Embed Size (px)
Citation preview

DIS
SE
RT
AT
ION
S | T
IINA
IKÄ
VA
LK
O | P
ED
IAT
RIC
SL
EE
P D
ISO
RD
ER
ED
BR
EA
TH
ING
– CA
US
ES
AN
D... | N
o 373
uef.fi
PUBLICATIONS OF THE UNIVERSITY OF EASTERN FINLAND
Dissertations in Health Sciences
ISBN 978-952-61-2247-2ISSN 1798-5706
Dissertations in Health Sciences
PUBLICATIONS OF THE UNIVERSITY OF EASTERN FINLAND
TIINA IKÄVALKO
PEDIATRIC SLEEP DISORDERED BREATHING – CAUSES AND CONSEQUENCES
The aim of this doctoral thesis was to investigate the risk factors, diagnostic
method and consequences of pediatric sleep disordered breathing (SDB) in a population
sample of children from the Physical Activity and Nutrition in Children (PANIC) Study. The results showed that dentofacial and
pharyngeal morphology but not excess body fat raises the risk for SDB among 7-year-olds. Certain morphological and functional features at the age of 7 years may predict
developing SDB at the age of 10 years. SDB associates with low psychological well-being
in boys aged 7-year.
TIINA IKÄVALKO


Pediatric Sleep Disordered Breathing
– Causes and Consequences


TIINA IKÄVALKO
Pediatric Sleep Disordered Breathing
– Causes and Consequences
To be presented by permission of the Faculty of Health Sciences, University of Eastern Finland forpublic examination in Canthia Auditorium CA102, Kuopio, on Friday, October 14th 2016, at 12 noon
Publications of the University of Eastern Finland Dissertations in Health Sciences
Number 373
Department of Dentistry, Institute of Clinical Medicine, School of Medicine,Faculty of Health Sciences, University of Eastern Finland
Kuopio2016

Grano OyKuopio, 2016
Series Editors:Professor Tomi Laitinen, M.D., Ph.D.
Institute of Clinical Medicine, Clinical Physiology and Nuclear MedicineFaculty of Health Sciences
Professor Hannele Turunen, Ph.D.Department of Nursing Science
Faculty of Health Sciences
Professor Kai Kaarniranta, M.D., Ph.D.Institute of Clinical Medicine, Ophthalmology
Faculty of Health Sciences
Associate Professor (Tenure Track) Tarja Malm, Ph.D.A.I. Virtanen Institute for Molecular Sciences
Faculty of Health Sciences
Lecturer Veli-Pekka Ranta, Ph.D. (pharmacy)School of Pharmacy
Faculty of Health Sciences
Distributor:University of Eastern Finland
Kuopio Campus LibraryP.O.Box 1627
FI-70211 Kuopio, Finlandhttp://www.uef.fi/kirjasto
ISBN (print): 978-952-61-2247-2ISBN (pdf): 978-952-61-2248-9
ISSN (print): 1798-5706ISSN (pdf): 1798-5714
ISSN-L: 1798-5706

III
Author’s address: Institute of Dentistry/School of MedicineUniversity of Eastern FinlandKUOPIOFINLAND
Supervisors: Professor Riitta Pahkala, DDS, Ph.D. Institute of Dentistry/School of Medicine University of Eastern Finland KUOPIO FINLAND
Professor Timo Lakka, M.D., Ph.D.Physiology/Institute of BiomedicineUniversity of Eastern FinlandKUOPIOFINLAND
Docent Henri Tuomilehto, M.D., Ph.D.Oivauni Sleep ClinicInstitute of Public Health and Clinical NutritionUniversity of Eastern FinlandKUOPIO
FINLANDProfessor Matti Närhi, DDS, Ph.D.Institute of Dentistry/School of MedicineUniversity of Eastern FinlandKUOPIOFINLAND
Reviewers: Professor Pertti Pirttiniemi, DDS, Ph.D.Department of Oral Development and Orthodontics/Institute of DentistryUniversity of OuluOULUFINLANDOuti Saarenpää-Heikkilä, M.D., Ph.D.Unit of Child Neurology/Department of PediatricsTampere University HospitalTAMPERE
FINLAND
Opponent: Professor Timo Peltomäki, DDS, Ph.D.School of MedicineUniversity of TampereOral and Maxillofacial UnitTampere University HospitalTAMPEREFINLAND

IV

V
Ikävalko, TiinaPediatric Sleep Disordered Breathing – Causes and ConsequencesUniversity of Eastern Finland, Faculty of Health SciencesPublications of the University of Eastern Finland. Dissertations in Health Sciences 373. 2016. 83 p.
ISBN (print): 978-952-61-2247-2ISBN (pdf): 978-952-61-2248-9ISSN (print): 1798-5706ISSN (pdf): 1798-5714ISSN-L: 1798-5706
ABSTRACT
Sleep disordered breathing (SDB) is one of the most common sleep disturbances among children; itrepresents a continuum of symptoms from habitual snoring (HS) to obstructive sleep apnea (OSA).The prevalence of OSA among children and adolescents has been reported to range between 0.1 and13% and that of snoring between 2 and 34%. Children with SDB can suffer from diverse symptoms,such as hyperactivity, sometimes excess daytime sleepiness, restless sleep, nightmares, nocturnalenuresis and bruxism. Deviant craniofacial morphology and high body adiposity are known risks forchildhood SDB and treatment modalities aim to influence these factors. When left untreated, SDB canreduce psychological well-being and quality of life, cause impairment in growth and cognition andboth metabolic and cardiorespiratory morbidity. The present study is based on the data of the Physical Activity and Nutrition in Children (PANIC)Study, which is an ongoing physical activity and dietary intervention study in a population sampleof children from the city of Kuopio, Finland. The study population was 512 at the baseline when thechildren were 6–8 years of age, and 440 after 2.2-years´ follow-up when they were 9-11 years. The aimof the study was to investigate the risk factors for pediatric SDB, to evaluate the feasibility of thelateral view photograph of the face for recognizing the facial convexity in order to diagnose thecondition, to assess the role of the SDB for psychological well-being of the children, and to estimatethe possible predictors for developing SDB during follow-up. The results showed that abnormal dentofacial and pharyngeal morphology, but not excess body fat,was associated with SDB in children 6-8 years of age. Children with tonsillar hypertrophy, cross biteand convex facial profile should always be examined as regards their sleeping habits, snoring andpauses in breathing during sleep. Facial convexity is typically determined by the orthodontist but itseemed to be difficult for other health care professionals. SDB was more prevalent in boys with lowpsychological well-being than in boys with normal psychological well-being. The association did notexist in girls. Furthermore, deviant dentofacial morphology, mouth breathing, body adiposity andmale gender seemed to predict SDB in childhood. Orthodontic treatment also seemed to associatewith SDB. In conclusion, the study showed that the causes and consequences of pediatric SDB manifestthemselves with the whole entity of SDB, including the milder forms of the condition. The findingsof the study are useful in identifying children at increased risk for developing SDB. Children withthese features could be candidates for early intervention to prevent the progression of SDB later inlife. This can only happen via better understanding and earlier recognition of the underlyingmechanisms for developing SDB and an intensive collaboration between different medicalspecialities.
National Library of Medicine Classification: WE 705, WF 143, WM 188, WU 140.5Medical Subject Headings: Adipose Tissue; Bruxism; Child; Craniofacial Abnormalities; Early MedicalIntervention; Finland; Mouth Breathing; Quality of Life; Risk Factors; Sleep; Sleep Apnea Syndromes; SleepApnea, Obstructive; Snoring

VI

VII
Ikävalko, TiinaLasten unenaikaiset hengityshäiriöt – syyt ja seurauksetItä-Suomen yliopisto, terveystieteiden tiedekuntaPublications of the University of Eastern Finland. Dissertations in Health Sciences 373. 2016. 83 s.
ISBN (nid): 978-952-61-2247-2ISBN (pdf): 978-952-61-2248-9ISSN (nid): 1798-5706ISSN (pdf): 1798-5714ISSN-L: 1798-5706
TIIVISTELMÄ
Unenaikaiset hengityshäiriöt (sleep disordered breathing, SDB) ovat yksi yleisimmistä lastenunihäiriöistä. Käsitteellä tarkoitetaan oireiden kirjoa lievimmästä oireesta eli kuorsauksestavaikeimpaan oireeseen eli obstruktiiviseen uniapneaan. Lapsilla ja nuorilla uniapnean esiintyvyysvaihtelee 0.1-13 %:n välillä ja kuorsauksen vastaavasti 2-34 %:n välillä. Unenaikaisistahengityshäiriöistä kärsivillä lapsilla on moninaisia oireita, esimerkiksi yliaktiivisuutta, joskuspäiväaikaista väsymystä, levotonta unta, painajaisia, yökastelua ja bruksismia. Tyypillisiäunenaikaisten hengityshäiriöiden riskitekijöitä ovat poikkeamat hampaiston, kasvojen ja nielunalueen morfologiassa sekä kehon kohonnut rasvapitoisuus. Unenaikaisten hengityshäiriöiden hoitopyrkii vaikuttamaan edellä mainittuihin tekijöihin. Hoitamattomana tila voi heikentää lapsenpsyykkistä hyvinvointia ja elämänlaatua, aiheuttaa oppimisvaikeuksia ja metabolista ja sydän- javerisuonielimistön sairastuvuutta sekä hidastaa kasvua. Tutkimus perustuu Lasten liikunta- ja ravitsemustutkimuksen (Physical Activity and Nutrition inChildren (PANIC) Study) aineistoon. Kyseessä on interventiotutkimus, jossa oli lähtötilanteessatutkittavana 512 6-8-vuotiasta lasta ja 2.2 vuoden seurannan jälkeen 440 9-11-vuotiasta lasta.Tutkimuksen tarkoitus oli tutkia lapsuuden unenaikaisten hengityshäiriöiden riskitekijöitä, arvioidaeri ammattiryhmien kykyä tunnistaa yhtä riskitekijää eli kuperaa kasvoprofiilia, tutkia unenaikaistenhengityshäiriöiden vaikutusta lapsen psykologiseen hyvinvointiin sekä arvioida unenaikaistenhengityshäiriöiden mahdollisia ennusmerkkejä. Tutkimustulokset osoittivat, että poikkeava kasvojen ja pään sekä nielun alueen morfologia oliyhteydessä unenaikaisiin hengityshäiriöihin 6-8-vuotiaiden lasten ikäryhmässä. Jos lapsella onsuurentuneet tonsillat, ristipurenta ja kupera kasvoprofiili, tulisi selvittää myös nukkumistavat sekämahdolliset kuorsaus ja hengityskatkokset. Kehon rasvapitoisuudella ei ollut vaikutusta riskiin.Oikomishoidon erikoishammaslääkäri pystyi tunnistamaan kuperan kasvoprofiilin melkoluotettavasti, mutta muille lasten kanssa työskenteleville terveydenhuollon ammattilaisille se olivaikeaa. Unenaikaiset hengityshäiriöt olivat yleisempiä psyykkisesti huonommin voivilla pojilla.Tytöillä tätä yhteyttä ei havaittu. Unenaikaisten hengityshäiriöiden esiintymistä ja ilmaantumistaseuranta-aikana ennusti poikkeava hampaiston ja kasvojen alueen morfologia, suuhengitys, kehonrasvapitoisuus ja miessukupuoli. Myös oikomishoidolla näytti olevan yhteyttä unenaikaisiinhengityshäiriöihin. Merkittävä johtopäätös oli, että lapsilla unenaikaisten hengityshäiriöiden riskit ja seurauksetilmenevät väestötasolla silloinkin, kun mukana ovat sairauden lievimmät muodot. Tutkimustuloksetovat hyödyllisiä, kun halutaan jo nuorella iällä tunnistaa ne lapset, joilla on riski unenaikaisiinhengityshäiriöihin ja joita kannattaa jo aikaisessa vaiheessa ryhtyä hoitamaan moniammatillisesti.Näin voidaan mahdollisesti estää tilan paheneminen myöhemmällä iällä.
Luokitus: WE 705, WF 143, WM 188, WU 140.5Yleinen Suomalainen asiasanasto: ehkäisevä hammaslääketiede; hengitys; häiriöt; lapset; moniammatillisuus;morfologia; riskitekijät; uni; uniapnea-oireyhtymä; unihäiriöt

VIII

IX
Acknowledgements
This study was carried out at the Institutes of Biomedicine and Dentistry, University ofEastern Finland, Kuopio, during the years 2008–2016.I wish to express my deepest gratitude to my principle supervisor, Professor Riitta Pahkala.I sincerely admire your enthusiasm, vigor and efficiency in doing anything, and especiallyscientific work. Things are certainly not left around waiting on your table. The journey fromthe phone call I received from you in the blueberry forest to this day has been a long one, butyour endless eagerness and warm encouragement have kept me going.I owe my deep gratitude to the principal investigator of the PANIC study, Professor TimoLakka. Your expertise and virtuosity in the academic world have in many ways increasedmy understanding of the area of research. I warmly thank Professor Matti Närhi for all thehelp and constructive comments during these years. Your long knowledge in research hasbeen an important part of my work. I also owe my warmest thanks to docent HenriTuomilehto. Despite your busy schedule and work world-wide, you have supported me andtaught me much about clinical sleep medicine.Likewise, I express my warm gratitude to the official reviewers of my thesis, Professor PerttiPirttiniemi and Outi Saarenpää-Heikkilä, MD, PhD, for their constructive comments andvaluable suggestions to improve the quality of my thesis. I also warmly thank AnnaVuolteenaho, MA, for her skillful revision of the language of my thesis.I warmly and sincerely thank Riitta Myllykangas for all the possible and impossible help youhave given me during these years. Not only your expertise in statistics but also your practicalinsight have been a sine qua non for my work. You have always had the time to listen andunderstand – regarding all areas of life, and I have really enjoyed working with you.The unique PANIC group deserves my special thanks. The Medistudia nerve center has beena place where I have always felt welcome – if I needed any help or advice I got it from you.The researcher group works hard for the best interests of children and I am proud to be apart of it.I am grateful to all my co-authors for their contribution to this work. Especially the co-operation with Professor Soili Lehto has been extremely rewarding.The whole staff of the Institute of Dentistry, University of Eastern Finland, and Oral andMaxillofacial Department, Kuopio University Hospital, is warmly acknowledged for theirhelp, support and kind understanding. During the hectic years while building new dentaleducation in Kuopio the atmosphere has always been one of empathy and open forconstructive discussion, for which I am grateful.I thank all the children and families participating the PANIC study for their time and patienceand I hope the co-operation will continue in the coming years. Furthermore, I thank KuopioSocial and Health Center for providing the facilities and skillful, friendly assistants duringthe examinations.I warmly thank my dear friends and their families for the support and presence they havegiven me during all these years. Despite long silent times I have known in my heart that youare there. I owe you my thanks and love for keeping me in touch with life.I owe my deep thanks to my beloved parents who have supported me in all the stages of mylife, unconditionally and lovingly. Likewise, I owe my warm gratitude to my dear parents-in-law. Especially the times spent in your paradise, the cottage at Konnevesi, have constantly

X
given me rest and strength to keep going. I also give my sincere thanks to my relatives forall the joyful moments I have spent with you.I owe my special loving thanks to my dear children. Vertti, my beloved firstborn, you havechallenged me with your intellect and given me inspiration and new fresh views of life.Miina, the middle one, your empathy and sensitive presence warm my heart, not to mentionyour delicious sweet creations that gave me pleasure and (sometimes even too much) energyduring hard times. Kerttu, my dear youngest one, your bounce and rationality is somethingI can only admire – you are a woman who stands on her own two feet. I am proud andprivileged to be the mom of each of you and give my endless love to you.Finally, I cannot express enough gratitude to my dear husband, Harri. The journey of myresearch has been long, but it is nothing compared to our journey of almost 32 years ofmarriage. These years have been filled with work and rest, ordinariness and celebration,going and staying. Altogether, our journey has been filled with love. Thank you for yourendless support and belief in me – not to mention practical love in terms of delicious suppersin late evenings when I came home from work hungry and tired. During all our yearstogether – you have made my day!In appreciation of their financial support for this work, I thank the Institute of Biomedicine,University of Eastern Finland, the Finnish Dental Society Apollonia, the Northern SavoDental Society and the Research Foundation of Respiratory Diseases.
Kuopio, October 2016
Tiina Ikävalko

XI
List of the original publications
This dissertation is based on the following original publications:
I Ikävalko T, Tuomilehto H, Pahkala R, Tompuri T, Laitinen T, Myllykangas R,Vierola A, Lindi V, Närhi M, Lakka TA. Craniofacial morphology but not excessbody fat is associated with risk of having sleep-disordered breathing –the PANIC study (a questionnaire-based inquiry in 6-8-year-olds). EuropeanJournal of Pediatrics 171: 1747-1752, 2012.
II Ikävalko T, Närhi M, Lakka T, Myllykangas R, Tuomilehto H, Vierola A, PahkalaR. Lateral facial profile may reveal the risk for sleep disordered breathing inchildren - the PANIC-study. Acta Odontologica Scandinavica 73: 550-555, 2015.
III Ikävalko T, Lehto S, Lintu N, Väistö J, Eloranta A-M, Haapala EA, Vierola A,Myllykangas R, Tuomilehto H, Brage S, Pahkala R, Närhi M, Lakka TA. Health-related correlates of psychological well-being among girls and boys 6-8 years ofage - the PANIC study. Submitted.
IV Ikävalko T, Närhi M, Eloranta A-M, Lintu N, Myllykangas R, Vierola A,Tuomilehto H, Lakka T, Pahkala R. Predictors of sleep disordered breathing inchildren – the PANIC study. Submitted.
The publications were adapted with the permission of the copyright owners.

XII

XIII
Contents
1 INTRODUCTION .................................................................................................................. 1
2 REVIEW OF THE LITERATURE ......................................................................................... 32.1 Normal sleep of the children ................................................................................ 3
2.1.1 The functions of sleeping .............................................................................. 32.1.2 Quantity of sleep ............................................................................................ 32.1.3 Cycles of sleep ................................................................................................ 42.1.4 Respiratory patterns of sleep ........................................................................ 5
2.2 Sleep disordered breathing (SDB) – general aspects .......................................... 62.2.1 Historical aspects ........................................................................................... 62.2.2 Definition and classification .......................................................................... 62.2.3 Epidemiology – prevalence of OSA in adults .............................................. 7
2.3 SDB in children ...................................................................................................... 82.3.1 Prevalence ....................................................................................................... 82.3.2 Symptoms ..................................................................................................... 122.3.3 Risk factors ................................................................................................... 122.3.4 Pathophysiology .......................................................................................... 152.3.5 Consequences ............................................................................................... 162.3.6 Diagnostics ................................................................................................... 182.3.7 Treatment of pediatric SDB ......................................................................... 192.3.8 Other orthodontic aspects ........................................................................... 202.3.9 Childhood SDB associations to adult SDB ................................................. 20
3 AIMS OF THE STUDY ........................................................................................................ 23
4 STUDY DESIGN AND STUDY POPULATION ............................................................. 254.1 Ethical considerations ......................................................................................... 254.2 Design of the physical activity and nutrition in children (PANIC) study ..... 254.3 Participants .......................................................................................................... 27
5 METHODS ............................................................................................................................ 295.1 Assessments ......................................................................................................... 29
5.1.1 Dentofacial and pharyngeal morphology .................................................. 295.1.2 Sleep .............................................................................................................. 295.1.3 Body composition and fitness ..................................................................... 305.1.4 Photograph ................................................................................................... 305.1.5 Well-being measurements ........................................................................... 325.1.6 Physical activity and inactivity ................................................................... 325.1.7 Dietary assessments ..................................................................................... 325.1.8 Socioeconomic background and characteristics of the parents ................ 33
5.2 Reliability of the measures ................................................................................. 335.3 Statistical methods .............................................................................................. 33
6 RESULTS ............................................................................................................................... 356.1 Basic characteristics ............................................................................................. 35

XIV
6.2 Risk factors for sleep disordered breathing among children aged 6-8and 9-11- years (Study I, IV) .............................................................................. 39
6.3 Predictors of sleep disordered breathing in children (Study IV) .................... 416.4 Recognizing convexity and vertical proportions of the lateral facial
profile (Study II).................................................................................................. 436.5 Correlates of psychological well-being among girls and boys 6-8 years
of age – the role of sleep disordered breathing (Study III) .............................. 44
7 DISCUSSION ....................................................................................................................... 517.1 Dentofacial and pharyngeal morphology with and risk for sleep
disordered breathing .......................................................................................... 517.2 Prediction of SDB ................................................................................................ 527.3 The psychological consequences of SDB ........................................................... 547.4 Strengths and limitations.................................................................................... 55
8 CONCLUSIONS AND FUTURE PERSPECTIVE ............................................................ 59
REFERENCES .............................................................................................................................. 61
APPENDIX
ORIGINAL PUBLICATIONS I–IV

XV
Abbreviations
ADHD Attention-deficit/hyperactivity disorder
AHI Apnea/hypopnea index
ATE Adenotonsillectomy
ATH Adenotonsillar hypertrophy
BMI Body mass index
BMI-SDS Body mass index standard deviation score
CI Confidence interval
CP Cerebral palsy
CRP C - reactive protein
DASH Dietary Approach to Stop Hypertension
DXA Dual-energy x-ray absorptiometry
EEG Electro-encephalography
EMG Electro-myography
EOG Electro-oculography
G´ Soft tissue Glabella
h/day Hours/day
HILMO Care register for health care (hoitoilmoitusjärjestelmä)
HS Habitual snoring
ICC Intra-class correlation coefficient
IgA, G, M Immunoglobulin A, G, M
IOTF International Obesity Task Force
kg Kilogram
m Meter
Me` Soft tissue Menton
MetS Metabolic syndrome
min/day Minutes/day
mmHg Mercury millimeter

XVI
n Number of participants
N Non-REM sleep
Na` Soft tissue Nasion
NHP Natural head position
OR Odds ratio
OSA Obstructive sleep apnea
p Probability of rejecting the null hypothesis
PANIC Physical Activity and Nutrition in Children
PCO2 Carbon dioxide pressure
Pg` Soft tissue Pogonion
PS Primary snoring
PSG Polysomnography
PSWB Psychological well-being
R, REM Rapid eye movement
RDI Respiration disturbance index
S Stage
SD Standard deviation
SDB Sleep disordered breathing
Sn Subnasale
SPSS Statistical Package for Social Sciences
UARS Upper airway resistance syndrome
w/kg Watt/kilogram

1 Introduction
Sleep disordered breathing (SDB) is one of the most common sleep disturbances amongchildren; it represents a spectrum of symptoms from simple habitual snoring (HS) toobstructive sleep apnea (OSA). The prevalence of OSA among pediatric population has beenreported to range between 0.1 and 13% and that of snoring between 2 and 34%. The mostcommon risk factor for pediatric SDB is adenotonsillar hypertrophy (ATH) (Arens et al. 2003,Dayyat et al. 2007). Excess body adiposity is a well-recognized risk factor for SDB in adults(Leinum et al. 2009), but it has also been suggested to be a significant risk factor for pediatricSDB (Marcus et al. 1996, Ng et al. 2004, Verhulst et al. 2008). Further, children with deviantcraniofacial morphology, such as a retrusive and vertically growing mandible, narrowmaxilla, distal molar occlusion and lateral cross bite are at risk for developing SDB(Löfstrand-Tideström et al. 1999, Flores-Mir et al. 2013). The early detection of SDB in children must be highlighted, because there is a growing bodyof evidence which associates the disadvantageous health consequences of SDB with otherhealth problems, such as day-time hyperactivity, attention-deficit/hyperactivity disorder(ADHD) type manifestations and other behavioural and cognitional difficulties, night-timeenuresis, systemic low-grade inflammation, metabolic disturbances and altered somaticgrowth and development (Gozal 2001, Marcus et al. 2012). It would be beneficial if children with SDB – the whole spectrum of it – could be recognizedearly in childhood so that they could be candidates for early intervention and treatment toprevent the progression of SDB later on. The objective of this doctoral thesis was toinvestigate the risk factors and consequences of pediatric SDB in a population sample ofFinnish children.

2

3
2 Review of the literature
2.1 NORMAL SLEEP OF THE CHILDREN
2.1.1 The functions of sleepingSleep is defined as a physiological and behavioral state characterized by partial isolation fromthe environment. It is a period of reduced activity and associated with a typical posture, suchas lying down with eyes closed in humans. Sleep results in a decreased responsiveness toexternal stimuli and is a state that is relatively easy to reverse, which distinguishes sleep fromother states of reduced consciousness, such as hibernation and coma (Siegel 2011). Today itis generally accepted that sleep associates with mental and physical health issues – in bothadults and children. The functions of sleeping are multifold: fatigue reversal, biochemicalrefreshment, immune function, memory improvement and psychological well-being(Lavigne et al. 2009). Altogether, sleep is an essential part of our lives and a criticaldeterminant of health. For children, maturational changes contribute to the unique featuresof childhood sleep.
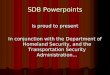
2.1.2 Quantity of sleepA caregiver´s 24-hour cycle concerning the sleep-wake system is a target for newbornchildren. They consolidate their sleep/wake patterns during the first months of life, at thesame time learning to sleep through the night. A study of Henderson shows, that at the ageof 5 months more than half of infants are sleeping simultaneously with their parents(Henderson et al. 2010). The period of sleep children need daily decreases by age – 12–16hours when they are four to twelve months old, 11–14 hours when they are one to two yearsold, 10–13 hours when they are three to five years old, and 9–12 hours at the age of 6-12 years.Compared with adults, teenagers still require more sleep – approximately 8–10 hours(Paruthi et al. 2016). Elderly people tend to go to sleep earlier and wake up earlier, and theirsleep is often light and fragmented (Floyd et al. 2000). Their night time sleep is usuallyshorter, and they usually need to take naps in the daytime (Foley et al. 2007). From birth todeath, the total amount of sleep required daily declines steadily (Figure 1).

4
Figure 1. Change of sleep and activity patterns in the course life
It is characteristic of the modern 24/7 society that it may be challenging for both adultsand children to get enough rest and sleep. In fact, an inadequate amount of sleep seems to bea consequence of the modern life-style, associated with the technology of our time (Jenni andO'Connor 2005). A brief history of sleep recommendations for children concludes, thatchildren never get enough sleep according to current recommendations (Matricciani et al.2012). However, it is universally acknowledged that there is a lack of scientific evidence forsleep recommendations for children. In general, the recommended amount of sleep forinfants and toddlers is 12–15 hours, for school-aged children 10–11 hours and for teens 8–9.5hours (Matricciani et al. 2013).
2.1.3 Cycles of sleepA typical daily cycle for humans is approximately 16 hours of wakefulness and activity and8 hours of sleep and resting, in parallel with the rhythm by which society functions. Thepropensity to fall asleep depends on the duration of the preceding wakefulness episode.When the duration of being awake increases, sleep pressure accumulates and reaches acritical point, when sleep onset is reached. The process is called the homeostatic process andruns parallel with the daily 24-hour rhythm (Borbèly 2009). Twice a day (4 PM and 4 AM)there is a strong sleep pressure, and at certain point after sleep deprivation the pressure is sopowerful that an individual will fall asleep regardless of any strategy to fight against sleeping(Lavigne et al. 2009). Light helps humans to control their sleep-wake cycle by sending aretinal signal to the hypothalamic suprachiasmatic nucleus, which is a network of brain cellsand genetic control acting as a pacemaker to the circadian timing system and promoting asleep-wake rhythm in adaptation to the environment (Moore 2013). Within the 24-hour sleep-wake system there is a separate system that governs sleep onsetand maintenance, known as the ultradian rhythm, by which sleep can be divided into fourrecurrent periods. One period consists of non-rapid eye movement (non-REM, N) sleep andrapid eye movement (REM, R) sleep (Iber et al. 2007), which are characterized by typicalelectro-myographic (EMG), electro-oculographic (EOG) and electro-encephalographic (EEG)features. Onset of sleep is usually through N sleep. N1 (stage 1, S1) is a transitional stage betweenwakefulness and sleep. It is the lightest sleep, which can easily be discontinued, and in whichthe arousal threshold is at its lowest. EMG shows a gradual diminution of muscle tonus andEOG slow, possibly asynchronous eye movements. Typical EEG patterns show rhythmic

5
alpha waves changing into a relatively low-voltage asynchronous slow activity pattern. Inadults N1 lasts few minutes in one period and constitutes approximately 2-5% of total sleep. N2 (S2) still can be described as light sleep. EMG patterns show further decline in muscleactivity. Heart rate and reactions to stimuli from the outside diminish. EEG is characterizedby the development of high-voltage waves with K-complex and sleep spindles. N2 lasts 15–30 min/period in adults and may constitute half of the total sleep time. N3 (S3 and S4) sleep is the deepest sleep, the one in which EEG slow delta waves dominateand neuronal activity is at its lowest. The temperature of the brain is also at a minimum andthe activation of ventilation and the cardiorespiratory system reduces. N3 constitutes 15-20%of total sleep time, lasting 30-40 minutes/period in adults. R sleep is characterized by intermixed low-voltage cerebral activity, showing sawtoothwaves and typically no K-complex. EMG shows substantially reduced muscle tone, evenatonia. Hallmarks of R sleep are phasic eye movements, which can be registered by EOG. Ingeneral, R sleep can be characterized as an activated brain in a paralyzed body. 20-25%(approximately 30 min/period) of total sleep time is R sleep. Age modifies the pattern of sleep stages. The length of one cycle of an adult is 90-100minutes on average and that of the newborn only 50-60 min. Typically, the proportion of Rsleep decreases by age. A newborn baby has R sleep more than a half of her/his sleeping time,while toddlers have R sleep approximately 20% of total sleep time. N3 is dominating inyoung children, being approximately 25% of total sleep time (Montgomery-Downs et al.2006). (Culebras 2002, Carskadon and Dement 2011)
2.1.4 Respiratory patterns of sleepRespiratory patterns of sleep go through multiple maturational changes from infancy toadulthood. A visible sign of change is a decrease of the breathing frequency during sleep: anewborn baby breaths approximately 40 times per minute, an infant 30 times, a preschoolchild 20 times, a school-aged child and an adolescent 18 times per minute. The rates are notin relation to body weight and boys seem to have higher breathing rates than girls (Ross andRosen 2014). Furthermore, respiration frequency is decreased during sleep compared withdaytime activity and varies in parallel to sleep states. In N sleep minute ventilation decreasesand upper airway resistance increases. During R sleep respiration is irregular in terms of bothfrequency and volume (Ross and Rosen 2014). Short central respiratory pauses are a common finding in healthy children during R sleep.The frequency of the central pauses expressed with apnea episodes per hour of total sleeptime decrease from 2.4 in 1-year-old children to 0.5 in 12-year-olds (Scholle et al. 2011). Ingeneral, overnight polysomnographic (PSG) records of healthy children undergodevelopmental changes during childhood, most of the differences occurring when childrenare approximately 5-6 years old. For example, average obstructive apnea index shows slightincrease and in line with the study of Scholle, central apnea index shows slight decrease.Further, the older children sleep a greater amount of sleep time in supine position(Montgomery-Downs et al. 2006). Generally, the respiratory process is conducted by metabolic and physiologic factors.Carotic and aortic chemoreceptors sense the arterial concentration of oxygen and carbondioxide being responsible for most ventilator responses to variations in concentrations. It isnoteworthy, that in newborns peripheral chemoreceptors adopt a greater role in controllingthe ventilation process compared with adults. During development peripheral

6
chemoreceptors undergo a progressive diminution in sensibility (Marcus et al. 1994, Rossand Rosen 2014).
2.2 SLEEP DISORDERED BREATHING (SDB) – GENERAL ASPECTS
2.2.1 Historical aspectsFat boy Joe, a comically drawn figure in a book by Charles Dickens published in 1837, was achubby, rubicund, perpetually hungry servant boy, who fell asleep snoring loudly in themiddle of his tasks at any time of the day. This was the first time the obvious obesity-hypoventilation syndrome and perhaps also sleep apnea were described in the literature.Later on, the association between obesity and sleeping problems has come to be a target ofinterest, and in the medical literature the condition was described as obesity-hypoventilationsyndrome in 1955 (Auchinloss et al. 1955) and as Pickwickian syndrome in 1956 (Bickelmannet al. 1956). Since the 1980`s, medical research and knowledge of the associations of sleep,breathing and obesity and also other risk factors have increased enormously among healthprofessionals as well as among the general public.
2.2.2 Definition and classificationSDB is a continuum of medical disorders that encompasses the conditions snoring (primaryand habitual), upper airway resistance syndrome (UARS) and OSA (Figure 2). The mildestsymptom and often a hallmark of OSA is snoring. There is no generally accepted,unambiguous definition for snoring. In American English the condition is defined as “tobreathe during sleep with harsh, snorting noises caused by vibration of the soft palate”(American Heritage Dictionary of the English Language 2016). In practice, the humanconception of the typical sound is the golden standard. It is generated at the level of the upperairway, the typical features being a noisy sound when the soft palate vibrates and restrictsthe passage of air to and from the lungs. Primary snoring (PS) means snoring without anypathologies, e.g. daytime sleepiness, sleep disturbances, apnea, hypoventilation, hypoxemiaand hypercarbia (Ng et al. 2006). Habitual snoring (HS) refers to snoring more than threenights per week (Li et al. 2015). UARS is characterized by inspiratory flow limitation, increased upper airway resistanceand frequent cortical arousals, but without apneas, hypopneas or desaturation(Guilleminault et al. 1993). In the literature there are some considerations for UARS to be adistinct entity separately to OSA, because there are some differences in the clinicalpresentation (Stoohs et al. 2008). Further, the progression from UARS to OSA is questionable,and there is no scientific evidence to demonstrate the evolution of this condition. However,currently the International Classification of Sleep Disorders does not define UARS as aspecific entity; it is described as a subgroup of OSA (Iber et al. 2007). OSA, which is the most serious symptom of the condition, is defined as a disorder ofbreathing during sleep characterized by prolonged partial upper airway obstruction,intermittent complete or partial obstruction (obstructive apnea or hypopnea) or both andprolonged and intermittent obstruction that disrupts normal ventilation during sleep(American Academy of Sleep Medicine 2014). In adult OSA patients these events occurthroughout the sleep. In children, obstructive apneas occur mostly during R sleep (Goh et al.

7
2000). The severity of OSA is assessed by the number of apneas and hypopneas per slepthour and expressed by the apnea/hypopnea-index (AHI). OSA is a chronic progressivedisease, the progress of the condition mainly depending on weight gain and, to a lesserdegree, time (Berger et al. 2009).Sleep apnea can also be generated at the level of the central nervous system (central sleepapnea), neurophysiologically being due to a temporary failure in the pontomedullarypacemaker that generates the breathing rhythm. Central apneas (in addition to obstructiveapneas) usually associate with different syndromes (e.g. Prader Willi and Down syndrome)and further, central apneas can be seen with congestive heart failure or chronic opioid use(Javaheri and Dempsey 2013). The present dissertation focuses on the obstructivemanifestation of the condition.
Figure 2. The spectrum of SDB from primary snoring to severe sleep apnea
2.2.3 Epidemiology – prevalence of OSA in adultsGenerally, the most recent estimates of the prevalence of OSA vary between 15–20% amongthe adult population (Peromaa-Haavisto et al. 2015). The prevalence of the condition isincreased in the presence of a certain risk factor; i.e., obesity, increasing age, male gender,family history, craniofacial disorders, tobacco smoking and alcohol consumption. Accordingto Finnish population studies and the register of hospital treatment periods (HILMO) of theFinnish National Research and Development Centre for Welfare and Health (Stakes),approximately 150,000 Finnish adult patients suffered from OSA more than ten years ago(Laitinen et al. 2003), the prevalence being 2.8%. In parallel with the global obesity epidemic,the prevalence of OSA has increased. Furthermore, the condition is still roughlyunderdiagnosed. Globally, the estimates for the prevalence of OSA vary surprisingly little,suggesting that the prevalence is equal in Western societies and developing countries (Kapur2010).

8
2.3 SDB IN CHILDREN
In children, the most severe manifestation of SDB, obstructive sleep apnea, was firstdescribed by Guilleminault in 1976 (Guilleminault et al. 1976). In their work they reportedthe cases of eight children, 5 to 14 years, who suffered from excessive daytime sleepiness,decrease in school performance, abnormal daytime behavior, nocturnal enuresis, morningheadache, abnormal weight and progressive development of hypertension. The symptomswere associated with loud snoring and breathing pauses while sleeping and the conditionwas diagnosed by nocturnal polygraphic monitoring. Since then, the diagnostics and criteriafor pediatric SDB have been under refining. Especially in children, SDB is believed to beunrecognized and underdiagnosed (Alkhalil and Lockey 2011), thus obviously, thediagnostics of pediatric SDB is still a matter of discussion.
2.3.1 PrevalenceSleep disturbances are currently a public health concern throughout the world. Theyinfluence millions of people and their prevalence is increasing both in adults and in children.The frequencies of pediatric SDB and its different manifestations are outlined in Table 1. Thelarge variation in the prevalencies of SDB and its different manifestations is somewhatconfusing. It seems that the condition is difficult to assess because of the disparity of thedefinition and diagnostic methods. Snoring, which can be defined as the mildest form of SDB or on the other hand the hallmarkof SDB, is very common. Almost every child snores when suffering from an upper airwayinfection or allergic rhinitis. On the other hand some children snore every night – withoutany co-existing medical condition. The prevalence of childhood snoring has been reportedto be between 2 and 34%, varying by definition. For comparison, the study using thedefinition of “snoring sometimes or often” the prevalence is 29.0% (Sanchez-Armengol et al.2001) while definition “snoring loudly frequently or almost always” shows the prevalence10.5% (Goodwin et al. 2003). According to a meta-analysis the global prevalence of snoringin children as observed by the parents by any definition is 7.45% (Lumeng and Chervin 2008).
The meta-analysis of population based studies shows that the prevalence of parental-reported apnea in the children usually varies between 0.2 and 4.0%. The same study reportsa wide variation of prevalence of OSA diagnosed with polysomnography, the ranges beingfrom 0.1 to 13.0%, even though most studies agree on ranges from 1 to 4%. The prevalenceof UARS is seldom reported in the literature (Lumeng and Chervin 2008).
The prevalence of the whole entity, – SDB, encompassing all the above-mentionedsymptoms and reported by the parents, has mostly been estimated to vary between theranges 4 and 11% (Lumeng and Chervin 2008, Bixler et al. 2009). The condition is suggestedto be most common among pre-school children, at which age the lymphoid tissue of thepharynx is large in relation to the pharyngeal airway (Linder-Aronson and Leighton 1983).Some studies suggest that in that group, SDB affects up to one third of the children(Castronovo et al. 2003, Bonuck et al. 2011).
Generally, sleep disorders are suggested to be more prevalent in boys (Paavonen et al.2000) and like in adults, boys to have more SDB compared with girls (Gill et al. 2012). Thereare also studies to show no gender difference in the prevalence of SDB (Goodwin et al. 2003,

9
Liukkonen et al. 2008). It must be highlighted, that the epidemiologic data on this issue iscontroversial because of variations in definition and diagnostics, sampling methods, racialaspects and also the effect of age. More effort is definitely needed to harmonize the issue interms of diagnostic criteria and epidemiology.

10
T ab l
e 1.
The
rep
orte
d pr
eval
ence
s of
chi
ldre
n w
ith s
ympt
oms
of S
DB a
ccor
ding
to
loca
tion
, ag
e, s
ever
ity
and
diag
nost
ics
Au
thor
(s)
Loca
tion
nA
ge
(yrs
)S
nor
ing
%S
DB
%U
AR
SP
SG
%O
SA
PSG
%
An u
ntas
eree
et
al.
(200
1)Th
aila
nd11
426-
138.
5ha
bitu
al s
noring
a0.
69AH
I1
San
chez
-Arm
engo
l et
al.
(200
1)Sp
ain
101
12-1
629
.0so
met
imes
or
ofte
n3d
Kar
a et
al.
(200
2)Tu
rkey
1211
6-13
2.4
habi
tual
sno
ring
b
Cas
tron
ovo
et a
l. (2
003)
Ital
y60
42-
834
.5 a
lway
s an
d of
ten
12.0
pat
holo
gic
snor
ing/
PSG
c
13O
DI
5
Goo
dwin
et
al.
(200
3)U
SA
1494
4-11
10.5
loud
ly f
requ
ently
or
alm
ost
alw
ays
Ros
en e
t al
. (2
003)
USA
850
8-11
2.2
/PSG
i
Chn
g et
al.
(200
4)Sin
gapo
re10
279
4-7
28.1
sno
ring
d
6.0
hab
itual
sno
ring
e
Got
tlieb
et
a l. (2
004)
USA
205
512
.13
nigh
ts/w
eek
29.8
/PS
Gj
24.2
pare
nt-r
epor
tedj
Zha
n g e
t al
. (2
004)
Aust
ralia
996
4-12
24.9
hab
itual
f and
infr
eque
nt s
nori
ngg
15.2
hab
itual
sno
ring
Jonh
son
& R
o th
(200
6)U
SA
1014
13-1
66.
0 ev
ery
or n
early
ever
yni
ght
6.0
wee
kly,
par
ent-
repo
rted
k
Liuk
kone
n et
al
. (2
008)
Finl
and
1071
1-6
18.7
2n
ight
s/w
eek
Tab l
e 1.
Con
tinue
s

11
Tab l
e 1.
Con
tinue
s
Urs
chitz
et
al.
(201
0)G
erm
any
1144
7-12
1.9
AH
I1
Bro
ckm
ann
et a
l. (2
012)
Ger
man
y11
147-
126.
1 pr
imar
y sn
orin
g/PS
Gh
1n1
AH
I1
Fad z
il Ab
dulla
h et
al.
(201
2)M
alay
sia
505
6-10
14.9
par
ent-
repo
rted
d
Ala
b i e
t al
. (2
012)
Nig
eria
909
3-16
34.2
oft
en o
r al
way
s
Sau
er e
t al
. 20
12G
erm
any
4318
5.5
3.3
pare
nt-r
epor
tedd
0.21
AH
I1
Vah
er e
t al
. (2
013)
Esto
nia
706
8-9
16.5
par
ent-
repo
rted
l
An u
ntas
eree
et
al.
(201
4)Th
aila
nd98
35 8.5
13 s
noring
mos
t ni
ghts
10.9
sno
ring
mos
t ni
ghts
Gud
nado
ttir e
t al
. (2
016)
Sw
eden
731
tota
l18
116
1
0-11
6-8
9-11
4.8
pare
nt-r
epor
tedm
6.1
pare
nt r
epor
tedm
3.7
pare
nt-r
epor
tedm
Gup
ta e
t al
. (2
016)
Indi
a83
19
urba
n 10
.2d
rura
l 13.
5d
asn
orin
g on
mos
t nig
hts
bsn
orin
g ev
ery
nigh
t c
snor
ing
pres
ent m
ore
than
30%
of t
he to
tal s
leep
tim
ed
not d
efin
ede
snor
ing
freq
uent
ly o
r con
stan
tly (i
.e. >
3 ni
ghts
per
wee
k)f sn
orin
g >
4 tim
es p
er w
eek
gin
freq
uent
snor
ing
< 4
times
per
wee
kh
snor
ing,
AH
I<1,
RDI
<1 a
nd O
DI<4
i AHI
5 an
d pa
rent
-rep
orte
d sn
orin
g an
d fa
lling
asle
ep w
atch
ing
tele
visio
n or
in sc
hool
j freq
uent
snor
ing,
loud
or n
oisy
bre
athi
ng d
urin
g sle
ep o
r witn
esse
d ap
nea
klo
ud sn
orin
g, g
aspi
ng/c
hoki
ng, s
nort
ing,
aw
aken
ing
with
gas
ping
or c
hoki
ng o
r mom
enta
ry p
erio
ds o
f sto
pped
or a
bnor
mal
bre
athi
ngl he
avy
or lo
ud b
reat
hing
, sno
ring,
disr
uptio
n of
bre
athi
ng d
urin
g sle
epm
freq
uent
snor
ing,
apn
ea o
r cho
king
dur
ing
slee
pn A
HI<1
and
RDI
1

12
2.3.2 SymptomsChildren with SDB have diverse symptoms that differ from those in adult population.Especially in children there is much individual variation in the symptoms which makes itdifficult to make a diagnosis based on the symptoms. While awake, children with SDB are often mouth breathers (Ali et al. 1993, Kawashima etal. 1999, Xu et al. 2006). Furthermore, hyponasal speech, nasal congestion, swallowingdifficulties, poor appetite and prolonged duration of meals (Ahlqvist-Rastad et al. 1988,Kawasihima et al. 1999, Sakellaropoulou et al. 2012) are reported to be the symptoms ofchildhood SDB. Also morning headache and daytime naps are typical to the children withSDB (Xu et al. 2006, Zarowski et al. 2007). The most common and recognized symptom of childhood SDB while asleep is snoring(Lumeng and Chervin 2008). Nocturnal oral breathing is also typical symptom of SDB(Bonuck et al. 2011). The children with more serious manifestations of SDB have breathingpauses observed by the caregivers (Bonuck et al. 2011). Restless sleep and body movementswith odd sleeping positions, nightmares, excessive vocalization and sweating are typicalnight-time symptoms (Ersu et al. 2004). Furthermore, some studies suggest nocturnalenuresis to associate with childhood SDB (Ersu et al. 2004, Alexopoulos et al. 2014). Theremay also be difficulties in breathing with an inward movement of the upper chest duringinspiration (Wang et al. 1998). The downward motion of the diaphragm causes the abdomento move outward when negative intrathoracic pressure manifests as paradox inwardmovement of the rib cage (Bower and Gungor 2000). This confusing motion of the chest oftenfrightens parents and leads them to consult a doctor. It is suggested that the main symptoms in children might change with age (Sinha andGuilleminault 2010). Infants, among whom the prevalence of snoring is 9%, (Piteo et al. 2011)are described as having “noisy breathing” and poor suck. Toddlers snore loudly and sleeprestlessly, moving around the bed. With pre-school children enuresis and problems withwaking up may become an issue. In children of school-age, diversity of the symptomsincreases. Long-term sequelae of the condition are apparent in this age group, and behavioraland cognitional consequences start to appear. In adolescence, psychological problems, suchas depression become more apparent (Sinha and Guilleminault 2010). Furthermore, studies show that there is an association between childhood SDB and sleepbruxism (Kawashima et al. 1999, Ohayon et al. 2001). Interestingly, high and moderateexposure to second-hand smoke (which is also shown to be a risk factor for childhood SDB)is associated with sleep bruxism in children (Montaldo et al. 2012, Jara et al. 2015).
2.3.3 Risk factorsLymphoid tissue of the pharynxPharyngeal lymphoid tissue consists of adenoid (pharyngeal tonsil), tonsils (palatine tonsils)and lingual tonsils and together they form an entity called Waldeyer´s ring. The majorfunction of this tissue is to participate in the generation of antigen-specific immune responseswith formation of immunoglobulin (IgA, IgG and IgM) -producing plasma-cells. This activeimmunologic cascade leads to physiologic proliferation of the lymphoid tissue in childhood(Gross and Harrison 2000). Adenotonsillar hypertrophy (ATH) is the most common riskfactor for pediatric SDB (Arens et al. 2003, Dayyat et al. 2007). The volume of the adenoid and

13
tonsils increases from birth up to the age of twelve years, the peak of the proportional sizerelated to the skeletal structures occuring around 5-6 years of age (Dayyat et al. 2007). Duringthe first eight years of life, pharyngeal lymphoid tissue is likely to be exposed to stimuli thatpromote cellular proliferation (Papaioannou et al. 2013). For this reason, childhood SDB ismost common during pre-school and early school years (Corbo et al. 2001). Even thoughnasal resistance decreases from 9 to 13 years of age, there is a transient prepubertal increasein the resistance, a phenomenon suggested to result from hormonal changes (Crouse et al.2000). Many environmental and medical factors may irritate and cause proliferation of thelymphoid tissue, e.g. passive smoking (Zhu et al. 2013), seasonal variability (Walter et al.2013), atopy and allergic rhinitis (Ishman et al. 2012) and asthma (Malakasioti et al. 2011). Inaddition, infection by respiratory syncytial virus, sinus problems and recurrent upper airwayinfections may predispose children to ATH (Redline et al. 1999, Goldbart et al. 2007,Tsaoussoglou et al. 2014). Lingual tonsil hypertrophy may be found in SDB children in with and without medicalconditions such as obesity and several craniofacial anomalies. Obesity and 21-trisomy havebeen shown to be risk factors for adenotonsillectomy (ATE) failure, the reason beingundiagnosed lingual tonsil hypertrophy as a possible reason for failure (Kuo and Parikh2014).
Craniofacial morphologyAccording to recent studies, dental malocclusion and craniofacial characteristics of childrenwith SDB seems to differ from those of children without it. A Swedish study examined acohort of 4-year-old children. Children with SDB had smaller cranial base angle and lowerratio of posterior/anterior total face height. They also had a narrow maxilla, a deep palatalheight, a short lower dental arch and more lateral cross bite than the controls. The treatmentof obstruction (ATE) seemed to diminish the mandibular inclination but the tendency for anarrower maxilla persisted (Löfstrand-Tideström et al. 1999, Löfstrand-Tideström andHultcrantz 2007, Hultcrantz and Löfstrand-Tideström 2009, Löfstrand-Tideström andHultcrantz 2010). An Italian study with untreated 4.5-year-old children with apneas showedcharacteristics of skeletal Class II sagittal relation with retrognathic mandible and increasedskeletal discrepancy (Marino et al. 2009). A study in Finnish children with SDB showeddeviations in the dental occlusion compared with non-SDB children, the typicalcharacteristics being increased overjet, a reduced overbite and narrow upper and short lowerdental arches (Pirilä-Parkkinen et al. 2009). Cephalometrically, the same children had aretrusive and vertically growing mandible, long and thick soft palate, low positioned hyoidbone, large craniocervical angle, narrow airway diameter at the level of naso- andoropharynx and large diameter at the tongue level compared with children without SDB(Pirilä-Parkkinen et al. 2010). In summary, a recent systematic review and meta-analysis byFlores-Mir and colleagues suggested retrusive chin, steep mandibular plane, verticaldirection of growth and a tendency toward Class II malocclusion to be the typicalcharacteristics of SDB children (Flores-Mir et al. 2013). Altogether, these features may causean abnormal breathing pattern, and lead to further alterations to the oral and facial muscularbalance. It is likely that skeletal and occlusal development in children is further affected bythis association, possibly resulting in risk of SDB (Peltomäki 2007).

14
Craniofacial anomaliesChildren with many developmental craniofacial anomalies are at increased risk for SDB(Moraleda-Cibrian et al. 2014). Structural and functional changes present in the upper airwayof infants with cleft lip and/or palate confer an increased risk of SDB (Smith et al. 2014). Inolder children with cleft lip and/or palate dysfunction of the palatal structures controllingthe soft tissue and morphological abnormalities of the maxilla and mandible producing asmall nasopharyngeal lumen result in high risk for SDB. The risk is compounded by surgicaloperations to correct the structural anomalies which further decrease the airway dimensions(MacLean et al. 2009). In children with trisomy 21 the risks for SDB are associating generalized hypotonia andpharyngeal collapsibility, independent of age, gender, and body mass index (BMI) (Fung etal. 2012) and macroglossia. The high prevalence of SDB in children with BeckwithWiedermann syndrome is multifactorial and not solely the result of a large tongue (Follmaret al. 2014). Young patients with achondroplasia may suffer from obstructed airways (Reidet al. 1987). Furthermore, syndromes associated with midface hypoplasia (Treacher Collins,Crouzon, Apert and Pfeiffer syndrome) and mandibular micrognathia (Pierre Robin andMarfan syndrome) predisposes to SDB (Spier et al. 1986, Hoeve et al. 2003, Sinha andGuilleminault 2010).
Other risk factorsMultiple medical conditions may increase the risk for SDB. Children with asthma have twiceas much SDB than those without it. The association between asthma and SDB seems to beevident from a physiological context, an inflammatory pathway of the airway being the linkbetween the conditions (Brockmann et al. 2014). Often the obstruction to the upper airwayexists at the level of the nose. Common causes of nasal obstruction include allergic rhinitis,septal deviation, chronic sinusitis and nasopharyngeal stenosis; all raising the risk for SDB(Li and Lee 2009). Infants and toddlers with gastroesophageal reflux may have an increasedrisk for SDB (Koivusalo et al. 2011). In neuromuscular diseases, such as Duchenne musculardystrophy and congenital myopathy, inspiratory muscle weakness may lead to alveolarhypoventilation and reduced pulmonary gas exchange and further, to SDB (Anderson et al.2012). Children with cerebral palsy (CP) have a more than three-fold higher risk of SDBcompared with normally developing children. Interestingly, sleep problems among childrenwith CP include insomnia and excessive daytime sleepiness more often compared tonormally developing children (Sandella et al. 2011). Laryngomalacia in young children alsoraises the risk for SDB (Li and Lee 2009). Furthermore, history of prematurity (Manuel et al.2013) associates with the SDB. The recent systemic review showed a significant association between childhood SDB andsecondhand smoke (i.e. parental smoking) and recommended smoking cessation tocaregivers (Jara et al. 2015). Furthermore, a parental history of SDB raises the risk for thecondition. This familial clustering suggests that genetic factors may constitute a risk factorfor OSA and SDB (Friberg et al. 2009).

15
ObesityIt is disquieting that overweight and obesity are becoming more common in children andadolescents in many developed countries (Kipping et al. 2008). In Finland, 10% of childrenand 26% of adolescents are overweight (Vuorela et al. 2009). Furthermore, the sameresearcher group showed that in the last decades the prevalence of overweight and obesityhas even increased among adolescents, especially in boys (Vuorela et al. 2011). Excess bodyadiposity is a well-recognized risk factor for SDB in adults (Leinum et al. 2009), but it has alsobeen suggested to be an important risk factor for pediatric SDB (Marcus et al. 1996, Ng et al.2004, Verhulst et al. 2008). The mechanism by which obesity predisposes to SDB may be themass loading of the upper airway and respiratory muscles causing modification tomorphology and function, reduction of chest compliance, changes in respiratory drive andimpairment of functional residual capacity, all increasing the risk of upper airwayobstruction (Kohler and van den Heuvel 2008). Age and ethnicity modify the impact ofobesity on SDB. In older children there are more associations between body adiposity andSDB compared with younger ones, and in terms of ethnicity, the same association appears tobe more prevalent among African American and Asian children (Kohler and van den Heuvel2008). A large neck circumference of the children is also associated with SDB (Redline et al.1999). It is suggested that two types of SDB exist, one associated with ATH among normalweighted children and the other associating primarily with obesity without ATH (Dayyat etal. 2007). Interestingly, it has recently been demonstrated that deviations in craniofacialmorphology are much more common in normal weight than overweight adult patients withOSA, implying that there may be two different phenotypes of adult SDB; one related to excessadipose tissue and the other to craniofacial abnormalities (Pahkala et al. 2011).
2.3.4 PathophysiologyThe upper airway is a complex structure that is usually divided into four anatomicalsubsegments: nasopharynx (between the nares and hard palate), velopharynx (between thehard palate and soft palate), oropharynx (from the soft palate to the epiglottis) andhypopharynx (from the base of the tongue to the larynx) (Ayappa and Rapoport 2003). Thisstructure is surrounded by more than 20 muscles that actively modify the airway lumen(Fouke et al. 1986). There is also lymphoid tissue, i.e., adenoid, tonsils and lingual tonsils.The main bony structures that determine the area of the airway lumen are the hyoid boneand the mandible. The transition from wake to sleep relaxes the muscles of the upper airway,resulting in collapsibility of the airway structures and an increased resistance to airflow. Inhealthy subjects this increase may be 3-5 mmHg in PCO2 (Horner 2008a). Upper airway obstruction takes place during inspiration in parallel with an increase of thepressure surrounding the structures, and there are three elements that contribute to this:morphological narrowing, abnormal neuromuscular control and inflammation (Sinha andGuilleminault 2010). The airway is narrowest at the level of the oropharynx behind the softpalate. When the upper airways are morphologically narrow, the relaxation during sleep ofpharyngeal muscle tonus may predispose to clinically significant diminutions in inspiratoryairflow and limitation of it (snoring and hypopneas) and even pause of airflow because oftotal airway closure (obstructive apneas). A major contributor to this cascade is posteriormovement of the tongue (Horner 2008a). The neuromuscular control cascades responsible for the tonic sleep-state-dependent inputs

16
to the motoneurons innervating the pharyngeal muscles are defined by information gainedfrom animal studies (Horner 2001, Horner 2008b). Serotonin and noradrenaline-containingneurons give excitatory stimuli to the motoneurons of the pharyngeal muscles. Theseneurons are most active in wakefulness, less active in N sleep and least active in R sleep,which may lead to decreased pharyngeal muscle activity in sleep (Chan et al. 2006). There isalso neuromuscular compensation with increasing respiratory effort sustaining patency ofthe upper airway, and this sometimes leads to arousal (Katz and D'Ambrosio 2008). Inflammation, both local and systemic, can lead to increased resistance of the upper airway.Acute or chronic inflammation of lymphoid tissue contributes to chronic activation of thecell-mediated and humoral immune response, resulting in ATH and furthermore, causingobstruction of the airway (Zautner 2012). In terms of systemic inflammation it has beenshown that C-reactive protein (CRP) levels are increased in patients with SDB, independentof body adiposity (Tauman et al. 2004, Kheirandish-Gozal et al. 2006). Episodic hypoxia andarousal launch endothelial dysfunction and systemic inflammation (Kato et al. 2000,Apostolidou et al. 2008), the same process leading to sympathetic activation. This may leadto increased insulin resistance (Punjabi et al. 2004) and blood pressure (O'Brien and Gozal2005).
2.3.5 ConsequencesPsychological effects, cognition and quality of lifeToday, there is a lot of evidence of the behavioral and cognitional difficulties associated withchildhood SDB. SDB of any severity is associated with poor behavior but not with poorcognitive performance (Jackman et al. 2012) and furthermore, SDB is associated with reducedquality of life in 3- to 5-year-olds (Jackman et al. 2013). A study of Gozal shows thatneurocognitive deficits seem to co-exist with the most severe manifestations of SDB (Gozalet al. 2010). Mood disorder symptoms are also shown to associate with SDB (Aronen et al.2009). On the other hand, it has been shown that there is only minimal association with SDBand children´s typical mood, expressive language skills, visual perception, and workingmemory, but there is a significantly stronger association with parent reported emotioninstability (e.g. deterioration in behavior and emotion regulation, school performance,constant and selective attention and alertness) (Beebe 2006). Children with SDB have lowergeneral intellectual ability regardless of severity compared to those with no SDB. Impairmenthas also been observed in academic and executive functioning (Bourke et al. 2011).Furthermore, among preschool children SDB seems to associate with reduced quality of lifeof both the children and their families (Jackman et al. 2013). It has also been shown in alongitudinal study with young children that snoring predicts mental disturbances inadolescence (Gozal 2001). Difficulties in behavior and emotions, such as hyperactivity,aggression, irritability, rebelliousness, conduct problems and impaired concentration arecommon with pediatric SDB (American Thoracic Society 1999). Excessive daytime sleepinessis sometimes observed in children, prevalence varying from 7% to 43% (Carroll et al. 1995,Chervin et al. 2006). Large variation may be explained by the different methods used fordetermining excess daytime sleepiness as well as confounding factors, such as obesity (Gozaland Kheirandish-Gozal 2009). ADHD is a complex, life-lasting disorder which is typically associated with inattentiveness,hyperactivity and impulsivity. The literature shows, that children with ADHD suffer frommore sleep disorders than children without it (Kurnatowski et al. 2008, Chiang et al. 2010,

17
Souly et al. 2013). Most parents of ADHD children have reported their children to suffer fromlow quality sleep; typical complaints were snoring, arousals, motor restlessness and legdiscomfort at night (Silvestri et al. 2009). The signs and symptoms of ADHD children arenotably similar to those of SDB. It has been shown, that SDB can lead to mental characteristicsidentical to ADHD (Chervin et al. 2002) and has even been suggested that surgical treatmentof ATH might result in a significant decrease in the severity of ADHD-like symptoms (Amiriet al. 2015). The mechanism of the impairing effect of SDB on psychological context is under debate.Milder and at the same time more common manifestations of the SDB may even have thestrongest effects on psychological functions with pre-school children (Jackman et al. 2012).The study of Jackman suggests, that theoretically snoring itself may be more harmfulrespiratory event among young children than apneas or hypopneas. Snoring may lead tosignificant physiological changes (e.g. inflammation or sleep fragmentation) even to an equalor greater extent than apneas and hypopneas. Literature shows that the milder forms(snoring) may cause problems with sleep fragmentation and severe forms (OSA) by hypoxia(O`Brien et al. 2004). As a consequence, sleep homeostasis may be disturbed. Regardless ofthe severity of the symptom or body adiposity, children with SDB had more deterioration inquality of life and depressive symptoms than children without the condition (Crabtree et al.2004). Further, sleep disturbances cause simply fatigue and stress in both children andparents, and that fact interferes with multiple aspects of children´s lives, including the mentalcontext. In terms of the causality, the recovery of mild/moderate SDB by ATE is associatedwith improved behavior and functioning, suggesting that the relation between SDB anddaytime problems in children is a causal one (Ali et al. 1996).
Growth impairmentGrowth impairment is shown to be a typical feature of advanced SDB (Bonuck et al. 2009).The decline of growth with SDB may occur because of a disruption of growth hormonesecretion in parallel with disruption of the sleep architecture. Nieminen concludes in histhesis that growth impairment in pediatric OSA is associated with reduced concentrations ofinsulin-like growth factors and binding protein, suggesting reduced night-time growthhormone secretion to be secondary to upper airway obstruction (Nieminen 2002). Thealteration of nocturnal secretion of growth hormone may also affect the mandibular ramus,which is in line with morphological differences in the SDB children compared with childrenwith no SDB (Peltomäki 2007). In addition, in the case of SDB child with ATH there may bevarious craniofacial and myofunctional alterations negatively affecting other functions suchas mastication, swallowing, and speech (Souza et al. 2013). Furthermore, there may be specialfeatures such as insufficient lip closure, low position of the tongue, flabby tongue,mastication with half-open lips, position of the lower lip between the incisors and alteredswallowing (Valera et al. 2003). It is suggested that these characteristics may drain the child´scaloric resources which would otherwise be used for somatic growth. Furthermore, SDB maylead to growth failure via increased energy expenditure during restless sleep (Marcus et al.1994, Li et al. 2003).
Cardiovascular consequencesSDB in adults is a risk factor for hypertension and cardiovascular morbidity in the generalpopulation (Peppard et al. 2000). The association of childhood SDB and hypertension is not

18
straightforward. There are studies showing that children with any severity of SDB may haveelevated blood pressure (Marcus et al. 1998, Enright et al. 2003, Kwok et al. 2003). On theother hand, a meta-analysis found no evidence that moderate to severe SDB in childhoodincreases the risk of hypertension (Zintzaras and Kaditis 2007). Studies have shown that endothelial function is often altered with childhood OSA (Gozalet al. 2007). The inflammatory cascade which leads to endothelial dysfunction may have animportant role in the relation between SDB and cardiovascular disease. The presence ofcirculating inflammatory markers, such as CRP could support this theory. A recent studywith obese children and adolescents found no association between OSA and CRP levels.However, an association between CRP and measures of adiposity was found. The studysuggests that obesity, but not SDB results in an increased inflammatory status as measuredby CRP (Van Eyck et al. 2014).
Metabolic impactsChildhood OSA, sometimes co-existing with increased body adiposity, increases the risk ofthe metabolic syndrome (MetS) (Waters et al. 2007). MetS is the clustering of a set ofcardiometabolic risk factors thought to put the individual at increased risk of thedevelopment of cardiovascular diseases and type 2 diabetes (Owens and Galloway 2014). Onthe other hand, childhood obesity associates with OSA and high levels of insulin (Gozal etal. 2008). The strongest predictors of MetS in adulthood are childhood elevation of fastinginsulin levels and increased body mass index (BMI) (Brunner et al. 2002). Furthermore,insulin resistance in childhood is associated with increased risk for later cardiovascularmorbidity and mortality (Bao et al. 1996). The treatment of OSA in obese children issuggested to correct the insulin levels (Waters et al. 2007); this relationship between OSA andinsulin resistance has not been observed with normal weight children (Gozal et al. 2008).Altogether, metabolic changes in childhood OSA may be related to obesity, OSA acting as animportant mediator.
2.3.6 DiagnosticsThe diagnosis of childhood SDB is based on the anamnesis and clinical examination of thechildren and further, on supporting deviant findings in a polysomnographic record. A sleephistory screening for the symptoms of SDB should be part of routine health care visits,including oral health examinations. If there is a history of snoring, a detailed anamnesisshould be obtained, e.g. breathing breaks, enuresis, diaphoresis, daytime behavior/learningproblems or restless sleep (Section on Pediatric Pulmonology, Subcommittee on ObstructiveSleep Apnea Syndrome. American Academy of Pediatrics 2002). Physical findings of clinicalexamination are often normal. There may be findings relating to ATH, such as mouthbreathing, hyponasal speech or nasal obstruction. However, a recent meta-analysis suggeststhat clinical assessment of tonsil size by Brodsky classification (Brodsky 1989) is a weakpredictor of the severity of SDB (Kaditis et al. 2016). Sometimes there may be symptoms ofimpaired growth, systemic hypertension or an increased pulmonic component of the secondheart sound indicating pulmonary hypertension, even though these findings are rare andnonspecific (De Luca Canto et al. 2014). The golden standard for the diagnostics of SDB is overnight, attended, in-laboratory PSG(Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome.American Academy of Pediatrics 2002), which is the only diagnostic technique shown to

19
quantitate the ventilation and sleep abnormalities associated with the condition. It is anoninvasive test involving the measurement of a number of physiologic functions overnight,typical recordings including electrocardiography, electroencelography, pulse oximetry,oronasal airflow measured by both pressure sensor and thermistor, abdominal and chest wallmovements, partial pressure of carbon dioxide and video recording (Apostolidou et al. 2008).It can be performed at any age, but specific pediatric measuring and scoring criteria shouldbe used. In children, International Classification of Sleep Disorders (3rd edition) classifies AHIof equal or greater than 1 event per hour as abnormal (American Academy on Sleep Medicine2014). However, the relative complexity and high costs of PSG have spurred the quest foralternative diagnostic methods, especially for screening for the condition in children. The history of the symptoms of possible SDB can also be obtained by using thequestionnaires. A meta-analysis reviewed the diagnostic value of alternative methods(clinical history and physical examination) for childhood SDB (De Luca Canto et al. 2014).The authors concluded that in terms of screening for the condition questionnaires could bean acceptable method to determine the children who need to be referred to a sleep medicinespecialist, and they suggested the use of this method especially for dentists. A recent studyassessed the meaning of symptom history in detecting OSA (Kang et al. 2015). The symptomrecord consists of questions such as snoring patterns, night-time and daytime clinicalsymptoms and other OSA-related symptoms. The snoring pattern was evaluated by askingparents about the snoring frequency and duration, and further about the daytime symptoms(sleepiness, attention/hyperactivity problems, depression, low self-esteem, shyness and lowschool performance). The night-time symptoms included breathing pauses, awakenings,enuresis, nightmares and diaphoresis. Other OSA-related symptoms were also included inthe recordings. For example, snoring frequency had a sensitivity of 77% with a specificity of48% and tonsil size a sensitivity of 77% with specificity of 65% in detecting OSA. The resultsof this study suggest combining both history of symptoms and anatomical findings for ascreening scheme of childhood OSA.
2.3.7 Treatment of pediatric SDBOverweight or obese children are encouraged to a healthy way of life and weight loss. Inyoung children the implication of obesity as a risk for SDB is not very significant, althoughhigher body adiposity may predict development of SDB in the coming years (Kohler and vanden Heuvel 2008). ATE is suggested to be an effective and curative treatment modality in cases wherepediatric SDB and ATH co-exist (Laitinen et al. 2003, Wei et al. 2007) but there are also severalstudies which have failed to show any strong association with ATH and SDB (Li et al. 2002,Lam et al. 2006). It is shown that a significant number of children do not achieve completerecovery for SDB after the operation. Residual SDB after ATE may be associated with otherrisk factors, such as body adiposity or deviant craniofacial morphology (Bhattacharjee et al.2010). Furthermore, an American multicenter, single-blinded, randomized and controlledtrial (Marcus et al. 2013) studied children with OSA and ATH, allocating the children intotwo groups: ATE group and watchful waiting group. The results showed that after sevenmonths 42% of the children in the watchful waiting group no longer met the criteria of OSA.The study suggests that watchful waiting may be a rational option if a child has low OSAsymptom burden, little snoring, low AHI and normal waist circumference (Chervin et al.2015). However, the American Academy of Pediatrics suggests ATE as the primary treatment

20
for children with SDB and ATH (Marcus et al. 2012). In the case of deviant craniofacial morphology or malocclusion, orthodontic treatment issuggested as a primary treatment in children without ATH and as an additional treatment toATE when SDB persists (Praud and Dorion 2008, Huynh et al. 2016). There are studies toshow that orthodontic treatment, such as maxillary expansion (Guilleminault and Li 2004,Ashok et al. 2014, Machado-Júnior et al. 2016a) and functional treatments advancingmandible (Hanggi et al. 2008, Villa et al. 2012, Machado-Júnior et al. 2016b) may be effectiveas a treatment for pediatric SDB and also as prevention of adult SDB. However, it is alsosuggested that there is not enough evidence to show the efficacy of oral appliances orfunctional appliances in the treatment of pediatric OSA (Carvalho et al. 2007). Children withsevere syndromic craniofacial abnormalities may need invasive surgery, such astracheostomy, osteotomies or osteodistraction (Robison and Otteson 2011).
2.3.8 Other orthodontic aspectsAdequate spatial volume of the upper airways is a prerequisite for physiological respiration.A recent study shows that during development of children from 6 to 17 years of age, upperairway dimensions remain on average outstandingly unchanged, suggesting that the airwaydimensions are established in early childhood (Mislik et al. 2014). Small upper airwaydimensions that have developed in early childhood may expose to SDB and OSA later in life(Papaioannou et al. 2013) when normal soft-tissue changes caused by obesity, ageing orgenetics affect the patency of the oropharynx (Martin et al. 1997). In addition to impairedchildhood growth, spatial volume can be affected by ATH or nasal congestion caused byedema of the nasal mucosa, deviated nasal septum or nasal polyps. The obstruction may leadto postural adaptation (i.e., extension of the head), forward or downward positioning of themandible, tongue positioning forwards and open-mouth posture – all of which arephenomena to ensure adequate airway volume and furthermore, associated with at leastpartial oral breathing (Behlfelt et al. 1990). “Adenoid face” or “long face syndrome” are terms widely used when describing typicalcharacteristics associated with partial oral breathing. The classic facial features are narrowand long dimensions, lip apart posture at rest, short upper lip, flattened nose with smallnostrils, protruding upper incisors and further, self-reported “mouth breathing”. Behindthese traits lies typical malocclusion: increased facial height, over-erupted posterior teeth,backwards and downwards rotated mandible, class II occlusal relationship, open biteanteriorly, increased overjet, narrow V-shaped maxillary arch, high palatal vault and lateralcross bite (Linder-Aronson 1970, Macari et al. 2012). However, the debate about theorthodontic relevance of upper airway obstruction and its assumed effect on facial growthhas been ongoing for over a century, but no final conclusion has yet been reached (Vig 1998).
2.3.9 Childhood SDB associations to adult SDBThere are a few studies to evaluate the possible progression and natural evolution ofpediatric SDB, but without consensus. Among children, as well as among adults, male sexand body adiposity seem to be risk factors for the SDB (Goodwin et al. 2010, Spilsbury et al.2015), which suggests strong support for screening, preventing, and treating overweight inall age groups. On the other hand, milder forms of pediatric SDB do not seem to evolve intomoderate-to-severe SDB in adolescence (Bixler et al. 2016). However, no patient regardlessof age can contract OSA suddenly, over one night - there is always a history of evolution

21
from milder symptoms of the condition to the more severe ones. Craniofacial and occlusal development occurs in childhood. Adult patients with SDB havedeviations in craniofacial morphology and dental occlusion similar to those found in childrenwith SDB (Löfstrand-Tideström et al. 1999, Pahkala et al. 2011). It is obvious that withouttreatment, a child with craniofacial and dental risk factors and SDB, even after ATE, mayhave the condition. This raises the question of whether adulthood SDB could be preventedin some individuals by focusing on orthodontic treatment already in childhood.

22

23
3 Aims of the study
The general aim of this doctoral thesis was to investigate the risk factors, diagnostic methodand consequences of pediatric SDB in a population sample of Finnish children.
The specific aims of the doctoral thesis were
1. to study the associations of dentofacial and pharyngeal morphology and body fat withthe risk of having SDB in 6- to 8-year-old children (Study I).
2. to evaluate the lateral view photograph of the face as a tool for assessingmorphological properties as a risk factor for SDB in children and to investigate howreliably a group of health care professionals can visually observe the profile ofchildren from photographs to assess the convexity of their faces. A further aim was tostudy the feasibility of the use of photograph for the visual observation of the facialprofile (Study II).
3. to assess the determinants of psychological well-being in girls and boys attendingtheir first grade at primary school and further, to evaluate the role of SDB in it (StudyIII).
4. to analyze the associations of dentofacial and pharyngeal morphology and body fatwith the risk of having SDB at the age of 9-11 years and to evaluate the influence ofmouth breathing and orthodontic treatment on the condition. (Study IV).

24

25
4 Study design and study population
4.1 ETHICAL CONSIDERATIONS
The Research Ethics Committee of the Hospital District of Northern Savo reviewed andapproved the study protocol. All participating children and their parents gave their informedwritten consent.
4.2 DESIGN OF THE PHYSICAL ACTIVITY AND NUTRITION INCHILDREN (PANIC) STUDY
This dissertation was conducted as a part of the Physical Activity and Nutrition in Children(PANIC) Study. The PANIC study is a long-term controlled exercise and diet interventionstudy in a representative population sample of primary school children from the city ofKuopio, Finland (Figure 3). Altogether 736 children aged 6-8 years who started the first gradein primary schools of Kuopio in 2007–2009 were invited to participate in the baselineexaminations between October 2007 and November 2009. The participants were allocatedinto the exercise and diet intervention group (n=309) and the control group (n=203). Thechildren and their parents in the intervention group received intensive, family-basedphysical activity and diet counselling for two years. The control children did not receive anyintervention during the period. Because the intervention did not have any influence on theresults of the present study (data not shown), the participants were analyzed as one group,without allocation. A follow-up study was carried out with 440 children in 2009-2012 withthe same assessments as in the baseline study. Thereafter, a less intensive intervention willbe continued until adulthood in the intervention group. The participants will be examined inadolescence and in early adulthood.

26
Figure 3. Flow chart of the Physical Activity and Nutrition in Children (PANIC) Study population

27
The general aim of the PANIC study is to identify the risk factors and risk groups forchronic diseases already in early childhood and to study the effects of physical activity,sedentary behavior, diet, genetic factors, sleep and pain experience on health and well-beingamong children and adolescents. This doctoral dissertation follows a cross-sectional study design using the baselinemeasurements in studies I, II and III. The children in the intervention group had not receivedany exercise or diet intervention at the time of the baseline measurements, and theintervention and control children were treated similarly during the measurements.Therefore, this dissertation treats the baseline data as a cohort. Study IV is a follow-up study.
4.3 PARTICIPANTS
Invitation letters were sent to the children´s principal custodians by mail according to theregistration for the first class of 16 public schools in Kuopio. Private schools and classes forpreparing education for immigrant children and classes for children with special needs wereexcluded from the study. The parents were asked to contact the coordinator of the study toparticipate. If the parents did not get in touch, their willingness to participate was inquiredby telephone. Of the 736 invited children, 512 (70%) participated in the baselineexaminations. The participation rate varied between 55% and 87% among the schoolsincluded. Of the 512 children, 248 (48%) were girls and 264 (52%) were boys. The participantsdid not differ in terms of gender distribution, age or BMI-SDS from other children of the sameage from primary schools of Kuopio based on available school health examination data (datanot shown). Table 2 shows the number of participants, inclusion criteria and outcome variable(s) inStudies I-IV.
Table 2. Number of participants, inclusion criteria and outcome variable(s) in studies I-IV
Study Number ofparticipantsAll, Girls
Inclusion criteria Outcome variable(s)
I 466, 226 Dentofacial and pharyngeal morphology recordsavailableSleep questionnaire availableBody fat percentage measurement available
SDB
II 382, 184 Photograph in the lateral facial projectionavailable
Reliability of the method
III 412, 205 Psychological, physical and social well-beingquestionnaires availableSleep questionnaire availableBody fat percentage measurement availableCardiorespiratory fitness measurement available
Psychological well-being
IV 329, 161 Dentofacial and pharyngeal morphology recordsavailableSleep questionnaire availableBody fat percentage measurement available
SDB, incidence of SDB

28

29
5 Methods
5.1 ASSESSMENTS
5.1.1 Dentofacial and pharyngeal morphologyDentofacial and pharyngeal morphology were clinically evaluated by a standard orthodonticscreening method by one experienced orthodontist (T.I.). The occlusion was assessedaccording to the modified method of Björk (Björk et al. 1964) in the intercuspal position. Therecorded variables included molar occlusion (distal, normal or mesial), overjet (mm),overbite (mm), crowding ( 2 mm), spacing ( 2 mm), anterior and lateral open bite ( 2 mm)as well as cross bite and scissors bite. In cross bite, one or more lower posterior teeth arebuccal to the upper counterpart(s), while in scissors bite, the whole occlusal surface of theupper posterior teeth is buccal to that of the lower antagonistic teeth. The shape of the palatewas visually defined as wide, normal or narrow. The existence of adipose tissue under thechin was assessed visually. Facial profile (convexity, concavity and vertical dimension) wasalso assessed visually. To assess the actual airway between the tonsils the children wereasked to breathe through their nose, which then relaxes the pharynx and palatal area. Thetonsils were considered hypertrophied if there was 1 cm or less space between the tonsils.The definition corresponds to classes 3-4 of the Brodsky classification (Brodsky 1989). Softpalatal morphology was classified according to the Mallampati Classification, which is basedon clinical examination with maximal mouth opening and tongue protrusion in the seatedposition (Mallampati et al. 1985). Dominant mouth breathing was assessed visually duringthe clinical examination. Previous or ongoing orthodontic treatment was checked from thechild´s dental records and classified according to the most prevalent treatment modalities inFinnish children among the studied age groups: Quad helix, head gear, or other (mostlyeruption guidance appliance). Noteworthy, if an examination showed treatment need, a childwas referred to an appropriate professional (i.e., dentist, orthodontist, physician).
5.1.2 SleepSleep, SDB and associated factors were assessed by a questionnaire. The questions in thesleep questionnaire used were based on an established Finnish questionnaire that have beenused to screen for sleep disturbances and SDB (Partinen and Gislason 1995). The parentsfilled out the questions regarding the child’s quantity and quality of sleep, symptoms of SDB,frequency of upper airway infections and previous operative treatments, such as ATE.Unfortunately, the parents did not reliably remember their child`s possible ATE, so thisimportant data could not be used in the present study. SDB was defined as witnessedbreathing pauses (apneas) (sometimes, usually or always/almost always) and/or frequent(most of the sleeping time or frequently) and/or loud (quite loudly, loudly or extremelyloudly) snoring and/or nocturnal mouth breathing (usually or always/almost always)observed by the parents. In other words, if the child had one or more of above-mentionedsymptoms, he/she was defined as having SDB. Sleep duration was assessed using a combined heart rate and movement sensor (Actiheart,

30
CamNtech, Cambridge, UK), a single piece monitor that clips onto two standardelectrocardiogram electrodes (Bio Protech Inc., Munmak-eup, South Korea) that were placedon the child’s chest in a standardized manner (Brage et al. 2005). Children were asked to wearthe Actiheart device continuously for at least four consecutive days that included twoweekdays and two weekend days. The duration of sleep was evaluated over an average of4.1 nights and analyzed manually from the heart rate and movement data by one exercisespecialist and confirmed by one physician, if needed. Falling asleep was defined as the timepoint when the accelerometer counts had reached zero and the heart rate had settled downfor at least five minutes. Waking up was defined as the time point when the accelerometercounts and heart rate had increased continuously from zero. Sleep duration was calculatedas the time between these two time points.
5.1.3 Body composition and fitnessBody height was measured with head position being in the Frankfurt plane without shoes bya wall-mounted stadiometer with an accuracy of 1 mm. Body weight was measured by thebioimpedance method using the Inbody 720® device (Biospace Co. Ltd., Seoul, Korea) withan accuracy of 100 g. Both parameters were measured after an overnight fast. BMI wascalculated as weight (kg) divided by height (m) squared. Z-scores for height, weight and BMIwere assessed with an obesity calculator that uses age- and sex-specific British growthreference data from 1990 (Cole et al. 1995). BMI-SDS was calculated using Finnish growthreferences (Saari et al. 2011). Overweight and obesity were defined using the age- and sex-specific BMI cut-offs derived from growth curves corresponding to BMI values 25 and 30 inadults 18 years of age, published by the International Obesity Task Force (IOTF) (Cole et al.2000). Body fat percentage was assessed by the dual-energy x-ray absorptiometry (DXA)method using the Lunar® device (Lunar Prodigy Advance, GE Healthcare, Madison,Wisconsin, USA) in the afternoon in the non-fasting state. The cardiorespiratory fitness of thechildren was tested with an electromagnetic cycle ergometer with a pediatric saddle module(Ergoselect 200 K, Ergoline, Bitz, Germany) as previously described in detail (Lintu et al.2014).
5.1.4 PhotographA standardized method was used for photographing the participants. The photos were takenusing a Canon EOS 300D® digital camera in the lateral projection of the face at a distance oftwo meters. The children were standing in a natural head position (NHP) in front of a mirrorwith a little bubble level taped on their temple to control the correct head position. The paper prints of the photos were gathered into a folder and a short instruction guidealong with the profile figures was formulated. The folder was examined first by a referenceorthodontist (T.I.) and then by seven other healthcare professionals who work with children,i.e., another orthodontist, a dentist with extensive orthodontic experience, a general dentalpractitioner, an otorhinolaryngologist, a pediatrician, an oral hygienist and a public healthnurse. In addition, a dental student examined the folder. The observers classified the profilesvisually as normal/mildly convex, clearly convex or straight/concave based on three modelpictures (Figure 4).

31
Figure 4. Formula of normal/mildly convex, evidently convex and straight/concave profiles andinstructions to the observers
The photographic data was digitized and analyzed by Wincepht® 8.0 software in order toanalyze the profiles more objectively and further, to compare the subjective and objectiveassessment. Soft tissue landmarks Glabella (G`), Subnasale (Sn) and Pogonion (Pg`) weredigitally identified to calculate the angle G`- Sn - Pg` indicating the angle of facial convexity(Legan and Burstone 1980). Furthermore, soft tissue Nasion (Na`) and soft tissue Menton(Me`) were identified for the purpose of analyzing the reliability of the measurement of thevertical proportions (Sn`-Me`/Na`-Me`) of the face (Figure 5).
Figure 5. Digitized soft tissue landmarks on lateral facial photographs. Soft tissue Glabella (G`),Subnasale (Sn), Soft tissue Pogonion (Pg`), soft tissue Nasion (Na`) and soft tissue Menton(Me`)

32
5.1.5 Well-being measurementsThe parents completed the questionnaire concerning the child`s well-being during theprevious three months. The questionnaire was developed by the PANIC-researchers to assessthe most important components of well-being in general populations of children. Thequestionnaire was not validated or piloted, but the Cronbach´s Alpha analysis showed highinternal consistencies for the psychological well-being score (Cronbach’s Alpha 0.91), thephysical well-being score (Cronbach’s Alpha 0.83) and the social well-being score(Cronbach’s Alpha 0.76). The questionnaire had three parts: 1) psychological well-being, 2)physical well-being and 3) social well-being. Altogether 19 items were used to inquire aboutpsychological well-being (i.e., timidity, tearfulness, insecurity, anxiety, frustration,depression, restlessness, squeamishness or anger, aggressiveness, difficulties inconcentration, problems in concentration with homework, difficulties with homework,unwillingness go to school, troublemaking in class, discouragement, feeling of inferiority,forgetting things, sleeping difficulties, difficulties in reaching the age-appropriate level indoing things). Physical well-being was inquired with 12 items (i.e., problems with thefollowing activities: sitting, standing, walking, running, lifting or carrying things, eating ordrinking, washing, dressing up, performing housework as well as experiences of physicalpain, physical tiredness, difficulties in reaching the age-appropriate level in doing things).Social well-being was inquired with 6 items, (i.e., difficulties getting along with otherchildren, being bullied, arguing with other children, bullying other children, lack of interestin hobbies, difficulties in reaching the age-appropriate level in doing things). Each item wasrated on a 5-point scale (0=not at all, 1=once or twice in three months, 2=sometimes, 3=often,4= every day or almost every day). The total well-being scores from the questionnaire indicatethe status of physical well-being (range of possible score 0-48), psychological well-being(range of possible score 0-76) and social well-being (range of possible score 0-24).
5.1.6 Physical activity and inactivityThe assessments of the physical activity and sedentary activities were recorded during ausual week – on five week days and two weekend days (Väistö et al. 2014). Parents wereasked for information on regular physical activity, unstructured activity, physical education,physical activity at school and while commuting to and from school and during recess by thePANIC Physical Activity Questionnaire. The total amount of physical activity was calculatedas minutes per day. Habitual sedentary activity was also assessed by the same questionnaire.The amount of total sedentary activity was calculated by summing the time spent on eachsedentary activity type and was expressed as minutes per day weighted by the number ofweekdays and weekend days. Media use was calculated by summing up watching televisionand videos, using a computer, playing video games, using a mobile phone and playingmobile games and reported as minutes per day. The questionnaire was validated byActiheart monitoring (Väistö et al. 2014).
5.1.7 Dietary assessmentsFood consumption and nutrient intake were assessed by food records administered by theparents on four predefined consecutive days, as described previously (Eloranta et al. 2012).The food records were reviewed by a clinical nutritionist and analyzed using The Micro

33
Nutrica® dietary analysis software, Version 2.5 (The Social Insurance Institution of Finland).The Dietary Approach to Stop Hypertension (DASH) Score was used as an indicator of ahealthy diet and calculated as described previously (Fung et al. 2008). The DASH is acommonly used dietary quality index, which was originally developed for treatment ofhypertension in adults, but is also commonly used in children (Moore et al. 2005). In brief,the intake of seven food and nutrient groups, including fruit and fruit juices, vegetables,high-fiber ( 5%) grain products, low-fat (<1%) milk and sour milk products, red meat andsausage, sugar-sweetened beverages and sodium, were categorized into quintiles and scoredfrom 1 to 5. The highest quintile achieved the maximum score of 5 and the lowest quintileachieved the minimum score of 1. Reverse scoring was applied for red meat and sausages,sugar-sweetened beverages and sodium. The resulting 7 component scores were summed tocreate the overall DASH Score. A higher score indicates a higher dietary quality.
5.1.8 Socioeconomic background and characteristics of the parentsThe characteristics of the parents were reported with a structured questionnaire from bothmother and father. Parental socioeconomic status was assessed by the highest educationallevel in the family. Parents selected the appropriate level from three education categories:vocational, polytechnic and university. The total annual income of the households wasencoded into three categories (<€30,000/year, €30,001-€60,000/year and >€60,000/year).Possible unemployment, daily smoking and alcohol consumption (portions/week) werereported.
5.2 RELIABILITY OF THE MEASURES
The inter-examiner reliability for assessing the facial convexity (yes or no), mandibularretrusion (yes or no) and vertical proportions of the face (increased lower facial height yes orno) was measured using Cohen´s Kappa coefficients by comparing the assessments of threeexperienced orthodontists (Landis and Koch 1977). The assessments were performed withsixty randomly selected facial photographs of the studied children (Study I and IV). The intra-examiner reliability of the measures of the angle of convexity and the vertical proportions ofthe face were investigated by comparing the first and second assessment, two weeks apart,of the reference orthodontist (T.I.) using intra-class correlation coefficient (ICC) and its 95%confidence interval (CI) (Study II).
5.3 STATISTICAL METHODS
Statistical analyses were performed using the SPSS statistical software for Windows versions17.0-21.0. All associations and differences in averages were considered statistically significantif the P-value was <0.05. Chi-square or Fisher’s Exact test and Student’s t-test were used to compare the differencesin the prevalence of dental malocclusions and other craniofacial abnormalities, theprevalence of overweight or obesity and the means of BMI z-score and body fat percentagebetween children with and without SDB and between boys and girls (Study I and IV). Chi-square statistics were also used to analyze differences in the prevalence of having asthma or

34
SDB, differences in parental education, level of income, and smoking and employment statusbetween genders and low and normal psychological well-being groups (Study III). Student’st-test or Mann-Whitney U-test (depending on the normality of the variable distribution) wereused to analyze the differences in continuous variables, i.e., body fat percentage,cardiorespiratory fitness, duration of daily media use, duration of daily sedentary andphysical activities, sleep duration, daily supply of energy, the scores of physical,psychological and social well-being between genders as well as between low and normalpsychological well-being (Study III). Multivariate logistic regression analysis was used toinvestigate the associations of craniofacial abnormalities, dental malocclusions and body fatpercentage with the risk of having SDB (Study I and IV). The associations between the mostdeteriorated psychological well-being and parental education, parental daily smoking, SDB,media use and cardiorespiratory fitness were also estimated by logistic regression model(Study III). All independent variables as well as age and sex were entered stepwise into theregression models. Pearson correlation coefficients were calculated between the scores ofphysical well-being, psychological well-being and social well-being (Study III). The changein dental malocclusions and other craniofacial anomalies during the 2.2-year follow-up wasanalyzed by McNemar test (Study IV).

35
6 Results
6.1 BASIC CHARACTERISTICS
The characteristics of the children at the baseline and after 2.2-year follow-up are presentedin Table 3. At the baseline, 15.6% of the girls and 11.4% of the boys had either overweight(11.4% and 6.7%, respectively) or obesity (4.2% and 4.7%, respectively) and after follow-up15.3% of the girls and 18.8% of the boys had either overweight (12.5% and 15.2%,respectively) or obesity (2.8% and 3.6%, respectively). However, at both examinations thebody fat percent was higher among girls. The most common malocclusions at the baselineand after follow-up were dental crowding (51.7% and 42.8%, respectively), distal molarocclusion (29.5% and 25.4%, respectively) and mandibular retrusion (28.4% and 34.1%,respectively). The proportion of children with decreased palatal width was 11.6% at thebaseline and 10.9% after follow-up, while 14.9% had cross bite at the baseline and 8.7% afterfollow-up. Facial convexity at the baseline and increased lower facial height after follow-upwere more frequent among boys. Defined by the highest educational background of the family member, 18.7% of the familieshad a vocational school degree or less, 45.4% had a polytechnic degree and 35.9% a universitydegree. Annual household income was €30,000 in 18.5% of the families, €30,001-€60,000 in44.0% of the families and >€60,000 in 37.5% of the families.

36
Tabl
e 3.
Char
acte
rist
ics
of t
he c
hild
ren
at t
he b
asel
ine
and
afte
r 2.
2-ye
ar fol
low
-up
At
ba s
elin
eA
fter
2.2
-yea
r fo
llow
-up
All
child
ren
(n=
49
1)n
(%)
Gir
ls(n
=2
36)
n (%
)
Boy
s(n
=2
55)
n (%
)
pA
ll ch
ildre
n(n
=4
14)
n (%
)
Gir
ls(n
=2
02)
n (%
)
Boy
s(n
=2
12)
n (%
)
p
Ag e
, ye
ars,
mea
n (
SD
)
BM
I,m
ean
(SD
)
BM
I-SD
S,
Finn
ish
refe
renc
e va
lues
,
mea
n (
SD)
Bod
y fa
t pe
rcen
tage
,m
ean
(SD
)
Sle
ep d
isor
dere
d br
eath
ing
(SD
B)
7.6
(0.4
)
16.2
(2.
2)
0.05
(1.
1)
19.9
(8.
3)
46 (
9.9)
7.6
(0.4
)
16.2
(2.
2)
-0.0
1 (1
.0)
22.5
(7.
8)
17 (
7.6)
7.7
(0.4
)
16.2
(2.
1)
0.10
(1.
1)
17.4
(8.
0)
29 (
12.0
)
0.24
7
0.98
4
0.26
5
<0.
001
0.10
5
10.1
(0.
4)
17.2
(2.
7)
-0.1
3 (1
.1)
23.4
(9.
3)
38 (
11.6
)
10.1
(0.
4)
17.1
(2.
6)
-0.1
5 (1
.0)
25.3
(8.
5)
15 (
9.3)
10.1
(0.
5)
17.4
(2.
8)
-0.1
1 (1
.1)
21.5
(9.
6)
23 (
13.7
)
0.24
2
0.16
4
0.69
4
<0.
001
0.11
8
Dis
tal m
olar
occ
lusi
on
Cro
ss b
ite
Ope
n bi
te
Cro
wdi
ng
Sci
ssor
s bi
te
Con
vex
faci
al p
rofil
e
Incr
ease
d lo
wer
fac
ial h
eigh
t
Man
dibu
lar
retr
usio
n
Dec
reas
ed p
alat
al w
idth
Tons
illar
hyp
ertr
ophy
Ver
tical
ly r
estr
icte
d th
roat
Thic
k ne
ck
Adi
pose
tis
sue
unde
r th
e ch
in
Mou
th b
reat
hing
Ort
hodo
ntic
tre
atm
ent
145
(29.
5)
73 (
14.9
)
14 (
2.9)
254
(51.
7)
4 (0
.8)
159
(32.
4)
103
(21.
0)
139
(28.
4)
58 (
11.6
)
44 (
9.0)
211
(43.
3)
71 (
14.5
)
155
(32.
3)
47 (
9.6)
33 (
6.7)
77 (
32.6
)
33 (
14.0
)
5 (2
.1)
124
(52.
8)
1 (0
.4)
66 (
28.1
)
44 (
18.7
)
58 (
24.7
)
31 (
13.2
)
22 (
9.4)
100
(42.
6)
35(1
4.9)
72 (
31.3
)
19 (
8.1)
17 (
7.2)
68 (
26.7
)
40 (
15.7
)
9 (3
.5)
130
(51.
2)
3 (1
.2)
93 (
36.6
)
59 (
23.2
)
81 (
31.9
)
27 (
10.3
)
22 (
8.8)
111
(44.
0)
36 (
14.2
)
83 (
33.2
)
28 (
11.0
)
16 (
6.3)
0.14
8
0.59
6
0.34
4
0.72
6
0.62
5
0.04
4
0.22
2
0.07
7
0.31
6
0.81
9
0.82
1
0.73
9
0.65
7
0.27
0
0.68
1
105
(25.
4)
36 (
8.7)
5 (1
.2)
177
(42.
8)
11 (
2.7)
154
(37.
3)
94 (
22.8
)
141
(34.
1)
45 (
10.9
)
35 (
8.5)
129
(31.
4)
9 (2
.2)
71 (
17.4
)
23 (
5.7)
79 (
19.5
)
60 (
29.7
)
17 (
8.4)
2 (1
.0)
85 (
42.1
)
3 (1
.5)
72 (
35.8
)
35 (
17.4
)
61 (
30.3
)
22 (
10.9
)
19 (
9.5)
63 (
31.5
)
4 (2
.0)
33 (
16.6
)
8 (4
.1)
44 (
22.4
)
45 (
21.3
)
19 (
9.0)
3 (1
.4)
92 (
43.4
)
8 (3
.8)
82 (
38.7
)
59 (
27.8
)
80 (
37.7
)
23 (
10.8
)
16 (
7.6)
66 (
31.3
)
5 (2
.4)
38 (
18.2
)
15 (
7.2)
35 (
16.7
)
0.05
1
0.84
4
0.52
3
0.78
7
0.12
6
0.54
8
0.01
2
0.11
4
0.97
5
0.48
6
0.96
2
0.53
9
0.67
0
0.18
7
0.14
8

37
Table 4 shows the questions and the distribution of parents´ answers in sleepquestionnaire, based on which the children were defined as having SDB, both at thebaseline and after follow-up. The most frequent answers were “usually breathingthrough the mouth” and “snoring quite loudly”. Observed apneas were few innumber.
Table 4. Prevalence of single signs indicating SDB in the sleep questionnaire filled out by theparents
Childrenexamined at
baseline(n=466)
n %
Childrenexamined at
2.2-year follow-up (n=329)
n %Does your child breathe through the mouth at night? never rarely sometimesusually
always or almost always
95 (20.4)199 (42.7)134 (28.8)
29 (6.2)9 (1.9)
71 (21.6)137 (41.6)95 (28.9)21 (6.4)5 ( 1.5)
Have you noticed any pauses in your child’s breathingpattern during sleep? no rarelysometimes
usually always or almost always
443 (95.1)14 (3.0)6 (1.3)3 (0.6)0 (0.0)
320 (97.3)3 (0.9)6 (1.8)0 (0.0)0 (0.0)
How do you describe your child’s snoring best? no snoring snores rarelysnores in certain positions
snores most of the sleeping time snores frequently
253 (54.3)164 (35.1)
41 (8.8)9 (1.9)0 (0.0)
179 (54.4)126 (38.3)
20 (6.1)3 (0.9)1 (0.3)
How loudly does your child snore? no snoring lowquite loudly
loudly extreme loudly
241 (52.6)194 (42.4)
19 (4.1)3 (0.7)1 (0.2)
180 (54.7)135 (41.0)
13 (4.0)0 (0.0)1 (0.3)
Alternatives in italics included as having SDB

38
At the baseline, 9.9% (n=46) of the children had SDB, and there was no statisticallysignificant difference in the prevalence between the genders. Of the children, 41 (8.8%)snored in certain positions, 38 (8.2%) had nocturnal mouth breathing, 23 (5.0%) snoredloudly, 9 (1.9%) snored frequently and 3 (0.6%) had frequent apneas. After follow-up,11.6% (n=38) had SDB, with no statistically significant difference between genders.Compared with the SDB prevalence of the same children at the age of 7, after follow-up in 5.2% (n=17) SDB persisted, in 6.4% (n=21) new cases appeared and in 4.8% (n=16)previous SDB disappeared (Figure 6).
Figure 6. Changes (%) in SDB from 6-8 to 9-11 years of age
no SDB84 %
appeared6 %
unchanged5 %
disappeared5 %

39
The changes in the dentofacial and pharyngeal morphology, mouth breathing andorthodontic treatment during the follow-up time are shown in the Table 5. In parallelwith an increase in the number of children with previous or ongoing orthodontictreatment, many dental malocclusions have been corrected. Only the prevalence ofmandibular retrusion increased during follow-up time.
Table 5. Dentofacial and pharyngeal abnormalities in children at the age of 7 years and at the age of10 years, longitudinally
At the age of 6-8
years
n (%)
At the age of 9-11
years
n (%)
pa
Distal molar occlusion
Cross bite
Open bite
Crowding
Scissors bite
Convex facial profile
Increased lower facial height
Mandibular retrusion
Decreased palatal width
Tonsillar hypertrophy
Vertically restricted throatb
Thick neck
Adipose tissue under the chin
Mouth breathing
Orthodontic treatment
117 (29.0)
55 (13.6)
13 (3.2)
207 (51.4)
4 (1.0)
132 (32.8)
88 (21.9)
113 (28.1)
48 (12.0)
40 (10.1)
175 (43.9)
57 (14.3)
121 (31.1)
33 (8.2)
28 (6.9)
99 (24.5)
35 (8.6)
5 (1.2)
171 (42.4)
11 (2.7)
149 (37.1)
91 (22.6)
138 (34.3)
45 (11.2)
33 (8.3)
123 (30.8)
9 (2.3)
66 (17.0)
23 (5.7)
79 (19.5)
0.033
0.013
0.039
0.001
0.118
0.060
0.830
0.008
0.771
0.324
<0.001
<0.001
<0.001
0.143
<0.001
aBy McNemar TestbDefined as Mallampati et.al. Class III or IV
6.2 RISK FACTORS FOR SLEEP DISORDERED BREATHING AMONGCHILDREN AGED 6-8 AND 9-11- YEARS (STUDY I, IV)
Characteristics of the children with and without SDB at the baseline and after 2.2-yearfollow-up are presented in Table 6. Children 6-8 years of age with SDB were morelikely to have cross bite, convex facial profile, increased lower facial height,mandibular retrusion, hypertrophic tonsils and mouth breathing than those withoutit. After follow-up, at the age of 9-11 years, children with SDB were more likely tohave convex facial profile, mandibular retrusion and mouth breathing. There were no

40
statistically significant differences in the prevalence of body fat percentage or othercharacteristics between the children with SDB and those without it.
Table 6. Characteristics of the children with SDB and those without it at the baseline andat 2.2-year follow-up
Children examined at baseline(n=466)
Children examined at 2.2-yearfollow-up (n=329)
ChildrenwithSDB
(n=46)
Childrenwithout
SDB(n=420)
p-value
Childrenwith SDB
(n=38)
Childrenwithout
SDB(n=291)
p-value
Distal molar occlusion
Cross bite
Open bite
Crowding
Scissors bite
Convex facial profile
Increased lower facial height
Mandibular retrusion
Maxillary retrusion
Decreased palatal width
Tonsillar hypertrophy
Vertically restricted throata
Mouth breathing
Orthodontic treatment
Thick neck
15 (32.6)
13 (28.3)
3 (6.5)
23 (50.0)
1 (2.0)
24 (54.5)
16 (34.8)
21 (45.7)
0 (0)
8 (17.4)
12 (26.1)
22 (47.8)
13 (28.3)
6 (13.0)
5 (10.9)
124 (29.5)
54 (12.9)
10 (2.4)
217 (51.9)
3 (0.7)
131 (31.3)
85 (20.3)
116 (27.6)
7 (1.7)
45 (10.8)
32 (7.7)
178 (42.7)
31 (7.4)
26 (6.2)
62 (14.8)
0.664
0.005
0.097
0.905
0.308
0.004
0.024
0.012
1.000
0.182
<0.001
0.504
<0.001
0.081
0.468
13 (34.2)
5 (13.2)
0 (0)
13 (34.2)
3 (7.9)
20 (52.6)
12 (31.6)
20 (52.6)
3 (7.9)
8 (21.1)
6 (15.8)
10 (26.3)
7 (18.4)
10 (26.3)
1 (2.6)
68 (23.4)
24 (8.2)
3 (1.0)
127 (43.6)
8 (2.7)
104 (35.7)
58 (19.9)
93 (32.0)
6 (2.1)
31 (10.7)
19 (6.5)
90 (30.9)
12 (4.1)
52 (17.9)
4 (1.4)
0.145
0.356
1.000
0.269
0.122
0.043
0.099
0.012
0.073
0.103
0.053
0.561
0.003
0.211
0.461
Adipose tissue under the chin 16 (34.8) 133 (32.4) 0.748 11 (28.9) 47 (16.3) 0.056
Body fat percentageb 19.7 (8.8) 20.0 (8.3) 0.829 25.5 (10.1) 23.1 (9.1) 0.135b
Data are numbers (percentages) and p-values are from Chi-Square Test or from Fisher’s ExactTestaDefined as Mallampati et al. Class III or IVbData are means (standard deviations) and p-values are from Student’s T-test
The risk factors for SDB at the baseline and after 2.2-year follow-up are presented inTable 7. Children aged 6-8 years with SDB were more likely to have tonsillarhypertrophy, cross bite and convex facial profile than those without it. Children withtonsillar hypertrophy had a 3.7-fold higher risk of suffering SDB than those withnormal size tonsils after adjustment for age, sex and body fat percentage. Furthermore,children with cross bite had a 3.3-fold higher risk of having SDB than those without

41
cross bite, while children with a convex facial profile had a 2.6-fold higher risk ofhaving SDB than those with a normal facial profile. Other craniofacial abnormalitiesor body fat percentage were not associated with the risk of having SDB among thisage group. Children 9-11 years of age with SDB were more likely to have mouthbreathing, adipose tissue under the chin and previous or ongoing orthodontictreatment. Children with mouth breathing had a 5.4-fold higher risk of suffering SDBthan children with nasal breathing.
Table 7. The risk factors for SDB at the age of 6-8 years and at the age of 9-11 years
Relative risk 95% confidence
interval
p-value
Risk factors at the age of 6-8
Tonsillar hypertrophy
Cross bite
Convex facial profile
Risk factors at the age of 9-11
Adipose tissue under the chin
Mouth breathing
3.7
3.3
2.6
2.3
5.4
1.7-8.2
1.5-7.1
1.4-5.1
1.10-5.06
1.93-15.30
0.001
0.003
0.004
0.029
0.001
Data are from stepwise logistic regression models, the effect of gender was considered in eachstep.Only statistically significant determinants are given
6.3 PREDICTORS OF SLEEP DISORDERED BREATHING INCHILDREN (STUDY IV)
Risk factors and prediction of SDBMale gender, distal molar occlusion, mouth breathing and increased body fatpercentage at the baseline were associated with increased risk of having SDB at the2.2-year follow-up (Table 8). Mouth breathing was the strongest baseline predictor ofSDB at the 2.2-year follow-up. Children with mouth breathing at baseline had a 4.4-fold higher risk of SDB at the 2.2-year follow-up than those without it. It is noteworthythat the intervention setting of the PANIC study did not have an impact on the results(data not shown).

42
Table 8. Baseline predictors for having SDB at 2.2-year follow-up among all 329 children
Relative risk 95% confidence
interval
p-value
Male gender 2.2 1.0-4.6 0.042
Distal molar occlusion 2.2 1.1-4.6 0.032
Mouth breathing 4.4 1.7-11.4 0.002
1 SD increase in body fat percentage 1.5 1.1-2.1 0.015
Data are from stepwise logistic regression models, the effect of gender was considered in eachstep.Only statistically significant determinants are given.
Mandibular retrusion, adipose tissue under the chin and a history of orthodontictreatment at baseline were associated with increased risk of developing SDB duringthe 2.2-year follow-up (Table 9). Further, a vertically restricted throat seemed to be aprotective factor against SDB and vice versa, a vertically large or normal throatincreased the risk for SDB. However, there was a clear tendency for the children withvertically large or normal throat to have hypertrophied tonsils. A history oforthodontic treatment was the strongest baseline predictor of developing SDB duringthe 2.2-year follow-up. Children who had a history of orthodontic treatment atbaseline had a 5.0-fold higher risk of SDB than those without it.
Table 9. Baseline predictors for incident SDB at 2.2-year follow-up among 296 childrenwho had no SDB at baseline
Relative risk 95% confidence
interval
p-
value
Mandibular retrusion 3.4 1.3-8.9 0.012
Vertically restricted throata 0.2 0.1-0.7 0.011
Adipose tissue under the chin 2.8 1.1-7.2 0.034
Orthodontic treatment 5.0 1.3-18.4 0.016
aDefined as Mallampati et.al. Class III or IVData are from stepwise logistic regression models, the effect of gender was considered in eachstep.Only statistically significant determinants are given

43
6.4 RECOGNIZING CONVEXITY AND VERTICAL PROPORTIONS OFTHE LATERAL FACIAL PROFILE (STUDY II)
At the baseline the prevalence of SDB in children with the most convex profilesexpressed with the lowest quintile of the angle G`- Sn - Pg` ( 164.2°) was almosttwofold (14.5%) compared with those with a normal profile (8.1%) (p = 0.084). Of allthe profiles clinically classified as convex by the reference orthodontist (T.I.), 67.1%were the most convex profiles expressed with the lowest quintile of the angle G`- Sn -Pg`. Of the convex profiles assessed visually with a photograph by the same examiner,64.3% were in the lowest quintile. The intra-examiner reliability of measures of theangle of convexity (G`- Sn - Pg`) and further, the vertical proportions of the face (Sn`-Me`/N`-Me`) were investigated by comparing the first and second assessment, twoweeks apart, of the reference orthodontist using intra-class correlation coefficient(ICC) and its 95% confidence interval (CI). The ICC (95% CI) between the twomeasurements was 0.980 (0.951-0.992) for the angle of convexity and 0.829 (0.671-0.915) for the vertical proportion of the face. The Kappa values for the measures of facial profile with the photographs betweenthe reference orthodontist and the other health care professionals varied between0.000 and 0.579 and the proportion of agreement varied between 55.6% and 78.8%(Figure 7). The highest Kappa value (0.579) and the highest proportion of agreement(78.8%) were observed between the two orthodontists. The Kappa value for therepeated measurements of the facial profile of the reference orthodontist was 0.920and the proportion of agreement was 93.3%. The Kappa values of the measurementsof the first 200 photos and the last 200 photos did not differ. In order to test the inter-examiner reliability for the measures of facial profile withthe photographs between three experienced orthodontists, the Kappa values variedfrom 0.500 to 0.899 (good to excellent agreement) for facial convexity, from 0.167 to0.533 (poor to good agreement) for mandibular retrusion and from 0.558 to 0.896 (goodto excellent agreement) for vertical proportions of the face.

44
Figure 7. The number of evidently convex profiles identified by eight observers fromfacial photographs (total n=382). On the top of the bars: inter-examiner kappa-valuesand agreement percentages with reference observer
6.5 CORRELATES OF PSYCHOLOGICAL WELL-BEING AMONG GIRLSAND BOYS 6-8 YEARS OF AGE – THE ROLE OF SLEEPDISORDERED BREATHING (STUDY III)
At the age of 6-8 years, the girls had a higher body fat percentage and total sedentarybehavior, a better diet quality assessed by the DASH score, higher psychological andsocial well-being scores and lower levels of cardiorespiratory fitness, total physicalactivity and screen-based sedentary behavior than the boys (Table 10 and 11).

45
Table 10. Classified characteristics of the children
Allchildren(n=412)
n %
Girls(n=205)
n %
Boys(n=207)
n %
p-valuea
fordifference
Asthma
Sleep disordered breathing
Parental education Vocational Polytechnic University
Parental income€30,000
€30,001-€60,000 >€60,000
Parental daily smoking
Mother’s unemployment
Father’s unemployment
Mother’s alcohol consumption, portions/week
Father’s alcohol consumption, portions/week
36 (8.8)
41 (10.0)
77 (18.7)187 (45.4)148 (35.9)
75 (18.5)178 (44.0)152 (37.5)
98 (23.8)
24 (5.8)
26 (6.8)
2.6 (3.1)
6.4 (6.6)
16 (8.0)
16 (7.8)
36 (17.6)104 (50.7)65 (31.7)
41 (20.2)95 (46.8)67 (33.0)
42 (20.5)
15 (7.3)
11 (5.9)
2.4 (2.8)
6.2 (7.0)
20 (9.7)
25 (12.1)
41 (19.8)83 (40.1)83 (40.1)
34 (16.8)83 (41.1)85 (42.1)
56 (27.1)
9 (4.4)
15 (7.8)
2.8 (3.4)
6.6 (6.1)
0.602
0.147
0.088
0.166
0.118
0.215
0.544
0.339
0.481
afrom the Fisher’s Exact Test or Chi-square statistics

46
Table 11. Metric characteristics of children
Allchildren(n=412)
mean(SD)
Girls(n=205)
mean(SD)
Boys(n=207)
mean(SD)
p-valuea
fordifference
Age, years
Body fat percentage
Cardiorespiratory fitness, w/kg lean mass
Total sedentary behavior, min/day
Total physical activity, min/day
Screen-based sedentary behavior, min/day
Sleep durationb, h/night
DASH score
Psychological well-beingc
Physical well-beingd
Social well-beinge
7.6 (0.3)
19.9 (8.1)
3.7 (0.5)
215 (106)
111 (41)
102 (52)
9.7 (0.5)
21.0 (4.4)
10.1 (9.0)
2.8 (3.7)
2.2 (2.6)
7.6 (0.4)
22.6 (7.6)
3.5 (0.5)
224 (107)
103 (38)
90 (47)
9.7 (0.5)
21.6 (4.2)
8.9 (8.2)
2.4 (3.0)
1.7 (2.1)
7.7 (0.4)
17.2 (7.7)
3.8 (0.5)
206 (105)
119 (43)
114 (55)
9.6 (0.5)
20.3 (4.5)
11.4 (9.5)
3.1 (4.2)
2.6 (2.9)
0.364
<0.001
<0.001
0.048
<0.001
<0.001
0.631
0.004
0.006
0.196
<0.001
afrom Student’s T-test or Mann-Whitney U TestbUsing combined heart rate and movement sensorcScore ranging between 0 and 76 according to 19 itemsdScore ranging between 0 and 48 according to 12 itemseScore ranging between 0 and 24 according to 6 items

47
SDB was more common in boys with low psychological well-being than in boys withnormal psychological well-being. Cardiorespiratory fitness was lower in girls withlow psychological well-being than in girls with normal psychological well-being. Thelevels of screen-based sedentary behavior were higher and daily parental smokingwas more common in boys with low psychological well-being than in boys withnormal psychological well-being (Table 12 and 13).
Table 12. Classified characteristics of girls and boys with low and normal psychologicalwell-being (PSWB)
Girls (n=205) Boys (n=207)
Low PSWB n %
NormalPSWBn %
p-valuea
LowPSWBn %
NormalPSWBn %
p-valuea
Asthma
Sleep disordered breathing
4 (6.2)
3 (4.5)
12 (8.8)
13 (9.4)
0.513
0.231
6 (7.6)
17 (21.3)
14 (11.0)
8 (6.3)
0.419
0.001
Parental education Vocational Polytechnic or university
16 (24.2) 50 (75.8)
20 (14.4)119 (85.6)
0.08320 (25.0)60 (75.0)
21 (16.5)106 (83.5)
0.137
Parental income €30,000 >€30,000
14 (21.5)51 (78.5)
27 (19.6)111 (80.4)
0.74416 (20.5)62 (79.5)
18 (14.5)106 (85.5)
0.267
Parental daily smoking 13 (19.7) 29 (20.9) 0.847 28 (35.0) 28 (22.0) 0.041
Mother’s unemployment
Father’s unemployment
5 (7.6)
5 (8.3)
10 (7.2)
6 (4.7)
0.922
0.321
5 (6.3)
6 (8.6)
4 (3.2)
9 (7.4)
0.293
0.767
Mother’s alcoholconsumption, portions/week
Father’s alcoholconsumption, portions/week
2.3 (2.8)
5.8 (5.6)
2.5 (2.8)
6.5 (7.6)
0.609
0.620
3.2 (3.8)
7.0 (6.7)
2.6 (3.1)
6.3 (5.7)
0.331
0.606
afrom the Fisher’s Exact Test or Chi-square statistics

48
Table 13. Metric characteristics of girls and boys with low and normal psychological well-being (PSWB)
Girls (n=205) Boys (n=207)
LowPSWB
mean(SD)
NormalPSWB
mean(SD)
p-valuea
LowPSWB
mean(SD)
NormalPSWB
mean(SD)
p-valuea
Body fat percentage 23.1 (7.1) 22.4 (7.9) 0.322 18.1 (8.7) 16.6 (7.0) 0.470
Cardiorespiratory fitness, w/kglean mass 3.4 (0.4) 3.6 (0.5) 0.004 3.7 (0.5) 3.9 (0.5) 0.081
Total sedentary behavior,min/day 237 (117) 218 (102) 0.277 229 (123) 192 (89) 0.065
Total physical activity, min/day 100 (36) 104 (38) 0.471 114 (42) 122 (43) 0.173
Screen based sedentarybehavior, min/day 91 (45) 90 (49) 0.491 128 (62) 105 (47) 0.012
Sleep durationb, h/night 9.7 (0.5) 9.7 (0.5) 0.971 9.6 (0.6) 9.7 (0.5) 0.076
DASH score 21.7 (4.1) 21.6 (4.3) 0.913 20.2 (4.9) 20.4 (4.2) 0.810
afrom Mann-Whitney U Test or Student’s T-testbUsing combined heart rate and movement sensor
Boys with SDB were four times more likely to have increased risk of low psychologicalwell-being than boys without SDB (Table 14). Girls who were in the highest third ofcardiorespiratory fitness were less likely to have low psychological well-being thangirls in the lowest third. Boys with at least two hours of screen-based sedentarybehavior per day had two fold higher risk of low psychological well-being than boyswith lower levels of screen-based sedentary behavior. Moreover, boys whose parentssmoked daily had a higher risk of low psychological well-being than boys whoseparents did not smoke. Girls whose parents had lower education had a higher risk oflow psychological well-being than girls whose parents had higher education.

49
Table 14. Risk factors for having low psychological well-being in girls and boys
Girls (n=205) Boys (n=207 p-value forinteraction
withgenderORa (95% CI) p ORa (95% CI) p
Age, years 1.20 (0.51-2.83) .674 1.14 (0.49-2.63) .766 0.935
Screen-based sedentarybehavior <2h/day
2h/day1.00
0.66 (0.31-1.42) .2911.00
1.93 (1.04-3.57) .037
0.084
Cardiorespiratory fitness, w/kglean mass <3.48 3.48-3.88 >3.88
1.000.86 (0.43-1.71)0.26 (0.10-0.68)
.663
.006
1.000.66 (0.29-1.49)0.63 (0.29-1.39)
.311
.252
0.410
Sleep disordered breathing No Yes
1.000.32 (0.08-1.24) .099
1.004.24 (1.63-11.00) .003
0.013
Parental education Polytechnic or university Vocational
1.002.34 (1.05-5.25) .039
1.001.07 (0.48-2.36) .868
0.755
Parental daily smoking No Yes
1.000.69 (0.31-1.42) .354
1.002.10 (1.06-4.15) .034
0.105
aThe values are odds ratios (OR) and their 95% confidence intervals (CI) from logistic regressionmodels in which all variables were entered simultaneously.

50

51
7 Discussion
7.1 DENTOFACIAL AND PHARYNGEAL MORPHOLOGY WITH ANDRISK FOR SLEEP DISORDERED BREATHING
The present study shows that children with SDB represent different dentofacial andpharyngeal morphology compared with those with no SDB. Typical dentofacialfeatures of SDB children are cross bite, convexity of the facial profile, increased lowerfacial height and mandibular retrusion. The present study is in line with the previousstudies, such as a Finnish study showing 7-year-old children with SDB to have distalposition and posterior rotation of the mandible and increased lower facial height(Pirilä-Parkkinen et al. 2010), and with many other studies (Löfstrand-Tideström et al.1999, Marino et al. 2009). The results of a recent study show that cross bite and openbite associate with SDB (Carvalho et al. 2014). A systematic review and meta-analysissummarize a retrusive chin, steep mandibular plane, vertical direction of mandibulargrowth and a tendency toward Class II malocclusion to be the typical characteristicsof the SDB children (Flores-Mir et al. 2013). The most common malocclusions in both 6- to 8- and 9- to 11-year old children weredental crowding, distal molar occlusion and mandibular retrusion, showing quitetypical distribution of malocclusions among Finnish children (Eskeli 2015). Facialconvexity at the baseline and increased lower facial height after follow-up were morefrequent among boys. The results concerning gender difference among schoolchildren in the prevalence of malocclusions are contradictory (Myllärniemi 1970,Kerosuo et al. 1991, Thilander et al. 2001, Tak et al. 2013). The present study alsoshowed changes in the prevalence of dental malocclusions during the follow-up time,which goes in parallel with an increase in the number of children with previous orongoing orthodontic treatment. Furthermore, both 6- to 8 and 9- to 11-year-old children with SDB were more likelyto have tonsillar hypertrophy than those without it, the association being moresignificant in the younger age group. The result of the present study agrees with otherstudies showing that ATH significantly raises the risk for pediatric SDB (Arens et al.2003, Dayyat et al. 2007). The mass of the lymphoid tissue of the pharynx increasesfrom birth to twelve years, the volume being at maximum related to the skeletalstructures at the age of 5-6 years (Dayyat et al. 2007), and in line with this, SDB is mostcommon in pre-school and early school years (Corbo et al. 2001). Furthermore, thereis a transient prepubertal increase in nasal resistance, a phenomenon suggested toresult from the prepubertal hypertrophy of adenoid tissue or hormonal changescausing mucosal swelling of the nasal passage (Linder-Aronson and Leighton 1983),which further explicates the association of hypertrophied lymphatic tissue with SDB

52
in young school-aged children. However, there are studies to suggest that the importance of obesity as a risk forSDB increases along with age in parallel with ATH and other morphological riskfeatures decreasing in relevance (Kohler and Heuvel 2008). Furthermore, it issuggested that there are two different phenotypes of pediatric SDB; one characterizedby ATH with no obesity (type I) and the other by obesity in the presence of only minorATH (type II) (Dayyat et al. 2007). The present study showed that mouth breathing, often co-existing withlymphadenoid hypertrophy, at the age of 6–8 years was associated with increased riskof SDB after follow-up. Interestingly, children with a vertically large or normal throathad increased risk of SDB. The same children also tended to have hypertrophiedtonsils more often than those with vertically a restricted throat. This may indicate thatthose children had developed a lowered position of the tongue to improve theirbreathing, which is in line with the results of the classical study of Linder-Aronson(Linder-Aronson 1970). On the other hand, a study by Suri suggests that a verticallyrestricted throat significantly predicts a poor outcome of the treatment of SDB withATE which suggests that a delay in treating the hypertrophied adenoid and tonsilsmay promote abnormal craniofacial growth, leading to residual SDB (Suri et al. 2015).The inconsistent results concerning the association of pharyngeal morphology andSDB warrants future studies with a larger study group and PSG-testing fordetermining the sleep disorder to confirm the observations of the present study. This raises the old question of the chicken and the egg. All the aforementionedfactors concerning dentofacial and pharyngeal characteristics of a child with SDB maylead to an abnormal function, including oral breathing, which seems to alter oral andfacial muscular balance and is likely to affect skeletal and occlusal development andfurther, may increase the risk for SDB (Peltomäki 2007). It is noteworthy, that in thepresent study children with SDB represent the whole spectrum of the condition – fromthe mildest manifestation with primary snoring to actual breathing pause, i.e., apneaobserved by the parents. In fact, almost all of the SDB children in the present studywere snorers and/or nocturnal mouth breathers. As both malocclusions and the wholespectrum of SDB are quite prevalent, it is not only to the advantage of individualswith a burden of symptoms and consequences, but also to the advantage of a societyin terms of economics to recognize and understand the close relation between thesetwo different conditions.
7.2 PREDICTION OF SDB
The results of the study indicate that typical features predicting SDB could easily berecognized in health centers by dental professionals within normal oral examinations.Certain morphological and functional features at the age of 6-8 years may predictdeveloping SDB at the age of 9-11 years. Especially high body adiposity and mouth

53
breathing, as well as distal molar occlusion seemed to predispose to the developmentof SDB already in childhood. Furthermore, as in adults (Neelapu et al. 2016), malegender also increased the risk of SDB. Adipose tissue under the chin, mandibularretrusion, vertically normal/large throat and orthodontic treatment were associatedwith incident SDB during the follow-up. Body adiposity has been observed to be an important risk factor for developing SDBin children (Kohler and van den Heuvel 2008, Verhulst et al. 2008). A recent studyshowed that especially an increased amount of visceral fat was associated with severemanifestations of SDB in a population sample of children (Bixler et al. 2016). Inaccordance with the results of these studies, the present study showed that a highbody fat percentage at the age of 6-8 years was associated with a higher risk of havingSDB 2.2 years later, and furthermore, adipose tissue under the chin was associatedwith increased risk of developing SDB during 2.2-year follow-up. In children, theassociations of overweight and obesity with SDB may not be straightforward, and therelationship may be modified by other factors, such as age and craniofacialmorphology (Kohler and van den Heuvel 2008). It can be speculated, that thesignificance of the body adiposity for SDB increases in parallel with age, whichwarrants future studies concerning the PANIC children. The mechanism by which adiposity predisposes to SDB may be the mass loading ofthe upper airway and respiratory muscles (Ng et al. 2006) causing alterations to thestructure and function of these muscles, the reduction of chest wall compliance,changes in respiratory drive and the impairment of functional residual capacity, all ofwhich increase the risk of upper airway obstruction (Kohler and van den Heuvel2008). It is alarming that overweight and obesity are becoming more common inchildren and adolescents in many developed countries (Kipping et al. 2008). InFinland, 10% of children and 26% of adolescents have been found to be overweight(Vuorela et al. 2009). In fact, obese children have been observed to have an increasedrisk of persistent SDB even after ATE, which is the first-line treatment for pediatricSDB (Kohler and van den Heuvel 2008). Interestingly, a history of orthodontic treatment at baseline was associated withincreased risk of developing SDB during the follow-up. This most likely associatedwith the malocclusions and deviant craniofacial morphology that require orthodontictreatment. In line with previous studies the present study showed typical deviationsin dentofacial morphology associating with SDB. In Finland these deviations, such ascross bite, are often diagnosed and early orthodontic treatment initiated in the primaryschool years. However, the impact of different treatment modalities would requirefurther examination since basically, early orthodontic treatment is thought to preventSDB in adulthood by modifying the deviant craniofacial morphology in a morefavorable direction (Hanggi et al. 2008, Ashok et al. 2014).
The physical activity and nutrition intervention of the PANIC study did not haveany effect on the results of the present study, which was a predictable result. The studyshowed, that the obesity, which is a relevant target to healthy lifestyle intervention,was not a risk for SDB among young children. On the other hand, dentofacial and

54
pharyngeal risk factors of SDB cannot be supposed to be affected by the intervention.It is noteworthy that recent papers published within the PANIC study show that anindividualized and family-based lifestyle intervention increased physical activity,attenuated increase in sedentary behavior, enhanced diet quality and further, had abeneficial effect on plasma fatty acid composition in children (Viitasalo et al. 2016,Venäläinen et al. 2016). Further follow-up studies will show if the healthy lifestyleintervention will have an impact on the prevalence or symptoms of SDB in the comingyears. Although some risk features (i.e., retrusive mandible and facial convexity) may notbe unambiguously recognized, most of them are well-known parts of the normalprotocol of oral health professionals when executing regular oral examinations. Itwould be beneficial if children with typical features associated with SDB – the wholespectrum of it – could be recognized early in childhood so that they could becandidates for early intervention and treatment to prevent the progression of SDBover the coming years.
7.3 THE PSYCHOLOGICAL CONSEQUENCES OF SDB
The present study shows that at the age of 6-8 years SDB compromises psychologicalwell-being of boys. There are many recent studies to show that poor behavior, mooddisorder symptoms, emotion instability, impaired psychological functions andreduced quality of life associates with SDB (Beebe 2006, Aronen et al. 2009, Jackmanet al. 2012). The determinants of the quality of life can be affected in both children andtheir families (Jackman et al. 2012) and further predict behavioral and emotionalproblems in adolescence (Gozal 2001). Further, it has been demonstrated thatregardless of the severity of SDB or body adiposity, children with SDB have decreasedquality of life and well-being compared to children without SDB (Rosen et al. 2002,Crabtree et al. 2004). Taken together, these observations underline the importance ofrecognizing the psychological aspects of SDB. The exact mechanisms behind the association of psychological aspects and SDB areunclear. The mechanism may depend on the severity of the condition: milder forms(snoring) with sleep fragmentation and severe forms (OSA) with hypoxia (O´Brien etal. 2004). It is possible, that any dislocation of sleep in a child leads to modification ofneurochemical substrates at the prefrontal cortex level (Beebe and Gozal 2002),resulting in psychological effects. Milder and at the same time more commonmanifestations of SDB may even have the strongest effects on psychological functionsin pre-school children (Jackman et al. 2012). Further, any sleep disturbance, includingSDB may simply cause fatigue and stress in both children and parents, and thisinterferes with multiple aspects of a child´s life, including the mental context. It is unclear, why the results of the present study on the psychological contextconcern only boys. In general, some questionnaire-based studies show boys to havemore SDB compared with girls (Ersu et al. 2004, Gill et al. 2012). The present study

55
showed opposite findings, agreeing with other questionnaire-based studies showingno gender difference in the prevalence of SDB (Liukkonen et al. 2008, Anuntaseree etal. 2014). However, the sample sizes in most studies, including the present study,studying SDB in children have been too modest to examine the gender differences inchildren in more detail. It is possible, that boys are more sensitive to sleepfragmentation. The reason why boys with SDB are doing worse than girls with SDB ismost likely multi-factorial; physiologic or later puberty-related hormonal changesmay potentiate the effect of gender on SDB prevalence. The discrepancy of resultswarrants more future research concerning the gender differences in SDB. The psychological consequences of SDB are likely to manifest themselves in school(Smith et al. 2016), fortunately the phenomenon being at least partly reversible. Schoolchildren with academic scores ranked in the lowest 10th percentile with SDB seemedto get significantly improved grades after ATE compared with those not operated(Gozal 1998). However, there is also a risk for a “learning debt”, since a large surveystudy showed that school children with loud and frequent snoring are likely to havelow grades in school several years after the snoring has been treated (Gozal and Pope2001), the fact that further calls for early intervention to treat SDB. More future studiesare warranted to study the impact of different treatment modalities, such as ATE andorthodontic treatment, to the association of childhood SDB and school performance. The present study suggests observation and recognition of the psychological aspectsof childhood SDB. At home, it is important to be conscious of the fact that SDB is atreatable medical condition, which may largely compromise the well-being of thechild. In schools, among both teachers and school nurses, knowledge of thepsychological and cognitional aspects of this relatively common condition would havelong-lasting effects for the lives of the children. It is possible, that there is a treatabledisease behind poor school performance.
7.4 STRENGTHS AND LIMITATIONS
The strength of the study is the relative large population sample of children aged 6-8and 9-11 years. The results are based on comprehensive and valid assessments ofdental malocclusions and other craniofacial abnormalities, body composition,cardiorespiratory fitness, physical activity, sedentary behavior and parentalsocioeconomic status. However, there are some limitations in the study. Because of the large population-based study sample it was not possible to conductnocturnal polysomnography, which is the golden standard for diagnosing breathing-based sleeping problems in both children and adults (Section on PediatricPulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome. AmericanAcademy of Pediatrics 2002). Instead, SDB was defined as apneas, frequent or loudsnoring or nocturnal mouth breathing observed by the parents and registered by aquestionnaire. The questions in the sleep questionnaire are based on an establishedFinnish questionnaire that has been used to screen for sleep disturbances and SDB

56
(Partinen and Gislason 1995), and modified in the present study for the parents to fillout on behalf of their children. The parents answered the questions concerning thechild’s quantity and quality of sleep and signs of SDB. It is possible, that because ofsleeping in different room that the children, some parents may have been unaware oftheir child´s sleeping pattern as well as mode of breathing, thus causing inaccuracy inreporting. The size of the adenoids was not examined. Reliable methods would have beennasofiberoscopy with local anesthesia or magnetic resonance imaging. However, ashypertrophy of adenoid and tonsils typically coexist and indicate the amount oflymphoid tissue in the pharynx, it may not be relevant to consider them as differentconditions. The shape of the palate was visually defined as wide, normal or narrow.The evaluation with digital study models after scanning the dentition and palatalvault would have given exact metrically measures of the palatal dimensions(Chalmers et al. 2015). Instead, the results are based on visual assessment of anexperienced orthodontist. The aforementioned limitations are caused by theepidemiological character of the present study and the burden of numerous othermedical examinations performed on the children participating in the PANIC study. The associations of certain dental malocclusions, such as scissors bite and open bite,with SDB could not be analyzed because of their low prevalence and thus, insufficientstatistical power. Further, mouth breathing was clinically identified using open lips asa hallmark, which may overestimate the proportion of mouth breathers. Habitualopen-lip posture does not always coexist with mouth breathing, which requiresobjective airway temperature or pressure recordings for a secure diagnosis(Leiberman et al. 1990). Furthermore, reliable assessment of retrusive mandibleseemed to be difficult even for experienced orthodontists in the group of 6- to 8-year-old children. However, the analysis of inter-examiner reliability was based on lateralfacial photographs. Unfortunately, it was not possible to perform a clinical analysis ofmeasurement reliability, which might have given better results. Further, at thebaseline the cross-sectional study design makes it difficult to draw conclusions aboutcausal relationships. The findings may not be directly generalized to all ethnic and agegroups, since almost all children were Caucasian and 6- to 11 years of age. At the time of initiating the PANIC study in 2007, there were no questionnairessuitable for investigating psychological, social and physical well-being in a populationsample of healthy children, as most of the questionnaires available were meant forpediatric patients. Therefore the PANIC researcher group developed a questionnairefor the purpose. An established questionnaire with piloting and validating wouldhave enhanced the generalizability of the presented findings more reliably. Anotherweakness of the questionnaire is that some of the 19 items do not specifically measurepsychological well-being but also reflect social well-being, as indicated by therelatively strong correlation between the psychological and social well-being scores.Moreover, the questionnaire was filled out by the parents. Finally, in general,questionnaires may overestimate the magnitude of the associations and genderdifferences in psychological research because the answers to the questions may reflect

57
the gender-specific attitudes of parents (Eisenberg et al. 1998).

58

59
8 Conclusions and future perspective
The results of this doctoral thesis indicate that children with SDB represent differentdentofacial and pharyngeal morphology compared with those without SDB. Typicalfeatures predicting SDB could be recognized in health centers by dental and otherhealth care professionals working with children. Furthermore, SDB affects thepsychological well-being in childhood. Noteworthy, the above-mentionedphenomena are seen among the whole study group with SDB – even though almostall of the cases in the present study represent milder forms of SDB.
The main findings and conclusions are summarized in respect to the aims of the thesisas follows:
1. Dentofacial and pharyngeal morphology of children with SDB differs fromthose without SDB. Typical features associating with SDB are convexity of thefacial profile, mandibular retrusion and increased lower facial height. Inaddition, tonsillar hypertrophy and dominant mouth breathing associate withSDB. If a child suffers from symptoms of SDB, his or her facial status, dentalocclusion and mode of breathing should be examined. On the other hand,children with risk features should be examined as regards to their sleepinghabits, snoring and pauses in breathing during sleep.
2. The study suggests that certain morphological and functional features, such asdeviant dentofacial and pharyngeal morphology, mouth breathing and bodyadiposity at the age of 6-8 years may predict SDB in the coming years.Furthermore, male gender predicts SDB in childhood. These findings are usefulin identifying children at increased risk for developing SDB.
3. Facial convexity, being an important determinant of pediatric SDB, is difficultto recognize. The fact that the sagittal characteristics are most reliablyrecognized by an orthodontist indicates that one would need to be trained andexperienced for the purpose and furthermore, need sufficient basic knowledgeof the growth and development of the face.
4. SDB associates with low psychological well-being in boys aged 6-8-year. Sinceclinicians make complex management decisions including invasive surgicalinterventions concerning the treatment of pediatric SDB, it is important also torecognize the psychological aspects of the condition. It is possible, that there isa treatable disease behind the poor school performance. The present study

60
indicates that there may be modifiable health-related correlates behindemotional and behavioral problems.
The present study suggests that children with current or developing SDB could becandidates for early intervention to prevent the progression of SDB later in life. In thefuture, more longitudinal population-based studies are warranted to confirm thepresent observations among children and further, to clarify the whole picture ofchildhood SDB. Studying pediatric populations provides an incomparableopportunity to recognize early determinants of SDB and its natural evolution. Earlyintervention with lifestyle counselling, surgery and orthodontic treatment may detectthe progression of childhood SDB to adulthood OSA. This can only happen throughbetter understanding and earlier recognition of the underlying mechanisms behindthe development of SDB and an intensive collaboration between different medicalspecialities.

61
References
AHLQVIST-RASTAD, J., HULTCRANTZ, E. and SVANHOLM, H. (1988) Childrenwith tonsillar obstruction: indications for and efficacy of tonsillectomy. ActaPaediatrica Scandinavica, 77(6), pp. 831-835.
ALABI, B.S., ABDULKARIM, A.A., MUSA, I.O., ADEGBOYE, O., AREMU, S.K.,ABDUR-RAHMAN, L.O., OMOKANYE, H.K., KATIBI, O.S., BELLO, O.A., ANOBA,S. and ABD'RAZAQ-FOLORUNSHO, M. (2012) Prevalence of snoring and symptomsof sleep disordered breathing among primary school pupils in Ilorin, Nigeria.International Journal of Pediatric Otorhinolaryngology, 76(5) pp. 646-648.
ALEXOPOULOS, E.I., MALAKASIOTI, G., VARLAMI, V., MILIGKOS, M.,GOURGOULIANIS, K. and KADITIS, A.G. (2014) Nocturnal enuresis is associatedwith moderate-to-severe obstructive sleep apnea in children with snoring. PediatricResearch, 76(6), pp. 555-559.
ALI, N.J., PITSON, D. and STRADLING, J.R. (1996) Sleep disordered breathing: effectsof adenotonsillectomy on behaviour and psychological functioning. European Journalof Pediatrics, 155(1), pp. 56-62.
ALI, N.J., PITSON, D.J. and STRADLING, J.R. (1993) Snoring, sleep disturbance, andbehaviour in 4-5 year olds. Archives of Disease in Childhood, 68(3), pp. 360-366.
ALKHALIL, M. and LOCKEY, R. (2011) Pediatric obstructive sleep apnea syndrome(OSAS) for the allergist: update on the assessment and management. Annals of Allergy,Asthma & Immunology, 107(2), pp. 104-109.
AMERICAN ACADEMY OF SLEEP MEDICINE (2014) The International Classificationof Sleep Disorders. 3rd ed. Darien, Illinois.
AMERICAN HERITAGE DICTIONARY OF THE ENGLISH LANGUAGE (2016)Available at: http://americanheritage.yourdictionary.com/
AMERICAN THORACIC SOCIETY (1999) Cardiorespiratory sleep studies inchildren. Establishment of normative data and polysomnographic predictors ofmorbidity. American Journal of Respiratory and Critical Care Medicine, 160(4), pp. 1381-1387.

62
AMIRI, S., ABDOLLAHIFAKHIM, S., LOTFI, A., BAYAZIAN, G., SOHRABPOUR, M.and HEMMATJOO, T. (2015) Effect of adenotonsillectomy on ADHD symptoms ofchildren with adenotonsillar hypertrophy and sleep disordered breathing.International Journal of Pediatric Otorhinolaryngology, 79(8), pp. 1213-1217.
ANDERSON, V.B., MCKENZIE, J.A., SETON, C., FITZGERALD, D.A., WEBSTER,R.I., NORTH, K.N., JOFFE, D.A. and YOUNG, H.K. (2012) Sniff nasal inspiratorypressure and sleep disordered breathing in childhood neuromuscular disorders.Neuromuscular Disorders, 22(6), pp. 528-533.
ANUNTASEREE, W., ROOKKAPAN, K., KUASIRIKUL, S. and THONGSUKSAI, P.(2001) Snoring and obstructive sleep apnea in Thai school-age children: prevalenceand predisposing factors. Pediatric Pulmonology, 32, pp. 222-227.
ANUNTASEREE, W., SANGSUPAWANICH, P., MO-SUWAN, L., RUANGNAPA, K.and PRUPHETKAEW, N. (2014) Prospective cohort study on change in weight statusand occurrence of habitual snoring in children. Clinical Otolaryngology 39(3) pp. 164-168.
APOSTOLIDOU, M.T., ALEXOPOULOS, E.I., CHAIDAS, K., NTAMAGKA, G.,KARATHANASI, A., APOSTOLIDIS, T.I., GOURGOULIANIS, K. and KADITIS, A.G.(2008) Obesity and persisting sleep apnea after adenotonsillectomy in Greek children.Chest, 134(6), pp. 1149-1155.
ARENS, R., MCDONOUGH, J.M., CORBIN, A.M., RUBIN, N.K., CARROLL, M.E.,PACK, A.I., LIU, J. and UDUPA, J.K. (2003) Upper airway size analysis by magneticresonance imaging of children with obstructive sleep apnea syndrome. AmericanJournal of Respiratory and Critical Care Medicine, 167(1), pp. 65-70.
ARONEN, E.T., LIUKKONEN, K., SIMOLA, P., VIRKKULA, P., USCHAKOFF, A.,KORKMAN, M., KIRJAVAINEN, T. and PITKÄRANTA, A. (2009) Mood is associatedwith snoring in preschool-aged children. Journal of Developmental and BehavioralPediatrics, 30(2), pp. 107-114.
ASHOK, N., VARMA, N.K., AJITH, V.V. and GOPINATH, S. (2014) Effect of rapidmaxillary expansion on sleep characteristics in children. Contemporary ClinicalDentistry, 5(4), pp. 489-494.
AUCHINCLOSS, J.H.,Jr, COOK, E. and RENZETTI, A.D. (1955) Clinical andphysiological aspects of a case of obesity, polycythemia and alveolar hypoventilation.The Journal of Clinical Investigation, 34(10), pp. 1537-1545.
AYAPPA, I. and RAPOPORT, D.M. (2003) The upper airway in sleep: physiology ofthe pharynx. Sleep Medicine Reviews, 7(1), pp. 9-33.

63
BAO, W., SRINIVASAN, S.R. and BERENSON, G.S. (1996) Persistent elevation ofplasma insulin levels is associated with increased cardiovascular risk in children andyoung adults. The Bogalusa Heart Study. Circulation, 93(1), pp. 54-59.
BEEBE, D.W. (2006) Neurobehavioral morbidity associated with disordered breathingduring sleep in children: a comprehensive review. Sleep, 29(9), pp. 1115-1134.
BEEBE, D.W. and GOZAL, D. (2002) Obstructive sleep apnea and the prefrontalcortex: towards a comprehensive model linking nocturnal upper airway dysfunctionto daytime cognitive and behavioral deficits. Journal of Sleep Research, 11(1), pp. 1-16.
BEHLFELT, K., LINDER-ARONSON, S. and NEANDER, P. (1990) Posture of thehead, the hyoid bone, and the tongue in children with and without enlarged tonsils.European Journal of Orthodontics, 12(4), pp. 458-467.
BERGER, G., BERGER, R. and OKSENBERG, A. (2009) Progression of snoring andobstructive sleep apnoea: the role of increasing weight and time. The EuropeanRespiratory Journal, 33(2), pp. 338-345.
BHATTACHARJEE, R., KHEIRANDISH-GOZAL, L., SPRUYT, K., MITCHELL, R.B.,PROMCHIARAK, J., SIMAKAJORNBOON, N., KADITIS, A.G., SPLAINGARD, D.,SPLAINGARD, M., BROOKS, L.J., MARCUS, C.L., SIN, S., ARENS, R., VERHULST,S.L. and GOZAL, D. (2010) Adenotonsillectomy outcomes in treatment of obstructivesleep apnea in children: a multicenter retrospective study. American Journal ofRespiratory and Critical Care Medicine, 182(5), pp. 676-683.
BICKELMANN, A.G., BURWELL, C.S., ROBIN, E.D. and WHALEY, R.D. (1956)Extreme obesity associated with alveolar hypoventilation; a Pickwickian syndrome.The American Journal of Medicine, 21(5), pp. 811-818.
BIXLER, E.O., FERNANDEZ-MENDOZA, J., LIAO, D., CALHOUN, S., RODRIGUEZ-COLON, S.M., GAINES, J., HE, F. and VGONTZAS, A.N. (2016) Natural history ofsleep disordered breathing in prepubertal children transitioning to adolescence. TheEuropean Respiratory Journal, 47(5), pp. 1402-1409.
BIXLER, E.O., VGONTZAS, A.N., LIN, H.M., LIAO, D., CALHOUN, S., VELA-BUENO, A., FEDOK, F., VLASIC, V. and GRAFF, G. (2009) Sleep disordered breathingin children in a general population sample: prevalence and risk factors. Sleep, 32(6),pp. 731-736.
BJÖRK, A., KREBS, B. and SOLOW, B. (1964) A method for epidemiologicalregistration of malocclusion. Acta Odontologica Scandinavica, 22, pp. 27-41.

64
BONUCK, K.A., CHERVIN, R.D., COLE, T.J., EMOND, A., HENDERSON, J., XU, L.and FREEMAN, K. (2011) Prevalence and persistence of sleep disordered breathingsymptoms in young children: a 6-year population-based cohort study. Sleep, 34(7), pp.875-884.
BONUCK, K.A., FREEMAN, K. and HENDERSON, J. (2009) Growth and growthbiomarker changes after adenotonsillectomy: systematic review and meta-analysis.Archives of Disease in Childhood, 94(2), pp. 83-91.
BORBÉLY, A.A. (2009) Refining sleep homeostasis in the two-process model. Journalof Sleep Research, 18(1), pp. 1-2.
BOURKE, R., ANDERSON, V., YANG, J.S., JACKMAN, A.R., KILLEDAR, A., NIXON,G.M., DAVEY, M.J., WALKER, A.M., TRINDER, J. and HORNE, R.S. (2011) Cognitiveand academic functions are impaired in children with all severities of sleep-disorderedbreathing. Sleep Medicine, 12(5), pp. 489-496.
BOWER, C.M. and GUNGOR, A. (2000) Pediatric obstructive sleep apnea syndrome.Otolaryngologic Clinics of North America, 33(1), pp. 49-75.
BRAGE, S., BRAGE, N., FRANKS, P.W., EKELUND, U. and WAREHAM, N.J. (2005)Reliability and validity of the combined heart rate and movement sensor Actiheart.European Journal of Clinical Nutrition, 59(4), pp. 561-570.
BROCKMANN, P.E., BERTRAND, P. and CASTRO-RODRIGUEZ, J.A. (2014)Influence of asthma on sleep disordered breathing in children: a systematic review.Sleep Medicine Reviews, 18(5), pp. 393-397.
BROCKMANN, P.E., URSCHITZ, M.S., SCHLAUD, M. and POETS, C.F. (2012)Primary snoring in school children: prevalence and neurocognitive impairments. Sleepand Breathing, 16(1):23-29.
BRODSKY, L. (1989) Modern assessment of tonsils and adenoids. Pediatric Clinics ofNorth America, 36(6), pp. 1551-1569.
BRUNNER, E.J., HEMINGWAY, H., WALKER, B.R., PAGE, M., CLARKE, P.,JUNEJA, M., SHIPLEY, M.J., KUMARI, M., ANDREW, R., SECKL, J.R.,PAPADOPOULOS, A., CHECKLEY, S., RUMLEY, A., LOWE, G.D., STANSFELD,S.A. and MARMOT, M.G. (2002) Adrenocortical, autonomic, and inflammatory causesof the metabolic syndrome: nested case-control study. Circulation, 106(21), pp. 2659-2665.

65
CARROLL, J.L., MCCOLLEY, S.A., MARCUS, C.L., CURTIS, S. and LOUGHLIN,G.M. (1995) Inability of clinical history to distinguish primary snoring fromobstructive sleep apnea syndrome in children. Chest, 108(3), pp. 610-618.
CARSKADON, M. A. and DEMENT, W.C. (2011) Normal human sleep, in: Kryger,M.H., Roth, T. and Dement, W.C. (eds.) Principles and Practice of Sleep Medicine, 5th ed.,Elsevier Saunders, St. Louis, Missouri, pp. 16-26.
CARVALHO, F.R., LENTINI-OLIVEIRA, D., MACHADO, M.A., PRADO, G.F.,PRADO, L.B. and SACONATO, H. (2007) Oral appliances and functional orthopaedicappliances for obstructive sleep apnoea in children. The Cochrane Database of SystematicReviews, 2(2), CD005520.
CARVALHO, F.R., LENTINI-OLIVEIRA, D.A., CARVALHO, G.M., PRADO, L.B.,PRADO, G.F., and CARVALHO, L.B. (2014) Sleep-disordered breathing andorthodontic variables in children--pilot study. International Journal of PediatricOtorhinolaryngology, 78(11), pp. 1965-1969. doi: 10.1016/j.ijporl.2014.08.040.
CASTRONOVO, V., ZUCCONI, M., NOSETTI, L., MARAZZINI, C., HENSLEY, M.,VEGLIA, F., NESPOLI, L. and FERINI-STRAMBI, L. (2003) Prevalence of habitualsnoring and sleep-disordered breathing in preschool-aged children in an Italiancommunity. The Journal of Pediatrics, 142(4), pp. 377-382.
CHALMERS, E.V., MCINTYRE, G.T., WANG, W., GILLGRASS, T., MARTIN, C.B.,and MOSSEY, P.A. (2016) Intraoral 3D scanning or dental impressions for theassessment of dental arch relationships in cleft care: Which is superior? Cleft PalateCraniofacial Journal, 53(5), pp. 568-77. doi: 10.1597/15-036.
CHAN, E., STEENLAND, H.W., LIU, H. and HORNER, R.L. (2006) Endogenousexcitatory drive modulating respiratory muscle activity across sleep-wake states.American Journal of Respiratory and Critical Care Medicine, 174(11), pp. 1264-1273.
CHERVIN, R.D., ARCHBOLD, K.H., DILLON, J.E., PANAHI, P., PITUCH, K.J.,DAHL, R.E. and GUILLEMINAULT, C. (2002) Inattention, hyperactivity, andsymptoms of sleep-disordered breathing. Pediatrics, 109(3), pp. 449-456.
CHERVIN, R.D., ELLENBERG, S.S., HOU, X., MARCUS, C.L., GARETZ, S.L., KATZ,E.S., HODGES, E.K., MITCHELL, R.B., JONES, D.T., ARENS, R., AMIN, R., REDLINE,S. and ROSEN, C.L. (2015) Prognosis for spontaneous resolution of OSA in children.Chest, 148(5), pp. 1204-1213.
CHERVIN, R.D., WEATHERLY, R.A., RUZICKA, D.L., BURNS, J.W., GIORDANI,B.J., DILLON, J.E., MARCUS, C.L., GARETZ, S.L., HOBAN, T.F. and GUIRE, K.E.

66
(2006) Subjective sleepiness and polysomnographic correlates in children scheduledfor adenotonsillectomy vs other surgical care. Sleep, 29(4), pp. 495-503.
CHIANG, H.L., GAU, S.S., NI, H.C., CHIU, Y.N., SHANG, C.Y., WU, Y.Y., LIN, L.Y.,TAI, Y.M. and SOONG, W.T. (2010) Association between symptoms and subtypes ofattention-deficit hyperactivity disorder and sleep problems/disorders. Journal of SleepResearch, 19(4), pp. 535-545.
CHNG, S.Y., GOH, D.Y., WANG, X.S., TAN, T.N. and ONG, N.B. (2004) Snoring andatopic disease: a strong association. Pediatric Pulmonology, 38, pp. 210-216.
COLE, T.J., BELLIZZI, M.C., FLEGAL, K.M. and DIETZ, W.H. (2000) Establishing astandard definition for child overweight and obesity worldwide: international survey.British Medical Journal 320(7244), pp. 1240-1243.
COLE, T.J., FREEMAN, J.V. and PREECE, M.A. (1995) Body mass index referencecurves for the UK, 1990. Archives of Disease in Childhood, 73(1), pp. 25-29.
CORBO, G.M., FORASTIERE, F., AGABITI, N., PISTELLI, R., DELL'ORCO, V.,PERUCCI, C.A. and VALENTE, S. (2001) Snoring in 9- to 15-year-old children: riskfactors and clinical relevance. Pediatrics, 108(5), pp. 1149-1154.
CRABTREE, V.M., VARNI, J.W. and GOZAL, D. (2004) Health-related quality of lifeand depressive symptoms in children with suspected sleep-disordered breathing.Sleep, 27(6), pp. 1131-1138.
CROUSE, U., LAINE-ALAVA, M.T. and WARREN, D.W. (2000) Nasal impairment inprepubertal children. American Journal of Orthodontics and Dentofacial Orthopedics,118(1), pp. 69-74.
CULEBRAS, A. (2002) Normal sleep, in Lee-Chiong, T.L. Jr., Sateia, M.J. andCarskadon, M. A. (eds.) Sleep Medicine, Hanley & Belfus Inc, Philadelphia, pp. 1-6.
DAYYAT, E., KHEIRANDISH-GOZAL, L. and GOZAL, D. (2007) ChildhoodObstructive Sleep Apnea: One or Two Distinct Disease Entities? Sleep Medicine Clinics,2(3), pp. 433-444.
DE LUCA CANTO, G., SINGH, V., MAJOR, M.P., WITMANS, M., EL-HAKIM, H.,MAJOR, P.W. and FLORES-MIR, C. (2014) Diagnostic capability of questionnaires andclinical examinations to assess sleep-disordered breathing in children: a systematicreview and meta-analysis. Journal of the American Dental Association, 145(2), pp. 165-178.

67
EISENBERG, N., FABES, R.A., SHEPARD, S.A., MURPHY, B.C., JONES, S. andGUTHRIE, I.K. (1998) Contemporaneous and longitudinal prediction of children'ssympathy from dispositional regulation and emotionality. Developmental Psychology,34(5), pp. 910-924.
ELORANTA, A.M., LINDI, V., SCHWAB, U., TOMPURI, T., KIISKINEN, S., LAKKA,H.M., LAITINEN, T. and LAKKA, T.A. (2012) Dietary factors associated withoverweight and body adiposity in Finnish children aged 6-8 years: the PANIC Study.International Journal of Obesity, 36(7), pp. 950-955.
ENRIGHT, P.L., GOODWIN, J.L., SHERRILL, D.L., QUAN, J.R., QUAN, S.F. andTUCSON CHILDREN'S ASSESSMENT OF SLEEP APNEA STUDY (2003) Bloodpressure elevation associated with sleep-related breathing disorder in a communitysample of white and Hispanic children: the Tucson Children's Assessment of SleepApnea study. Archives of Pediatrics & Adolescent Medicine, 157(9), pp. 901-904.
ERSU, R., ARMAN, A.R., SAVE, D., KARADAG, B., KARAKOC, F., BERKEM, M. andDAGLI, E. (2004) Prevalence of snoring and symptoms of sleep-disordered breathingin primary school children in Istanbul. Chest, 126(1), pp. 19-24.
ESKELI, R. (2015) Eruption pattern and occlusal development of the permanent dentitionamong different population and ethnic groups. PhD thesis. University of Eastern Finland.
FADZIL ABDULLAH, A.A., JAMALLUDIN, A.R., NORRASHIDAH, A.W.,NORZILA, M.Z., ASIAH KASSIM, K., RUS ANIDA, A., HASNIAH A.L., RAMLI, Z.and SAMSINAH H. (2012) Prevalence of sleep disordered breathing symptomsamong Malay school children in a primary school in Malaysia. Medical Journal ofMalaysia, 67(2) pp. 181-185.
FLORES-MIR, C., KORAYEM, M., HEO, G., WITMANS, M., MAJOR, M.P. andMAJOR, P.W. (2013) Craniofacial morphological characteristics in children withobstructive sleep apnea syndrome: a systematic review and meta-analysis. Journal ofthe American Dental Association, 144(3), pp. 269-277.
FLOYD, J.A., MEDLER, S.M., AGER, J.W. and JANISSE, J.J. (2000) Age-relatedchanges in initiation and maintenance of sleep: a meta-analysis. Research in Nursing &Health, 23(2), pp. 106-117.
FOLEY, D.J., VITIELLO, M.V., BLIWISE, D.L., ANCOLI-ISRAEL, S., MONJAN, A.A.and WALSH, J.K. (2007) Frequent napping is associated with excessive daytimesleepiness, depression, pain, and nocturia in older adults: findings from the NationalSleep Foundation '2003 Sleep in America' Poll. American Journal of Geriatric Psychiatry,15(4), pp. 344-350.

68
FOLLMAR, A., DENTINO, K., ABRAMOWICZ, S. and PADWA, B.L. (2014)Prevalence of sleep-disordered breathing in patients with Beckwith-Wiedemannsyndrome. The Journal of Craniofacial Surgery, 25(5), pp. 1814-1817.
FOUKE, J.M., TEETER, J.P. and STROHL, K.P. (1986) Pressure-volume behavior of theupper airway. Journal of Applied Physiology, 61(3), pp. 912-918.
FRIBERG, D., SUNDQUIST, J., LI, X., HEMMINKI, K. and SUNDQUIST, K. (2009)Sibling risk of pediatric obstructive sleep apnea syndrome and adenotonsillarhypertrophy. Sleep, 32(8), pp. 1077-1083.
FUNG, E., WITMANS, M., GHOSH, M., CAVE, D. and EL-HAKIM, H. (2012) Upperairway findings in children with Down syndrome on sleep nasopharyngoscopy: case-control study. Journal of Otolaryngology - Head & Neck Surgery, 41(2), pp. 138-144.
FUNG, T.T., CHIUVE, S.E., MCCULLOUGH, M.L., REXRODE, K.M., LOGROSCINO,G. and HU, F.B. (2008) Adherence to a DASH-style diet and risk of coronary heartdisease and stroke in women. Archives of Internal Medicine, 168(7), pp. 713-720.
GILL, A.I., SCHAUGHENCY, E. and GALLAND, B.C. (2012) Prevalence and factorsassociated with snoring in 3-year olds: early links with behavioral adjustment. SleepMedicine, 13(9), pp. 1191-1197.
GOH, D.Y., GALSTER, P. and MARCUS C.L. (2000) Sleep architecture and respiratorydisturbances in children with obstructive sleep apnea. American Journal of Respiratoryand Critical Care Medicine, 162(2 Pt 1), pp. 682-686.
GOLDBART, A.D., MAGER, E., VELING, M.C., GOLDMAN, J.L., KHEIRANDISH-GOZAL, L., SERPERO, L.D., PIEDIMONTE, G. and GOZAL, D. (2007) Neurotrophinsand tonsillar hypertrophy in children with obstructive sleep apnea. Pediatric Research,62(4), pp. 489-494.
GOODWIN, J.L., BABAR, S.I., KAEMINGK, K.L., ROSEN, G.M., MORGAN, W.J.,SHERRILL, D.L. and QUAN, S.F. (2003) Symptoms related to sleep-disorderedbreathing in white and Hispanic children: the Tucson Children's Assessment of SleepApnea Study. Chest, 124, pp.196-203.
GOODWIN, J.L., VASQUEZ, M.M., SILVA, G.E. and QUAN, S.F. (2010) Incidence andremission of sleep-disordered breathing and related symptoms in 6- to 17-year oldchildren--the Tucson Children's Assessment of Sleep Apnea Study. The Journal ofPediatrics, 157(1), pp. 57-61.
GOTTLIEB, D.J., CHASE C., VEZINA, R.M., HEEREN, T.C., CORWIN, M.J.,AUERBACH, S.H., WEESE-MAYER, D.E. and LESKO, S.M. (2004) Sleep-disordered

69
breathing symptoms are associated with poorer cognitive function in 5-year-oldchildren. Journal of Pediatrics, 145, pp. 458-464.
GOZAL, D. (2001) Morbidity of obstructive sleep apnea in children: facts and theory.Sleep & Breathing, 5(1), pp. 35-42.
GOZAL, D. (1998) Sleep-disordered breathing and school performance in children.Pediatrics, 102(3 Pt 1), pp. 616-620.
GOZAL, D., CAPDEVILA, O.S. and KHEIRANDISH-GOZAL, L. (2008) Metabolicalterations and systemic inflammation in obstructive sleep apnea among nonobeseand obese prepubertal children. American Journal of Respiratory and Critical CareMedicine, 177(10), pp. 1142-1149.
GOZAL, D. and KHEIRANDISH-GOZAL, L. (2009) Obesity and excessive daytimesleepiness in prepubertal children with obstructive sleep apnea. Pediatrics, 123(1), pp.13-18.
GOZAL, D., KHEIRANDISH-GOZAL, L., BHATTACHARJEE, R. and SPRUYT, K.(2010) Neurocognitive and endothelial dysfunction in children with obstructive sleepapnea. Pediatrics, 126(5), pp. e1161-1167.
GOZAL, D., KHEIRANDISH-GOZAL, L., SERPERO, L.D., SANS CAPDEVILA, O.and DAYYAT, E. (2007) Obstructive sleep apnea and endothelial function in school-aged nonobese children: effect of adenotonsillectomy. Circulation, 116(20), pp. 2307-2314.
GOZAL, D. and POPE, D.W. Jr. (2001) Snoring during early childhood and academicperformance at ages thirteen to fourteen years. Pediatrics, 107(6), pp. 1394-1399.
GROSS, C.W. and HARRISON, S.E. (2000) Tonsils and adenoids. Pediatrics in Review /American Academy of Pediatrics, 21(3), pp. 75-78.
GUDNADOTTIR, G., EHNHAGE, A., BENDE, M., ANDERSSON, M., CERVIN, A.,CARDELL, L.O. and HELLGREN, J. (2016) Healthcare provider contact for childrenwith symptoms of sleep-disordered breathing: a population survey. Journal ofLaryngology & Otology, 130(3):296-301.
GUILLEMINAULT, C., ELDRIDGE, F.L., SIMMONS, F.B. and DEMENT, W.C. (1976)Sleep apnea in eight children. Pediatrics, 58(1), pp. 23-30.
GUILLEMINAULT, C. and LI, K.K. (2004) Maxillomandibular expansion for thetreatment of sleep-disordered breathing: preliminary result. The Laryngoscope, 114(5),pp. 893-896.

70
GUILLEMINAULT, C., STOOHS, R., CLERK, A., CETEL, M. and MAISTROS, P.(1993) A cause of excessive daytime sleepiness. The upper airway resistancesyndrome. Chest, 104(3), pp. 781-787.
GUPTA, R., GOEL, D., KANDPAL, S.D., MITTAL, N., DHYANI, M. and MITTAL, M.(2016) Prevalence of sleep disorders among primary school children. Indian Journal ofPediatrics [Epub ahead of print]
HANGGI, M.P., TEUSCHER, U.M., ROOS, M. and PELTOMÄKI, T.A. (2008) Long-term changes in pharyngeal airway dimensions following activator-headgear andfixed appliance treatment. European Journal of Orthodontics, 30(6), pp. 598-605.
HENDERSON, J.M., FRANCE, K.G., OWENS, J.L. and BLAMPIED, N.M. (2010)Sleeping through the night: the consolidation of self-regulated sleep across the firstyear of life. Pediatrics, 126(5), pp. e1081-1087. doi: 10.1542/peds.2010-0976
HOEVE, L.J., PIJPERS, M. and JOOSTEN, K.F. (2003) OSAS in craniofacial syndromes:an unsolved problem. International Journal of Pediatric Otorhinolaryngology, 67 Suppl 1,pp. S111-S113.
HORNER, R.L. (2001) The neuropharmacology of upper airway motor control in theawake and asleep states: implications for obstructive sleep apnoea. RespiratoryResearch, 2(5), pp. 286-294.
HORNER, R.L. (2008a) Pathophysiology of obstructive sleep apnea. Journal ofCardiopulmonary Rehabilitation and Prevention, 28(5), pp. 289-298.
HORNER, R.L. (2008b) Neuromodulation of hypoglossal motoneurons during sleep.Respiratory Physiology & Neurobiology, 164(1-2), pp. 179-196.
HULTCRANTZ, E. and LÖFSTRAND-TIDESTRÖM, B. (2009) The development ofsleep disordered breathing from 4 to 12 years and dental arch morphology.International Journal of Pediatric Otorhinolaryngology, 73(9), pp. 1234-1241.
HUYNH, N.T., DESPLATS, E. and ALMEIDA, F.R. (2016) Orthodontics treatments formanaging obstructive sleep apnea syndrome in children: A systematic review andmeta-analysis. Sleep Medicine Reviews, 25, pp. 84-94.
IBER, C., ANCOLI-ISRAEL, S., and QUAN, S.F. for the American Academy of SleepMedicine (2007) The AASM manual for the scoring of sleep and associated events:rules, terminology, and technical specifications. 1st ed., Westchester, Illinois.

71
ISHMAN, S.L., SMITH, D.F., BENKE, J.R., NGUYEN, M.T. and LIN, S.Y. (2012) Theprevalence of sleepiness and the risk of sleep-disordered breathing in children withpositive allergy test. International Forum of Allergy & Rhinology, 2(2), pp. 139-143.
JACKMAN, A.R., BIGGS, S.N., WALTER, L.M., EMBULDENIYA, U.S., DAVEY, M.J.,NIXON, G.M., ANDERSON, V., TRINDER, J. and HORNE, R.S. (2013) Sleepdisordered breathing in early childhood: quality of life for children and families. Sleep,36(11), pp. 1639-1646.
JACKMAN, A.R., BIGGS, S.N., WALTER, L.M., EMBULDENIYA, U.S., DAVEY, M.J.,NIXON, G.M., ANDERSON, V., TRINDER, J. and HORNE, R.S. (2012) Sleep-disordered breathing in preschool children is associated with behavioral, but notcognitive, impairments. Sleep Medicine, 13(6), pp. 621-631.
JARA, S.M., BENKE, J.R., LIN, S.Y. and ISHMAN, S.L. (2015) The association betweensecondhand smoke and sleep-disordered breathing in children: a systematic review.The Laryngoscope, 125(1), pp. 241-247.
JAVAHERI, S. and DEMPSEY, J.A. (2013) Central sleep apnea. ComprehensivePhysiology, 3(1), pp. 141-163.
JENNI, O.G. and O'CONNOR, B.B. (2005) Children's sleep: an interplay betweenculture and biology. Pediatrics, 115(1 Suppl), pp. 204-216.
JOHNSON, E.O., and ROTH, T. (2006) An epidemiologic study of sleep-disorderedbreathing symptoms among adolescents. Sleep, 29, pp.1135-1142.
KADITIS, A.G., ALONSO ALVAREZ, M.L., BOUDEWYNS, A., ALEXOPOULOS, E.I.,ERSU, R., JOOSTEN, K., LARRAMONA, H., MIANO, S., NARANG, I., TRANG, H.,TSAOUSSOGLOU, M., VANDENBUSSCHE, N., VILLA, M.P., VANWAARDENBURG, D., WEBER, S. and VERHULST, S. (2016) Obstructive sleepdisordered breathing in 2- to 18-year-old children: diagnosis and management. TheEuropean Respiratory Journal, 47(1), pp. 69-94.
KANG, K.T., WENG, W.C., LEE, C.H., HSIAO, T.Y., LEE, P.L., LEE, Y.L. and HSU,W.C. (2015) Detection of pediatric obstructive sleep apnea syndrome: history oranatomical findings? Sleep Medicine, 16(5), pp. 617-624.
KAPUR, V.K. (2010) Obstructive sleep apnea: diagnosis, epidemiology, andeconomics. Respiratory Care, 55(9), pp. 1155-1167.
KARA, C.O., ERGIN, H., KOCAK, G., KILIC, I. and YURDAKUL, M. (2002)Prevalence of tonsillar hypertrophy and associated oropharyngeal symptoms in

72
primary school children in Denizli, Turkey. International Journal of PediatricOtorhinolaryngology, 66, pp. 175-179.
KATO, M., ROBERTS-THOMSON, P., PHILLIPS, B.G., HAYNES, W.G., WINNICKI,M., ACCURSO, V. and SOMERS, V.K. (2000) Impairment of endothelium-dependentvasodilation of resistance vessels in patients with obstructive sleep apnea. Circulation,102(21), pp. 2607-2610.
KATZ, E.S. and D'AMBROSIO, C.M. (2008) Pathophysiology of pediatric obstructivesleep apnea. Proceedings of the American Thoracic Society, 5(2), pp. 253-262.
KAWASHIMA, S., NIIKUNI, N., LO, C.H., KOHNO, M., NAKAJIMA, I. andAKASAKA, M. (1999) Clinical findings in Japanese children with obstructive sleepapnea syndrome: focus on dental findings. Journal of Oral Science, 41(3), pp. 99-103.
KEROSUO, H., LAINE, T., NYYSSÖNEN, V. and HONKALA, E. (1991) Occlusalcharacteristics in groups of Tanzanian and Finnish urban schoolchildren. AngleOrthodontist, 61(1), pp. 49-55.
KHEIRANDISH-GOZAL, L., CAPDEVILA, O.S., TAUMAN, R. and GOZAL, D. (2006)Plasma C-reactive protein in nonobese children with obstructive sleep apnea beforeand after adenotonsillectomy. Journal of Clinical Sleep Medicine, 2(3), pp. 301-304.
KIPPING, R.R., JAGO, R. and LAWLOR, D.A. (2008) Obesity in children. Part 1:Epidemiology, measurement, risk factors, and screening. British Medical Journal, 337,pp. a1824.
KOHLER, M.J. and VAN DEN HEUVEL, C.J. (2008) Is there a clear link betweenoverweight/obesity and sleep disordered breathing in children? Sleep MedicineReviews, 12(5), pp. 347-361; 363-364.
KOIVUSALO, A.I., PAKARINEN, M.P., WIKSTRÖM, A. and RINTALA, R.J. (2011)Assessment and treatment of gastroesophageal reflux in healthy infants with apneicepisodes: a retrospective analysis of 87 consecutive patients. Clinical Pediatrics, 50(12),pp. 1096-1102.
KUO, C.Y. and PARIKH, S.R. (2014) Can lingual tonsillectomy improve persistentpediatric obstructive sleep apnea? The Laryngoscope, 124(10), pp. 2211-2212.
KURNATOWSKI, P., PUTYNSKI, L., LAPIENIS, M. and KOWALSKA, B. (2008)Physical and emotional disturbances in children with adenotonsillar hypertrophy. TheJournal of Laryngology and Otology, 122(9), pp. 931-935.

73
KWOK, K.L., NG, D.K. and CHEUNG, Y.F. (2003) BP and arterial distensibility inchildren with primary snoring. Chest, 123(5), pp. 1561-1566.
LAITINEN, L.A., ANTTALAINEN, U., PIETINALHO, A., HÄMÄLÄINEN, P.,KOSKELA, K. and EXPERT ADVISORY GROUP LISTED IN FOREWORD (2003)Sleep apnoea: Finnish National guidelines for prevention and treatment 2002-2012.Respiratory Medicine, 97(4), pp. 337-365.
LAM, Y.Y., CHAN, E.Y., NG, D.K., CHAN, C.H., CHEUNG, J.M., LEUNG, S.Y.,CHOW, P.Y. and KWOK, K.L. (2006) The correlation among obesity, apnea-hypopneaindex, and tonsil size in children. Chest, 130(6), pp. 1751-1756.
LANDIS, J.R. and KOCH, G.G. (1977) The measurement of observer agreement forcategorical data. Biometrics, 33(1), pp. 159-174
LAVIGNE, G.J., MORIN, C.M. and CARRA, M.C. (2009) The nature of sleep, inLavigne, G.J., Cistulli, P.A. and Smith, M.T. (eds.) Sleep Medicine for Dentists,Quintessence Publishing Co, Inc, pp. 3-10.
LEGAN, H.L. and BURSTONE, C.J. (1980) Soft tissue cephalometric analysis fororthognathic surgery. Journal of Oral Surgery, 38(10), pp. 744-751.
LEIBERMAN, A., OHKI, M., FORTE, V., FRASCHETTI, J. and COLE, P. (1990)Nose/mouth distribution of respiratory airflow in 'mouth breathing' children. ActaOto-Laryngologica, 109(5-6), pp. 454-460.
LEINUM, C.J., DOPP, J.M. and MORGAN, B.J. (2009) Sleep-disordered breathing andobesity: pathophysiology, complications, and treatment. Nutrition in Clinical Practice,24(6), pp. 675-687.
LI, A.M., WONG, E., KEW, J., HUI, S. and FOK, T.F. (2002) Use of tonsil size in theevaluation of obstructive sleep apnoea. Archives of Disease in Childhood, 87(2), pp. 156-159.
LI, A.M., YIN, J., CHAN, D., HUI, S. and FOK, T.F. (2003) Sleeping energy expenditurein paediatric patients with obstructive sleep apnoea syndrome. Hong Kong MedicalJournal, 9(5), pp. 353-356.
LI, H.Y. and LEE, L.A. (2009) Sleep-disordered breathing in children. Chang GungMedical Journal, 32(3), pp. 247-257.
LI, M., LI, K., ZHANG, X.W., HOU, W.S. and TANG, Z.Y. (2015) Habitual snoring andrisk of stroke: A meta-analysis of prospective studies. International Journal ofCardiology, 185, pp. 46-49.

74
LINDER-ARONSON, S. (1970) Adenoids. Their effect on mode of breathing and nasalairflow and their relationship to characteristics of the facial skeleton and the denition.A biometric, rhino-manometric and cephalometro-radiographic study on childrenwith and without adenoids. Acta Oto-Laryngologica, Suppl. 265, pp. 1-132.
LINDER-ARONSON, S. and LEIGHTON, B.C. (1983) A longitudinal study of thedevelopment of the posterior nasopharyngeal wall between 3 and 16 years of age.European Journal of Orthodontics, 5(1), pp. 47-58.
LINTU, N., TOMPURI, T., VIITASALO, A., SOININEN, S., LAITINEN, T.,SAVONEN, K., LINDI, V. and LAKKA, T.A. (2014) Cardiovascular fitness andhaemodynamic responses to maximal cycle ergometer exercise test in children 6-8years of age. Journal of Sports Sciences, 32(7), pp. 652-659.
LIUKKONEN, K., VIRKKULA, P., ARONEN, E.T., KIRJAVAINEN, T., andPITKÄRANTA, A. (2008) All snoring is not adenoids in young children. InternationalJournal of Pediatric Otorhinolaryngology 72(6), pp. 879-84.
LUMENG, J.C. and CHERVIN, R.D. (2008) Epidemiology of pediatric obstructivesleep apnea. Proceedings of the American Thoracic Society, 5(2), pp. 242-252.
LÖFSTRAND-TIDESTRÖM, B. and HULTCRANTZ, E. (2010) Development ofcraniofacial and dental arch morphology in relation to sleep disordered breathingfrom 4 to 12 years. Effects of adenotonsillar surgery. International Journal of PediatricOtorhinolaryngology, 74(2), pp. 137-143.
LÖFSTRAND-TIDESTRÖM, B. and HULTCRANTZ, E. (2007) The development ofsnoring and sleep related breathing distress from 4 to 6 years in a cohort of Swedishchildren. International Journal of Pediatric Otorhinolaryngology, 71(7), pp. 1025-1033.
LÖFSTRAND-TIDESTRÖM, B., THILANDER, B., AHLQVIST-RASTAD, J.,JAKOBSSON, O. and HULTCRANTZ, E. (1999) Breathing obstruction in relation tocraniofacial and dental arch morphology in 4-year-old children. European Journal ofOrthodontics, 21(4), pp. 323-332.
MACARI, A.T., BITAR, M.A., and GHAFARI, J.G. (2012) New insights on age-relatedassociation between nasopharyngeal airway clearance and facial morphology.Orthodontics & Craniofacial Research 15(3), pp. 188-197.
MACHADO-JÚNIOR, A.J., SIGNORELLI, L.G., ZANCANELLA, E. and CRESPO,A.N. (2016b) Randomized controlled study of a mandibular advancement appliancefor the treatment of obstructive sleep apnea in children: A pilot study. Medicina Oral,Patología Oral y Cirugía Bucal, 21(4), pp. e403-407.

75
MACHADO-JÚNIOR, A.J., ZANCANELLA, E. and CRESPO, A.N. (2016a) Rapidmaxillary expansion and obstructive sleep apnea: A review and meta-analysis.Medicina Oral, Patología Oral y Cirugía Bucal 21(4) pp. e465-469.
MACLEAN, J.E., HAYWARD, P., FITZGERALD, D.A. and WATERS, K. (2009) Cleftlip and/or palate and breathing during sleep. Sleep Medicine Reviews, 13(5), pp. 345-354.
MALAKASIOTI, G., GOURGOULIANIS, K., CHROUSOS, G. and KADITIS, A. (2011)Interactions of obstructive sleep-disordered breathing with recurrent wheezing orasthma and their effects on sleep quality. Pediatric Pulmonology, 46(11), pp. 1047-1054.
MALLAMPATI, S.R., GATT, S.P., GUGINO, L.D., DESAI, S.P., WARAKSA, B.,FREIBERGER, D. and LIU, P.L. (1985) A clinical sign to predict difficult trachealintubation: a prospective study. Canadian Anaesthetists' Society Journal, 32(4), pp. 429-434.
MANUEL, A., WITMANS, M. and EL-HAKIM, H. (2013) Children with a history ofprematurity presenting with snoring and sleep-disordered breathing: a cross-sectionalstudy. The Laryngoscope, 123(8), pp. 2030-2034.
MARCUS, C.L., BROOKS, L.J., DRAPER, K.A., GOZAL, D., HALBOWER, A.C.,JONES, J., SCHECHTER, M.S., WARD, S.D., SHELDON, S.H., SHIFFMAN, R.N.,LEHMANN, C., SPRUYT, K. and AMERICAN ACADEMY OF PEDIATRICS (2012)Diagnosis and management of childhood obstructive sleep apnea syndrome.Pediatrics, 130(3), pp. e714-755.
MARCUS, C.L., CARROLL, J.L., KOERNER, C.B., HAMER, A., LUTZ, J. andLOUGHLIN, G.M. (1994) Determinants of growth in children with the obstructivesleep apnea syndrome. The Journal of Pediatrics, 125(4), pp. 556-562.
MARCUS, C.L., CURTIS, S., KOERNER, C.B., JOFFE, A., SERWINT, J.R. andLOUGHLIN, G.M. (1996) Evaluation of pulmonary function and polysomnography inobese children and adolescents. Pediatric Pulmonology, 21(3), pp. 176-183.
MARCUS, C.L., GLOMB, W.B., BASINSKI, D.J., DAVIDSON, S.L. and KEENS, T.G.(1994) Developmental pattern of hypercapnic and hypoxic ventilatory responses fromchildhood to adulthood. Journal of Applied Physiology, 76(1), pp. 314-320.
MARCUS, C.L., GREENE, M.G. and CARROLL, J.L. (1998) Blood pressure in childrenwith obstructive sleep apnea. American Journal of Respiratory and Critical Care Medicine,157, pp. 1098-1103.

76
MARCUS, C.L., MOORE, R.H., ROSEN, C.L., GIORDANI, B., GARETZ, S.L.,TAYLOR, H.G., MITCHELL, R.B., AMIN, R., KATZ, E.S., ARENS, R. et al. (2013) Arandomized trial of adenotonsillectomy for childhood sleep apnea. New EnglandJournal of Medicine, 368(25), pp. 2366-2376.
MARINO, A., MALAGNINO, I., RANIERI, R., VILLA, M.P. and MALAGOLA, C.(2009) Craniofacial morphology in preschool children with obstructive sleep apnoeasyndrome. European Journal of Paediatric Dentistry, 10(4), pp. 181-184.
MARTIN, S.E., MATHUR, R., MARSHALL, I. and DOUGLAS, N.J. (1997) The effectof age, sex, obesity and posture on upper airway size. The European Respiratory Journal,10(9), pp. 2087-2090.
MATRICCIANI, L., BLUNDEN, S., RIGNEY, G., WILLIAMS, M.T. and OLDS, T.S.(2013) Children's sleep needs: is there sufficient evidence to recommend optimal sleepfor children? Sleep, 36(4), pp. 527-534.
MATRICCIANI, L.A., OLDS, T.S., BLUNDEN, S., RIGNEY, G. and WILLIAMS, M.T.(2012) Never enough sleep: a brief history of sleep recommendations for children.Pediatrics, 129(3), pp. 548-556.
MISLIK, B., HANGGI, M.P., SIGNORELLI, L., PELTOMÄKI, T.A. and PATCAS, R.(2014) Pharyngeal airway dimensions: a cephalometric, growth-study-based analysisof physiological variations in children aged 6-17. European Journal of Orthodontics,36(3), pp. 331-339.
MONTALDO, L., MONTALDO, P., CAREDDA, E. and D'ARCO, A. (2012)Association between exposure to secondhand smoke and sleep bruxism in children: arandomised control study. Tobacco Control, 21(4), pp. 392-395.
MONTGOMERY-DOWNS, H.E., O'BRIEN, L.M., GULLIVER, T.E. and GOZAL, D.(2006) Polysomnographic characteristics in normal preschool and early school-agedchildren. Pediatrics, 117(3), pp. 741-753.
MOORE, L.L., SINGER, M.R., BRADLEE, M.L., DJOUSSE, L., PROCTOR, M.H.,CUPPLES, L.A. and ELLISON, R.C. (2005) Intake of fruits, vegetables, and dairyproducts in early childhood and subsequent blood pressure change. Epidemiology,16(1), pp. 4-11.
MOORE, R.Y. (2013) The suprachiasmatic nucleus and the circadian timing system.Progress in Molecular Biology and Translational Science, 119, pp. 1-28.
MORALEDA-CIBRIAN, M., BERGER, M., EDWARDS, S.P., KASTEN, S.J.,BUCHMAN, S.R. and O'BRIEN, L.M. (2014) Association between symptoms of sleep-

77
disordered breathing and speech in children with craniofacial malformations. Journalof Clinical Sleep Medicine, 10(6), pp. 671-676.
MYLLÄRNIEMI, S. (1970) Malocclusion in Finnish rural children. PhD thesis. Proceedingsof the Finnish Dental Society, 66, pp. 221-264.
NEELAPU, B.C., KHARBANDA, O.P., SARDANA, H.K., BALACHANDRAN, R.,SARDANA, V., KAPOOR, P., GUPTA, A. and VASAMSETTI, S. (2016) Craniofacialand upper airway morphology in adult obstructive sleep apnea patients: A systematicreview and meta-analysis of cephalometric studies. Sleep Medicine Reviews, doi:10.1016/j.smrv.2016.01.007. [Epub ahead of print] .
NG, D.K., CHOW, P.Y., CHAN, C.H., KWOK, K.L., CHEUNG, J.M. and KONG, F.Y.(2006) An update on childhood snoring. Acta Paediatrica, 95(9), pp. 1029-1035.
NG, D.K., LAM, Y.Y., KWOK, K.L. and CHOW, P.Y. (2004) Obstructive sleep apnoeasyndrome and obesity in children. Hong Kong Medical Journal, 10(1), pp. 44-48.
NIEMINEN, P. (2002) Snoring and obstructive sleep apnea in young children. A 6-monthfollow-up study. PhD thesis. University of Oulu.
O'BRIEN, L.M. and GOZAL, D. (2005) Autonomic dysfunction in children with sleep-disordered breathing. Sleep, 28(6), pp. 747-752.
O'BRIEN, L.M., MERVIS, C.B., HOLBROOK, C.R., BRUNER, J.L., SMITH, N.H.,MCNALLY, N., MCCLIMMENT, M.C. and GOZAL, D. (2004) Neurobehavioralcorrelates of sleep-disordered breathing in children. Journal of Sleep Research, 13(2), pp.165-172.
OHAYON, M.M., LI, K.K., GUILLEMINAULT, C. (2001) Risk factors for sleepbruxism in the general population. Chest, 119(1), pp. 53-61.
OWENS, S. and GALLOWAY, R. (2014) Childhood obesity and the metabolicsyndrome. Current Atherosclerosis Reports, 16(9), pp. 436-014-0436-y.
PAAVONEN, E.J., ARONEN, E.T., MOILANEN, I., PIHA, J., RÄSÄNEN, E.,TAMMINEN, T., and ALMQVIST, F. (2000) Sleep problems of school-aged children: acomplementary view. Acta Paediatrica, 89(2), pp. 223-228.
PAHKALA, R., PUUSTINEN, R., TUOMILEHTO, H., AHLBERG, J. and SEPPÄ, J.(2011) Risk factors for sleep-disordered breathing: the role of craniofacial structure.Acta Odontologica Scandinavica, 69(3), pp. 137-143.

78
PAPAIOANNOU, G., KAMBAS, I., TSAOUSSOGLOU, M.,PANAGHIOTOPOULOU-GARTAGANI, P., CHROUSOS, G. and KADITIS, A.G.(2013) Age-dependent changes in the size of adenotonsillar tissue in childhood:implications for sleep-disordered breathing. The Journal of Pediatrics, 162(2), pp. 269-274.
PARTINEN, M. and GISLASON, T. (1995) Basic Nordic Sleep Questionnaire (BNSQ):a quantitated measure of subjective sleep complaints. Journal of Sleep Research, 4(S1),pp. 150-155.
PARUTHI, S., BROOKS, L.J., D'AMBROSIO, C., HALL, W.A., KOTAGAL, S., LLOYD,R.M., MALOW, B.A., MASKI, K., NICHOLS, C., QUAN, S.F., ROSEN, C.L.,TROESTER, M.M. and WISE, M.S. (2016) Recommended amount of sleep for pediatricpopulations: A consensus statement of the American Academy of Sleep Medicine.Journal of Clinical Sleep Medicine, 12(6), pp. 785-786. doi: 10.5664/jcsm.5866.
PELTOMÄKI, T. (2007) The effect of mode of breathing on craniofacial growth--revisited. European Journal of Orthodontics, 29(5), pp. 426-429.
PEPPARD, P.E., YOUNG, T., PALTA, M. and SKATRUD, J. (2000) Prospective studyof the association between sleep-disordered breathing and hypertension. The NewEngland Journal of Medicine, 342(19), pp. 1378-1384.
PEROMAA-HAAVISTO, P., TUOMILEHTO, H., KOSSI, J., VIRTANEN, J.,LUOSTARINEN, M., PIHLAJAMAKI, J., KAKELA, P. and VICTORZON, M. (2016)Prevalence of obstructive sleep apnoea among patients admitted for bariatric surgery.A prospective multicentre trial. Obesity Surgery, 26(7), pp. 1384-1390.
PIRILÄ-PARKKINEN, K., LÖPPÖNEN, H., NIEMINEN, P., TOLONEN, U. andPIRTTINIEMI, P. (2010) Cephalometric evaluation of children with nocturnal sleep-disordered breathing. European Journal of Orthodontics, 32(6), pp. 662-671.
PIRILÄ-PARKKINEN, K., PIRTTINIEMI, P., NIEMINEN, P., TOLONEN, U.,PELTTARI, U. and LÖPPÖNEN, H. (2009) Dental arch morphology in children withsleep-disordered breathing. European Journal of Orthodontics, 31(2), pp. 160-167.
PITEO, A.M., LUSHINGTON, K., ROBERTS, R.M., VAN DEN HEUVEL, C.J.,NETTELBECK, T., KOHLER, M.J., MARTIN, A.J. and KENNEDY, J.D. (2011)Prevalence of snoring and associated factors in infancy. Sleep Medicine, 12(8):787-792.
PRAUD, J.P. and DORION, D. (2008) Obstructive sleep disordered breathing inchildren: beyond adenotonsillectomy. Pediatric Pulmonology, 43(9), pp. 837-843.

79
PUNJABI, N.M., SHAHAR, E., REDLINE, S., GOTTLIEB, D.J., GIVELBER, R.,RESNICK, H.E. and SLEEP HEART HEALTH STUDY INVESTIGATORS (2004) Sleep-disordered breathing, glucose intolerance, and insulin resistance: the Sleep HeartHealth Study. American Journal of Epidemiology, 160(6), pp. 521-530.
REDLINE, S., TISHLER, P.V., SCHLUCHTER, M., AYLOR, J., CLARK, K. andGRAHAM, G. (1999) Risk factors for sleep-disordered breathing in children.Associations with obesity, race, and respiratory problems. American Journal ofRespiratory and Critical Care Medicine, 159, pp. 1527-1532.
REID, C.S., PYERITZ, R.E., KOPITS, S.E., MARIA, B.L., WANG, H., MCPHERSON,R.W., HURKO, O., PHILLIPS, J.A.,3rd and ROSENBAUM, A.E. (1987)Cervicomedullary compression in young patients with achondroplasia: value ofcomprehensive neurologic and respiratory evaluation. The Journal of Pediatrics, 110(4),pp. 522-530.
ROBISON, J.G. and OTTESON, T.D. (2011) Increased prevalence of obstructive sleepapnea in patients with cleft palate. Archives of Otolaryngology--Head & Neck Surgery,137(3), pp. 269-274.
ROSEN, C.L., LARKIN, E.K., KIRCHNER, H.L., EMANCIPATOR, J.L., BIVINS, S.F.,SUROVEC, S.A., MARTIN, R.J. and REDLINE, S. (2003) Prevalence and risk factorsfor sleep-disordered breathing in 8- to 11-year-old children: association with race andprematurity. Journal of Pediatrics, 142, pp. 383-389.
ROSEN, C.L., PALERMO, T.M., LARKIN, E.K. and REDLINE, S. (2002) Health-relatedquality of life and sleep-disordered breathing in children. Sleep, 25(6), pp. 657-666.
ROSS, K.R. and ROSEN, C.L. (2014) Sleep and respiratory physiology in children.Clinics in Chest Medicine, 35(3), pp. 457-467.
SAARI, A., SANKILAMPI, U., HANNILA, M.L., KIVINIEMI, V., KESSELI, K. andDUNKEL, L. (2011) New Finnish growth references for children and adolescents aged0 to 20 years: Length/height-for-age, weight-for-length/height, and body mass index-for-age. Annals of Medicine, 43(3), pp. 235-248.
SAKELLAROPOULOU, A.V., HATZISTILIANOU, M.N., EMPORIADOU, M.N.,AIVAZIS, V.T., GOUDAKOS, J., MARKOU, K. and ATHANASIADOU-PIPEROPOULOU, F. (2012) Association between primary nocturnal enuresis andhabitual snoring in children with obstructive sleep apnoea-hypopnoea syndrome.Archives of Medical Science 8(3), pp. 521-527.
SANCHEZ-ARMENGOL, A., FUENTES-PRADERA, M.A., CAPOTE-GILL, F.,GARCIA-DIAZ, E., CANO-GOMEZ, S., CARMONA-BERNAL, C. and CASTILLO-

80
GOMEZ, J. (2001) Sleep-related breathing disorders in adolescents aged 12 to 16years:clinical and polygrapgic findings. Chest, 119, pp. 1393-1400.
SANDELLA, D.E., O'BRIEN, L.M., SHANK, L.K. and WARSCHAUSKY, S.A. (2011)Sleep and quality of life in children with cerebral palsy. Sleep Medicine, 12(3), pp. 252-256.
SAUER, C., SCHLÜTER, B., HINZ, R. and GESCH, D. (2012) Childhood obstructivesleep apnea syndrome: an interdisciplinary approach: a prospective epidemiologicalstudy of 4,318 five-and-a-half-year-old children. Journal of Orofacial Orthopedics, 73(5)pp. 342-358.
SCHOLLE, S., WIATER, A. and SCHOLLE, H.C. (2011) Normative values ofpolysomnographic parameters in childhood and adolescence: cardiorespiratoryparameters. Sleep Medicine, 12(10), 988-96.
SECTION ON PEDIATRIC PULMONOLOGY, SUBCOMMITTEE ONOBSTRUCTIVE SLEEP APNEA SYNDROME. AMERICAN ACADEMY OFPEDIATRICS (2002) Clinical practice guideline: diagnosis and management ofchildhood obstructive sleep apnea syndrome. Pediatrics, 109(4), pp. 704-712.
SIEGEL, J.M. (2011) REM sleep, in Kryger, M.H., Roth, T. and Dement, W.C. (eds.)Principles and Practice of Sleep Medicine, 5th ed., Elsevier Saunders, St. Louis, Missouripp. 92-111.
SILVESTRI, R., GAGLIANO, A., ARICO, I., CALARESE, T., CEDRO, C., BRUNI, O.,CONDURSO, R., GERMANO, E., GERVASI, G., SIRACUSANO, R., VITA, G. andBRAMANTI, P. (2009) Sleep disorders in children with Attention-Deficit/Hyperactivity Disorder (ADHD) recorded overnight by video-polysomnography. Sleep Medicine, 10(10), pp. 1132-1138.
SINHA, D. and GUILLEMINAULT, C. (2010) Sleep disordered breathing in children.The Indian Journal of Medical Research, 131, pp. 311-320.
SMITH, D.L., GOZAL, D., HUNTER, S.J., PHILBY, M.F., KAYLEGIAN, J. andKHEIRANDISH-GOZAL, L. (2016) Impact of sleep disordered breathing onbehaviour among elementary school-aged children: a cross-sectional analysis of alarge community-based sample. European Respiratory Journal, doi:10.1183/13993003.00808-2016. [Epub ahead of print]
SMITH, C.B., WALKER, K., BADAWI, N., WATERS, K.A. and MACLEAN, J.E. (2014)Impact of sleep and breathing in infancy on outcomes at three years of age for childrenwith cleft lip and/or palate. Sleep, 37(5), pp. 919-925.

81
SOUZA, J.F., GRECHI, T.H., ANSELMO-LIMA, W.T., TRAWITZKI, L.V. andVALERA, F.C. (2013) Mastication and deglutition changes in children with tonsillarhypertrophy. Brazilian Journal of Otorhinolaryngology, 79(4), pp. 424-428.
SOYLU, E., SOYLU, N., YILDIRIM, Y.S., POLAT, C. and SAKALLIOGLU, O. (2013)The prevelance of psichiatric symptoms in preschool children with adenotonsillarhypertrophy. International Journal of Pediatric Otorhinolaryngology, 77(7), pp. 1094-1098.
SPIER, S., RIVLIN, J., ROWE, R.D. and EGAN, T. (1986) Sleep in Pierre Robinsyndrome. Chest, 90(5), pp. 711-715.
SPILSBURY, J.C., STORFER-ISSER, A., ROSEN, C.L. and REDLINE, S. (2015)Remission and incidence of obstructive sleep apnea from middle childhood to lateadolescence. Sleep, 38(1), pp. 23-29.
STOOHS, R.A., KNAACK, L., BLUM, H.C., JANICKI, J. and HOHENHORST, W.(2008) Differences in clinical features of upper airway resistance syndrome, primarysnoring, and obstructive sleep apnea/hypopnea syndrome. Sleep Medicine, 9(2), pp.121-128.
SURI, J.C., SEN, M.K., VENKATACHALAM, V.P., BHOOL, S., SHARMA, R., ELIAS,M. and ADHIKARI, T. (2015) Outcome of adenotonsillectomy for children with sleepapnea. Sleep Medicine, 16(10), pp. 1181-1186.
TAK, M., NAGARAJAPPA, R., SHARDA, A.J., ASAWA, K., TAK, A., JALIHAL, S.and KAKATKAR, G. (2013) Prevalence of malocclusion and orthodontic treatmentneeds among 12-15 years old school children of Udaipur, India. European Journal ofDentistry, 7(Suppl 1), pp. S45–S53.
TAUMAN, R., IVANENKO, A., O'BRIEN, L.M. and GOZAL, D. (2004) Plasma C-reactive protein levels among children with sleep-disordered breathing. Pediatrics,113(6), pp. e564-9.
THILANDER, B., PENA, L., INFANTE, C., PARADA, S.S. and DE MAYORGA, C.(2001) Prevalence of malocclusion and orthodontic treatment need in children andadolescents in Bogota, Colombia. An epidemiological study related to different stagesof dental development. European Journal of Orthodontics, 23(2), pp. 153-167.
TSAOUSSOGLOU, M., HATZINIKOLAOU, S., BALTATZIS, G.E., LIANOU, L.,MARAGOZIDIS, P., BALATSOS, N.A., CHROUSOS, G. and KADITIS, A.G. (2014)Expression of leukotriene biosynthetic enzymes in tonsillar tissue of children withobstructive sleep apnea: a prospective nonrandomized study. JAMA Otolaryngology--Head & Neck Surgery, 140(10), pp. 944-950.

82
URSCHITZ, M.S., BROCKMANN, P.E., SCHLAUD, M. and POETS, C.F. (2010)Population prevalence of obstructive sleep apnoea in a community of German thirdgraders. European Respiratory Journal, 36(3) pp. 556-568.
VAHER, H., KASENÕMM, P., VASAR, V. and VELDI, M. (2013) A survey ofparentally reported sleep health disorders in Estonian 8-9 year old children. BMCPediatrics, 13 pp. 200.
VALERA, F.C., TRAVITZKI, L.V., MATTAR, S.E., MATSUMOTO, M.A., ELIAS, A.M.and ANSELMO-LIMA, W.T. (2003) Muscular, functional and orthodontic changes inpre school children with enlarged adenoids and tonsils. International Journal of PediatricOtorhinolaryngology, 67(7), pp. 761-770.
VAN EYCK, A., VAN HOORENBEECK, K., DE WINTER, B.Y., RAMET, J., VANGAAL, L., DE BACKER, W. and VERHULST, S.L. (2014) Sleep-disordered breathingand C-reactive protein in obese children and adolescents. Sleep & Breathing, 18(2), pp.335-340.
VENÄLÄINEN, T.M., VIITASALO, A.M., SCHWAB, U.S., ELORANTA, A-M.,HAAPALA, E.A., JALKANEN, H.P., DF DE MELLO, V., LAAKSONEN, D.E., LINDI,V., ÅGREN, J.J. and LAKKA, T.A. (2016) Effect of a 2-y dietary and physical activityintervention on plasma fatty acid composition and estimated desaturase and elongaseactivities in children: the Physical Activity and Nutrition in Children Study. AmericanJournal of Clinical Nutrition, 104, pp. 1–9.
VERHULST, S.L., VAN GAAL, L., DE BACKER, W. and DESAGER, K. (2008) Theprevalence, anatomical correlates and treatment of sleep-disordered breathing inobese children and adolescents. Sleep Medicine Reviews, 12(5), pp. 339-346.
VIG, K.W. (1998) Nasal obstruction and facial growth: the strength of evidence forclinical assumptions. American Journal of Orthodontics and Dentofacial Orthopedics,113(6), pp. 603-611.
VIITASALO, A., ELORANTA, A-M., LINTU, N., VÄISTÖ, J., VENÄLÄINEN, T.,KIISKINEN, S., KARJALAINEN, P., PELTOLA, J., LAMPINEN, E.K., HAAPALA,E.A., PAANANEN, J., SCHWAB, U., LINDI, V., and LAKKA, T.A. (2016) The effectsof a 2-year individualized and family-based lifestyle intervention on physical activity,sedentary behavior and diet in children. Preventive Medicine 2016 87, pp. 81-8. doi:10.1016/j.ypmed.2016.02.027.
VILLA, M.P., MIANO, S. and RIZZOLI, A. (2012) Mandibular advancement devicesare an alternative and valid treatment for pediatric obstructive sleep apnea syndrome.Sleep & Breathing, 16(4), pp. 971-976.

83
VUORELA, N., SAHA, M.T. and SALO, M. (2009) Prevalence of overweight andobesity in 5- and 12-year-old Finnish children in 1986 and 2006. Acta Paediatrica, 98(3),pp. 507-512.
VUORELA, N., SAHA, M.T. and SALO, M.K. (2011) Change in prevalence ofoverweight and obesity in Finnish children - comparison between 1974 and 2001. ActaPaediatrica, 100(1), pp. 109-115.
VÄISTÖ, J., ELORANTA, A.M., VIITASALO, A., TOMPURI, T., LINTU, N.,KARJALAINEN, P., LAMPINEN, E.K., ÅGREN, J., LAAKSONEN, D.E., LAKKA,H.M., LINDI, V. and LAKKA, T.A. (2014) Physical activity and sedentary behaviourin relation to cardiometabolic risk in children: cross-sectional findings from thePhysical Activity and Nutrition in Children (PANIC) Study. The International Journalof Behavioral Nutrition and Physical Activity, 11, pp. 55-5868-11-55.
WALTER, L.M., NISBET, L.C., NIXON, G.M., DAVEY, M.J., ANDERSON, V.,TRINDER, J., WALKER, A.M. and HORNE, R.S. (2013) Seasonal variability inpaediatric obstructive sleep apnoea. Archives of Disease in Childhood, 98(3), pp. 208-210.
WANG, R.C., ELKINS, T.P., KEECH, D., WAUQUIER, A. and HUBBARD, D. (1998)Accuracy of clinical evaluation in pediatric obstructive sleep apnea. Otolaryngology--Head and Neck Surgery, 118(1), pp. 69-73.
WATERS, K.A., MAST, B.T., VELLA, S., DE LA EVA, R., O'BRIEN, L.M., BAILEY, S.,TAM, C.S., WONG, M. and BAUR, L.A. (2007) Structural equation modeling of sleepapnea, inflammation, and metabolic dysfunction in children. Journal of Sleep Research,16(4), pp. 388-395.
WEI, J.L., MAYO, M.S., SMITH, H.J., REESE, M. and WEATHERLY, R.A. (2007)Improved behavior and sleep after adenotonsillectomy in children with sleep-disordered breathing. Archives of Otolaryngology - Head and Neck Surgery, 133(10), pp.974-979.
XU, Z., CHEUK, D.K. and LEE, S.L. (2006) Clinical evaluation in predicting childhoodobstructive sleep apnea. Chest, 130(6), pp. 1765-1771.
ZAROWSKI, M., M ODZIKOWSKA-ALBRECHT, J. and STEINBORN, B. (2007) Thesleep habits and sleep disorders in children with headache. Advances in MedicalSciences, 52(Suppl 1), pp.194-196.
ZAUTNER, A.E. (2012) Adenotonsillar disease. Recent Patents on Inflammation &Allergy Drug Discovery, 6(2), pp. 121-129.

84
ZHANG, G., SPICKETT, J., RUMCHEV, K., LEE, A.H. and STICK, S. (2004) Snoringin primary school children and domestic environment: a Perth school based study.Respiratory Research, 5, pp. 19.
ZHU, Y., AU, C.T., LEUNG, T.F., WING, Y.K., LAM, C.W. and LI, A.M. (2013) Effectsof passive smoking on snoring in preschool children. The Journal of Pediatrics, 163(4),pp. 1158-1162.
ZINTZARAS, E. and KADITIS, A.G. (2007) Sleep-disordered breathing and bloodpressure in children: a meta-analysis. Archives of Pediatrics & Adolescent Medicine,161(2), pp. 172-178.

APPENDIX


PANIC-STUDY
Child’s sleep questionnaireThe questionnaire is filled by either one of the parents
1. How many hours does your child sleep in the night on average____________(½ hour accuracy rate)
2. How quickly does your child fall asleep after going to bed?(1) within 10 minutes or faster(2) within 10-20 minutes(3) within 30 minutes or more
3. How does your child sleep after falling asleep?(1) very peaceful(2) quite peaceful(3) partly peaceful, partly restless(4) quite restless(5) very restless
4. How many times your child awakens during the night?(1) none(2) once(3) twice(4) 3-4 times(5) at least 5 times
5. Is your child usually sleepy during daytime?(1) never or less than once a month(2) less than once a week(3) in 1-2 days a week(4) in 3-5 days a week(5) in 6 days a week or daily
6. How often have your child taken naps during the day during last 3 months?(1) never(2) less than once a week(3) in 1-2 days a week(4) in 3-5 days a week(5) in 6 days a week or daily
7. Does your child seem during daytime more tired compared to the otherchildren at same age?
(1) no, clearly more lively(2) no, quite more lively

(3) no difference(4) yes, quite more tired(5) yes, clearly more tired
8. Does your child have obsessional tendency to fall asleep?(1) never(2) less than once a week(3) in 1-2 days a week(4) in 3-5 days a week(5) in 6 days a week or daily
9. Have your child suffered from insomnia during last 3 months?(1) never(2) less than once a week(3) in 1-2 nights a week(4) in 3-5 nights a week(5) in 6 nights a week or every night
10. Does your child grind teeth during sleep?(1) never(2) less than once a week(3) in 1-2 nights a week(4) in 3-5 nights a week(5) in 6 nights a week or every night
11. Does your child suffer headache in the mornings?(1) never(2) less than once a week(3) in 1-2 mornings a week(4) in 3-5 mornings a week(5) in 6 mornings a week or every morning
12. Have your child had frightening dreams during last 3 months?(1) never(2) less than once a week(3) in 1-2 nights a week(4) in 3-5 nights a week(5) in 6 nights a week or every night
13. Have your child had sleepwalking or talking during sleep during last 3months?
(1) never(2) less than once a week(3) in 1-2 nights a week(4) in 3-5 nights a week(5) in 6 nights a week or every night

14. Does your child usually have blocked nose in the evenings or in the nights?(1) never(2) less than once a week(3) in 1-2 nights a week(4) in 3-5 nights a week(5) in 6 nights a week or every night
15. Have your child had tonsillitis or does she/he often complain of sore throat?(1) never(2) 1-2 times in all(3) 3-5 times in all or 1-2 times during one year(4) 3-5 times in a year(5) more than 5 times in a year
16. Have your child had ear infections?(1) never(2) 1-2 times in all(3) 3-5 times in all or 1-2 times during a year(4) 3-5 times in a year(5) more than 5 times in year
17. Have your child undergone tonsillectomy or/and adenoidectomy?(1) yes, both(2) yes, tonsillectomy(3) yes, adenoidectomy(4) no
18. Does your child breathe through the mouth at night?(1) never(2) rarely(3) sometimes(4) usually(5) always or almost always
19. Have you noticed any pauses in your child’s breathing pattern during sleep?(1) no(2) rarely(3) sometimes(4) usually(5) always or almost always
20. How do you describe your child’s snoring best?(1) no snoring(2) snores rarely(3) snores in certain position(4) snores most of the sleeping time

(5) snores frequently21. How loudly does your child snore?
(1) no snoring(2) low(3) quite loudly(4) loudly(5) extremely loudly
22. How do you describe your child’s snoring compared to the situation a yearago?
(1) much lower(2) lower(3) almost the same(4) some worse(5) much worse


DIS
SE
RT
AT
ION
S | T
IINA
IKÄ
VA
LK
O | P
ED
IAT
RIC
SL
EE
P D
ISO
RD
ER
ED
BR
EA
TH
ING
– CA
US
ES
AN
D... | N
o 373
uef.fi
PUBLICATIONS OF THE UNIVERSITY OF EASTERN FINLAND
Dissertations in Health Sciences
ISBN 978-952-61-2247-2ISSN 1798-5706
Dissertations in Health Sciences
PUBLICATIONS OF THE UNIVERSITY OF EASTERN FINLAND
TIINA IKÄVALKO
PEDIATRIC SLEEP DISORDERED BREATHING – CAUSES AND CONSEQUENCES
The aim of this doctoral thesis was to investigate the risk factors, diagnostic
method and consequences of pediatric sleep disordered breathing (SDB) in a population
sample of children from the Physical Activity and Nutrition in Children (PANIC) Study. The results showed that dentofacial and
pharyngeal morphology but not excess body fat raises the risk for SDB among 7-year-olds. Certain morphological and functional features at the age of 7 years may predict
developing SDB at the age of 10 years. SDB associates with low psychological well-being
in boys aged 7-year.
TIINA IKÄVALKO

![[XLS]kuk.results.tripod.comkuk.results.tripod.com/BTECH1C.xls · Web viewSurender Tinku 05 sdb 352 05 sdb 120 05 sdb 395 05 sdb 433 05 sdb 467 05 sdb 458 05 sdb 359 05 sdb 370 05](https://img.pdfslide.us/doc/110x75/5ae703757f8b9aee078da099/xlskuk-viewsurender-tinku-05-sdb-352-05-sdb-120-05-sdb-395-05-sdb-433-05-sdb.jpg)