Embed Size (px)
Citation preview
Distraction Osteogenesis of Multiple Ribs for the Treatment of Acquired Thoracic DystrophyMerisa L. Piper, MD, Lawrence Delrosario, MD, William Y. Hoffman, MD
Division of Plastic and Reconstructive Surgery, Department
of Surgery, University of California, San Francisco, San
Francisco, California
Dr Piper coordinated and supervised data
collection; Drs Piper and Delrosario assisted
in writing the initial manuscript; Drs Piper and
Hoffman reviewed and revised the manuscript; Dr
Delrosario performed the initial data collection;
Dr Hoffman conceptualized and designed the
technique; and all authors approved the fi nal
manuscript as submitted and agree to be
accountable for all aspects of the work.
DOI: 10.1542/peds.2015-2053
Accepted for publication Nov 20, 2015
Address correspondence to William Hoffman, MD,
Division of Plastic Surgery, University of California,
San Francisco, 505 Parnassus Ave, Suite M593, San
Francisco, CA 94143. E-mail: william.hoffman@ucsf.
edu
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright © 2016 by the American Academy of
Pediatrics
FINANCIAL DISCLOSURE: The authors have
indicated they have no fi nancial relationships
relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors
have indicated they have no potential confl icts of
interest to disclose.
Surgical correction of pectus
excavatum has evolved to be less
invasive and cause less morbidity.1,2
Nevertheless, it is still associated
with a variety of complications. A
hypoplastic, abnormally developed
thorax has been described in
patients after repair by the open
Ravitch technique or other modified
open repair techniques on young
children.3–5 The proposed etiology of
this thoracic dystrophy is decreased
longitudinal rib growth resulting from
extensive resection of rib cartilage and
injury to the costochondral junction
in young patients during repair.4,5
The disruption of the cartilage growth
plate limits the growth and proper
development of the chest wall. This
results in decreased thoracic volume
and may cause restricted pulmonary
function and cardiac compression.3,5,6
The optimal treatment approach to
increase thoracic volume by surgical
intervention has been controversial
and must accommodate chest wall
expansion as children continue to
grow.7–13
Distraction osteogenesis, first
presented by Codivilla in 1905 and
revisited by Ilizarov starting in the
1950s,14 describes the phenomenon
in which separation and gentle
traction of skeletal elements
leads to metabolic activation and
eventual bone formation between
the separated skeletal elements.15,16
Distraction osteogenesis has been
used in a wide variety of orthopedic
and craniomaxillofacial applications,
particularly after traumatic injury or
from congenital deformities. Here, we
present the case of a 17-year-old boy
with symptomatic acquired thoracic
dystrophy after repair of pectus
excavatum who was successfully
treated with distraction osteogenesis.
abstractAcquired thoracic dystrophy is a complication associated with early open
repair of pectus excavatum resulting from extensive cartilage resection.
The condition can cause serious functional and physiologic impairments,
including cardiac compression and restrictive pulmonary function.
We describe a 17-year-old boy with acquired thoracic dystrophy after
Ravitch repair of pectus excavatum during infancy, whom we treated
with distraction osteogenesis. The patient had a marked deformity of the
chest wall and general hypoplasia of the central portion of the ribcage,
with resultant symptomatic dyspnea on exertion and reduced pulmonary
function. After osteotomies and distraction osteogenesis of bilateral
ribs 4–8 using customized distraction devices, he had improved thoracic
contour, resolution of dyspnea, and decreased restrictive pulmonary
symptoms. This case suggests that distraction osteogenesis, already used
extensively in craniomaxillofacial and orthopedic surgery, may be a novel
method for management of this condition.
CASE REPORTPEDIATRICS Volume 137 , number 3 , March 2016 :e 20152053
To cite: Piper ML, Delrosario L, Hoffman WY.
Distraction Osteogenesis of Multiple Ribs for
the Treatment of Acquired Thoracic Dystrophy.
Pediatrics. 2016;137(3):e20152053
by guest on June 25, 2018www.aappublications.org/newsDownloaded from
PIPER et al
PATIENT DESCRIPTION
The patient initially presented to the
plastic surgery service at University
of California, San Francisco, at
age 11 years for consultation for
arrested sternal growth after a
Ravitch repair of pectus excavatum
at age 2. This deficient growth led
to inadequate bony protection of
the heart and upper abdominal
viscera. Because a short sternum is
not typical with this condition, we
speculate that it is related to the
early age of his initial surgery and
presumed devascularization of the
sternum. He subsequently underwent
methyl methacrylate chest wall
reconstruction with rectus abdominis
muscle coverage to address the
hypoplastic sternum and complex
chest wall deformity. However, he
returned after a hiatus of several
years with a marked deformity of his
chest wall and general hypoplasia of
the central portion of the ribcage (Fig
1). He had symptomatic dyspnea on
exertion, was unable to participate in
sports, which negatively impacted his
self-esteem, and was self-conscious of
his appearance. Pulmonary function
tests revealed a 50% reduction in
vital capacity and forced expiratory
volume. After extensive discussions
with our pediatric pulmonology
and pediatric surgery colleagues,
we decided to pursue bilateral
distraction osteogenesis of ribs 4–8
when the patient was 17 years old to
increase his overall thoracic volume.
OPERATIVE TECHNIQUE
After the patient was positioned
supine with arms extended, lazy-S
incisions were made bilaterally over
the anterior axillary line. The serratus
anterior was divided in 3 locations to
permit access to the ribs of interest. A
small incision was made at the lower
border of each rib to dissect a small
periosteal pocket, permitting us to
divide the rib while maintaining the
periosteum as a sleeve to promote
osteogenesis. Osteotomies of bilateral
ribs 4–8 were performed by using a
reciprocating saw.
The 10 rib distractors used were
custom manufactured by KLS Martin
(Jacksonville, FL), based on a design
originally used for placement on
metacarpals. They were chosen
over midface distractors because of
their increased rigidity; the custom
manufacturing extended their length
to 3 cm. The distraction device was
placed across the osteotomy gap in
a supraperiosteal position, using 4
screws (2-mm diameter, 11-mm total
length) on each side. The activating
rods were brought out anteriorly
through small separate skin incisions.
All distractors were placed in a
similar fashion with the exception
of the fourth rib on the patient’s
right side. The fourth rib was located
slightly inferior to the third rib and
pectoralis muscle, and consequently
the activating rod would not
reach the skin. An osteotomy was
performed on the right fourth rib but
no distractor was placed, with the
expectation that it would follow the
distraction of the other four ribs on
that side. After excellent fixation of
all devices was obtained, muscle and
soft tissue were closed in a layered
fashion (Fig 2).
After a latency period of 5 days,
distraction began at a frequency
of twice a day, for 1 mm of total
daily lengthening for each of the
9 distractors. The patient was
discharged on postoperative day 9,
and the family continued distraction
at home until the total distraction
distance of 3 cm was achieved. Two
e2
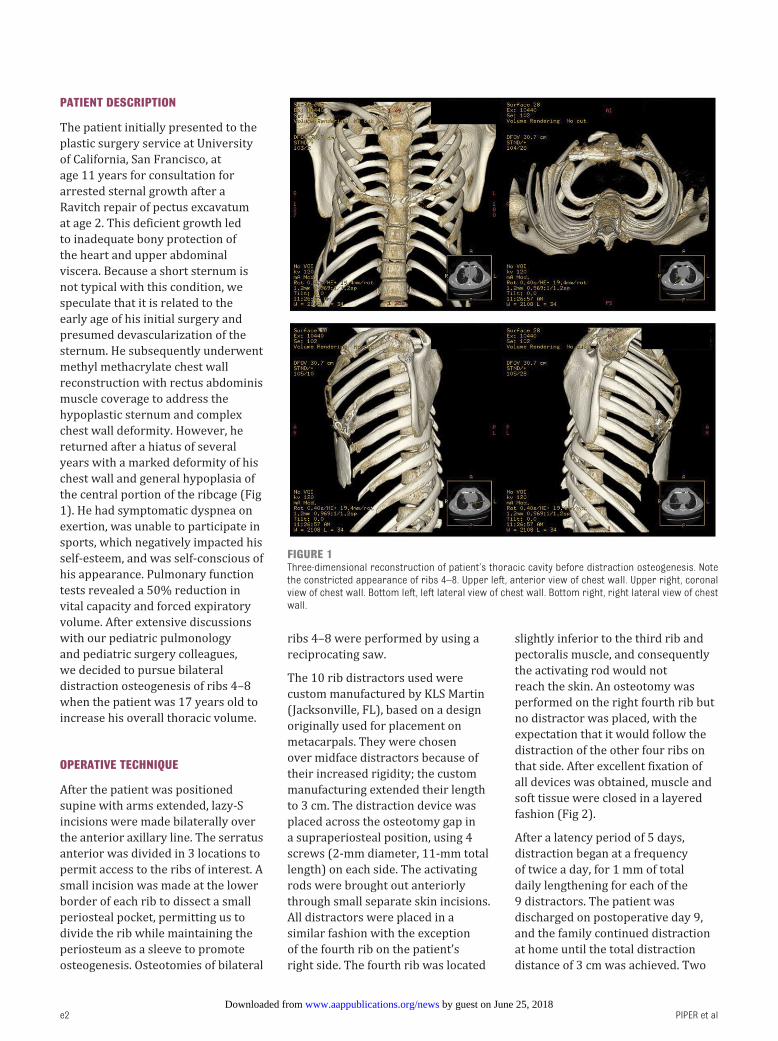
FIGURE 1Three-dimensional reconstruction of patient’s thoracic cavity before distraction osteogenesis. Note the constricted appearance of ribs 4–8. Upper left, anterior view of chest wall. Upper right, coronal view of chest wall. Bottom left, left lateral view of chest wall. Bottom right, right lateral view of chest wall.
by guest on June 25, 2018www.aappublications.org/newsDownloaded from
PEDIATRICS Volume 137 , number 3 , March 2016
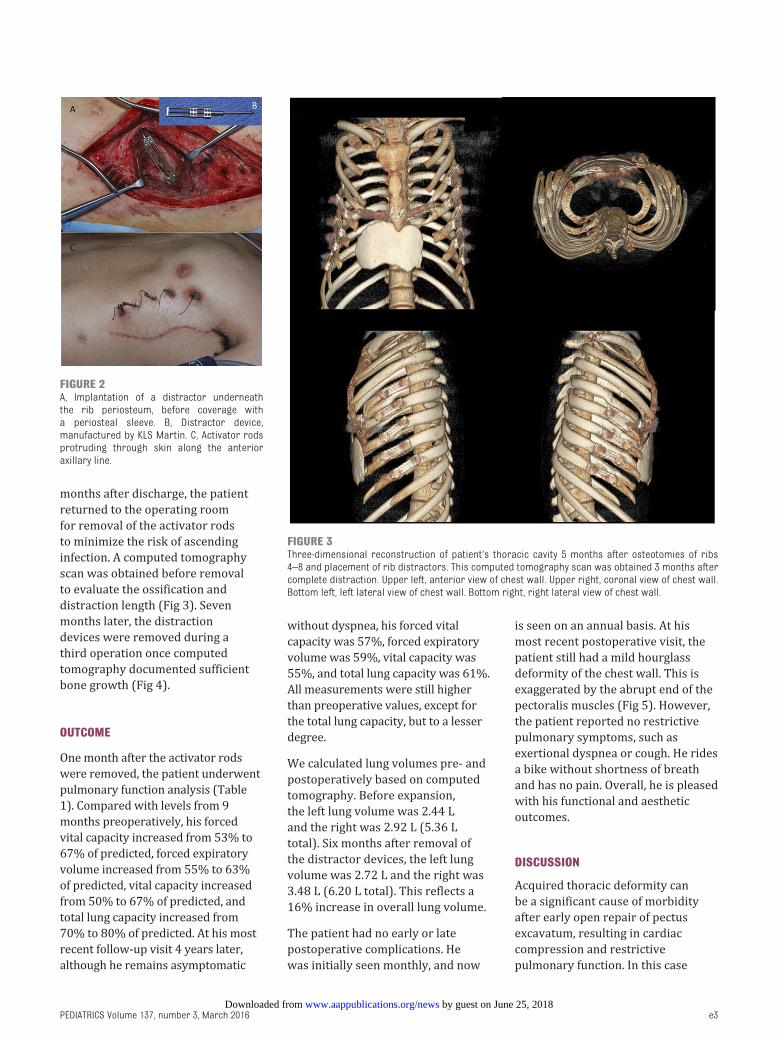
months after discharge, the patient
returned to the operating room
for removal of the activator rods
to minimize the risk of ascending
infection. A computed tomography
scan was obtained before removal
to evaluate the ossification and
distraction length (Fig 3). Seven
months later, the distraction
devices were removed during a
third operation once computed
tomography documented sufficient
bone growth (Fig 4).
OUTCOME
One month after the activator rods
were removed, the patient underwent
pulmonary function analysis (Table
1). Compared with levels from 9
months preoperatively, his forced
vital capacity increased from 53% to
67% of predicted, forced expiratory
volume increased from 55% to 63%
of predicted, vital capacity increased
from 50% to 67% of predicted, and
total lung capacity increased from
70% to 80% of predicted. At his most
recent follow-up visit 4 years later,
although he remains asymptomatic
without dyspnea, his forced vital
capacity was 57%, forced expiratory
volume was 59%, vital capacity was
55%, and total lung capacity was 61%.
All measurements were still higher
than preoperative values, except for
the total lung capacity, but to a lesser
degree.
We calculated lung volumes pre- and
postoperatively based on computed
tomography. Before expansion,
the left lung volume was 2.44 L
and the right was 2.92 L (5.36 L
total). Six months after removal of
the distractor devices, the left lung
volume was 2.72 L and the right was
3.48 L (6.20 L total). This reflects a
16% increase in overall lung volume.
The patient had no early or late
postoperative complications. He
was initially seen monthly, and now
is seen on an annual basis. At his
most recent postoperative visit, the
patient still had a mild hourglass
deformity of the chest wall. This is
exaggerated by the abrupt end of the
pectoralis muscles (Fig 5). However,
the patient reported no restrictive
pulmonary symptoms, such as
exertional dyspnea or cough. He rides
a bike without shortness of breath
and has no pain. Overall, he is pleased
with his functional and aesthetic
outcomes.
DISCUSSION
Acquired thoracic deformity can
be a significant cause of morbidity
after early open repair of pectus
excavatum, resulting in cardiac
compression and restrictive
pulmonary function. In this case
e3
FIGURE 2A, Implantation of a distractor underneath the rib periosteum, before coverage with a periosteal sleeve. B, Distractor device, manufactured by KLS Martin. C, Activator rods protruding through skin along the anterior axillary line.
FIGURE 3Three-dimensional reconstruction of patient’s thoracic cavity 5 months after osteotomies of ribs 4–8 and placement of rib distractors. This computed tomography scan was obtained 3 months after complete distraction. Upper left, anterior view of chest wall. Upper right, coronal view of chest wall. Bottom left, left lateral view of chest wall. Bottom right, right lateral view of chest wall.
by guest on June 25, 2018www.aappublications.org/newsDownloaded from
PIPER et al
report, we present a novel method
for managing this complication using
distraction osteogenesis, a technique
often used in craniomaxillofacial and
orthopedic surgery. The particularly
challenging aspect of this case was to
attempt distraction with the constant
respiratory movement of the ribs.
The distractors proved capable of
maintaining fixation under these
conditions and allowing for new bone
formation. The success of distraction
osteogenesis in restructuring the
thoracic cavity acts as a proof of
principle that this technique may be
used in a broader scope to treat other
acquired and congenital thoracic
conditions.
However, as with all surgical
procedures, this procedure has
drawbacks. First, it requires 3
separate surgeries: distractor
placement, activator rod removal,
and distractor removal. This means
3 episodes of general anesthesia,
potential hospitalizations, and
periods of postoperative recovery.
Second, this technique is painful
during the distraction process, as
well as after the 3 surgeries. Third,
the distractor devices are expensive,
∼$5000 per piece, although we did
receive a bulk discount. Finally,
there is bilateral scarring, which
may be unsightly. However, the
alternative surgical options also have
drawbacks. Sternal split with rib
graft placement improves pulmonary
function, but leaves the intrathoracic
organs vulnerable to injury and does
not adequately address cosmetic
concerns.13 A vertical expandable
prosthetic titanium rib requires a
large incision, has minimal benefit in
children older than 8 years, and can
cause significant tension on the soft
tissues, leading to erosion.7 Risks of
anterior chest wall reconstruction
with release and elevation of
the sternum include supporting
retrosternal bar migration, migration
and exposure of the rib grafts and
sternal wires, and difficulty in
e4
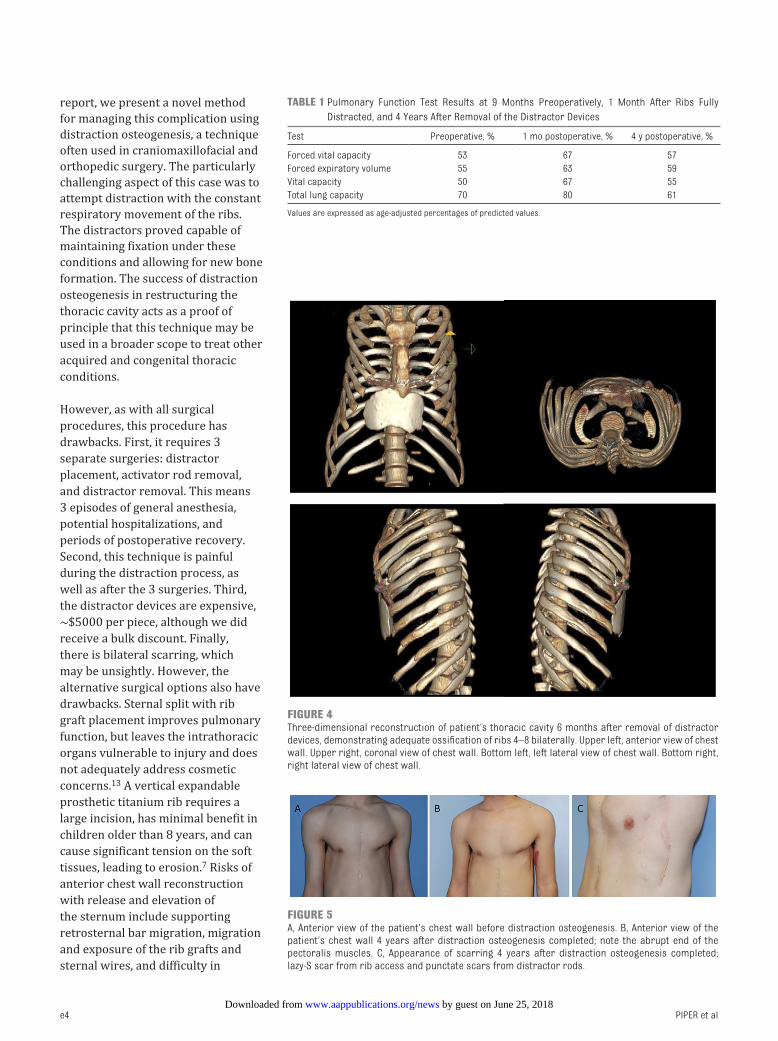
FIGURE 4Three-dimensional reconstruction of patient’s thoracic cavity 6 months after removal of distractor devices, demonstrating adequate ossifi cation of ribs 4–8 bilaterally. Upper left, anterior view of chest wall. Upper right, coronal view of chest wall. Bottom left, left lateral view of chest wall. Bottom right, right lateral view of chest wall.
TABLE 1 Pulmonary Function Test Results at 9 Months Preoperatively, 1 Month After Ribs Fully
Distracted, and 4 Years After Removal of the Distractor Devices
Test Preoperative, % 1 mo postoperative, % 4 y postoperative, %
Forced vital capacity 53 67 57
Forced expiratory volume 55 63 59
Vital capacity 50 67 55
Total lung capacity 70 80 61
Values are expressed as age-adjusted percentages of predicted values.
FIGURE 5A, Anterior view of the patient’s chest wall before distraction osteogenesis. B, Anterior view of the patient’s chest wall 4 years after distraction osteogenesis completed; note the abrupt end of the pectoralis muscles. C, Appearance of scarring 4 years after distraction osteogenesis completed; lazy-S scar from rib access and punctate scars from distractor rods.
by guest on June 25, 2018www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 3 , March 2016
controlling hemorrhage as the sternum
is separated from scar tissue.17
Despite the drawbacks, our
patient had substantial functional
and aesthetic improvement, as
evidenced by higher levels in his
pulmonary function tests, increased
lung volumes, and greater self-
esteem. His pulmonary function
never normalized, however, and
in fact declined over time after
initial postoperative improvement.
Although this was suboptimal, he
remains asymptomatic. The decline
may indicate additional growth of
the patient without commensurate
growth of the chest wall. Therefore,
there may be a theoretical benefit
to performing this operation when
the patient is younger, so that the
ribs and lungs may continue to grow
together. We believe this outcome
could also be improved by increasing
the length of distraction, and propose
to do this in future cases or even to
perform distraction at 2 points in
the rib (for example, anterior and
posterior axillary lines). In addition,
a device that follows the curvature
of the ribs could improve both the
aesthetic, as well as the functional,
outcome. Overall, the symmetry of
this patient’s chest wall has remained
stable over 4 years despite continued
growth and skeletal maturity.
Distraction osteogenesis may provide
a safe and effective alternative for
surgical management of acquired
thoracic dystrophy.
ACKNOWLEDGMENTS
Thank you to Pamela Derish for her
review of the manuscript. Thank you
also to Dr. Brian Haas for his assistance
with calculating lung volumes.
REFERENCES
1. Kelly RE Jr, Cash TF, Shamberger RC, et
al. Surgical repair of pectus excavatum
markedly improves body image
and perceived ability for physical
activity: multicenter study. Pediatrics.
2008;122(6). Available at: www.
pediatrics. org/ cgi/ content/ full/ 122/ 6/
e1218
2. Davis JT, Weinstein S. Repair of the
pectus deformity: results of the Ravitch
approach in the current era. Ann
Thorac Surg. 2004;78(2):421–426
3. Haller JA Jr, Shermeta DW, Tepas JJ,
Bittner HR, Golladay ES. Correction of
pectus excavatum without prostheses
or splints: objective measurement
of severity and management of
asymmetrical deformities. Ann Thorac
Surg. 1978;26(1):73–79
4. Actis Dato GM, Cavaglià M, Actis Dato
A, Centofanti P, di Summa M. Too large
resection of pectus excavatum in
young patients: a reason to worry?
Ann Thorac Surg. 1996;62(4):
1242–1243
5. Robicsek F, Fokin AA. How not to do
it: restrictive thoracic dystrophy
after pectus excavatum repair.
Interact Cardiovasc Thorac Surg.
2004;3(4):566–568
6. Chen CH, Liu HC, Hung TT, Chen CH.
Restrictive chest wall deformity as
a complication of surgical repair for
pectus excavatum. Ann Thorac Surg.
2010;89(2):599–601
7. Waldhausen JH, Redding GJ, Song
KM. Vertical expandable prosthetic
titanium rib for thoracic insuffi ciency
syndrome: a new method to treat
an old problem. J Pediatr Surg.
2007;42(1):76–80
8. Weber TR, Kurkchubasche AG.
Operative management of asphyxiating
thoracic dystrophy after pectus repair.
J Pediatr Surg. 1998;33(2):262–265
9. Aronson DC, Van Nierop JC, Taminiau
A, Vos A. Homologous bone graft for
expansion thoracoplasty in Jeune’s
asphyxiating thoracic dystrophy. J
Pediatr Surg. 1999;34(3):500–503
10. Davis JT, Long FR, Adler BH, Castile RG,
Weinstein S. Lateral thoracic expansion
for Jeune syndrome: evidence of rib
healing and new bone formation. Ann
Thorac Surg. 2004;77(2):445–448
11. Kaddoura IL, Obeid MY, Mroueh SM,
Nasser AA. Dynamic thoracoplasty for
asphyxiating thoracic dystrophy. Ann
Thorac Surg. 2001;72(5):1755–1758
12. Robicsek F. Innovative single-stage
repair of severe asymmetric pectus
excavatum defects. Ann Thorac Surg.
2005;80(6):2419
13. Weber TR. Further experience with the
operative management of asphyxiating
thoracic dystrophy after pectus repair.
J Pediatr Surg. 2005;40(1):170–173
14. Ilizarov GA. The Transosseous
Osteosynthesis: Theoretical and
Clinical Aspects of the Regenerations
and Growth of Tissue. New York:
Springer-Verlag; 1992
15. Ilizarov GA. The tension-stress effect
on the genesis and growth of tissues:
Part II. the infl uence of the rate and
frequency of distraction. Clin Orthop
Relat Res. 1989;(239):263–285
16. Ilizarov GA. The tension-stress effect on
the genesis and growth of tissues. part
I. the infl uence of stability of fi xation
and soft-tissue preservation. Clin
Orthop Relat Res. 1989;(238):249–281
17. Sacco Casamassima MG, Goldstein
SD, Salazar JH, et al. Operative
management of acquired Jeune’s
syndrome. J Pediatr Surg.
2014;49(1):55–60, discussion 60
e5 by guest on June 25, 2018www.aappublications.org/newsDownloaded from

originally published online February 11, 2016; Pediatrics Merisa L. Piper, Lawrence Delrosario and William Y. Hoffman
Thoracic DystrophyDistraction Osteogenesis of Multiple Ribs for the Treatment of Acquired
ServicesUpdated Information &
015-2053http://pediatrics.aappublications.org/content/early/2016/02/09/peds.2including high resolution figures, can be found at:
References
015-2053#BIBLhttp://pediatrics.aappublications.org/content/early/2016/02/09/peds.2This article cites 14 articles, 1 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/plastic_surgery_subPlastic Surgeryhttp://www.aappublications.org/cgi/collection/surgery_subSurgeryfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 25, 2018www.aappublications.org/newsDownloaded from
originally published online February 11, 2016; Pediatrics Merisa L. Piper, Lawrence Delrosario and William Y. Hoffman
Thoracic DystrophyDistraction Osteogenesis of Multiple Ribs for the Treatment of Acquired
http://pediatrics.aappublications.org/content/early/2016/02/09/peds.2015-2053located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 25, 2018www.aappublications.org/newsDownloaded from