Embed Size (px)
Citation preview

Tampere University Dissertations 441
Genetics of Inflammatory Mediators of Atopy and
Asthma in Adults
KATI ÅDJERS


i
Tampere University Dissertations 441
KATI ÅDJERS
Genetics of Inflammatory Mediators of Atopy and Asthma in Adults
ACADEMIC DISSERTATION To be presented, with the permission of
the Faculty Council of the Faculty of Medicine and Health Technology of Tampere University,
for public discussion in the Jarmo Visakorpi auditorium of the ARVO building, Arvo Ylpön katu 34, Tampere,
on 13 August 2021, at 12 o’clock.

ii
ACADEMIC DISSERTATION
Tampere University, Faculty of Medicine and Health Technology Finland
Responsible supervisor
Professor (emeritus) Mikko Hurme Tampere University Finland
Supervisor Docent Jussi Karjalainen Tampere University Finland
Pre-examiners Docent Terttu Harju University of Oulu Finland
Docent Varpu Elenius University of Turku Finland
Opponent Professor Johannes Savolainen University of Turku Finland
Custos
Professor Olli Silvennoinen Tampere University Finland
The originality of this thesis has been checked using the Turnitin OriginalityCheck service. Copyright ©2021 author Cover design: Roihu Inc.
ISBN 978-952-03-2028-7 (print) ISBN 978-952-03-2029-4 (pdf) ISSN 2489-9860 (print) ISSN 2490-0028 (pdf) http://urn.fi/URN:ISBN:978-952-03-2029-4
PunaMusta Oy – Yliopistopaino Joensuu 2021

iii
To my family

iv

v
ACKNOWLEDGEMENTS
This study was carried out at the Department of Microbiology and Immunology of the Medical School of the University of Tampere, Finland. I owe a debt of gratitude to my supervisor Professor Mikko Hurme for granting
me the opportunity to prepare this dissertation. The elaboration and implementation of this project would have been impossible without him. I want to express my most profound gratitude to Docent Jussi Karjalainen, also
my supervisor, for friendly guidance, patience, and the learning opportunities he has provided me. I would never have completed this project without him and cannot thank him enough! I want to thank Professor Olli Silvennoinen for his valuable contribution. I also
express my thanks to Professors Heikki Hyöty and Hannu Kankaanranta for their collaboration. I am most grateful to the official reviewers of this thesis, Docents Terttu Harju
and Varpu Elenius. Thank you for your invaluable time. Your comments and concerns have improved this thesis immeasurably. I also thank Docent Sanna Toppila-Salmi, Docent Tanja Pessi, Miia Virta, PhD,
Carita Eklund, PhD, and all the co-writers of the studies for their valuable contributions. I also express my sincere thanks to Heini Huhtala, MSc, for her guidance in statistical matters. Further, I thank Ms Sinikka Repo-Koskinen and Ms Eija Spare or their work in the laboratory at the Department of Microbiology and Immunology. My sincere thanks go to all colleagues and friends at the Department of
Ophthalmology of Tampere University Hospital and other locations for encouraging me to complete this dissertation. I also want to thank Carolyn Brimley Norris, PhD, for language revision of my
thesis and for patiently teaching me academic writing. I am happy to thank my mother Eija and father Jukka for their endless support.
I also want to thank our beloved daughters Emilia and Matilda for bringing joy and happiness to my life during these years. I finally express my deepest gratitude to my husband, Pasi Ylitepsa, MD, for his love, patience, and support.

vi
This study received financial support from the Finnish Medical Society Duodecim, the Finnish Society of Allergology and Immunology, the Jane and Aatos Erkko Foundation, the Finnish Cultural Foundation, the Tampere Tuberculosis Foundation, the Väinö and Laina Kivi Foundation, and the Yrjö Jahnsson Foundation, the Finnish Anti-Tuberculosis Association Foundation, the Ida Montin Foundation, the Research Fund of Tampere University Hospital, the Academy of Finland, and the Rehabilitation Fund of the Finnish Social Insurance Institution.
Pirkkala, May 2021
Kati Ådjers

vii
ABSTRACT
The prevalence of atopic disorders such as asthma, allergic rhinitis and allergic conjunctivitis in many populations is close to 30% and has continued to increase in many developed countries, causing a major burden on the individuals, their health care systems, and on society. The biological bases of these disorders and of atopy in general have undergone investigation to a great extent, but many aspects still need clarification, for example in order to target novel therapies to patients who would benefit. Our studies examined whether functional single nucleotide polymorphisms of
candidate genes IL1A, IL4RA, TLR4, IL4, and NOS3 exert their effects individually on the risk or severity of atopy or asthma, or whether two polymorphisms of different candidate genes show an interactive effect. The aim was also to observe factors associated with polymorphism rs20541 of IL13 and other factors with or without allergic comorbidities such as subject-reported allergic rhinitis and allergic conjunctivitis symptoms in adult asthma patients. A total of 1,156 asthma patients and 1,792 non-asthmatic subjects as controls
participated in our studies, all of them having participated in a Finnish population-based case-control study conducted to investigate the risk factors and predictors of the outcome of adult asthma. Inclusion criteria for subjects with asthma were age over 30 years and entitlement to special reimbursement for asthma medication from the Social Insurance Institution of Finland. Allergic rhinitis and conjunctivitis were defined by questionnaire. Of the participants 245 asthma patients and 405 matched control subjects were tested for atopic status by skin prick tests and by measurement of serum IgE levels, and we also determined variety of polymorphisms of candidate genes previously linked to atopy or asthma. We demonstrated in our non-asthma control group, which represented the
general population reasonably well, an epistatic effect on atopy between IL1A and IL4RA genes. The predisposing combination was the carrier status of genotype TT of IL4RA +22446 and genotype GG of IL1A +4845. An increased risk for asthma appeared in the female carriers of allele G of TLR4 +896 and allele T of IL4 -590. Additionally, an epistatic effect of allele T of NOS3 +894 and genotype GG of IL1A +4845 influenced degree of atopy. We also showed that allele A of IL13 rs20541

viii
affected the risk for allergic rhinitis and conjunctivitis in asthma patients. In addition, carriers of allele A of IL13 rs20541 were predisposed towards multisensitization in asthma. Our findings suggest that gene-gene interactions affect susceptibility to atopy and
asthma as well as severity of atopy in Finnish adults. Even if single nucleotide polymorphisms of candidate genes show no individual effects, two separate polymorphisms can potentiate the effects of each other, predisposing carriers of certain allele combinations to clinical manifestations. An effect of TLR and IL4 genes was apparent only in female subjects, indicating sex-dependent differences in the body’s defense mechanisms. Our results indicate that key features of adult atopic asthma phenotype may be high prevalence of the allele A of IL13 rs20541, a multisensitization pattern, and allergic rhinitis and conjunctivitis symptoms.

ix
TIIVISTELMÄ
Atooppisten sairauksien kuten astman, allergisen nuhan tai sidekalvotulehduksen esiintyvyys on monissa väestöissä jopa 30 % ja ainakin kehittyvissä maissa edelleen lisääntymässä. Kyseisistä sairauksista aiheutuu sekä yksilölle että yhteiskunnalle merkittäviä haittoja ja kustannuksia. Sairauksien genetiikkaa, immunologiaa, patofysiologiaa ja ympäristötekijöitä on tutkittu laajalti, mutta edelleen lisää tietoa tarvitaan, jotta osataan esimerkiksi kohdentaa uusia hoitomuotoja niistä eniten hyötyville. Tutkimuksissamme selvitimme, vaikuttavatko funktionaalisten
kandidaattigeenien IL1A, IL4RA, TLR4, IL4 ja NOS3 yhden nukleotidin polymorfismit joko yksin tai yhdessä atopiataipumukseen, atopian vaikeusasteeseen tai riskiin sairastua astmaan. Tavoitteena oli myös selvittää, liittyvätkö IL13 geenin polymorfismi rs20541 ja allerginen nuha sekä allerginen sidekalvotulehdus aikuisiän astmaan. Tutkimuksiin osallistui 1156 iältään yli 30-vuotiasta astmaa sairastavaa ja 1792
kaltaistettua vertailuhenkilöä. Astmakriteerinä käytettiin Kelan myöntämää astmalääkkeiden erityiskorvausoikeutta. Allergisen nuhan ja sidekalvotulehduksen esiintyminen selvitettiin oirekyselyllä. Perinnöllisten tekijöiden vaikutusta selvitettiin kliinisesti tutkittujen 245 astmapotilaan ja 405 kaltaistetun vertailuhenkilon vaestopohjaisessa otoksessa. Tutkituille tehtiin ihopistotestit ja määritettiin seerumin IgE-tasot. Genotyypitykset aiempien tutkimusten mukaan mahdollisista astman tai atopian riskigeeneistä tehtiin aikaisemmin kuvattuja menetelmiä käyttäen. Tutkimuksissamme selvisi, että melko hyvin normaaliväestöä edustavien
vertailuhenkilöiden IL1A ja IL4RA geeneillä oli yhteisvaikutus (ns. epistaattinen vaikutus) atopiariskiin. IL1A-geenin polymorfismin +4845 genotyypin GG ja IL4RA-geenin polymorfismin +22446 genotyypin TT todettiin altistavan atopialle. Naisilla havaittiin vastaavasti astmariskin lisääntyminen TLR4-geenin polymorfismin +896 alleelin G ja IL4-geenin polymorfismin -590 alleelin T suhteen. NOS3-geenin polymorfismin +894 alleeli T ja IL1A polymorfismin +4845 genotyyppi GG vaikuttivat vastaavalla tavalla atopian vaikeusastetta lisäten. Totesimme myös IL13-geenin polymorfismin rs20541 alleelin A lisäävän allergisen nuhan ja

x
sidekalvotulehduksen riskiä astmapotilailla. Näillä potilailla myös esiintyi herkistymistä useammille allergeeneille ihopistokokeissa. Löydöksemme suomalaisilla aikuisilla astmapotilailla tukevat ajatusta, että eri
geenit vaikuttavat yhdessä atopiaan ja astmaan. Vaikka yksittäinen geeni ei vaikuttaisi taudille altistavasti, kahden eri geenin polymorfismit voivat vahvistaa toistensa vaikutusta ja altistaa molempien riskialleelien kantajat taudille. TLR4- ja IL4-geenien yhteisvaikutus havaittiin vain naisilla, mikä vahvistaa löydöksiä sukupuoliriippuvaisista eroista elimistön puolustusmekanismeissa. Tutkimuksemme mukaan IL13 geenin polymorfismin rs20541 alleeli A, herkkyys useille allergeeneille ihopistokokeissa sekä allergisen nuhan ja sidekalvotulehduksen oirekuva saattavat olla tärkeitä aikuisten atooppisen astman fenotyyppiin liittyviä tekijöitä.

xi
CONTENTS
1 Introduction .......................................................................................................................... 19
2 Review of the literature ....................................................................................................... 21 2.1 Atopy ......................................................................................................................... 21
2.1.1 Definition ............................................................................................... 21 2.1.2 Prevalence .............................................................................................. 21 2.1.3 Pathogenesis and phenotypes ............................................................. 22
2.2 Asthma ...................................................................................................................... 25 2.2.1 Definition ............................................................................................... 25 2.2.2 Prevalence .............................................................................................. 25 2.2.3 Phenotypes and pathogenesis ............................................................. 26
2.3 Allergic rhinitis ......................................................................................................... 30 2.3.1 Definition .............................................................................................. 30 2.3.2 Prevalence .............................................................................................. 30 2.3.3 Phenotypes and pathogenesis ............................................................. 31
2.4 Allergic conjunctivitis ............................................................................................. 31 2.4.1 Definition ............................................................................................... 31 2.4.2 Prevalence .............................................................................................. 32 2.4.3 Phenotypes and pathogenesis ............................................................. 32
2.5 Genetics of atopy and asthma ............................................................................... 35 2.5.1 Associated genes ................................................................................... 35 2.5.2 Interaction .............................................................................................. 37
2.6 Some inflammatory mediators previously associated with atopy and asthma ....................................................................................................................... 37 2.6.1 Interleukin-1 .......................................................................................... 37 2.6.2 Interleukin-4 .......................................................................................... 38 2.6.3 Toll-like receptor 4 ............................................................................... 39 2.6.4 Endothelial nitric oxide synthase (eNOS, NOS3) ........................... 41 2.6.5 Interleukin-13 ........................................................................................ 42
3 Aims of the study ................................................................................................................. 43
4 Subjects and methods ......................................................................................................... 44 4.1 Subjects ..................................................................................................................... 44 4.2 Methods .................................................................................................................... 45
4.2.1 Allergy testing ........................................................................................ 45 4.2.2 Genetic testing ....................................................................................... 45

xii
4.2.2.1 IL1A SNP +4845 (rs17561) ............................................. 46 4.2.2.2 IL4RA +22446 (rs1805012) ............................................. 46 4.2.2.3 TLR4 +896 (rs 4986791) .................................................. 46 4.2.2.4 IL4 -590 (rs 2243250) ....................................................... 47 4.2.2.5 NOS3 +894 (rs1799983) .................................................. 47 4.2.2.6 IL13 +2044 (rs 20541) ...................................................... 47
4.2.3 Statistical methods ............................................................................... 48
5 Results ................................................................................................................................... 49 5.1 Allergy tests and other atopic conditions ........................................................... 49 5.2 Polymorphisms ....................................................................................................... 51
5.2.1 IL1A and IL4RA .................................................................................. 51 5.2.2 TLR4 and IL4 ....................................................................................... 52 5.2.3 IL1A and NOS3 ................................................................................... 53 5.2.4 IL13 ........................................................................................................ 53
6 Discussion ............................................................................................................................ 55
7 Conclusions .......................................................................................................................... 62
8 References ............................................................................................................................ 63

xiii
ABBREVIATIONS
AC Allergic conjunctivitis AD Atopic dermatitis AKC Atopic keratoconjunctivitis AR Allergic conjunctivitis ARC Allergic rhinoconjunctivitis CD Cluster of differentiation DNA Deoxyribonucleic acid eNOS Endothelial nitric oxide synthase FeNO Fraction of exhaled nitric oxide FEV1 Forced expiratory volume in one second GWAS Genome-wide association scan IFN Interferon Ig Immunoglobulin IL Interleukin IL4R Interleukin 4 receptor ILC Innate lymphoid cells ILL Innate-like lymphocytes LAR Local allergic rhinitis LPS Lipopolysaccharide NERD NSAID-exacerbated respiratory disease NO Nitric oxide NOS Nitric oxide synthase NP Nasal polyposis PAC Perennial allergic conjunctivitis PCR Polymerase chain reaction PEF Peak expiratory flow SAC Seasonal allergic conjunctivitis SPT Skin prick test Th T helper TLR Toll-like receptor

xiv
TNF Tumor necrosis factor Treg Regulatory T cell TSLP Thymic stromal lymphopoietin VKC Vernal keratoconjunctivitis

xv
ORIGINAL PUBLICATIONS
The thesis is based on the following original publications, which are referred in the text by the Roman numerals I-IV.
Publication I Ådjers, K., Pessi, T., Karjalainen, J., Huhtala, H., & Hurme, M. (2004). Epistatic effect of IL1A and IL4RA genes on the risk of atopy. Journal of allergy and clinical immunology, 113(3), 445–447.
Publication II Ådjers, K., Karjalainen, J., Pessi, T., Eklund, C., & Hurme, M. (2005). Epistatic effect of TLR4 and IL4 genes on the risk of asthma in females. International archives of allergy and immunology, 138(3), 251–256.
Publication III Pessi, T., Ådjers, K., Karjalainen, J., Rontu, R., Hurme, M. (2006) The interaction of IL1A and endothelial nitric oxide synthase polymorphisms is associated with the degree of atopy. Journal of allergy and clinical immunology, 118(1), 246-8.
Publication IV Ådjers, K., Luukkainen A., Pekkanen, J., Hurme, M., Huhtala H., Renkonen R., Wang, D., Mäkelä, M., Karjalainen J., Toppila-Salmi, S. (2017) Self-reported allergic rhinitis and/or allergic conjunctivitis associate with IL13 rs20541 polymorphism in Finnish adult asthma patients. International archives of allergy and immunology, 172(2), 123-128.
The original publications are reprinted with the permission of the copyright holders.

xvi

xvii
AUTHOR’S CONTRIBUTION
I Kati Ådjers has performed the statistical analyses, interpreted the results, and written the manuscript.
II Kati Ådjers has participated in planning and performing the laboratory examinations, performed the statistical analyses, interpreted the results, and written the manuscript.
III Kati Ådjers has performed the statistical analyses, interpreted the results, and participated in writing the manuscript.
IV Kati Ådjers has participated in planning the study, performing some of the statistical analyses, interpreting results and writing the manuscript.

xviii

19
1 INTRODUCTION
The prevalence of atopic disorders, underlying bronchial asthma, allergic rhinitis (AR), allergic conjunctivitis (AC) and atopic dermatitis (AD), is close to 30 % in many populations and continues to increase in many developed countries, causing for those affected and their society a major burden. Determinants of atopic disorders are genetic and environmental factors. (Cookson, 1999; Rosenwasser, 1996) The gene–environment relationship can be captured in the phrase “genetics loads the gun and the environment pulls the trigger” (Turner, 2017). The genetics, immunology, pathomechanisms and environmental effects of atopic disorders and atopy in general have been under considerable investigation, with much left unknown. In addition, most of the studies have been performed in children with not all the phenotypes considered.
An interesting approach to learning about the mechanisms of allergic diseases involves searching for associations between the diseases and the functional polymorphisms of various genes, especially the ones coding for molecules involved in immune responses. Genome-wide association scans (GWAS) compare the DNA of individuals with the disease to DNA of individuals without it in order to discover which genetic variants are associated with the disease. Several GWASs on asthma, AR, atopy, allergy, and IgE have appeared. (Welter et al., 2014). GWASs do not, however, identify the causal variants associated with a disease, and the estimated cumulative genetic risk of the variants identified with asthma alone has been under 15% (Mathias, 2014). Despite the large number of candidate genes identified for asthma by GWAS and
basic research, few of those discoveries have been rigorously replicated. Several candidate genes examined have still failed later replication. This may be due to a variety of endotypes of asthma. In this dissertation, we investigated the effects of certain candidate genes
previously associated with asthma or atopy in a study group of Finnish adult asthma patients and non-asthmatic control subjects. We examined the polymorphisms of Interleukin (IL) 1A, Interleukin 4 receptor (IL4R) A, Toll-like receptor (TLR) 4, IL4

20
and endothelial nitric oxide synthase (eNOS, NOS3) and their interactions in atopy and asthma because of these genes’ biological importance. Factors associated with polymorphism rs20541 of IL13 and other factors with or without allergic comorbidities such as subject-reported AR and AC symptoms we also observed in adult asthma patients.

21
2 REVIEW OF THE LITERATURE
2.1 Atopy
2.1.1 Definition
Atopy can be defined (according to Joint Allergy Academies for ICD-11) as a personal or familial tendency to become sensitized and produce Immunoglobulin (Ig)E antibodies in response to ordinary exposures to allergens (Tanno et al., 2016). The skin prick test (SPT) serves as a means to examine IgE-mediated allergic responses, and the results are quite well in accordance with anamnestic data on atopy (Burrows et al., 1989). On many occasions, terminology is ambiguous, with the words “atopy” and
“allergy” incorrectly used as synonyms. Allergy is a hypersensitivity reaction initiated by proven or strongly suspected immunologic mechanisms; it can be IgE-mediated or non-IgE-mediated and triggered by substances to which the subject has been exposed and sensitized (Tanno et al., 2016). Atopic disorders typically affect the nose, eyes, skin, and lungs. These
include allergic asthma, allergic rhinitis, allergic conjunctivitis, atopic dermatitis, IgE-mediated drug allergy, IgE-mediated insect bites, urticaria and angioedema, and anaphylactic shock (Justiz Vaillant et al., 2020).
2.1.2 Prevalence
The prevalence of atopic diseases such as eczema and hay fever, determined by the symptoms, is almost 30% in many populations in spite of the use of self-reported diagnosis of different definitions (Asher et al., 2006; Barnish et al., 2015). Until recently, the prevalence of asthma, AR, and AD in many developed countries has been increasing (de Marco et al., 2012; Duggan et al., 2012; Gershon et al., 2010; Hansen et al., 2013). Hygiene level and socioeconomic conditions have improved simultaneously, alongside a decrease in the incidence of several infectious diseases

22
and biodiversity and an increase in the consumption of fossil fuels (Bach, 2002; Hanski et al., 2012; Shafiee et al., 2009). An association of adult-onset asthma and allergic multimorbidity decreases with
age: the proportion of allergic multimorbidity and allergic polysensitization among asthma patients increases with later decades of birth. More studies are essential to investigate whether this results from a cohort effect, i.e. change in host-microbiome-environmental interactions during development over time, or from an aging effect. (Lynch et al., 2016; Toppila-Salmi et al., 2019).
2.1.3 Pathogenesis and phenotypes
Research had already generated theories linking autoimmune disease and hygiene, but in 1989, Strachan proposed a theory, the “hygiene hypothesis,” based on studies of the relationship between hay fever and microbial infections in early childhood and adolescence (Blackley, 1959; Leibowitz et al., 1966; Strachan, 1989). Infectious diseases, especially gastrointestinal infections, during early childhood have reduced the risk of development of atopic diseases in later life. Conversely, the absence of infectious diseases increases risk. This has been assumed to explain the rapid increase in atopic diseases occurring in developed countries during recent decades. (Wills-Karp et al., 2001). The hygiene hypothesis holds that decreased biodiversity and improved hygiene in early life reduce microbial exposures essential in priming the immune response and protective against atopic disorders. This hypothesis has been expanded to cover asthma and autoimmune diseases. (Hanski et al., 2012; Okada et al., 2010). At cellular level, T helper (Th)1–Th2 deviation has served to explain the
protective influence of infectious agents of immunological disorders. These Th cells comprise two subsets, Th1 and Th2 based on the cytokine pattern they produce (Romagnani et al., 1997). Th1 T cells produce inflammatory cytokines such as IL-2, interferon (IFN)-γ, and tumor necrosis factor (TNF)-α; all function in cell-mediated immunity, whereas Th2 T cells that produce IL-4, IL-5, IL-6, and IL-13 contribute to IgE production and allergic responses. Differentiation of Th cells is under the influence of factors derived from infectious agents, factors such as bacterial lipopolysaccharide (LPS), and by the cytokine profile induced. The presence of these factors favors differentiation towards the Th1 direction; the absence of any stimuli, towards the Th2 direction. (Perussia et al., 2003). Considering the reciprocal down-regulation of Th1 and Th2 cells, the lack of microbial burden in early childhood in

23
developed countries, normally favoring a Th1-biased immunity, redirects the immune response towards the Th2 phenotype. As a consequence, this predisposes the host to allergy. (Okada et al., 2010). These observations are reasonably well in accordance with the concept of a
common mechanisms underlying microbiome-mediated protection against allergy and autoimmunity. Many hypotheses can explain the aspects of these mechanisms, including antigenic competition, immunoregulation, nonantigenic ligands, and gene-environment interactions. (Okada et al., 2010). Today, immune responses are classified into type 1, type 2, and type 3 immunity,
which refer to both the innate and the adaptive arms of the immune response. Type 1 effector responses can be defined by Th1 and Th17 cells, cytotoxic T cells, innate lymphoid cells (ILCs) 1 and 3, and IgM, IgA and specific IgG antibody classes. These mediate immunity to many microorganisms such as bacteria, viruses, fungi, and protozoa and help to maintain tumor immune surveillance. (Annunziato et al., 2015). On the other hand, type 2 immune responses include CD4+ Th2 cells, ILC2s,
eosinophils, basophils, mast cells, IL-4- and IL-13-activated macrophages, IgE, and IL-4, IL-5, IL-9, IL-13, thymic stromal lymphopoietin (TSLP), IL-25 and IL-33. Type 2 immunity protects against extracellular parasites by promoting barrier defences, helps to maintain metabolic homeostasis, and enhances tissue remodeling following injury. (Gause et al., 2013; Heredia et al., 2013; Nguyen et al., 2011; Urban et al., 1998; Wu et al., 2011; Wynn, 2004; Wynn et al., 2013). Although type 2 responses have important functions protecting the host, when dysregulated, chronic, or hyperreactive, they can contribute to the development of diseases, such as allergic disorders (Palm et al., 2012). Type 3 immunity seems to protect from extracellular bacteria and fungi. Type 3
immune responses consist of RORgt+ lymphocytes, CD4+ Th17 cells, CD8+ TC17 cells, ILC3s, IL-17 and IL-22. (Annunziato et al., 2015). Recently, what has become clear is that the commensal microbes colonizing the
gut, lung, and skin mediate regulatory effects on type 2 immune responses. In the absence of microbes, germ-free mice present with increased type 2 immune responses with elevated levels of IL-4, circulating basophils, serum IgE, and with higher susceptibility to allergy. (Cahenzli et al., 2013; Herbst et al., 2011; Hill et al., 2012; Mccoy et al., 2006). Cellular and molecular pathways are poorly known. Regulatory T cells (Tregs) seem to dampen the induction of type 2 immunity.
They are characterized by their capacity to secrete both IL-10 and transforming growth factor β (Chen et al., 1994). Tregs suppress the allergen-induced specific T cell activation and effector cells included in allergic inflammation, ones such as mast

24
cells, basophils, and eosinophils, and Tregs also inhibit IgE production (Akdis et al., 1998; Jutel et al., 2008; Meiler et al., 2008; Verhagen et al., 2006). The induction of IL-10-producing allergen-specific Tregs that express transcription factor FOXP3 seems to be the most important mechanism of allergen-specific immunotherapy. It plays an important role in the peripheral T cell allergy development against specific allergens that occurs during the traditional subcutaneous route of allergen immunotherapy (Akdis et al., 1998; Francis et al., 2003; Jutel et al., 2003; Savolainen et al., 2004). Synthesis of Treg-type cytokines such as IL-10 also occurs during sublingual immunotherapy (Bohle et al., 2007; Burastero et al., 2008; Cosmi et al., 2006; Savolainen et al., 2006). Microbial colonization induces intestinal Tregs (Atarashi et al., 2013; Geuking et
al., 2011; Lathrop et al., 2011). This happens through production of the short-chain fatty acids butyrate and propionate (Arpaia et al., 2013; Furusawa et al., 2013; Smith et al., 2013). Mice deficient in the FOXP3 enhancer conserved noncoding sequence 1 generate no microbially induced Tregs. As a consequence, they develop increased Type 2 responses and mucosal inflammation in the gastrointestinal tract and the lungs. (Josefowicz et al., 2012). Microbial control of type 2 immune responses seems also to involve other cell
types like epithelial cells, dendritic cells, ILCs, and other innate cell types. The amount of ILC2 in the lungs of germ-free and of colonized mice seems to be equal, indicating that their recruitment may not require microbial signals. (Monticelli et al., 2011) Instead, microbial control of intestinal macrophages and ILC3 plays a role in the induction of Tregs and is required to induce tolerance and to control reactivity to food antigens (Mortha et al., 2014). Several experiments indicate that infectious agents are able to protect against
allergic diseases through mechanisms independent of their constitutive antigens. This leads to stimulation of receptors that are not antigen specific. TLRs can illustrate this reasonably well. Considering the capacity of TLRs to stimulate cytokine production and immune responses, it can be assumed that stimulating them by infectious ligands would cause or exacerbate allergic responses. (Lang et al., 2005; Okada et al., 2010; Schaub et al., 2004). For a long time, allergic diseases and their associated clinical traits have been
recognized as being heritable. Twin and migration studies performed on families provide the earliest evidence for genetic contributions. (Coca et al., 1923; Davis et al., 1961; Duffy et al., 1990; Manolio et al., 2003; Palmer et al., 2000). Twin studies of eczema and hay fever suggest that hereditary factors explain up to 80% of these atopic conditions (Thomsen et al., 2006, 2007). Genetic factors play a major role in

25
predisposition to atopy. They regulate the total IgE synthesis and produce IgE antibodies to specific epitopes. The tendency to overproduce IgE depends on inheritance of several genes. However, the full inheritance pattern is known to be multigenic. (Qi et al., 2018). Atopic diseases sometimes develop as an atopic march. This gradually
development describes the progression of atopic disorders in children from AD in infants to AR and asthma later in childhood (Spergel et al., 2003). Some patients may have long-lasting disease whereas others may improve as they age (Spergel, 2010). The risk for developing atopic diseases is complex, and the pattern described in the atopic march is not always a simple progression; it applies to only some patients and has been under investigation predominantly in childhood asthma. Although these disorders share risk factors, the development of disease varies among individuals depending on genetics and environment (Cookson, 1999; Rosenwasser, 1996).
2.2 Asthma
2.2.1 Definition
Asthma is a heterogeneous disease commonly characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms underlying wheeze, shortness of breath, chest tightness, and cough that vary over time and in intensity, together with variable expiratory airflow limitation. This definition has been based on consideration of the characteristics that are typical of asthma before the commencement of controller treatment. These features distinguish it from other respiratory conditions. Nevertheless, one possibility is that airflow limitation becomes persistent later on in the course of the disease. (Global Initiative for Asthma, 2020).
2.2.2 Prevalence
Asthma is a chronic respiratory disease affecting 1% to 18% of the population and all age groups among countries. Its prevalence is still increasing. Some countries have, however, seen a decline in asthma hospitalizations and deaths (Haahtela et al., 2017). In Finland, the prevalence of asthma in adults has been estimated to be around 10% (Jousilahti et al., 2016). Asthma still imposes an unacceptable burden on

26
individuals, on health care systems, and on society. Despite the maximal medical therapy, the percentage of asthma patients who have severe disease and are symptomatic reaches 5% to 10 %. (Global Initiative for Asthma, 2020; Wenzel, 2006). The childhood prevalence of asthma is higher in boys. Nevertheless, the
prevalence is approximately 20% higher in women than in men, demonstrating a shift after puberty. (Almqvist et al., 2008; Carey et al., 2007; Leynaert et al., 2012). Moreover, potential genetic and hormonal contributors, as well as sex differences in concomitant conditions such as obesity and cigarette smoking may lead increased asthma risk (Raghavan et al., 2016). Besides asthma, the protective role of puberty has been apparent also in other allergic diseases, for instance, in vernal keratoconjunctivitis mainly occurring in boys and disappearing after puberty (Leonardi et al., 2012). Androgens produced by post-pubertal men generally suppress immune cell reactivity in a variety of systems, although the exact pathomechanisms are still quite poorly understood (Kissick et al., 2014; Klein et al., 2016; Kurukulaaratchy et al., 2011).
2.2.3 Phenotypes and pathogenesis
Asthma can be divided into many phenotypes traditionally defined on the basis of their relation to specific triggers, to immunopathology, or to clinical phenotype such as frequency of exacerbations or treatment resistance (Brightling et al., 2012). During the last few years, a strategy has been evolving to associate molecular mechanisms with phenotype: dividing asthma into endotypes which describe these distinct functional or pathophysiologic mechanisms at a cellular and molecular level (Kuruvilla et al., 2019). Cluster analyses have recently revealed considerable information on various asthma phenotypes and endotypes (Hsiao et al., 2019; Ilmarinen et al., 2017; Newby et al., 2014; Schatz et al., 2014; Wu et al., 2019). According to data from twin studies, data regarding phenotypic variability in
asthma severity, genetic factors determine approximately 25%. Nongenetic factors include environmental and psychosocial factors, behavioral traits, and comorbidities. (Thomsen et al., 2012). Various environmental exposures are associated with asthma. In the case of childhood asthma, these include respiratory viruses, especially rhino- and RSV viruses, exposure to second-hand smoke, to inhaled chemicals, mold, and ambient air pollutants, and also include some deficiencies in maternal diet (Bergroth et al., 2020; Dick et al., 2014; Jartti et al., 2019, 2020). In adult asthma, factors

27
associated with asthma risk include smoking, obesity, allergic conditions, inflammatory upper airway diseases, occupational exposure agents, residential dampness and mold, outdoor pollutants, psychosocial factors, and depression (Guarnieri et al., 2014; Jarvis et al., 2012; Karjalainen et al., 2002; Quansah et al., 2012; Siroux et al., 2019; Toppila-Salmi et al., 2015; Toppila-Salmi et al., 2019). Asthma has long been associated with atopy; it has traditionally been regarded as
an atopic condition, but factors unrelated to atopy have also emerged, ones proving to be important in disease development (Anderson, 2005; Zimmerman et al., 1988). Important causes of this non-atopic asthma include smoking, pollutants, and occupational-exposure agents, and non-atopic asthma can easily be more persistent than atopic asthma, with few obvious triggers other than infection. Viral respiratory infections can also trigger asthma in adulthood. (Anderson, 2005; Diamant et al., 2007; Rees et al., 2010). Atopic asthma generally starts in childhood or adolescence, with certain triggers that provoke wheezing. It is also frequently associated with a family history of allergic diseases. (Diamant et al., 2007; Townshend et al., 2007). The disease typically results from an allergic response to specific allergens such as house-dust mite, grass and tree pollen, and dander from domestic pets (Ward et al., 2010). This corticosteroid-dependent asthma has further been divided into two subtypes according to the presence or absence of airway eosinophilia (Wenzel et al., 1999). The broad consensus supports dividing severe asthma phenotypes according to
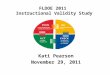
their tendency to type 2 inflammation (Figure 1). Allergic asthma in the majority of patients is associated with type 2 inflammation (Holgate, 2015). Such lung inflammation is mostly affected by the overproduction of type 2 cytokines such as IL-4, IL-5, and IL-13. IL-4 produced by Th2 cells is critical for allergen-specific production of IgE, which releases inflammatory mediators upon cross-linking of the high-affinity IgE receptors on the surfaces of mast cells and basophils. IL-5 supports the development of eosinophils in the bone marrow and enrolls eosinophils into the lung mucosa and interstitium. Enzymatic activity of the allergens damages the epithelial cell layers and activates mucosal dendritic cells that stimulate allergen-specific naive CD4 T cells in lymph nodes to differentiate into type 2 cytokine-producing Th2 cells. (Lambrecht et al., 2014).

28
Figure 1. Severe asthma endotypes (modified from Wenzel, 2012 with permission of the publisher).
The involvement of innate lymphoid cells and innate-like lymphocytes (ILLs) in the pathogenesis of asthma has recently inspired valuable insight into asthma research. ILCs are innate immune cells lacking the T cell and B cell receptors, and they are able to rapidly secrete various cytokines, especially effector cytokines IL-5, IL-13, and IL-17, in response to stimuli. (Vivier et al., 2018). The ILLs are subpopulations of T or B cells expressing T and B cell receptors but functioning very similarly to ILCs (Lanier, 2013; Spits et al., 2013). Both of them lack antigen-specificity, reside in tissues, and are located at mucosal sites where infection and inflammation frequently occur, the important one in asthma being the respiratory tract (Chou et al., 2018). ILLs and ILCs are involved in the pathogenesis of asthma, and therefore, as the treatment targets of both Th2 and non-Th2 asthma, they offer potential strategies (Huang et al., 2019). ILC2s in particular are potent sources of IL-13 and IL-5. ILC2 activation
promotes eosinophil infiltration, mucus secretion, and airway hyperreactivity, but does not affect IgE production (Martinez-Gonzalez et al., 2015). ILC2-derived IL-13 promotes the migration of lung dendritic cells into the draining lymph node. There it initiates Th2 cell differentiation. (Halim et al., 2014). In allergic airway inflammation, allergens seem to provoke the release of alarmins
such as IL-33. These stimulate lung-resident ILC2 into secreting type 2 cytokines, which cause allergic inflammation and promote Th2 cell activation and subsequently
Non Type 2
Early-onset allergic
NSAID-exacerbated respiratory disease
Allergen specific IgE
NeutrophilicPaucigranulocytic Obesity Smoking
Type 2
ASA or NSAID sensitivity
Late-onset eosinophilic
Eosinophilia Lack of inflammation in airways
Sputum neutrophils
Antibiotics
Lifestyle and behavior changes
Biomarker testing
Targeted therapy
PollutantsOccupationalexposure agents

29
develop adaptive B cell responses and IgE production. (Martinez-Gonzalez et al., 2015). Female ILC2s can produce significantly higher amounts of IL-5 and IL-13 than do male ILCS2 cells. Type 2 cytokine gene expression is higher in IL-33-stimulated female ILC2s than in male ILC2s. (Warren et al., 2017). The majority of asthma patients represent type 2 inflammation, which is
associated with certain cytokines, especially IL-4, IL-5, and IL-13, and inflammatory cells such as eosinophils, mast cells, basophils, type 2 Th lymphocytes, and plasma cells producing IgE. Airway epithelial cells play a large role in regulating type 2 inflammation, and cytokines IL-25, IL-33, and TSLP seem to be involved here. (Fahy, 2015). The suggested biomarkers of type 2 immune response in asthma comprise blood
eosinophilia, specific IgE, serum periostin level, serum dipeptidyl peptidase 4, sputum eosinophilia, IL-13 levels in induced sputum, and fraction of exhaled nitric oxide (FeNO) in exhaled breath (Berry et al., 2016). IgE can be targeted by anti-IgE biologicals such as omalizumab. Prediction of response to corticosteroids and novel anti-IL-4/IL13 and anti-IL-5 treatments (dubilumab, mepolizumab, reslizumab, benralizumab) depend on measurement of blood eosinophilia (Cavkaytar et al., 2013; Ortega et al., 2014; Pavord et al., 2012). Sputum eosinophil levels can serve in prediction of the response to anti-IL-13 and anti-IL-5 therapy (Bel et al., 2014; Ortega et al., 2014; Green et al., 2002; Haldar et al., 2009; Nair et al., 2009). Measuring serum periostin, serum dipeptidyl peptidase 4 levels, and sputum IL-13 levels has also revealed them to be valuable markers when one is considering anti-IL-13 therapy (Brightling et al., 2015; Corren et al., 2011; Piper et al., 2013). FeNO values indicate eosinophilic airway inflammation in steroid-naive asthma patients (Hanania et al., 2013). Higher baseline FeNO can also predict a greater reduction in frequency of exacerbations upon anti-IL-4/IL-13 treatment (Castro et al., 2018). The discovery of non-type 2 asthma has illuminated new ways to understand this
disease. Asthma patients without strong type 2 inflammation frequently exhibit a poor response to corticosteroids; their disease is often more challenging to manage. (Mims, 2015). In non-type 2 asthma, sputum neutrophils have served as an indicator of neutrophilic endotype. Other suggested biomarkers are adipokine, IL-8, and IL-17. (Bullens et al., 2006; Gounni et al., 2001) For the time being, these have no clinical applications in asthma, although there do exist biologicals targeting cytokines of non-type 2 inflammation, such as IL-12, IL-23, IL-17, IL-1, IL-31, and TNF-a. These have been useful against some other allergic conditions. (Tan et al., 2016).

30
2.3 Allergic rhinitis
2.3.1 Definition
Allergic rhinitis is an IgE-mediated inflammation of the nasal mucosa resulting from inhaled allergen introduction in a sensitized individual (Bousquet et al., 2001; Maurer et al., 2007). AR was defined in 1929 as a process which included three cardinal symptoms: sneezing, nasal obstruction, and mucus discharge (Hansel, 1929). Although frequently regarded as merely a seasonal nuisance, AR can involve
minimum persistent mucosal inflammation which can synergize with infective inflammation. Hence, individuals with AR sometimes have additional difficulties with viral colds. (Ciprandi et al., 1995; Cirillo et al., 2007) AR also affects one’s social life, school performance, and work productivity, particularly for patients with severe forms of the disease (Bousquet et al., 2001; Bousquet et al., 2006; Canonica et al., 2007).
2.3.2 Prevalence
The prevalence of AR ranges from 10% to 40%, depending on geographic location. The highest incidence occurs in school-aged children, and it does not typically manifest until the second year of life at the earliest. (Asher et al., 2006; Bauchau et al., 2004). In Finland, AR prevalence estimates are around 30% and still increasing (Jousilahti et al., 2016). Up to 80% of asthma patients also have AR (Bousquet et al., 2008). On the other
hand, individuals with AR have a 5– to 6-fold greater risk for developing asthma (Leynaert et al., 2004). A case-control study of French adult asthma patients showed that 92.4% of AR patients reported AC symptoms (Burte et al., 2015). In a Cameroonian community-based survey, 15.9% of adult asthma patients reported AC symptoms, but only 5.2% of the non-asthma controls reported ARC symptoms (Pefura-Yone et al., 2015). One Finnish population-based study in adults discovered that for incident asthma, ARC doubles the risk (Pallasaho et al., 2011).

31
2.3.3 Phenotypes and pathogenesis
AR has traditionally been characterized by presumed cause and seasonal or perennial presentation. At present, AR is divided into two types based on symptom duration. Intermittent AR shows symptoms for less than 4 days per week or for fewer than 4 consecutive weeks, whereas persistent AR patients have symptoms occurring more than 4 days per week for at least 4 consecutive weeks. Persistent AR patients are therefore symptomatic most of the time. (Wallace et al., 2008). Intermittent forms of AR are typically a reaction to pollen produced by trees, grasses, and weeds; persistent forms, on the other hand, are most often caused by animal dander, dust mites, and molds (Bousquet et al. 2008). AR can be defined as mild when patients experience no impairment of sleep, of daily activities, of work or school performance, or if they suffer any troublesome symptoms; it is moderate to severe when these problems accumulate (Bousquet et al., 2001). A phenotype of local allergic rhinitis (LAR) can be characterized by nasal Th2
allergic response and local production of specific IgE. LAR is the diagnosis in any case with a positive response to a nasal provocation test or with specific IgE in the nasal mucosa with no evidence of systemic atopy. (Arasi et al., 2016). In LAR, biomarkers can be detectable, ones such as nasal IL-5 and thymic stromal lymphopoietin (Zicari et al., 2016).
2.4 Allergic conjunctivitis
2.4.1 Definition
The term “allergic conjunctivitis” refers to hypersensitivity disorders affecting the lid, conjunctiva, or cornea or any combination of these. When rhinitis is also present, the condition may be known as rhinoconjunctivitis or conjunctivorhinitis depending on the main symptoms. Ocular allergy has been defined as an anterior ocular surface inflammatory disorder mediated primarily by triggering of the IgE-mast cell system. (Bielory et al., 2007).

32
2.4.2 Prevalence
Because conjunctival symptoms often go unreported in medical interviews or in questionnaire-based epidemiologic studies on rhinitis or asthma, AC prevalence has been difficult to define, presumably leading, in many epidemiologic studies, to underestimations. A variety of studies suggest a high comorbidity of conjunctivitis and rhinitis. Conjunctival symptoms are often considered a minor problem, although that is not always how ophthalmologists consider it. The surveys that target specifically ocular symptoms do not indicate conjunctival symptoms being minor, either. (Palmares et al., 2010). The epidemiology of ocular allergy is mostly based on allergic rhinoconjunctivitis
(ARC) studies. Seasonal ARC may affect 3% to 42% and perennial ARC affect 1% to 18% of various populations, varying by climate and age (Brozek et al., 2010). Most recent estimates suggest that in the United States, ocular allergies affect as
high as 15% to 25% of the population (Miraldi Utz et al., 2014; O’Brien, 2013; Ono et al., 2005). The prevalence of AC is similar in Europe, Japan, and Australia, and is increasing worldwide (Rosario et al., 2011). One American survey discovered that 35% of families interviewed experienced allergies, and half reported associated eye symptoms (Stahl et al., 2004). According to another American study, ocular symptoms were the only manifestation of allergy in approximately 25% of allergic adults (Singh et al., 2010). A European survey reported that among patients with AR, itchy, red eyes afflicted 71% and watery eyes afflicted 67% (Canonica et al., 2007). The prevalence of AC was higher in female subjects (Geraldini et al., 2013).
2.4.3 Phenotypes and pathogenesis
Ocular allergy can be classified into several clinical forms. These fall into two main groups, the first including the more frequent, seasonal (SAC) and a perennial allergic conjunctivitis (PAC). Since the definitions of seasonal and perennial do not include specific duration, international consensus panels have recently suggested the terms “intermittent”, i.e. less than 4 weeks in duration, or “persistent”, i.e. more than 4 weeks in duration, these being in accordance with the definitions of AR. (Bielory et al., 2020). The second group involves the reasonably rare chronic, severe forms of ocular
allergy: vernal keratoconjunctivitis (VKC) and atopic keratoconjunctivitis (AKC). These conditions can include corneal findings and require ophthalmologic management. (Leonardi et al., 2008). AKC and VKC show clinical and

33
pathophysiological traits differing from those of SAC and PAC, although these share some common markers of allergy (Bielory et al., 1992). At times, contact-lens-associated or ocular-prosthesis-associated giant papillary
conjunctivitis can be included among ocular allergies. Nonetheless, they are not true allergic diseases, but chronic ocular microtrauma-related disorders. (Leonardi et al., 2008). Seasonal and perennial AC are typically caused by a IgE-mediated reaction to
environmental airborne allergens. The most common allergens are grass and tree pollens, mites, mold, and animal dander. SAC is usually acute or subacute and can be determined by peaks of self-limiting signs and symptoms. In repeated allergen stimulations during pollen season, the symptoms of itching, redness, and lid swelling become persistent. Tearing, mucous discharge, and burning are also typical. When redness, burning, itching, and chemosis persist for months, the disease can be considered PAC. (Ono et al., 2005). Traditionally, AC has been considered an ocular manifestation of type I allergy mediated by IgE antibodies. Nonetheless, a recent study also suggests the existence of local AC, a phenotype of AC, in which only the local levels of IgE is elevated. (Yamana et al., 2019). Although not lifethreatening, ocular allergy symptoms make a remarkable impact
on the productivity and quality of life (Virchow et al., 2011). AKC or VKC are quite rare, but can be severe and sight-threatening (Chen et al., 2014; De Smedt et al., 2013). The most prevalent symptom of ocular allergy is tearing; about three-fourth of
these patients suffer from it. Approximately half the patients have photophobia and itching, and more than one-third have foreign-body sensation. (Geraldini et al., 2013). In another study, itching occurred in 90% and redness in 85%. Lid-skin problems were involved in 22% of cases and keratitis in 11%. (Leonardi et al., 2015). In the pathogenesis of ocular allergy, mast cells play a key role. During the pollen
season, one study found, median mast cell numbers in the lamina propria were 61% higher in SAC patients than in normal subjects. In allergic patients, they also remained increased out of season. (Anderson et al., 1997). Histamine from degranulated mast cells binds histamine receptors 1 to 4 on
vascular endothelial cells, neuronal fibers, goblet cells, immune cells, and on the conjunctival epithelium (Bielory et al., 2005). Selective agents which bind to these receptors offer possibilities for therapeutic effects (Wade et al., 2012). Histamine receptor subtype agonists influence many processes of allergic inflammation, ones such as stimulation and release of adhesion molecules, chemokines, and cytokines, and activation of dendritic cells, all of these leading to maturation of antigen-

34
presenting cells and activation of CD4 Th2-lymphocytes. Such lymphocytes and also mast cells seem to be the most important immune cells involved in allergic inflammatory responses of the ocular surface. (Bielory et al., 2020). Activated mast cells can release several cytokines affecting the mucosa and can
induce chemokines and adhesion molecules contributing to the recruitment of inflammatory cells (Anderson et al., 2001). Furthermore, mediators released during the late phase of allergic inflammation of the ocular surface, ones such as lipid mediators formed from the mast cell membrane arachidonic acids and cytokines recruit and activate eosinophils, lymphocytes, monocytes, and neutrophils. These mediators offer targets for therapeutic interventions (Leonardi et al., 2006). A variety of ophthalmologic studies report local cytokine dynamics in the eye,
including the palpebral conjunctiva and lacrimal fluid (Fukagawa et al., 2000; Kumagai et al., 2000; Matsuda et al., 2009; Sugita et al., 2017; Uchio et al., 2000). As a source of biomarkers in the development of clinical assays for ocular allergies, tears show potential. Neutrophils, eosinophils, and lymphocytes with different cellular profiles are evident in tears in acute and chronic ocular allergies. (Bonini et al., 1990; Pelikan, 2012) T cells and B cells, as well as CD4:CD8 T-cell ratios in tears are reportedly higher in AKC than in control subjects, whereas increased Th2 cell levels in tears appear in VKC (Avunduk et al., 1998; Leonardi et al., 1999). Increased tear levels of IgE, tryptase, histamine, and eosinophil cationic protein may serve as biomarkers of ocular allergy (Bourcier et al., 1998; Leonardi, 2013). VKC is an example of a gender-specific protective action by pubertal factors.
This disease occurs predominantly in childhood and adolescence and almost always in boys. It disappears after puberty in 90% of patients and is quite rare in Europe and much more frequent in subtropical countries. (Bremond-Gignac et al., 2008; Leonardi et al., 2012). Half the patients represent hyper IgE. VKC has been associated with T cell-mediated responses and immense eosinophil infiltration; a trigger can be non-specific hyper-activity such as sunlight, wind, or dust. (Laffont et al., 2017).

35
2.5 Genetics of atopy and asthma
2.5.1 Associated genes
An interesting approach to the discovery of mechanisms of allergic diseases is to search for associations between the diseases and polymorphisms of various genes, especially those coding for molecules involved in immune responses. However, seeking the genetic factors involved in asthma and atopic diseases can be likened to trying to find a needle in a haystack. (Barnes, 2015). Since the arrival of the polymerase chain reaction, genetic fingerprinting has
involved amplifying deoxyribonucleic acid (DNA) fragments in the human genome, trying to find the restriction-fragment-length polymorphisms. These microsatellite markers spanning the human genome have enabled family based GWAS. Technology has led to many GWAS on asthma and its associated phenotypes (CSGA, 1997; Daniels et al., 1996; Dizier et al., 2000; Hakonarson et al., 2002; Laitinen et al., 2001; Malerba et al., 1999; Ober et al., 1998; Ober, et al., 2000; Van Eerdewegh et al., 2002; Wjst et al., 1999; Yokouchi et al., 2000, 2002). Multiple chromosomal regions have been identified as candidate loci, with six novel asthma genes identified by positional cloning (Allen et al., 2003; Laitinen et al., 2004; Nicolae et al., 2005; Noguchi et al., 2005; Van Eerdewegh et al., 2002; Zhang et al., 2003). GWAS have functioned similarly for AR (Dizier et al., 2005; Haagerup et al., 2001; Kruse et al., 2012; Kurz et al., 2005; Yokouchi et al., 2002). By March 2020, 135 GWAS on asthma, 12 on AR, 38 on allergy, and 10 on IgE,
had appeared (NHGRI-EBI GWAS Catalog, 2020). However, GWAS do not identify the causal variants associated with a disease, and the estimated cumulative genetic risk of the variants identified for asthma alone has been under 15% (Mathias, 2014). Early-onset asthma has a stronger genetic component and greater heritability than does adult-onset of asthma. It has been associated with more than 2.5 times the number of genome-wide significant loci compared with adult-onset asthma, despite the greater sample sizes for the latter. (Ferreira et al., 2019; Pividori et al., 2019). Despite the large number of candidate genes for asthma identified in GWASs and
in basic immunological research, few of those discoveries have been rigorously replicated. Ot the variety of candidate genes examined, all have failed in subsequent replication studies (Barnes, 2015; Bønnelykke et al., 2014; Ober et al., 2006; Vercelli, 2008; Zhang et al., 2008). The most strongly linked and also replicated genes include the ORMDL3-GSDMA-GSDMB locus on chromosome 17, as well as DENND1B,

36
GAB1, HLA, IKZF4, IL1RL1, IL33, IL2RB, IL6R, LRRC32, PDE4D, RORA, SLC30A8, SMAD3, TLR1, TSLP, and cadherin-related family member (CDHR) 3 (Barnes, 2015; Bønnelykke et al., 2014; Moffatt et al., 2007, 2010; Portelli et al., 2015). These genes are involved in epithelial barrier function and innate and adaptive immune responses (Moffatt et al., 2007, 2010; Portelli et al., 2015). CDHR3, a childhood asthma susceptibility gene product, is a recognized rhinovirus C receptor (Basnet et al., 2019; Bochkov et al., 2015). Nevertheless, the effects of all these loci are weak, accounting for only a minor proportion of asthma heritability (Barnes, 2015). Many studies consider asthma to be one disease, even though it includes several endotypes, and this may in part explain the weakness of the effects found. Genes also been quite extensively replicated include the beta 2 adrenergic
receptor gene, IL4, IL4RA, IFNG, IFNGR1, STAT6, GATA3, and TBX21 (Basehore et al., 2004; Haller et al., 2009; Liggett, 1995; Munthe-Kaas et al., 2008; Pykäläinen et al., 2005). In addition, genes involving in the cellular responses characterizing atopic disease, genes such as IL13 and its receptor and the FCER1B gene have been replicated (Howard et al., 2002; Kabesch et al., 2006; Potaczek et al., 2009; Vladich et al., 2005; Wu et al., 2010). Loci associated with total IgE concentrations overlap quite poorly with those
related to asthma, indicating that atopy may not be the primary driver of susceptibility (Noguchi et al., 2005; Zhang et al., 2003). Quantitative genetic scores of the combined effect of numerous common SNPs separately show a weak influence on asthma risk, indicating that asthma has a strong polygenic component (Laitinen et al., 2001). This accords with findings of familial segregation of this disease (Haagerup et al., 2001). Examples of genes associated with atopy in general are cytokine gene cluster IL3,
IL4, IL5, IL13, CD14, beta-2-adrenergic receptor, and GM-CSF. IL-4 and IL-13 promote IgE switching, whereas IL-5 stimulates eosinophil growth and activation. Beta-2-adrenergic receptors regulate contraction of bronchial smooth muscles. In addition, MHC class II alleles regulate T cell responses to environmental antigens, and the high-affinity IgE receptor beta-subunit is involved in mast cell activation. Genes for stem cell factor intervene in mast cell growth and differentiation, and IFN-g inhibits IL-4 synthesis, whereas STAT6 mediates IL-4 signal transduction. Other genes associated with atopy are IL4RA, DPP10 (a protein that regulates chemokine and cytokine activity), ADAM33 metalloproteinase (an enzyme involved in airway remodeling), and CD80/CD86, RANTES, and PHF11, all three of which encode for a transcriptional regulator of the clonal expansion of B cells and

37
immunoglobulin expression. (Barnes et al., 1999; Blumenthal, 2005; Pinto et al., 2008; Weidinger et al., 2004). The genetics of asthma severity is under investigation in association studies.
Polymorphisms in the ADRB2, ARG1, ARG2, CTLA4, IL4, IL4R, IL18, TGFB1, TLR4, SERPINE1, and ADAM33 genes seem to play a role in asthma severity in several populations (Chiang et al., 2007; Harada et al., 2009; Holloway et al., 2000; Lee et al., 2002; Pulleyn et al., 2001; Tripathi et al., 2011; Vonk et al., 2010; Wenzel et al., 2007; Zhang et al., 2011).
2.5.2 Interaction
On many occasions, the effect of a gene mutation has been dependent on the presence or absence of mutations of one or more other genes. This phenomenon in genetics is called epistasis. The effect of the mutation therefore depends on the genetic background in which it appears. (Gros et al., 2009; Phillips, 2008). The concept of gene-gene interaction has recently gained attention in genetic
studies (Lee et al., 2012; Liu et al., 2012). Applying an epistatic analysis to clinical genetic research makes it possible to examine the interactions of two or more genes involving the whole system of the human body. Such analysis can reveal the reality of dynamic molecular mechanisms and possibly provide a breakthrough to overcome the GWAS limitations. (Yoshikawa et al., 2014). As an example, FUT2 and ABO genes have recently been found to have an epistatic effect in raising the risk of childhood asthma (Ahluwalia et al., 2020).
2.6 Some inflammatory mediators previously associated with atopy and asthma
2.6.1 Interleukin-1
The innate immune system is the first step in defense of the body, a response initiated by nonspecific, nondirected phagocytosis, complement activation, or by the activation of innate immune receptors. The immune receptors react to structures conserved in many pathogens rather than against certain antigens or peptides. The link between innate and adaptive immune immunity can be demonstrated by

38
vaccination: supporting innate immune activation is a usual means to generate an adaptive immune response. (Janeway et al., 2002). Resident and invading immune cells mediate the initial immune response.
Resident tissue macrophages and epithelial cells carry an excess of immune receptors; these cells can produce innate cytokines to attract invading macrophages or support neutrophils by producing cytokines or chemokines (Akira et al., 2006) The most important cytokines associated with the innate immune response are IL-1α, IL-1β, IL-6, IL-18, IL-33, and TNF-a, all of which can act both locally and systemically (Schroder et al., 2010). Currently, we recognize eleven cytokines in the IL-1 family: IL-1α, IL-1β, IL-
1RA, IL-18, IL-36Ra, IL-36α, IL-37, IL-36β, IL-36γ, IL-38, and IL-33. IL-1, a major pro-inflammatory cytokine, appears in two forms, IL-1α and IL-1β. Several cell types can synthesize these cytokines, which play a major role in the initiation of the immune response. IL-1α is present in the cytosol and on the plasma membrane of cells, and it mediates much of the skin’s inflammatory reaction. (Dinarello, 2018; Dinarello, 1996; La et al., 2001). IL-1β has plays an important role in contact sensitization (Kermani et al., 2000). IL-1α and IL-1β are coded for by various genes located in the longer arm of chromosome 2 (Cox et al., 1998). Polymorphisms of these genes influence the strength of inflammation, based on
both in vivo and in vitro studies. Several polymorphisms have been associated with the severity of or the susceptibility to many inflammatory diseases. (Bidwell et al., 1999) A G/T base exchange at +4845 (rs17561) in exon 5 of the IL1A gene results in an amino acid substitution of alanine for serine (Velden et al., 1993). This SNP is associated with atopy in non-asthmatic adults, suggesting that allele G predisposes to atopy (Karjalainen et al., 2002; Pessi et al., 2003). The same polymorphism has also been linked to nasal polyposis, a condition often found coexisting with asthma (Erbek et al., 2007; Karjalainen et al., 2003).
2.6.2 Interleukin-4
IL-4 plays an important role in regulating Th2 cell proliferation and survival and IgE synthesis, and is essential in the initiation of allergic airway responses and of humoral responses (Brusselle et al., 1995; Corry et al., 1996; Coyle et al., 1995; Dabbagh et al., 1999; Gavett et al., 1997; Henderson et al., 2000; Tepper et al., 1990). IL-4, a major anti-inflammatory cytokine, is produced by activated T cells, mast
cells, and basophils. It plays a central role in the regulation of B-cell– and T-cell–

39
mediated immune responses. (Paul et al., 1994). The IL-4R is an important component of the IL-4 pathway, since IL-4 exerts its biological effects through two types of heterodimeric transmembrane receptor complexes: the type I receptor exclusively binding IL-4 and comprising IL-4Rα and γc subunits, and the type II receptor binding both IL-4 and IL-13 and comprising IL-4Rα and IL-13Rα1 subunits (Gour et al., 2015). In vitro studies have shown that a variant of the IL4 gene promoter, –590 C/T,
associates with IL-4 activity and higher binding activity to nuclear transcription factors, allele T being the high producer of IL-4. (Rosenwasser et al., 1997). Allele T has also been associated in several in vivo studies with high total IgE levels and with asthma and atopy (Amirzargar et al., 2009; Basehore et al., 2004; Beghé et al., 2003; Berenguer et al., 2014; Davoodi et al., 2015; Hussein et al., 2017; Kabesch et al., 2003; Liu et al., 2003; Marsh et al., 1994; Noguchi et al., 1998, 2001; Rosenwasser et al., 1995; Walley et al., 1996; Zhang et al., 2016). In the IL4RA gene, coding for IL-4 receptor α and located in the shorter arm of
chromosome 16, exist a number of SNPs associating with atopic diseases (Deichmann et al., 1997; Hackstein et al., 2001; Hershey et al., 1997; S. Kruse et al., 1999; Lozano et al., 2001; Mitsuyasu et al., 1998; Ober et al., 2000; Paul et al., 1994). The T/C base exchange at +22446 (known as cys406arg, rs1805012) in exon 9 of the IL4RA gene has been associated with atopy. This base exchange accounts for an amino acid substitution of cysteine for arginine. The allele T coding for cysteine predisposes to atopy. (Howard et al., 2002; Ober et al., 2000).
2.6.3 Toll-like receptor 4
Innate and adaptive immunity are the two types of immunity in humans for overcoming pathogens. The functionality of innate immunity depends on germline-encoded receptors, pattern recognition receptors, to which the TLRs belong. They recognize various pathogen-associated molecular patterns, which are highly conserved structures in micro-organisms and are essential for their survival. (Botos et al., 2011; Mogensen, 2009). In humans, the toll-like receptors (TLR) include 11 members: TLR1, TLR2,
TLR3, TLR4, TLR5, TLR6, TLR7, TLR8, TLR9, TLR10, and TLR11 (Takeda et al., 2003). The TLR4 is the main receptor for bacterial endotoxin, playing a principal role in the innate immune response to gram-negative pathogens and respiratory syncytial virus (Aderem et al., 2000; Lien et al., 2000). Because endotoxin binds to

40
TLR4, it initiates an intracellular signaling pathway resulting in the activation of nuclear transcription factors. A single A/G base exchange at +896 (rs4986791) in the TLR4 gene induces an amino acid substitution of glycine for asparagine (at amino acid position 299). This results in reduced cell-surface expression of TLR4, disruption of LPS-mediated signaling and reduced systemic inflammatory response to low-dose inhaled endotoxin. (Arbour et al., 2000; Michel et al., 2003). As stated in the hygiene hypothesis, early exposure to high endotoxin levels
protects from asthma and atopy, whereas low doses cause an increase in disease prevalence (Eisenbarth et al., 2002; Strachan, 1989). Exposure to endotoxin may be a risk factor for asthma; the TLR4 gene seems to modify the endotoxin effects. (Reed et al., 2001; Schwartz, 2001; Tulić et al., 2000; Werner et al., 2003). Research suggests that bronchial epithelial cells are important in driving naive T
cell differentiation towards T-helper 2 (Th2) cells by activating dendritic cells (Hammad et al., 2009; Ryu et al., 2013; Soumelis et al., 2002). This process is mediated by TLR4 signaling through the interaction of epithelial cells and environmental aeroantigens. TLR4 activation seems to stimulate the expression of several epithelium-derived alarmins, ones including TSLP and IL-25 and IL-33 (Allakhverdi et al., 2007; Bartemes et al., 2012). TSLP signaling in airway epithelial cells seems to play a role in initiating airway remodeling by stimulating the Th2 cell response (Chen et al., 2013). Recently, TLR4 antagonist has, in a chronic asthma mouse model, proven a somewhat efficient treatment for airway remodeling, possibly through the inhibition of TSLP overexpression and through Th2 airway inflammation (Li et al., 2017). It has also become apparent in mild asthma patients that tezepelumab, a humanized mAb against TSLP, reduces exacerbation rate and improves FEV1 in patients with moderate to severe asthma and reduced allergen-induced bronchoconstriction and airway inflammation (Corren et al., 2017; Gauvreau et al., 2014). The A/G base exchange at +896 (Asp299Gly mutation) inhibits TLR4-mediated
signaling. The gene sequence change in receptor responsible for LPS signaling can alter the responsiveness of the host to microbial agents. (Werner et al., 2003). TLR4 SNP at +896 has been associated with asthma in children, G being the predisposing allele (Fagerås Böttcher et al., 2004; Zhao et al., 2017). Negative findings have also appeared as to the association between TLR4 polymorphisms and asthma and atopy (Davoodi et al., 2015; Noguchi et al., 2004; Raby et al., 2002; Yang et al., 2004).

41
2.6.4 Endothelial nitric oxide synthase (eNOS, NOS3)
Nitric oxide (NO) is a reactive radical with an important role in the regulation of vascular tone, platelet aggregation, and neurotransmission. It has been regarded as a cytotoxic molecule which is, as part of the first line of host defense in infection, associated with the response of phagocytic cells to pathogens. (MacMicking et al., 1997; Moncada et al., 1993). NO also regulates the adaptive immune response, connecting innate and adaptive immunity (Taylor-Robinson et al., 1993). Nitric oxide seems to play an important role in allergic inflammation, with FeNO
a recognized as a biomarker of airway inflammation. (Saito et al., 2004) Higher FeNO is associated with atopic conditions (Leung et al., 2005; Shirai et al., 2006). In atopic asthma, treatment of human bronchial epithelial cells with NO suppresses Th2 cell proliferation (Eriksson et al., 2005). The amino acid L-arginine is the precursor of NO synthesis by vascular
endothelial cells (Palmer et al., 1988). Human beings have three isoforms of NOS, all of which are expressed in airway epithelium. Neuronal NOS or nNOS is encoded by NOS1, inducible NOS or iNOS by NOS2A, and endothelial NOS or eNOS by NOS3. (Ricciardolo et al., 2006; Sheffield et al., 2006). In endothelial cells, NO is mostly synthesized by NOS3, a dimer consisting of
two identical 134 kD monomers (Albrecht et al., 2003; List et al., 1997). NOS3 is responsible for the production of most endothelium-derived NO. It is induced in a several cell types by proinflammatory cytokines, such as IL-1, TNF-a, IFN-g, and by microbial products such as LPSs. (Kolb et al., 1998). NOS3 regulation seems to be influenced by genetic polymorphisms in
the NOS3 gene, which in humans is located in the 7q35–7q36 region of chromosome 7 (Marsden et al., 1993). Many polymorphic sites exist in the human NOS3 gene (Cooke et al., 2007). The SNP +894 (rs1799983), located in exon 7, corresponds to a guanine to thymine change, resulting in a glutamine to aspartate substitution at position 298 of the protein. (Marsden et al., 1993). In vitro, decreased NOS3 activity has been observable in endothelial cells carrying
the variant Asp allele for the Glu298Asp polymorphism (Joshi et al., 2007). Furthermore, subjects carrying the variant allele have also been shown reduced platelet NO formation in vivo (Godfrey et al., 2007; Tanus-Santos et al., 2002). Studies on the role of the SNP +894 of the NOS3 in the pathogenesis of atopy
have produced inconsistent results (Hollá et al., 2002; Leung et al., 2005; Storm van’s Gravesande et al., 2003; Yanamandra et al., 2005). In a recent study of children with

42
asthma, this polymorphism was correlated with sensitization to common seasonal aeroallergens (Iordanidou et al., 2017).
2.6.5 Interleukin-13
IL-4 and IL-13 are encoded by adjacent genes in chromosome 5q and share several regulatory elements; they transmit signals through a shared receptor complex IL-4Rα/IL-13Rα1. (Wills-Karp, 2004). Originally, these cytokines were assumed to work in similar ways, but later studies report discoveries of differences in receptor distribution, utilization, and affinity between IL-4 and IL-13. In addition, unique innate lymphoid 2 cells rather produce IL-13, rather than IL-4. (Price et al., 2010). IL-13 plays an important role in the effector phase of the immune response and induces the main manifestations of allergic disease including airway hyperresponsiveness, mucus production, airway smooth muscle alterations, and sub-epithelial fibrosis (Emson et al., 1998; Grünig et al., 1998; Webb et al., 2000; Wills-Karp et al., 1998; Zhu et al., 1999). Many SNPs associating with atopy occur in GWAS (Li et al., 2015). IL-13, has
shown to be an important mediator of allergy and asthma (Rael et al., 2011). Several polymorphisms have been discovered in the IL13 gene, among them rs20541 (+2044 G/A, R130Q G/A), which seems, in many populations, to associate with allergy or asthma phenotypes or with both (Vladich et al., 2005). This SNP is located in exon 4 at position +2044 and causes a change of arginine to glutamine at codon 130 (R130Q), a change presumably affecting ligand-receptor interaction. (Heinzmann et al., 2000) In one recent study, rs20541 polymorphism was associated with a positive SPT result, but no significant link has emerged between rs20541 polymorphism and asthma treatment and symptom severity (Accordini et al., 2016; Narożna et al., 2016). One report in Japanese with asthma shows an association between the IL13 AA rs20541 genotype and airway remodeling (Nakamura et al., 2016). Considering the new possibilities of anti-IL13 therapy, the IL13 gene has become an interesting target of research.

43
3 AIMS OF THE STUDY
1. To examine the roles in asthma and atopy of certain single nucleotide polymorphisms of IL1A, IL4RA, TLR4, IL4, NOS3, and IL13 genes
2. To investigate whether interactions exist between these polymorphisms in relation to asthma and atopic conditions
3. To investigate the genetic differences between asthma and atopy
4. To estimate whether differences exist in genetic effects between genders

44
4 SUBJECTS AND METHODS
4.1 Subjects
Our study population comprised 1,156 asthma patients and 1,792 non-asthmatic subjects. They had taken part in a Finnish population-based case-control study investigating the risk factors and predictors of adult asthma outcome. Approval for the study came from the ethics committee of Tampere University Hospital, and all subjects gave their informed consent. Of these subjects, 245 with asthma and 405 matched controls (mean age 60; range 31-89) were included in the first three studies. In the fourth study, all the participants underwent analysis regarding their answers on their allergic symptoms, and 193 with asthma were examined more thoroughly for several other factors. Inclusion criteria for asthma patients were age over 30 and being entitled to
special reimbursement for asthma medication from the Social Insurance Institution of Finland (KELA). This entitlement depends on the criteria for persistent asthma being fulfilled, as certified by a chest specialist, and documentation of typical asthma history, clinical features, and asthma course. The diagnosis required at least one of the following physiologic criteria: (1) variation of 20% or greater in diurnal peak expiratory flow (PEF) recording (in reference to maximal value); (2) increase of 15% or greater in PEF or forced expiratory volume in one second (FEV1) with a β2-agonist; or (3) a decrease of 15% or greater during exercise testing in PEF or FEV1 . Furthermore, by the time of the decision, an at least 6-month period of continuous regular use of medication for asthma must had elapsed. This method of case ascertainment has been described in detail and evaluated (Karjalainen et al., 2001; Kauppi et al., 1998). For each subject, one to two control subjects without asthma or chronic
obstructive pulmonary disease were initially selected from a register covering the entire Finnish population, with no other exclusion criteria applied. Patients and control subjects were matched for age, sex, and area of residence. Determination of AR depended upon subjects’ answer to the question (here
translated from Finnish): Have you ever had hay fever or other rhinitis symptoms

45
that are related to pollens or animals?” AC or AD similarly depended on the answer to “Have you ever had allergic eye or allergic skin symptoms?”
4.2 Methods
4.2.1 Allergy testing
The phenotypes studied were persistent asthma, atopy, and allergic rhinoconjunctivitis. Atopy determination was by means of skin prick testing that specially trained nurses performed with a panel of 22 common allergen extracts (ALK A/S, Copenhagen, Denmark). These allergens were selected to cover exposures in both urban and rural environments and included dog, cat, Acarus siro, birch, mugwort, alder, Tyrophagus putrescentieae, meadow foxtail, Dermatophagoides farina, Lepidoglyphus destructor, timothy grass, barley, Dermatophagoides pteronyssinus, oats, Aspergillus fumigatus, cow dander, horse, barley flour, Alternaria alternata, Cladosporium herbarum, wheat flour, and rye flour. SPT responses we considered positive if at least one allergen caused a wheal with
a diameter at least 3 mm larger than produced by the negative control. Allergy testing by the SPT method took place for 99.1% of asthma patients (93 male, 150 female), and for 99.3% of control subjects (150 male, 252 female). Degree of atopy we defined as the number of positive SPTs. The SPT-positive patients fell into two groups: those with one or two positive SPTs (SPT1[1]) or with three or more positive SPTs (SPT1[2]). Total serum IgE detection was by the immunoluminometry method in an
accredited laboratory, according to manufacturer's instructions (Ciba Corning Diagnostics, Halstead, United Kingdom). The determination of IgE quartiles was for asthma patients and for control subjects separately.
4.2.2 Genetic testing
Genomic DNA from peripheral blood was anticoagulated with ethylenediaminetetraacetic acid (EDTA), using the QIAamp DNA Blood Mini Kit (QIA-GEN) according to manufacturer’s instructions. Allele distributions in all genetic testing always followed the Hardy-Weinberg equilibrium.

46
4.2.2.1 IL1A SNP +4845 (rs17561)
We analyzed the base exchange at position +4845 (rs17561) of the IL1A gene by the modified method of van den Velden and Reitsma. (Velden et al., 1993) Polymerase chain reaction (PCR) primers 5′-ATG GTT TTA GAA ATC ATC AAG CCT AGG GCA-3′ and 5′-AAT GAA AGG AGG GGA GGA TGA CAG AAA TGT-3′ amplified exon 5 but introduced a mutation (T-G) in the flanking primer that facilitates analysis of this polymorphism by SAT I (MBI Fermentas, Vilna, Lithuania) digestion. PCR conditions were one minute of denaturation at 95 °C, followed by 35 cycles
at 94 °C for one minute, 56 °C for one minute, and 72 °C for two minutes and a final 5-minute extension at 72 °C. Digestion of PCR products with SAT I yielded 122 bp plus 76 bp plus 29 bp (allele 1), and 153 bp plus 76 bp (allele 2). In 645 subjects who underwent skin testing, IL1A genotyping was successful in 638 (98.9%).
4.2.2.2 IL4RA +22446 (rs1805012)
For the T/C polymorphism at +22446 of the IL4RA gene, we performed PCR under standard conditions with primers 5′-CAG CAT GGT GCC CAG TGG AG-3′ and 5′-CTT GGG AAC TCA TCC CAG GGC-3′. The PCR amplification conditions were as follows: 94 °C for two minutes, then 33 cycles at 94 °C for one minute each, at 57 °C for one minute, at 72 °C for one minute, and at 72 °C for a final 10-minute extension. Digestion of the PCR product with Tsp45I yielded 344 bp (allele T) and 271 bp plus 63 bp (allele C).
4.2.2.3 TLR4 +896 (rs 4986791)
The A/G polymorphism at +896 (rs 4986791) of the TLR4 gene we analyzed by an allele-specific hybridization method (TaqMan). The forward primer was 5’-TGA CCA TTG AAG AAT TCC GAT TAG CA-3’, the reverse primer 5’-ACA CTC ACC AGG GAA AAT GAA GAA-3’, and hybridization probes were FAM-5’-CCT CGA TGGTAT TAT T-3’ and VIC-5’-TAC CTC GAT GAT ATT ATT-3’. Amplification took place in an ABI Prism Sequence Detector 7000 (Applied Biosystems, Foster City, Calif., USA) in 100-well plates. The final volume was 5 µl containing 0.8 µl of DNA solution at a concentration of 5 ng/µl, 0.1 µl of each

47
primer (100 pmol/µl), 0.1 µl of each probe (100 pmol/µl), 2.5 µl of TaqMan Universal PCR Master Mix (Perkin-Elmer), and 1.3 µl of distilled water. Every assay included controls for the wild type and mutations. The PCR conditions were as follows: initial holding at 50 °C for two minutes, denaturation at 95 °C for 10 minutes, followed by 40 cycles of denaturation (95 °C for 15 s), then annealing and extension in one step (60 °C for 60 s).
4.2.2.4 IL4 -590 (rs 2243250)
For analyses of the C/T polymorphism at –590 (rs2243250) of the IL4 gene, the region containing the Ava II polymorphic site was amplified by PCR. (Noguchi et al., 1998) The PCR reaction mix contained 1 µl of each primer diluted to 20 pmol/µl, 0.5 µl dNTP mix, 5 µl PCR buffer of 200 mM (NH4)2SO4 and 0.1% Tween 20, 10 µl of 25 mM MgCl2, 0.25 µl Taq polymerase, 1 µl DMSO, 4 µl sample, and 27.25 µl distilled water. The forward primer was 5’-TAA ACT TGG GAG AAC ATG GT-3’ and reverse primer 5’-TGG GGA AAG ATA GAG TAA TA-3’. The PCR conditions were two minutes at 94 °C, followed by 35 cycles of 40
seconds at 94 °C, 40 seconds at 58 °C and 50 s at 72 °C, and a final 10 minutes at 72 °C. The digestion was performed overnight in a mix containing 12.5 µl of sample, 2.5 µl Ava II buffer, 0.25 µl Ava II, and 9.75 µl distilled water. Fragments were analyzed by electrophoresis on 3.5% MetaPhor agarose with Tris-borate.
4.2.2.5 NOS3 +894 (rs1799983)
The T/G polymorphism at +894 (rs1799983) of the NOS3 gene we analyzed by an allele-specific hybridization method (TaqMan; Applied Biosystems). The nucleotide sequences of the primers and probes used in the PCR we deduced from published sequences deposited in the GenBank database and chosen and synthesized in conjunction with Applied Biosystems method.
4.2.2.6 IL13 +2044 (rs 20541)
The G/A polymorphism at +2044 (rs20541) of the IL-13 gene we analyzed by the ABI Prism 7000 sequence detection system for both PCR and allelic discrimination

48
(Applied Biosystems). A commercial kit was from Applied Biosystems (TaqMan®, Assay on Demand, Purchase number 185118655).
4.2.3 Statistical methods
For allele-distribution comparisons in the case of a single gene, we used the χ2 test of Statistica (version Windows 5.1.D; StatSoft Inc, Tulsa, OK) for calculating the P value. In the case of two genes, we used the Fisher exact test of SPSS (version 11.1; SPSS Inc, Chicago, IL). Comparisons were by nonparametric Fisher’s exact, Kruskal-Wallis, and Mann-
Whitney U tests and binary logistic regression. Models for binary logistic regression were adjusted by eight potential confounding factors: age, age of asthma onset, gender, occupation, nasal polyps (NP), NSAID-exacerbated respiratory disease (NERD), parental allergy, and either the IL13 rs20541 genotype or the number of positive SPT values. Two-tailed P values <.05 we considered statistically significant. We performed the analyses with SPSS (version 11.1; SPSS Inc, Chicago, IL). We used CIA software (version 1.1; Martin J. Gardner & British Medical Journal)
for carrying out the calculations of odds ratios.

49
5 RESULTS
5.1 Allergy tests and other atopic conditions
In the first three studies, we investigated the same study group (Table 1). The percentage of SPT+ responses was 56.8% in the asthma group and 37.8% in the non-asthmatic group. In the asthma group, more showed positive skin test responses among female subjects (62.0% vs 47.3%; P = .025, χ2 testing, df = 1). The numbers of positive skin test reactions in patients of both sexes were comparable. In the control group, the percentage of subjects with positive skin test responses was 38.9% in female subjects and 37.3% in male subjects (P = .756, χ2 testing, df = 1). No difference in the number of positive reactions in skin tests appeared between the sexes either in the asthma or the control group (Table 2).
Table 1. Characteristics of the study group (modified from Karjalainen et al., 2002 with the permission of the publisher).
Variable Asthma (n = 245) Non-asthma (n = 405)
Age: mean ± SD (y) 59 ± 11 60 ± 11
Sex: n (female/male) 152/93 254/151 Smoking: n (non/ex/current) 123/80/42 237/89/79
Atopy1): n 137 154
Rhinitis symptoms2) 134 111 Eye symptoms2) 104 92
Skin symptoms3) 84 97
1) One or more skin-prick-test positive reactions.2) P < .001 3) P < .004 for difference between groups, χ2 test.

50
Table 2. Positive reactions to specific allergens in skin tests in asthma patients and control subjects (modified from Karjalainen et al., 2002 with the permission from the publisher).
Positive reactions within group
Asthma patients (n=243)
Control subjects (n = 402)
Allergen Number of reactions %
Number of reactions % P value
Corrected1) P value
Pollens Birch 40 16.5 25 6.2 <.001 <.001 Mugwort 40 16.5 24 6.0 <.001 <.001 Alder 38 15.6 25 6.2 <.001 .002 Meadow foxtail 28 11.9 26 6.5 .016 NS Timothy grass 31 12.8 21 5.2 <.001 .015 Animals Dog 69 28.4 57 14.2 <.001 <.001 Cat 53 21.8 39 9.7 <.001 <.001 Cow 133 7.8 10 2.5 .002 .034 Horse 20 8.2 8 2.0 <.001 .004 Moulds Alternaria alternata 12 4.9 13 3.2 NS NS Cladosporium herbarum 12 4.9 10 2.5 NS NS Aspergillus fumigatus 27 11.1 16 4.0 <.001 .010 Grains Barley 28 11.9 19 4.7 <.001 .016 Oats 17 7.0 27 6.7 NS NS Flours Barley 16 6.6 9 2.2 .0102) NS Rye 6 2.5 28 0.7 NS2) NS Wheat 11 4.5 9 2.2 NS2) NS Mites Acarus siro 40 16.5 51 12.7 NS NS Dermatophagoides pteronyssinus 21 8.6 27 6.7 NS NS Tyrophagus putrescentiae 24 9.9 36 9.0 NS NS Dermatophagoides farinae 24 9.9 31 7.7 NS NS Lepidoglyphus destructor 20 8.2 33 8.2 NS NS 1) Bonferroni correction applied 2) Yates correction applied

51
In the fourth study, a total of 716 (61.9%) asthma patients and 524 (29.2%) control subjects reported AR symptoms that associated significantly with asthma (OR 3.85, 95% CI 3.19–4.64, P < .001, by conditional logistic regression). The corresponding percentages of subjects reporting AC were 40.7% and 19.6%, and those reporting AD were 33.6 and 22.8%. They also associated significantly with asthma (AC: OR 2.73, 95% CI 2.32–3.21, P < .001; AD: OR 1.7, 95% CI 1.48–2.05, P < .001). Only the presence of AR and/or AC were chosen for further evaluation due to their higher prevalence compared to AD. Regarding only the asthma subgroup (n=193), several factors were associated
with AR/AC symptoms, including the polysensitization pattern, sensitization to pollen or animal dander allergen(s), 3–17 positive SPT values, female gender, younger age, younger age at asthma onset, office/service work, nasal polyposis, NERD, and parental allergy (Table 1, Study IV). The following factors did not associate with AR/AC asthma: asthma-symptom severity or duration, smoking habits, FEV1, body mass index, peripheral blood eosinophils, and total serum IgE. Furthermore, the following also showed no association: subject-reported use of
peroral or inhaled corticosteroids, education or occupational education, childhood spent in the countryside or on a farm, or parental asthma (P > .05, data not shown). The 3 to 17 positive SPT values associated significantly with AR/AC (raw OR 5.20, 95% CI 1.90-14.27, P = .001; adjusted OR 4.59, 95% CI 1.48-14.26, P = .008) emerged when 0 to 2 positive SPT values was the reference. Having one or more positive SPT values was not significantly associated with AR/AC (OR 1.01, 95% CI 0.50-2.05, P = .97), when zero positive SPT value was the reference. The median sum of positive SPT results and SPT wheal diameter was greater in
the asthma subgroups with AR and/or AC symptoms than in the subgroup without AR/AC (Figure 1, Study IV). The highest sum of positive SPT results and the largest SPT wheal diameter were both detected in the asthma subgroup with both AR and AC symptoms.
5.2 Polymorphisms
5.2.1 IL1A and IL4RA
We grouped the subjects according to carrier status for IL1A allele T and IL4RA allele C. Carriers of IL1A allele T had the genotype GT or TT; accordingly, the

52
carriers of IL4RA allele C had the genotype TC or CC. The non-asthma group showed no significant association between IL4RA allele carrier status and SPT (Table 2, Study I). Data published earlier showed that distribution of IL1A allele carriers between those with SPT+ responses and those with SPT– responses differed (P = .001; χ2 test) (Karjalainen et al., 2002; Pessi et al., 2003). This difference in distribution resulted from an increase in the frequency of allele-T carriers among subjects with SPT responses. As for the noncarriers of allele C of the IL4RA gene, IL1A allele carrier
distribution differed significantly between those subjects with SPT+ responses and those with SPT– responses in the non-asthma group (P < .001; Fisher exact test). A combination of noncarriers of allele C of IL4RA and noncarriers of allele T of IL1A was more likely to appear among SPT+ subjects than among SPT– subjects (odds ratio, 2.32; 95% CI, 1.47-3.67). We did not, however, find any significant association of IL1A and SPT in the case of allele C of the IL4RA gene. The asthma group showed no association of IL1A, IL4RA, and SPT results (data not shown).
5.2.2 TLR4 and IL4
For both the asthma and non-asthma groups, the genotype frequencies were 0.83 for AA, 0.16 for AG, and 0.01 for GG each at +896 of the TLR4 gene. At -590 of the IL4 gene, the genotype frequencies were 0.41 for CC, 0.45 for CT, and 0.14 for TT if the subjects had asthma and 0.47 for CC, 0.41 for CT, and 0.12 for TT in the case of non-asthmatic subjects. The genotype frequencies of neither gene differed significantly between the asthma and non-asthma groups. For atopic and nonatopic subjects, the genotype frequencies were 0.83 for AA,
0.16 for AG, and 0.01 for GG at +896 of the TLR4 gene. At –590 of the IL4 gene, these genotype frequencies were 0.38 for CC, 0.44 for CT, and 0.17 for TT among atopic subjects and 0.50 for CC, 0.40 for CT, and 0.10 for TT among non-atopic subjects. A trend toward genotype frequencies of the IL4 gene differing between atopic subjects and those without atopy emerged, allele T being predisposing to atopy. This was apparent both in those with asthma (P = .076, c2 test) and without asthma (P = .072, c2 test). The genotype frequencies of the TLR4 gene did not differ between these groups. Subject grouping was based on their carrier status for TLR4 allele G (genotype AG or GG) and IL4 allele T (CT or TT), with genotype distribution following the Hardy-Weinberg equilibrium.

53
There emerged no association between TLR4 allele carrier status and asthma (Table 1, Study II). The distribution of IL4 allele carriers did not differ significantly between those subjects with or without asthma, but a trend was detectable in female subjects (P = .073, c2 test). This difference in distribution was the result of an increase in frequency of the carriers of allele T among those with asthma. An epistatic effect between TLR4 and IL4 polymorphisms appeared in female subjects (P = .037, binary logistic regression). Among carriers of allele G of the TLR4 gene, IL4 allele carrier distribution differed significantly between female asthma and non-asthmatic subjects (P = .011, Fisher’s exact test). For female carriers of allele T of IL4 who were also carriers of allele G of TLR4 gene, the odds ratio was 4.16 (95% CI, 1.41–12.3), when compared to the group in which the subjects were carriers of allele G of TLR4 but non-carriers of allele T of IL4. When compared to all other groups, the odds ratio was 2.26 (95% CI, 1.11–4.59). No significant association between IL4 and asthma appeared as to allele A of the TLR4 gene. No association of any kind occurred in male subjects, nor any epistatic effect on the risk for atopy.
5.2.3 IL1A and NOS3
As in Table 1, Study III, and as mentioned earlier, IL1A genotype GG led to risk for sensitization to allergens (OR 2.09; 95% CI, 1.23-3.57; P = .006, c2 test; df= 1). NOS3 polymorphism had no independent effect on sensitization to allergens, but it interacted with the IL1A gene. We calculated the interaction of these genes by multinomial logistic regression
analysis. The model showed a slight interaction between these genes and degree of sensitization (P = .08). Interaction was significant between the SPT-negative and SPT1(2) groups (P = .026), but not between the SPT-negative and SPT1(1) groups (P = .785, bilogistic regression analysis) (Table 2, Study III). The combination of allele T of NOS3 and genotype GG of IL1A was predisposing to higher degree of atopy. If age and sex were included in the model, no results changed (data not shown).
5.2.4 IL13
Regarding the subsample of 454 who underwent clinical tests, neither the IL13 rs20541 GA or AA genotype was associated with the asthma phenotype (P = .63,

54
OR 1.10, 95% CI 0.74–1.64). Regarding only the asthma subgroup, the IL13 rs20541 GA or AA genotype was associated with AR/AC symptoms (P = .002) (Table 3).
Table 3. IL13 SNP rs20541 in asthma patients with and without allergic rhinitis (AR) and/or allergic conjunctivitis (AC) (based on data from Ådjers et al., 2017).
AR and/or AC IL13 rs20541 genotype no (n = 72) yes (n = 121) P value GG 34 (48.6) 28 (23.7) .002 GA 29 (41.4) 65 (55.1) AA 7 (10.0) 25 (21.2)
In logistic regression analyses of the asthma group, the IL13 rs20541 GA or AA genotype associated significantly with AR/AC (raw OR 3.04, 95% CI 1.61–5.71, P = 0.001; adjusted OR 3.06, 95% CI 1.42–6.58, P = 0.004) when the IL13 rs20541 GG genotype was the reference. However, S-IgE showed no association with the IL13 rs20541 GA or AA genotype in asthma patients (P > 0.05, data not shown).

55
6 DISCUSSION
Initially, we assessed SPT findings and the distribution of IL1A and IL4RA genotype combinations in asthma patients and non-asthmatic subjects, demonstrating an epistatic effect between IL1A and IL4RA genes in the non-asthmatic group. Being a non-carrier of allele C (genotype TT) of IL4RA and at the same time also being a non-carrier of allele T (genotype GG) of IL1A had an interactive effect on one’s risk for atopy. As in earlier studies, noncarriers of allele T of IL1A have more often shown
SPT+ results than have carriers of this allele (Karjalainen et al., 2002). Moreover, being a non-carrier of allele C of IL4RA has been associated with SPT+ results and high IgE levels (Howard et al., 2002; Ober et al., 2000). Our control subjects could be expected to represent the general population quite
well. A diagnosis of asthma or chronic obstructive pulmonary disease was the sole exclusion criterion. According to the asthma criteria we chose, asthma prevalence in the Finnish adult population was, at the time of the study, 3.3% (National Agency for Medicine and Kela, 1998). Since this percentage is relatively low, our study population’s lack of asthma patients can be considered of minor significance, allowing our findings to be applied to the general population. The interaction we discovered might elucidate some basic mechanisms of
atopy. The IL1A +4845 GG genotype is presumably associated with a low capacity to produce IL-1α and since a weak inflammatory response favors the differentiation of Th2 cells, we can hypothesize that in such subjects, IL-4 levels are elevated (Perussia et al., 2003). Accordingly, if the high IL-4-responding IL4RA T allele is concurrently present, the Th2 differentiation and subsequently atopy seems even more remarkable. In our second study, we evaluated whether TLR4 and IL4 genotypes or their
combinations exert any effect on asthma or atopy in the same population-based sample of asthma patients and non-asthmatic subjects. Although an association between asthma and IL4 genotype has been evident in several populations, in our own study the genotypes of neither the TLR4 SNP at +896 nor IL4 SNP at –590 were associated with asthma (Amirzargar et al., 2009; Basehore et al., 2004; Beghé et al., 2003; Berenguer et al., 2014; Davoodi et al., 2015; Hussein et al., 2017; Kabesch

56
et al., 2003; Liu et al., 2003; Marsh et al., 1994; Noguchi et al., 1998, 2001; Rosenwasser et al., 1995; Walley et al., 1996; Zhang et al., 2016). Contradictory results have also appeared (Walley et al., 1996; Yang et al., 2004). Our female carriers both of allele G (AG or GG) of TLR4 and of allele T (CT or
TT) of IL4 showed an increased risk for asthma. Thus, since these alleles alone had no effect on risk for asthma, they showed an epistatic effect to control a single phenotype. No effect on atopy emerged. Nevertheless, this finding does not eliminate the possibility of this combination of genes being associated with atopy severity. This has been true for asthma patients. (Yang et al., 2004). The epistatic effect of TLR4 and IL4 genes occurred only in females. What may
explain this is the sex-dependent differences in the body’s defense mechanisms (Lahita, 2000). Because the frequencies of the alleles do not vary by gender, the functions of the alleles or their interactions with other genes may vary. Asthma has been shown to be more prevalent in males before adolescence, but in puberty this trend changes. This trend does not apply only to asthma but also to most allergic disorders. (Almqvist et al., 2008; Carey et al., 2007; de Marco et al., 2000; Holgate, 2015). In asthma, potential genetic and hormonal contributors and sex differences in
concomitant conditions such as obesity and cigarette smoking may enhance asthma risk (Raghavan et al., 2016). Estrogens have been thought to impact the change from male to female predominance in allergic diseases, but still not very much evidence supports any disease-promoting effect of estrogens by the estrogen-receptor expression in specific immune cell subsets linked in type 2 inflammation. Recent studies have indicated an impact of sex-linked factors on ILC2 responsiveness and on homeostatic regulation (Laffont et al., 2017; Warren et al., 2017). Androgens affect ILC2 development and expansion through androgen-receptor signaling (Laffont et al., 2017). Despite allele G of the TLR4 gene (frequency of carriers 0.17) in the population
being uncommon, the epistatic effect that we discovered may account for the diverse mechanisms of asthma and atopy. Early exposure to high endotoxin levels seem to protect against the development of asthma and atopy later in life through Th cell differentiation towards Th1 polarization (Strachan, 1989). Bacterial LPS signaling through TLR4 may play a significant role in this (Arbour et al., 2000; Burte et al., 2015; Liu, 2002). A low level of inhaled LPS is necessary to induce Th2 responses to inhaled antigens, whereas a high level of inhaled LPS induces Th1 responses (Eisenbarth et al., 2002).

57
The allele G of TLR4 is responsible for diminished inflammatory responses and an impaired bronchoconstrictor response to inhaled LPS. This indicates its role in promoting Th2 responses (Arbour et al., 2000; Fagerås Böttcher et al., 2004). On the other hand, the allele T of IL4 has been associated with high IL-4 production (Nakashima et al., 2002). When these alleles are combined, the risk for asthma naturally increases. This epistatic effect on asthma can be assumed to be caused by IL4 potentiating the signal through TLR4, although the exact mechanism implicated remains unknown. The differing findings of this study in relation to asthma and atopy may be due
to IL-4 effects other than induced IgE production, effects such as activity of T cells (Grabstein et al., 1987). These effects also include the tendency of IL-4 to cause increased production of other Th2 cytokines, ones such as IL-3, IL-5, IL-9, and IL-13. These cytokines cause increased eosinophil growth and mucus production, and they induce airway hyperreactivity. (Lorentz et al., 2000). It is also possible that, among those with intrinsic asthma, IL-4 is stored within their bronchial mucosa (Humbert et al., 1996). In our third study, we showed that the NOS3 gene had no independent effect on
atopy, but an epistatic effect of IL1A and NOS3 genes on the degree of atopy did occur. Allele T of NOS3 and genotype GG of IL1A seemed to predispose to a higher degree of atopy. Exhaled NO levels in adults correlate with atopy rather than with bronchial
hyperreactivity and lung function (Ali et al., 2003; Ho et al., 2000). The effect of the NOS3 gene on atopy seems to depend on some other proinflammatory gene, and one candidate may be IL1A. This interaction between NOS3 and IL1A genes may explain some earlier conflicting findings as to the effect of NOS3 polymorphisms on atopy. (Hollá et al., 2002; Leung et al., 2005; Storm van’s Gravesande et al., 2003; Yanamandra et al., 2005). Both NOS3 and IL1A genes are included in the initiation of the immune response
and seem to affect the Th1/Th2 balance. NO has shown an enhancing effect on the induction and differentiation of Th1 cells at the inductive phase, but it has hardly any effect on fully committed T cells. On the other hand, at noncytotoxic concentrations, NO downregulates the Th1-type cytokines and leads to increased amounts of the Th2-associated molecules (Kolb et al., 1998). High NO synthesis has been associated with atopy and the genotypes of TT and GT of the NOS3 gene (Ali et al., 2003; Yoon et al., 2001). Findings demonstrate that carriers of genotype GG of IL1A have a markedly higher risk for SPT positivity (Karjalainen et al., 2002). Presumably, allele G is associated with a low capacity to produce IL-1a, and the

58
weak inflammatory response induced is known to favor the differentiation of Th2 cells (Perussia et al., 2003). For those having two atopy risk genes, such as a high NO-producing allele of the NOS3 gene together with the IL1A atopy-risk gene, Th2 responses like sensitization to allergens are even further increased. The possibility that the NOS3 gene exerts its effects during the diagnostic phase
cannot be confidently excluded. The high-producer allele T of the NOS3 gene might make the SPT more sensitive by inducing stronger endothelial enlargement at the site of allergen application (Yoon et al., 2001). However, this does not seem very probable, since we did not observe any effect involving the NOS3 genotype on the response induced by the histamine control treatment (data not shown). In our fourth study, we reported that, in asthma patients, the IL13 rs20541 GA
or AA genotype affected risk for AR/AC. Carriers of allele A of IL13 rs20541 were predisposed towards multisensitization and AR/AC symptoms. This same allele was not associated with the whole asthma group, indicating that this genotype may be characteristic of a true atopic asthma endotype. Those with asthma also showed a dose-dependent association between sensitization and AR/AC symptoms. This finding is in line with findings indicating that sensitization is not a dichotomous value (Just et al., 2014; Toppila-Salmi et al., 2015). To conclude, our studies showed that the genes that we investigated or
combinations of those genes had significant effects on atopy, asthma, severity of atopy, or AR/AC symptoms in asthma (Table 4).
Table 4. Genetic findings of our studies.
Study Gene(s) Risk
I IL1A + IL4RA Atopy (SPT) II TLR4 + IL4 Asthma in females III IL1A + NOS3 Severity of atopy
IV
IL13
AR/AC symptoms in asthma Multisensitization
The current global challenge is to prevent atopic diseases and the asthma burden (Bousquet et al., 2008; Burte et al., 2015; Pallasaho et al., 2011; Pefura-Yone et al., 2015). Many asthma patients fail to respond to therapy (Chung, 2015). The finding in our fourth study of a high prevalence of AR/AC symptoms in adult asthma patients is in line with such observations (Bousquet et al., 2008; Burte et al., 2015; Pallasaho et al., 2011; Pefura-Yone et al., 2015). Nasal polyposis and NERD were

59
also linked with AR/AC asthma. Hence, we conclude that there may be atopic and eosinophilic characteristics in adult AR/AC asthma. Female gender was associated with AR/AC asthma, reflecting gender differences
in asthma pathogenesis (Zein et al., 2015). Parental allergy, young age, and younger age at onset seemed to associate with AR/AC symptoms, which may indicate the burden of the atopic asthma phenotype in Finland. The association of office/service work with AR/AC symptoms was also a new discovery. Younger patients presumably work in these kinds of occupations, and they also show more polysensitization and AR/AC symptoms. Our fourth study revealed no association between S-IgE and AR/AC asthma or
the IL13 polymorphism, indicating that a variety of genome-environmental interactions influence S-IgE. Nor did there emerge any association between AR/AC and asthma severity. Reports state that variation exists in severity among the atopic asthma phenotypes, depending on eosinophilia, female gender, and early multiple allergies, and our results agree with this (Just et al., 2014; Simpson et al., 2010). Due to its natural variation, the coding region of the IL13 gene has been a
potential genetic determinant of predisposion to allergy, and the IL13 rs20541 G/A polymorphism has been linked to allergic asthma (Black et al., 2009; Nie et al., 2013; Vladich et al., 2005). IL-13 R130Q has been significantly more active than wild-type IL-13 in inducing STAT6 and CD23 in monocytes and inducing hydrocortisone-dependent IgE switching in B cells, and it is neutralized less effectively (Vladich et al., 2005). The IL-13 variant could not engage T cells. Enhanced allergic inflammation in carriers of allele A of IL13 rs20541 seems to depend upon increased IL-13-mediated Th2 effector functions, not upon the increased Th2 differentiation. Other IL13 polymorphisms, ones not examined in our studies such as +1923C/T, have been significantly correlated with asthma (Liu et al., 2013). In addition, the IL13-RAD50 and IL4-KIF3A have been linked to AR and asthma (Li et al., 2015). Yet, not all patients with severe asthma show the IL-13 endotype. Recently, much progress has occurred in research into type 2 immunity,
elucidating new aspects of the cellular and molecular mechanisms of asthma and other allergic diseases. A complex network of cells and molecules of both the innate and adaptive immune system mediates type 2 immune responses in the lungs. Epithelial-derived alarmins like IL-25, IL-33, and TSLP are of major importance in initiating type 2 responses, whereas IL-4, IL-5, and IL-13 are the main effector mediators that continue the response. In addition to T cells, DC, MC, and eosinophils, ILC2 have been important in type 2 immunity. Knowledge of these

60
cellular and molecular aspects, combined with the knowledge of genetics, has clarified the pathomechanisms of atopic diseases and asthma. Asthma and other atopic diseases typically result from several genetic
determinants and environmental factors (Ferreira et al., 2011). During the past few decades, genome-wide linkage analyses, biologically probable candidate gene approaches, and genome-wide association studies have featured in investigations concerning nucleotide variants as genetic factors. GWASs have proven useful in discovering new genetic variants of these complex diseases. (Lasky-Su et al., 2012). What is difficult to discover, however, is any new susceptibility loci in small-sample-size analyses, since each variant exerts only a small effect, and several variants seemingly promising in the original GWAS do not meet the levels of significance. The ultimate goal of genomic medicine is to translate knowledge from newly identified variants to the clinic for prediction, diagnosis, and management. Our studies were implemented by use of candidate-gene-based association
analysis, which is considered an admissible method in studying complex genetic traits. It has, however, also met with criticism, due to the insufficient quality of thus-far published reports (Nature Genetics, 1999). The limitations of GWAS analyses in complex human disease have moved the focus from linkage analysis and microsatellite markers towards SNP genotyping and analytical strategies based on association and haplotype analysis (Risch, 2000). As of November 22, 2020, a keyword search for "asthma and polymorphism"
returned 4,449 publications. Many associated SNPs have odds ratios below 2.0, which indicates that the candidate-gene approach has revealed information on genetic variants causing a significant risk for increase in likelihood of asthma, but the part they play in development of this disease may be a bit smaller than earlier suspected. Therefore, over the past decade, whole-genome SNP genotyping arrays have served for investigation of the genetic background of multifactorial diseases such as asthma. Thus far, the research focus has been on asthma in general, even though asthma encompasses a variety of different endotypes. Changing the focus towards the endotypes may offer more information. Each of our studies has revealed a few pieces of the complex network of the
genetics of adult asthma and atopy. Since our first studies, the fields of genetics and immunology of atopy, atopic diseases, and asthma have seen the rise several new observations. As an example, implementation of the clinical application of IL-4 and IL-13 has been in the form of dubilumab, a human monoclonal antibody that binds specifically to the IL-4Rα subunit of the receptor complexes for IL-4 and IL-13. Not all of those with Th2 asthma, however, respond to this novel anti-IL-4 or anti-IL-13

61
therapy (Bagnasco et al., 2016). The anti-IL-5 agents mepolizumab and reslizumab, as well as the anti-IL-5R agent benralizumab and anti-IgE agent omalizumab have also appeared to be effective in certain forms of severe asthma (Bel et al., 2014; Castro et al., 2011, 2015; Chang et al., 2006; Chupp et al., 2017; FitzGerald et al., 2016; Haldar et al., 2009; Hom et al., 2017; Nair et al., 2009; Ortega et al., 2014; Pavord et al., 2012). Tezepelumab, an anti-TSLP agent, has recently been under investigation in treatment of uncontrolled asthma (Corren et al., 2017). These biological agents have begun a new era in treatment of asthma and have extended our understanding of differing asthma endotypes. Further studies are vital regarding specific biomarkers and risk-conferring genes for targeting this expensive therapy at those who will benefit from it, and hopefully, targeting development of more treatment options. With increasing understanding of various asthma endotypes, prophylactic and therapeutic vaccines will also presumably join our current asthma therapeutics (Elenius et al., 2016). Our most recent findings suggest that high prevalence of allele A of IL13 rs20541,
multisensitization pattern, and AR/AC symptoms are characteristic of an adult atopic asthma phenotype. Further studies should evaluate the pathomechanisms involved and reveal the effects of these findings in larger populations.

62
7 CONCLUSIONS
In our first three studies, we examined in a study group of Finnish adult asthma patients and non-asthmatic control subjects whether there exists any individual effect of a candidate gene SNP on the risk or severity of atopy or asthma or whether two SNPs of different candidate genes show an interactive effect. We demonstrated an epistatic effect on atopy between IL1A and IL4RA genes in the non-asthmatic control group. The carriers of genotype TT of IL4RA +22446 and genotype GG of IL1A +4845 had an interactive effect on the risk for atopy. The female carriers of allele G of TLR4 +896 and allele T of IL4 -590 also showed an increased risk for asthma. Furthermore, an epistatic effect emerged for allele T of NOS3 +894 and genotype GG of IL1A +4845 on atopy degree. These findings suggest that, in addition to gene-environment interactions, gene-gene interactions affect one’s susceptibility to atopy and asthma as well as affecting atopy severity. Two separate polymorphisms can potentiate each other’s effects, predisposing carriers of certain alleles or genotypes to clinical manifestations. Indicating sex-dependent differences in the body’s defense mechanisms, an epistatic effect of TLR and IL4 genes on asthma appeared only in females. Furthermore, female gender was associated with AR/AC asthma, reflecting differences in asthma pathogenesis between the genders. Our fourth study showed that allele A of IL13 SNP rs20541 affected the risk for
AR/AC in asthma patients. Carriers of allele A of this SNP were also predisposed towards multisensitization in asthma. Our findings therefore suggest that possibly characteristic of an adult atopic asthma phenotype are three manifestations: high prevalence of allele A of IL13 rs20541, multisensitization pattern, and AR/AC symptoms. This finding, however, calls for further studies in larger populations. Since the time of our initial studies, increased knowledge of relevant cellular and
molecular aspects, as well as of genetics, has revealed more particulars regarding the complex network of atopic diseases and asthma. There still exist many issues needing attention, however, with more research required to clarify their pathomechanisms in the struggle against these common conditions imposing a great burden on individuals and on society.

63
8 REFERENCES
Accordini, S., Calciano, L., Bombieri, C., Malerba, G., Busse, W. (2016). An Interleukin 13 Polymorphism Is Associated with Symptom Severity in Adult Subjects with Ever Asthma. PLOS ONE, 11(3), e0151292.
Aderem, A., & Ulevitch, R. (2000). Toll-like Receptors in the Induction of the Innate Immune Response. Nature, 406(6797).
Ådjers, K., Luukkainen, A., Pekkanen, J., Hurme, M., Huhtala, H., Renkonen, R., Wang, D. Y., Mäkelä, M. J., Karjalainen, J., & Toppila-Salmi, S. (2017). Self-Reported Allergic Rhinitis and/or Allergic Conjunctivitis Associate with IL13 rs20541 Polymorphism in Finnish Adult Asthma Patients. International Archives of Allergy and Immunology, 172(2), 123–128.
Ahluwalia, T. S., Eliasen, A. U., Sevelsted, A., Pedersen, C.-E. T., Stokholm, J., Chawes, B., Bork-Jensen, J., Grarup, N., Pedersen, O., Hansen, T., Linneberg, A., Sharma, A., Weiss, S. T., Evans, M. D., Jackson, D. J., Morin, A., Krogfelt, K. A., Schjørring, S., Mortensen, P. B., Hougaard, D. M., Bybjerg-Grauholm, J., Bækvad-Hansen, M., Mors, O., Nordentoft, M., Børglum, A. D., Werge, T., Agerbo, E., Gern, J. E., Lemanske, R. F., Ober, C., Pedersen, A. G., Bisgaard, H., & Bønnelykke, K. (2020). FUT2–ABO epistasis increases the risk of early childhood asthma and Streptococcus pneumoniae respiratory illnesses. Nature Communications, 11(1), 6398.
Akdis, C. A., Blesken, T., Akdis, M., Wüthrich, B., & Blaser, K. (1998). Role of interleukin 10 in specific immunotherapy. The Journal of Clinical Investigation, 102(1), 98–106.
Akira, S., Uematsu, S., & Takeuchi, O. (2006). Pathogen recognition and innate immunity. Cell, 124(4), 783–801.
Albrecht, E. W. J. A., Stegeman, C. A., Heeringa, P., Henning, R. H., & van Goor, H. (2003). Protective role of endothelial nitric oxide synthase. The Journal of Pathology, 199(1), 8–17.
Ali, M., Khoo, S.-K., Turner, S., Stick, S., Le Souëf, P., & Franklin, P. (2003). NOS1 polymorphism is associated with atopy but not exhaled nitric oxide levels in healthy children. Pediatric Allergy and Immunology : Official Publication of the European Society of Pediatric Allergy and Immunology, 14(4), 261–265.
Allakhverdi, Z., Comeau, M. R., Jessup, H. K., Yoon, B.-R. P., Brewer, A., Chartier, S., Paquette, N., Ziegler, S. F., Sarfati, M., & Delespesse, G. (2007). Thymic stromal lymphopoietin is released by human epithelial cells in response to microbes, trauma, or inflammation and potently activates mast cells. The Journal of Experimental Medicine, 204(2), 253–258.
Allen, M., Heinzmann, A., Noguchi, E., Abecasis, G., Broxholme, J., Ponting, C. P., Bhattacharyya, S., Tinsley, J., Zhang, Y., Holt, R., Jones, E. Y., Lench, N., Carey, A., Jones, H., Dickens, N. J., Dimon, C., Nicholls, R., Baker, C., Xue, L., Townsend, E., Kabesch, M., Weiland, S. K., Carr, D., von Mutius, E., Adcock, I. M., Barnes, P. J., Lathrop, G. M., Edwards, M., Moffatt, M. F., & Cookson, W. O. C. M. (2003).

64
Positional cloning of a novel gene influencing asthma from Chromosome 2q14. Nature Genetics, 35(3), 258–263.
Almqvist, C., Worm, M., Leynaert, B., & working group of GA2LEN WP 2.5 Gender. (2008). Impact of gender on asthma in childhood and adolescence: a GA2LEN review. Allergy, 63(1), 47–57.
Amirzargar, A. A., Movahedi, M., Rezaei, N., Moradi, B., Dorkhosh, S., Mahloji, M., & Mahdaviani, S. A. (2009). Polymorphisms in IL4 and iLARA confer susceptibility to asthma. Journal of Investigational Allergology & Clinical Immunology, 19(6), 433–438.
Anderson, D. F., Macleod, J. D. A., Baddeley, S. M., Bacon, A. S., McGill, J. I., Holgate, S. T., & Roche, W. R. (1997). Seasonal allergic conjunctivitis is accompanied by increased mast cell numbers in the absence of leucocyte infiltration. Clinical & Experimental Allergy, 27(9), 1060–1066.
Anderson, D., Zhang, S., Bradding, P., McGill, J. I., Holgate, S. T., & Roche, W. R. (2001). The relative contribution of mast cell subsets to conjunctival TH2-like cytokines. Investigative Ophthalmology & Visual Science, 42(5), 995–1001.
Anderson, H. (2005). Prevalence of asthma. BMJ (Clinical Research Ed.), 330(7499), 1037–1038.
Annunziato, F., Romagnani, C., & Romagnani, S. (2015). The 3 major types of innate and adaptive cell-mediated effector immunity. Journal of Allergy and Clinical Immunology, 135, 626–635.
Arasi, S., Pajno, G. B., Lau, S., & Matricardi, P. M. (2016). Local allergic rhinitis: A critical reappraisal from a paediatric perspective. Pediatric Allergy and Immunology : Official Publication of the European Society of Pediatric Allergy and Immunology, 27(6), 569–573.
Arbour, N., Lorenz, E., Schutte, B., Zabner, J., Kline, J., Jones, M., Frees, K., Watt, J., & Schwartz, D. (2000). TLR4 Mutations Are Associated With Endotoxin Hyporesponsiveness in Humans. Nature Genetics, 25(2).
Arpaia, N., Campbell, C., Fan, X., Dikiy, S., van der Veeken, J., deRoos, P., Liu, H., Cross, J. R., Pfeffer, K., Coffer, P. J., & Rudensky, A. Y. (2013). Metabolites produced by commensal bacteria promote peripheral regulatory T-cell generation. Nature, 504(7480), 451–455.
Asher, M. I., Montefort, S., Björkstén, B., Lai, C. K., Strachan, D. P., Weiland, S. K., & Williams, H. (2006). Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. The Lancet, 368(9537), 733–743.
Atarashi, K., Tanoue, T., Oshima, K., Suda, W., Nagano, Y., Nishikawa, H., Fukuda, S., Saito, T., Narushima, S., Hase, K., Kim, S., Fritz, J. V., Wilmes, P., Ueha, S., Matsushima, K., Ohno, H., Olle, B., Sakaguchi, S., Taniguchi, T., Morita, H., Hattori, M., & Honda, K. (2013). Treg induction by a rationally selected mixture of Clostridia strains from the human microbiota. Nature, 500(7461), 232–236.
Avunduk, A. M., Avunduk, M. C., & Tekelioğlu, Y. (1998). Analysis of tears in patients with atopic keratoconjunctivitis, using flow cytometry. Ophthalmic Research, 30(1), 44–48.
Bach, J.-F. (2002). The Effect of Infections on Susceptibility to Autoimmune and Allergic Diseases. New England Journal of Medicine, 347(12), 911–920.
Bagnasco, D., Ferrando, M., Varricchi, G., Passalacqua, G., & Canonica, G. W. (2016). A Critical Evaluation of Anti-IL-13 and Anti-IL-4 Strategies in Severe Asthma. International Archives of Allergy and Immunology, 170(2), 122–131.

65
Barnes, K. C. (2015). Genes and atopic phenotypes. In Allergy, Immunity and Tolerance in Early Childhood : The First Steps of the Atopic March, edited by Hugh A. Sampson, and Hans Ulrich Wahn. Elsevier Science & Technology.
Barnes, K. C., Freidhoff, L. R., Nickel, R., Chiu, Y.-F., Juo, S.-H., Hizawa, N., Naidu, R. P., Ehrlich, E., Duffy, D. L., Schou, C., Levett, P. N., Marsh, D. G., & Beaty, T. H. (1999). Dense mapping of chromosome 12q13.12-q23.3 and linkage to asthma and atopy. Journal of Allergy and Clinical Immunology, 104(2), 485–491.
Barnish, M. S., Tagiyeva, N., Devereux, G., Aucott, L., & Turner, S. (2015). Diverging prevalences and different risk factors for childhood asthma and eczema: a cross-sectional study. BMJ Open, 5(6).
Bartemes, K. R., & Kita, H. (2012). Dynamic role of epithelium-derived cytokines in asthma. Clinical Immunology (Orlando, Fla.), 143(3), 222–235.
Basehore, M. J., Howard, T. D., Lange, L. A., Moore, W. C., Hawkins, G. A., Marshik, P. L., Harkins, M. S., Meyers, D. A., & Bleecker, E. R. (2004). A comprehensive evaluation of IL4 variants in ethnically diverse populations: association of total serum IgE levels and asthma in white subjects. The Journal of Allergy and Clinical Immunology, 114(1), 80–87.
Basnet, S., Bochkov, Y. A., Brockman-Schneider, R. A., Kuipers, I., Aesif, S. W., Jackson, D. J., Lemanske, R. F., Ober, C., Palmenberg, A. C., Gern, J. E., & Gern, J. E. (2019). CDHR3 Asthma-Risk Genotype Affects Susceptibility of Airway Epithelium to Rhinovirus C Infections. American Journal of Respiratory Cell and Molecular Biology, 61(4), 450–458.
Bauchau, V., & Durham, S. (2004). Prevalence and rate of diagnosis of allergic rhinitis in Europe. The European Respiratory Journal, 24(5).
Beghé, B., Barton, S., Rorke, S., Peng, Q., Sayers, I., Gaunt, T., Keith, T. P., Clough, J. B., Holgate, S. T., & Holloway, J. W. (2003). Polymorphisms in the interleukin-4 and interleukin-4 receptor alpha chain genes confer susceptibility to asthma and atopy in a Caucasian population. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 33(8), 1111–1117.
Bel, E. H., Wenzel, S. E., Thompson, P. J., Prazma, C. M., Keene, O. N., Yancey, S. W., Ortega, H. G., Pavord, I. D., & SIRIUS Investigators. (2014). Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. The New England Journal of Medicine, 371(13), 1189–1197.
Berenguer, A. G., Fernandes, A. T., Oliveira, S., Rodrigues, M., Ornelas, P., Romeira, D., Serrão, T., Rosa, A., & Câmara, R. (2014). Genetic polymorphisms and asthma: findings from a case-control study in the Madeira island population. Biological Research, 47(1), 40.
Bergroth, E., Aakula, M., Elenius, V., Remes, S., Piippo-Savolainen, E., Korppi, M., Piedra, P. A., Bochkov, Y. A., Gern, J. E., Camargo, C. A., Jartti, T., & Jartti, T. (2020). Rhinovirus Type in Severe Bronchiolitis and the Development of Asthma. The Journal of Allergy and Clinical Immunology. In Practice, 8(2), 588-595.e4.
Berry, A., & Busse, W. W. (2016). Biomarkers in asthmatic patients: Has their time come to direct treatment? The Journal of Allergy and Clinical Immunology, 137(5), 1317–1324.
Bidwell, J., Keen, L., Gallagher, G., Kimberly, R., Huizinga, T., McDermott, M. F., Oksenberg, J., McNicholl, J., Pociot, F., Hardt, C., & D’Alfonso, S. (1999). Cytokine gene polymorphism in human disease: on-line databases. Genes and Immunity, 1(1), 3–19.

66
Bielory, L., Delgado, L., Katelaris, C. H., Leonardi, A., Rosario, N., & Vichyanoud, P. (2020). ICON: Diagnosis and management of allergic conjunctivitis. Annals of Allergy, Asthma & Immunology : Official Publication of the American College of Allergy, Asthma, & Immunology, 124(2), 118–134.
Bielory, L., & Frohman, L. P. (1992). Allergic and immunologic disorders of the eye. The Journal of Allergy and Clinical Immunology, 89(1 Pt 1), 1–15.
Bielory, L., & Ghafoor, S. (2005). Histamine receptors and the conjunctiva. Current Opinion in Allergy and Clinical Immunology, 5(5), 437–440.
Bielory, L., Katelaris, C. H., Lightman, S., & Naclerio, R. M. (2007). Treating the ocular component of allergic rhinoconjunctivitis and related eye disorders. MedGenMed : Medscape General Medicine, 9(3), 35.
Black, S., Teixeira, A. S., Loh, A. X. W., Vinall, L., Holloway, J. W., Hardy, R., & Swallow, D. M. (2009). Contribution of functional variation in the IL13 gene to allergy, hay fever and asthma in the NSHD longitudinal 1946 birth cohort. Allergy, 64(8), 1172–1178.
Blackley, C. H. (1959). Experimental researches on the causes and nature of catarrhus aestivus (hay-fever or hay-asthma). Experimental Researches on the Causes and Nature of Catarrhus Aestivus (Hay-Fever or Hay-Asthma).
Blumenthal, M. N. (2005). The role of genetics in the development of asthma and atopy. Current Opinion in Allergy and Clinical Immunology, 5(2), 141–145.
Bochkov, Y. A., Watters, K., Ashraf, S., Griggs, T. F., Devries, M. K., Jackson, D. J., Palmenberg, A. C., & Gern, J. E. (2015). Cadherin-related family member 3, a childhood asthma susceptibility gene product, mediates rhinovirus C binding and replication. Proceedings of the National Academy of Sciences of the United States of America, 112(17), 5485–5490.
Bohle, B., Kinaciyan, T., Gerstmayr, M., Radakovics, A., Jahn-Schmid, B., & Ebner, C. (2007). Sublingual immunotherapy induces IL-10-producing T regulatory cells, allergen-specific T-cell tolerance, and immune deviation. The Journal of Allergy and Clinical Immunology, 120(3), 707–713.
Bonini, S., Bonini, S., Bucci, M. G., Berruto, A., Adriani, E., Balsano, F., & Allansmith, M. R. (1990). Allergen dose response and late symptoms in a human model of ocular allergy. The Journal of Allergy and Clinical Immunology, 86(6 Pt 1), 869–876.
Bønnelykke, K., Sleiman, P., Nielsen, K., Kreiner-Møller, E., Mercader, J. M., Belgrave, D., den Dekker, H. T., Husby, A., Sevelsted, A., Faura-Tellez, G., Mortensen, L. J., Paternoster, L., Flaaten, R., Mølgaard, A., Smart, D. E., Thomsen, P. F., Rasmussen, M. A., Bonàs-Guarch, S., Holst, C., Nohr, E. A., Yadav, R., March, M. E., Blicher, T., Lackie, P. M., Jaddoe, V. W. V, Simpson, A., Holloway, J. W., Duijts, L., Custovic, A., Davies, D. E., Torrents, D., Gupta, R., Hollegaard, M. V, Hougaard, D. M., Hakonarson, H., & Bisgaard, H. (2014). A genome-wide association study identifies CDHR3 as a susceptibility locus for early childhood asthma with severe exacerbations. Nature Genetics, 46(1), 51–55.
Botos, I., Segal, D. M., & Davies, D. R. (2011). The structural biology of Toll-like receptors. Structure (London, England : 1993), 19(4), 447–459.
Bourcier, T., Moldovan, M., Goldschild, M., Becquet, F., Brignole, F., Goguel, A., & Baudouin, C. (1998). Value of lacrymal IgE determination and conjunctival cytology in the diagnosis of chronic conjunctivitis. Journal Francais d’ophtalmologie, 21(3), 209–213.

67
Bousquet, J., Khaltaev, N., Cruz, A. A., Denburg, J., … Williams, D. (2008). Allergic Rhinitis and its Impact on Asthma (ARIA) 2008*. Allergy, 63(s86), 8–160.
Bousquet, J., Neukirch, F., Bousquet, P. J., Gehano, P., Klossek, J. M., Le Gal, M., & Allaf, B. (2006). Severity and impairment of allergic rhinitis in patients consulting in primary care. The Journal of Allergy and Clinical Immunology, 117(1), 158–162.
Bousquet, J., Van Cauwenberge, P., Khaltaev, N., Aria Workshop Group, & World Health Organization. (2001). Allergic rhinitis and its impact on asthma. The Journal of Allergy and Clinical Immunology, 108(5 Suppl), S147-334.
Bremond-Gignac, D., Donadieu, J., Leonardi, A., Pouliquen, P., Doan, S., Chiambarretta, F., Montan, P., Milazzo, S., Hoang-Xuan, T., Baudouin, C., & Aymé, S. (2008). Prevalence of vernal keratoconjunctivitis: a rare disease? The British Journal of Ophthalmology, 92(8), 1097–1102.
Brightling, C., Chanez, P., Leigh, R., O’Byrne, P. M., Korn, S., She, D., May, R. D., Streicher, K., Ranade, K., & Piper, E. (2015). Efficacy and safety of tralokinumab in patients with severe uncontrolled asthma: a randomised, double-blind, placebo-controlled, phase 2b trial. The Lancet. Respiratory Medicine, 3(9), 692–701.
Brightling, C., Gupta, S., Gonem, S., & Siddiqui, S. (2012). Lung damage and airway remodelling in severe asthma. Clinical & Experimental Allergy, 42(5), 638–649.
Brozek, J. L., Bousquet, J., Baena-Cagnani, C. E., Bonini, S., Canonica, G. W., Casale, T. B., van Wijk, R. G., Ohta, K., Zuberbier, T., Schünemann, H. J., Global Allergy and Asthma European Network, & Grading of Recommendations Assessment, Development and Evaluation Working Group. (2010). Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. The Journal of Allergy and Clinical Immunology, 126(3), 466–476.
Brusselle, G., Kips, J., Joos, G., Bluethmann, H., & Pauwels, R. (1995). Allergen-induced airway inflammation and bronchial responsiveness in wild-type and interleukin-4-deficient mice. American Journal of Respiratory Cell and Molecular Biology, 12(3), 254–259.
Bullens, D. M. A., Truyen, E., Coteur, L., Dilissen, E., Hellings, P. W., Dupont, L. J., & Ceuppens, J. L. (2006). IL-17 mRNA in sputum of asthmatic patients: linking T cell driven inflammation and granulocytic influx? Respiratory Research, 7(1), 135.
Burastero, S. E., Mistrello, G., Falagiani, P., Paolucci, C., Breda, D., Roncarolo, D., Zanotta, S., Monasterolo, G., & Rossi, R. E. (2008). Effect of sublingual immunotherapy with grass monomeric allergoid on allergen-specific T-cell proliferation and interleukin 10 production. Annals of Allergy, Asthma & Immunology : Official Publication of the American College of Allergy, Asthma, & Immunology, 100(4), 343–350.
Burrows, B., Martinez, F. D., Halonen, M., Barbee, R. A., & Cline, M. G. (1989). Association of asthma with serum IgE levels and skin-test reactivity to allergens. The New England Journal of Medicine, 320(5), 271–277.
Burte, E., Bousquet, J., Varraso, R., Gormand, F., Just, J., Matran, R., Pin, I., Siroux, V., Jacquemin, B., & Nadif, R. (2015). Characterization of Rhinitis According to the Asthma Status in Adults Using an Unsupervised Approach in the EGEA Study. PloS One, 10(8), e0136191.
Cahenzli, J., Köller, Y., Wyss, M., Geuking, M. B., & McCoy, K. D. (2013). Intestinal Microbial Diversity during Early-Life Colonization Shapes Long-Term IgE Levels. Cell Host & Microbe, 14(5), 559–570.
Canonica, G. W., Bousquet, J., Mullol, J., Scadding, G. K., Virchow, J. C., & Schatz, M. (2007). A survey of the burden of allergic rhinitis in Europe. Allergy, 62(s85), 9–16.

68
Carey, M. A., Card, J. W., Voltz, J. W., Arbes, S. J., Germolec, D. R., Korach, K. S., & Zeldin, D. C. (2007). It’s all about sex: gender, lung development and lung disease. Trends in Endocrinology & Metabolism, 18(8), 308–313.
Castro, M., Corren, J., Pavord, I. D., Maspero, J., Wenzel, S., Rabe, K. F., Busse, W. W., Ford, L., Sher, L., FitzGerald, J. M., Katelaris, C., Tohda, Y., Zhang, B., Staudinger, H., Pirozzi, G., Amin, N., Ruddy, M., Akinlade, B., Khan, A., Chao, J., Martincova, R., Graham, N. M. H., Hamilton, J. D., Swanson, B. N., Stahl, N., Yancopoulos, G. D., & Teper, A. (2018). Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. New England Journal of Medicine, 378(26), 2486–2496.
Castro, M., Mathur, S., Hargreave, F., Boulet, L.-P., Xie, F., Young, J., Wilkins, H. J., Henkel, T., Nair, P., & Res-5-0010 Study Group. (2011). Reslizumab for poorly controlled, eosinophilic asthma: a randomized, placebo-controlled study. American Journal of Respiratory and Critical Care Medicine, 184(10), 1125–1132.
Castro, M., Zangrilli, J., Wechsler, M. E., Bateman, E. D., Brusselle, G. G., Bardin, P., Murphy, K., Maspero, J. F., O’Brien, C., & Korn, S. (2015). Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. The Lancet. Respiratory Medicine, 3(5), 355–366.
Cavkaytar, O., Yilmaz, E. A., & Kalayci, O. (2013). Dupilumab in persistent asthma. The New England Journal of Medicine, 369(13), 1275–1276.
Chang, T. W., & Shiung, Y.-Y. (2006). Anti-IgE as a mast cell-stabilizing therapeutic agent. The Journal of Allergy and Clinical Immunology, 117(6), 1203–1212; quiz 1213.
Chen, J. J., Applebaum, D. S., Sun, G. S., & Pflugfelder, S. C. (2014). Atopic keratoconjunctivitis: A review. Journal of the American Academy of Dermatology, 70(3), 569–575.
Chen, Y., Kuchroo, V. K., Inobe, J., Hafler, D. A., & Weiner, H. L. (1994). Regulatory T cell clones induced by oral tolerance: suppression of autoimmune encephalomyelitis. Science (New York, N.Y.), 265(5176), 1237–1240.
Chen, Z.-G., Zhang, T.-T., Li, H.-T., Chen, F.-H., Zou, X.-L., Ji, J.-Z., & Chen, H. (2013). Neutralization of TSLP inhibits airway remodeling in a murine model of allergic asthma induced by chronic exposure to house dust mite. PloS One, 8(1), e51268.
Chiang, C.-H., Tang, Y.-C., Lin, M.-W., & Chung, M.-Y. (2007). Association between the IL-4 promoter polymorphisms and asthma or severity of hyperresponsiveness in Taiwanese. Respirology, 12(1), 42–48.
Chou, C., & Li, M. O. (2018). Tissue-Resident Lymphocytes Across Innate and Adaptive Lineages. Frontiers in Immunology, 9, 2104.
Chung, K. F. (2015). Targeting the interleukin pathway in the treatment of asthma. The Lancet, 386(9998), 1086–1096.
Chupp, G. L., Bradford, E. S., Albers, F. C., Bratton, D. J., Wang-Jairaj, J., Nelsen, L. M., Trevor, J. L., Magnan, A., & Brinke, A. ten. (2017). Efficacy of mepolizumab add-on therapy on health-related quality of life and markers of asthma control in severe eosinophilic asthma (MUSCA): a randomised, double-blind, placebo-controlled, parallel-group, multicentre, phase 3b trial. The Lancet Respiratory Medicine, 5(5), 390–400.
Ciprandi, G., Buscaglia, S., Pesce, G., Pronzato, C., Ricca, V., Parmiani, S., Bagnasco, M., & Canonica, G. W. (1995). Minimal persistent inflammation is present at mucosal level in patients with asymptomatic rhinitis and mite allergy. The Journal of Allergy and Clinical Immunology, 96(6 Pt 1), 971–979.

69
Cirillo, I., Marseglia, G., Klersy, C., & Ciprandi, G. (2007). Allergic patients have more numerous and prolonged respiratory infections than nonallergic subjects. Allergy, 62(9), 1087–1090.
Coca, A., & Cooke, R. A. (1923). On the Classification of the Phenomena of Hypersensitiveness. In The Journal of Immunology (Vol. 8, Issue 3). Williams & Wilkins.
Cooke, G. E., Doshi, A., & Binkley, P. F. (2007). Endothelial nitric oxide synthase gene: prospects for treatment of heart disease. Pharmacogenomics, 8(12), 1723–1734.
Cookson, W. (1999). The alliance of genes and environment in asthma and allergy. Nature, 402(6760supp), 5–11.
Corren, J., Lemanske, R. F., Hanania, N. A., Korenblat, P. E., Parsey, M. V, Arron, J. R., Harris, J. M., Scheerens, H., Wu, L. C., Su, Z., Mosesova, S., Eisner, M. D., Bohen, S. P., & Matthews, J. G. (2011). Lebrikizumab treatment in adults with asthma. The New England Journal of Medicine, 365(12), 1088–1098.
Corren, J., Parnes, J. R., Wang, L., Mo, M., Roseti, S. L., Griffiths, J. M., & van der Merwe, R. (2017). Tezepelumab in Adults with Uncontrolled Asthma. New England Journal of Medicine, 377(10), 936–946.
Corry, D. B., Folkesson, H. G., Warnock, M. L., Erle, D. J., Matthay, M. A., Wiener-Kronish, J. P., & Locksley, R. M. (1996). Interleukin 4, but not interleukin 5 or eosinophils, is required in a murine model of acute airway hyperreactivity. The Journal of Experimental Medicine, 183(1), 109–117.
Cosmi, L., Santarlasci, V., Angeli, R., Liotta, F., Maggi, L., Frosali, F., Rossi, O., Falagiani, P., Riva, G., Romagnani, S., Annunziato, F., & Maggi, E. (2006). Sublingual immunotherapy with Dermatophagoides monomeric allergoid down-regulates allergen-specific immunoglobulin E and increases both interferon-gamma- and interleukin-10-production. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 36(3), 261–272.
Cox, A., Camp, N. J., Nicklin, M. J., di Giovine, F. S., Duff, G. W., Thomson, W., Pepper, L., & al., et. (1998). An analysis of linkage disequilibrium in the interleukin-1 gene cluster, using a novel grouping method for multiallelic markers. American Journal of Human Genetics, 62(5), 1180–1188.
Coyle, A. J., Le Gros, G., Bertrand, C., Tsuyuki, S., Heusser, C. H., Kopf, M., & Anderson, G. P. (1995). Interleukin-4 is required for the induction of lung Th2 mucosal immunity. American Journal of Respiratory Cell and Molecular Biology, 13(1), 54–59.
CSGA. (1997). A genome-wide search for asthma susceptibility loci in ethnically diverse populations. Nature Genetics, 15(4), 389–392.
Dabbagh, K., Takeyama, K., Lee, H.-M., Ueki, I. F., Lausier, J. A., & Nadel, J. A. (1999). IL-4 Induces Mucin Gene Expression and Goblet Cell Metaplasia In Vitro and In Vivo. The Journal of Immunology, 162(10).
Daniels, S. E., Bhattacharrya, S., James, A., Leaves, N. I., Young, A., Hill, M. R., Faux, J. A., Ryan, G. F., le Söuef, P. N., Lathrop, G. M., Musk, A. W., & Cookson, W. O. C. M. (1996). A genome-wide search for quantitative trait loci underlying asthma. Nature, 383(6597), 247–250.
Davis, L., Marten, R., & ISarkany, I. (1961). Atopic eczema in European and Negro West Indian infants in London. The British Journal of Dermatology, 73.
Davoodi, P., Mahesh, P. A., Holla, A. D., & Ramachandra, N. B. (2015). A preliminary study on the association of single nucleotide polymorphisms of interleukin 4 (IL4), IL13,

70
IL4 receptor alpha (IL4Rα) & Toll-like receptor 4 (TLR4) genes with asthma in Indian adults. The Indian Journal of Medical Research, 142(6), 675–680.
de Marco, R., Cappa, V., Accordini, S., Rava, M., … Verlato, G. (2012). Trends in the prevalence of asthma and allergic rhinitis in Italy between 1991 and 2010. The European Respiratory Journal, 39(4), 883–892.
de Marco, R., Locatelli, F., Sunyer, J., & Burney, P. (2000). Differences in incidence of reported asthma related to age in men and women. A retrospective analysis of the data of the European Respiratory Health Survey. American Journal of Respiratory and Critical Care Medicine, 162(1), 68–74.
De Smedt, S., Wildner, G., & Kestelyn, P. (2013). Vernal keratoconjunctivitis: an update. The British Journal of Ophthalmology, 97(1), 9–14.
Deichmann, K., Bardutzky, J., Forster, J., Heinzmann, A., & Kuehr, J. (1997). Common Polymorphisms in the Coding Part of the IL4-Receptor Gene. Biochemical and Biophysical Research Communications, 231(3), 696–697.
Diamant, Z., Diderik Boot, J., Christian Virchow, J., Z, D., JD, B., & JC, V. (2007). Summing up 100 years of asthma. Respiratory Medicine, 101(3).
Dick, S., Friend, A., Dynes, K., AlKandari, F., Doust, E., Cowie, H., Ayres, J. G., & Turner, S. W. (2014). A systematic review of associations between environmental exposures and development of asthma in children aged up to 9 years. BMJ Open, 4(11), e006554.
Dinarello, C. A. (2018). Overview of the IL-1 family in innate inflammation and acquired immunity. Immunological Reviews, 281(1), 8–27.
Dinarello, CA A. (1996). Biologic basis for interleukin-1 in disease. Blood, 87(6), 2095–2147. Dizier, M.-H., Bouzigon, E., Guilloud-Bataille, M., Bétard, C., Bousquet, J., Charpin, D.,
Gormand, F., Hochez, J., Just, J., Lemainque, A., Le Moual, N., Matran, R., Neukirch, F., Oryszczyn, M.-P., Paty, E., Pin, I., Vervloet, D., Kauffmann, F., Lathrop, M., Demenais, F., & Annesi-Maesano, I. (2005). Genome screen in the French EGEA study: detection of linked regions shared or not shared by allergic rhinitis and asthma. Genes & Immunity, 6(2), 95–102.
Dizier, M. H., Besse-Schmittler, C., Guilloud-Bataille, M., Annesi-Maesano, I., Boussaha, M., Bousquet, J., Charpin, D., Degioanni, A., Gormand, F., Grimfeld, A., Hochez, J., Hyne, G., Lockhart, A., Luillier-Lacombe, M., Matran, R., Meunier, F., Neukirch, F., Pacheco, Y., Parent, V., Paty, E., Pin, I., Pison, C., Scheinmann, P., Thobie, N., Vervloet, D., Kauffmann, F., Feingold, J., Lathrop, M., & Demenais, F. (2000). Genome Screen for Asthma and Related Phenotypes in the French EGEA Study. American Journal of Respiratory and Critical Care Medicine, 162(5), 1812–1818.
Duffy, D. L., Martin, N. G., Battistutta, D., Hopper, J. L., & Mathews, J. D. (1990). Genetics of asthma and hay fever in Australian twins. The American Review of Respiratory Disease, 142(6 Pt 1), 1351–1358.
Duggan, E. M., Sturley, J., Fitzgerald, A. P., Perry, I. J., & Hourihane, J. O. (2012). The 2002-2007 trends of prevalence of asthma, allergic rhinitis and eczema in Irish schoolchildren. Pediatric Allergy and Immunology, 23(5), 464–471.
Eisenbarth, S. C., Piggott, D. A., Huleatt, J. W., Visintin, I., Herrick, C. A., & Bottomly, K. (2002). Lipopolysaccharide-enhanced, toll-like receptor 4-dependent T helper cell type 2 responses to inhaled antigen. The Journal of Experimental Medicine, 196(12), 1645–1651.
Elenius, V., & Jartti, T. (2016). Vaccines: could asthma in young children be a preventable disease? . Pediatric Allergy and Immunology, 27(7), 682–686.

71
Emson, C. L., Bell, S. E., Jones, A., Wisden, W., & McKenzie, A. N. (1998). Interleukin (IL)-4-independent induction of immunoglobulin (Ig)E, and perturbation of T cell development in transgenic mice expressing IL-13. The Journal of Experimental Medicine, 188(2), 399–404.
Erbek, S. S., Yurtcu, E., Erbek, S., Atac, F. B., Sahin, F. I., & Cakmak, O. (2007). Proinflammatory cytokine single nucleotide polymorphisms in nasal polyposis. Archives of Otolaryngology--Head & Neck Surgery, 133(7), 705–709.
Eriksson, U., Egermann, U., Bihl, M. P., Gambazzi, F., Tamm, M., Holt, P. G., & Bingisser, R. M. (2005). Human bronchial epithelium controls TH2 responses by TH1-induced, nitric oxide-mediated STAT5 dephosphorylation: implications for the pathogenesis of asthma. Journal of Immunology (Baltimore, Md. : 1950), 175(4), 2715–2720.
Fagerås Böttcher, M., Hmani-Aifa, M., Lindström, A., Jenmalm, M. C., Mai, X.-M., Nilsson, L., Zdolsek, H. A., Björkstén, B., Söderkvist, P., & Vaarala, O. (2004). A TLR4 polymorphism is associated with asthma and reduced lipopolysaccharide-induced interleukin-12(p70) responses in Swedish children. The Journal of Allergy and Clinical Immunology, 114(3), 561–567.
Fahy, J. V. (2015). Type 2 inflammation in asthma--present in most, absent in many. Nature Reviews. Immunology, 15(1), 57–65.
Ferreira, M. A. R., Matheson, M. C., Duffy, D. L., Marks, G. B., Hui, J., Le Souëf, P., Danoy, P., Baltic, S., Nyholt, D. R., Jenkins, M., Hayden, C., Willemsen, G., Ang, W., Kuokkanen, M., Beilby, J., Cheah, F., de Geus, E. J. C., Ramasamy, A., Vedantam, S., Salomaa, V., Madden, P. A., Heath, A. C., Hopper, J. L., Visscher, P. M., Musk, B., Leeder, S. R., Jarvelin, M.-R., Pennell, C., Boomsma, D. I., Hirschhorn, J. N., Walters, H., Martin, N. G., James, A., Jones, G., Abramson, M. J., Robertson, C. F., Dharmage, S. C., Brown, M. A., Montgomery, G. W., Thompson, P. J., & Australian Asthma Genetics Consortium. (2011). Identification of IL6R and chromosome 11q13.5 as risk loci for asthma. Lancet (London, England), 378(9795), 1006–1014.
Ferreira, M. A. R., Mathur, R., Vonk, J. M., Szwajda, A., Brumpton, B., Granell, R., Brew, B. K., Ullemar, V., Lu, Y., Jiang, Y., 23andMe Research Team, P. K. E., eQTLGen Consortium, R., BIOS Consortium, D. A., Magnusson, P. K. E., Karlsson, R., Hinds, D. A., Paternoster, L., Koppelman, G. H., & Almqvist, C. (2019). Genetic Architectures of Childhood- and Adult-Onset Asthma Are Partly Distinct. American Journal of Human Genetics, 104(4), 665–684.
FitzGerald, J. M., Bleecker, E. R., Nair, P., Korn, S., Ohta, K., Lommatzsch, M., Ferguson, G. T., Busse, W. W., Barker, P., Sproule, S., Gilmartin, G., Werkström, V., Aurivillius, M., Goldman, M., & CALIMA study investigators. (2016). Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet (London, England), 388(10056), 2128–2141.
Francis, J. N., Till, S. J., & Durham, S. R. (2003). Induction of IL-10+CD4+CD25+ T cells by grass pollen immunotherapy. The Journal of Allergy and Clinical Immunology, 111(6), 1255–1261.
Fukagawa, K., Nakajima, T., Saito, H., Tsubota, K., Shimmura, S., Natori, M., & Hirai, K. (2000). IL-4 Induces Eotaxin Production in Corneal Keratocytes but Not in Epithelial Cells. International Archives of Allergy and Immunology, 121(2), 144–150.
Furusawa, Y., Obata, Y., Fukuda, S., Endo, T. A., Nakato, G., Takahashi, D., Nakanishi, Y., Uetake, C., Kato, K., Kato, T., Takahashi, M., Fukuda, N. N., Murakami, S., Miyauchi,

72
E., Hino, S., Atarashi, K., Onawa, S., Fujimura, Y., Lockett, T., Clarke, J. M., Topping, D. L., Tomita, M., Hori, S., Ohara, O., Morita, T., Koseki, H., Kikuchi, J., Honda, K., Hase, K., & Ohno, H. (2013). Commensal microbe-derived butyrate induces the differentiation of colonic regulatory T cells. Nature, 504(7480), 446–450.
Gause, W. C., Wynn, T. A., Allen, J. E., WC, G., TA, W., & JE, A. (2013). Type 2 immunity and wound healing: evolutionary refinement of adaptive immunity by helminths. Nature Reviews. Immunology, 13(8), 607–614.
Gauvreau, G. M., O’Byrne, P. M., Boulet, L.-P., Wang, Y., Cockcroft, D., Bigler, J., FitzGerald, J. M., Boedigheimer, M., Davis, B. E., Dias, C., Gorski, K. S., Smith, L., Bautista, E., Comeau, M. R., Leigh, R., & Parnes, J. R. (2014). Effects of an anti-TSLP antibody on allergen-induced asthmatic responses. The New England Journal of Medicine, 370(22), 2102–2110.
Gavett, S. H., O’Hearn, D. J., Karp, C. L., Patel, E. A., Schofield, B. H., Finkelman, F. D., & Wills-Karp, M. (1997). Interleukin-4 receptor blockade prevents airway responses induced by antigen challenge in mice. The American Journal of Physiology, 272(2 Pt 1), L253-61.
Geraldini, M., Neto, H. J. C., Riedi, C. A., & Rosário, N. A. (2013). Epidemiology of ocular allergy and co-morbidities in adolescents. Jornal de Pediatria, 89(4), 354–360.
Gershon, A. S., Guan, J., Wang, C., & To, T. (2010). Trends in Asthma Prevalence and Incidence in Ontario, Canada, 1996-2005: A Population Study. American Journal of Epidemiology, 172(6), 728–736.
Geuking, M. B., Cahenzli, J., Lawson, M. A. E., Ng, D. C. K., Slack, E., Hapfelmeier, S., McCoy, K. D., & Macpherson, A. J. (2011). Intestinal Bacterial Colonization Induces Mutualistic Regulatory T Cell Responses. Immunity, 34(5), 794–806.
Global Initiative for Asthma. (2020). 2020 Global Initiative for Asthma Report: Global Strategy for Asthma Management and Prevention. ginasthma.org
Godfrey, V., Chan, S.-L., Cassidy, A., Butler, R., Choy, A., Fardon, T., Struthers, A., & Lang, C. (2007). The functional consequence of the Glu298Asp polymorphism of the endothelial nitric oxide synthase gene in young healthy volunteers. Cardiovascular Drug Reviews, 25(3), 280–288.
Gounni, A. S., Lamkhioued, B., Koussih, L., Ra, C., Renzi, P. M., & Hamid, Q. (2001). Human neutrophils express the high-affinity receptor for immunoglobulin E (Fc epsilon RI): role in asthma. FASEB Journal : Official Publication of the Federation of American Societies for Experimental Biology, 15(6), 940–949.
Gour, N., & Wills-Karp, M. (2015). IL-4 and IL-13 signaling in allergic airway disease. Cytokine, 75(1), 68–78.
Grabstein, K. H., Park, L. S., Morrissey, P. J., Sassenfeld, H., Price, V., Urdal, D. L., & Widmer, M. B. (1987). Regulation of murine T cell proliferation by B cell stimulatory factor-1. Journal of Immunology, 139(4), 1148–1153.
Green, R. H., Brightling, C. E., Woltmann, G., Parker, D., Wardlaw, A. J., & Pavord, I. D. (2002). Analysis of induced sputum in adults with asthma: identification of subgroup with isolated sputum neutrophilia and poor response to inhaled corticosteroids. Thorax, 57(10), 875–879.
Gros, P.-A., Nagard, H. Le, & Tenaillon, O. (2009). The Evolution of Epistasis and Its Links With Genetic Robustness, Complexity and Drift in a Phenotypic Model of Adaptation. Genetics, 182(1), 277.

73
Grünig, G., Warnock, M., Wakil, A. E., Venkayya, R., Brombacher, F., Rennick, D. M., Sheppard, D., Mohrs, M., Donaldson, D. D., Locksley, R. M., & Corry, D. B. (1998). Requirement for IL-13 independently of IL-4 in experimental asthma. Science (New York, N.Y.), 282(5397), 2261–2263.
Guarnieri, M., & Balmes, J. R. (2014). Outdoor air pollution and asthma. Lancet (London, England), 383(9928), 1581–1592.
Haagerup, A., Bjerke, T., Schøitz, P. O., Binderup, H. G., Dahl, R., & Kruse, T. A. (2001). Allergic rhinitis – a total genome-scan for susceptibility genes suggests a locus on chromosome 4q24-q27. European Journal of Human Genetics, 9(12), 945–952.
Haahtela, T., Herse, F., Karjalainen, J., Klaukka, T., Linna, M., Leskelä, R.-L., Selroos, O., & Reissell, E. (2017). The Finnish experience to save asthma costs by improving care in 1987-2013. The Journal of Allergy and Clinical Immunology, 139(2), 408-414.e2.
Hackstein, H., Hecker, M., Kruse, S., Bohnert, A., Ober, C., Deichmann, K. A., & Bein, G. (2001). A novel polymorphism in the 5′ promoter region of the human interleukin-4 receptor α-chain gene is associated with decreased soluble interleukin-4 receptor protein levels. Immunogenetics, 53(4), 264–269.
Hakonarson, H., Bjornsdottir, U. S., Halapi, E., Palsson, S., Adalsteinsdottir, E., Gislason, D., Finnbogason, G., Gislason, T., Kristjansson, K., Arnason, T., Birkisson, I., Frigge, M. L., Kong, A., Gulcher, J. R., & Stefansson, K. (2002). A major susceptibility gene for asthma maps to chromosome 14q24. American Journal of Human Genetics, 71(3), 483–491.
Haldar, P., Brightling, C. E., Hargadon, B., Gupta, S., Monteiro, W., Sousa, A., Marshall, R. P., Bradding, P., Green, R. H., Wardlaw, A. J., & Pavord, I. D. (2009). Mepolizumab and exacerbations of refractory eosinophilic asthma. The New England Journal of Medicine, 360(10), 973–984.
Halim, T. Y. F., Steer, C. A., Mathä, L., Gold, M. J., Martinez-Gonzalez, I., McNagny, K. M., McKenzie, A. N. J., & Takei, F. (2014). Group 2 innate lymphoid cells are critical for the initiation of adaptive T helper 2 cell-mediated allergic lung inflammation. Immunity, 40(3), 425–435.
Haller, G., Torgerson, D. G., Ober, C., & Thompson, E. E. (2009). Sequencing the IL4 locus in African Americans implicates rare noncoding variants in asthma susceptibility. The Journal of Allergy and Clinical Immunology, 124(6), 1204-9.e9.
Hammad, H., Chieppa, M., Perros, F., Willart, M. A., Germain, R. N., & Lambrecht, B. N. (2009). House dust mite allergen induces asthma via Toll-like receptor 4 triggering of airway structural cells. Nature Medicine, 15(4), 410–416.
Hanania, N. A., Wenzel, S., Rosén, K., Hsieh, H.-J., Mosesova, S., Choy, D. F., Lal, P., Arron, J. R., Harris, J. M., & Busse, W. (2013). Exploring the Effects of Omalizumab in Allergic Asthma. American Journal of Respiratory and Critical Care Medicine, 187(8), 804–811.
Hansel, F. K. (1929). Clinical and histopathologic studies of the nose and sinuses in allergy. Journal of Allergy, 1(1), 43–70.
Hansen, T. E., Evjenth, B., & Holt, J. (2013). Increasing prevalence of asthma, allergic rhinoconjunctivitis and eczema among schoolchildren: three surveys during the period 1985-2008. Acta Paediatrica, 102(1), 47–52.
Hanski, I., von Hertzen, L., Fyhrquist, N., Koskinen, K., Torppa, K., Laatikainen, T., Karisola, P., Auvinen, P., Paulin, L., Mäkelä, M. J., Vartiainen, E., Kosunen, T. U., Alenius, H., & Haahtela, T. (2012). Environmental biodiversity, human microbiota,

74
and allergy are interrelated. Proceedings of the National Academy of Sciences of the United States of America, 109(21), 8334–8339.
Harada, M., Obara, K., Hirota, T., Yoshimoto, T., Hitomi, Y., Sakashita, M., Doi, S., Miyatake, A., Fujita, K., Enomoto, T., Taniguchi, M., Higashi, N., Fukutomi, Y., Nakanishi, K., Nakamura, Y., & Tamari, M. (2009). A Functional Polymorphism in IL-18 Is Associated with Severity of Bronchial Asthma. American Journal of Respiratory and Critical Care Medicine, 180(11), 1048–1055.
Heinzmann, A., Mao, X.-Q., Akaiwa, M., Kreomer, R. T., Gao, P.-S., Ohshima, K., Umeshita, R., Abe, Y., Braun, S., Yamashita, T., Roberts, M. H., Sugimoto, R., Arima, K., Arinobu, Y., Yu, B., Kruse, S., Enomoto, T., Dake, Y., Kawai, M., Shimazu, S., Sasaki, S., Adra, C. N., Kitaichi, M., Inoue, H., Yamauchi, K., Tomichi, N., Kurimoto, F., Hamasaki, N., Hopkin, J. M., Izuhara, K., Shirakawa, T., & Deichmann, K. A. (2000). Genetic variants of IL-13 signalling and human asthma and atopy. Human Molecular Genetics, 9(4), 549–559.
Henderson, W. R., Chi, E. Y., Maliszewski, C. R., Neben, T. Y., Finnerty, H., Henderson, S. L., O’Hara, R. M., Beier, D. R., Turner, K. J., Wood, C. R., & Collins, M. (2000). Soluble IL-4 receptor inhibits airway inflammation following allergen challenge in a mouse model of asthma. Journal of Immunology (Baltimore, Md. : 1950), 164(2), 1086–1095.
Herbst, T., Sichelstiel, A., Schär, C., Yadava, K., Bürki, K., Cahenzli, J., McCoy, K., Marsland, B. J., & Harris, N. L. (2011). Dysregulation of Allergic Airway Inflammation in the Absence of Microbial Colonization. American Journal of Respiratory and Critical Care Medicine, 184(2), 198–205.
Heredia, J. E., Mukundan, L., Chen, F. M., Mueller, A. A., Deo, R. C., Locksley, R. M., Rando, T. A., & Chawla, A. (2013). Type 2 innate signals stimulate fibro/adipogenic progenitors to facilitate muscle regeneration. Cell, 153(2), 376–388.
Hershey, G. K. K., Friedrich, M. F., Esswein, L. A., Thomas, M. L., & Chatila, T. A. (1997). The Association of Atopy with a Gain-of-Function Mutation in the α Subunit of the Interleukin-4 Receptor. New England Journal of Medicine, 337(24), 1720–1725.
Hill, D. A., Siracusa, M. C., Abt, M. C., Kim, B. S., Kobuley, D., Kubo, M., Kambayashi, T., LaRosa, D. F., Renner, E. D., Orange, J. S., Bushman, F. D., & Artis, D. (2012). Commensal bacteria–derived signals regulate basophil hematopoiesis and allergic inflammation. Nature Medicine, 18(4), 538–546.
Ho, L. P., Wood, F. T., Robson, A., Innes, J. A., & Greening, A. P. (2000). Atopy influences exhaled nitric oxide levels in adult asthmatics. Chest, 118(5), 1327–1331.
Holgate, S. (2015). Asthma. In Mucosal Immunology (pp. 1833–1856). Elsevier. Hollá, L., Bucková, D., Kuhrová, V., Stejskalová, A., Francová, H., Znojil, V., & Vácha, J.
(2002). Prevalence of Endothelial Nitric Oxide Synthase Gene Polymorphisms in Patients With Atopic Asthma. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 32(8).
Holloway, Dunbar, Riley, Sawyer, Fitzharris, Pearce, Le Gros, L., & Beasley. (2000). Association of beta2-adrenergic receptor polymorphisms with severe asthma. Clinical & Experimental Allergy, 30(8), 1097–1103.
Hom, S., & Pisano, M. (2017). Reslizumab (Cinqair): An Interleukin-5 Antagonist for Severe Asthma of the Eosinophilic Phenotype. P & T : A Peer-Reviewed Journal for Formulary Management, 42(9), 564–568.

75
Howard, T. D., Koppelman, G. H., Xu, J., Zheng, S. L., Postma, D. S., Meyers, D. D. A., Bleecker, E. R. E., Meyers, A., Aarden, L., Zee, J. van der, Solway, J., Blumenthal, M., King, R., Xu, J., Meyers, D. D. A., Bleecker, E. R. E., & Cox, N. (2002). Gene-gene Interaction in Asthma: IL4RA and IL13 in a Dutch Population With Asthma. American Journal of Human Genetics, 70(1), 230–236.
Hsiao, H.-P., Lin, M.-C., Wu, C.-C., Wang, C.-C., & Wang, T.-N. (2019). Sex-Specific Asthma Phenotypes, Inflammatory Patterns, and Asthma Control in a Cluster Analysis. The Journal of Allergy and Clinical Immunology. In Practice, 7(2), 556-567.e15.
Huang, C., Li, F., Wang, J., & Tian, Z. (2019). Innate-like Lymphocytes and Innate Lymphoid Cells in Asthma. Clinical Reviews in Allergy & Immunology.
Humbert, M., Durham, S. R., Ying, S., Kimmitt, P., Barkans, J., Assoufi, B., Pfister, R., Menz, G., Robinson, D. S., Kay, A. B., & Corrigan, C. J. (1996). IL-4 and IL-5 mRNA and protein in bronchial biopsies from patients with atopic and nonatopic asthma: evidence against "intrinsic" asthma being a distinct immunopathologic entity. American Journal of Respiratory and Critical Care Medicine, 154(5), 1497–1504.
Hussein, I. A., & Jaber, S. H. (2017). Genotyping of IL-4 -590 (C/T) Gene in Iraqi Asthma Patients. Disease Markers, 2017, 5806236.
Ilmarinen, P., Tuomisto, L. E., Niemelä, O., Tommola, M., Haanpää, J., & Kankaanranta, H. (2017). Cluster Analysis on Longitudinal Data of Patients with Adult-Onset Asthma. The Journal of Allergy and Clinical Immunology: In Practice, 5(4), 967-978.e3.
Iordanidou, M., Paraskakis, E., Tavridou, A., Chatzimichael, A., & Manolopoulos, V. G. (2017). Endothelial nitric oxide synthase gene polymorphisms are associated with sensitization to seasonal aeroallergens in asthmatic children. World Journal of Pediatrics : WJP, 13(1), 34–40.
Janeway, C. A., & Medzhitov, R. (2002). Innate immune recognition. Annual Review of Immunology, 20, 197–216.
Jartti, T., Bønnelykke, K., Elenius, V., & Feleszko, W. (2020). Role of viruses in asthma. Seminars in Immunopathology, 42(1), 61–74.
Jartti, T., Smits, H. H., Bønnelykke, K., Bircan, O., Elenius, V., Konradsen, J. R., Maggina, P., Makrinioti, H., Stokholm, J., Hedlin, G., Papadopoulos, N., Ruszczynski, M., Ryczaj, K., Schaub, B., Schwarze, J., Skevaki, C., Stenberg-Hammar, K., Feleszko, W., & EAACI Task Force on Clinical Practice Recommendations on Preschool Wheeze, E. T. F. on C. P. R. on P. (2019). Bronchiolitis needs a revisit: Distinguishing between virus entities and their treatments. Allergy, 74(1), 40–52.
Jarvis, D., Newson, R., Lotvall, J., Hastan, D., Tomassen, P., Keil, T., Gjomarkaj, M., Forsberg, B., Gunnbjornsdottir, M., Minov, J., Brozek, G., Dahlen, S. E., Toskala, E., Kowalski, M. L., Olze, H., Howarth, P., Krämer, U., Baelum, J., Loureiro, C., Kasper, L., Bousquet, P. J., Bousquet, J., Bachert, C., Fokkens, W., & Burney, P. (2012). Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy, 67(1), 91–98.
Josefowicz, S. Z., Niec, R. E., Kim, H. Y., Treuting, P., Chinen, T., Zheng, Y., Umetsu, D. T., & Rudensky, A. Y. (2012). Extrathymically generated regulatory T cells control mucosal TH2 inflammation. Nature, 482(7385), 395–399.
Joshi, M. S., Mineo, C., Shaul, P. W., & Bauer, J. A. (2007). Biochemical consequences of the NOS3 Glu298Asp variation in human endothelium: altered caveolar localization and impaired response to shear. FASEB Journal : Official Publication of the Federation of American Societies for Experimental Biology, 21(11), 2655–2663.

76
Jousilahti, P., Haahtela, T., Laatikainen, T., Mäkelä, M., & Vartiainen, E. (2016). Asthma and respiratory allergy prevalence is still increasing among Finnish young adults. The European Respiratory Journal, 47(3), 985–987.
Just, J., Saint-Pierre, P., Gouvis-Echraghi, R., Laoudi, Y., Roufai, L., Momas, I., & Annesi Maesano, I. (2014). Childhood Allergic Asthma Is Not a Single Phenotype. The Journal of Pediatrics, 164(4), 815–820.
Justiz Vaillant, A. A., Modi, P., & Jan, A. (2020). Atopy. In StatPearls. StatPearls Publishing. Jutel, M., & Akdis, C. A. (2008). T-Cell Regulatory Mechanisms in Specific Immunotherapy.
In T Cell Regulation in Allergy, Asthma and Atopic Skin Diseases (Vol. 94, pp. 158–177). Karger Publishers.
Jutel, M., Akdis, M., Budak, F., Aebischer-Casaulta, C., Wrzyszcz, M., Blaser, K., & Akdis, C. A. (2003). IL-10 and TGF-beta cooperate in the regulatory T cell response to mucosal allergens in normal immunity and specific immunotherapy. European Journal of Immunology, 33(5), 1205–1214.
Kabesch, M., Schedel, M., Carr, D., Woitsch, B., Fritzsch, C., Weiland, S. K., & von Mutius, E. (2006). IL-4/IL-13 pathway genetics strongly influence serum IgE levels and childhood asthma. The Journal of Allergy and Clinical Immunology, 117(2), 269–274.
Kabesch, M., Tzotcheva, I., Carr, D., Höfler, C., Weiland, S. K., Fritzsch, C., von Mutius, E., & Martinez, F. D. (2003). A complete screening of the IL4 gene. Journal of Allergy and Clinical Immunology, 112(5), 893–898.
Karjalainen, A., Kurppa, K., Martikainen, R., Karjalainen, J., & Klaukka, T. (2002). Exploration of asthma risk by occupation--extended analysis of an incidence study of the Finnish population. Scandinavian Journal of Work, Environment & Health, 28(1), 49–57.
Karjalainen, A., Kurppa, K., Martikainen, R., Klaukka, T., & Karjalainen, J. (2001). Work Is Related to a Substantial Portion of Adult-onset Asthma Incidence in the Finnish Population. American Journal of Respiratory and Critical Care Medicine, 164(4), 565–568.
Karjalainen, J., Hulkkonen, J., Pessi, T., Huhtala, H., Nieminen, M. M., Aromaa, A., Klaukka, T., & Hurme, M. (2002). The IL1A genotype associates with atopy in nonasthmatic adults. Journal of Allergy and Clinical Immunology, 110(3), 429–434.
Karjalainen, J., Joki-Erkkilä, V.-P., Hulkkonen, J., Pessi, T., Nieminen, M. M., Aromaa, A., Klaukka, T., & Hurme, M. (2003). The IL1A genotype is associated with nasal polyposis in asthmatic adults. Allergy, 58(5), 393–396.
Kauppi, P., Laitinen, L. A., Laitinen, H., Kere, J., & Laitinen, T. (1998). Verification of self-reported asthma and allergy in subjects and their family members volunteering for gene mapping studies. Respiratory Medicine, 92(11), 1281–1288.
Kermani, F., Flint, M. S., & Hotchkiss, S. A. M. (2000). Induction and Localization of Cutaneous Interleukin-1β mRNA during Contact Sensitization. Toxicology and Applied Pharmacology, 169(3), 231–237.
Kissick, H. T., Sanda, M. G., Dunn, L. K., Pellegrini, K. L., On, S. T., Noel, J. K., & Arredouani, M. S. (2014). Androgens alter T-cell immunity by inhibiting T-helper 1 differentiation. Proceedings of the National Academy of Sciences of the United States of America, 111(27), 9887–9892.
Klein, S. L., & Flanagan, K. L. (2016). Sex differences in immune responses. Nature Reviews. Immunology, 16(10), 626–638.
Kolb, H., Kolb-Bachofen, V., H, K., & V, K.-B. (1998). Nitric oxide in autoimmune disease: cytotoxic or regulatory mediator? Immunology Today, 19(12), 556–561.

77
Kruse, L. V., Nyegaard, M., Christensen, U., Møller-Larsen, S., Haagerup, A., Deleuran, M., Hansen, L. G., Venø, S. K., Goossens, D., Del-Favero, J., & Børglum, A. D. (2012). A genome-wide search for linkage to allergic rhinitis in Danish sib-pair families. European Journal of Human Genetics : EJHG, 20(9), 965–972.
Kruse, S., Japha, T., Tedner, M., Sparholt, S., Forster, J., Kuehr, J., & Deichmann, K. (1999). The polymorphisms S503P and Q576R in the interleukin-4 receptor α gene are associated with atopy and influence the signal transduction. Immunology, 96(3).
Kumagai, N., Fukuda, K., & Nishida, T. (2000). Synergistic effect of TNF-alpha and IL-4 on the expression of thymus- and activation-regulated chemokine in human corneal fibroblasts. Biochemical and Biophysical Research Communications, 279(1), 1–5.
Kurukulaaratchy, R. J., Karmaus, W., Raza, A., Matthews, S., Roberts, G., & Arshad, S. H. (2011). The influence of gender and atopy on the natural history of rhinitis in the first 18 years of life. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 41(6), 851–859.
Kuruvilla, M. E., Lee, F. E.-H., & Lee, G. B. (2019). Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clinical Reviews in Allergy & Immunology, 56(2), 219–233.
Kurz, T., Altmueller, J., Strauch, K., Rüschendorf, F., Heinzmann, A., Moffatt, M. F., Cookson, W. O. C. M., Inacio, F., Nürnberg, P., Stassen, H. H., & Deichmann, K. A. (2005). A genome-wide screen on the genetics of atopy in a multiethnic European population reveals a major atopy locus on chromosome 3q21.3. Allergy, 60(2), 192–199.
La, E., & Fischer, S. M. (2001). Transcriptional regulation of intracellular IL-1 receptor antagonist gene by IL-1 alpha in primary mouse keratinocytes. Journal of Immunology, 166(10), 6149–6155.
Laffont, S., Blanquart, E., & Guéry, J.-C. (2017). Sex Differences in Asthma: A Key Role of Androgen-Signaling in Group 2 Innate Lymphoid Cells. Frontiers in Immunology, 8, 1069.
Laffont, S., Blanquart, E., Savignac, M., Cénac, C., Laverny, G., Metzger, D., Girard, J.-P., Belz, G. T., Pelletier, L., Seillet, C., & Guéry, J.-C. (2017). Androgen signaling negatively controls group 2 innate lymphoid cells. The Journal of Experimental Medicine, 214(6), 1581–1592.
Lahita, R. (2000). Gender and the immune system. J Gend Specif Med, 3, 19–22. Laitinen, T., Daly, M. J., Rioux, J. D., Kauppi, P., Laprise, C., Petäys, T., Green, T., Cargill,
M., Haahtela, T., Lander, E. S., Laitinen, L. A., Hudson, T. J., & Kere, J. (2001). A susceptibility locus for asthma-related traits on chromosome 7 revealed by genome-wide scan in a founder population. Nature Genetics, 28(1), 87–91.
Laitinen, T., Polvi, A., Rydman, P., Vendelin, J., Pulkkinen, V., Salmikangas, P., Mäkelä, S., Rehn, M., Pirskanen, A., Rautanen, A., Zucchelli, M., Gullstén, H., Leino, M., Alenius, H., Petäys, T., Haahtela, T., Laitinen, A., Laprise, C., Hudson, T. J., Laitinen, L. A., & Kere, J. (2004). Characterization of a common susceptibility locus for asthma-related traits. Science (New York, N.Y.), 304(5668), 300–304.
Lambrecht, B. N., & Hammad, H. (2014). The immunology of asthma. Nature Immunology, 16(1), 45–56.
Lang, K. S., Recher, M., Junt, T., Navarini, A. A., Harris, N. L., Freigang, S., Odermatt, B., Conrad, C., Ittner, L. M., Bauer, S., Luther, S. A., Uematsu, S., Akira, S., Hengartner,

78
H., & Zinkernagel, R. M. (2005). Toll-like receptor engagement converts T-cell autoreactivity into overt autoimmune disease. Nature Medicine, 11(2), 138–145.
Lanier, L. L. (2013). Shades of grey--the blurring view of innate and adaptive immunity. Nature Reviews. Immunology, 13(2), 73–74.
Lasky-Su, J., Himes, B. E., Raby, B. A., Klanderman, B. J., Sylvia, J. S., Lange, C., Melen, E., Martinez, F. D., Israel, E., Gauderman, J., Gilliland, F., Sleiman, P., Hakonarson, H., Celedón, J. C., Soto-Quiros, M., Avila, L., Lima, J. J., Irvin, C. G., Peters, S. P., Boushey, H., Chinchilli, V. M., Mauger, D., Tantisira, K., Weiss, S. T., & SHARP investigators. (2012). HLA-DQ strikes again: genome-wide association study further confirms HLA-DQ in the diagnosis of asthma among adults. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 42(12), 1724–1733.
Lathrop, S. K., Bloom, S. M., Rao, S. M., Nutsch, K., Lio, C.-W., Santacruz, N., Peterson, D. A., Stappenbeck, T. S., & Hsieh, C.-S. (2011). Peripheral education of the immune system by colonic commensal microbiota. Nature, 478(7368), 250–254.
Lee, S., Kwon, M.-S., & Park, T. (2012). Network Graph Analysis of Gene-Gene Interactions in Genome-Wide Association Study Data. Genomics & Informatics, 10(4), 256.
Lee, S. Y., Lee, Y. H., Shin, C., Shim, J. J., Kang, K. H., Yoo, S. H., & In, K. H. (2002). Association of asthma severity and bronchial hyperresponsiveness with a polymorphism in the cytotoxic T-lymphocyte antigen-4 gene. Chest, 122(1), 171–176.
Leibowitz, U., Antonovsky, A., Medalie, J. M., Smith, H. A., Halpern, L., & Alter, M. (1966). Epidemiological study of multiple sclerosis in Israel. II. Multiple sclerosis and level of sanitation. Journal of Neurology, Neurosurgery, and Psychiatry, 29(1), 60–68.
Leonardi, A. (2013). Allergy and allergic mediators in tears. Experimental Eye Research, 117, 106–117.
Leonardi, A., Bogacka, E., Fauquert, J. L., Kowalski, M. L., Groblewska, A., Jedrzejczak-Czechowicz, M., Doan, S., Marmouz, F., Demoly, P., & Delgado, L. (2012). Ocular allergy: recognizing and diagnosing hypersensitivity disorders of the ocular surface. Allergy, 67(11), 1327–1337.
Leonardi, A., Curnow, S. J., Zhan, H., & Calder, V. L. (2006). Multiple cytokines in human tear specimens in seasonal and chronic allergic eye disease and in conjunctival fibroblast cultures. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 36(6), 777–784.
Leonardi, A., DeFranchis, G., Zancanaro, F., Crivellari, G., De Paoli, M., Plebani, M., & Secchi, A. G. (1999). Identification of local Th2 and Th0 lymphocytes in vernal conjunctivitis by cytokine flow cytometry. Investigative Ophthalmology & Visual Science, 40(12), 3036–3040.
Leonardi, A., Motterle, L., & Bortolotti, M. (2008). Allergy and the eye. Clinical and Experimental Immunology, 153 Suppl(Suppl 1), 17–21.
Leonardi, A., Piliego, F., Castegnaro, A., Lazzarini, D., La Gloria Valerio, A., Mattana, P., & Fregona, I. (2015). Allergic conjunctivitis: a cross-sectional study. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 45(6), 1118–1125.
Leung, T. F., Liu, E. K. H., Tang, N. L. S., Ko, F. W. S., Li, C. Y., Lam, C. W. K., & Wong, G. W. K. (2005). Nitric oxide synthase polymorphisms and asthma phenotypes in Chinese children. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 35(10), 1288–1294.

79
Leung, T. F., Wong, G. W. K., Ko, F. W. S., Lam, C. W. K., & Fok, T. F. (2005). Clinical and atopic parameters and airway inflammatory markers in childhood asthma: a factor analysis. Thorax, 60(10), 822–826.
Leynaert, B., Neukirch, C., Kony, S., Guénégou, A., Bousquet, J., Aubier, M., & Neukirch, F. (2004). Association between asthma and rhinitis according to atopic sensitization in a population-based study. The Journal of Allergy and Clinical Immunology, 113(1), 86–93.
Leynaert, B., Sunyer, J., Garcia-Esteban, R., Svanes, C., Jarvis, D., Cerveri, I., Dratva, J., Gislason, T., Heinrich, J., Janson, C., Kuenzli, N., de Marco, R., Omenaas, E., Raherison, C., Gómez Real, F., Wjst, M., Zemp, E., Zureik, M., Burney, P. G. J., Anto, J. M., & Neukirch, F. (2012). Gender differences in prevalence, diagnosis and incidence of allergic and non-allergic asthma: a population-based cohort. Thorax, 67(7), 625–631.
Li, J., Zhang, Y., & Zhang, L. (2015). Discovering susceptibility genes for allergic rhinitis and allergy using a genome-wide association study strategy. Current Opinion in Allergy and Clinical Immunology, 15(1), 33–40.
Li, M., Wang, Z.-N., Yang, L.-F., Yan, Y., Cai, L.-M., Li, Y.-T., Qiao, Y.-K., & Chen, Z.-G. (2017). TLR4 antagonist suppresses airway remodeling in asthma by inhibiting the T-helper 2 response. Experimental and Therapeutic Medicine, 14(4), 2911–2916.
Lien, E., Means, T. K., Heine, H., Yoshimura, A., Kusumoto, S., Fukase, K., Fenton, M. J., Oikawa, M., Qureshi, N., Monks, B., Finberg, R. W., Ingalls, R. R., & Golenbock, D. T. (2000). Toll-like receptor 4 imparts ligand-specific recognition of bacterial lipopolysaccharide. Journal of Clinical Investigation, 105(4), 497.
Liggett, S. B. (1995). Genetics of beta2-adrenergic receptor variants in asthma. Clinical & Experimental Allergy, 25(s2), 89–94.
List, B. M., Klösch, B., Völker, C., Gorren, A. C., Sessa, W. C., Werner, E. R., Kukovetz, W. R., Schmidt, K., & Mayer, B. (1997). Characterization of bovine endothelial nitric oxide synthase as a homodimer with down-regulated uncoupled NADPH oxidase activity: tetrahydrobiopterin binding kinetics and role of haem in dimerization. The Biochemical Journal, 323(Pt 1), 159–165.
Liu, A. H. (2002). Endotoxin exposure in allergy and asthma: reconciling a paradox. The Journal of Allergy and Clinical Immunology, 109(3), 379–392.
Liu, X., Beaty, T. H., Deindl, P., Huang, S.-K., Lau, S., Sommerfeld, C., Fallin, M. D., Kao, W. L., Wahn, U., & Nickel, R. (2003). Associations between total serum IgE levels and the 6 potentially functional variants within the genes IL4 , IL13 , and IL4RA in German children: The German Multicenter Atopy Study. Journal of Allergy and Clinical Immunology, 112(2), 382–388.
Liu, Y., Liu, T., Nie, W., Lai, G., Xiu, Q., Liu, Y., Liu, T., Nie, W., Lai, G., & Xiu, Q. (2013). Interleukin-13 +1923C/T polymorphism is associated with asthma risk: a meta-analysis. BioMed Research International, 2013, 1–9.
Liu, Y., Maxwell, S., Feng, T., Zhu, X., Elston, R. C., Koyutürk, M., & Chance, M. R. (2012). Gene, pathway and network frameworks to identify epistatic interactions of single nucleotide polymorphisms derived from GWAS data. BMC Systems Biology, 6(Suppl 3), S15.
Lorentz, A., Schwengberg, S., Sellge, G., Manns, M. P., & Bischoff, S. C. (2000). Human intestinal mast cells are capable of producing different cytokine profiles: role of IgE receptor cross-linking and IL-4. Journal of Immunology, 164(1), 43–48.

80
Lozano, F., Places, L., Vila, J.-M., Padilla, O., Arman, M., Gimferrer, I., Suarez, B., Lopez de la Iglesia, A., Miserachs, N., Vives, J., F, L., L, P., JM, V., O, P., M, A., I, G., B, S., A, L. de la I., N, M., & J, V. (2001). Identification of a Novel Single-Nucleotide Polymorphism (Val554Ile) and Definition of Eight Common Alleles for Human IL4RA Exon 11. Tissue Antigens, 57(3), 216–220.
Lynch, S. V, & Boushey, H. A. (2016). The microbiome and development of allergic disease. Current Opinion in Allergy and Clinical Immunology, 16(2), 165–171.
MacMicking, J., Xie, Q., & Nathan, C. (1997). Nitric oxide and macrophage function. Annual Review of Immunology, 15(1), 323–350.
Malerba, G., Trabetti, E., Patuzzo, C., Lauciello, M. C., Galavotti, R., Pescollderungg, L., Boner, A. L., & Pignatti, P. F. (1999). Candidate genes and a genome-wide search in Italian families with atopic asthmatic children. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 29 Suppl 4, 27–30.
Manolio, T. A., Barnes, K. C., Beaty, T. H., Levett, P. N., Naidu, R. P., & Wilson, A. F. (2003). Sex differences in heritability of sensitization to Blomia tropicalis in asthma using regression of offspring on midparent (ROMP) methods. Human Genetics, 113(5), 437–446.
Marsden, P. A., Q Heng, H. H., Scherer, S. W., Stewart, R. J., Xiao-Mei Shi, A. V, Tsui, L.-C., & Schappert, K. T. (1993). Structure and Chromosomal Localization of the Human Constitutive Endothelial Nitric Oxide Synthase Gene*. In The Journal of Biological Chemistry (Vol. 268, Issue 23).
Marsh, D. G., Neely, J. D., Breazeale, D. R., Ghosh, B., Freidhoff, L. R., Ehrlich-Kautzky, E., Schou, C., Krishnaswamy, G., & Beaty, T. H. (1994). Linkage analysis of IL4 and other chromosome 5q31.1 markers and total serum immunoglobulin E concentrations. Science (New York, N.Y.), 264(5162), 1152–1156.
Martinez-Gonzalez, I., Steer, C. A., & Takei, F. (2015). Lung ILC2s link innate and adaptive responses in allergic inflammation. Trends in Immunology, 36(3), 189–195.
Mathias, R. A. (2014). Introduction to genetics and genomics in asthma: genetics of asthma. Advances in Experimental Medicine and Biology, 795, 125–155.
Matsuda, A., Okayama, Y., Terai, N., Yokoi, N., Ebihara, N., Tanioka, H., Kawasaki, S., Inatomi, T., Katoh, N., Ueda, E., Hamuro, J., Murakami, A., & Kinoshita, S. (2009). The Role of Interleukin-33 in Chronic Allergic Conjunctivitis. Investigative Opthalmology & Visual Science, 50(10), 4646.
Maurer, M., & Zuberbier, T. (2007). Undertreatment of rhinitis symptoms in Europe: findings from a cross-sectional questionnaire survey. Allergy, 62(9), 1057–1063.
Mccoy, K. D., Harris, N. L., Diener, P., Hatak, S., Odermatt, B., Hangartner, L., Senn, B. M., Marsland, B. J., Geuking, M. B., Hengartner, H., Macpherson, A. J. S. S., & Zinkernagel, R. M. (2006). Natural IgE Production in the Absence of MHC Class II Cognate Help. Immunity, 24(3), 329–339.
Meiler, F., Klunker, S., Zimmermann, M., Akdis, C. A., & Akdis, M. (2008). Distinct regulation of IgE, IgG4 and IgA by T regulatory cells and toll-like receptors. Allergy, 63(11), 1455–1463.
Michel, O., LeVan, T., Stern, D., Dentener, M., Thorn, J., Gnat, D., Beijer, M., Cochaux, P., Holt, P., Martinez, F., & Rylander, R. (2003). Systemic responsiveness to lipopolysaccharide and polymorphisms in the toll-like receptor 4 gene in human beings. The Journal of Allergy and Clinical Immunology, 112(5).

81
Mims, J. W. (2015). Asthma: definitions and pathophysiology. International Forum of Allergy & Rhinology, 5(S1), S2–S6.
Miraldi Utz, V., & Kaufman, A. R. (2014). Allergic eye disease. Pediatric Clinics of North America, 61(3), 607–620.
Mitsuyasu, H., Izuhara, K., Mao, X., Gao, P., Arinobu, Y., Enomoto, T., M, K., S, S., Y, D., N, H., T, S., & JM, H. (1998). Ile50Val Variant of IL4R Alpha Upregulates IgE Synthesis and Associates With Atopic Asthma. Nature Genetics, 19(2).
Moffatt, M. F., Gut, I. G., Demenais, F., Strachan, D. P., Bouzigon, E., Heath, S., Mutius, E. von, Farrall, M., Lathrop, M., Cookson, W. O. C. M. C. M., von Mutius, E., Farrall, M., Lathrop, M., Cookson, W. O. C. M. C. M., & GABRIEL Consortium. (2010). A Large-Scale, Consortium-Based Genomewide Association Study of Asthma. New England Journal of Medicine, 363(13), 1211–1221.
Moffatt, M. F., Kabesch, M., Liang, L., Dixon, A. L., Strachan, D., Heath, S., Depner, M., von Berg, A., Bufe, A., Rietschel, E., Heinzmann, A., Simma, B., Frischer, T., Willis-Owen, S. A. G., Wong, K. C. C., Illig, T., Vogelberg, C., Weiland, S. K., von Mutius, E., Abecasis, G. R., Farrall, M., Gut, I. G., Lathrop, G. M., & Cookson, W. O. C. (2007). Genetic variants regulating ORMDL3 expression contribute to the risk of childhood asthma. Nature, 448(7152), 470–473.
Mogensen, T. H. (2009). Pathogen recognition and inflammatory signaling in innate immune defenses. Clinical Microbiology Reviews, 22(2), 240–273, Table of Contents.
Moncada, S., & Higgs, A. (1993). The L-arginine-nitric oxide pathway. The New England Journal of Medicine, 329(27), 2002–2012.
Monticelli, L. A., Sonnenberg, G. F., Abt, M. C., Alenghat, T., Ziegler, C. G. K., Doering, T. A., Angelosanto, J. M., Laidlaw, B. J., Yang, C. Y., Sathaliyawala, T., Kubota, M., Turner, D., Diamond, J. M., Goldrath, A. W., Farber, D. L., Collman, R. G., Wherry, E. J., & Artis, D. (2011). Innate lymphoid cells promote lung-tissue homeostasis after infection with influenza virus. Nature Immunology, 12(11), 1045–1054.
Mortha, A., Chudnovskiy, A., Hashimoto, D., Bogunovic, M., Spencer, S. P., Belkaid, Y., & Merad, M. (2014). Microbiota-dependent crosstalk between macrophages and ILC3 promotes intestinal homeostasis. Science (New York, N.Y.), 343(6178), 1249288.
Munthe-Kaas, M. C., Carlsen, K. H., Håland, G., Devulapalli, C. S., Gervin, K., Egeland, T., Carlsen, K. L., & Undlien, D. (2008). T cell-specific T-box transcription factor haplotype is associated with allergic asthma in children. The Journal of Allergy and Clinical Immunology, 121(1), 51–56.
Nair, P., Pizzichini, M. M. M., Kjarsgaard, M., Inman, M. D., Efthimiadis, A., Pizzichini, E., Hargreave, F. E., & O’Byrne, P. M. (2009). Mepolizumab for prednisone-dependent asthma with sputum eosinophilia. The New England Journal of Medicine, 360(10), 985–993.
Nakamura, Y., Suzuki, R., Mizuno, T., Abe, K., Chiba, S., Horii, Y., Tsuboi, J., Ito, S., Obara, W., Tanita, T., Kanno, H., & Yamauchi, K. (2016). Therapeutic implication of genetic variants of IL13 and STAT4 in airway remodelling with bronchial asthma. Clinical & Experimental Allergy, 46(9), 1152–1161.
Nakashima, H., Miyake, K., Inoue, Y., Shimizu, S., Akahoshi, M., Tanaka, Y., Otsuka, T., & Harada, M. (2002). Association between IL-4 genotype and IL-4 production in the Japanese population. Genes and Immunity, 3(2), 107–109.
Narożna, B., Hoffmann, A., Sobkowiak, P., Schoneich, N., Bręborowicz, A., & Szczepankiewicz, A. (2016). Polymorphisms in the interleukin 4, interleukin 4

82
receptor and interleukin 13 genes and allergic phenotype: A case control study. Advances in Medical Sciences, 61(1), 40–45.
National Agency for Medicine and Kela. (1998). The national sickness insurance and reimbursement of medicine expenses. Finnish Statistics on Medicines 1997.
Nature Genetics. (1999). Freely associating. Nature Genetics, 22(1), 1–2. Newby, C., Heaney, L. G., Menzies-Gow, A., Niven, R. M., Mansur, A., Bucknall, C.,
Chaudhuri, R., Thompson, J., Burton, P., Brightling, C., & Network, on behalf of the B. T. S. S. R. A. (2014). Statistical Cluster Analysis of the British Thoracic Society Severe Refractory Asthma Registry: Clinical Outcomes and Phenotype Stability. PLoS ONE, 9(7), e102987.
Nguyen, K. D., Qiu, Y., Cui, X., Goh, Y. P. S., Mwangi, J., David, T., Mukundan, L., Brombacher, F., Locksley, R. M., & Chawla, A. (2011). Alternatively activated macrophages produce catecholamines to sustain adaptive thermogenesis. Nature, 480(7375), 104–108.
NHGRI-EBI GWAS Catalog. (2020). NHGRI-EBI GWAS Catalog. https://www.ebi.ac.uk/gwas/
Nicolae, D., Cox, N. J., Lester, L. A., Schneider, D., Tan, Z., Billstrand, C., Kuldanek, S., Donfack, J., Kogut, P., Patel, N. M., Goodenbour, J., Howard, T., Wolf, R., Koppelman, G. H., White, S. R., Parry, R., Postma, D. S., Meyers, D., Bleecker, E. R., Hunt, J. S., Solway, J., & Ober, C. (2005). Fine mapping and positional candidate studies identify HLA-G as an asthma susceptibility gene on chromosome 6p21. American Journal of Human Genetics, 76(2), 349–357.
Nie, W., Liu, Y., Bian, J., Li, B., & Xiu, Q. (2013). Effects of Polymorphisms -1112C/T and +2044A/G in Interleukin-13 Gene on Asthma Risk: A Meta-Analysis. PLoS ONE, 8(2), e56065.
Noguchi, E., Nishimura, F., Fukai, H., Kim, J., Ichikawa, K., Shibasaki, M., & Arinami, T. (2004). An association study of asthma and total serum immunoglobin E levels for Toll-like receptor polymorphisms in a Japanese population. Clinical & Experimental Allergy, 34(2), 177–183.
Noguchi, E., Nukaga-Nishio, Y., Jian, Z., Yokouchi, Y., Kamioka, M., Yamakawa-Kobayashi, K., Hamaguchi, H., Matsui, A., Shibasaki, M., & Arinami, T. (2001). Haplotypes of the 5′ region of the IL-4 gene and SNPs in the intergene sequence between the IL-4 and IL-13 genes are associated with atopic asthma. Human Immunology, 62(11), 1251–1257.
Noguchi, E., Shibasaki, M., Arinami, T., Takeda, K., Yokouchi, Y., Kawashima, T., Yanagi, H., Matsui, A., & Hamaguchi, H. (1998). Association of asthma and the interleukin-4 promoter gene in Japanese. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 28(4), 449–453.
Noguchi, E., Yokouchi, Y., Zhang, J., Shibuya, K., Shibuya, A., Bannai, M., Tokunaga, K., Doi, H., Tamari, M., Shimizu, M., Shirakawa, T., Shibasaki, M., Ichikawa, K., & Arinami, T. (2005). Positional Identification of an Asthma Susceptibility Gene on Human Chromosome 5q33. American Journal of Respiratory and Critical Care Medicine, 172(2), 183–188.
O’Brien, T. P. (2013). Allergic conjunctivitis: an update on diagnosis and management. Current Opinion in Allergy and Clinical Immunology, 13(5), 543–549.
Ober, C., Cox, N. J., Abney, M., Di Rienzo, A., Lander, E. S., Changyaleket, B., Gidley, H., Kurtz, B., Lee, J., Nance, M., Pettersson, A., Prescott, J., Richardson, A., Schlenker,

83
E., Summerhill, E., Willadsen, S., & Parry, R. (1998). Genome-wide search for asthma susceptibility loci in a founder population. The Collaborative Study on the Genetics of Asthma. Human Molecular Genetics, 7(9), 1393–1398.
Ober, C., & Hoffjan, S. (2006). Asthma genetics 2006: the long and winding road to gene discovery. Genes & Immunity, 7(2), 95–100.
Ober, C., Leavitt, S. A., Tsalenko, A., Howard, T. D., Hoki, D. M., Daniel, R., Newman, D. L., Wu, X., Parry, R., Lester, L. A., Solway, J., Blumenthal, M., King, R. A., Xu, J., Meyers, D. A., Bleecker, E. R., Cox, N. J., et al. (2000). Variation in the Interleukin 4-receptor Alpha Gene Confers Susceptibility to Asthma and Atopy in Ethnically Diverse Populations. American Journal of Human Genetics, 66(2), 517–526.
Ober, C., Tsalenko, A., Parry, R., & Cox, N. J. (2000). A second-generation genomewide screen for asthma-susceptibility alleles in a founder population. American Journal of Human Genetics, 67(5), 1154–1162.
Okada, H., Kuhn, C., Feillet, H., & Bach, J.-F. (2010). The ‘hygiene hypothesis’ for autoimmune and allergic diseases: an update. Clinical and Experimental Immunology, 160(1), 1.
Ono, S. J., & Abelson, M. B. (2005). Allergic conjunctivitis: update on pathophysiology and prospects for future treatment. The Journal of Allergy and Clinical Immunology, 115(1), 118–122.
Ortega, H. G., Liu, M. C., Pavord, I. D., Brusselle, G. G., FitzGerald, J. M., Chetta, A., Humbert, M., Katz, L. E., Keene, O. N., Yancey, S. W., Chanez, P., & MENSA Investigators. (2014). Mepolizumab treatment in patients with severe eosinophilic asthma. The New England Journal of Medicine, 371(13), 1198–1207.
Pallasaho, P., Juusela, M., Lindqvist, A., Sovijärvi, A., Lundbäck, B., & Rönmark, E. (2011). Allergic rhinoconjunctivitis doubles the risk for incident asthma--results from a population study in Helsinki, Finland. Respiratory Medicine, 105(10), 1449–1456.
Palm, N. W., Rosenstein, R. K., & Medzhitov, R. (2012). Allergic host defences. Nature, 484(7395), 465–472.
Palmares, J., Delgado, L., Cidade, M., Quadrado, M. J., Filipe, H. P., & Season Study Group. (2010). Allergic conjunctivitis: a national cross-sectional study of clinical characteristics and quality of life. European Journal of Ophthalmology, 20(2), 257–264.
Palmer, L. J., Burton, P. R., James, A. L., Musk, A. W., & Cookson, W. O. (2000). Familial aggregation and heritability of asthma-associated quantitative traits in a population-based sample of nuclear families. European Journal of Human Genetics, 8(11), 853–860.
Palmer, R. M., Ashton, D. S., & Moncada, S. (1988). Vascular endothelial cells synthesize nitric oxide from L-arginine. Nature, 333(6174), 664–666.
Paul, W. E., & Seder, R. A. (1994). Lymphocyte Responses and Cytokines. Cell, 76(2), 241–251.
Pavord, I. D., Korn, S., Howarth, P., Bleecker, E. R., Buhl, R., Keene, O. N., Ortega, H., & Chanez, P. (2012). Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet (London, England), 380(9842), 651–659.
Pefura-Yone, E. W., Kengne, A. P., Balkissou, A. D., Boulleys-Nana, J. R., Efe-de-Melingui, N. R., Ndjeutcheu-Moualeu, P. I., Mbele-Onana, C. L., Kenmegne-Noumsi, E. C., Kolontchang-Yomi, B. L., Theubo-Kamgang, B. J., Ebouki, E. R., Djuikam-Kamga, C. K., Magne-Fotso, C. G., Amougou, F., Mboumtou, L., Ngo-Yonga, M., Petchou-Talla, E. L., Afane-Ze, E., Kuaban, C., (RGRDC), R. G. for R. D. in C., & Research

84
Group for Respiratory Disease in Cameroon (RGRDC). (2015). Prevalence of asthma and allergic rhinitis among adults in Yaounde, Cameroon. PloS One, 10(4), e0123099.
Pelikan, Z. (2012). Cytological changes in tears during the secondary conjunctival response induced by nasal allergy. The British Journal of Ophthalmology, 96(7), 941–948.
Perussia, B., & Loza, M. J. (2003). Linear ‘2–0–1’ lymphocyte development: hypotheses on cellular bases for immunity. Trends in Immunology, 24(5), 235–241.
Pessi, T., Karjalainen, J., Hulkkonen, J., & Nieminen, M. M. (2003). A common IL-1 complex haplotype is associated with an increased risk of atopy. In J Med Genet (Vol. 40).
Phillips, P. C. (2008). Epistasis—the essential role of gene interactions in the structure and evolution of genetic systems. Nature Reviews. Genetics, 9(11), 855.
Pinto, L. A., Stein, R. T., & Kabesch, M. (2008). Impact of genetics in childhood asthma. Jornal de Pediatria, 0(0).
Piper, E., Brightling, C., Niven, R., Oh, C., Faggioni, R., Poon, K., She, D., Kell, C., May, R. D., Geba, G. P., & Molfino, N. A. (2013). A phase II placebo-controlled study of tralokinumab in moderate-to-severe asthma. The European Respiratory Journal, 41(2), 330–338.
Pividori, M., Schoettler, N., Nicolae, D. L., Ober, C., & Im, H. K. (2019). Shared and distinct genetic risk factors for childhood-onset and adult-onset asthma: genome-wide and transcriptome-wide studies. The Lancet. Respiratory Medicine, 7(6), 509–522.
Portelli, M. A., Hodge, E., & Sayers, I. (2015). Genetic risk factors for the development of allergic disease identified by genome-wide association. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 45(1), 21–31.
Potaczek, D. P., Nishiyama, C., Sanak, M., Szczeklik, A., & Okumura, K. (2009). Genetic variability of the high-affinity IgE receptor α-subunit (FcεRIα). Immunologic Research, 45(1), 75–84.
Price, A. E., Liang, H.-E., Sullivan, B. M., Reinhardt, R. L., Eisley, C. J., Erle, D. J., & Locksley, R. M. (2010). Systemically dispersed innate IL-13-expressing cells in type 2 immunity. Proceedings of the National Academy of Sciences of the United States of America, 107(25), 11489–11494.
Pulleyn, L. J., Newton, R., Adcock, I. M., & Barnes, P. J. (2001). TGFβ1 allele association with asthma severity. Human Genetics, 109(6), 623–627.
Pykäläinen, M., Kinos, R., Valkonen, S., Rydman, P., Kilpeläinen, M., Laitinen, L. A., Karjalainen, J., Nieminen, M., Hurme, M., Kere, J., Laitinen, T., & Lahesmaa, R. (2005). Association analysis of common variants of STAT6, GATA3, and STAT4 to asthma and high serum IgE phenotypes. The Journal of Allergy and Clinical Immunology, 115(1), 80–87.
Qi, S., Liu, G., Dong, X., Huang, N., Li, W., & Chen, H. (2018). Microarray data analysis to identify differentially expressed genes and biological pathways associated with asthma. Experimental and Therapeutic Medicine, 16(3), 1613.
Quansah, R., Jaakkola, M. S., Hugg, T. T., Heikkinen, S. A. M., & Jaakkola, J. J. K. (2012). Residential Dampness and Molds and the Risk of Developing Asthma: A Systematic Review and Meta-Analysis. PLoS ONE, 7(11), e47526.
Raby, B. A., Klimecki, W. T., Laprise, C., Renaud, Y., Faith, J., Lemire, M., Greenwood, C., Weiland, K. M., Lange, C., Palmer, L. J., Lazarus, R., Vercelli, D., Kwiatkowski, D. J., Silverman, E. K., Martinez, F. D., Hudson, T. J., & Weiss, S. T. (2002). Polymorphisms in Toll-Like Receptor 4 Are Not Associated with Asthma or Atopy-

85
related Phenotypes. American Journal of Respiratory and Critical Care Medicine, 166(11), 1449–1456.
Rael, E. L., Lockey, R. F., Masoli, M., Fabian, D., … Abbas, A. (2011). Interleukin-13 Signaling and Its Role in Asthma. World Allergy Organization Journal, 4(3), 54–64.
Raghavan, D., & Jain, R. (2016). Increasing awareness of sex differences in airway diseases. Respirology (Carlton, Vic.), 21(3), 449–459.
Reed, C. E., & Milton, D. K. (2001). Endotoxin-stimulated innate immunity: A contributing factor for asthma. Journal of Allergy and Clinical Immunology, 108(2), 157–166.
Rees, J., & Pattani, S. (2010). Asthma Sixth Edition. John Wiley & Sons, Chichester. Ricciardolo, F. L. M., Di Stefano, A., Sabatini, F., & Folkerts, G. (2006). Reactive nitrogen
species in the respiratory tract. European Journal of Pharmacology, 533(1–3), 240–252. Risch, N. J. (2000). Searching for genetic determinants in the new millennium. Nature,
405(6788), 847–856. Romagnani, S., Romagnani, S., Abbas, A. K., Murphy, K. M., … al., et. (1997). The Th1/Th2
paradigm. Immunology Today, 18(6), 263–266. Rosario, N., & Bielory, L. (2011). Epidemiology of allergic conjunctivitis. Current Opinion in
Allergy and Clinical Immunology, 11(5), 471–476. Rosenwasser, L. (1996). Genetics of asthma and atopy. Toxicology Letters, 86(2–3), 73–77. Rosenwasser, L., & Borish, L. (1997). Genetics of Atopy and Asthma: The Rationale behind
Promoter-based Candidate Gene Studies (IL-4 and IL-10). American Journal of Respiratory and Critical Care Medicine, 156(4), S152–S155.
Rosenwasser, L., Klemm, D. J., Dresback, J. K., Inamura, H., Mascali, J. J., Klinnert, M., & Borish, L. (1995). Promoter polymorphisms in the chromosome 5 gene cluster in asthma and atopy. Clinical & Experimental Allergy, 25(s2), 74–78.
Ryu, J.-H., Yoo, J.-Y., Kim, M.-J., Hwang, S.-G., Ahn, K. C., Ryu, J.-C., Choi, M.-K., Joo, J. H., Kim, C.-H., Lee, S.-N., Lee, W.-J., Kim, J., Shin, D. M., Kweon, M.-N., Bae, Y. S., & Yoon, J.-H. (2013). Distinct TLR-mediated pathways regulate house dust mite-induced allergic disease in the upper and lower airways. The Journal of Allergy and Clinical Immunology, 131(2), 549–561.
Saito, J., Inoue, K., Sugawara, A., Yoshikawa, M., Watanabe, K., Ishida, T., Ohtsuka, Y., & Munakata, M. (2004). Exhaled nitric oxide as a marker of airway inflammation for an epidemiologic study in schoolchildren. The Journal of Allergy and Clinical Immunology, 114(3), 512–516.
Savolainen, J., Jacobsen, L., & Valovirta, E. (2006). Sublingual immunotherapy in children modulates allergen-induced in vitro expression of cytokine mRNA in PBMC. Allergy, 61(10), 1184–1190.
Savolainen, J., Laaksonen, K., Rantio-Lehtimäki, A., & Terho, E. O. (2004). Increased expression of allergen-induced in vitro interleukin-10 and interleukin-18 mRNA in peripheral blood mononuclear cells of allergic rhinitis patients after specific immunotherapy. Clinical and Experimental Allergy : Journal of the British Society for Allergy and Clinical Immunology, 34(3), 413–419.
Schatz, M., Hsu, J.-W. Y., Zeiger, R. S., Chen, W., Dorenbaum, A., Chipps, B. E., & Haselkorn, T. (2014). Phenotypes determined by cluster analysis in severe or difficult-to-treat asthma. Journal of Allergy and Clinical Immunology, 133(6), 1549–1556.
Schaub, B., Bellou, A., Gibbons, F. K., Velasco, G., Campo, M., He, H., Liang, Y., Gillman, M. W., Gold, D., Weiss, S. T., Perkins, D. L., & Finn, P. W. (2004). TLR2 and TLR4 stimulation differentially induce cytokine secretion in human neonatal, adult, and

86
murine mononuclear cells. Journal of Interferon & Cytokine Research : The Official Journal of the International Society for Interferon and Cytokine Research, 24(9), 543–552.
Schroder, K., & Tschopp, J. (2010). The inflammasomes. Cell, 140(6), 821–832. Schwartz, D. A. (2001). Does Inhalation of Endotoxin Cause Asthma? American Journal of
Respiratory and Critical Care Medicine, 163(2), 305–306. Shafiee, S., & Topal, E. (2009). When will fossil fuel reserves be diminished? Energy Policy,
37(1), 181–189. Sheffield, M., Mabry, S., Thibeault, D. W., & Truog, W. E. (2006). Pulmonary nitric oxide
synthases and nitrotyrosine: findings during lung development and in chronic lung disease of prematurity. Pediatrics, 118(3), 1056–1064.
Shirai, T., Inui, N., Suda, T., & Chida, K. (2006). Correlation between peripheral blood T-cell profiles and airway inflammation in atopic asthma. The Journal of Allergy and Clinical Immunology, 118(3), 622–626.
Simpson, A., Tan, V. Y. F., Winn, J., Svensén, M., Bishop, C. M., Heckerman, D. E., Buchan, I., & Custovic, A. (2010). Beyond Atopy. American Journal of Respiratory and Critical Care Medicine, 181(11), 1200–1206.
Singh, K., Axelrod, S., & Bielory, L. (2010). The epidemiology of ocular and nasal allergy in the United States, 1988-1994. The Journal of Allergy and Clinical Immunology, 126(4), 778-783.e6.
Siroux, V., Boudier, A., Nadif, R., Lupinek, C., Valenta, R., & Bousquet, J. (2019). Association between asthma, rhinitis, and conjunctivitis multimorbidities with molecular IgE sensitization in adults. Allergy, 74(4), 824–827.
Smith, P. M., Howitt, M. R., Panikov, N., Michaud, M., Gallini, C. A., Bohlooly-Y, M., Glickman, J. N., & Garrett, W. S. (2013). The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science (New York, N.Y.), 341(6145), 569–573.
Soumelis, V., Reche, P. A., Kanzler, H., Yuan, W., Edward, G., Homey, B., Gilliet, M., Ho, S., Antonenko, S., Lauerma, A., Smith, K., Gorman, D., Zurawski, S., Abrams, J., Menon, S., McClanahan, T., Waal-Malefyt, R. de, Bazan, F., Kastelein, R. A., & Liu, Y.-J. (2002). Human epithelial cells trigger dendritic cell–mediated allergic inflammation by producing TSLP. Nature Immunology, 3(7), 673–680.
Spergel, J. M. (2010). Epidemiology of Atopic Dermatitis and Atopic March in Children. Immunology and Allergy Clinics of North America, 30(3), 269–280.
Spergel, J. M., & Paller, A. S. (2003). Atopic dermatitis and the atopic march. The Journal of Allergy and Clinical Immunology, 112(6 Suppl), S118-27.
Spits, H., Artis, D., Colonna, M., Diefenbach, A., Di Santo, J. P., Eberl, G., Koyasu, S., Locksley, R. M., McKenzie, A. N. J., Mebius, R. E., Powrie, F., & Vivier, E. (2013). Innate lymphoid cells--a proposal for uniform nomenclature. Nature Reviews. Immunology, 13(2), 145–149.
Stahl, J. L., & Barney, N. P. (2004). Ocular allergic disease. Current Opinion in Allergy and Clinical Immunology, 4(5), 455–459.
Storm van’s Gravesande, K., Wechsler, M. M. E., Grasemann, H., Silverman, E. E. S., Le, L., Palmer, L. J. L., & Drazen, J. J. M. (2003). Association of a missense mutation in the NOS3 gene with exhaled nitric oxide levels. American Journal of Respiratory and Critical Care Medicine, 168(2), 228–231.
Strachan, D. P. (1989). Hay fever, hygiene, and household size. BMJ (Clinical Research Ed.), 299(6710), 1259–1260.

87
Sugita, J., Asada, Y., Ishida, W., Iwamoto, S., Sudo, K., Suto, H., Matsunaga, T., Fukuda, K., Fukushima, A., Yokoi, N., Ohno, T., Azuma, M., Ebihara, N., Saito, H., Kubo, M., Nakae, S., & Matsuda, A. (2017). Contributions of Interleukin-33 and TSLP in a papain-soaked contact lens-induced mouse conjunctival inflammation model. Immunity, Inflammation and Disease, 5(4), 515–525.
Takeda, K., Kaisho, T., & Akira, S. (2003). Toll-like receptors. Annual Review of Immunology, 21, 335–376.
Tan, H.-T. T., Sugita, K., & Akdis, C. A. (2016). Novel Biologicals for the Treatment of Allergic Diseases and Asthma. Current Allergy and Asthma Reports, 16(10), 70.
Tanno, L. K., Calderon, M. A., Smith, H. E., Sanchez-Borges, M., Sheikh, A., Demoly, P., & Joint Allergy Academies, on behalf of J. A. (2016). Dissemination of definitions and concepts of allergic and hypersensitivity conditions. The World Allergy Organization Journal, 9, 24.
Tanus-Santos, J. E., Desai, M., Deak, L. R., Pezzullo, J. C., Abernethy, D. R., Flockhart, D. A., & Freedman, J. E. (2002). Effects of endothelial nitric oxide synthase gene polymorphisms on platelet function, nitric oxide release, and interactions with estradiol. Pharmacogenetics, 12(5), 407–413.
Taylor-Robinson, A. W., Phillips, R. S., Severn, A., Moncada, S., & Liew, F. Y. (1993). The role of TH1 and TH2 cells in a rodent malaria infection. Science (New York, N.Y.), 260(5116), 1931–1934.
Tepper, R. I., Levinson, D. A., Stanger, B. Z., Campos-Torres, J., Abbas, A. K., & Leder, P. (1990). IL-4 induces allergic-like inflammatory disease and alters T cell development in transgenic mice. Cell, 62(3), 457–467.
Thomsen, S. F., Ulrik, C. S., Kyvik, K. O., Hjelmborg, J. v. B., Skadhauge, L. R., Steffensen, I., & Backer, V. (2007). Importance of genetic factors in the etiology of atopic dermatitis: A twin study. Allergy and Asthma Proceedings, 28(5), 535–539.
Thomsen, S. F., Ulrik, C. S., Kyvik, K. O., Hjelmborg, J. von B., Skadhauge, L. R., Steffensen, I., & Backer, V. (2006). Genetic and environmental contributions to hay fever among young adult twins. Respiratory Medicine, 100(12), 2177–2182.
Thomsen, S. F., van der Sluis, S., Kyvik, K. O., & Backer, V. (2012). A study of asthma severity in adult twins. The Clinical Respiratory Journal, 6(4), 228–237.
Toppila-Salmi, S., Huhtala, H., Karjalainen, J., Renkonen, R., Mäkelä, M. J., Wang, D. Y., & Pekkanen, J. (2015). Sensitization pattern affects the asthma risk in Finnish adult population. Allergy, 70(9), 1112–1120.
Toppila-Salmi, S., Chanoine, S., Karjalainen, J., Pekkanen, J., Bousquet, J., & Siroux, V. (2019). Risk of adult-onset asthma increases with the number of allergic multimorbidities and decreases with age. Allergy, 74(12), 2406–2416.
Townshend, J., Hails, S., & McKean, M. (2007). Diagnosis of asthma in children. BMJ (Clinical Research Ed.), 335(7612), 198–202.
Tripathi, P., Awasthi, S., Prasad, R., Husain, N., & Ganesh, S. (2011). Association of ADAM33 gene polymorphisms with adult-onset asthma and its severity in an Indian adult population. In J. Genet (Vol. 90).
Tulić, M. K., Wale, J. L., Holt, P. G., & Sly, P. D. (2000). Modification of the inflammatory response to allergen challenge after exposure to bacterial lipopolysaccharide. American Journal of Respiratory Cell and Molecular Biology, 22(5), 604–612.
Turner, S. (2017). Gene-Environment Interactions-What Can These Tell Us about the Relationship between Asthma and Allergy? Frontiers in Pediatrics, 5, 118.

88
Uchio, E., Ono, S. Y., Ikezawa, Z., Ohno, S., Uchio, Ono, Ikezawa, & Ohno. (2000). Tear levels of interferon-gamma, interleukin (IL) -2, IL-4 and IL-5 in patients with vernal keratoconjunctivitis, atopic keratoconjunctivitis and allergic conjunctivitis. Clinical & Experimental Allergy, 30(1), 103–109.
Urban, J. F., Noben-Trauth, N., Donaldson, D. D., Madden, K. B., Morris, S. C., Collins, M., & Finkelman, F. D. (1998). IL-13, IL-4Ralpha, and Stat6 are required for the expulsion of the gastrointestinal nematode parasite Nippostrongylus brasiliensis. Immunity, 8(2), 255–264.
Van Eerdewegh, P., Little, R. D., Dupuis, J., Del Mastro, R. G., Falls, K., Simon, J., Torrey, D., Pandit, S., McKenny, J., Braunschweiger, K., Walsh, A., Liu, Z., Hayward, B., Folz, C., Manning, S. P., Bawa, A., Saracino, L., Thackston, M., Benchekroun, Y., Capparell, N., Wang, M., Adair, R., Feng, Y., Dubois, J., FitzGerald, M. G., Huang, H., Gibson, R., Allen, K. M., Pedan, A., Danzig, M. R., Umland, S. P., Egan, R. W., Cuss, F. M., Rorke, S., Clough, J. B., Holloway, J. W., Holgate, S. T., & Keith, T. P. (2002). Association of the ADAM33 gene with asthma and bronchial hyperresponsiveness. Nature, 418(6896), 426–430.
Velden, P. A. v. d., & Reitsma, P. H. (1993). Amino acid dimorphism in IL1A is detectable by PCR amplification. Human Molecular Genetics, 2(10), 1753–1753.
Vercelli, D. (2008). Discovering susceptibility genes for asthma and allergy. Nature Reviews Immunology, 8(3), 169–182.
Verhagen, J., Blaser, K., & Akdis, M. (2006). Mechanisms of Allergen-Specific Immunotherapy: T-Regulatory Cells and More. Immunology and Allergy Clinics of North America, 26(2), 207–231.
Virchow, J. C., Kay, S., Demoly, P., Mullol, J., Canonica, W., & Higgins, V. (2011). Impact of ocular symptoms on quality of life (QoL), work productivity and resource utilisation in allergic rhinitis patients--an observational, cross sectional study in four countries in Europe. Journal of Medical Economics, 14(3), 305–314.
Vivier, E., Artis, D., Colonna, M., Diefenbach, A., Di Santo, J. P., Eberl, G., Koyasu, S., Locksley, R. M., McKenzie, A. N. J., Mebius, R. E., Powrie, F., & Spits, H. (2018). Innate Lymphoid Cells: 10 Years On. Cell, 174(5), 1054–1066.
Vladich, F. D., Brazille, S. M., Stern, D., Peck, M. L., Ghittoni, R., & Vercelli, D. (2005). IL-13 R130Q, a common variant associated with allergy and asthma, enhances effector mechanisms essential for human allergic inflammation. The Journal of Clinical Investigation, 115(3), 747–754.
Vonk, J. M., Postma, D. S., Maarsingh, H., Bruinenberg, M., Koppelman, G. H., & Meurs, H. (2010). Arginase 1 and arginase 2 variations associate with asthma, asthma severity and β2 agonist and steroid response. Pharmacogenetics and Genomics, 20(3), 179–186.
Wade, L., Bielory, L., & Rudner, S. (2012). Ophthalmic antihistamines and H1-H4 receptors. Current Opinion in Allergy and Clinical Immunology, 12(5), 510–516.
Wallace, D. V, Dykewicz, M. S., Bernstein, D. I., Blessing-Moore, J., Cox, L., Khan, D. A., Lang, D. M., Nicklas, R. A., Oppenheimer, J., Portnoy, J. M., Randolph, C. C., Schuller, D., Spector, S. L., Tilles, S. A., Joint Task Force on Practice, American Academy of Allergy, Asthma & Immunology, American College of Allergy, Asthma and Immunology, & Joint Council of Allergy, Asthma and Immunology. (2008). The diagnosis and management of rhinitis: an updated practice parameter. The Journal of Allergy and Clinical Immunology, 122(2 Suppl), S1-84.

89
Walley, A. J., & Cookson, W. O. (1996). Investigation of an interleukin-4 promoter polymorphism for associations with asthma and atopy. Journal of Medical Genetics, 33(8), 689–692.
Ward, J. P. T., Ward, J., Leach, R. M., & Ward, J. P. T. (2010). The Respiratory System at a Glance. Wiley.
Warren, K. J., Sweeter, J. M., Pavlik, J. A., Nelson, A. J., Devasure, J. M., Dickinson, J. D., Sisson, J. H., Wyatt, T. A., & Poole, J. A. (2017). Sex differences in activation of lung-related type 2 innate lymphoid cells in experimental asthma. Annals of Allergy, Asthma & Immunology : Official Publication of the American College of Allergy, Asthma, & Immunology, 118(2), 233–234.
Webb, D. C., McKenzie, A. N., Koskinen, A. M., Yang, M., Mattes, J., & Foster, P. S. (2000). Integrated signals between IL-13, IL-4, and IL-5 regulate airways hyperreactivity. Journal of Immunology (Baltimore, Md. : 1950), 165(1), 108–113.
Weidinger, S., Klopp, N., Wagenpfeil, S., Rummler, L., Schedel, M., Kabesch, M., Schafer, T., Darsow, U., Jakob, T., Behrendt, H., Wichmann, H., Ring, J., & Illig, T. (2004). Association of a STAT 6 haplotype with elevated serum IgE levels in a population based cohort of white adults. Journal of Medical Genetics, 41(9), 658.
Welter, D., MacArthur, J., Morales, J., Burdett, T., Hall, P., Junkins, H., Klemm, A., Flicek, P., Manolio, T., Hindorff, L., & Parkinson, H. (2014). The NHGRI GWAS Catalog, a curated resource of SNP-trait associations. Nucleic Acids Research, 42(Database issue), D1001-6.
Wenzel, S. E. (2006). Asthma: defining of the persistent adult phenotypes. Lancet (London, England), 368(9537), 804–813.
Wenzel, S. E. (2012). Asthma phenotypes: the evolution from clinical to molecular approaches. Nature Medicine, 18(5), 716–725.
Wenzel, S. E., Balzar, S., Ampleford, E., Hawkins, G. A., Busse, W. W., Calhoun, W. J., Castro, M., Chung, K. F., Erzurum, S., Gaston, B., Israel, E., Teague, W. G., Curran-Everett, D., Meyers, D. A., & Bleecker, E. R. (2007). IL4Rα Mutations Are Associated with Asthma Exacerbations and Mast Cell/IgE Expression. American Journal of Respiratory and Critical Care Medicine, 175(6), 570.
Wenzel, S. E., Schwartz, L. B., Langmack, E. L., Halliday, J. L., Trudeau, J. B., Gibbs, R. L., & Chu, H. W. (1999). Evidence that severe asthma can be divided pathologically into two inflammatory subtypes with distinct physiologic and clinical characteristics. American Journal of Respiratory and Critical Care Medicine, 160(3), 1001–1008.
Werner, M., Topp, R., Wimmer, K., Richter, K., Bischof, W., Wjst, M., & Heinrich, J. (2003). TLR4 gene variants modify endotoxin effects on asthma. The Journal of Allergy and Clinical Immunology, 112(2), 323–330.
Wills-Karp, M. (2004). Interleukin-13 in asthma pathogenesis. Immunological Reviews, 202, 175–190.
Wills-Karp, M., Luyimbazi, J., Xu, X., Schofield, B., Neben, T. Y., Karp, C. L., & Donaldson, D. D. (1998). Interleukin-13: Central Mediator of Allergic Asthma. Science, 282(5397), 2258–2261.
Wills-Karp, M., Santeliz, J., & Karp, C. L. (2001). The germless theory of allergic disease: revisiting the hygiene hypothesis. Nature Reviews. Immunology, 1(1), 69–75.
Wjst, M., Fischer, G., Immervoll, T., Jung, M., Saar, K., Rueschendorf, F., Reis, A., Ulbrecht, M., Gomolka, M., Weiss, E. H., Jaeger, L., Nickel, R., Richter, K., Kjellman, N.-I. M., Griese, M., von Berg, A., Gappa, M., Riedel, F., Boehle, M., van Koningsbruggen, S.,

90
Schoberth, P., Szczepanski, R., Dorsch, W., Silbermann, M., Loesgen, S., Scholz, M., Bickeböller, H., & Wichmann, H.-E. (1999). A Genome-wide Search for Linkage to Asthma. Genomics, 58(1), 1–8.
Wu, D., Molofsky, A. B., Liang, H.-E., Ricardo-Gonzalez, R. R., Jouihan, H. A., Bando, J. K., Chawla, A., & Locksley, R. M. (2011). Eosinophils sustain adipose alternatively activated macrophages associated with glucose homeostasis. Science (New York, N.Y.), 332(6026), 243–247.
Wu, W., Bang, S., Bleecker, E. R., Castro, M., Denlinger, L., Erzurum, S. C., Fahy, J. V, Fitzpatrick, A. M., Gaston, B. M., Hastie, A. T., Israel, E., Jarjour, N. N., Levy, B. D., Mauger, D. T., Meyers, D. A., Moore, W. C., Peters, M., Phillips, B. R., Phipatanakul, W., Sorkness, R. L., & Wenzel, S. E. (2019). Multiview Cluster Analysis Identifies Variable Corticosteroid Response Phenotypes in Severe Asthma. American Journal of Respiratory and Critical Care Medicine, 199(11), 1358–1367.
Wu, X., Li, Y., Chen, Q., Chen, F., Cai, P., Wang, L., & Hu, L. (2010). Association and Gene-Gene Interactions of Eight Common Single-Nucleotide Polymorphisms with Pediatric Asthma in Middle China. Journal of Asthma, 47(3), 238–244.
Wynn, T. A. (2004). Fibrotic disease and the T(H)1/T(H)2 paradigm. Nature Reviews. Immunology, 4(8), 583–594.
Wynn, T. A., Chawla, A., & Pollard, J. W. (2013). Macrophage biology in development, homeostasis and disease. Nature, 496(7446), 445–455.
Yamana, Y., Fukuda, K., Ko, R., & Uchio, E. (2019). Local allergic conjunctivitis: a phenotype of allergic conjunctivitis. International Ophthalmology, 39(11), 2539–2544.
Yanamandra, K., Boggs, P., Thurmon, T., Lewis, D., Bocchini, J., & Dhanireddy, R. (2005). Novel Allele of the Endothelial Nitric Oxide Synthase Gene Polymorphism in Caucasian Asthmatics. Biochemical and Biophysical Research Communications, 335(2).
Yang, I. A., Holgate, S. T., & Holloway, J. W. (2004). Toll-like receptor polymorphisms and allergic disease: interpreting the evidence from genetic studies. Clinical & Experimental Allergy, 34(2), 163–166.
Yang, I., Barton, S., Rorke, S., Cakebread, J. A., Keith, T. P., Clough, J. B., Holgate, S. T., & Holloway, J. W. (2004). Toll-like receptor 4 polymorphism and severity of atopy in asthmatics. Genes & Immunity, 5(1), 41–45.
Yokouchi, Y., Nukaga, Y., Shibasaki, M., Noguchi, E., Kimura, K., Ito, S., Nishihara, M., Yamakawa-Kobayashi, K., Takeda, K., Imoto, N., Ichikawa, K., Matsui, A., Hamaguchi, H., & Arinami, T. (2000). Significant Evidence for Linkage of Mite-Sensitive Childhood Asthma to Chromosome 5q31–q33 near the Interleukin 12 B Locus by a Genome-wide Search in Japanese Families. Genomics, 66(2), 152–160.
Yokouchi, Y., Shibasaki, M., Noguchi, E., Nakayama, J., Ohtsuki, T., Kamioka, M., Yamakawa-Kobayashi, K., Ito, S., Takeda, K., Ichikawa, K., Nukaga, Y., Matsui, A., Hamaguchi, H., & Arinami, T. (2002). A genome-wide linkage analysis of orchard grass-sensitive childhood seasonal allergic rhinitis in Japanese families. Genes & Immunity, 3(1), 9–13.
Yoon, Y., Song, J., Hong, S. H., & Kim, J. Q. (2001). Plasma Nitric Oxide Concentrations and Nitric Oxide Synthase Gene Ploymorphisms in Coronary Artery Disease. Clinical Chemistry, 47(1), 151–151.
Yoshikawa, T., Kanazawa, H., Fujimoto, S., & Hirata, K. (2014). Epistatic effects of multiple receptor genes on pathophysiology of asthma – its limits and potential for clinical

91
application. Medical Science Monitor : International Medical Journal of Experimental and Clinical Research, 20, 64.
Zein, J. G., & Erzurum, S. C. (2015). Asthma is Different in Women. Current Allergy and Asthma Reports, 15(6), 28.
Zhang, J., Paré, P. D., & Sandford, A. J. (2008). Recent advances in asthma genetics. Respiratory Research, 9(1), 4.
Zhang, J., Zhou, G. H., Wei, T. T., & Chang, Z. S. (2016). Association between the interleukin 4 gene -590C/T promoter polymorphism and asthma in Xinjiang Uighur children. Genetics and Molecular Research : GMR, 15(3).
Zhang, Q., Qian, F. H., Zhou, L. F., Wei, G. Z., Jin, G. F., Bai, J. L., & Yin, K. S. (2011). Polymorphisms in Toll-Like Receptor 4 Gene Are Associated With Asthma Severity but not Susceptibility in a Chinese Han Population. In J Investig Allergol Clin Immunol (Vol. 21, Issue 5).
Zhang, Y., Leaves, N. I., Anderson, G. G., Ponting, C. P., Broxholme, J., Holt, R., Edser, P., Bhattacharyya, S., Dunham, A., Adcock, I. M., Pulleyn, L., Barnes, P. J., Harper, J. I., Abecasis, G., Cardon, L., White, M., Burton, J., Matthews, L., Mott, R., Ross, M., Cox, R., Moffatt, M. F., & Cookson, W. O. C. M. (2003). Positional cloning of a quantitative trait locus on chromosome 13q14 that influences immunoglobulin E levels and asthma. Nature Genetics, 34(2), 181–186.
Zhao, J., Shang, H., Cao, X., Huang, Y., Fang, X., Zhang, S., Xie, M., Xie, J., & Liu, X. (2017). Association of polymorphisms in TLR2 and TLR4 with asthma risk: An update meta-analysis. Medicine, 96(35), e7909.
Zhu, Z., Homer, R. J., Wang, Z., Chen, Q., Geba, G. P., Wang, J., Zhang, Y., & Elias, J. A. (1999). Pulmonary expression of interleukin-13 causes inflammation, mucus hypersecretion, subepithelial fibrosis, physiologic abnormalities, and eotaxin production. The Journal of Clinical Investigation, 103(6), 779–788.
Zicari, A. M., Occasi, F., Di Fraia, M., Mainiero, F., Porzia, A., Galandrini, R., Giuffrida, A., Bosco, D., Bertin, S., & Duse, M. (2016). Local allergic rhinitis in children: Novel diagnostic features and potential biomarkers. American Journal of Rhinology & Allergy, 30(5), 329–334.
Zimmerman, B., Feanny, S., Reisman, J., Hak, H., Rashed, N., McLaughlin, F. J., & Levison, H. (1988). Allergy in asthma. I. The dose relationship of allergy to severity of childhood asthma. The Journal of Allergy and Clinical Immunology, 81(1), 63–70.

92

93
PUBLICATIONS

94
Mec
hani
sms
of a
llerg
y
445
Rapid publication
Epistatic effect of IL1A and IL4RA geneson the risk of atopy
Kati Ådjers, MSc,a Tanja Pessi, PhD,a Jussi Karjalainen, MD, PhD,b
Heini Huhtala, MSc,c and Mikko Hurme, MD, PhDa,d Tampere, Finland
Background: Several studies have demonstrated a linkage orassociation of the atopic phenotype with T-cell cytokine genesinvolved in the regulation of the TH1/TH2 balance (eg, IL4,IL13, and their common receptor, IL4RA). We have recentlyshown that polymorphism of the pro-inflammatory cytokineIL1A gene is strongly associated with atopy.Objective: We now examined whether the polymorphisms ofIL1A (G/T at +4845) and IL4RA (T/C at +22446) would showan epistatic effect on the risk of atopy.Methods: Skin prick tests and gene polymorphism analyseswere performed in a population-based sample of asthmaticand nonasthmatic subjects.Results: Our results showed that in the nonasthmatic groupthe previously described elevated risk of atopy in noncarriersof allele T of IL1A (ie, having the genotype GG) was restrictedto individuals who were also noncarriers of allele C of IL4RA(genotype TT). This finding applies to the general populationof Finland, where 3.3% of adults are asthmatic.Conclusion: These data suggest that the IL1A and IL4RAgenes show an epistatic effect on the risk of atopy. (J AllergyClin Immunol 2004;113:445-7.)
Key words: IL1A, IL4RA, atopy, skin prick test, epistatic effectAtopic disorders underlying bronchial asthma,
eczema, and rhinoconjunctivitis are determined by genet-ic and environmental factors.1,2 Atopy is characterized bythe presence of specific IgE antibodies to common aller-gens and elevated total IgE concentrations. The skinprick test (SPT) is used to examine IgE-mediated allergicresponses, and the results are generally in line withanamnestic data on atopy.3
IL-1, a major pro-inflammatory cytokine, is found in 2forms, IL-1α and IL-1β. These molecules are synthesizedby a variety of cell types and play an important role in theinitiation of the immune response. IL-1α is found largely in
the cytosol and on the plasma membrane of cells4; it medi-ates much of the inflammatory reaction in the skin.5 IL-1βhas been shown to play the key role during contact sensiti-zation.6 IL-1α and IL-1β are coded for by different genes,which are located in the longer arm of chromosome 2.7
Both in vivo and in vitro findings have indicated thatpolymorphisms of these genes have an influence on thestrength of the inflammation. Several polymorphismshave been shown to be associated with severity of or sus-ceptibility to many inflammatory diseases.8 A single G/Tbase exchange at +4845 in exon 5 of the IL1A generesults in an amino acid substitution of alanine for ser-ine.9 This single nucleotide polymorphism (SNP) and ahaplotype of the IL1A, IL1B, and IL1RN genes contain-ing the same SNP as IL1A have recently been shown tobe associated with atopy in nonasthmatic adults. Thesestudies suggest that allele G predisposes to atopy.10,11
IL-4, a major anti-inflammatory cytokine produced byactivated T cells, mast cells, and basophils, plays a cen-tral role in the regulation of B-cell– and T-cell–mediatedimmune responses.12 The IL-4 receptor (IL-4R) itself isan essential component of the IL-4 pathway, because IL-4 exerts its biological effects through binding to the IL-4receptor complex. In the IL4RA gene, located in theshorter arm of chromosome 16, a number of SNPs havebeen reported.13-19 Among others, the T/C base exchangeat +22446 (known as cys406arg) in exon 9 of the IL4RAgene (resulting in an amino acid substitution of cysteinefor arginine) has been associated with atopy. In somestudies, the common allele T—ie, coding for cysteine—was found to predispose subjects to atopy.17,20
Because atopy has been mainly considered to be aTH2-related disease, the focus of the research has beenon TH2 cytokines. Linkage or association of the atopicphenotype with T-cell cytokine genes (IL4, IL13, IL4RA),which are involved in the regulation of the TH1/TH2 bal-ance, has been demonstrated in many studies.17,20 It isprobable that IL-1α also affects the TH1/TH2 balancebecause of its function in the initiation of the immuneresponse—specifically, promoting TH1 differentiation.21
Thus far, the results of allelic associations have only part-ly explained the predisposition to atopy and in somecases have even been contradictory. In the case of a mul-
From athe Department of Microbiology and Immunology, Medical School,University of Tampere; bthe Department of Respiratory Medicine, Tam-pere University Hospital; cthe School of Public Health, University of Tam-pere; and dthe Laboratory Centre, Tampere University Hospital.
This research was supported by the Finnish Anti-tuberculosis AssociationFoundation, the Finnish Allergy Research Foundation, the Research Fundof Tampere University Hospital, and the Rehabilitation Fund of the FinnishSocial Insurance Institution.
Received for publication August 18, 2003; revised December 30, 2003;accepted for publication December 31, 2003.
Reprint requests: Kati Ådjers, MSc, University of Tampere, Department ofMicrobiology and Immunology, Medical School, 33014 University ofTampere, Finland.
0091-6749/$30.00© 2004 American Academy of Allergy, Asthma and Immunologydoi:10.1016/j.jaci.2003.12.582
Abbreviations usedSNP: Single nucleotide polymorphismSPT: Skin prick test

95
446 Ådjers et al J ALLERGY CLIN IMMUNOLMARCH 2004
tifactorial disease, the predisposition might be betterexplained by a combination of alleles than by just a sin-gle allele. Therefore, we now examined whether the IL1Aand IL4RA polymorphisms show an epistatic effect onthe risk of atopy. The results of SPTs were analyzed in apopulation-based sample of adult asthmatic and nonasth-matic subjects, and the possible epistatic effect of theIL1A and IL4RA loci was determined in these groups.
METHODSA total of 245 asthmatic and 405 nonasthmatic subjects (age:
mean, 60 years; range, 31-89 years) participated in the study. Theparticipants were the subjects of a Finnish population-based case-control study conducted to investigate the risk factors and predictorsof the outcome of adult asthma. Approval for the study was obtainedfrom the ethics committee of Tampere University Hospital.Informed consent was obtained from all subjects.
The characteristics of the study group are shown in Table I. Moredetailed information on the subjects has been reported elsewhere.10
IL1A and IL4RA polymorphism testing and allergy testingthrough use of SPTs were carried out in 99.1% of the asthmatic sub-jects (150 females, 93 males) and 98.0% of the nonasthmatic sub-jects (247 females, 150 males).
The G/T polymorphism at +4845 of the IL1A gene was analyzedthrough use of the modified method of van den Velden and Reitsma.9The PCR primers used were 5ʹ-ATG GTT TTA GAA ATC ATC AAGCCT AGG GCA-3ʹ and 5ʹ-AAT GAA AGG AGG GGA GGA TGACAG AAA TGT-3ʹ. The PCR amplification was carried out under thefollowing cycling conditions: 95°C for 1 minute, then 35 cycles at94°C for 1 minute, at 56°C for 1 minute, at 72°C for 2 minutes, and at72°C for a final 5-minute extension. The PCR product was digestedwith the restriction enzyme SatI because of the introduction of a muta-tion (T/G) in the flanking primer. The digestion yielded 124 base pairs(bp) plus 76 bp plus 29 bp (allele G) and 153 bp plus 76 bp (allele T).
For the T/C polymorphism at +22446 of the IL4RA gene, PCRwas performed through use of the standard conditions and primers5ʹ-CAG CAT GGT GCC CAG TGG AG-3ʹ and 5ʹ-CTT GGG AACTCA TCC CAG GGC-3ʹ. The PCR amplification conditions wereas follows: 94°C for 2 minutes, then 33 cycles at 94°C for 1 minute,at 57°C for 1 minute, at 72°C for 1 minute, and at 72°C for a final10-minute extension. The digestion of the PCR product with Tsp45Iyielded 344 bp (allele T) and 271 bp plus 63 bp (allele C).
Atopy was determined through use of SPTs performed bytrained nurses with a panel of 22 allergen extracts selected to coverexposures in both urban and rural environments (ALK-Abelló, Hør-sholm, Denmark). More detailed information on the allergenextracts has been reported elsewhere.10 If at least 1 allergen showed
a wheal with a diameter at least 3 mm greater than that of the neg-ative control, the subject was considered SPT-positive.
The statistical method selected is indicated in the Results sec-tion. When allele distributions were compared in the case of a sin-gle gene, we used the χ2 test of Statistica (version Windows 5.1.D;StatSoft Inc, Tulsa, Okla) for calculating the P value. In the case of2 genes, the Fisher exact test of SPSS (version 11.1; SPSS Inc,Chicago, Ill) was used. Findings were considered significant in thecase of any P value less than or equal to .05. CIA software (version1.1; Martin J. Gardner & British Medical Journal) was used for car-rying out the calculations of odds ratios.
RESULTSFor the asthmatic subjects, the genotype frequencies
were 0.44 for GG, 0.47 for GT, and 0.08 for TT at +4845of the IL1A gene; at +22446 of the IL4RA gene, the geno-type frequencies were 0.85 for TT, 0.14 for TC, and0.004 for CC. For the nonasthmatic subjects, the geno-type frequencies were 0.47 for GG, 0.42 for GT, and 0.12for TT at +4845 of the IL1A gene; at +22446 of theIL4RA gene, the genotype frequencies were 0.80 for TT,0.18 for TC, and 0.01 for CC. The genotype frequenciesof both genes were not significantly different in the asth-matic and nonasthmatic groups.
The subjects were grouped according to their carrierstatus for IL1A allele T and IL4RA allele C. The carriers ofIL1A allele T had the genotype GT or TT. Accordingly, thecarriers of IL4RA allele C had the genotype TC or CC. Theallele distribution followed the Hardy-Weinberg equilibri-um. The percent of SPT+ responses was 56.8% in the asth-matic group and 37.8% in the nonasthmatic group.
In the nonasthmatic group, there was no significantassociation between IL4RA allele carrier status and SPTresult, as shown in Table II. As published earlier, dataobtained showed that the distribution of IL1A allele car-riers was different between the subjects with SPT+
responses and the subjects with SPT– responses (P =.001; χ2 test).10,11 This difference in the distribution wascaused by an increase in the frequency of the carriers ofallele T in the subjects with SPT- responses.
As shown in Table II in the case of the noncarriers ofallele C of the IL4RA gene, IL1A allele carrier distributiondiffered significantly between the subjects with SPT+
responses and the subjects with SPT– responses in thenonasthmatic group (P < .001; Fisher exact test). The com-bination of noncarriers of allele C of IL4RA and noncarri-ers of allele T of IL1A was more likely to be present inSPT+ subjects than in SPT– subjects (odds ratio, 2.32; 95%CI, 1.47-3.67). However, no significant association of IL1Aand SPT results was found in the case of allele C of theIL4RA gene. In the asthmatic group, no association ofIL1A, IL4RA, and SPT results was found (data not shown).
DISCUSSIONWe assessed SPT findings in asthmatic and nonasthmat-
ic subjects and evaluated whether the IL1A and IL4RA geno-type combinations affect the outcome of the SPTs. For thenonasthmatic group, our results demonstrated an epistaticeffect (ie, the interaction between 2 genes controls a singlephenotype): the combination of the noncarriers of allele C
Mechanism
s of allergy
TABLE I. Characteristics of the study groups
Subjects
Asthmatic NonasthmaticVariable (n = 245) (n = 405)
Age: mean ± SD (y) 59 ± 11 60 ± 11Sex: n (female/male) 152/93 254/151Smoking: n (non/ex/current) 123/80/42 237/89/79Atopy*: n 137 154Allergic symptoms
Rhinitis† 134 111Eye symptoms† 104 92Skin symptoms‡ 84 97
*One or more positive reactions in skin prick tests.†P < .001 and ‡P < .004 for difference between groups, as calculated withthe χ2 test.

96
Mec
hani
sms
of a
llerg
y
J ALLERGY CLIN IMMUNOLVOLUME 113, NUMBER 3
Ådjers et al 447
(ie, genotype TT) of IL4RA and the noncarriers of allele T(genotype GG) of IL1A had an interactive effect on the riskof atopy. Previously, noncarriers of allele T of IL1A werefound to show SPT+ results more often than carriers of thisallele.10 Noncarriers of allele C of IL4RA have also previ-ously been linked to SPT+ results and high IgE levels.17,20
Our data thus suggest that these alleles strengthen the effectsof each other and that certain allele combinations are need-ed for protection from or predisposition to atopy.
Our nonasthmatic subjects can be considered to repre-sent the general population reasonably well. A diagnosisof asthma or chronic obstructive pulmonary disease wasthe only exclusion criterion. In the Finnish adult popula-tion the prevalence of asthma, according the criteriaused, is 3.3%22; accordingly, the effect of the absence ofasthmatic patients is of minor significance in the popula-tion. Therefore, the data suggesting that the IL1A andIL4RA genes show an epistatic effect on the risk of atopymight be applied to the general population.
The epistatic effect described here might also be infor-mative regarding the basic mechanisms in atopy: the IL1A+4845 GG genotype is probably associated with a lowcapacity to produce IL-1α, and a weak inflammatoryresponse is known to favor the differentiation of the TH2cells.23 Thus it could be hypothesized that in individualswith the IL1A +4845 GG genotype the IL-4 levels are ele-vated; consequently, if the high IL-4–responding IL4RA Tallele is simultaneously present, the TH2 differentiation iseven more marked.
We thank Ms Sinikka Repo-Koskinen and Ms Eija Spåre forexpert technical assistance, and we thank Markku M. Nieminen,MD, PhD, Docent Timo Klaukka, MD, PhD, and Arpo Aromaa,MD, PhD, for their part in collecting the research material.
REFERENCES
1. Cookson W. The alliance of genes and environment in asthma and aller-gy. Nature 1999;402(6760 Suppl):5-11.
2. Rosenwasser LJ. Genetics of asthma and atopy. Toxicol Lett 1996;86:73-7.3. Burrows B, Martinez FD, Halonen M, Barbee RA, Cline MG. Associa-
tion of asthma with serum IgE levels and skin-test reactivity to allergens.N Engl J Med 1989;320:271-7.
4. Dinarello CA. Biologic basis for interleukin-1 in disease. Blood1996;87;2095-147.
5. La E, Fischer SM. Transcriptional regulation of intracellular IL-1 recep-tor antagonist gene by IL-1 alpha in primary mouse keratinocytes. JImmunol 2001;166:6149-55.
6. Kermani F, Flint MS, Hotchkiss SA. Induction and localization of cuta-
neous interleukin1 beta mRNA during contact sensitization. Toxicol ApplPharmacol 2000;169:231-7.
7. Cox A, Camp NJ, Nicklin MJ, di Giovine FS, Duff GW. An analysis of link-age disequilibrium in the interleukin-1 gene cluster, using a novel groupingmethod for multiallelic markers. Am J Hum Genet 1998;62:1180-8.
8. Bidwell J, Keen L, Gallagher G, Kimberly R, Huizinga T, McDermottMF, et al. Cytokine gene polymorphism in human disease: on-line data-bases. Genes Immun 1999;1:3-19.
9. van den Velden PA, Reitsma PH. Amino acid dimorphism in IL1A isdetectable by PCR amplification. Hum Mol Genet 1993;2:1753
10. Karjalainen J, Hulkkonen J, Pessi T, Huhtala H, Nieminen MM, AromaaA, et al. The IL1A genotype associates with atopy in non-asthmaticadults. J Allergy Clin Immunol 2002;110:429-34.
11. Pessi T, Karjalainen J, Hulkkonen J, Nieminen MM, Hurme M.A com-mon IL-1 complex haplotype is associated with an increased risk ofatopy.J Med Genet 2003;40:E66.
12. Paul WE, Seder RA. Lymphocyte responses and cytokines. Cell1994;76:241-51.
13. Deichmann K, Bardutzky J, Forster J, Heinzmann A, Kuehr J. Commonpolymorphisms in the coding part of the IL4-receptor gene. BiochemBiophys Res Commun 1997;231:696-7.
14. Hershey GK, Friedrich MF, Esswein LA, Thomas ML, Chatila TA. Theassociation of atopy with a gain-of-function mutation in the alpha subunitof the interleukin-4 receptor. N Engl J Med 1997;337:1720-5.
15. Mitsuyasu H, Izuhara K, Mao XQ, Gao PS, Arinobu Y, Enomoto T, et al.Ile50Val variant of IL4R alpha upregulates IgE synthesis and associateswith atopic asthma. Nat Genet 1998;19:119-20.
16. Kruse S, Japha T, Tedner M, Sparholt SH, Forster J, Kuehr J, et al. Thepolymorphisms S503P and Q576R in the interleukin-4 receptor alphagene are associated with atopy and influence the signal transduction.Immunology 1999;96:365-71.
17. Ober C, Leavitt SA, Tsalenko A, Howard TD, Hoki DM, Daniel R, et al.Variation in the interleukin 4-receptor alpha gene confers susceptibility toasthma and atopy in ethnically diverse populations. Am J Hum Genet2000;66:517-26.
18. Hackstein H, Hecker M, Kruse S, Bohnert A, Ober C, Deichmann KA, etal. A novel polymorphism in the 5ʹ promoter region of the human inter-leukin-4 receptor alpha-chain gene is associated with decreased solubleinterleukin-4 receptor protein levels. Immunogenetics 2001;53:264-9.
19. Lozano F, Places L, Vila JM, Padilla O, Arman M, Gimferrer I, et al.Identification of a novel single-nucleotide polymorphism (Val554Ile) anddefinition of eight common alleles for human IL4RA exon 11. TissueAntigens 2001;57:216-20.
20. Howard TD, Koppelman GH, Xu J, Zheng SL, Postma DS, Meyers DA,et al. Gene-gene interaction in asthma: IL4RA and IL13 in a Dutch pop-ulation with asthma. Am J Hum Genet 2002;70:230-6.
21. Von Stebut E, Ehrchen JM, Belkaid Y, Kostka SL, Molle K, Knop J, et al.Interleukin 1alpha promotes Th1 differentiation and inhibits disease pro-gression in Leishmania major-susceptible BALB/c mice. J Exp Med2003;198:191-9.
22. The national sickness insurance and reimbursement of medicine expens-es. Finnish Statistics on Medicines 1997. Helsinki: National Agency forMedicines and Kela; 1998.
23. Perussia B, Loza MJ. Linear ‘2-0-1’ lymphocyte development: hypothe-ses on cellular bases for immunity. Trends Immunol 2003;24:235-41.
TABLE II. Genotype distributions of IL4RA (single nucleotide polymorphism +22446), IL1A (single nucleotide polymor-phism +4845), and combinations of the IL4RA and IL1A genotypes in nonasthmatic subjects with positive and nega-tive skin prick test responses
Genotype combination SPT+ N (%) SPT– N (%) OR for comparison 95% CI P value*
IL4RA TT 125 (83.3) 195 (78.9) 1.33 0.79-2.26 .284IL4RA TC/CC 25 (16.7) 52 (21.1) 1 — —IL1A 4845 GG 85 (56.7) 99 (40.1) 1.95 1.30-2.95 .001IL1A 4845 GT/TT 65 (43.3) 148 (59.9) 1 — —IL4RA TT * IL1A 4845 GG 72 (57.6) 72 (36.9) 2.32 1.47-3.67 <.001IL4RA TT * IL1A 4845 GT/TT 53 (42.4) 123 (63.1) 1 — —IL4RA TC/CC * IL1A 4845 GG 13 (52.0) 27 (51.9) 1.00 0.39-2.61 1.000IL4RA TC/CC * IL1A 4845 12 (48.0) 25 (48.1) 1 — —
SPT+, Positive skin prick test result; SPT–, negative skin prick test result; OR, odds ratio.*Calculated through use of χ2 test for IL4RA and IL1A genotypes and through use of Fisher exact test for combinations of IL4RA and IL1A genotypes.

PUBLICATION II
Epistatic effect of TLR4 and IL4 genes on the risk of asthma in females
Ådjers, K., Karjalainen, J., Pessi, T., Eklund, C., & Hurme, M.
International archives of allergy and immunology, 138(3), 251–256. https://doi.org/10.1159/000088726


103
discharged home with transdermal fentanyl, oral fentanylfor breakthrough pain, acetaminophen, and hydroxyzine.The patient was already in possession of self-injectableepinephrine because of her latex allergy, and she wasfamiliar with its use in the event that she developeddyspnea secondary to the fentanyl after discharge. Thepatient reported only pruritis and intermittent, mild urti-caria with the use of the transdermal fentanyl patch inassociation with scheduled hydroxyzine. In addition, shedid not require the use of the oral fentanyl because herpain was adequately controlled with the transdermalformulation.Three months after discharge, the patient was readmit-
ted to the hospital for another shunt revision. Becausedoses of fentanyl necessary for pain control were notpreviously well tolerated, it was decided to attempt theadministration of hydromorphone based on the patient’sreport that this medication provided excellent pain controlin the past. The patient was premedicated with diphenhy-dramine and hydroxyzine, and escalating doses of hy-dromorphone were administered (Table II). The patienttolerated as much as 1 mg with the development of gener-alized pruritis but no urticaria or dyspnea. She was startedon a continuous hydromorphone infusion at 0.2 mg/h andwas maintained at this dose and taken to the operatingroom 8 hours later. The operation was once again suc-cessfully completed, but the patient was inadvertentlyadministered a bolus dose of 1 mg hydromorphone inthe postanesthesia care unit in addition to the continuousinfusion. This led to severe dyspnea requiring the adminis-tration of epinephrine intramuscularly. No further bolusdoses were administered after this event, and the patient’spain was well controlled by increasing the infusion rate by0.05 mg/h as needed, to a maximum of 0.35 mg/h, plus theaddition of acetaminophen. After achieving adequate paincontrol, the drip rate was decreased by 0.05 mg/h every8 hours to a minimum dose of 0.05 mg/h. Attempting towean at a faster rate or discontinuing the drip at a higherdose of hydromorphone led to loss of pain control.The patient has since been readmitted for repeat neu-
rosurgical procedures, and after premedication with di-phenhydramine and hydroxyzine, she has been placedimmediately on a continuous infusion of hydromorphoneat 0.2 mg/h with rate increases and decreases as notedabove. She is able to maintain good pain control with thisregimen and does not develop significant adverse events.To our knowledge, this is the first report of the use of
continuous opioid infusions to provide analgesia in anopioid-intolerant patient. This report demonstrates thatpatients who fail to respond to traditional measures for theprevention of pseudoallergic reactions secondary to opi-oid medications and who have an absolute need for thisclass of medication may tolerate continuous opioid infu-sions with slow dose escalations. Continuous infusionsmay be superior to bolus doses of opioids, such as inpatient-controlled analgesia, because histamine releasefrom mast cells secondary to opioids is dose-dependent,and the total dose of opioid administered and peak serumconcentrations attained are less with continuous infusions
than with bolus doses.5,6 In the case of hydromorphone,serum hydromorphone concentrations of at least 4 ng/mL are required for adequate analgesia.8 To achieve thisgoal, dosing guidelines recommend hydromorphone infu-sion rates of up to 0.2 mg/h with the addition of bolusdoses as needed.9 Because bolus doses of opioids maylead to pseudoallergic reactions in opioid-intolerant pa-tients, higher infusion rates than those routinely recom-mended may be required to achieve adequate pain control.
Haig Tcheurekdjian, MDa,b
Katherine Gundling, MDa
From the Division of Allergy and Immunology, Departments of aMedicine
and bPediatrics, University of California, San Francisco.
Disclosure of potential conflict of interest: The authors have declared that they
have no conflict of interest.
REFERENCES
1. Veien M, Szlam F, Holden J, Yamaguchi K, Denson DD, Levy JH. Mech-
anisms of nonimmunological histamine and tryptase release from human
cutaneous mast cells. Anesthesiology 2000;92:1074-81.
2. Joint Council of Allergy Asthma and Immunology. Practice parameters for
drug hypersensitivity. Ann Allergy Asthma Immunol 1999;83:S665-700.
3. Grammer LC, Greenberger PA. Individual drugs or problems: summary of
useful techniques. Allergy Asthma Proc 2005;26:66-72.
4. Nasser SMS, Ewan PW. Opiate-sensitivity: clinical characteristics and the
role of skin prick testing. Clin Exp Allergy 2001;31:1014-20.
5. Ebertz JM, Hermens JM, McMillan JC, Uno H, Hirshman C, Hanifin JM.
Functional differences between human cutaneous mast cells and basophils:
a comparison of morphine-induced histamine release. Agents Actions 1986;
18:455-62.
6. Hermens JM, Ebertz JM, Hanifin JM, Hirshman CA. Comparison of his-
tamine release in human skin mast cells induced by morphine, fentanyl,
and oxymorphone. Anesthesiology 1985;62:124-9.
7. White PF. Use of continuous infusion versus intermittent bolus adminis-
tration of fentanyl or ketamine during outpatient anesthesia. Anesthesiol-
ogy 1983;59:294-300.
8. Reidenberg MM, Goodman H, Erle H, Gray G, Lorenzo B, Leipzig RM,
et al. Hydromorphone levels and pain control in patients with severe
chronic pain. Clin Pharmacol Ther 1988;44:376-82.
9. Thompson Micromedex Healthcare Series DRUGDEX Evaluation [data-
base on internet]. Greenwood Village (CO): Thomson Healthcare, Inc;
1974-2006. Available at: http://www.thomsonhc.com/home/dispatch.
Accessed February 20, 2006.
Available online May 10, 2006.
doi:10.1016/j.jaci.2006.03.026
The interaction of IL1A and endothelial nitricoxide synthase polymorphisms is associatedwith the degree of atopy
To the Editor:There is increasing evidence that nitric oxide (NO)
may play an important role in allergic inflammation.Endothelial NO synthase (eNOS) is one of the enzymescatalyzing NO synthesis. It is induced in a variety of celltypes by proinflammatory cytokines, such as IL-1, TNF-a,IFN-g, and by microbial products such as LPSs.1 Previousstudies on the role of the eNOS gene in the pathogenesis ofatopy have produced conflicting results.2,3
IL-1a is a proinflammatory cytokine that mediates theinflammatory reaction in the skin.4 IL1a has also beenfound to accelerate cutaneous inflammation.5 We have
J ALLERGY CLIN IMMUNOL
JULY 2006284 Letters to the Editor
Lette
rsto
theEd
itor

104
earlier shown that IL1A (G/T base change at 14845) pol-ymorphism is associated with atopy; the risk for atopy washigher in subjects having genotype GG of IL1A gene.6
We have expanded the study by analyzing eNOS (T/Gbase change at1894) polymorphism from the same cohortand investigated whether these genes show an epistaticeffect on the degree of atopy.
Altogether 254 female and 151 male (mean age, 60years; age range, 31-89 years) participated in the study.The subjects were controls without asthma of a Finnishpopulation-based case-control study intended to investi-gate the risk factors of adult asthma. Detailed informationabout the whole material has been presented earlier in theJournal.6 IL1A (14845G>T, rs17561) polymorphism wasdetected as previously described.6 The eNOS (1894T>G,rs1799983) polymorphismwas analyzed by allele-specifichybridization method (TaqMan; Applied Biosystems,FosterCity, Calif). Thenucleotide sequences of the primersand probes used in the PCR were deduced from publishedsequences deposited in the GenBank database and chosenand synthesized in conjunction with Applied Biosystems(Foster City, Calif). The genotype distributions followedHardy-Weinberg equilibrium. Sensitization to allergenswas determined by skin prick test (SPT) performed as pre-viously described.6 The degree of atopy was defined as thenumber of positive SPTs. Thus, the SPT-positive patientswere divided into those with 1 or 2 positive SPTs(SPT1[1]) and 3 or more positive SPTs (SPT1[2]).
As seen in Table I, IL1A genotype GG increased therisk for sensitization to allergen; the number of patientsin SPT1(2) group was especially increased (odds ratio[OR], 2.09; 95% CI, 1.23-3.57; P 5 .006, x2 test; df 51). eNOS polymorphism did not have an independent
effect on sensitization to allergen but interacted withIL1A gene. The interaction of these genes was calculatedby using multinomial logistic regression analysis. Themodel showed that there is a slight interaction betweenthese genes on the degree of sensitization (P 5 .08;Table II). There was a significant interaction betweenthe SPT-negative and SPT1(2) groups (P 5 .026), butnot between the SPT-negative and SPT1(1) groups (P5 .785, bilogistic regression analysis; Table II). If theage and sex were included in the model, the results didnot change (data not shown).
Earlier studies have shown that exhaled NO levels inadults correlate with atopy (with a number of positiveSPTs and total IgE) rather than bronchial hyperreactivityand lung function.7,8 Here the eNOS gene did not have anindependent role in the pathogenesis of atopy. Its effectwas dependent on IL1A gene. In addition, eNOS poly-morphism itself or together with IL1A polymorphism didnot have an effect on asthma susceptibility (Pessi et al,Unpublished data, November 2005). It seems that theeffect of eNOS gene on atopy is dependent on another pro-inflammatory gene, like IL1A. This interaction betweeneNOS and IL1A genes may also explain some earlier con-flicting results2,3 on the effect of eNOS polymorphisms onatopy.
We cannot exclude the possibility that the effect of theeNOS gene is on the diagnostic phase—that is, the highproducer allele T of eNOS gene9 makes the SPTmore sen-sitive by inducing stronger endothelial enlargement on thesite of allergen application. However, we did not observeany effect of the eNOS genotype on the response inducedby the histamine control (data not shown), thus speakingagainst this alternative.
TABLE I. Independent effect of IL1A (single nucleotide polymorphism 14845) and eNOS (single nucleotide
polymorphism 1894) on sensitization on allergen: the degree of atopy*
SPT2 SPT1(1) SPT1(2) SPT2 vs SPT1(1) SPT2 vs SPT1(2)
N % N % N % P P
IL1A GG 99 40.1 43 55.1 42 58.3 .02 .006IL1A GT/ TT 148 59.9 35 44.9 30 41.7
eNOS TT/ TG 112 45.3 41 52.6 31 43.1 .226 .73
eNOS GG 135 54.7 37 47.4 41 56.9
*P value calculated in 2 3 2 table by x2 test.
TABLE II. Epistatic effect of IL1A (single nucleotide polymorphism 14845) and eNOS (single nucleotide
polymorphism 1894) on sensitization on allergen: the degree of atopy
Interaction analyses
SPT2 SPT1(1) SPT1(2) All groups SPT2 vs SPT1(1) SPT2 vs SPT1(2)
N % N % N % P* Py Py
eNOS TT/TG&IL1A GG 44 39.3 23 56.1 23 74.2 .08 .785 .026eNOS TT/TG&IL1A GT/TT 68 60.7 18 43.9 8 25.8
eNOS GG&IL1A GG 55 40.7 20 54.1 19 46.3
eNOS GG&IL1A GT/TT 80 59.3 17 45.9 22 53.7
*Multinomial logistic regression analysis.
!Bilogistic regression analysis.
J ALLERGY CLIN IMMUNOL
VOLUME 118, NUMBER 1Letters to the Editor 285
Letters
toth
eEd
itor

105
In our study, we show for the first time that IL1A andeNOS genes have an interactive effect on the degree ofatopy (ie, the epistatic effect of 2 genes). Both genes areinvolved in the initiation of the immune response andprobably affect the TH1/TH2 balance.1 At the inductivephase of TH1 cells, NO has shown an enhancing effecton the induction and differentiation of TH1 cells, whereasit has little or no effect on fully committed T cells. On theother hand, NO at noncytotoxic concentrations has beendemonstrated to downregulate the TH1-type cytokinesand/or increase the TH2-associated molecules.1 The highNO synthesis is linked to atopy7 and to the genotypes ofTT and GT of eNOS gene.9 Previously, we showed thatsubjects having genotype GG of IL1A had a significantlyincreased risk for SPT positivity.6 Probably the allele Gis associated with low capacity to produce IL-1a, a weakinflammatory response induced is known to favor the dif-ferentiation of the TH2 cells.10 Thus, it can be concludedthat if a subject has 2 atopy risk genes, such as a highNO-producing allele of eNOS gene together with IL1Aatopy risk gene, TH2 responses like sensitization to aller-gens are even further increased.
Tanja Pessi, PhDa
Kati Adjers, MSca
Jussi Karjalainen, MD, PhDb
Riikka Rontu, PhDc
Mikko Hurme, MD, PhDa,c
From athe Department of Microbiology and Immunology and bthe Department
of Respiratory Medicine, Medical School, University of Tampere; and cthe
Center for Laboratory Medicine, Tampere University Hospital, Finland.
Supported by the Academy of Finland, the Tampere Tuberculosis Foundation,
the Medical Research Fund of Tampere University Hospital, and the Reha-
bilitation Fund of the Finnish Social Insurance Institution.
Disclosure of potential conflict of interest: The authors have declared that they
have no conflict of interest.
REFERENCES
1. Kolb H, Kolb-Bachofen V. Nitric oxide in autoimmune disease: cyto-
toxic or regulatory mediator? Immunol Today 1998;19:556-61.
2. Holla LI, Buckova D, Kuhrova V, Stejskalova A, Francova H, Znojil V,
et al. Prevalence of endothelial nitric oxide synthase gene polymor-
phisms in patients with atopic asthma. Clin Exp Allergy 2002;32:1193-8.
3. Yanamandra K, Boggs PB, Thurmon TF, Lewis D, Bocchini JA Jr,
Dhanireddy R. Novel allele of the endothelial nitric oxide synthase
gene polymorphism in Caucasian asthmatics. Biochem Biophys Res
Commun 2005;335:545-9.
4. La E, Fischer SM. Transcriptional regulation of intracellular IL-1 recep-
tor antagonist gene by IL-1 alpha in primary mouse keratinocytes.
J Immunol 2001;166:6149-55.
5. Konishi H, Tsutsui H, Murakami T, Yumikura-Futatsugi S, Yamanaka
K, Tanaka M, et al. IL-18 contributes to the spontaneous development
of atopic dermatitis-like inflammatory skin lesion independently of IgE/
stat6 under specific pathogen-free conditions. Proc Natl Acad Sci U S A
2002;99:11340-5.
6. Karjalainen J, Hulkkonen J, Pessi T, Huhtala H, Nieminen MM, Aromaa
A, et al. The IL1A genotype associates with atopy in nonasthmatic
adults. J Allergy Clin Immunol 2002;110:429-34.
7. Ali M, Khoo SK, Turner S, Stick S, Le Souef P, Franklin P. NOS1 pol-
ymorphism is associated with atopy but not exhaled nitric oxide levels in
healthy children. Pediatr Allergy Immunol 2003;14:261-5.
8. Ho LP, Wood FT, Robson A, Innes JA, Greening AP. Atopy influences
exhaled nitric oxide levels in adult asthmatics. Chest 2000;118:1327-31.
9. Yoon Y, Song J, Hong SH, Kim JQ. Plasma nitric oxide concentrations
and nitric oxide synthase gene polymorphisms in coronary artery disease.
Clin Chem 2000;46:1626-30.
10. Perussia B, Loza MJ. Linear ‘‘2-0-1’’ lymphocyte development: hypoth-
eses on cellular bases for immunity. Trends Immunol 2003;24:235-41.
Available online May 28, 2006.
doi:10.1016/j.jaci.2006.03.032
J ALLERGY CLIN IMMUNOL
JULY 2006286 Letters to the Editor
Lette
rsto
theEd
itor

PUBLICATION IV
Self-reported allergic rhinitis and/or allergic conjunctivitis associate with IL13 rs20541 polymorphism in Finnish adult asthma patients
Ådjers, K., Luukkainen A., Pekkanen, J., Hurme, M., Huhtala H., Renkonen R., Wang, D., Mäkelä, M., Karjalainen J., Toppila-Salmi, S.
International archives of allergy and immunology, 172(2), 123-128. https://doi.org/10.1159/000456009


112