Embed Size (px)
Citation preview
A CLINICAL STUDY ON SURGICAL MANAGEMENT
OF FRACTURE SHAFT OF FEMUR WITH
INTRAMEDULLARY INTERLOCKING NAIL
DISSERTATION SUBMITTED TO
UNIVERSITY OF SEYCHELLES
AMERICAN INSTITUTE OF MEDICINE
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE
DEGREE
M.Ch (Orthopaedic Surgery)
Submitted by
Dr. AKASH SABHARWAL
CERTIFICATE BY THE CANDIDATE
I certify that this dissertation is the result of my three
years of study, record and follow up of the cases during
private practice carried out under the guidance and
supervision of Dr. K.B. Raj, M.S. Ortho, Senior
Consultant Orthopaedic Surgeon of Shree Jeewan
Hospital, NewDelhi and prepared in fulfillment to the
requirement of M.Ch. Certification Program In
Orthopaedic Surgery in accordance with standards and
guidelines set by the University of Seychelles, American
Institute of Medicine (USAIM) and Boolean Education. I
undertake that the thesis is original and that no
copyrights have been infringed upon.
Date :01/11/11 Dr. Akash Sabharwal
ABSTRACT
Background
Orthopaedic surgeons often encounter diaphyseal femur fractures, because
these fracture most often result from high-energy trauma, one must have high index of
suspicion for complications. Currently surgery is indicated for most femur fractures
because of high rate of union, low rate of complications and advantage of early
stabilization which decreases the morbidity and mortality rate in patients. While the
main stay of the treatment has been reamed interlocking intramedullary nailing.
Methods
We studied a total of 20 patients of fracture shaft of femur admitted in the
Orthopaedic Department of Shree Jeewan Hospital, New Delhi treated with reamed
femur intramedullary interlocking nailing. The common age group was ranging from
20 to 71 yrs with average age group of 36 yrs. 16 patients were males, 4 were females.
13 patients had closed fracture, 5 had Gustillo Anderson Grade I compound and 2 had
Grade II compound fracture. In 11 patients fracture was at M/3rd
, in 5 patients it was
at L/3rd
level and in 4 patients it was at U/3rd
level. 2 patients were operated by open
interlocking nail and other 18 by closed technique using C-arm.
Results
Injury surgery interval was 6.20 days on an average. Mean time for union was
more in patients treated by open procedure(20 weeks) as compared to closed
technique (18.35 weeks). We found 1 patient developed superficial infection, which
healed completely and 1 had deep infection with nonunion. In our series of 20
patients, 12 patients had excellent results, 6 patients had good results, 1 fair result and
1 poor result.
Conclusions
Interlocking intramedullary nailing is a very effective and successful method
of definitive primary treatment, in most types of fractures of the shaft of the femur. It
is effective in controlling rotational and longitudinal forces that act across the fracture
site. Interlocking nail provides strong fixation, rotational stability and earliest return
to functional status, as the rate of healing is good with this method. It allows early
weight bearing and reduced rehabilitation.
Key words: Femoral shaft fractures; reamed femoral intramedullary interlocking
nailing.
ABBREVIATIONS
Yrs. : Years
M : Male
F : Female
U\3rd
: Upper third
P\3rd
: Proximal third
M\3rd
: Middle third
L\3rd
: Lower third
D\3rd
: Distal third
Comm. : Comminution
MVA : Motor vehicular accidents
RTA : Road traffic accident
Asso. Injury : Associated injury
Proc. : Procedure
ORIF : Open reduction and internal fixation
CRIF : Closed reduction and internal fixation
R.O.M. : Range of movement
Pre op : Pre operative
Post op : Post operative
AP : Antero-posterior
Lat : Lateral
Trans. : Transverse
L : Left
R : Right
LLD : Limb length discrepancy
FWB : Full weight bearing
PWB : Partial weight bearing
NWB : Non weight bearing
INDEX
Sl.
No. TOPICS
PAGE
NO.
1. Introduction 6
2. Aims and Objectives 11
3. Review of Literature 12
4. Materials and Methods 31
5. Observation and Results 43
6. Discussion 73
7. Conclusion 87
Bibliography 88
INTRODUCTION
Fractures of the shaft of the femur are commonly encountered in routine
orthopedic practice. As femur is the longest weight bearing bone in the body with
plenty of surrounding soft tissue envelope, they are usually fractured due to high-
energy trauma and fracture may result in prolonged morbidity and extensive disability
unless treatment is appropriate. Several techniques are now available for their
treatment.
They are challenging problems to treat, as there is usually comminution at the
fracture site and associated soft tissue injuries. In addition, there can be difficulty in
assessing malrotation at the fracture site. They can be life threatening, because of
open wounds, hemorrhagic shock, fat embolism, ARDS1 or multiple organ failure
2.
Further there may be physical impairment due to fracture shortening, malalignment,
and prolonged immobilization, due to traction or casting. This may lead to increased
morbidity.
So the aim of fracture treatment is to obtain union of the fracture, in as near
anatomical position, with minimal impairment of function. The spectrum of injury is
so great that no single method of treatment is relevant to all diaphyseal fracture femur.
The type and location of fracture, degree of comminution, age of the patient
and patients social and economic demands and other factors influence the method of
treatment. The technique chosen should cause minimal soft tissue and bone damage.
The goal should be to achieve anatomic alignment and early mobilization with
functional rehabilitation of limb.
Many modalities of treatment have evolved over the years for this fracture.
The method studied for this dissertation is Surgical Management of Fracture Shaft
of Femur with Intramedullary Interlocking Nail.
The history of femoral fracture management goes way back before the turn of
the century. Most of the treatments involved splinting or encasing the thigh with a
variety of materials. The early use in ancient civilization of wood splints wrapped
with sinews of leather or fibrous plants3
and various fabrics encased with wax4. This
had given way to bandages stiffened with gum5 and more recently fabrics hardened
with plaster of paris6. None of these methods offered sufficient strength to maintain
fracture alignment.
Femoral shaft fractures can be managed conservatively or surgically.
Conservative management in the form of skeletal traction followed by hip spica or
cast brace has limited indication. Since most patients are polytraumatized, it has
become essential to treat these patients surgically unless and until it is
contraindicated. The surgical treatment has gone into revolutionary changes over the
period of time and with advent of new antibiotics and better surgical procedures, even
open fractures can be fixed internally.
Internal fixation is done by different methods like:
Dynamic compression plate and screws
Intramedullary nailing with or without interlocking
Closed intramedullary nailing, introduced by G. B. Kuntscher in 19407, is
one of the methods of choice for treatment of short oblique or transverse fracture. He
presented his first case of intramedullary fixation using a V shaped cross section
designed nail in medical society of Kiel in 1939. Later he presented additional 12
cases treated by intramedullary fixation in german surgical society in berlin. Although
rotational stability is limited, can be achieved by interfragmentery interdigitation at
the fracture site. Thus this type of nailing is restricted to transverse and short oblique
fracture in the mid shaft. They do not offer adequate axial and rotational stability in
comminuted and unstable fractures.
Among all different methods of internal fixation, intramedullary fixation has
became popular during the last few decades, due to the following attributes :-
The nail provides internal stabilization along the axial line of forces; as nail
lies in the axis of femur.
Predictable realignment of bone.
Rapid regeneration of bone and union of fracture8,9
allows intermittent
dynamic axial compression with weight bearing, which promotes fracture
consolidation.
Early functional use of limb.
Prevention of excess dissection of fracture site and protection of surrounding
soft tissue envelope when done biologically, resulting in abundant callus with
less need for bone grafting.
Minimal potential for contamination.
Limitation of conventional intramedullary nail
Intramedullary nail cannot coincide with the shape of medullary canal.
Narrowing of the femur at isthmus.
Torsional forces are not controlled.
Anterolateral bowing of the femur not maintained.
It is used mainly in M\3rd diaphyseal fractures10
due to their limitation in
controlling short segment.
Advantages of interlocking nail over the conventional nailing
For best fitting of intramedullary nail, the concept of reaming was introduced.
Medullary canal can be broadened at the isthmus with reaming, so that larger
and thicker nail can be introduced. Flexible nails due their elastic recoil after
negotiating the isthmus, take the shape of the femur.
Torsional forces are controlled with static locking in interlocking nail.
The interlocking nail is curved, so that it matches the antero-lateral bowing of
femur.
When the segment is short, additional fixation can be achieved with 2 locking
screws in the neck of the femur for P\3rd
fracture (Reconstruction nail) and the
same for the D\3rd
fracture.
Thus interlocking femur provides
Near anatomical reduction.
Rigid fixation along the axial line of forces.
Minimum or no dissection at fracture site.
Rotational stability.
Minimal scarring.
Maintenance of limb length.
Minimal blood loss.
Low infection rate
The interlocking nail system combines the best of both i.e. not only does it
offer axial and rotational stability in comminuted and unstable fractures, but also
involves minimal interference with soft tissue around the bone11,8
especially when
introduced in a closed manner.
Interlocking nailing of femur has now become the treatment of choice in
almost all fractures, located between the lesser trochanter and femoral condyles,
regardless of the fracture pattern and degree of comminution.12,13
Our ultimate goal of femoral fracture management is restoration of alignment,
rotation and length, preservation of blood supply to aid union, prevention of infection
and early rehabilitation of the patient.
AIMS AND OBJECTIVES
1. To assess and study femoral diaphyseal fractures with special reference to
fracture anatomy, pattern and status of stability.
2. To assess the results obtained in the management of these fracture with
intramedullary interlocking nail and compare the results with other previously
done studies for treatment of fracture shaft femur with intramedullary nailing.
3. To evaluate the status of this technique and method in a moderate setup with
special emphasis on:
a. Time for radiological union
b. Period of hospitalization
c. Early mobilization
d. Period of weight bearing after nailing
REVIEW OF LITERATURE
Historically the management of fracture shaft femur has been complicated by
problems like malunion and non union. Before the turn of the century, fracture shaft
femur used to be treated with methods like splinting with wood splints wrapped with
leather or fibrous plants and various fabrics encased with wax or gum.
The introduction of Steinnman pin in 1907 changed overall management.
Skeletal traction was used to maintain length and alignment of fracture fragments.
First attempted internal fixation though unsuccessful was by Lapuyand and
Sirco in 1775
In 1897, Ronsohoff promoted open reduction internal fixation for irreducible
fractures.
Rush and Rush14
in 1939 reported the use of intramedullary pins for femur
fracture in United States.
Extensive research and development of intramedullary surgery was done by
Professor Gerhard Kuntscher7 in 1940. He was the first to develop a device as well
as a technique to internally fix femur shaft fractures, in 1950 he developed the
technique of medullary reaming and closed insertion of an intramedullary nail without
exposing the fractures. Kuntscher in 1968 proposed a new device for intramedullary
fixation of comminuted femoral fractures, Detensor Nail.
AO/ASIF15
group to develop internal fixation was formed in 1958. AO/ASIF
originally developed a thin walled flexible and partly slotted femoral intramedullary
nail with a clover leaf cross section and a slight curvature of the axis. The slot was
placed on the convex side.
Rokkanen et al16
1969 studied his cases by comparing open or closed nailing
with conservative treatment of fracture shaft femur. Showed that results of nailed
cases are far better than conservative management. In operated cases results of closed
nailing are better than open nailing. He emphasized need for closed nailing.
Klemm and Schelman1 in 1972 made the interlocking design following
which in 1974, Grosse and Kempf from france invented the GK interlocking nail.
The addition of interlocking screws to the nail as originally introduced by Klemm and
Schelman enhanced the properties of the intramedullary implant and widened the
range of indications.
Connolly et al17
1973 studied 143 femoral shaft fractures for close reduction
and early cast brace ambulation. Results were comparable to other conservative
methods. Showed 25% complication rate. Also showed close monitoring of transverse
and short oblique fractures of middle third shaft femur as they tend to displace in cast
brace.
Mooney et al18
1974 studied treatment of shaft femur with initial period of
sliding traction and once the fracture gums up case brace, was given and patient was
mobilised. This gave better functional results in the form of good knee range of
movements.
Steen Jensen et al19
1976 compared results of plating and nailing of femoral
shaft fractures. He reported frequency of non union, infection, implant failure more in
plating. Early weight bearing was possible in nailed group. Stressing need for using
intramedullary nailing.
Reis N. D. et al20
1977 studied different modalities of treatment in
infraisthmal fracture shaft femur. They showed need for additional derotation plate
along with simple intramedullary nail. Advocate use of AO compression plates for
these fractures to achieve near anatomical reduction. Also rules out role of
conservative treatment when surgery is not contraindicated.
Rothwell et al21
1978 showed the importance of complete instrumentation,
proper positioning of patient on table to improve results. Also observed the decreased
infection rate following closed nailing, so insisting closed nailing.
William Allen et al22
1978 studied the efficacy of fluted rod. It is longer in
torsion and bending thus allowing early mobilization. Effective in non union and
pathological fractures. No nail breakage reported. Anatomical reduction necessary
before nail insersion to avoid comminution during nailing.
Magerl et al23
1979 studied plating in treatment of femoral shaft fractures
showing comparable results. Documented need for interfragmentary compression,
rigid internal fixation, primary or early secondary bone grafting to reduce
complication rate. His study had high complication rate.
Aginski et al24
1979 describes effect of reaming and biomechanics of nailing.
Showed need for use of compression nailing. Reaming causes blocking of blood
supply causing ischemia of fracture fragments. So, reaming should be minimum.
Vacuum suction along with reaming reduces blocking of blood vessels and thus
reduces ischemia.
Seligson et al25
1979 showed increase rate of complications with use of pins
and plaster technique of treatment of fracture shaft femur like pin track infection,
shortening, angulation, malrotation and frequent hospitalization due to loss of
reduction.
Stephen Montgomery26
1981 described effect of roller traction in those
patients in whom surgery was contraindicated. Average healing time was 14 weeks
and complications comparable to other series & showed the need of patient
cooperation.
Kenneth Johnson at al27
1984 describes failure rate of 66% with roller
traction,39% with intramedullary nailing with circlage wires and 4% failure rate with
interlocking nailing. Proving superiority of interlocking nailing, this technique was
technically demanding so complete set up and instrumentation was required. Roller
traction and nailing with circlage wire has high results of nonunion malunion and
infection.
Winquist et al28
1984 showed 99.1% union rate. Advocates early nailing in
polytrauma patients. Showed need for adequate preoperative traction whenever
nailing was delayed, proper positioning on table and correct entry point through
piriformis fossa. Rotational forces were well controlled by interlocking nails.
Marion et al29
1985 demonstrated correct entry point for nailing of fracture
shaft femur. It was at the junction of neck femur and greater trochanter and just
anterior or in the piriformis fossa.
Marion Harper et al30
1985 showed that results of closed or open fluted
nailing were equal. Near anatomical reduction before insertion of nail to prevent
fracture comminution. Some of the cases need postoperative external splinting or
traction to prevent malunion, mostly in comminuted fractures.
Kempf Grosse et al1 1985 described locked intramedullary nails control
rotation and telescoping by locking nail with the bone. Closed nailing further
increased advantages of locking. Dynamisation was required before weight bearing.
Thoresen et al31
1985 described excellent result with Grosse Kempf nailing.
Static mode of interlocking was preferred over dynamic mode. Dynamic nailing could
not control rotational and longitudinal instability so high rate of malunion. Static
nailing did not delay fracture union which control rotational and longitudinal
instability effectively.
White et al32
1986 described excellent results with Brooker Willis with mean
healing union time of 4.4 months in 99% of cases. This nail has advantages of distal
and proximal locking through same incision proximally. Thus avoiding separate
incision for distal locking and additional radiational exposure that is used for distal
locking. Its rigidity was questionable intorsion and compression suggested by high
incidence of shortening and malunion in rotation.
Wiss et al13
1986 studied 112 comminuted fracture shaft femur treated with
Grosse Kempf nail with 98% union rate with low incidence of shortening, infection,
and malunion or non union. He reported that closed interlocking intramedullary
nailing had advantages over other methods of treatment. Also showed that immediate
stabilization allow early mobilization and thus good postoperative results.
Huckstep et al33
1986 showed excellent results with Huckstep nails even in
cases of non union. Advantages were made by titanium alloy an inert material,
minimum reaming required, locking screws hold rotation, and square cross section did
not disturb medullary blood supply. Full length of the nail was needed to be spanned.
It was much stronger than femur and other nails.
Brumback et al2 1988 to reduce error of decision he advised need for high
quality preoperative radiographs to analyse pattern of fracture and comminution and
also to detect intraoperative comminution of fracture due to reaming and nailing
which were indications for static locking. This prevents malunion. Dynamic locking
was reserved for transverse or short oblique fracture of shaft femur.
He also showed that static locking of intramedullary nails in femoral shaft
fractures did not appreciably inhibit the process of healing of the fracture and that
routine conversion to dynamic intramedullary fixation, although occasionally
necessary, need not be performed.
Christie et al34
1988 evaluated 50 cases of fracture shaft femur treated with
Brooker –Willis nail. Showed 26% of technical difficulties. These difficulties were
more in number in early period of series which reduced with experience. Difficulties
were more associated with supine position.
David Lhowe et al 198835
treated open fractures of the femoral shaft by
immediate nailing in 67 patients. 36% of grade I, 45% of grade II, and 12% of grade
III compound fractures. All fractures healed within four months after injury without
infection.
Donald Wiss et al 199036
recommended static locking of all segmental
fractures, with dynamic reserved for fractures which show minimal evidence of
bridging callus 16-20weeks post operatively.
Blumberg et al37
1990 compared Brooker-Willis nail versus Russel-Taylor
nail for technical difficulties. Difficulties were like inserting proximal or distal
locking screws or deploying fins. Showed that Russel-Taylor nail had less technical
difficulties, less operative time, less blood loss. Result of both group were similar.
Dana Covey et al38
1990 studied biomechanical properties and showed that
slotted nails are stronger in bending and weaker in torsion than non slotted nails
(comparing Brooker Willis nail with Russel Taylor nail)
Stambough et al 199139
retrospectively reviewed 99 cases of stable and
unstable femoral shaft fractures treated with GK intramedullary nails. Union rate was
99% with acceptable alignment. No incidence of deep infection was noted inspite of
16 open fractures. Non union was reported in 2 cases. They concluded that although
GK interlocking intramedullary fixation was technically demanding, they gave
excellent results in management of stable and unstable, open and closed fractures of
the femoral shaft.
Wu et al 199310
treated 35 segmented femoral fractures either with closed
intramedullary nails (most were Grosse-Kempf interlocking nails) or an open method
technique (most were open Kuntscher nails with supplementary wires). Follow up
period was one year. There was an 82.9% union rate and a union period of 6.1±1.9
months. The closed intramedullary nailing showed superiority to the old method
group. They concluded that closed Intramedullary nailing is better than open
treatment for segmental femoral shaft fractures.
Gregory et al 199640
treated 24 patients with ipsilateral fractures of femur and
tibia between 1989 and 1995. Both bones were fixed by intramedullary nailing. Femur
being fixed by retrograde insertion of femoral nail and tibia by unreamed insertion of
an interlocking tibial nail. Five femoral fractures and 14 tibial fractures were open.
Associated injuries were present in 18 of the 24 patients with injuries of pelvis and
head being most prevalent. Twenty patients with 22 extremities had sufficient follow
up at an average of 2 months. Both fractures in 14 extremities had healed or were
healing uneventfully at final review. Five additional operative procedures were
required in the three complicated femora (two nail dynamizations, one bone graft, and
two exchange nailing procedures). Thirteen additional operative procedures were
required in five complicated tibie (one nail dynamization, six debridement procedures,
five bone grafts. and one muscle flap) after the initial hospitalization. Functional
results were good or excellent in 13 of the 20 patients (65%) and 15 of the 22
extremities (68%) available at final review. No significant knee problem related to the
femoral nailing technique was identified.
Wu, Chang Gumng Memorial Hospital, Taiwan 199741
. Studied the effect
of dynamization over fracture healing in femur shaft fractures treated by interlocking
nailing. 28 static femoral interlocking nails were dynamized after 4 months, because
of poor fracture healing, 144 patients achieved a solid union with a union period of
5.2 +1- 2.0 months after dynamization. 21% of cases had more 2cms of shortening, all
occurred in cases of nonunion. He concluded that dynamization should be attempted
in cases of delayed union.
Clatworthy et al42
1998 studied effect of reaming. Reamed interlock
intramedullary nailing united faster than unreamed interlocking intramedullary
nailing. Also observed increased rate of implant failure associated with unreamed
interlocking intramedullary nailing.
George et al 199843
studied the optimal location of a single distal Interlocking
screw in intramedullary nailing of distal third femoral shaft fractures fixed by
intramedullary nail at the varying distance from osteotomy site of fiberglass femoral
model, 2.5cms, 5cms and 7.Scms. These models were subjected to axial, rotational
and bending displacement and measured through a transducer. They concluded that as
the distance of single distal interlocking in static I.M nail increased, it affected the
rotational stability but not axial or angular stability.
Interlocking nailing has now been used in comminuted and unstable fractures
of femur. Philip Hajek 199944
studied the torsional and compressive biochemical
characteristics of system of interlocking nails in 16 femora obtained from 8 cadavers.
No difference was found in torsional rigidity or axial load when one compared to two
distal screw had been used.
Furlong et al 199945
retrospectively studied exchange nailing for femoral
shaft aseptic non-unions. They reviewed 25 patients who had reamed exchange
femoral nailing for established aseptic non-unions. 24 patients (96%) united after
exchange nailing without the need for additional procedure. The mean time to union
was 29.27 weeks. The patients who had open bone grafting performed at the same
time tended to unite quicker. They believed that the nail type is less important than the
biological effect of reaming, bone grafting and dynamization. This study
demonstrated that reamed femoral nailing for aseptic femoral non-unions remains an
effective treatment.
Woimnky et al 199946
studied 551 fractures on 515 patients out of 882 cases
operated in their institute between 1986 and 1996. These patients had fracture of the
femoral shaft with interlocking nails inserted by closed techniques. They reported
union rate of 98.9%. Six cases of infection, one nail breakage and 13 locking bolts
breakage were reported. They concluded that reamed intramedullary nailing of
femoral shaft fracture results in low rate of non-union, mal-union, infection and
hardware failure.
Debrauwer et al 200047
treated 40 cases of femoral diaphyseal fractures
between March 1995 to December 1999 by antegrade femoral reamed interlocking
titanium alloy nail. 35 were closed fractures, 5 were open fractures. One was of Grade
I, Two of Grade II and three cases of Grade III (According to Gustilo’s classification).
The mean time for healing was 17.85 weeks (rage 18 to 50 weeks). They reported 3
cases of delayed union which united after dynamization. One malunion for which
corrective osteotomy was done. One case of non-union that healed after exchange
nailing.
Tornetta 200048
did a prospective randomized study to compare reamed
femoral nailing with unreamed femoral nailing. 170 patients with 172 femoral
fractures were randomized to an unreamed or reamed group. Intra-operative blood
loss was greater in the reamed group. The time to union was 80±35 days for reamed
and 109±62 for unreamed group. This difference was most dramatic in distal femoral
fractures with union in reamed group being 80 days when compared to 158 days in
unreamed group. They concluded that fractures treated with reamed nails healed faster
than those treated with unreamed nails, especially distal fractures.
Hak et al 200049
studied 23 patients with fractures non union femoral shaft
with reamed intra-medullary nail inside. All patients were treated by exchange reamed
femoral nailing. Diameter of the nail was 1-3 mm larger than the previous nail. Canal
was over reamed by 1 mm than the nail. All nails were statically locked. They
reported that exchange reamed femoral nailing was successful in 18 cases (78.3%). 3
patients had to undergo additional procedures for fracture union, tobacco was found to
be detrimental in fracture healing. All 8 non-smokers healed after exchange nailing
where as 10 of 15 smokers healed after exchange nailing.
Brumback and Virkus 200050
studied that all intramedullary nailing creates
some loss of endosteal blood supply and increase in intra-medullary pressure resulting
in marrow embolization. These effects although transient appeared more pronounced
with reamed than non-reamed technique. Femoral fractures treated with non-reamed
technique showed higher incidence of delayed union and non-union. They concluded
that reamed intramedullary interlocking fixation remains the treatment of choice for
femoral shaft fractures in adults.
Hossan Elshafie et al 200051
treated nine patients with ipsilateral fractures of
neck and shaft of the femur by Russell-Taylor reconstruction femoral nail. All
fractures healed. Average time for union for neck of femur is 4.2 months and shaft
fracture is 6.9 months. No cases of A.V.N or non-union of femoral neck fractures
were reported. One hip healed with mild virus deformity. One shaft had delayed
union. One case developed late infection of femoral shaft.
Tornetta and Tibruzi 200052
reported a prospective, randomized comparison
of antegrade and retrograde procedures in 60 patients with 69 fractures of the femoral
shaft. All nails were inserted after appropriate reaming. There was no difference in
operating time, blood loss, technical complications, size of the nail or reamer, or
transfusion requirements. There were more problems of length and rotation using a
retrograde technique on a radiolucent table than with an antegrade approach on a
fracture table. All fractures in both groups healed and there was no difference in the
time taken to achieve union. They concluded that, although retrograde nailing is a
promising technique the skills required need practice.
Momberger et al 200053
treated 50 femoral shaft fractures in adolescents with
reamed interlocking IM nails between 1991 to 1998. Patients were in age group 10-16
years (31 boys and 17 girls). They utilized greater trochanter as entry point. No
patients had angular or rotational deformities. No patients developed AVN of femoral
head. They concluded that IM nailing through greater trochanter as starting point is
safe and effective methods for femoral fracture treatment in adolescent’s age group.
Lin et al 200154
studied the stress analysis on the locking screw for femoral
interlocking nailing. The stresses on the locking screw were analyzed as a function of
the distances from the fracture to the locking screw in the distal fragment under two
situations one with cortical contact another without cortical contact in the distal
fragment. With nail cortical contact, the screw’s stress decreased with increase in the
length of nail cortical contact and the distance between the distal locking screw and
the fractures site. The screw stresses were much higher without nail cortical contact
than with contact and continued to increase as the nail was inserted further.
Arazi et al 200155
studied the effect of early weight bearing after statically
locked reamed IM nailing of comminuted femoral fractures. 30 cases were included
(Winquist type I, II, III, IV) and treated with static reamed interlocking nailing. 24
patients were followed up at least 1 year, early weight bearing was encouraged and
most of the patients would start between the first 2 and 4 weeks post operatively. All
fractures healed without Complications. No cases of nail bending or breakage were
reported. One case each was repeated in both proximal and distal locking screw
bending. They concluded that early weight bearing in static reamed ILN of Winquist
type II, III, IV femoral fractures is a safe and effective method.
Philahjmaki, Harri K, July 200256
studied 278 patients with 280 fractures
during 7 years period. To assess effectiveness of different surgical options in the
treatment of non-union of femoral shaft fractures after initial intramedullary nailing.
Out of 280 fractures non-union occurred in 35 fractures (12.5%). To achieve solid
union, one operation was sufficient in 25 fractures. Two surgeries in 6 fractures and 4
needed 3 operations. There were 5 patients with autogenous bone grafting alone. All 5
required further re-operation for non-union. 4 out of 17 patients required re-operation
after dynamization. After 8 cases of exchange nailing, 1 case required re-operation for
non-union. Solid union was achieved after 6 months of initial operation. They
concluded that exchange nailing without extra cortical bone grafting seems to be the
most effective method of treating disturbed union of femoral shaft fractures after
intramedullarq nailing. Autogenous extracortical bone grafting alone is insufficient
and dynamization predisposes to shortening of bone.
Nork Seon E, MD, Agel Julia et al, University of Mississipi, 200357
performed a retrospective study of 743 patients treated with reamed intramedullary
nailing of femoral shaft fractures was done to assess clinical impact of bilateral femur
fracture on mortality, hospital stay, length of intensive care. 689 patients had
unilateral injuries and 54 patients had bilateral injuries. Mortality in patients with
bilateral fractures was 5.6% compared to 1.5% in unilateral fracture patients. Of the
two groups, bilateral femur fractures were associated with higher mortality, longer
length of stay in hospital and longer stay in intensive care units compared with
patients with unilateral femur injuries.
Chen, Chin En, Kojih Young, 200358
treated 23 patients with infections after
intramedullary nailing of femoral fractures. All fractures were unhealed at
presentation. Patients were divided into 2 groups. Group-I (12 patients)
intramedullary nails were retained and in group-II (11 patients) intramedullary nails
were removed at the time of debridement and fractures were stabilized with external
fixators.
In group-I, all fractures healed within a average period of 9 months (5-15
months) in group-II 7 fractures healed with average of 10 months (range 4-24
months). Infected non-union was noted in 2 patients. More complications occurred in
group-II patients compared to group-I. They concluded that retention of
intramedullary nail is performed if the fixation is stable and infection is under control.
External fixation is suitable for uncontrollable osteomyelitis or infected non-union.
Schipper IB, Steyerborg EW et al, January 200459
studied treatment of
unstable proximal femoral fractures. By comparison of gamma-nail and proximal
femoral nail and found out that intraoperative blood loss was less with proximal
femoral nail (220 ml versus 287 ml, p=0.001). Postoperatively more lateral protrusion
of the hip screws of proximal femoral nail (7.6%) was documented compared with
gamma nail (1.6%, p=0.02). Functional outcome and consolidation were equal for
both implants.
Wolinsky, Philiph MD, University of California 200460
studied effect of
reamed intramedullary nailing and systemic inflammatory response. Stabilization of
the femoral shaft with reamed intramedullary nailing could cause complications in
certain subset of patients. Initially, it was though that patients with thoracic injuries
were at risk of complications. But this has been shown not to be the case. Current
thought is avoiding reamed intramedullary nailing in patients who have an over
stimulated immune system and/or who are under resuscitated. These patients could
react better to initial treatment with an external fixator with later conversion to
reamed intramedullary nailing.
T C Wong, 200461
indicated retrograde intramedullary nailing in patients who
have had an arthrodesis of the ipsilateral hip and suffer a femoral shaft fracture distal
to the implant in the hip.
Tigani, Fravisini, Stagni, Pascarella, Boriani, 200562
studied 175 closed
femoral shaft fractures to evaluate the effect of dynamization on time to bony
union.They concluded that time to union was significantly shorter in static group(103
days) compared to the dynamized group(126 days)
Meena RC, Kundnani V, Hussain Z, 200663
studied closed vs open
interlocking nailing for fracture shaft femur and concluded that open interlocking of
fracture of long bones can be applied at very basic level of Indian health infrastructure
where facilities of IITV and surgical expertise are still lacking.The results obtained by
them were comparable to closed nailing.
Ogbemudia, Enemudo, Edomwonyl, 200764
reported a case of closed
interlocked nailing of a fractured femur without X-ray guide in 1st trimester
pregnancy.They made a longitudinal anterolateral cortical window on the lateral
condyle of the femur and confirmation of the distal intramedullary placement of the
guide wire was made by visualizing the wire through the cortical window.
Wu Chia-Chieh, Yu Chen-Tung, Hsieh Chen-Pu, Chen Shih-Jen, Chang
Inglin, 200865
reported a case of femoral head avascular necrosis after open antegrade
interlocking nailing of proximal third femoral shaft fracture in a male adult.

CLASSIFICATION
There are number of classification systems, however no system is universally
accepted.
AO / ASIF classification -
AO /ASIF (Association for the study of Internal fixation) classification of
fractures of the shaft of the femur. Simple fractures (type A) are
distinguished by the degree of obliquity of the fracture line. Wedge
fractures (type B) are subclassified according to the anatomy of the
wedge fracture. Complex fractures (type C) can be spiral, segmental, or
irregular 69
A) Simple fracture Al - Simple spiral
A2 - Simple Oblique (300 or more)
A3 - Simple transverse
B) Wedge fractures B1 -Spiral wedge
B2 - Bending wedge
B3 - Fragmented wedge
C) Complex fractures C1 –Complex Spiral
i) With 2 intermediate fragments
ii) With 3 intermediate fragments
iii) With >3 intermediate fragments
C2 – Complex segmental
i) With 1 intermediate segment
ii) With 1 intermediate segment
and an additional wedge
fracture
iii) With 2 intermediate segments
C3 – Complex irregular
i) With 2 or 3 intermediate
fragments
ii) With shattering limited to <5cm
length of bone
iii) With shattering >5cm of bone
Figure -8: AO classification
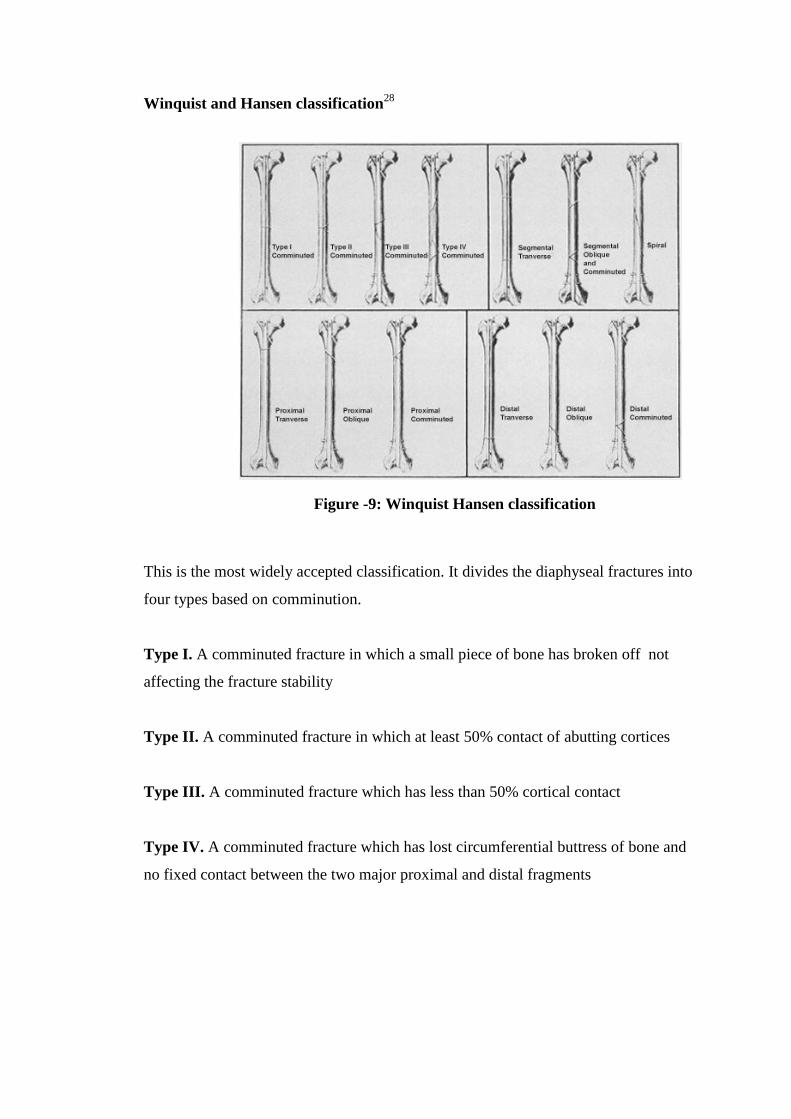
Winquist and Hansen classification28
This is the most widely accepted classification. It divides the diaphyseal fractures into
four types based on comminution.
Type I. A comminuted fracture in which a small piece of bone has broken off not
affecting the fracture stability
Type II. A comminuted fracture in which at least 50% contact of abutting cortices
Type III. A comminuted fracture which has less than 50% cortical contact
Type IV. A comminuted fracture which has lost circumferential buttress of bone and
no fixed contact between the two major proximal and distal fragments
Figure -9: Winquist Hansen classification
Depending on geometry of fracture line9
Transverse < 30o
Oblique > 30o
Spiral
Segmental
Wedge Butterfly fragment
Comminuted
OPEN FRACTURES - GUSTILLO ANDERSON’S CLASSIFICATION 70
Type I < 1cm wound on skin and clean wound
Type II > 1cm laceration on skin but is without extensive soft tissue damage,
skin flaps , or avulsions.
Type III
IIIA Soft tissue laceration or flaps but maintain adequate soft tissue
coverage of bone, or resulting from high energy trauma regardless of
the size of the wound
IIIB Extensive soft tissue loss with periosteal stripping and exposure of
bone with massive contamination.
IIIC Open fracture with arterial injury which requires repair regardless of
the size of the soft tissue wound
Depending on location
Proximal third
Mid shaft
Distal third
MATERIAL AND METHODS
This is a report of 20 cases of unstable fractures of the femur, treated at the
Orthopaedic Department of Shree Jeewan Hospital, New Delhi with closed
reamed intramedullary interlocking nail between. This includes a prospective study of
20 cases.
These cases of unstable fracture shaft femur were treated by femur
interlocking nail, which is locally available and is based on AO design nail with
proximal locking jig and two proximal and distal holes and one oblique proximal
locking hole.
Data is collected from the patients attending the orthopedic department with
fracture shaft of femur and satisfying the inclusion criteria.
Inclusion criteria
Fracture involving the diaphysis of femur
Grade I,II Gustillo Anderson compound fracture
Segmental fracture
Comminuted fracture (Winquest Hansen classification28
)
Exclusion criteria
Grade-III Gustillo Anderson compound fracture
Management in the casualty
1. Patient’s airway was assessed.
2. Breathing and circulation were assessed.
3. Other major injuries were ruled out.
4. To combat blood loss at the fracture site, IV fluids were started.
5. Limb was immobilized in Thomas splint or skeletal traction/skin traction was
given.
6. Analgesics, antibiotics, tetanus toxoid and blood transfusion were given as
needed.
In wards
1. Detailed history was taken about age, sex, occupation, mode of injury, past
history and associated medical illness.
2. Thorough clinical examination and general condition was assessed.
3. Associated orthopaedic and other systemic injuries were assessed and
managed accordingly.
4. X-rays are taken in 2 planes, AP and lateral including x-ray of ipsilateral hip
and knee joints
5. All the fractures were classified according to AO classification.

Preoperative assessment
Preoperatively the length of nail was measured
clinically and radiographically.
Clinically –The length was measured from the
tip of greater trochanter to the joint line and 20-
30 mm was deducted(on the normal side). Nails
of 1 size above and below the measured length
were kept ready.
Radiographically –The length was measured
from the tip of the greater trochanter to the
upper border of patella. Diameter of nail was
determined from the breadth of the medullary
canal at isthmus after substracting 15% of
radiological magnification.
Routine preoperative investigation assessment included.
• Haemoglobin percentage
• Urine for sugar, albumin and microscopy
• Recording of blood pressure
• BT, CT, RBS, Blood urea, Serum creatinine
• E.C.G.
• Radiological assessment.
o AP and lateral radiograph of thigh with hip and knee
o Chest PA/AP view – as a baseline radiograph to assess any
development of fat embolism later.
Rt. Femur AP
view
Rt. Femur Lat. view
Figure -13: X-ray right
femur AP and lateral
Preoperative Preparation
1. Patient were kept fasting for 8-10 hrs. before surgery
2. IV fluids were given as needed.
3. Adequate amount of blood bottles were kept ready after cross matching if
required post operatively.
4. IV antibiotic was given 30 min before surgery
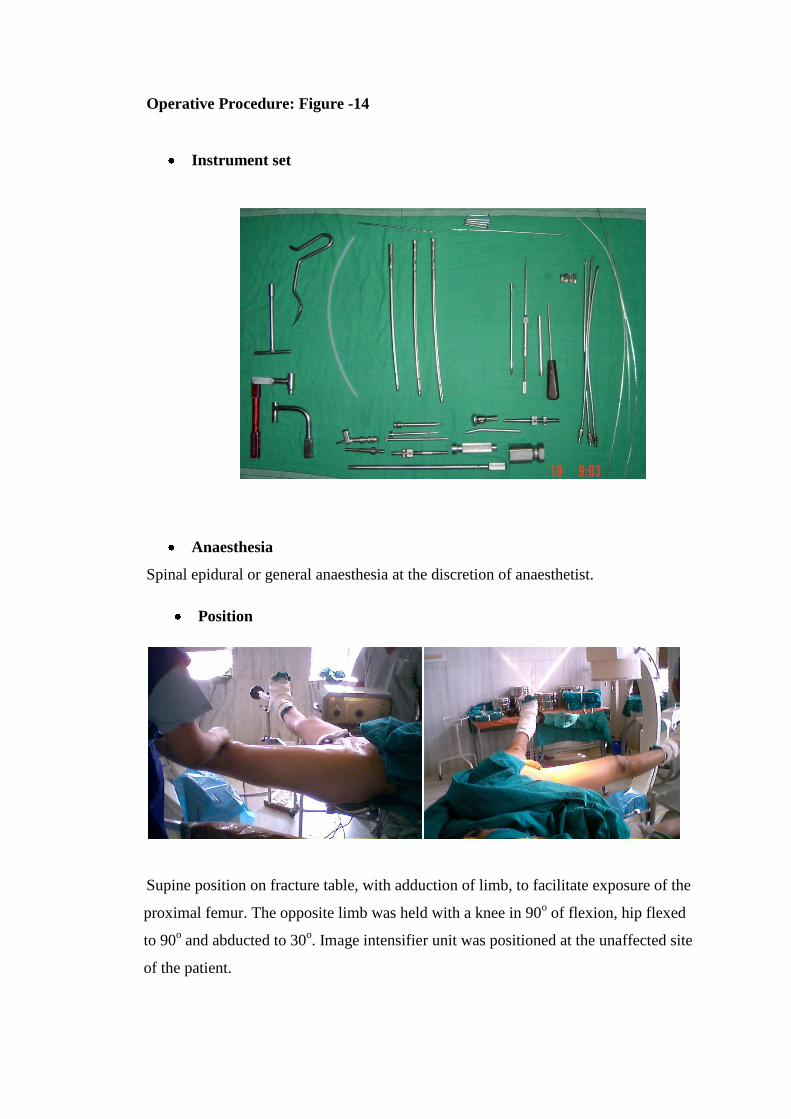
Operative Procedure: Figure -14
Instrument set
Anaesthesia
Spinal epidural or general anaesthesia at the discretion of anaesthetist.
Supine position on fracture table, with adduction of limb, to facilitate exposure of the
proximal femur. The opposite limb was held with a knee in 90o of flexion, hip flexed
to 90o and abducted to 30
o. Image intensifier unit was positioned at the unaffected site
of the patient.
Position
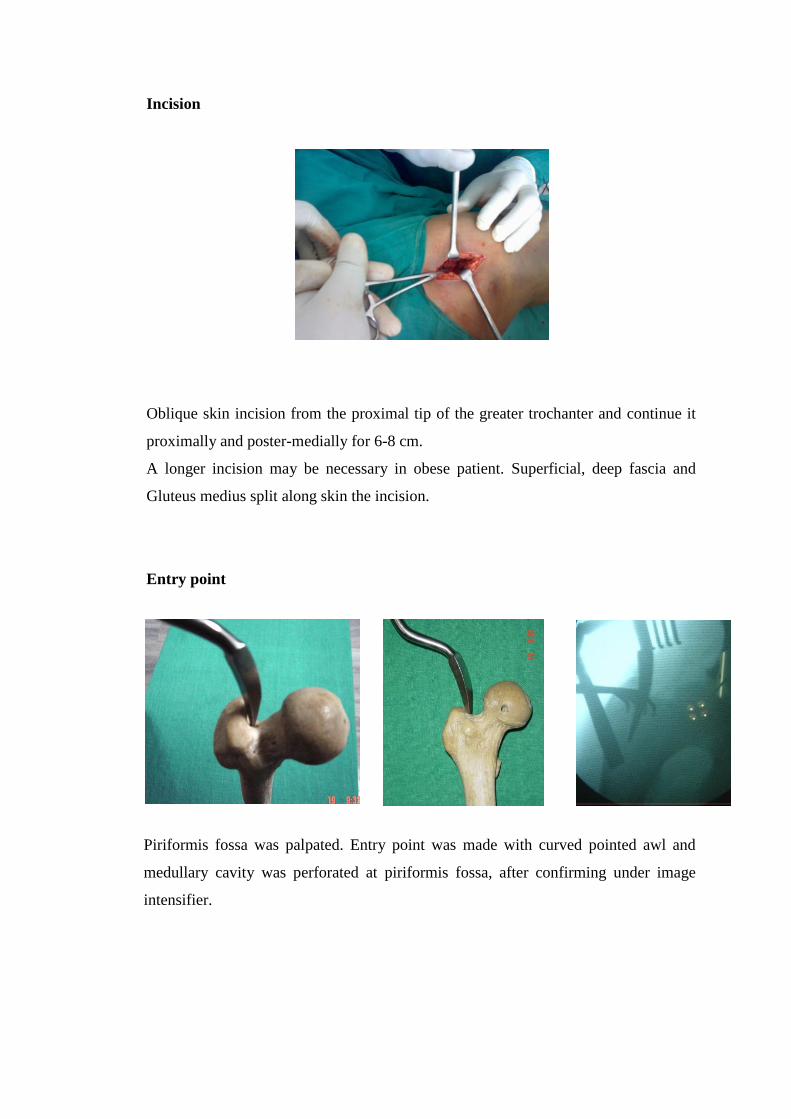
Incision
Oblique skin incision from the proximal tip of the greater trochanter and continue it
proximally and poster-medially for 6-8 cm.
A longer incision may be necessary in obese patient. Superficial, deep fascia and
Gluteus medius split along skin the incision.
Entry point
Piriformis fossa was palpated. Entry point was made with curved pointed awl and
medullary cavity was perforated at piriformis fossa, after confirming under image
intensifier.
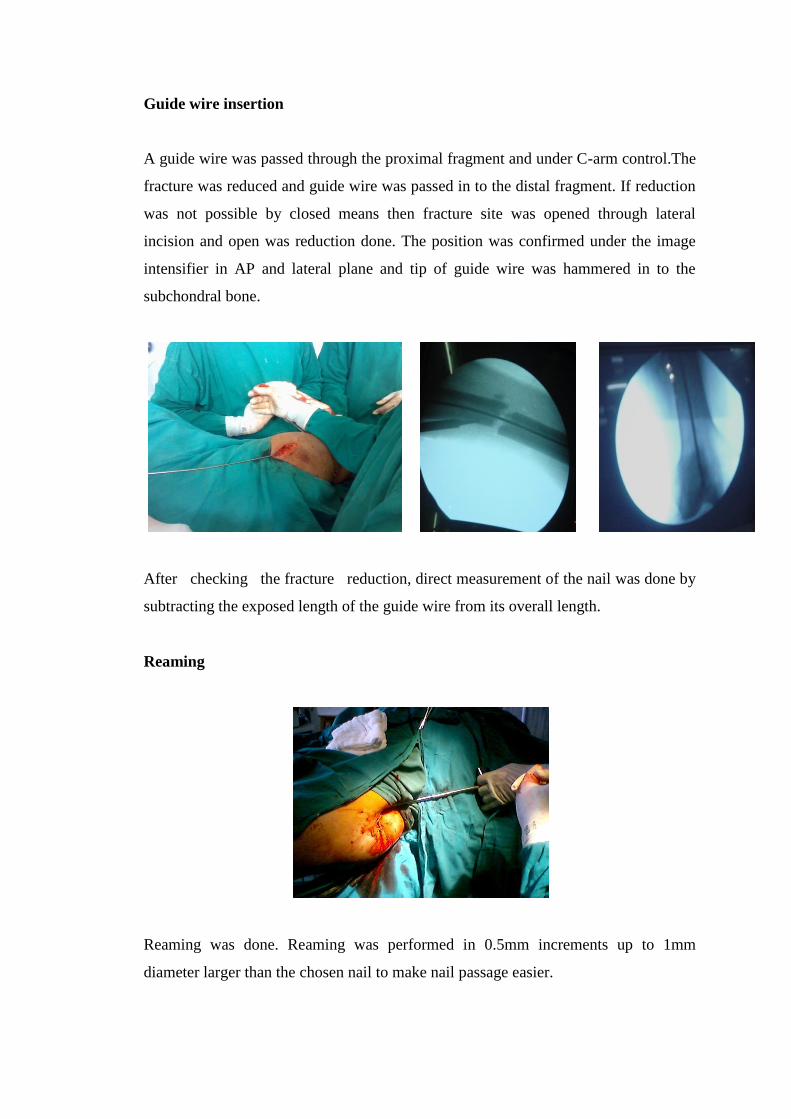
Guide wire insertion
A guide wire was passed through the proximal fragment and under C-arm control.The
fracture was reduced and guide wire was passed in to the distal fragment. If reduction
was not possible by closed means then fracture site was opened through lateral
incision and open was reduction done. The position was confirmed under the image
intensifier in AP and lateral plane and tip of guide wire was hammered in to the
subchondral bone.
After checking the fracture reduction, direct measurement of the nail was done by
subtracting the exposed length of the guide wire from its overall length.
Reaming
Reaming was done. Reaming was performed in 0.5mm increments up to 1mm
diameter larger than the chosen nail to make nail passage easier.
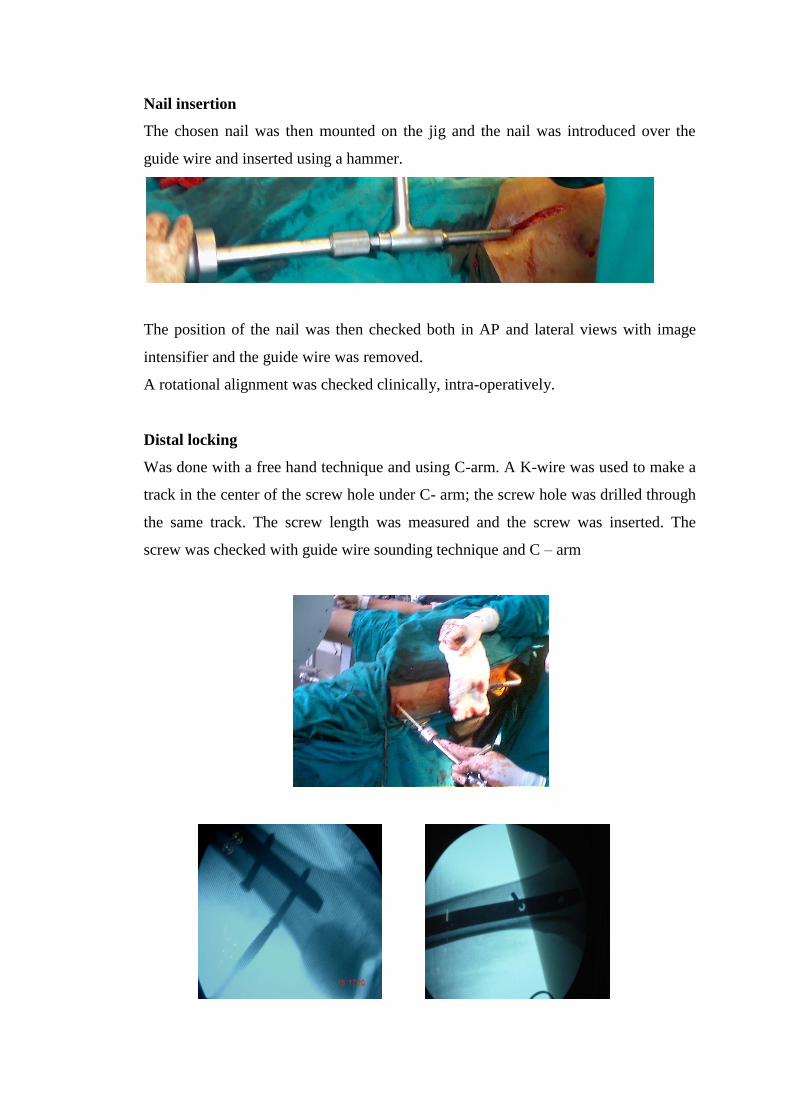
Nail insertion
The chosen nail was then mounted on the jig and the nail was introduced over the
guide wire and inserted using a hammer.
The position of the nail was then checked both in AP and lateral views with image
intensifier and the guide wire was removed.
A rotational alignment was checked clinically, intra-operatively.
Distal locking
Was done with a free hand technique and using C-arm. A K-wire was used to make a
track in the center of the screw hole under C- arm; the screw hole was drilled through
the same track. The screw length was measured and the screw was inserted. The
screw was checked with guide wire sounding technique and C – arm
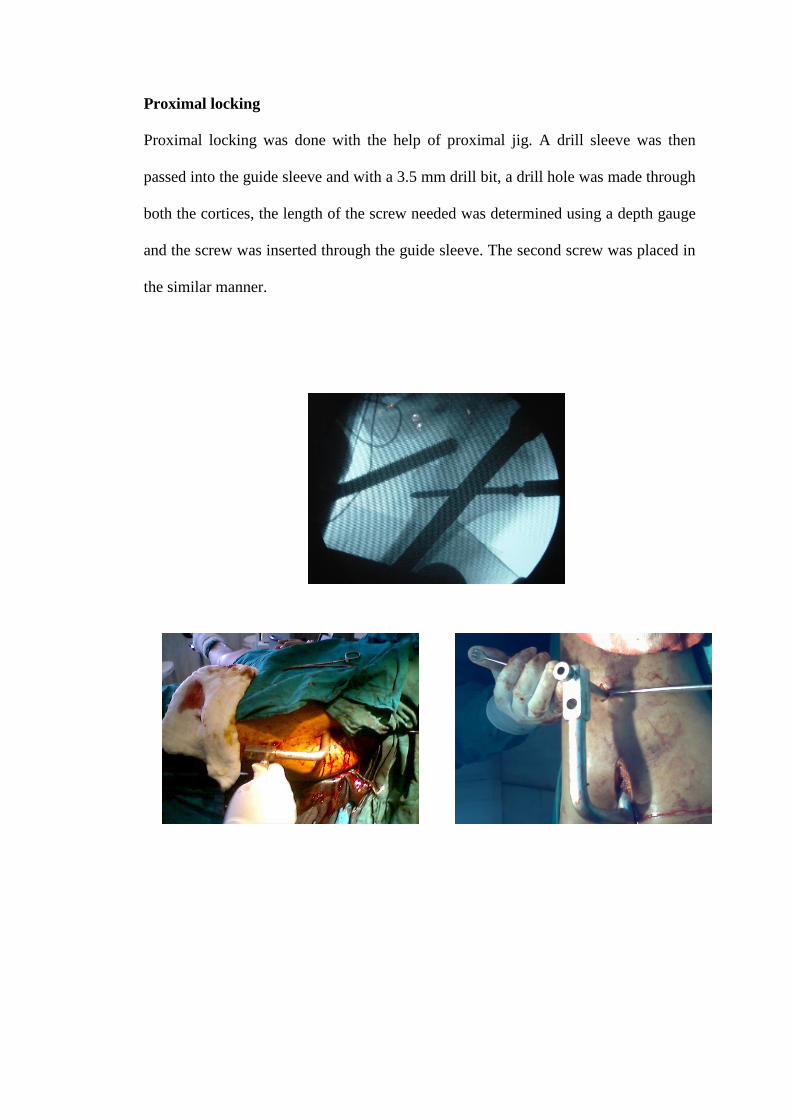
Proximal locking
Proximal locking was done with the help of proximal jig. A drill sleeve was then
passed into the guide sleeve and with a 3.5 mm drill bit, a drill hole was made through
both the cortices, the length of the screw needed was determined using a depth gauge
and the screw was inserted through the guide sleeve. The second screw was placed in
the similar manner.
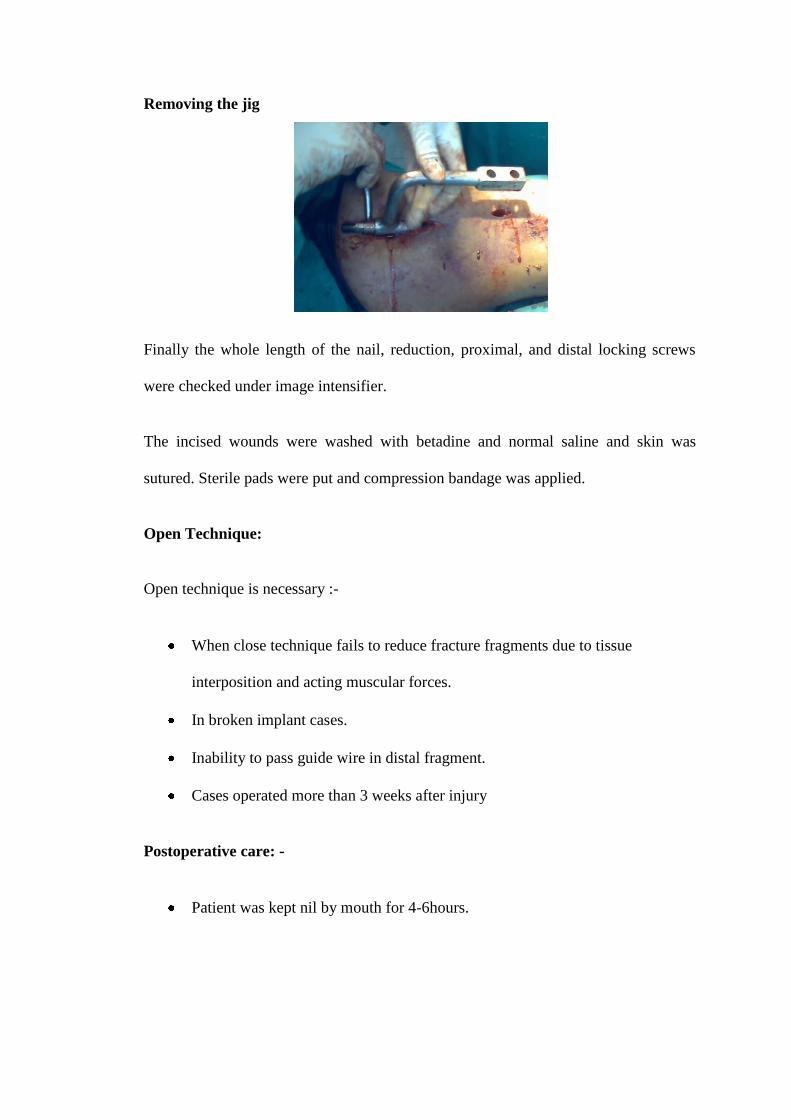
Removing the jig
Finally the whole length of the nail, reduction, proximal, and distal locking screws
were checked under image intensifier.
The incised wounds were washed with betadine and normal saline and skin was
sutured. Sterile pads were put and compression bandage was applied.
Open Technique:
Open technique is necessary :-
When close technique fails to reduce fracture fragments due to tissue
interposition and acting muscular forces.
In broken implant cases.
Inability to pass guide wire in distal fragment.
Cases operated more than 3 weeks after injury
Postoperative care: -
Patient was kept nil by mouth for 4-6hours.
Intra venous fluids, blood transfusions were given as needed. Intra venous
antibiotics were continued for 5 days and then oral antibiotics were given for
next 5 days if needed.
Analgesics were given according to the needs of the patient.
Postoperative radiographs in AP and lateral view were taken.
Head low position was given for 24 hours.
Quadriceps strengthening and active assisted range of motion started on 1st
postoperative day.
Drain removed on 2nd
or 3rd
postoperative day depending on status of oozing
from the operative site.
The patients were mobilized with crutches or walker as soon as pain and local
condition permit with total non-weight bearing.
Static quadriceps and hamstring exercises were explained to the patient.
Sutures were removed on the 14th
postoperative day and patients were
discharged. They were advised to weight bear according to their fracture
pattern and sign of union on follow up radiographs. Follow-ups were done at
6th
, 12th
, 18th
and 24th
weeks and patients were assessed clinically and
radiographically.
For evaluation of results Thoresen et al classification system was used.
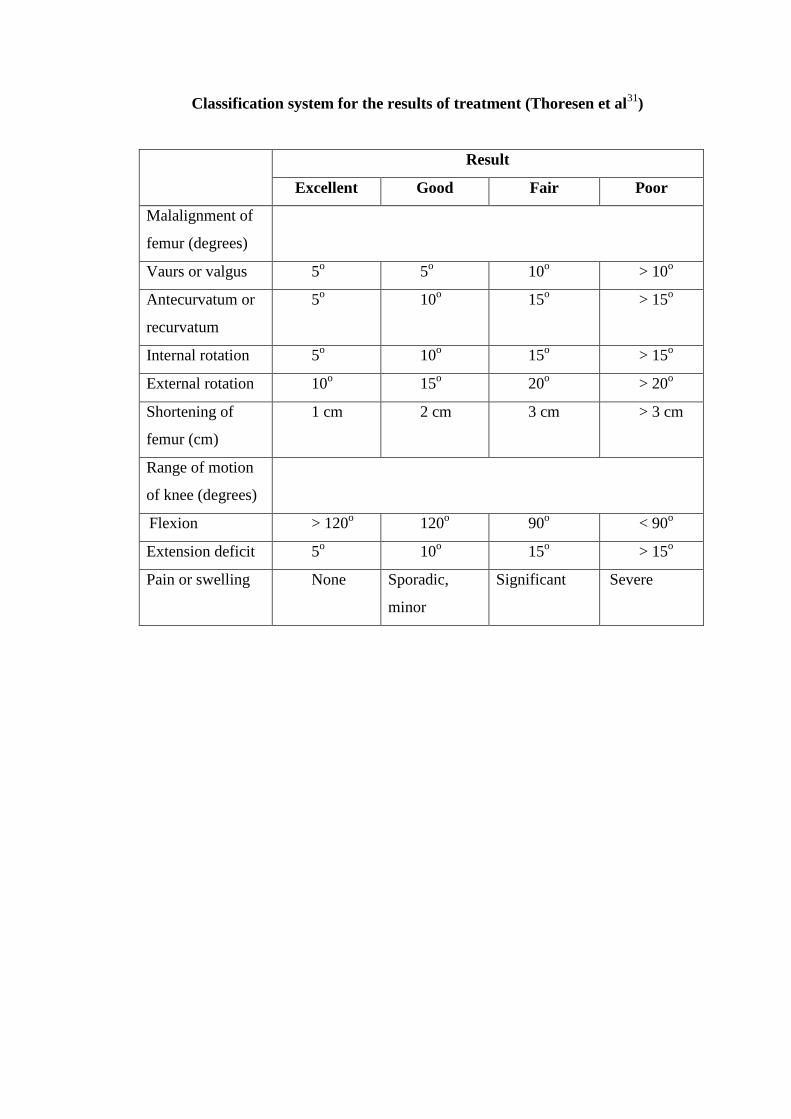
Classification system for the results of treatment (Thoresen et al31
)
Result
Excellent Good Fair Poor
Malalignment of
femur (degrees)
Vaurs or valgus 5o 5
o 10
o > 10
o
Antecurvatum or
recurvatum
5o 10
o 15
o > 15
o
Internal rotation 5o 10
o 15
o > 15
o
External rotation 10o 15
o 20
o > 20
o
Shortening of
femur (cm)
1 cm 2 cm 3 cm > 3 cm
Range of motion
of knee (degrees)
Flexion > 120o 120
o 90
o < 90
o
Extension deficit 5o 10
o 15
o > 15
o
Pain or swelling None Sporadic,
minor
Significant Severe
1
9
4
3
2
1
0
1
2
3
4
5
6
7
8
9
No.
of
Patients
11-20 21-30 31-40 41-50 51-60 61 & above
Age Distribution
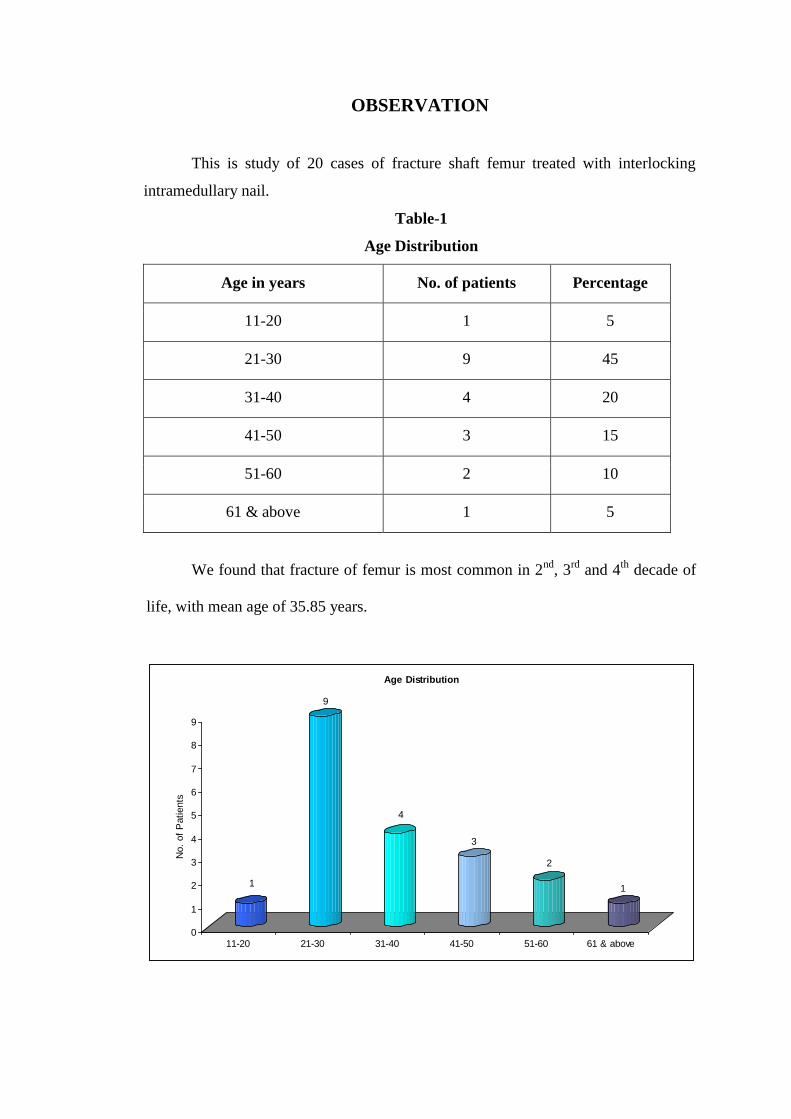
OBSERVATION
This is study of 20 cases of fracture shaft femur treated with interlocking
intramedullary nail.
Table-1
Age Distribution
Age in years No. of patients Percentage
11-20 1 5
21-30 9 45
31-40 4 20
41-50 3 15
51-60 2 10
61 & above 1 5
We found that fracture of femur is most common in 2nd
, 3rd
and 4th
decade of
life, with mean age of 35.85 years.
80%
20%
Sex Distribution
Male
Female
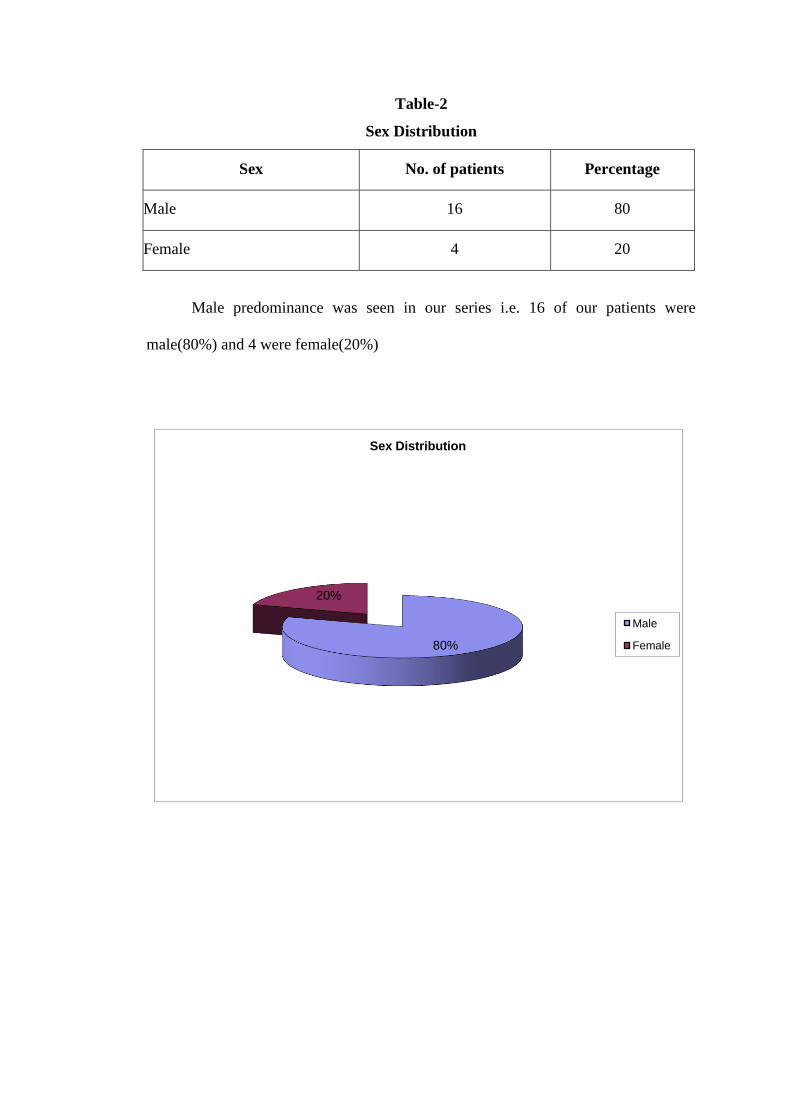
Table-2
Sex Distribution
Sex No. of patients Percentage
Male 16 80
Female 4 20
Male predominance was seen in our series i.e. 16 of our patients were
male(80%) and 4 were female(20%)
17
2
10
0
2
4
6
8
10
12
14
16
18
No.
of
patients
Vehicular accident Fall Agricultural sector Sports injury
Mode of Trauma
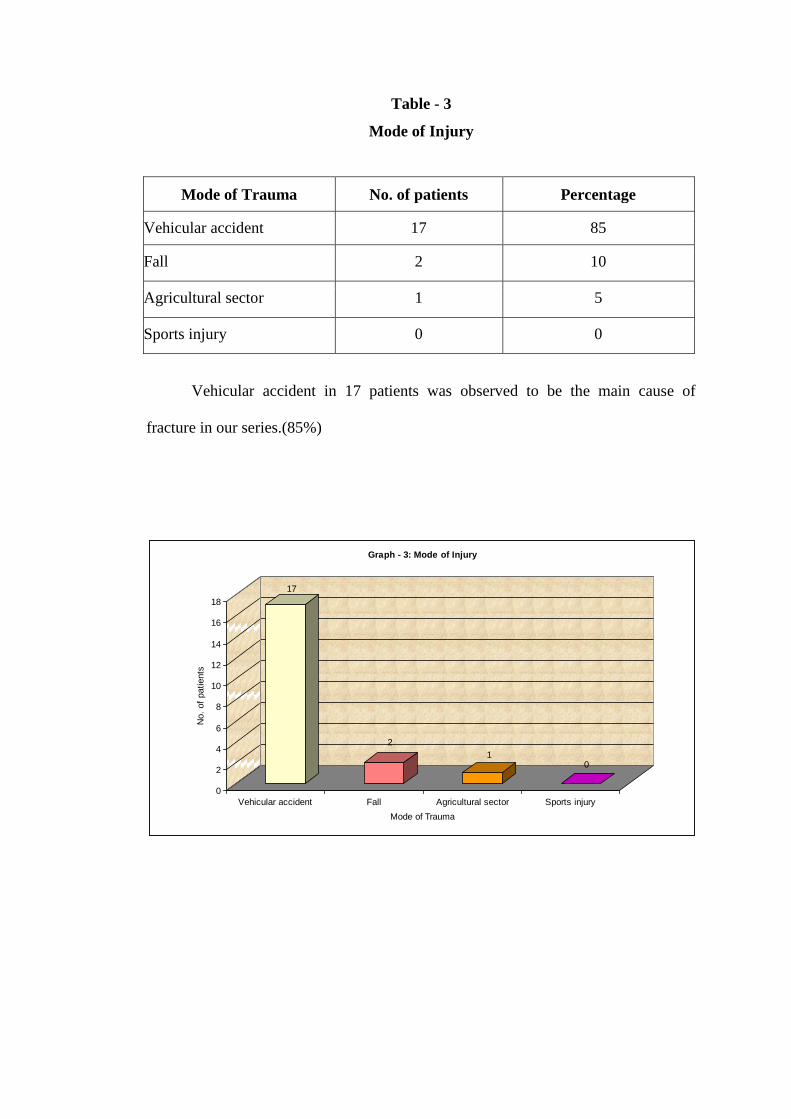
Graph - 3: Mode of Injury
Table - 3
Mode of Injury
Mode of Trauma No. of patients Percentage
Vehicular accident 17 85
Fall 2 10
Agricultural sector 1 5
Sports injury 0 0
Vehicular accident in 17 patients was observed to be the main cause of
fracture in our series.(85%)
01
17
0
7
19.7
0 1
19
0 0 0
0
2
4
6
8
10
12
14
16
18
20
No.
of
Patients
Mean Healing Time
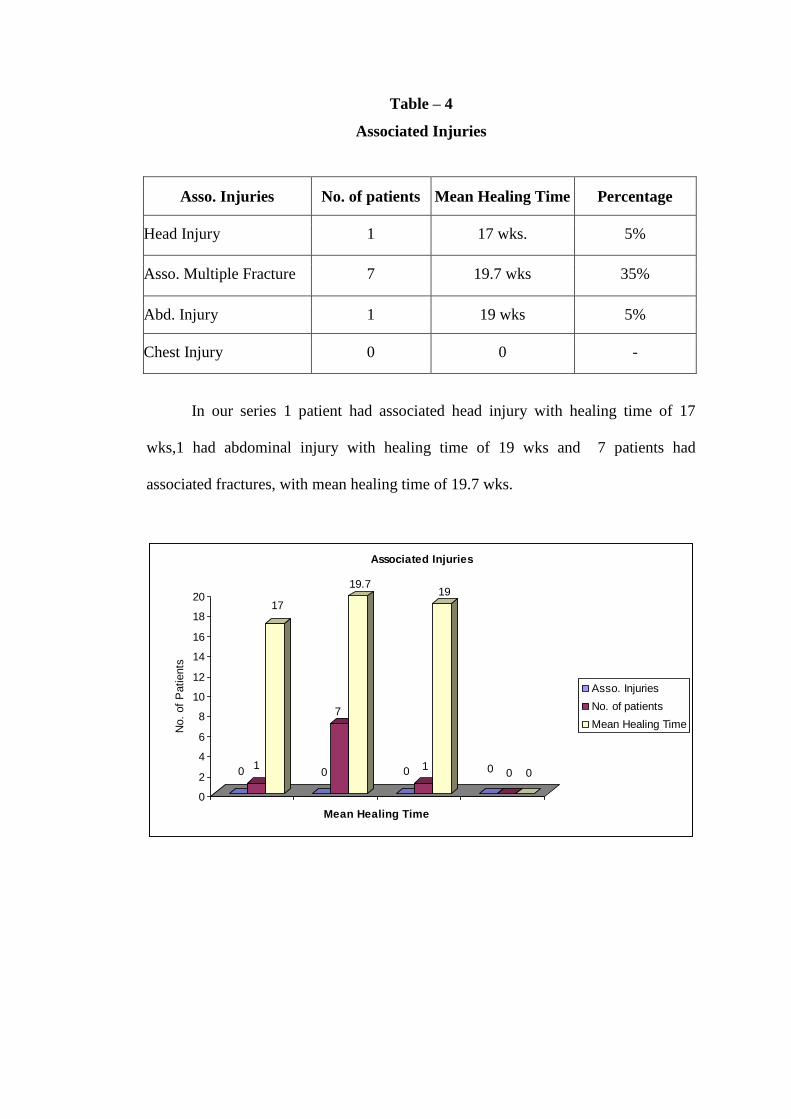
Associated Injuries
Asso. Injuries
No. of patients
Mean Healing Time
Table – 4
Associated Injuries
Asso. Injuries No. of patients Mean Healing Time Percentage
Head Injury 1 17 wks. 5%
Asso. Multiple Fracture 7 19.7 wks 35%
Abd. Injury 1 19 wks 5%
Chest Injury 0 0 -
In our series 1 patient had associated head injury with healing time of 17
wks,1 had abdominal injury with healing time of 19 wks and 7 patients had
associated fractures, with mean healing time of 19.7 wks.
4
11
5
0
2
4
6
8
10
12
No.
of
Patients
Upper third Middle third Lower third
Site of Fracture
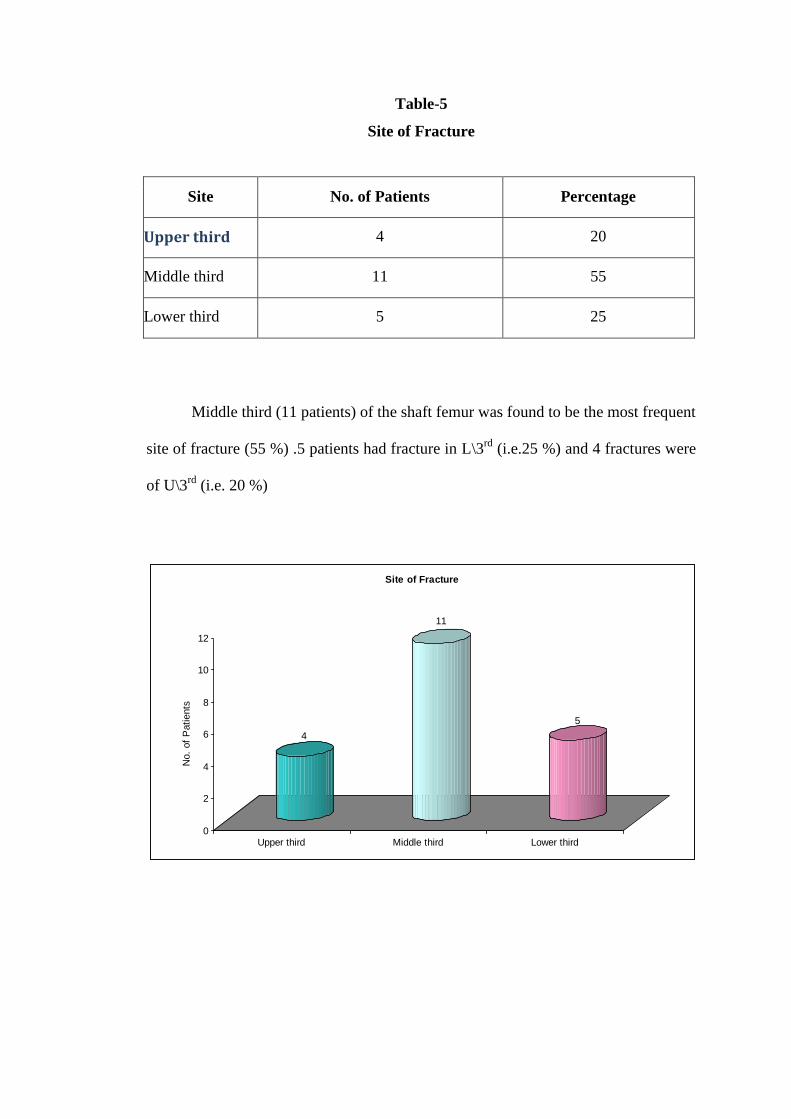
Table-5
Site of Fracture
Site No. of Patients Percentage
Upper third 4 20
Middle third 11 55
Lower third 5 25
Middle third (11 patients) of the shaft femur was found to be the most frequent
site of fracture (55 %) .5 patients had fracture in L\3rd
(i.e.25 %) and 4 fractures were
of U\3rd
(i.e. 20 %)
4
2
1
10
3
0
0
1
2
3
4
5
6
7
8
9
10
No.
of
Patients
Transverse Oblique Spiral Comminuted Butterfly Segmental
Pattern of fracture
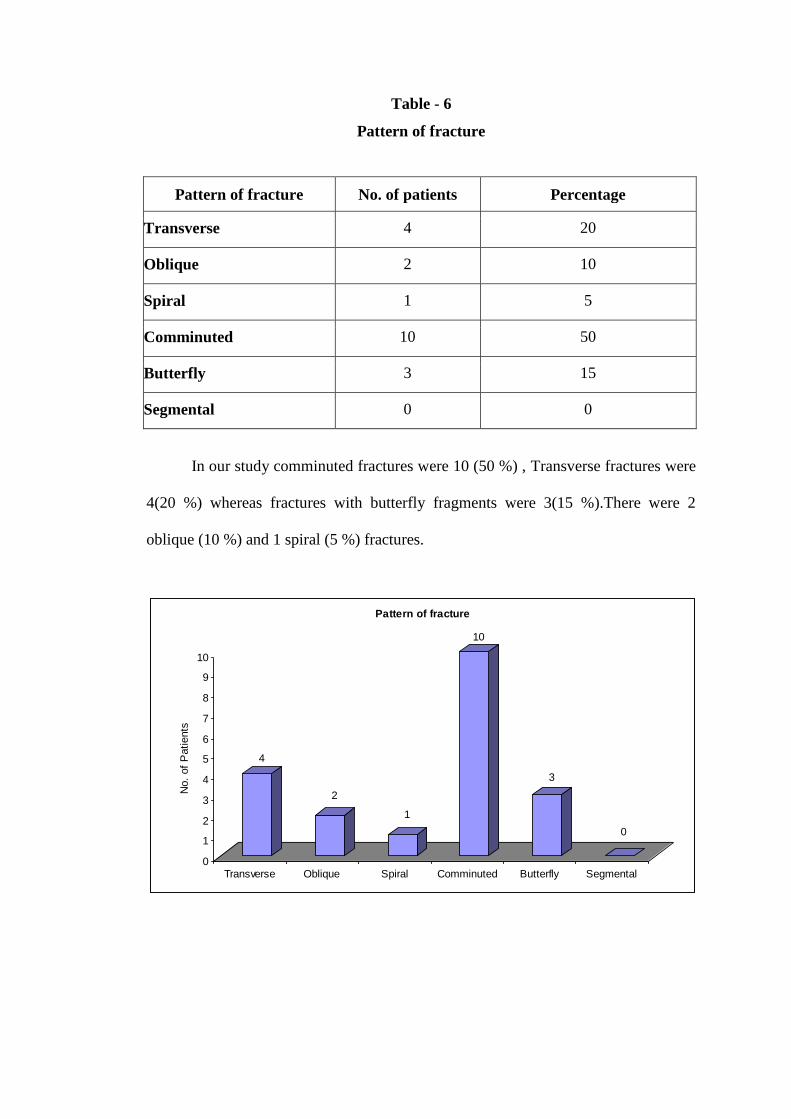
Table - 6
Pattern of fracture
Pattern of fracture No. of patients Percentage
Transverse 4 20
Oblique 2 10
Spiral 1 5
Comminuted 10 50
Butterfly 3 15
Segmental 0 0
In our study comminuted fractures were 10 (50 %) , Transverse fractures were
4(20 %) whereas fractures with butterfly fragments were 3(15 %).There were 2
oblique (10 %) and 1 spiral (5 %) fractures.
8
10
2
0
0
1
2
3
4
5
6
7
8
9
10
No.o
f P
atients
I II III IV
Winquist Hansen Classification
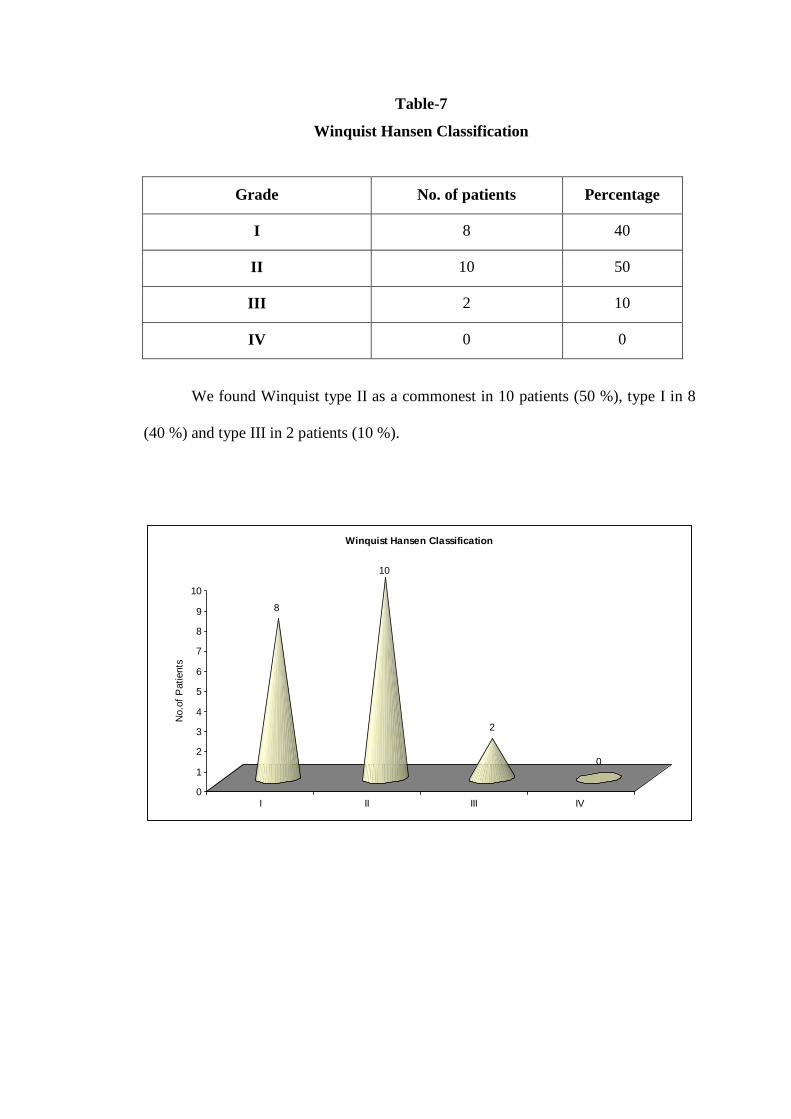
Table-7
Winquist Hansen Classification
Grade No. of patients Percentage
I 8 40
II 10 50
III 2 10
IV 0 0
We found Winquist type II as a commonest in 10 patients (50 %), type I in 8
(40 %) and type III in 2 patients (10 %).
13
7
5
2
0
0
2
4
6
8
10
12
14
No.o
f P
atients
Closed Open Open Gr.I Open Gr.II Open Gr.III
Open or Closed Fracture
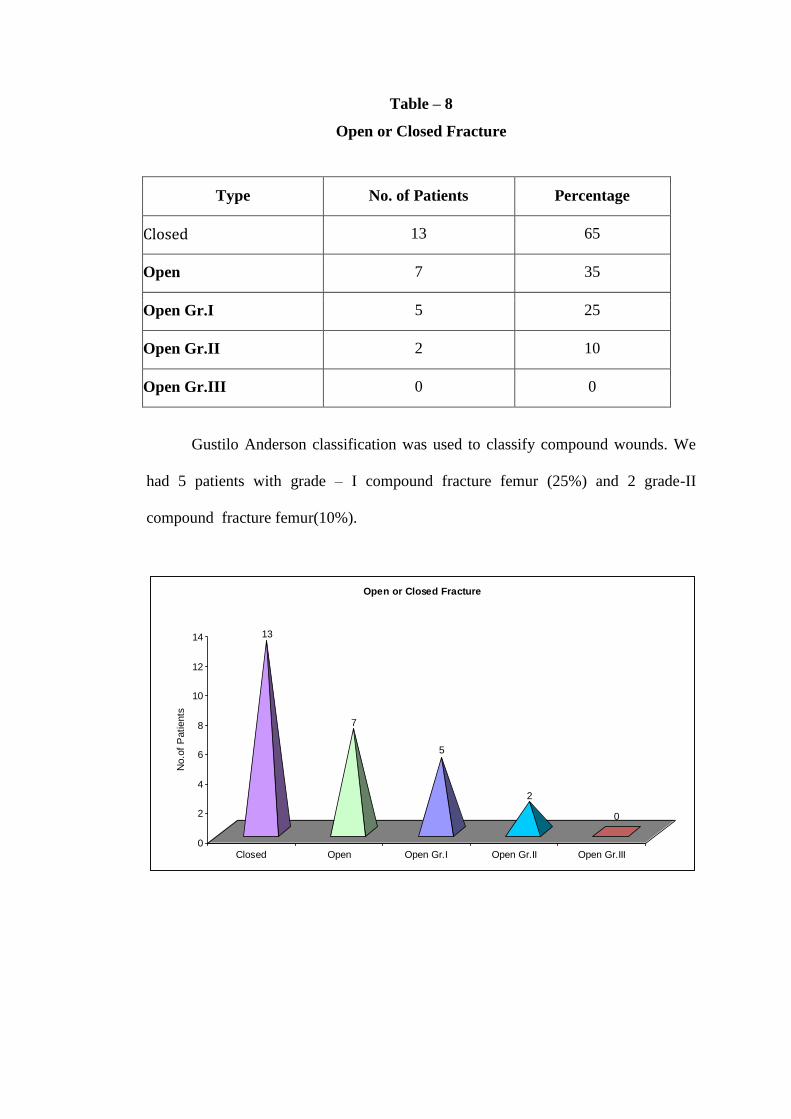
Table – 8
Open or Closed Fracture
Type No. of Patients Percentage
Closed 13 65
Open 7 35
Open Gr.I 5 25
Open Gr.II 2 10
Open Gr.III 0 0
Gustilo Anderson classification was used to classify compound wounds. We
had 5 patients with grade – I compound fracture femur (25%) and 2 grade-II
compound fracture femur(10%).
Closed or open nailing
90%
10%
Closed
Open
Table – 9
Closed or open nailing
Type No. of Patients Percentage
Closed 18 90
Open 2 10
Open nailing was done in 2 patients with Gr. II compound injuries.
17
2
0
2
4
6
8
10
12
14
16
18
No.
of
Patients
CRIF ORIF
Healing Time in Orif and Crif
Table - 10
Healing Time in ORIF and CRIF
Type No. of Patients Avg. healing time wk
CRIF 17 18.35 wks
ORIF 2 20wks
Open nailing was done in 2 patients and closed nailing in all other 18 patients.
Average healing time of union in open procedure was 20 wks and in closed procedure
it was 18.35 wks. Total average healing time of 19 patients who had union was 18.53
wks.
18
2
0
2
4
6
8
10
12
14
16
18
No.
of
Patients
Day 1-3 > 5 days
Non weight bearing
Commencement of non – weight bearing (NWB)
Post operative mobilization
It was done immediately after the patient recovered from anesthesia, isometric
exercises were initially begun followed by flexion extension exercises of hip and
knee in all 20 patients.
Table - 11
Commencement of non – weight bearing (NWB)
Non weight bearing No. of Patients Percentage
Day 1-3 18 90
> 5 days 2 10
Non-weight bearing crutch walking was begun early in 18 cases (90%)
between 1st
-3rd
post operative day, except in 2 patients (10%). The 1st patient who
had an associated humerus fracture had developed vulval edema on 1st post operative
day and had an internal rotation deformity which was corrected on 5th
postoperative
day so non-weight bearing crutch walking was started on 10th
day . Another patient
had ipsilateral lateral malleolus fracture so crutch walking was started on 14th
day.
18
2
0
2
4
6
8
10
12
14
16
18
No.
of
Cases
3-10 days > 2 weeks
Partial weight bearing
Partial weight bearing (PWB)
Table – 12
Partial weight bearing (PWB)
Partial weight bearing No. of cases Percentage
3-10 days 18 90
> 2 weeks 2 10
Partial weight bearing with walker was started between 3-10 days in 18 cases
(90%). One patient had ipsilateral lateral malleolus fracture. He was allowed to bear
partial weight after 24 days and the other patient had humerus fracture who started
partial weigh bearing after 21 days.
Average time for partial weight bearing in our study was 6.45 days.
4
9
4
2
1
0
1
2
3
4
5
6
7
8
9
Full
weig
ht
bearing
10th week 12th week 14th week 16th week Unable to
bear full
weight
No. of Cases
Full weight bearing
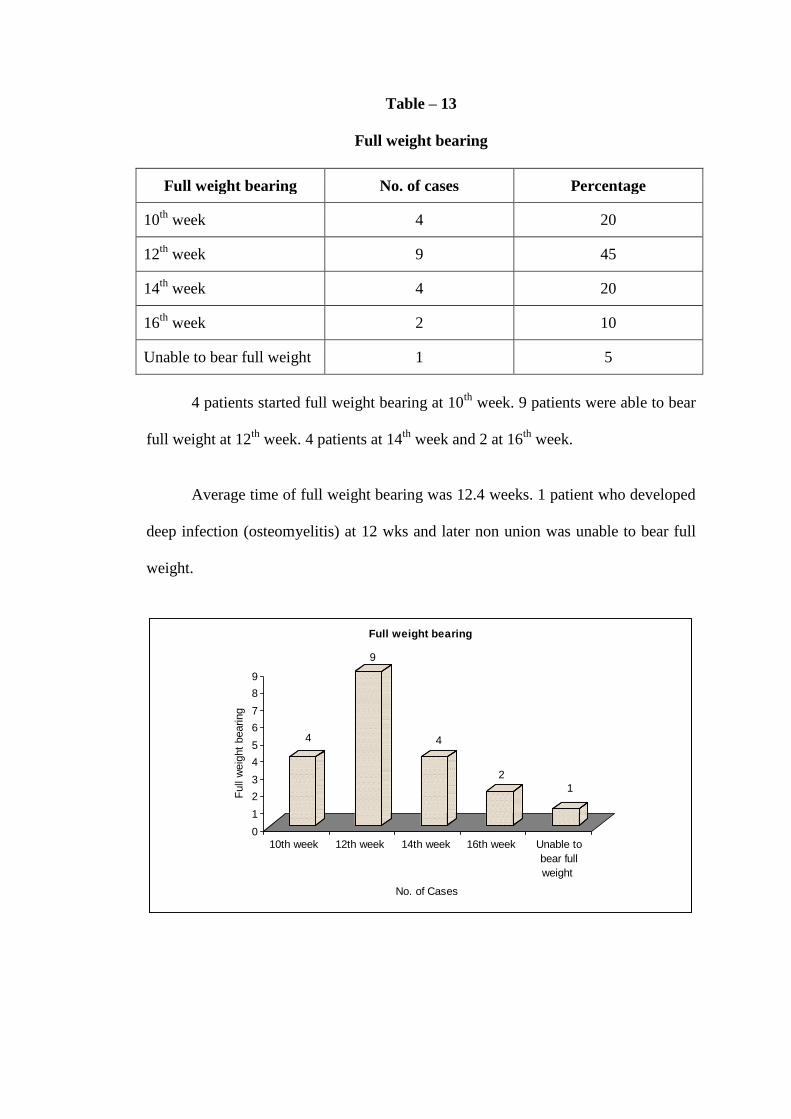
Table – 13
Full weight bearing
Full weight bearing No. of cases Percentage
10th
week 4 20
12th
week 9 45
14th
week 4 20
16th
week 2 10
Unable to bear full weight 1 5
4 patients started full weight bearing at 10th
week. 9 patients were able to bear
full weight at 12th
week. 4 patients at 14th
week and 2 at 16th
week.
Average time of full weight bearing was 12.4 weeks. 1 patient who developed
deep infection (osteomyelitis) at 12 wks and later non union was unable to bear full
weight.
18
2
0
2
4
6
8
10
12
14
16
18
No.
of
Patients
Static Dynamised
Type
Dynamisation required and healing time
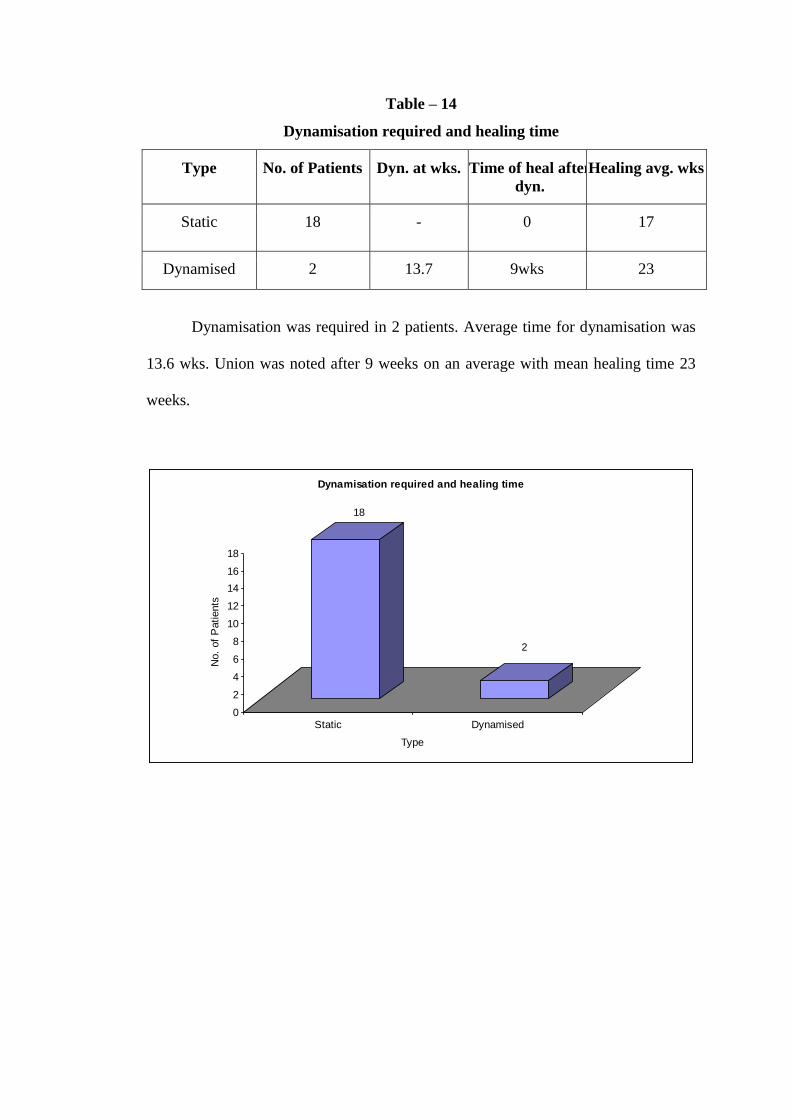
Table – 14
Dynamisation required and healing time
Type No. of Patients Dyn. at wks. Time of heal after
dyn.
Healing avg. wks
Static 18 - 0 17
Dynamised 2 13.7 9wks 23
Dynamisation was required in 2 patients. Average time for dynamisation was
13.6 wks. Union was noted after 9 weeks on an average with mean healing time 23
weeks.
3.5
7.4
6.2
0
1
2
3
4
5
6
7
8
No.
of
Patients
Blumberg 1990 Hanks 1996 Present Series
Injury-Surgery Interval
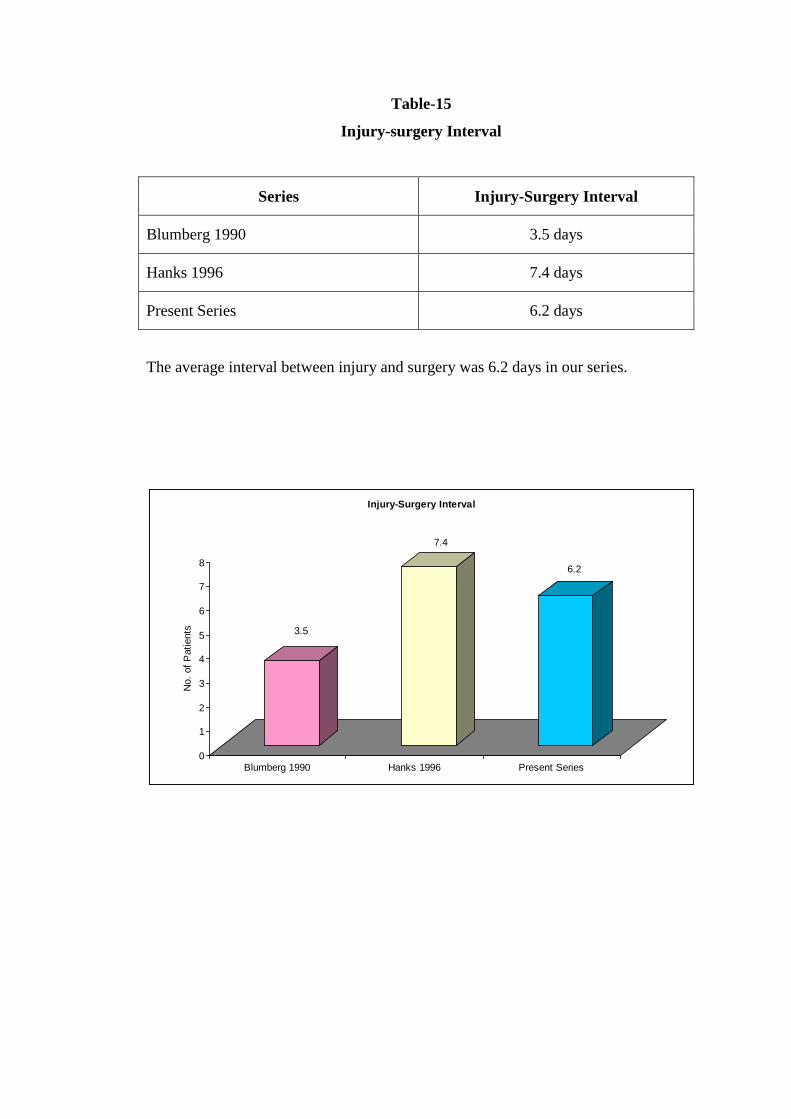
Table-15
Injury-surgery Interval
Series Injury-Surgery Interval
Blumberg 1990 3.5 days
Hanks 1996 7.4 days
Present Series 6.2 days
The average interval between injury and surgery was 6.2 days in our series.
182
195
170.5
155
160
165
170
175
180
185
190
195
Lhowe 1988 Wiss 1986 Our series
Operative time (in minutes)
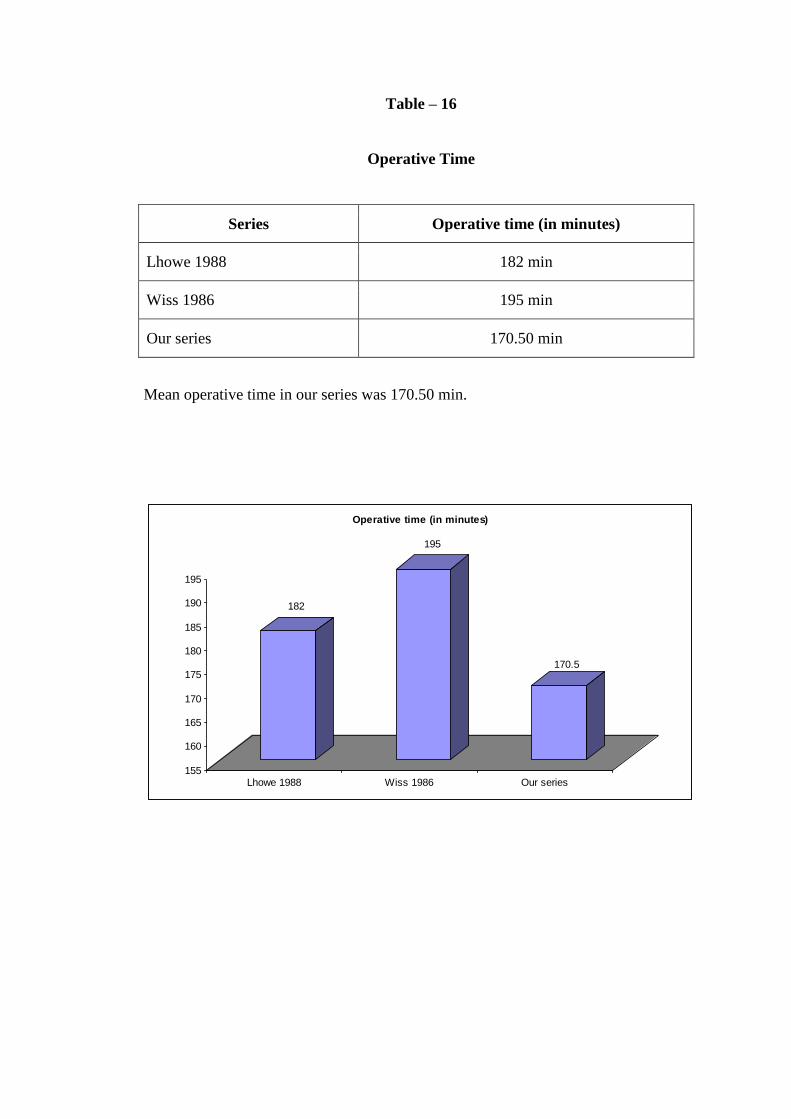
Table – 16
Operative Time
Series Operative time (in minutes)
Lhowe 1988 182 min
Wiss 1986 195 min
Our series 170.50 min
Mean operative time in our series was 170.50 min.
0 0 0 0 0
1
0
1 1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
No.
of
Patients
Bending of
nail
Impaction of
nail
Breakage of
locking
ARDS Vulval
oedema
Intraoperative complications
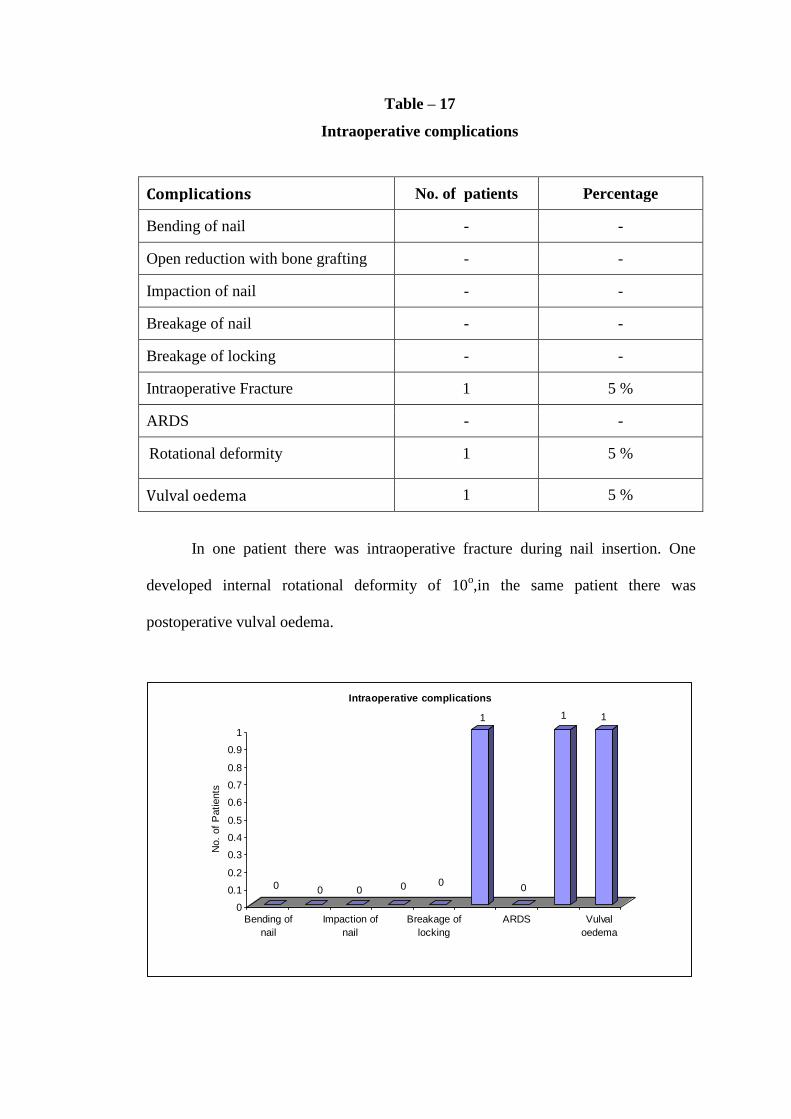
Table – 17
Intraoperative complications
Complications No. of patients Percentage
Bending of nail - -
Open reduction with bone grafting - -
Impaction of nail - -
Breakage of nail - -
Breakage of locking - -
Intraoperative Fracture 1 5 %
ARDS - -
Rotational deformity 1 5 %
Vulval oedema 1 5 %
In one patient there was intraoperative fracture during nail insertion. One
developed internal rotational deformity of 10o,in the same patient there was
postoperative vulval oedema.
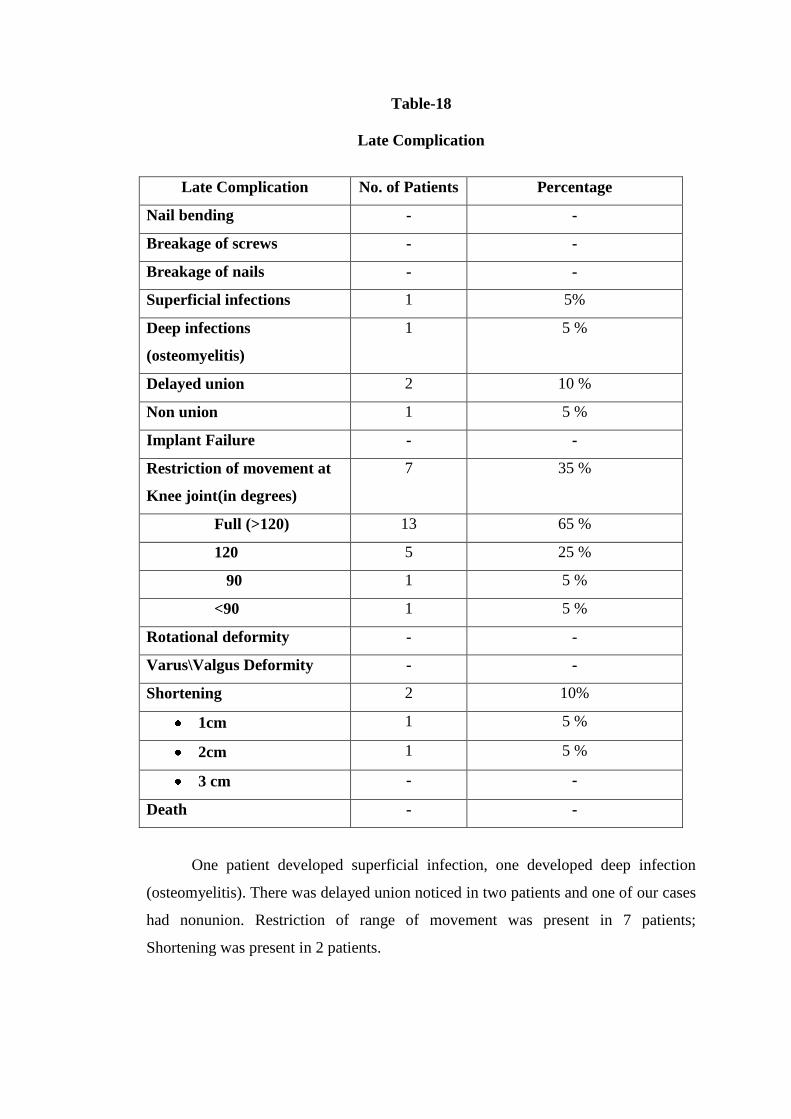
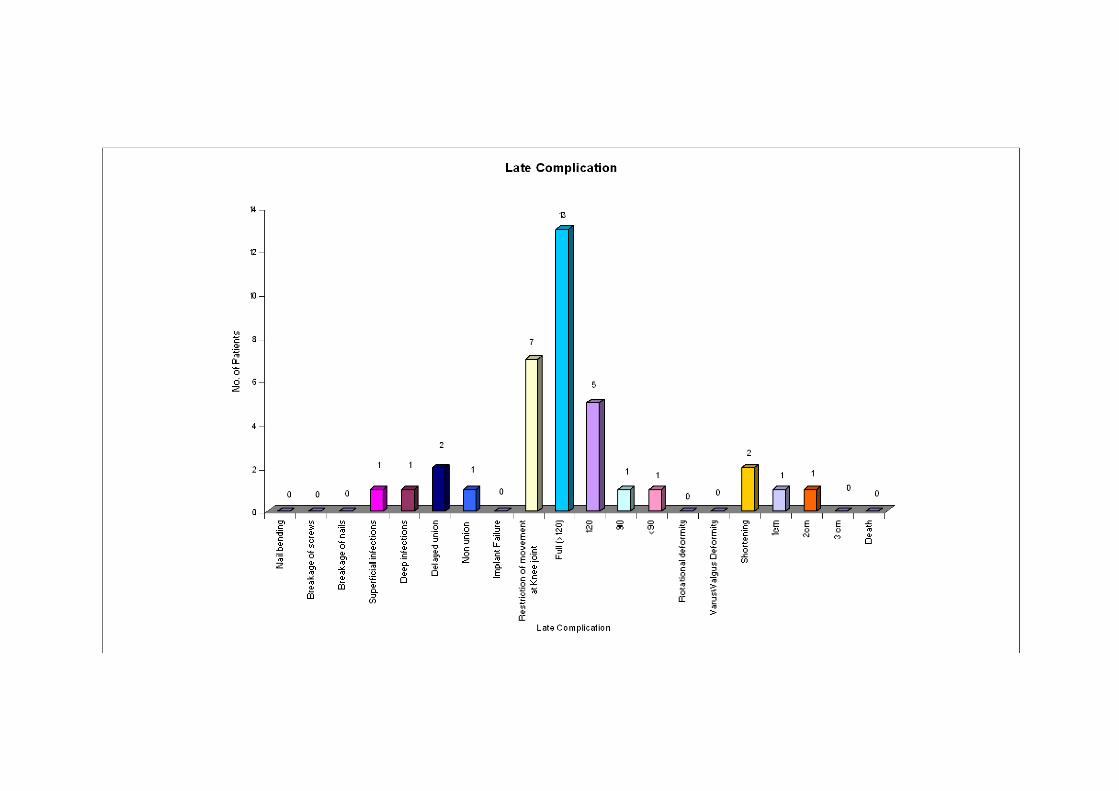
Table-18
Late Complication
Late Complication No. of Patients Percentage
Nail bending - -
Breakage of screws - -
Breakage of nails - -
Superficial infections 1 5%
Deep infections
(osteomyelitis)
1 5 %
Delayed union 2 10 %
Non union 1 5 %
Implant Failure - -
Restriction of movement at
Knee joint(in degrees)
7 35 %
Full (>120) 13 65 %
120 5 25 %
90 1 5 %
<90 1 5 %
Rotational deformity - -
Varus\Valgus Deformity - -
Shortening 2 10%
1cm 1 5 %
2cm 1 5 %
3 cm - -
Death - -
One patient developed superficial infection, one developed deep infection
(osteomyelitis). There was delayed union noticed in two patients and one of our cases
had nonunion. Restriction of range of movement was present in 7 patients;
Shortening was present in 2 patients.
63.463.8
60
19.517
30
15.414.9
5 1.6 4.25 5
0
10
20
30
40
50
60
70
Excellent Good Fair Poor
Comparison of Results
Alho et al
Thoresen et al
Our series
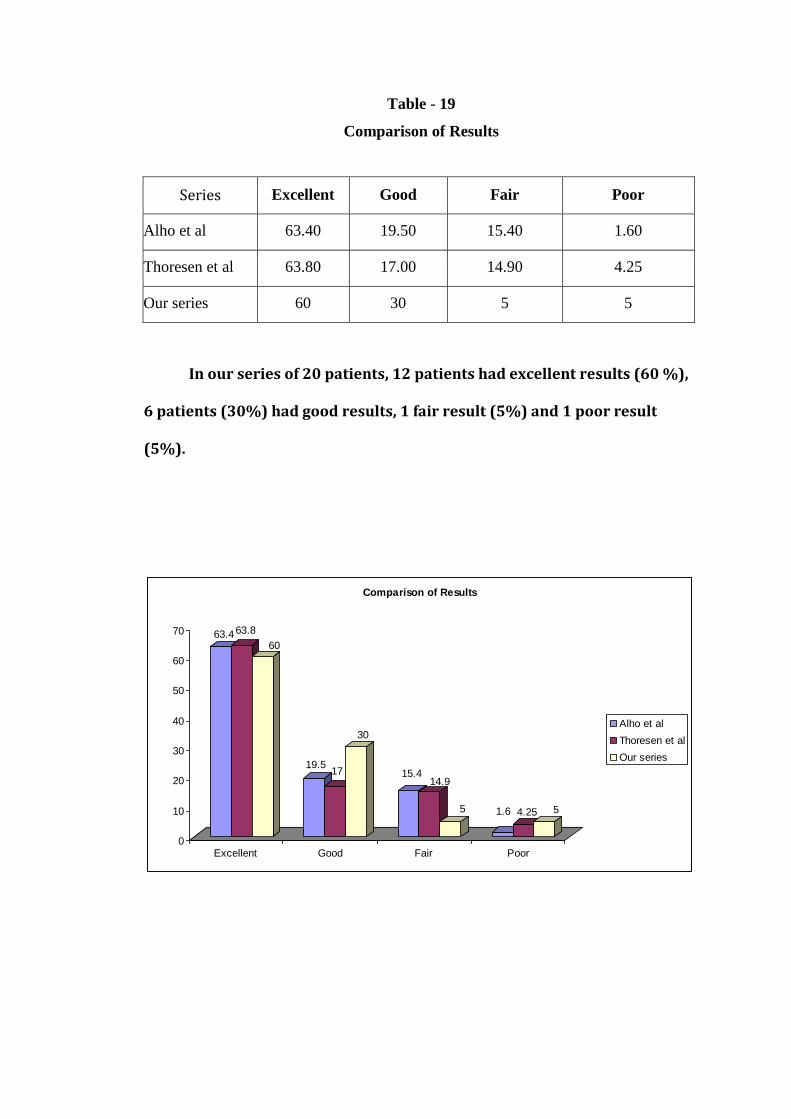
Table - 19
Comparison of Results
Series Excellent Good Fair Poor
Alho et al 63.40 19.50 15.40 1.60
Thoresen et al 63.80 17.00 14.90 4.25
Our series 60 30 5 5
In our series of 20 patients, 12 patients had excellent results (60 %),
6 patients (30%) had good results, 1 fair result (5%) and 1 poor result
(5%).
63
.40
%
63
.82
%
70
%
17
.%
23
..30
%
15
.40 %
1
.60
%
14
.90
4.2
5 %
19
.50
%
3.3
0 %
3.3
0 %
RESULTS
For evaluation of results in our series Thoresen et al classification system
was used.
We had 20 patients of which 12 patients had excellent results (60%) with full,
pain-free, function of the extremity.
We had 6 patients with good result (30%); 5 patients had range of motion
120o and shortening of 2 cm was observed in 1 patients.
We had 1 fair result (5%) of a patient, with compound Gr. II injury with range
of motion 90o.
1 poor result (5%) had non union, with range of motion < 90o
with a thigh
supported in a brace.
So overall we had, 90% excellent to good result and 10% fair to poor results,
with non-union in one case.
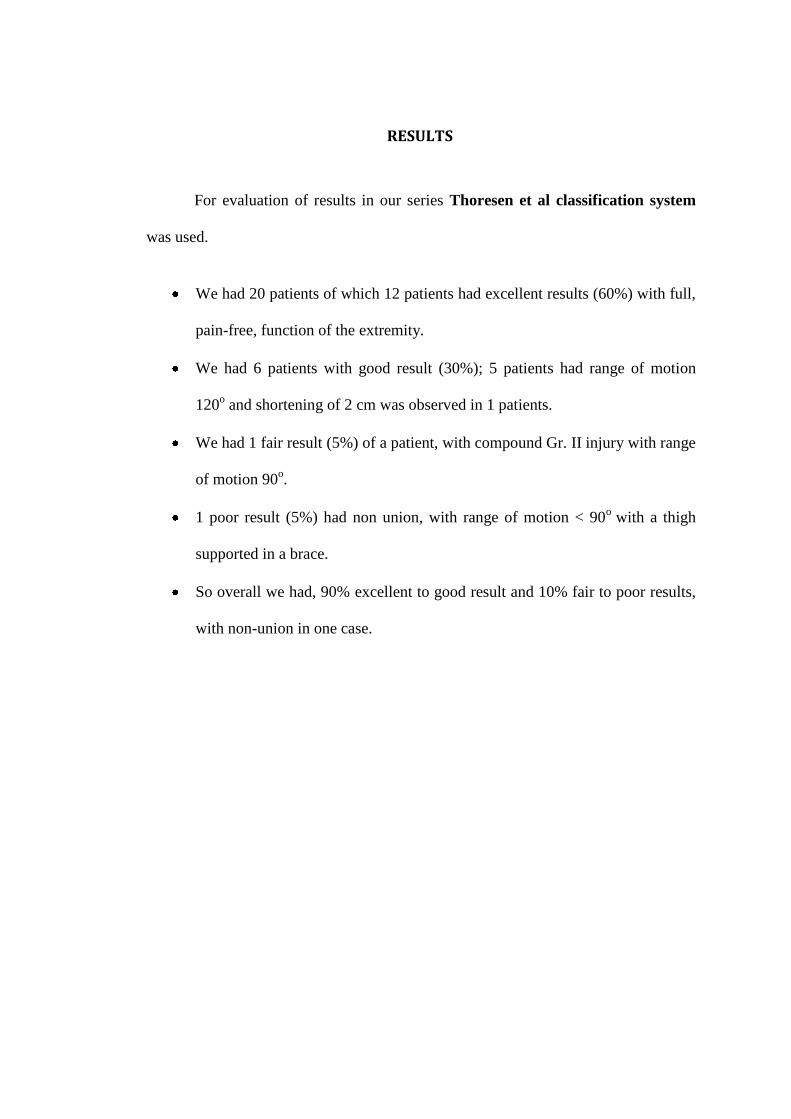
CLINICAL PHOTOS CASE NO. 4 (FIGURE -15)
Hip flexion with knee straight Hip flexion with knee flexed
Knee Flexion Full Weight Bearing
Squatting Sitting Cross-legged
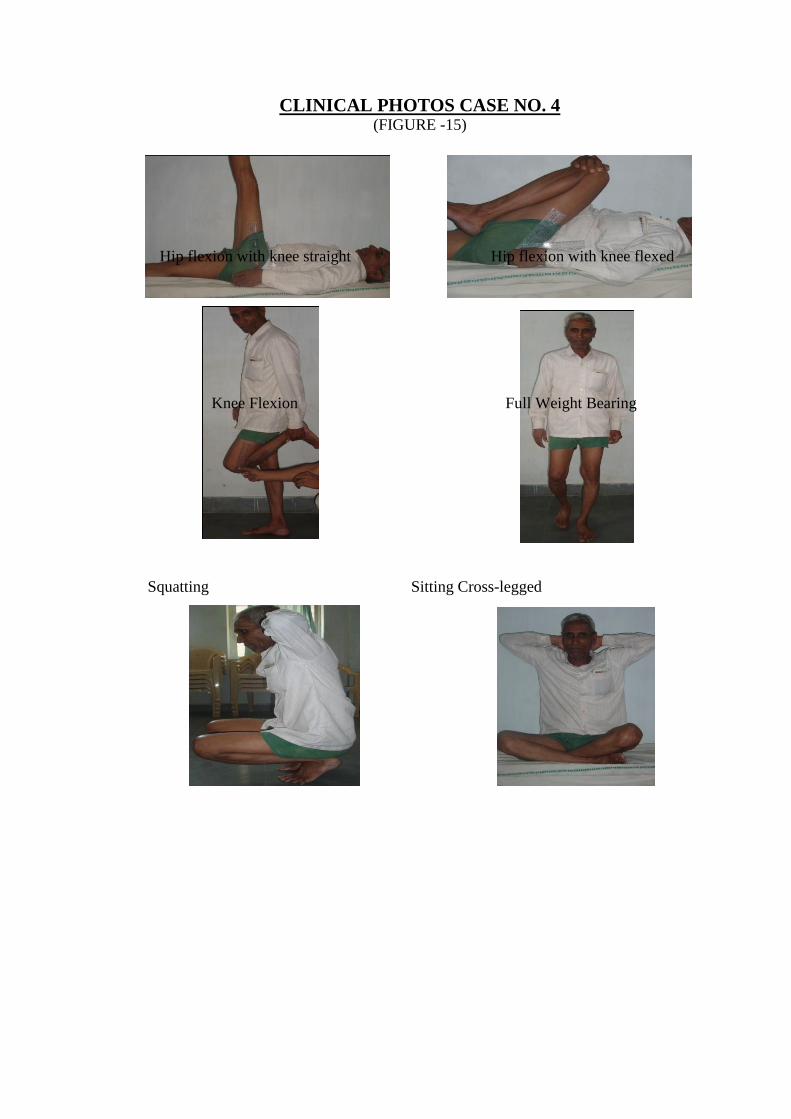
CASE NO. 6 (Figure -16)
Pre Operative AP & Lateral Post operative
Callus at 10 wks
Union at 17 wks
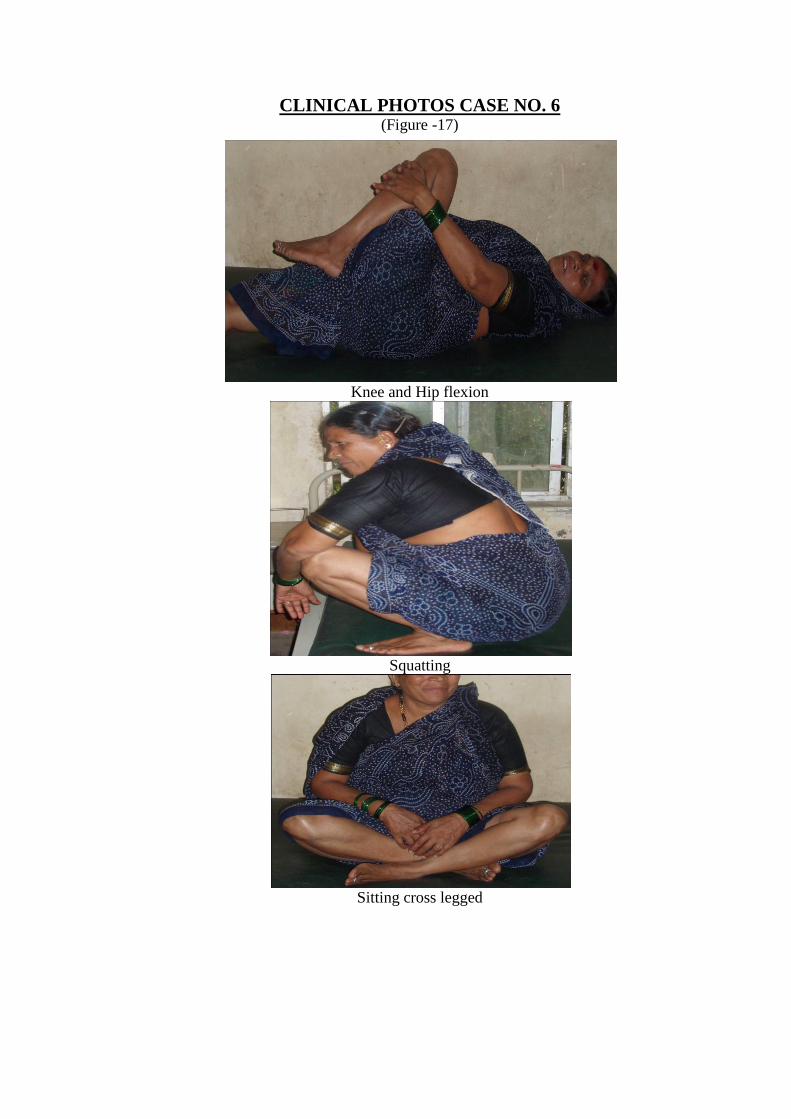
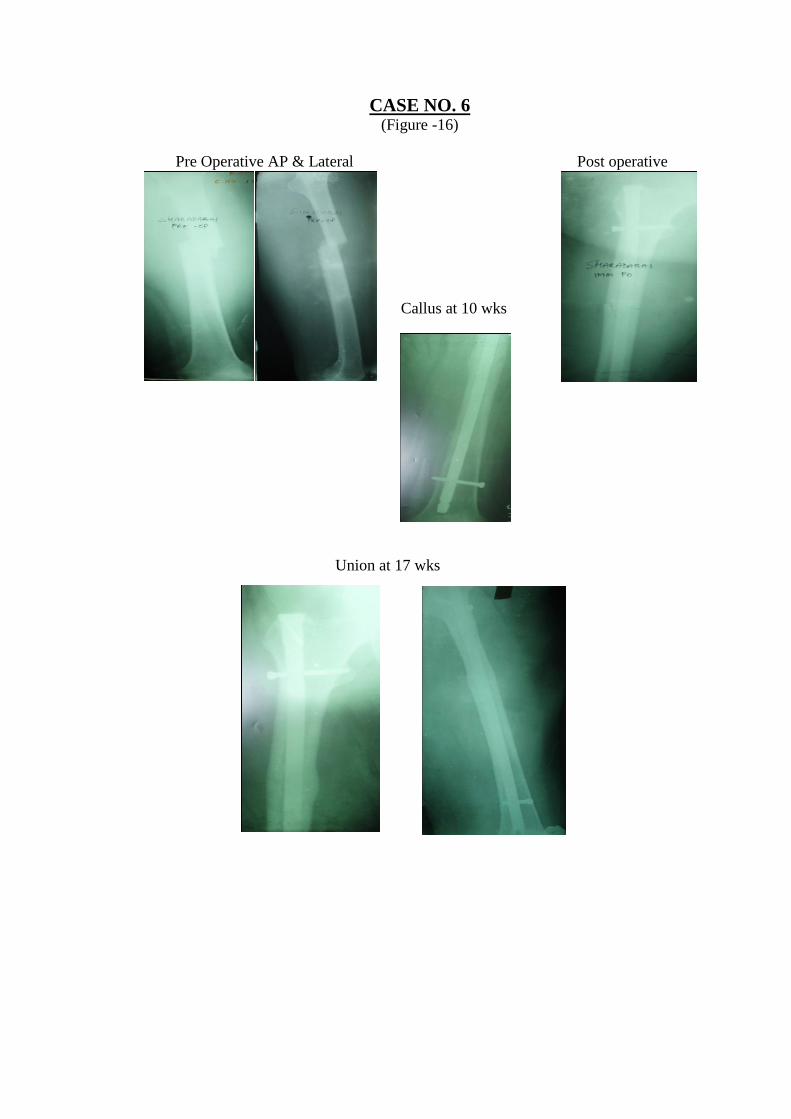
CLINICAL PHOTOS CASE NO. 6 (Figure -17)
Knee and Hip flexion
Squatting
Sitting cross legged
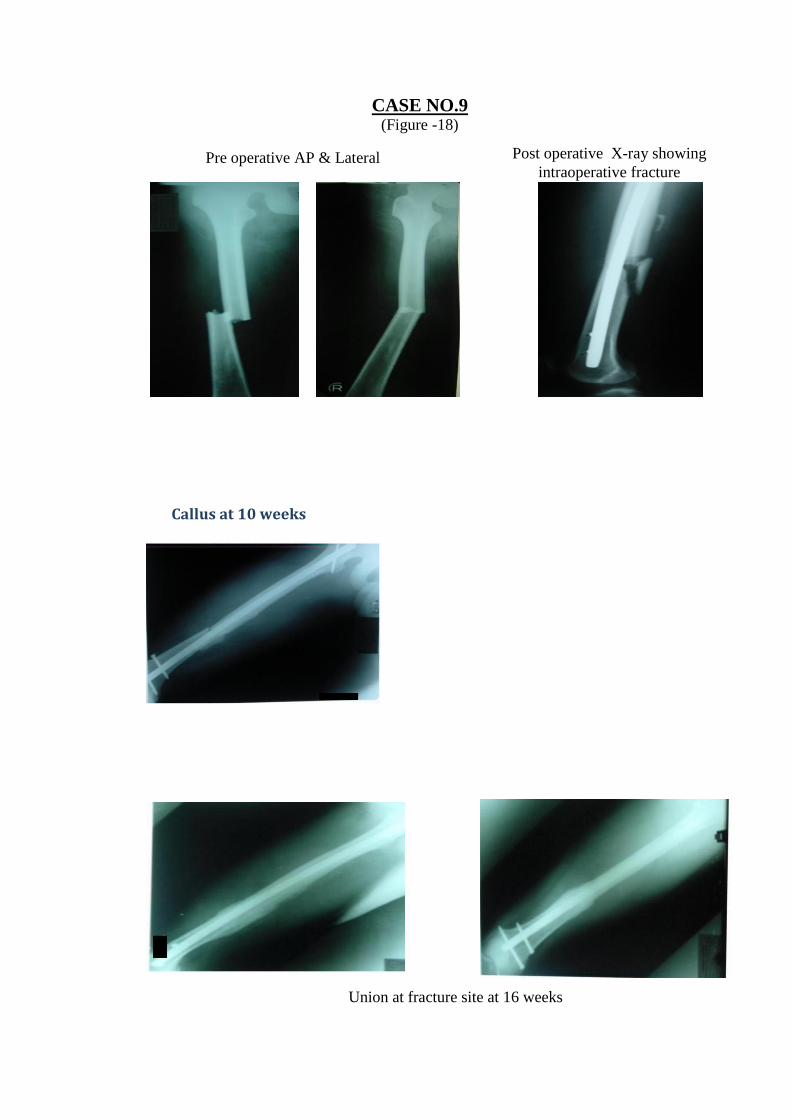
CASE NO.9
(Figure -18)
Pre operative AP & Lateral Post operative X-ray showing
intraoperative fracture
Union at fracture site at 16 weeks
Callus at 10 weeks
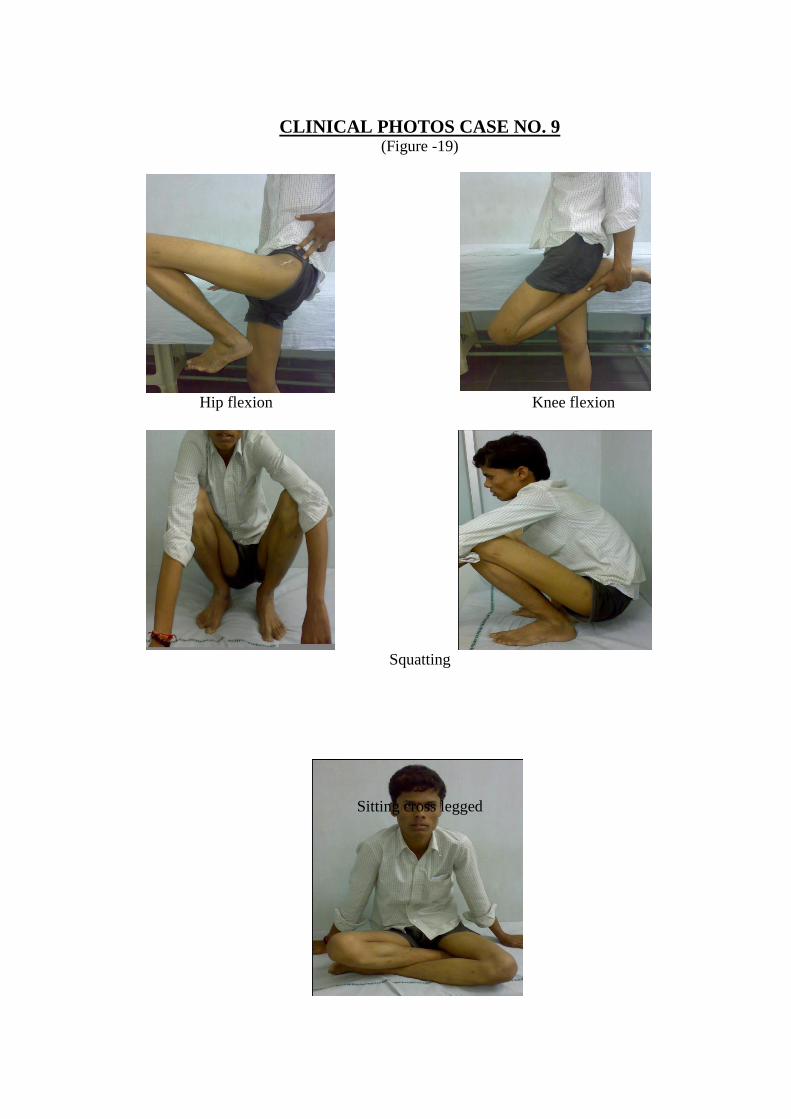
CLINICAL PHOTOS CASE NO. 9 (Figure -19)
Hip flexion Knee flexion
Squatting
Sitting cross legged
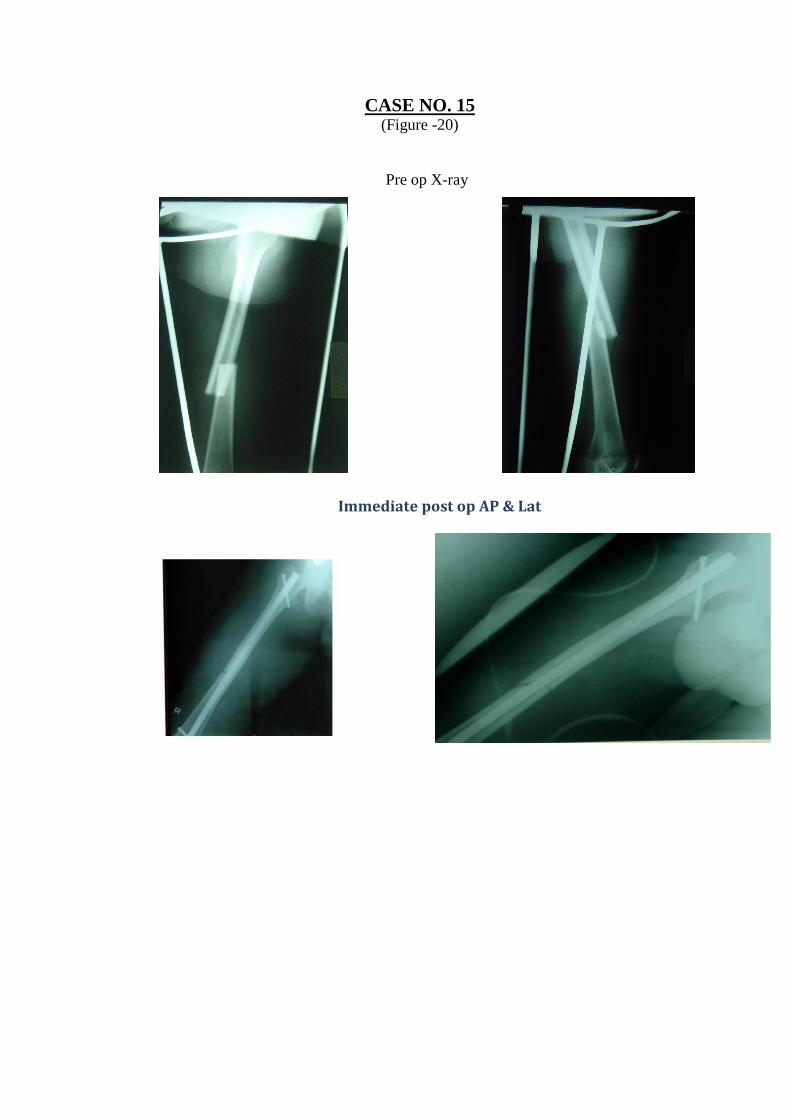
CASE NO. 15 (Figure -20)
Pre op X-ray
Immediate post op AP & Lat
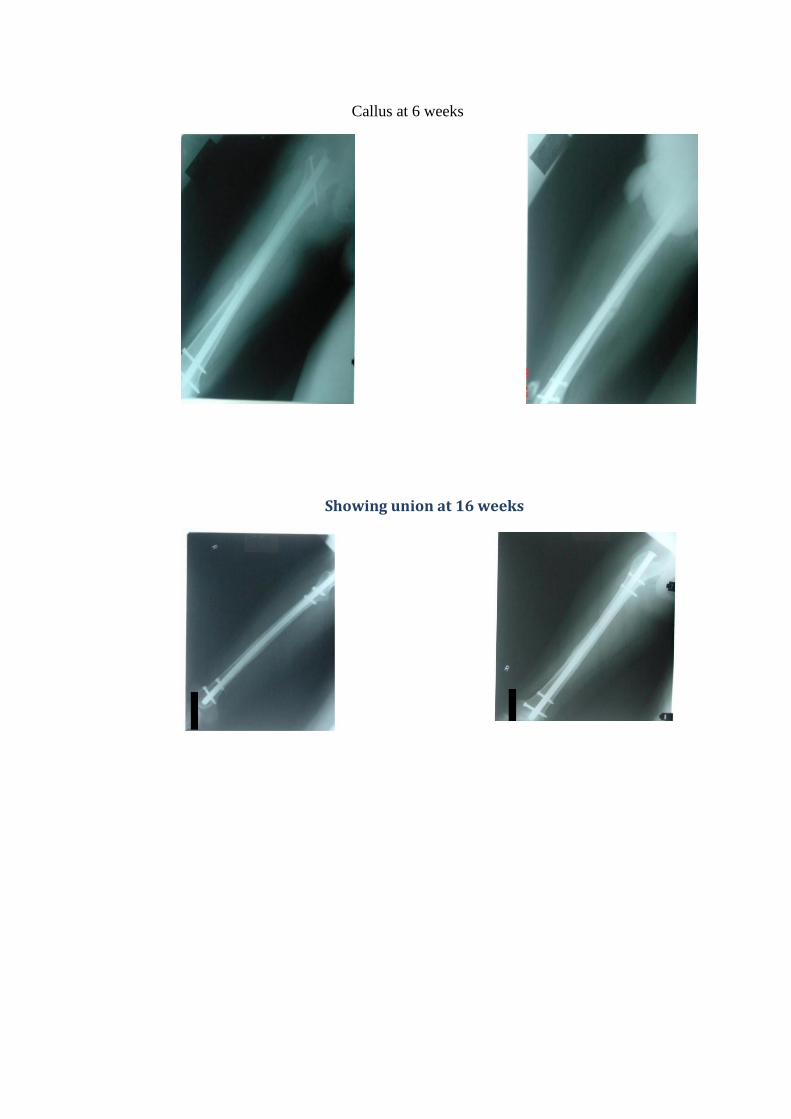
Callus at 6 weeks
Showing union at 16 weeks
CLINICAL PHOTOS CASE NO. 15 (Figure -21)
Sitting Cross-legged Squatting
Full weight bearing
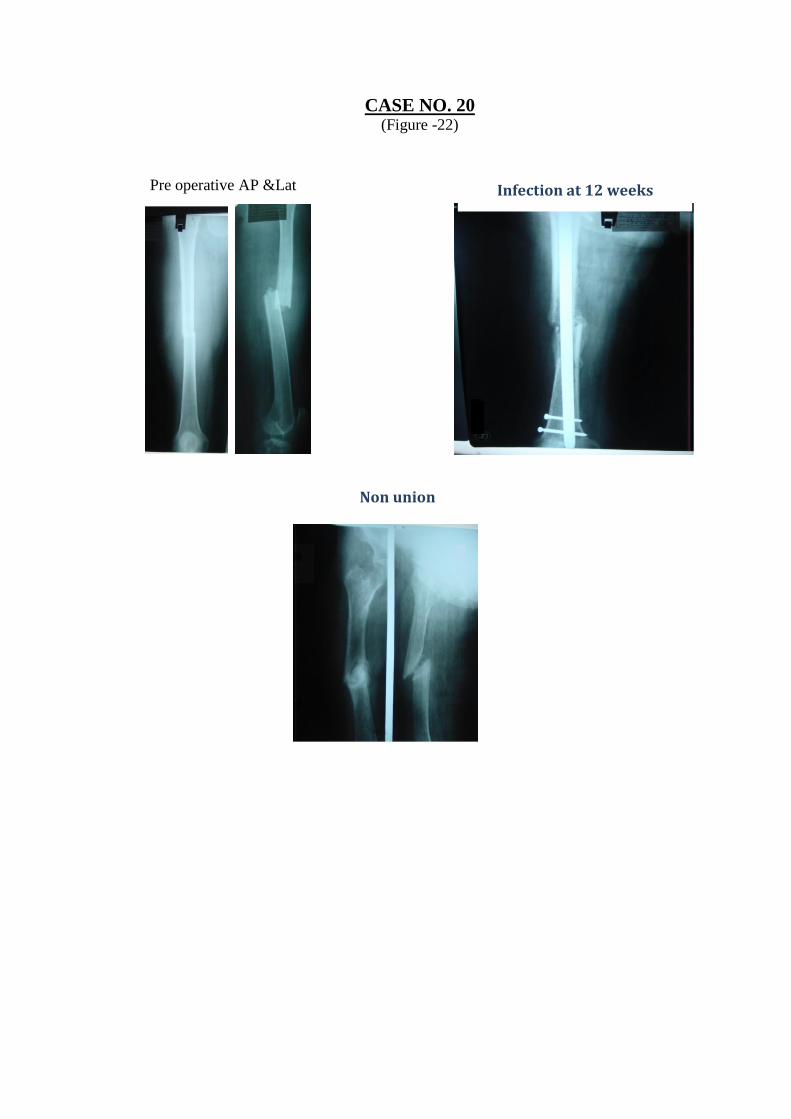
CASE NO. 20 (Figure -22)
Pre operative AP &Lat Infection at 12 weeks
Non union
DISCUSSION
The treatment of fractures of the shaft femur has been revolutionized by
advent of Kuntscher’s nail in 1940. The scope of femoral shaft nailing has been
broadened with reaming and interlocking of intramedullary nails. Since then
unacceptable rates of malunion and non-union shown by various methods of
conservative treatment has fallen dramatically.
Age distribution
We found that fracture of femur was most common in 2nd,
3rd
and 4th
decade of
life(80%) with mean age of 36 yrs, ranging from 20 to 71 yrs.(Table-1)
Winquist et al28
. in his series reported 3rd
, 4th
and 5th
decade as a common
age group i.e. 70 % middle age group population , with mean age 29 years age
group.
White et al.32
observed mean age of 28 years but same age distribution in 68
% of his patients.
Sex Distribution
Males were predominantly prone to fracture shaft of femur due to high
incidence found in motor vehicular accidents. 80% (16 patients) of our
patients were male (Table-2).
Wiss – Fleming13
(1986) Male predominance (83.7%) found in his 111
patients series.
Alho et al96
(1991) reported 55% male predominance in 120 patients
Mode of Injury and Associated Injuries
Our study had vehicular accident as the main cause of fracture of femoral shaft
i.e. 85 % (17 patients)(Table 3).
Winquist et al28
also had 77% of cases because of motor vehicular accidents.
This observation by various authors implies that fracture shaft femur is usually a
result of high energy trauma. So it is commonly associated with other injuries.
In our series 9 patients (45%) had associated injuries.
We had 1 abdominal injury (5 %), 1 head injury (5%), other fractures in 7
patients(35%) ( table 4).
Winquist et al28
in his study observed nearly same percentage of associated
injuries as in our study (30%).
White et al32
observed 76% of his cases were associated with other injuries.
Jensole Sojbjerg et al97
observed 50% of cases were associated with other
injuries.
Site of Fracture
Femoral shaft is divided into 3 segments upper, middle and lower third. M/3rd
femoral shaft was more commonly fractured in our series i. e. 55%(11 patients).
Same segment was observed to be involved in other series.
In our series there were 5 patients had a fracture in lower 3rd
i. e 25 % and 4
patients had in upper 3rd
i. e 20% (Table 5)
Thoresen et al31
in his study of 48 cases reported 50% of fractures of M\3rd
Wiss et al13
reported 50% cases in111 patients.
Alho et al96
1991 reported 56.9% of M\3rd
.in 120 cases.
Fracture Pattern
Our study had comminuted (50%) as a commonest fracture pattern where as
20% were of Transverse and 15% were fracture with Butterfly fragment were noted
(Table 6).
Klemm-Borner12
1989 showed comminuted 40.6%, Butterfly 21.1%,
Transverse16.4% in in293 patients.
Wiquist Hansen Classification28
Our study had Winquist type II 50% (10 patients), type I 40% (8 patients),
type III 10%.(2 patients) (Table 7)
Lhowe35
1984 reported type III 36%, type I 29%, type II 21% type IV 14% in
67 cases.
Brumback2 (1988) showed Winquist type III as commonest 52%, type II 20%,
IV 18% & I 10% in 81 cases.
Open and Closed Fractures
Our study included 7 compound fractures, (35%) out of which 5 were Gustillo
Anderson Grade I (25%) and 2 were Grade II (10%, Table 8).
Christie et al34
showed 16.6% open of which 6.6% were Grade I. 3.3% were
Grade II 6.6% in 117 cases.
Alho, Stromsoe96
(1991) had 12.2% open, of which 6.5% were Grade I, 4%
were Grade II and 1.6% were Grade III in 120 cases.
Grade I fractures were treated with interlocking nail after wound healing.
Grade II fractures were treated with debridement and antegrade open
interlocking nail in same setting. Total 2 patients were treated with open technique .
1st patient due to various causes was operated after 48hrs. of injury. Union was
observed after 19 wks . 2nd
patient with grade II injury came 8 days after injury at our
institution. According to patient outside debridement was done on 2nd
day of injury
without general anaesthesia. Debridement and open interlocking was done within 24
hrs. at our institution. The bone united with exuberant callus formation at 21wk.
A biological technique of minimal open reduction was used. There was minimal
handling and devitalisation of soft tissue and muscle attachments of the fragments
were meticulously preserved.98
Closed and open nailing
Closed nailing is definitely superior to open nailing.11,8
We had both cases of Gustillo Anderson compound Gr II injuries operated after
48 hrs. of injury with open nailing. There was no evidence of infection in our study.
(Table 9)
Johnson et al82
reported 13% infection rate with open nailing in 88 patients.
Wiss et al13
reported 8.3% of infection rate in 111 patients.
Felon G et al99
suggested early debridement of the wound and emphasized
adequacy of initial debridement.
Reaming
Intramedullary nailing of femoral shaft fracture without reaming results in a
significantly higher rate of nonunion compared with intramedullary nailing with
reaming91
All our cases were reamed irrespective of open or closed fractures. There were
2 cases of infection.
Pankovich100
reported unreamed intramedullary fixation of 9\13 open femoral
fractures with no infection rate.
Chapman101
reported open fractures treated with delayed (10-14 days)
reamed nailing with no infection.
In one patient hematoma, with fluctuation, was observed on 2nd
postoperative
day.
Hematoma could be due to excessive reaming. To avoid chances of infection,
some hematoma was aspirated102
. The fracture united at16 wks.
Malik et al103
reported 3.8% incidence of deep infection, in his study of 214
long bone fractures (30 open).
Healing Time
95% of patients in our series achieved union (19 patients). The average time
for healing of the fracture in our series was 18.53 wks. Different time period for
union was shown when fracture was treated with open and closed nailing procedure.
We found slower union in open nailing (20 wks) as compared with closed nailing
(18.35 wks)(Table-10)
Winquist et al had union rate of 99.1%
White et al observed union rate of 99%.
White et al showed 16 wks.
Winquist et al showed 13 wks of healing time.
Kenneth et al27
had 13.8 weeks union period.
Blumberg et al37
also mentioned 13 weeks of union time in 73 cases.
Commencement of non – weight bearing (NWB)
In our series(Table 11) non-weight bearing crutch walking was begun early in
18 cases (90%) between 1st
-3rd
post operative day, except in 2 patients (10%). The
1st patient who had an associated humerus fracture had developed vulval edema on
1st post operative day and had an internal rotation deformity which was corrected on
5th
postoperative day so non-weight bearing crutch walking was started on 10th
day .
Another patient had ipsilateral lateral malleolus fracture so crutch walking was
started on 14th
day.
Partial weight bearing(PWB)
In our series (Table 12) partial weight bearing with walker was started
between 3-10 days in 18 cases (90%). One patient had ipsilateral lateral malleolus
fracture. He was allowed to bear partial weight after 24 days and the other patient
had humerus fracture who started partial weigh bearing after 21 days.
Average time for partial weight bearing in our study was 6.45 days.
Full weight bearing
In our series (Table 13) 4 patients started full weight bearing at 10th
week. 9
patients were able to bear full weight at 12th
week. 4 patients at 14th
week and 2 at
16th
week.
Average time of full weight bearing was 12.4 weeks. 1 patient who developed
deep infection (osteomyelitis) at 12 wks and later non union was unable to bear full
weight.
Dynamisation
In our series, (table 14) we performed dynamisation of 2 cases, at average 13.7
wks after primary procedure. In both cases union occurred at 9 wks on an average
after dynamisation and one case with final 1cm shortening.
Wucc et al41
studied the effect of dynamisation on slow healing. He
performed dynamisation at 16 weeks on an average after statically interlocked nailing.
58% of his dynamised cases healed after 22 weeks. 20% of his dynamised cases had
more than 2 cm shortening and 10 out of 28 cases went into non-union inspite of
dynamisation.
Brumback et al2 concluded his study on union in statically interlocked nails
stating that conversion of static mode into dynamic mode is rarely necessary as most
statically locked fractures healed.
Injury- Surgery Interval
Interval between injury and surgery in our series was between 3 to 10 days.
Average 6.20 days (Table-15). The compound fracture (Grade II) were thoroughly
debrided and open interlocking was done in the same setting. Head injury patients
were operated after fitness was given by Neurosurgeons.
Lhowe Hansen35
treated 67 open fractures with average injury surgery
interval of 7 hrs.
Hanks104
(1986) reported it as 7.4 days
Blumberg37
(1990) reported it as 3.5 days in 73 patients.
Operative Time
The operative time ranged from 2-3 hrs (Avg.170.5 min). In our earlier
patients maximum time was required for distal locking. However, with increasing
familiarity with technique and implant distal locking was done earlier later on.
(Table-16)
In all our surgeries C-arm was used. So with the use of traction table reduction
was not a major problem.
Hoffmann and Sudkamp105
reported average operative time to be 2 hrs. with
the use of C-arm for closed reduction.
Lhowe35
in his series reported mean operative time of182 min in 67 patients.
Wiss13
had average time for static locking 3 hr 15 min in his111 cases in111
cases.
Hansen78
(1988) reported average 182 min. for locked intramedullary nailing.
Complications
Intraoperative complications (Table 17)
Intraoperative fracture was there in one of our cases, as reduction was not held
properly during nail insertion.
Christie et al34
reported intra operative comminution in 6 patients out of 117
patients(5.1 % ) due to wrong entry pont.
Alho et al96
reported 9 patients(7.5 %) in 120 cases with splintering of proximal
fragment
Rotational Deformity
In one patient there was internal rotation deformity of 10o observed on immediate
postoperative period. It was corrected after 5 days. Same patient developed vulval
oedema on 1st postoperative day for which catheterization was required. Catheter
was removed after 3 days when oedema was subsided. There was no any
complication observed.
Rotational control of unstable fractures can be very well achieved with locked
intramedullary fixation85
Rothwell106
reported 12% malrotation incidence with nonlocked fixation.
Wiss13
reported 7 % (8 patients) with 10o-30
o external rotation deformity in111
cases.
Winquist Hansen reported 7% with rotation deformities in type III and IV
comminuted fractures.
Christie34
reported 15o external rotation in 1 patient of his 117 patients study.
Lhowe35
reported in 2% of patients, in 67 cases.
Late Complications (Table 18)
Knee Range of movement
We had excellent knee range of movement in our cases. Early resumption of
range of movement exercises were started after surgery as per patient tolerance.
Seven patients had restricted range of movement of knee. Five patients had 120o
range of movement. One had compound Gustillo Anderson Gr II fracture shaft femur
which was united with exuberant callus formation. This could be the cause of
restricted range of motion (90o) due to Quadriceps adhesions. One had nonunion,
with range of movement less than 90o. Average knee range of movement in our study
was 120 degrees which is similar to those in other series.107, 31, 28
Wiss et al13
reported average knee flexion 125o with only 3 patients had less
than 90o flexion.
Shortening
In all, there was shortening in 2 patients (10%). 1cm shortening was noted in
1st patient (5%) and 2
nd patient had 2cm shortening (5%). For a patient with 2 cm
shortening, shoe raise was given and now patient is managing well, without any
difficulty in daily activities.
Interlocking nail has decreased incidence of the problem of shortening at the
fracture site, which was seen when conventional nailing was used for unstable
comminuted fractures.
Christie et al reported 2 patients (1.7 %) with more than 2 cm shortening both
had spiral fractures, which were dynamically locked, study of 117 patients.
Brumback in his study of 133 patients treated with Russel Taylor or Brooker
Willis Nail had 1 cm shortening in 2 patients and 1 patient had 2 cm shortening. All
were due to intraoperative fixation in a shortened position and not due to
postoperative loss of fixation.
Wiss 1985 reported 2.5% cases showing shortening in 117 patients.
Johnson27
reported shortening of 1-2 cm in 13% of cases.
Lhowe35
reported 7% cases with 1-2 cm shortening.
Infection
In our series, in one patient there was deep infection. She presented after 3
months of surgery with chronic osteomyelitis of femur. So implant removal was done
before fracture union and debridement was done. Cultures taken from the infection
site came positive for staphylococcus aureus. Daily dressing was started with thigh
supported in a brace. After a course of antibiotics, patient was offered for renailing.
Patient refused and now doing her daily activities with thigh in a brace. She is using a
walker .The range of movements with the brace is less than 90 degrees.
One patient developed superficial infection. Wound was debrided and
antibiotics were given. Wound healed completely.
Christie et al34
had 1 superficial infection, 14 patients had prolonged wound
discharge with no osteomyelitis.
Lhowe, Hansen78
had reported 67 open fractures treated by immediate nailing
with 5% wound seroma and 5% wound infection.
Klemm12
reported study of 293 patients with deep infection in 7 patients, 3 of
which were closed fractures.
Wiss13
reported only 1 superficial infection in 112 patients at the trochanteric
incision with no deep infection and no osteomyelitis.
Nonunion
In this series there was one case of infected nonunion, ( 5%)operated with
closed technique.
Nail was removed before union with debridement. After a course of antibiotics
patient was offered for nailing but she refused. Now patient is managing with a thigh
in a brace.
Rothwell106
in his study showed 6 % of non-union rate.
Alho et al96
had 0% rate with Grosse-Kempf nail in120 patients.
White et al32
has 1.1 % of nonunion with Brooker-Willis nail.
Delayed Union
In this series delayed union was seen in 2 patients. One dynamised at 14th
week. It was united well by 22 weeks. In other patient dynamisation was done at 14th
week and complete union was seen at 24th
weeks.
Christie et al34
reported delayed union in 2 patients (i.e.1.7 %) in 117
patients.
Klemm, Borner12
had 0.7% delayed union in 293 fractures.
Other complications
There was no case of femoral neck fracture, nail breakage, screw breakage,
lengthening, and medical complications like ARDS or pulmonary embolism
intraoperatively. There was no perioperative mortality.
Results
For evaluation of results in our series Thoresen et al classification system
was used.
We had 20 patients of which 12 patients had excellent results (60%) with full,
pain-free, function of the extremity.
We had 6 patients with good result (30%); 5 patients had range of motion 120o
and shortening of 2 cm was observed in 1 patients.

We had 1 fair result (5%) of a patient, with compound Gr. II injury with range
of motion 90o.
1 poor result (5%) had non union, with range of motion < 90o
with a thigh
supported in a brace.
So overall we had, 90% excellent to good result and 10% fair to poor results,
with non-union in one case.
Alho et al96
reported 63 % excellent results, 19.5% good results, 15.4 %fair
results and 1.6 % poor result in120 patients.
Thoresen et al31
reported 63.8 % excellent results,17 % good results,15% fair
results and 4.25 % poor results in his study of 48 cases.
CONCLUSION
Interlocking intramedullary nailing is a very effective and successful method of
definitive primary treatment, in most types of fractures of the shaft of the femur.
Interlocking nail is effective in controlling rotational and longitudinal forces that
act across the fracture site.
Interlocking nail provides strong fixation, rotational stability and earliest return to
functional status, as the rate of healing is good with this method.
It allows early weight bearing and reduced rehabilitation.
It allows resumption of knee range of movement exercises at early stage; so it is
possible to give good knee range of movement at the end. This is helpful
especially in polytrauma patients, for early mobility and to reduce morbidity and
mortality.
Supine position on traction table, with affected limb adducted, provides sufficient
access for the entry point. In our series closed reduction on traction table could be
achieved without skeletal traction.
Reaming and interlocking expands the scope of nailing, to include all segments of
femoral shaft.
Closed nailing is preferred over open nailing, due to its faster rate of healing.
During nail insertion, the reduction should be held properly, to avoid distal
cortical break.
Rotational alignment should be confirmed, before fixing the interlocking bolts to
avoid malrotation.
In compound fractures, the risk of osteomyelitis in relation to interval between
injury and the timing of debridement, considering our limited number of cases,
further evaluation is needed.
BIBLIOGRAPHY
1. Kempf I, Grosse A and Beck G: Closed locked intramedullary nailing — Its
application to comminuted fractures of the femur. J Bones & Joint Surg,
June1985; 67A(5): 709-720.
2. Brumback RJ, Lakatos R: Intramedullary nailing of femoral shaft fractures:
J. Bone Joint Surg Am., Nov.1988;70A(10): 92-4
3. Mast J: Planning Reduction Techniques in Fracture Surgery. New York,
Springer-Verlag, 1989.
4. Adams F (trans): The Genuine Works of Hippocrates, Baltimore. Williams &
Wilkins, 1939.
5. Solo Hall K, McCloy N: Cause and Treatment of Angulation of Femoral
Intramedullary Nails — Experimental Evidence on the Preferred Position of
the CloverLeaf Nail. Clin. Orthop., 2: 66-74, 1955.
6. Mathysen A: Du bage platre et deson application dans le traitement des
fractures, leige, 1854.
7. Kuntscher G: Intramedullary surgical technique and its place in orthopedic
surgery‖, J Bone & Joint Surg (Am), 1986; 47: 809-818.
8. Bucholz R, Jones A: Current concepts review - fractures of the shaft of
femur. J. Bone Joint Surg Am., 1991;73A:1561-1566.
9. Bucholz R, Rockwood & Green’s Fractures in Adults, 4th
Edn., Philadelphia
:Lippincott Williams and Wilkins,1996;1:2324-26.
10. Tarr R and Wiss DA: The mechanics and biology of intramedullary fracture
fixation. Clin. Orthop, 1986; 212: 10-17.
11. Anastopoulos G, Asimakopoulous A, Exarchou E, and Pantazopoulos:
―Closed interlocked nails in comminuted and segmental femoral shaft
fractures‖. J. Trauma, 1993;35(5): 772-775.
12. Klemm KW and Borner M: Interlocking nailing of complex fractures of the
femur and tibia. Clin Orthop, 1986; 212: 89-100.
13. Wiss DA, Fleming CH, Matta JM: "Comminuted and rotationally unstable
fractures of the femur treated with an interlocking nail". Clin
Orthop.,1986;212: 35-47.
14. Rush LV & Rush HL: Technique for longitudinal pin fixation of certain
fractures of the ulna and of the femur. J Bone & Joint Sung; 21: 619.
15. Weller S & Hontsch D: Medullary nailing of femur and tibia. Chapter- 4 in
Manual of Internal Fixation Techniques recommended by the AOASIF group,
3rd Edn, Muller ME, Allogwer M Ed., Spinger-Verlag, New York, 1990: 291.
16. Rokkanen P, Slatis P, Vankka E: Closed or open intramedullary nailing of
femoral shaft fractures. A comparison with conservatively treated cases. JBJS
Br., 1969;51B(2):30
17. Connolly JF, Dehne E and Lafokette B: Closed reduction and early cast
brace ambulation in the treatment of femoral fractues II. Results in one
hundred and forty-three fractures. J Bone & Joint Surg, 1973; 55A: 1581-99.
18. Mooney V: Cast bracing. Clin. Orthop.,1974;102: 159-166.
19. Jensen S, Johnson J, March A: Middle third femoral fractures treated with
medullary nailing or AO compression plating. J of Injury,1976;8:54
20. Reis ND et al : The infraisthmal fractures of the shaft of the femur. J. of
Injury, 1977;9:8-16.
21. Rothwell AG, Fitzpatrick CB: Closed Kuntschers nailing of femoral shaft
fractures A series of 100 consecutive patients. JBJS Br., 1978;60B(4):42
22. William C A, Gainesville: a fluted femoral intramedullary rod –
biomechanical analysis and preliminary clinical results. JBJS Am.,
Jun1978;60A(4):56-8
23. Magerl F, Wyss A, Brunner: Plate osteosynthesis of femoral shaft fractures
in adults. Clin. Orthop.,1979;138:62-73.
24. Aginsky J, Reis ND:The present state of medullary nailing of femur:
Biomechanical limitations and problems of blood supply to fracture due to
reaming. J of Injury, 1979;11:190-196
25. Seligson D, Harman K : Negative experience with pins in plaster for femoral
fractures. Clin. Orthop.,1979;138:243-245.
26. Montgomery SP, Mooney V: Femur fracture treatment with roller traction
and early ambulation. Clin. Orthop.,1981;156:196-200.
27. Johnson KD et al: comminuted femoral shaft fractures treated by roller
traction circle wires and intramedullary nail on an interlocking intramedullary
nail. JBJS Am., Oct. 1984;66A:68
28. Winquist RA and Hansen ST: Communuted fractures of the femoral shaft
treated by intramedullary nailing. Orthop Clin North Am, 1980; 11: 633.
29. Marion CH, Carson WL: Curvature of the femur and proximal entry point
for an intramedullary rod. Clin. Orthop.,1985;220:115-161.
30. Marion CH: fracture of femur treated with open and closed medullary nailing
using the fluted rod. JBJS Am,1985;67A:699-708.
31. Thoresen BO, Alho A, Ekel A et al : Interlocking intramedullary nailing in
femoral shaft fractures: report of 48 cases. JBJS Am., 1985; 67A(9): 1313-20.
32. White GM, Healy WL, Brumback RJ: The treatment of fractures of the
femoral shaft with the Brooker -Wills distal locking intramedullary nail. JBJS
Am., July 1986;68A(6):28-34
33. Huckstep RL: The Huckstep intramedullary compression nail, indications,
technique and results. Clin. Orthop.,1986;212:48-61.
34. Christie J, Court Brown C, Kinninmonth AW, Howie C: intramedullary
locking nails in the management of femoral shaft fractures. JBJS
Br.,1988;70B:206-210.
35. Lhowe DW: Immediate nailing of open fracture of the femoral shaft, JBJ
Surg, 1988; 70A: 812-820.
36. Donald A Wiss et al: Interlocked nailing for treatment of segmental fractures
of the femur. JBJS (Am), June 1990; 72A: 724-728.
37. Blumberg KD, Foster WC, Blumberg JF: A comparison of Brooker Wills &
Russel Taylor nails for treatment of fracture femoral shaft. J. Bone Joint Surg
Am., Aug 1990; 72A:1019-1024.
38. Covey D C, Saha Subrata: Biomechanical comparison of slotted and non
slotted nails in distal femoral shaft fractures. Clin. Orthop., 1990;252:246-251.
39. Stambough JL, Hopson CN, Cheeks ML: Stable and unstable fractures of
the femoral shaft. Orthop Rev., 1991 Oct; 20(10): 855-61.
40. Gregory P, DiCicco J, Karpik K, DiPasquale r, Hercovici D, Sanders R:
Ipsilateral fractures of the femur and tibia: Treatment with retrograde femoral
nailing and unreamed tibial nailing. J. Orthop Trauma, 1996; 10(5): 309-16.
41. Wu CC: The effect of dynamization on slowing the healing of femur shaft
fractures after interlocking nailing. J. Trauma, 1997 Aug; 43(2): 263-7.
42. Clatworthy MG, Clare DI et al: Reamed versus unreamed femoral nails a
randomized prospective trial JBJS Br., May1998;80B(3):76
43. George P, Lindsey RW, Noble PC, Alexander JW, Kamaric E: Optimal
location of a single distal interlocking screw in intramedullary nailing of distal
third femoral shaft fractures. J. Orthop Trauma, 1998 May; 12(4): 267-72.
44. Philip D Hajek: The use of one compared with two distal screws in the
treatment of femoral shaft fracture with interlocking intramedullary nailing.
JBJ Surg, 1991; 73A: 332-340.
45. Furlong AJ, Gainnoudia PV, Deboer P, Mathews SJ, MacDonald DA,
Smith RM: Exchange nailing of femoral shaft aseptic non-union. Injury, May
1999; 30(4): 245-9.
46. Wolinsky PR, McCarty E, Shyr Y, Johnson IC: Reamed intramedullary
nailing of the femur: 551 cases. J. Trauma, 1999 Mar; 46(3): 392-9.
47. Debrauwer S, Hendrix K, Verdonk R: Antegrade femoral nailing with a
reamed interlocking titanium alloy nail. Acta Orthop Belg, 2000 Dec; 66(5):
484-9.
48. Torentta P: Reamed versus non-reamed antegrade femoral nailing. Journal of
Orthopedic Trauma, Jan 2000; 14(1): 15-9.
49. Hak DJ, Lee SS, Goulet JA: Success of exchange reamed intramedullary
nailing for femoral shaft non-union or delayed union. J. Orthop Trauma, 2000
Mar-Apr; 14(3): 178-82
50. Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed
versus non-reamed. J. Am. Orthop Surg, 2000 Mar-Apr; 8(2): 83-90.
51. Hossam ElShafie M, Adel Morsey H, Emad Eid Y: Ipsilateral fracture of
the femoral neck and shaft — Treatment by reconstruction interlocking nail:
Arch Orthop Trauma Surg, 2001; 121(1-2): 71.
52. Torenta P: Antegrade or retrograde reamed femoral nailing — A prospective
randomized study. Journal of Bone and Joint Surgery — British Volume, July
2000; 82(5): 652-4.
53. Momberger N, Stevens P, Smith 3, Santora S, Scott S, Anderson J:
Intramedullary nailing of femoral fractures in adolescents. J Pediatr Orthop,
2000 Jul-Aug; 20(4): 48204.
54. Lin J, Lin SJ, Chen PQ, Yang SH: Stress analysis of the distal locking
screws for femoral interlocking nailing. J Orthop Res. 2001 Jan; 19(1): 57-63.
55. Arazi M, Ogun TC, Oktar MN, Memik R, Kutlu A: Early weight- bearing
after statically locked reamed intramedullary nailing of comminuted femoral
fractures: Is it a safe procedure? J. Trauma, 2001 Apr; 50(4): 711-6.
56. Pihlajamaki, Harri K, Salminen Sari T, Bostman Ole M: The treatment of
non-unions following intramedullary nailing of femoral shaft fractures.
Journal of Orthopedic Trauma, 2002 July; 16(6): 394- 402.
57. Nork Sean E, Agel Julie MA, Russell George V, Mills William J, Holt
Sarah MPH, Rout ML Chip Jr: Mortality after reamed intramedullary
nailing of bilateral femur fracture. Clinical Orthopedics & Related Research;
2003 Oct; 1(415): 272-278.
58. Chen Chin En, Ko Jih Yang, Wang Jun Wen, Wang Ching Jen: Infection
after intramedullary nailing of the femur. Journal of Trauma Injury Infection
& Critical Care, 2003 Aug; 55(2): 338-344.
59. Schipper IB, Steyerberg EW, Castelein RM, Van der Heljden FH WM,
Den Hoed, PT Kerver, AJH, Van Vugt AB: Treatment of unstable
trochanteric fractures: Randomized comparison of the gamma nail and the
proximal femoral nail. Journal of Bone & Joint Surgery — British Volume,
January 2004; 868(1): 86-94.
60. Wolinsky Philip: Reamed femoral nailing and the systemic inflammatory
response. Techniques in Orthopedics, 2004 March; 19(1): 25-29.
61. Wong T C: Retrograde nailing of femoral shaft fracture in patients with hip
arthrodesis. Singapore Med J, 2004;45(2): 85-87
62. Tigani D, Fravisini M, Stagni C, Pascarella R, Boriani S: Is dynamization
always necessary? Archive of Orthop&Trauma Surg, 2005;29(2):94-98
63. Meena RC, Kundnani V, Hussain Z: Fracture of the shaft of the
femur:Close vs open interlocking nailing. Indian J Orthop, 2006;40:243-6
64. Ogbemudia AO, Enemudo R, Edomwonyl E: Closed interlocked nailing of
a fractured femur without X-ray guide in 1st trimester pregnancy: A Case
Report. The Internet Journal of Third World Medicine, 2007;5(2):58-62
65. Wu Chia-Chieh, Yu Chen-Tung, Hsieh Chen-Pu, Chen Shih-Jen, Chang
Inglin: Femoral head avascular necrosis after interlocking nailing of a femoral
shaft fracture in a male adult: A Case Report. Archive of Orthop&Trauma
Surg, April 2008;128(4):399-402
66. Whittle AP: Fractures of lower extremity. Chapter-47, Cambell’s Operative
Orthopedics, 9th Edn., Vol. 3, Mosby, 2136-2179.
67. Starr AJ and Bucholz RW: Fractures of the shaft of femur. Chapter- 41,
Rock Wood & Green’s Fractures in Adults, 5th Edn., Vol. 2, Lippincott
Williams and Wilkins, 1683-1730.
68. Trueta J, Cavidias AX: ―Vascular changes caused by the kuntscher type of
nailing‖. JBJS Br., 1955;37B: 492-505.
69. Muller M, Allgower M, Schneider R, Willenegger H, Manual of internal
fixation, 3rd
edition, Berlin:Springer,1991:138-139.
70. Gustillo RB, Anderson JT: Prevention of infection in the treatment of one
thousand and five open fractures of long bones-Retrospective and prospective
analysis. JBJS Am., 1976;58A:453.
71. Connolly JF and King P: Closed reduction and early cast brace ambulation
in the treatment of femoral fractures. An in vivo quantitative analysis of
immobilization in skeletal traction and cast brace. J Bone & Joint Surg, 1973;
55A: 1559.
72. Mooney V, Nickel VL, Harvey JP Jr and Snelson R: Cast brace treatment
for fractures of the distal part of femur: A prospective controlled study of one
hundred and fifty patients. J Bone & Joint Surg; 1970; 52A: 1563.
73. Scudese Va: Femoral shaft fractures: Percutaneous multiple pin fixation, thigh
cylinder plaster cast and early weight bearing. Clin Orthop, 1971; 77: 164.
74. Alonso J, Geissler W, Hughes JL: External fixation of femoral fractures:
Indication and Limitations. Clin Orthop, 1989; 241: 83-88.
75. Dabezies EJ, D’Ambrosia R and Shoji H et al: Fractures of the femoral
shaft treated by external fixation with a wagner device. 3 Bone & Joint Surg.
Am. 1984; 66: 360-364.
76. Kessler SB, Hallfeldt KKJ, Perren SM and Schweiberer L: The effects of
reaming and intramedullary nailing on fracture healing. Clin Orthop, 1986
Nov; 212: 18-25.
77. Ruedi JP and Luscher JN: Results after internal fixation of comminuted
fractures of the femoral shaft with DC plates. Clin Orthop, 1979; 138: 74.
78. Hansen ST Jr and Lhowe DW: Diaphyseal fractures of the femur. Operative
Orthopedics, 2nd Edn., Chapman MW, JB Lippincott Company, 1993; 637-
650.
79. Kempf I, Grosse A and Rigaut P: The treatment of non-infected
pseudoarthrosis of the femur and tibia with locked intramedullary nailing. Clin
Orthop, 1986; 212: 142-154.
80. Kyle RF: Biomechanics of intramedullary nailing in fracture fixation. Orthop,
1985; 8:1356-1359.
81. Venkat S: Interlocking nails — A new era in fracture management‖. Chapter-
7, in Recent Advances in Orthopedics-II, 1st Edn., Kulkarni GS, Edn., JayPee
Brothers, New Delhi, 1997; 153-179.
82. Tenser A, Johnson K, Sherman M:Biomechanical considerations in
intramedullary techniques. J of Orthopaedics, 1988;3: 1-5
83. Brumback R, Ellison T, Poka A, Bathon G, Burgess AR: Intramedullary
nailing of femoral shaft fractures (III) :long term effects of static interlocking
fixation J. Bone Joint Surg Am, 1992 Jan;74A(1):106-112.
84. Rhinelander FW: Effects of medullary nailing on the normal blood supply of
diaphyseal cortex. Clin Orthop, 1998; 350: 5-17.
85. Russell TA: "Biomechanical concepts of femoral intramedullary nailing". Int.
J Orthop Trauma,1991;1:35.
86. Allen WC, Piotrowski G, Burstein AH, and Frankel VH: ―Biomechanical
principles of intramedullary fixation‖. Clin Orthop., 1968;60: 13-20.
87. Thakur AJ, The elements of fracture fixation ,2nd
Edn., New York: Churchill
Livingston ,1997:15.
88. Taylor JC, Russel TA: Clinical results of 100 femoral shaft fractures treated
with the Russell Taylor interlocking nail system. Annual meeting of American
Academy of Orthopaedic Surgeons, San Francisco, California, January 26,
1987.
89. Barron SE, Robb RA, Taylor WF: The effect of fixation with
intramedullary rods and plates on fracture site blood flow and bone
remodeling in dogs. J. Bone Joint Surg Am., 1977;59A: 376.
90. Holden EEA: Role of blood supply to soft tissue in the healing of diaphyseal
fractures. JBJS,1972 July;54A:993-1000.
91. The Canadian Orthopaedic Trauma Society: Results of a Multicentre
randomized clinical trial. JBJS Am., Nov 2003;85A(11):2093-95.
92. Webb LX, Winquist RA and Hansen ST: Intramedullary nailing and
reaming for delayed union or non-union of the femoral shaft. A report of 105
consecutive cases. Clin Orthop, 1986; 212: 133-141.
93. Rhinelander FW: Effects of medullary nailing on the normal blood supply of
diaphyseal cortex. In AAOS instructional course lectures, St. Louis, CV
Mosby, 1973: 161.
94. Wozasek GE, Simon P, Redl H, Schlag G: Intramedullary pressure changes
and fat intravasation during intramedullary nailing: an experimental study in
sheep. J Trauma, 1994 Feb;36(2):202-7
95. Wenda K, Ritter G, Degreif J, Rudigier J: Pathogenesis of pulmonary
complications following intramedullary nailing osteogenesis., JBJS,
September 1988;91(9): 432-5.
96. Alho A, Stromsoe K, Ekeland A: Locked intramedullary nailing of femoral
shaft fractures. Journal of trauma, 1991;31: 49-59
97. Sojbjerg J, Ciskjaer Soren et al: Locked nailing of comminuted and
Unstable fractures of the femur. JBJS Br., Jan1976;72B(1):28.
98. Leightor RK, Waddell JP, Kellam JF, Orrell KG: Open v\s Closed
intramedullary nailing of femoral shaft fractures. J. Trauma,1986;26:923-926.
99. Felon G, Borton D, Kumar R: Management of Compound Fractures: The
crucial timing of soft tissue coverage by early plastic surgical intervention.
RCSI Orth. Journal, July 2000;5:20
100. Pankovich AM: flexible intramedullary nailing femoral shaft fracture.
CORR,1981;160:185
101. Chapman MW: The role of intramedullary fixation in open fractures. Clin.
Orthop., 1986;12:212-35.
102. Leunig M, Hertel R: Thermal necrosis after tibial reaming for intramedullary
nail fixation. A report of 3 cases. J. Bone Joint Surg Am., 1991;77A:1247-
1251.
103. Malik MH, Horwood P, Diggle P, Khan SA: Factors affecting rates of
infection and non union in intramedullary nailing. JBJS Br., 2004
May;86(4):556-60.
104. Hanks GA, Foster WC, Cordea JA: Treatment of femoral shaft fractures
with the Brooker Willis interlocking intramedullary nail. Clin.
Orthop.,1988;226: 206-218.
105. Hoffmann R, Sudkamp NP: Internal fixation of proximal femoral fractures
with the AO / ASIF unreamed femoral nail and its modular locking system. J.
Trauma, 1993;38: 440-454.
106. Rothwell AG: Closed Kuntscher nailing for comminuted femoral shaft
fractures. JBJS Br;76B(2):12-16.
107. Schatzker J: open intramedullary nailing for fracture femur.
OCNA,1992;81(2):26





























