Embed Size (px)
Citation preview

Filippo Bogetto Andrea Aguglia
Disturbo bipolare e disturbo
ossessivo-compulsivo

The shift from an obsession to a
delusion may take either:
an affective form a paranoid form
delusional guilt to have
contaminated others
delusion to be persecuted as if
one had actually committed
some reprehensible act
Insel and Akiskal, Am J Psychiatry 1986

1. Prevalenza
!2. Impatto clinico
!3. Implicazioni terapeutiche
Il paziente con disturbo bipolare e
disturbo ossessivo-compulsivo

N=61.392
0
4,5
9
13,5
18
Bipolar Spectrum BD I BD II Subthreshold BD
10,111,8
17,7
12,5
OR=5.7
OR=9.0
OR=6.4
OR=4.1
p = .02
Merikangas et al., Arch Gen Psychiatry 2011; 68: 241-251

0
5
10
15
20
PD Social Phobia OCD
Unipolar Bipolar Sub-bipolar
p=.028
Faravelli et al. J Affect Disord, 2006; 94: 111-119
%
Lifetime comorbidity for anxiety disorders in bipolar,
sub threshold bipolar and unipolar disorder: the
Sesto Fiorentino study

Amerio et al, 2014
Adults: 1.8% - 35.1% !Children and adolescents: 20.7% - 48.5% !Sample size greater than 250 patients: 3% – 13.6%
Amerio et al., Acta Psychiatr Scand 2014; 129: 343-358
Lifetime prevalence rates of OCD in
bipolar patients: clinical studies

Current OCD comorbidity
0
5
10
15
20
All Bipolar Bipolar disorder I Bipolar disorder II
14,8
9,1
12,4
%
Albert et al. J Affect Disord 2008; 105: 297-303
OCD in Bipolar Disorder during euthymic phase
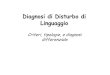
Cederlof et al., Schizophr Bull 2015; in press
OCD=19.814, BD=48.180, SCHZ=58.336, SCHA=14.904
Initial diagnosis of OCD Risk to develop BD or SCHZ or SCHA
Risk to develop OCD Initial diagnosis of BD or SCHZ or SCHA
SCHZ !BP !SCHA

Holma et al. J Clin Psychiatry 2008; 69: 1267-1275

Holma et al. J Clin Psychiatry 2008; 69: 1267-1275
Survival curve of time to diagnostic switch from
unipolar depression to bipolar disorder

%
Serie 1
0
25
50
75
100
OCD Social phobia Agoraphobia PD PTSD
57,9
73,777,8
85,790,5
N=413
Sala et al. J Clin Psychiatry 2012; 73: 87-94
Persistence of anxiety disorders in youth bipolar
patients: a five-years follow-up

1. Prevalenza
!2. Impatto clinico
!3. Implicazioni terapeutiche
Il paziente con disturbo bipolare e
disturbo ossessivo-compulsivo

Maina et al. Psychiatry Res, 2008; 158: 217-225
0
3,5
7
10,5
14
Bipolar I Bipolar II
Early-onsetLate-onset
p=.039
N=148
Early onset for Bipolar - OCD

0
20
40
60
80
Sexual obs Hoarding obs Repeating comp
Bipolar-OCD OCD
p<0,015
p<0,004
p<0,012
% o
f sp
ecifi
c O
C s
ympt
oms
Maina et al., Bipolar Disord 2007; 9: 722-729
N=204
OC symptoms and bipolar disorder
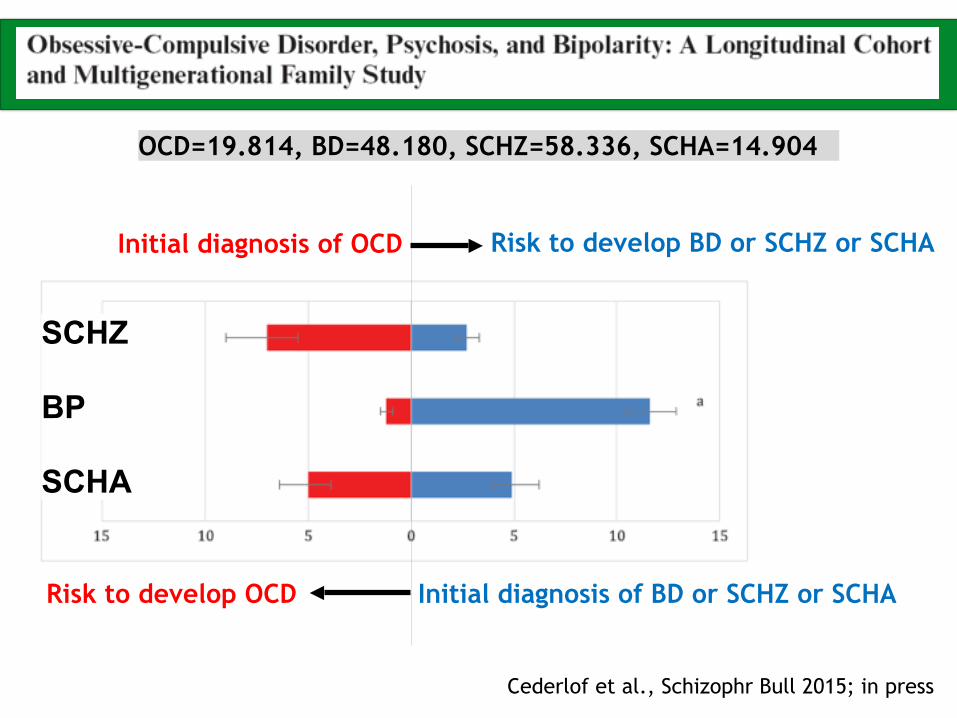
Tukel et al., Depress Anxiety 2006
Comparison of percentage of Bipolar disorder
in episodic and chronic OCD
Episodic course of OCD
0
5
10
15
20
25
4
21 Episodic (N=24) Chronic (N=104)
p=.01

Zutshi et al., Compr Psychiatry 2007; 48: 247-251
m/M
D
improvement of OC symptoms
in 64% of patients
worsening of OC symptoms
in 78% of patients

Perugi et al. J Affect Disord 2001; 67: 199-206
Obsessive-compulsive disorder (N=54)
0
10
20
30
40
50
60
Absent Present
47,852,2
%
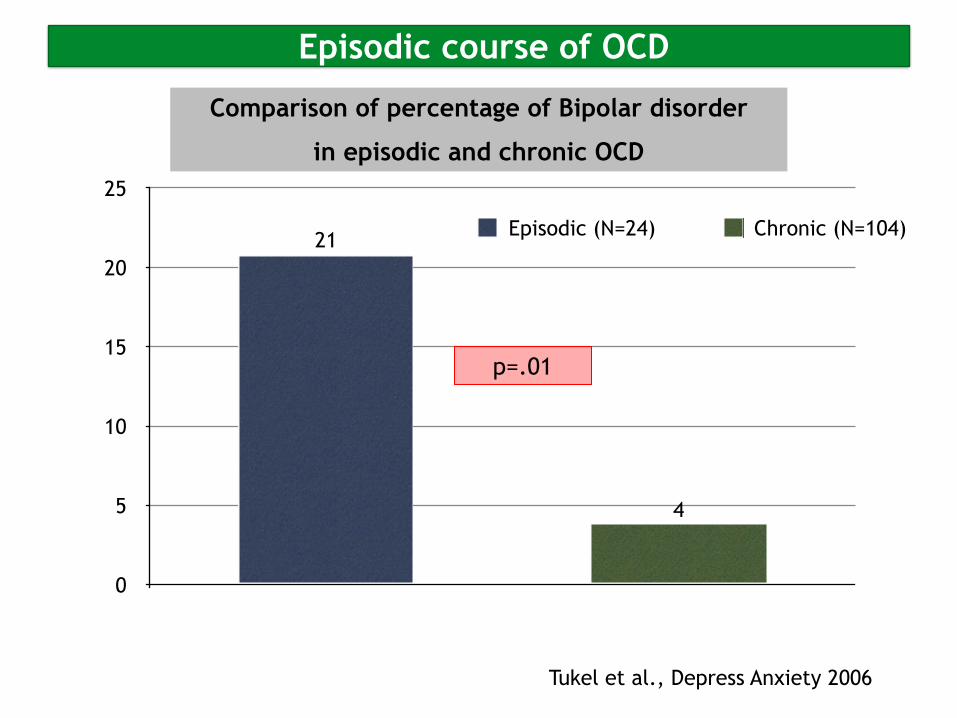
current psychotic symptoms
0
15
30
45
60
Bipolar Bipolar - OCD
30
53,6
p = .01
Shashidhara et al., J Affect Disord 2015; 174: 367-371
%
N=396

Maina et al., Bipolar Disord 2007; 9: 722-729
0
20
40
60
80
Cluster A personality Cluster B Personality More than one Personality disorder
32,829,0
21,3
61,957,0
42,9
BD-OCD OCD
p = .009
%
N=204
p = .027
p = .008

Simon et al, Am J Psychiatry 2004; 161: 2222-2229
OCD comorbid reduces euthymic period
Results from STEP-BD

20
40
60
80
100
Thought of death Thought of suicide Wants to die Attempted suicide
Without OCD With OCD
* P<.05
** P<.01
%
*
*
*
**
Chen & Dilsaver. Am J Psychiatry 1995; 152: 280-282
OCD comorbid increases suicidality

OCD comorbid increases suicidality
Results from STEP-BD
Simon et al, Am J Psychiatry 2004; 161: 2222-2229
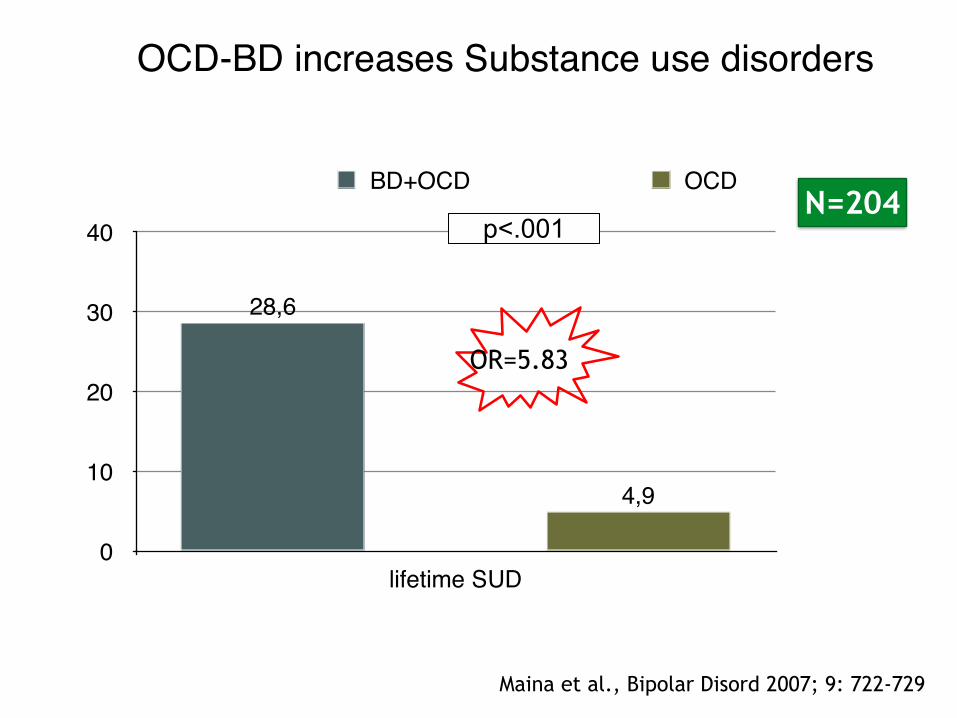
0
10
20
30
40
lifetime SUD
4,9
28,6
BD+OCD OCD
p<.001
OR=5.83
Maina et al., Bipolar Disord 2007; 9: 722-729
N=204
OCD-BD increases Substance use disorders

0
20
40
60
80
Rapid cycling History suicide attempts Lifetime alcohol dependence
no comorbidity anxiety comorbidity OCD comorbidity
Magalhaes et al., Compr Psychiatry 2010; 51: 353-356
%

Centorrino et al. Hum Psychopharmacol Clin Exp 2006; 21: 189–193
0
0,6
1,2
1,8
2,4
Re - hospitalizations/year
2,292,23
0,78
OCD BPD BPD + OCD

*
***
* * *
There is additional impairment due to anxiety in mood disorders
SF-36
N=105
*p≤.05 **p≤.005
Impact of Anxiety Disorder comorbidity on Quality of Life in Euthymic Bipolar Disorder Patients: all bipolar
Albert et al., J Affect Disord 2008; 105: 297-303

*p≤.05 **p≤.005
SF-36
N=61
Impact of Anxiety Disorder comorbidity on Quality of Life in Euthymic Bipolar Disorder Patients: bipolar II
Albert et al., J Affect Disord 2008; 105: 297-303

1. Prevalenza
!2. Impatto clinico
!3. Implicazioni terapeutiche
Il paziente con disturbo bipolare e
disturbo ossessivo-compulsivo

Raja and Azzoni, Bipolar Disord 2004; 6(3): 264-270
100% 42,8% 87,5%
These cases suggest herarchical priority to a bipolar
disorder diagnosis
Clinical management of obsessive-compulsive bipolar
comorbidity: a case series

Offidani et al., Psychother Psychosom 2013; 82: 132-141
Excessive mood elevation and behavioural activation with antidepressant
treatment of juvenile depressive and anxiety disorders: a systematic review

0
4
9
13
17
T0 T6 T12
Olanzapina
0
5
9
14
18
T0 T6 T12
Lamotrigina
HAM
-A s
core
s
HAM
-Asc
ores
N = 24 N = 23
p<0.05 p<0.05
Maina et al., J Clin Psychiatry 2008; 69: 609-614

Schaffer et al, Ann Clin Psychiatry 2012; 24: 6-22
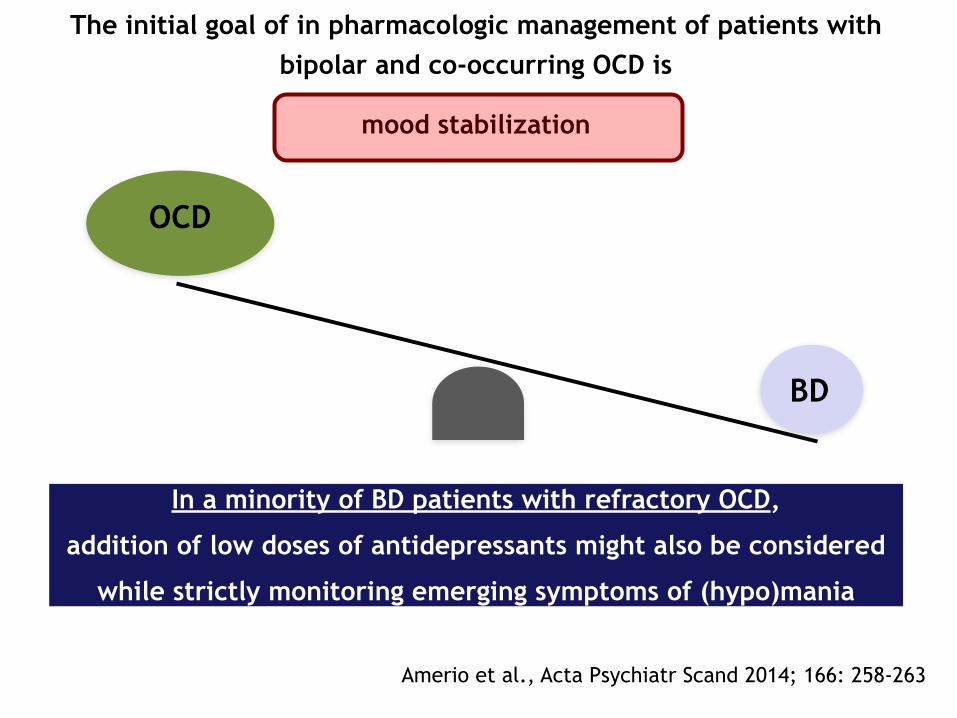
OCD
The initial goal of in pharmacologic management of patients with bipolar and co-occurring OCD is
mood stabilization
BD
In a minority of BD patients with refractory OCD,
addition of low doses of antidepressants might also be considered
while strictly monitoring emerging symptoms of (hypo)mania
Amerio et al., Acta Psychiatr Scand 2014; 166: 258-263

Deckersback et al., Am J Psychiatry 2014; 171: 178-186

Deckersback et al., Am J Psychiatry 2014; 171: 178-186
Obsessive-compulsive disorder

Amerio et al, 2014
BD-OCD is a critical issue in psychiatry;
!
OC symptoms usually are manifestations of depressive or (hypo)manic
mood episodes and persist during euthymic phase;
!
BD-OCD may respond better to mood stabilizers and atypical
antipsychotic: antidepressants should be used only in a minority of
refractory OCD.
Conclusions
Amerio et al., J Affect Disord 2014; 166: 258-263

Duffy et al., Br J Psychiatry 2014; 204: 122-128
Clinical stages in the evolution of bipolar disorder based on high risk studies










![SCID I [modalità compatibilità] - sitcc.it · Disturbo Psicotico breve 6. Disturbo Psicotico dovuto ad una CMG 7. ... Caso clinico SCID I Rassegna: Questo camionista sessantenne](https://img.pdfslide.us/doc/110x75/5baf469709d3f2a8728b8eb6/scid-i-modalita-compatibilita-sitccit-disturbo-psicotico-breve-6-disturbo.jpg)