Embed Size (px)
Citation preview

Diuretics

Diuretics
Diuretics are drugs which increase sodium and water excretion
by the kidney.
The term ‘diuresis’ means increased urine flow, while the term
‘saluresis’ means increased urinary sodium excretion.
All diuretics increase the excretion of water from the body,
although each class of diuretic does so in a distinct way.
Chemically, diuretics are a diverse group of compounds that
either stimulate or inhibit various hormones that naturally occur
in the body to regulate urine production by the kidneys.

The primary therapeutic goal of diuretic use is to reduce edema by reducing the
ECF volume.
1. For this to occur, NaCl output must exceed NaCl intake.
2. Diuretics primarily prevent Na+ entry into the tubule cell.
Once a diuretic enters the tubule fluid, the nephron site at which it acts
determines its effect.
In addition, the site of action also determines which electrolytes, other than
Na+, will be affected. All diuretics except spironolactone exert their effects
from the luminal (tubule fluid) side of the nephron.

Hence, it is necessary for diuretics to get into the
tubule fluid in order to be effective.
Mannitol does this by filtration at the glomerulus, however,
all other diuretics (except spironolactone) are fairly tightly
protein bound and undergo little filtration.
They reach the urine by secretion across the proximal
tubule via the organic acid or organic base secretory
pathway.

ROLE OF THE NEPHRON1. Kidneys control the extracellular fluid (ECF) volume by
adjusting NaCl and H2O excretion.
2. Each day the kidney filters more than 22 moles of Na.
To maintain NaCl balance, approximately 3 lbs of NaCl
must be reabsorbed by the renal tubules on a daily basis.
3. The body maintains blood pressure at the expense of ECF
volume.

4. When NaCl intake > output, i.e. congestive heart failure or
renal failure, edema develops.
5. Na+ reabsorption is driven primarily by Na+/K+
adenosine triphosphatase (ATPase) located at the
basolateral (blood side) membrane of epithelial cells
throughout the nephron.
6. The Na+/K+ is an energy-requiring pump which
exchanges 1 Na+ for 2 K+, thereby keeping a low Na+
concentration and a high K+ concentration within the cell.

7. On the luminal side, cell-specific pathways exist forpassive movement of Na+ down its electrochemicalgradient from lumen to cell.
These cells form the physiologic basis of diuretic action.



Acetazolamide
N-(5-sulfamoyl-1,3,4-thiadiazol-2-yl)acetamide

Furosemide
4-Chloro-2-[(furan-2-ylmethyl)amino]-5-sulfamoylbenzoic acid

Ethacrynic acid


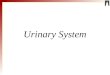
Carbonic Anhydrase InhibitorsMechanism of action
Bicarbonate is primarily reabsorbed in the proximal tubule. H+
ion is secreted into the lumen where it can combine with filtered
bicarbonate (HCO3-) to form H2CO3 that is then converted to
CO2 and H2O (catalyzed by carbonic anhydrase).
CO2 diffuses into the proximal tubule where it combines with
H2O to form H2CO3 (Carbonic acid) that then forms H+ and
HCO3-. HCO3- exits the proximal tubule on the blood side,
while H+ is again secreted into the tubule lumen.


If CA activity is inhibited, HCO3- reabsorption is reduced and
exits the proximal tubule in much larger amounts.
Because Na+ is the most abundant cation present in proximal
tubule fluid, it is the major cation which accompanies HCO3 -
out of the proximal tubule.
In the distal nephron, Na+ is largely reabsorbed (unlike HCO3 -)
and is exchanged for K+.
Therefore, acetazolamide primarily causes an increase in urinary
HCO3-, K+, and water excretion.
Effectiveness is reduced with continued therapy because plasma
[HCO3-] fall, reducing the amount of HCO3 - that appears in the
urine.



Structure–activity relationship Site1 Carbonic anhydrate inhibitors acetazolamide,methazolamide


1. Simple heterocyclic sulfonamides yielded the
prototypic carbonic anhydrase inhibitor
acetazolamide.
2. The sulfamoyl group is essential for the in vitro and
in vivo carbonic anhydrase activity.
3. The sulfamoyl nitrogen must remain unsubstituted
to retain both in vivo and in vitro activities.

4. Substitution of a methyl group on one of acetazolamide’s
ring nitrogen yields methazolamide retains carbonic
anhydrase inhibitory activity.
5. The moiety to which sulfamoyl group is attached must
possess aromatic character.
6. Heterocyclic sulfonamide, the derivative with highest
lipid/water partition coefficient and the lowest pKa values
has the greatest carbonic anhydrase activity and diuretic
activity.

Uses
1. Although acetazolamide is used for treatment of edema, the efficacy
of carbonic anhydrase inhibitors as single agents is low, and carbonic
anhydrase inhibitors are not employed widely in this regard.
2. However, studies indicate that the combination of acetazolamide
with diuretics that block Na+ reabsorption at more distal sites in the
nephron causes a marked response in patients who are resistant to
diuretic monotherapy.
3. Even so, the long-term usefulness of carbonic anhydrase
inhibitors often is compromised by the development of
metabolic acidosis.

Site 2 High ceiling or loop diuretics

Furosemide, Bumetanide and Ethacrynic Acid (LoopDiuretics)
Drugs in this group of diuretics inhibit the activity of the
Na+-K+-2Cl- symporter in the thick ascending limb of the
loop of Henle; hence these diuretics also are referred to as
loop diuretics.
Proximal tubule reabsorbs 65% of filtered Na+, diuretics
acting only in the proximal tubule have limited efficacy
because the thick ascending limb has a great reabsorptive
capacity and reabsorbs most of the rejectate from the
proximal tubule.

Diuretics acting predominantly at sites past the thick
ascending limb also have limited efficacy because only a
small percentage of the filtered Na+ load reaches these
more distal sites.
In contrast, inhibitors of Na+ – K+ – 2Cl– symport in the
thick ascending limb are highly efficacious, and for this
reason, they sometimes are called high-ceiling diuretics.

The efficacy of inhibitors of Na+ – K+ – 2Cl– symport in
the thick ascending limb of the loop of Henle is due to a
combination of two factors:
1. Approximately 25% of the filtered Na+ load normally is
reabsorbed by the thick ascending limb.
2. Nephron segments past the thick ascending limb do not
possess the reabsorptive capacity to rescue the flood of
rejectate exiting the thick ascending limb.


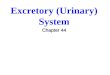
Furosemide and others act primarily in the thick ascending limb
and inhibit Na+ – K+ Cl – symport.
In the thick ascending limb, flux of Na+ – K+ and Cl- from the lumeninto the epithelial cell is mediated by Na+ – K+ 2Cl- symporter.
This symporter captures the energy in the Na+ electrochemical
gradient established by the basolateral Na+ pump and provides for
up hill transport of K+ and Cl– into the cell.
K+ channels in the luminal membrane provide a conductivepathway for the optical recycling of this cation and basolateral Cl–channels provide a basolateral exit mechanism for Cl–.

Inhibition of Na+ – K+ –2 Cl– symport binds to the Na+ – K+ – 2Cl–
symporter and blocks its function, bringing salt transport in this
segment of nephron to virtual stand still.
It is suggested that these drugs attach to the binding site of the
symporter.
The Na+ – K+– 2Cl– symporter has amino acid sequence of 1191
residues containing 12 putative membranes – spanning domains flanked
by long N and C termini in the cytoplasm.

NaCl reabsorption in thick ascending limb and mechanism of diureticaction of NaCl reabsorption in thick ascending limb and mechanism ofdiuretic action of Na+ – K+ – 2Cl– symport inhibitors. S = symporter, CH =ion channel

2-[2,3-dichloro-4-(2-methylidenebutanoyl)phenoxy]acetic acid

4-Chloro-2-[(furan-2-ylmethyl)amino]-5-sulfamoylbenzoic acid
3-butylamino-4-phenoxy-5-sulfamoyl-benzoic acid

2-chloro-5-(2H-tetrazol-5-yl)-4-[(thiophen-2-ylmethyl)amino]benzenesulfonamide

Uses
1. A major use of loop diuretics is in the treatment of acute pulmonary edema.
A rapid increase in venous capacitance in conjunction with a brisk
natriuresis reduces left ventricular filling pressures and thereby rapidly
relieves pulmonary edema.
2. Loop diuretics are also used widely for the treatment of chronic congestive
heart failure when diminution of extracellular fluid volume is desirable to
minimize venous and pulmonary congestion.
3. In this regard, a meta-analysis of randomized clinical trials demonstrates that
diuretics cause a significant reduction in mortality and the risk of worsening
heart failure, as well as an improvement in exercise capacity.

Adverse effect
Over use of these drugs can cause hyponatremia,
hypotension and circulatory collapse.
They can cause ototoxicity, vertigo. Drug interaction
may occur with aminoglycosides, propranolol,
probencid and thiazide diuretics.

Site 3 Thiazide and Thiazide like diuretics
MEDIUM EFFICACY DIURETICS
(Thiazides, Hydrothiazides and Thiazide-like Diuretics)
Chemistry
Inhibitors of Na+–Cl- symport are sulfonamides, and many are
analogues of 1, 2, 4-benzothiadiazine-1,1-dioxide.
Original inhibitors of Na+–Cl- symport were benzothiadiazine
derivatives, known as thiazide diuretics.
Drugs that are pharmacologically similar to thiazide diuretics are
called thiazide-like diuretics. The term thiazide diuretic is used here
to refer to all members of the class of inhibitors of Na+–Cl- symport.

Mechanism of action
The primary site of action of thiazide is the distal convulated tubule,
whereas the proximal tubule may represent a secondary site of
action.
In the distal convulated tubule, transport is powered by an Na+
pump in the basolateral membrane.
Cl then passively exists the basolateral membrane via a chloride
channel.


Thiazide diuretics inhibit the Na+–Cl–symporter,perhaps by competing for the chloride binding site.
The Na+ –Cl– symporter has a predicted size of 1023amino acid residues, has 12 putative membrane spanningdomains.
These domains exhibit 12 potential membrane-spanninghelices and they are flanked by long –NH2 and COOHterminal nonhydrophobic domains.

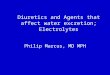
Development of thiazide and hydrothiazide diuretics
from chloraminophenamide

Structure–activity relationship
1. The SO2 group can be replaced with CO with increase in activity.
2. Saturation of 3, 4-double bond increase in activity.
3. Substitution of the ring nitrogen at position 2 with methyl increases
activity. However, at position 4 the methyl group reduces activity
with the heterocyclic ring more vulnerable to heterocyclic cleavage.
4. Substituent in the position 3, hydrophobic in character, increases
1000 times saluretic activity.
thiazide and hydrothiazide


Hydrochlorothiazide Hydroflumethiazide
ChlorothiazideBenzthiazide

5. Substituents include, –CH2Cl, –CHCl2, –CH2C6H5,
CH2CH2S-CH2C6H5. The increase in activity correlates with
the lipid solubility.
6. Substitutions in the 6 position by Cl, Br, or CF3 increase
activity, whereas H, or NH2 are weakly active.
7. A free sulfamoyl or potentially free sulfamoyl group at 7
position is essential for activity.
8. The loss of sulfamoyl group eliminated the diuretic effect, but
not the hypertensive effect.


Uses1. Thiazide diuretics are used for the treatment of the edema
associated with heart (congestive heart failure), liver
(hepatic cirrhosis), and renal (nephrotic syndrome, chronic
renal failure, and acute glomerulonephritis) disease.
2. With the possible exceptions of metolazone and
indapamide, most thiazide diuretics are ineffective when
the GFR is less than 30 to 40 ml/min.

Adverse effect
The most serious adverse effect is extracellular volumedepletion, hypotension, hyponatremia andhypochloremia.

POTASSIUM SPARING DIURETICS OR ANTI-KALIURETIC AGENTS
Inhibitors of renal epithelial Na+ channel. The body as awhole contains more K+ than Na+.
The saluretic diuretic agents also cause a concomitantincrease in K+ excretion; therefore producing hypokalemiais not desired.
Potassium-sparing diuretics produce decrease potassiumand hydrogen ions secretion.
Efforts to discover diuretics that would increase Na+excretion by inhibiting its exchange with K+ in the distalconvulated tubule produced two classes of potassiumsparing agents.
1. Direct acting anti-kaliuretic agents. 2. Aldosterone antagonist



Direct Acting Anti-KaliureticMechanism of action
These agents are used in combination with otherdiuretic agents (thiazide) for the treatment ofhypertension, edema associated with chroniccongestive heart failure or cirrhosis.
These agents inhibit active Na+ reabsorption.
The increased excretion of Na+ and Cl disrupts normalNa+ transport and produces a net change in theelectrogenic force across tubular a membrane, whichsubsequently reduces the net driving force for K+secretion.
Their action is independent of aldosterone.


Uses Because of the mild natriuresis induced by Na+-channel
inhibitors, these drugs seldom are used as sole agents inthe treatment of edema or hypertension.
Rather, their major utility is in combination with otherdiuretics. Coadministration of an Na+-channel inhibitoraugments the diuretic and antihypertensive response tothiazide and loop diuretics.
More important, the ability of Na+-channel inhibitors toreduce K+ excretion tends to offset the kaliuretic effects ofthiazide and loop diuretics; consequently, the combinationof an Na+ channel inhibitor with a thiazide or loop diuretictends to result in normal values of plasma K+.

Amiloride is also useful for lithium-inducednephrogenic diabetes insipidus because it blocks Li+transport into the cells of the collecting tubules.

Aldosterone Antagonist
Mechanism of action
Epithelial cells in the late distal tubule and collectingduct contain cytosolic MRs (mineralocorticoids) thathas a high affinity for aldosterone.
This receptor is a member of the superfamily ofreceptors for steroid hormones, thyroid hormones,vitamin D, and retinoids.