (Table 1). A low-residue liquid diet (i.e., one largely free of indigestible matter) is also commonly recommended, although this approach has not been rigorously studied.
Hospitalization is indicated if the patient is unable to tolerate oral intake or has pain severe enough to require narcotic analgesia, if symp-toms fail to improve despite adequate outpatient therapy, or if the patient has complicated diver-ticulitis. The patient should initially take noth-ing by mouth. If there is evidence of obstruction or ileus, a nasogastric tube should be inserted. Broad-spectrum intravenous antibiotic coverage is appropriate (Table 1).
If there is no improvement in pain, fever, and leukocytosis within 2 or 3 days, or if serial phys-ical examinations reveal new findings or evidence of worsening, repeat CT imaging is appropriate,
Figure!3.!CT!Scans!of!the!Colon!in!Four!Patients!!with!Diverticulitis!of!Varying!Severity.!
Panel A shows diverticula (arrow) and evidence of in-flammation and wall thickening (arrowhead), findings that are consistent with Hinchey stage 1 disease. Panel B shows a peridiverticular abscess (circled), a finding consistent with stage 2 disease. Panel C shows a drain within a large, confined diverticular abscess (circled) that communicated with the colon, which is consistent with stage 3 disease. Panel D shows evidence of free perforation (arrows) near thickened descending colon, a finding that is consistent with stage 3 or 4 disease. Images courtesy of Dr. Erik Paulson, Department of Radiology, Duke University Medical Center.
16p6
AUTHORFIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASEEMail Line
H/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
11-15-07
mleahy
35720
A
B
D
C
JacobsFig 3 a_d
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
Hinchey 1
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072060
avoided when acute diverticulitis is suspected be-cause of the risk of perforation or other exacerba-tion of the disease process. Expert opinion is in favor of performing these tests when the acute process has resolved, usually after approximately 6 weeks, to rule out the presence of other diseases, such as cancer and inflammatory bowel disease.
HospitalizationThe decision to hospitalize a patient for diverticu-litis depends on the patient’s clinical status. For most patients (i.e., immunocompetent patients who have a mild attack and can tolerate oral intake), outpatient therapy is reasonable. This involves 7 to 10 days of oral broad-spectrum antimicrobial ther-apy, including coverage against anaerobic micro-organisms. A combination of ciprofloxacin and metronidazole is often used, but other regimens are also effective (Table 1). A low-residue liquid diet (i.e., one largely free of indigestible matter) is also commonly recommended, although this approach has not been rigorously studied.
Hospitalization is indicated if the patient is unable to tolerate oral intake or has pain severe enough to require narcotic analgesia, if symp-toms fail to improve despite adequate outpatient therapy, or if the patient has complicated diver-ticulitis. The patient should initially take noth-ing by mouth. If there is evidence of obstruction or ileus, a nasogastric tube should be inserted. Broad-spectrum intravenous antibiotic coverage is appropriate (Table 1).
If there is no improvement in pain, fever, and leukocytosis within 2 or 3 days, or if serial phys-ical examinations reveal new findings or evidence of worsening, repeat CT imaging is appropriate,
Figure!3.!CT!Scans!of!the!Colon!in!Four!Patients!!with!Diverticulitis!of!Varying!Severity.!
Panel A shows diverticula (arrow) and evidence of in-flammation and wall thickening (arrowhead), findings that are consistent with Hinchey stage 1 disease. Panel B shows a peridiverticular abscess (circled), a finding consistent with stage 2 disease. Panel C shows a drain within a large, confined diverticular abscess (circled) that communicated with the colon, which is consistent with stage 3 disease. Panel D shows evidence of free perforation (arrows) near thickened descending colon, a finding that is consistent with stage 3 or 4 disease. Images courtesy of Dr. Erik Paulson, Department of Radiology, Duke University Medical Center.
16p6
AUTHORFIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASEEMail Line
H/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
11-15-07
mleahy
35720
A
B
D
C
JacobsFig 3 a_d
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
clinical pr actice
n engl j med 357;20 www.nejm.org november 15, 2007 2059
may have atypical signs and symptoms, are more likely to have free perforation, are less likely to have a response to conservative management, and have higher postoperative risks of complications and death than immunocompetent patients.2,14
Di agnosis a nd E va luation
The clinical manifestations of acute colonic diver-ticulitis vary with the extent of the disease process. In classic cases, patients report obstipation and ab-dominal pain that localizes to the left lower quad-rant. An abdominal or perirectal fullness, or “mass effect,” may be apparent. Stool guaiac testing may be trace-positive. A low-grade fever is common, as is leukocytosis.
Alternative diagnoses for lower abdominal pain must be considered. Sigmoid diverticulitis may mimic acute appendicitis if the colon is redundant or otherwise configured such that the inflamed portion resides in the suprapubic region of the right lower quadrant. Inflammatory bowel disease (especially Crohn’s disease), pelvic inflammatory disease, tubal pregnancy, cystitis, advanced colonic cancer, and infectious colitis may also have pre-sentations similar to that of diverticulitis.
Patients with free perforation have peritoneal irritation, including marked abdominal tenderness that begins suddenly and spreads rapidly to involve the entire abdomen with guarding and involun-tary rigidity. Peritonitis is an indication for emer-gency surgical exploration.
StagingThe severity of diverticulitis is often graded with the use of Hinchey’s criteria (Fig. 2), although this classification system does not take into account the effects of coexisting conditions on disease sever-ity or outcome. The risk of death is less than 5% for most patients with stage 1 or 2 diverticulitis, ap-proximately 13% for those with stage 3, and 43% for those with stage 4.15
Imaging and EndoscopyComputed tomography (CT) is recommended as the initial radiologic examination (Fig. 3). It has high sensitivity (approximately 93 to 97%) and specificity approaching 100% for the diagno-sis,16,17 and it allows delineation of the extent of the disease process.18,19 In occasional cases, when
it is difficult to distinguish between diverticulitis and carcinoma, limited contrast studies of the de-scending colon and rectum with the use of water-soluble contrast material may be helpful. The pres-ence of diverticula, inflammation of the pericolic fat or other tissues, bowel-wall thickness of more than 4 mm, or a peridiverticular abscess strongly suggests diverticulitis.2 CT may also reveal other disease processes accounting for lower abdominal pain, such as appendicitis, tubo-ovarian abscess, or Crohn’s disease.
Colonoscopy and sigmoidoscopy are typically
Figure!2.!Hinchey!Classification!Scheme.
Patients with stage 1 disease have small, confined pericolic or mesenteric abscesses, whereas those with stage 2 disease have larger abscesses, often confined to the pelvis. Stage 3 disease, or perforated diverticulitis, is pres-ent when a peridiverticular abscess has ruptured and caused purulent peritonitis. Rupture of an uninflamed and unobstructed diverticulum into the free peritoneal cavity with fecal contamination, the so-called free rup-ture, signifies stage 4 disease and carries the highest risk of an adverse outcome.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
Hinchey 2
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072060
avoided when acute diverticulitis is suspected be-cause of the risk of perforation or other exacerba-tion of the disease process. Expert opinion is in favor of performing these tests when the acute process has resolved, usually after approximately 6 weeks, to rule out the presence of other diseases, such as cancer and inflammatory bowel disease.
HospitalizationThe decision to hospitalize a patient for diverticu-litis depends on the patient’s clinical status. For most patients (i.e., immunocompetent patients who have a mild attack and can tolerate oral intake), outpatient therapy is reasonable. This involves 7 to 10 days of oral broad-spectrum antimicrobial ther-apy, including coverage against anaerobic micro-organisms. A combination of ciprofloxacin and metronidazole is often used, but other regimens are also effective (Table 1). A low-residue liquid diet (i.e., one largely free of indigestible matter) is also commonly recommended, although this approach has not been rigorously studied.
Hospitalization is indicated if the patient is unable to tolerate oral intake or has pain severe enough to require narcotic analgesia, if symp-toms fail to improve despite adequate outpatient therapy, or if the patient has complicated diver-ticulitis. The patient should initially take noth-ing by mouth. If there is evidence of obstruction or ileus, a nasogastric tube should be inserted. Broad-spectrum intravenous antibiotic coverage is appropriate (Table 1).
If there is no improvement in pain, fever, and leukocytosis within 2 or 3 days, or if serial phys-ical examinations reveal new findings or evidence of worsening, repeat CT imaging is appropriate,
Figure!3.!CT!Scans!of!the!Colon!in!Four!Patients!!with!Diverticulitis!of!Varying!Severity.!
Panel A shows diverticula (arrow) and evidence of in-flammation and wall thickening (arrowhead), findings that are consistent with Hinchey stage 1 disease. Panel B shows a peridiverticular abscess (circled), a finding consistent with stage 2 disease. Panel C shows a drain within a large, confined diverticular abscess (circled) that communicated with the colon, which is consistent with stage 3 disease. Panel D shows evidence of free perforation (arrows) near thickened descending colon, a finding that is consistent with stage 3 or 4 disease. Images courtesy of Dr. Erik Paulson, Department of Radiology, Duke University Medical Center.
16p6
AUTHORFIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASEEMail Line
H/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
11-15-07
mleahy
35720
A
B
D
C
JacobsFig 3 a_d
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
clinical pr actice
n engl j med 357;20 www.nejm.org november 15, 2007 2059
may have atypical signs and symptoms, are more likely to have free perforation, are less likely to have a response to conservative management, and have higher postoperative risks of complications and death than immunocompetent patients.2,14
Di agnosis a nd E va luation
The clinical manifestations of acute colonic diver-ticulitis vary with the extent of the disease process. In classic cases, patients report obstipation and ab-dominal pain that localizes to the left lower quad-rant. An abdominal or perirectal fullness, or “mass effect,” may be apparent. Stool guaiac testing may be trace-positive. A low-grade fever is common, as is leukocytosis.
Alternative diagnoses for lower abdominal pain must be considered. Sigmoid diverticulitis may mimic acute appendicitis if the colon is redundant or otherwise configured such that the inflamed portion resides in the suprapubic region of the right lower quadrant. Inflammatory bowel disease (especially Crohn’s disease), pelvic inflammatory disease, tubal pregnancy, cystitis, advanced colonic cancer, and infectious colitis may also have pre-sentations similar to that of diverticulitis.
Patients with free perforation have peritoneal irritation, including marked abdominal tenderness that begins suddenly and spreads rapidly to involve the entire abdomen with guarding and involun-tary rigidity. Peritonitis is an indication for emer-gency surgical exploration.
StagingThe severity of diverticulitis is often graded with the use of Hinchey’s criteria (Fig. 2), although this classification system does not take into account the effects of coexisting conditions on disease sever-ity or outcome. The risk of death is less than 5% for most patients with stage 1 or 2 diverticulitis, ap-proximately 13% for those with stage 3, and 43% for those with stage 4.15
Imaging and EndoscopyComputed tomography (CT) is recommended as the initial radiologic examination (Fig. 3). It has high sensitivity (approximately 93 to 97%) and specificity approaching 100% for the diagno-sis,16,17 and it allows delineation of the extent of the disease process.18,19 In occasional cases, when
it is difficult to distinguish between diverticulitis and carcinoma, limited contrast studies of the de-scending colon and rectum with the use of water-soluble contrast material may be helpful. The pres-ence of diverticula, inflammation of the pericolic fat or other tissues, bowel-wall thickness of more than 4 mm, or a peridiverticular abscess strongly suggests diverticulitis.2 CT may also reveal other disease processes accounting for lower abdominal pain, such as appendicitis, tubo-ovarian abscess, or Crohn’s disease.
Colonoscopy and sigmoidoscopy are typically
Figure!2.!Hinchey!Classification!Scheme.
Patients with stage 1 disease have small, confined pericolic or mesenteric abscesses, whereas those with stage 2 disease have larger abscesses, often confined to the pelvis. Stage 3 disease, or perforated diverticulitis, is pres-ent when a peridiverticular abscess has ruptured and caused purulent peritonitis. Rupture of an uninflamed and unobstructed diverticulum into the free peritoneal cavity with fecal contamination, the so-called free rup-ture, signifies stage 4 disease and carries the highest risk of an adverse outcome.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
Hinchey 3
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072060
avoided when acute diverticulitis is suspected be-cause of the risk of perforation or other exacerba-tion of the disease process. Expert opinion is in favor of performing these tests when the acute process has resolved, usually after approximately 6 weeks, to rule out the presence of other diseases, such as cancer and inflammatory bowel disease.
HospitalizationThe decision to hospitalize a patient for diverticu-litis depends on the patient’s clinical status. For most patients (i.e., immunocompetent patients who have a mild attack and can tolerate oral intake), outpatient therapy is reasonable. This involves 7 to 10 days of oral broad-spectrum antimicrobial ther-apy, including coverage against anaerobic micro-organisms. A combination of ciprofloxacin and metronidazole is often used, but other regimens are also effective (Table 1). A low-residue liquid diet (i.e., one largely free of indigestible matter) is also commonly recommended, although this approach has not been rigorously studied.
Hospitalization is indicated if the patient is unable to tolerate oral intake or has pain severe enough to require narcotic analgesia, if symp-toms fail to improve despite adequate outpatient therapy, or if the patient has complicated diver-ticulitis. The patient should initially take noth-ing by mouth. If there is evidence of obstruction or ileus, a nasogastric tube should be inserted. Broad-spectrum intravenous antibiotic coverage is appropriate (Table 1).
If there is no improvement in pain, fever, and leukocytosis within 2 or 3 days, or if serial phys-ical examinations reveal new findings or evidence of worsening, repeat CT imaging is appropriate,
Figure!3.!CT!Scans!of!the!Colon!in!Four!Patients!!with!Diverticulitis!of!Varying!Severity.!
Panel A shows diverticula (arrow) and evidence of in-flammation and wall thickening (arrowhead), findings that are consistent with Hinchey stage 1 disease. Panel B shows a peridiverticular abscess (circled), a finding consistent with stage 2 disease. Panel C shows a drain within a large, confined diverticular abscess (circled) that communicated with the colon, which is consistent with stage 3 disease. Panel D shows evidence of free perforation (arrows) near thickened descending colon, a finding that is consistent with stage 3 or 4 disease. Images courtesy of Dr. Erik Paulson, Department of Radiology, Duke University Medical Center.
16p6
AUTHORFIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASEEMail Line
H/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
11-15-07
mleahy
35720
A
B
D
C
JacobsFig 3 a_d
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
clinical pr actice
n engl j med 357;20 www.nejm.org november 15, 2007 2059
may have atypical signs and symptoms, are more likely to have free perforation, are less likely to have a response to conservative management, and have higher postoperative risks of complications and death than immunocompetent patients.2,14
Di agnosis a nd E va luation
The clinical manifestations of acute colonic diver-ticulitis vary with the extent of the disease process. In classic cases, patients report obstipation and ab-dominal pain that localizes to the left lower quad-rant. An abdominal or perirectal fullness, or “mass effect,” may be apparent. Stool guaiac testing may be trace-positive. A low-grade fever is common, as is leukocytosis.
Alternative diagnoses for lower abdominal pain must be considered. Sigmoid diverticulitis may mimic acute appendicitis if the colon is redundant or otherwise configured such that the inflamed portion resides in the suprapubic region of the right lower quadrant. Inflammatory bowel disease (especially Crohn’s disease), pelvic inflammatory disease, tubal pregnancy, cystitis, advanced colonic cancer, and infectious colitis may also have pre-sentations similar to that of diverticulitis.
Patients with free perforation have peritoneal irritation, including marked abdominal tenderness that begins suddenly and spreads rapidly to involve the entire abdomen with guarding and involun-tary rigidity. Peritonitis is an indication for emer-gency surgical exploration.
StagingThe severity of diverticulitis is often graded with the use of Hinchey’s criteria (Fig. 2), although this classification system does not take into account the effects of coexisting conditions on disease sever-ity or outcome. The risk of death is less than 5% for most patients with stage 1 or 2 diverticulitis, ap-proximately 13% for those with stage 3, and 43% for those with stage 4.15
Imaging and EndoscopyComputed tomography (CT) is recommended as the initial radiologic examination (Fig. 3). It has high sensitivity (approximately 93 to 97%) and specificity approaching 100% for the diagno-sis,16,17 and it allows delineation of the extent of the disease process.18,19 In occasional cases, when
it is difficult to distinguish between diverticulitis and carcinoma, limited contrast studies of the de-scending colon and rectum with the use of water-soluble contrast material may be helpful. The pres-ence of diverticula, inflammation of the pericolic fat or other tissues, bowel-wall thickness of more than 4 mm, or a peridiverticular abscess strongly suggests diverticulitis.2 CT may also reveal other disease processes accounting for lower abdominal pain, such as appendicitis, tubo-ovarian abscess, or Crohn’s disease.
Colonoscopy and sigmoidoscopy are typically
Figure!2.!Hinchey!Classification!Scheme.
Patients with stage 1 disease have small, confined pericolic or mesenteric abscesses, whereas those with stage 2 disease have larger abscesses, often confined to the pelvis. Stage 3 disease, or perforated diverticulitis, is pres-ent when a peridiverticular abscess has ruptured and caused purulent peritonitis. Rupture of an uninflamed and unobstructed diverticulum into the free peritoneal cavity with fecal contamination, the so-called free rup-ture, signifies stage 4 disease and carries the highest risk of an adverse outcome.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
Hinchey 4
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

TRATAMIENTO
• TRATAMIENTO
• NO COMPLICADA
• 75% de los casos
• 30% requieren cirugía
www.uptodate.com
COMPLICADA
25% con primer cuadro de diverticulitis

DIVERTICULITIS NO COMPLICADA
•
Tratamiento Médico
Extrahospitalario Intrahospitalario
www.uptodate.com

•
Tratamiento Médico
Extrahospitalario Intrahospitalario
www.uptodate.com
El tratamiento médico tiene de 70 a 100% de éxito

•
Tratamiento Médico
Extrahospitalario Intrahospitalario
www.uptodate.com
El tratamiento médico tiene de 70 a 100% de éxito

• Tratamiento intrahospitalario
• Enfermedad severa
• Ancianos
• Inmunodeprimidos
• Comorbilidades importantes
• Fiebre o leucocitosis www.uptodate.com

• Antibióticos
• Anaerobios
• B. fragilis, peptoestreptococos, clostridium, fusobacterias
• Gram negativos
• E. coli
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.
*Clindamicina
*
*
No respondedores-Enterococo: Ampicilina
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
clinical pr actice
n engl j med 357;20 www.nejm.org november 15, 2007 2061
and percutaneous or operative intervention may be required. Surgical consultation is indicated when the disease does not respond to medical manage-ment or there are repeated attacks; when there is abscess or fistula formation, obstruction, or free perforation20; or when there is uncertainty regard-ing the diagnosis.
Percutaneous DrainageFor patients in whom diverticulitis is complicated by peridiverticular abscess formation, the size of the abscess is an important determinant of the need for percutaneous drainage. Many patients who have small pericolic abscesses (4 cm or less in diameter) without peritonitis (Hinchey stage 1) can be treated conservatively with bowel rest and broad-spectrum antibiotics.21 For patients with peridiverticular abscesses that are larger than 4 cm in diameter22,23 (Hinchey stage 2), observation-al studies indicate that CT-guided percutaneous drainage can be beneficial. This procedure typi-cally eliminates or reduces the size of the ab-scess,21,24,25 with a reduction in pain, resolution of leukocytosis, and defervescence usually seen within several days.26 Percutaneous drainage may allow for elective rather than emergency surgery, increas-
ing the likelihood of a successful one-stage pro-cedure. Patients whose abscess cavities contain gross feculent material tend to respond poorly, and early surgical intervention is usually required.
Operative InterventionFewer than 10% of patients admitted with acute diverticulitis require surgical treatment during the same admission.5 The indications for and timing of surgery for diverticular disease are determined primarily by the severity of the disease, but other factors, including age and coexisting conditions, should also be considered.
The indications for emergency operative treat-ment include generalized peritonitis, uncontrolled sepsis, uncontained visceral perforation, the pres-ence of a large, undrainable (inaccessible) abscess, and lack of improvement or deterioration within 3 days of medical management; these features are characteristic of Hinchey stage 3 or 4 disease. In the past, three separate sequential operations were performed in patients with these complications (Fig. 4), but this course of treatment is no longer recommended for most patients because of high associated morbidity and mortality.27,28 With this approach, many patients, especially those who are
Table!1.!Some!Regimens!Commonly!Used!to!Treat!Diverticulitis.*
Drug!Regimen Dosage
Oral!regimens!for!outpatients
Metronidazole and a quinolone Metronidazole — 500 mg every 6 to 8 hr
Quinolone (e.g., ciprofloxacin — 500–750 mg every 12 hr)†
Metronidazole and trimethoprim–sulfamethoxazole Metronidazole — 500 mg every 6 to 8 hr
Trimethoprim–sulfamethoxazole — 160 mg trimethoprim and 800 mg sulfamethoxazole every 12 hr†
Amoxicillin–clavulanate Amoxicillin–clavulanate — 875 mg every 12 hr†
Intravenous!regimens!for!inpatients
Metronidazole and a quinolone Metronidazole — 500 mg every 6 to 8 hr
Quinolone (e.g., ciprofloxacin — 400 mg every 12 hr)†
Metronidazole and a third-generation cephalosporin Metronidazole — 500 mg every 6 to 8 hr
Third-generation cephalosporin (e.g., ceftriaxone — 1–2 g every 24 hr)
Beta-lactam with a beta-lactamase inhibitor Beta-lactam with a beta-lactamase inhibitor (e.g., ampicillin–sulbactam — 3 g every 6 hr)†
* All doses are for adults. This list is not exhaustive. † Dose adjustment may be needed, depending on the presence and degree of renal failure.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
• Pacientes externos

clinical pr actice
n engl j med 357;20 www.nejm.org november 15, 2007 2061
and percutaneous or operative intervention may be required. Surgical consultation is indicated when the disease does not respond to medical manage-ment or there are repeated attacks; when there is abscess or fistula formation, obstruction, or free perforation20; or when there is uncertainty regard-ing the diagnosis.
Percutaneous DrainageFor patients in whom diverticulitis is complicated by peridiverticular abscess formation, the size of the abscess is an important determinant of the need for percutaneous drainage. Many patients who have small pericolic abscesses (4 cm or less in diameter) without peritonitis (Hinchey stage 1) can be treated conservatively with bowel rest and broad-spectrum antibiotics.21 For patients with peridiverticular abscesses that are larger than 4 cm in diameter22,23 (Hinchey stage 2), observation-al studies indicate that CT-guided percutaneous drainage can be beneficial. This procedure typi-cally eliminates or reduces the size of the ab-scess,21,24,25 with a reduction in pain, resolution of leukocytosis, and defervescence usually seen within several days.26 Percutaneous drainage may allow for elective rather than emergency surgery, increas-
ing the likelihood of a successful one-stage pro-cedure. Patients whose abscess cavities contain gross feculent material tend to respond poorly, and early surgical intervention is usually required.
Operative InterventionFewer than 10% of patients admitted with acute diverticulitis require surgical treatment during the same admission.5 The indications for and timing of surgery for diverticular disease are determined primarily by the severity of the disease, but other factors, including age and coexisting conditions, should also be considered.
The indications for emergency operative treat-ment include generalized peritonitis, uncontrolled sepsis, uncontained visceral perforation, the pres-ence of a large, undrainable (inaccessible) abscess, and lack of improvement or deterioration within 3 days of medical management; these features are characteristic of Hinchey stage 3 or 4 disease. In the past, three separate sequential operations were performed in patients with these complications (Fig. 4), but this course of treatment is no longer recommended for most patients because of high associated morbidity and mortality.27,28 With this approach, many patients, especially those who are
Table!1.!Some!Regimens!Commonly!Used!to!Treat!Diverticulitis.*
Drug!Regimen Dosage
Oral!regimens!for!outpatients
Metronidazole and a quinolone Metronidazole — 500 mg every 6 to 8 hr
Quinolone (e.g., ciprofloxacin — 500–750 mg every 12 hr)†
Metronidazole and trimethoprim–sulfamethoxazole Metronidazole — 500 mg every 6 to 8 hr
Trimethoprim–sulfamethoxazole — 160 mg trimethoprim and 800 mg sulfamethoxazole every 12 hr†
Amoxicillin–clavulanate Amoxicillin–clavulanate — 875 mg every 12 hr†
Intravenous!regimens!for!inpatients
Metronidazole and a quinolone Metronidazole — 500 mg every 6 to 8 hr
Quinolone (e.g., ciprofloxacin — 400 mg every 12 hr)†
Metronidazole and a third-generation cephalosporin Metronidazole — 500 mg every 6 to 8 hr
Third-generation cephalosporin (e.g., ceftriaxone — 1–2 g every 24 hr)
Beta-lactam with a beta-lactamase inhibitor Beta-lactam with a beta-lactamase inhibitor (e.g., ampicillin–sulbactam — 3 g every 6 hr)†
* All doses are for adults. This list is not exhaustive. † Dose adjustment may be needed, depending on the presence and degree of renal failure.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.
• Pacientes internados
Imipenem (500 mg every six hours) OR meropenem (1 g every eight hours) OR ertapenem (1 g daily)
Monoterapia con carbapenimico
Cambio de acuerdo a resultado de cultivo
• Líquidos claros
• Ayuno + soluciones IV
• SNG en caso de obstrucción o íleo
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

• No hay estudios controlados sobre el uso de agentes antinflamatorios como mesalamina
Floch, MH, White, JA. Management of diverticular disease is changing. World J Gastroenterol 2006; 12:3225.Sheth, AA, Longo, W, Floch, MH. Diverticular disease and diverticulitis. Am J Gastroenterol 2008; 103:1550.

• Cirugía electiva después del primer ataque
• Imnunodeprimidos
• Jóvenes??
www.uptodate.com

• Vigilancia del curso clínico
• sospechar complicaciones si no mejora en 2 a 3 días
• Valorar tratamiento quirúrgico
www.uptodate.com

• Pronóstico después de la resolución
• 30 - 40%..........Permanecen asintomáticos
• 30 - 40%..........Sintomáticos
• 30%...................Segundo episodio
Después del tratamiento médico exitoso del primer episodio
Wolff, B, Chapman, J. Complicated diverticulitis: it is not yet time to rethink the rules!. Ann Surg 2006; 243:708.

• Pronóstico después de la resolución
• 30 - 40%..........Permanecen asintomáticos
• 30 - 40%..........Sintomáticos
• 30%...................Segundo episodio
60% de complicacionesMortalidad se duplica
Después del tratamiento médico exitoso del primer episodio
Wolff, B, Chapman, J. Complicated diverticulitis: it is not yet time to rethink the rules!. Ann Surg 2006; 243:708.

• Pronóstico después de la resolución
• 30 - 40%..........Permanecen asintomáticos
• 30 - 40%..........Sintomáticos
• 30%...................Segundo episodio
60% de complicacionesMortalidad se duplica
Después del tratamiento médico exitoso del primer episodio
Wolff, B, Chapman, J. Complicated diverticulitis: it is not yet time to rethink the rules!. Ann Surg 2006; 243:708.
Tratamiento MédicoQuirúrgico

• Recomendaciones después de la resolución
• Evaluación del colon 6 semanas después
• Extensión de la diverticulosis
• Descartar presencia de neoplasias
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

• Recomendaciones después de la resolución
• Evaluación del colon 6 semanas después
• Extensión de la diverticulosis
• Descartar presencia de neoplasias
COLONOSCOPIA*
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

• Recomendaciones después de la resolución
• Evaluación del colon 6 semanas después
• Extensión de la diverticulosis
• Descartar presencia de neoplasias
COLONOSCOPIA*SIGMOIDOSCOPIA*
+COLON POR ENEMA
www.uptodate.comDanny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

• Recomendaciones después de la resolución
• Evaluación del colon 6 semanas después
• Extensión de la diverticulosis
• Descartar presencia de neoplasias
COLONOSCOPIA*SIGMOIDOSCOPIA*
+COLON POR ENEMA
www.uptodate.com
*Contraindicado en evento agudo
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

DIVERTICULITIS COMPLICADA
• Maniobras de resucitación
• Antibióticos
• Tratamiento quirúrgico
www.uptodate.com

• Maniobras de resucitación
• Antibióticos
• Tratamiento quirúrgico
www.uptodate.com

Ampicilina 2 gr IV c/6 hrsGentamicina 1.5-2 mg/Kg IV c/8 hrs
Metronidazol 500 mgr IV c/8 hrs
Imipenem 500 mg IV c/6hrs
Piperacilina-Tazobactam 3.375 g IV c/6 hrs
www.uptodate.com
Tratamiento Antibiótico

• Maniobras de resucitación
• Antibióticos
• Tratamiento quirúrgico
www.uptodate.com

Indicaciones de Cirugía de Emergencia
Peritonitis generalizadaSepsis
Perforación visceral no contenidaAbsceso amplio no drenable
Falta de mejoría o deterioro en 3 días de tx médico
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.

Indicaciones de Cirugía de Emergencia
Peritonitis generalizadaSepsis
Perforación visceral no contenidaAbsceso amplio no drenable
Falta de mejoría o deterioro en 3 días de tx médico
Hinchey 3-4
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.
Tratamiento Quirúrgico
Emergencia Programada
Hinchey, EJ, Schaal, PG, Richards,GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978; 12:85.

Tratamiento Quirúrgico
Emergencia Programada
Hinchey, EJ, Schaal, PG, Richards,GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978; 12:85.

Tratamiento Quirúrgico
Emergencia Programada
Abierta
Hinchey, EJ, Schaal, PG, Richards,GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978; 12:85.

Tratamiento Quirúrgico
Emergencia Programada
Abierta
Hinchey, EJ, Schaal, PG, Richards,GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978; 12:85.

Tratamiento Quirúrgico
Emergencia Programada
Abierta Pb laparoscopiaAbierta
Hinchey, EJ, Schaal, PG, Richards,GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978; 12:85.
Tratamiento Quirúrgico
Emergencia Programada
Abierta Pb laparoscopiaAbierta
La clasificación de Hinchey determina la posibilidad de anastomosis primaria
Hinchey, EJ, Schaal, PG, Richards,GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978; 12:85.

Tratamiento Quirúrgico
Emergencia Programada
Abierta Pb laparoscopiaAbierta
La clasificación de Hinchey determina la posibilidad de anastomosis primaria
Hinchey, EJ, Schaal, PG, Richards,GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978; 12:85.
Hinchey I y II pueden tener preparación preoperatoria

• Preparación preoperatoria
• Antibióticos
• Cefalosporina de 2a o 3a generación
• En contaminación extensa se utiliza esquema para peritonitis
www.uptodate.com

Hinchey Procedimiento % Fuga % Morbilidad global
1Resección con anastomosis
primaria3.8 22
2Resección con anastomosis
primaria +/- estoma3.8 30
3Hartmann vs colostomía de derivación y colocación de un injerto de epiplón
--- Mortalidad 0 vs 6
4Hartmann vs colostomía de derivación e injerto de pedículo epiploico
--- Mortalidad 6 vs 2
Evolución después del Tratamiento Quirúrgico de la Enfermedad Diverticular complicada
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;20 www.nejm.org november 15, 20072064
intervention.38,44 A recent retrospective study sug-gests that patients with two or more episodes of uncomplicated diverticulitis are not at increased risk for poor outcomes if complications do not develop.45
In patients with diverticulosis, a fiber-rich diet, with or without long-term suppressive therapy with oral antibiotics, may be recommended to re-duce intracolonic pressure and reduce the risk of recurrence. Epidemiologic data and the results of a small, randomized, controlled trial involving 18 patients suggest that a high-fiber diet is ben-eficial,46 but conclusive data are lacking and prac-tice standards vary widely.47
Guidel ines
The American Society of Colon and Rectal Sur-geons has published practice guidelines48; rec-
ommendations in this article are generally con-sistent with those guidelines. According to the Surgical Infection Society, treatment with intra-venous antibiotics for 5 to 7 days is as effective as longer regimens.49
Conclusions a nd R ecommendations
The patient in the vignette is unable to hydrate him-self orally and should therefore be hospitalized. He should initially receive nothing by mouth and should be treated with intravenous fluids and broad-spectrum antibiotics (e.g., ciprofloxacin and metronidazole). A CT scan of the abdomen should be obtained; on the basis of the patient’s presen-tation, it would probably show Hinchey stage 1 or 2 disease. Prompt resolution of his signs and symp-toms can be expected within several days. If the
Figure!5.!Two-Stage!Operative!Approach!to!Diverticulitis.
During the first operation, the diseased segment of bowel is resected, an end colostomy is performed, and the dis-tal rectal stump is oversewn (Hartmann’s procedure). During a second procedure, colonic continuity is reestab-lished. The margin of resection should include the entire sigmoid colon — where the distal resection margin ex-tends to or just below the the distal portion of the peritoneum at the rectum — to reduce the risk of recurrence.
Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by ADRIANA BIOLOSTOZKY MD on August 31, 2009 .
Procedimiento de Hartmann
Danny O, Jacobs MD. Diverticulitis. N Engl J Med. 2007; 357: 2057-66.
• Cirugía
• mortalidad del 1.3 a 5 %
• severidad
• comorbilidades
www.uptodate.com
• 15% presenta progresión de la diverticulosis después de la cirugía
• 2-11% nueva intervención
• <27% continuan con síntomas debido a síndrome de intestino irritable
Wolff, BG, Ready, RL, MacCarty, RL, et al. Influence of sigmoid resection on progression of diverticular disease of the colon. Dis Colon Rectum 1984; 27:645.

Diverticulitis Complicada
AbscesoPerforaciónObstrucción/EstenosisFístula
16%10%5%2%
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

• Abscesos
• Drenaje percutaneo en > 4 cm
• el catéter permanece hasta lograr 10 cc/24 hrs (hasta 30 días)
Neff, CC, van Sonnenberg, E, Casola, G, et al. Diverticular abscesses: Percutaneous drainage. Radiology 1987; 163:15.

• Contraindicaciones del drenaje
• Ausencia de ruta de acceso
• Neumoperitoneo
• Peritonitis fecal
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
• Abscesos menores de 3 cm se pueden tratar con antibióticos
• en 22 pacientes con tx antibiótico:
• 41% resolución completa
• 36% cirugía
• 23% recurrencia o persistencia de los síntomas
Siewert, B, Tye, G, Kruskal, J, et al. Impact of CT-guided drainage in the treatment of diverticular abscesses: size matters. AJR Am J Roentgenol 2006; 186:680.

• Perforación
• mortalidad 20-30%
• tratamiento quirúrgico
www.uptodate.com

• Obstrucción/Estenosis
• rara vez es completa
• investigar carcinoma
• resección
www.uptodate.com

DIVERTICULOSIS

• Dieta rica en fibra
• 30 g de fibra al día
• Suplementos de fibra
• Metamucil
• Evitar ingesta de semillas (?)
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

SANGRADO

• Sangrado Diverticular
• no doloroso
• autolimitado
• 50% pueden tener hematoquezia
• es raro que coincida con diverticulitis aguda
• Más común en colon derecho. Tratamiento con colectomía total
www.uptodate.comHarrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.

ACP derecha
Localización con angiografíaEl tx con coil tiene 80% de éxito
Alternativamente se puede realizar resección oinfusión selectiva de vasopresina (isquemia, recurrencia en 50%)
Harrison's Principles of Internal Medicine, 17th Edition by Anthony S. Fauci, Eugene Braunwald, Dennis L. Kasper, and Stephen L. Hauser, 2008, Chapter 291.
Riesgo de isquemia <10%Riesgo de resangrado agudo <25%












![Pneumonia [Harrison's]](https://img.pdfslide.us/doc/110x75/54515befb1af9f83248b46c1/pneumonia-harrisons.jpg)