Embed Size (px)
Citation preview
Lehigh Valley Health NetworkLVHN Scholarly Works
Department of Medicine
Disseminated Mycobacterium Tuberculosis withUlceronecrotic Cutaneous Disease Presenting asCellulitisKelly L. Reed DOLehigh Valley Health Network, [email protected]
Nektarios I. Lountzis MDLehigh Valley Health Network, [email protected]
Follow this and additional works at: http://scholarlyworks.lvhn.org/medicine
Part of the Dermatology Commons, and the Medical Sciences Commons
This Poster is brought to you for free and open access by LVHN Scholarly Works. It has been accepted for inclusion in LVHN Scholarly Works by anauthorized administrator. For more information, please contact [email protected].
Published In/Presented AtReed, K., Lountzis, N. (2015, April 24). Disseminated Mycobacterium Tuberculosis with Ulceronecrotic Cutaneous Disease Presenting asCellulitis. Poster presented at: Atlantic Dermatological Conference, Philadelphia, PA.
Lehigh Valley Health Network, Allentown, PennsylvaniaKelly L. Reed, DO and Nektarios Lountzis, MD
Case Presentation:
Disseminated Mycobacterium Tuberculosis with Ulceronecrotic Cutaneous Disease Presenting as Cellulitis
Discussion:Cutaneous tuberculosis (CTB) was first described in the literature in 1826 by Laennec and has since been reported to manifest in a variety of clinical presentations. The most common cause is infection with the acid-fast bacillus Mycobacterium tuberculosis via either primary exogenous inoculation (direct implantation of mycobacterium into the skin), secondary to endogenous spread (hematogenous or direct extension of mycobacterium to the skin from an internal source, typically lung), or as a cutaneous reaction known as a tuberculid (reactive eruption without the presence of mycobacterium in the skin). Occasionally M.bovis and the bacilli Calmette-Guérin (BCG) vaccine have been reported to cause cutaneous disease. Cutaneous tuberculosis accounts for <1-2% of all cases of TB and most often affects immunocompromised hosts due to HIV infection or medications, such as TNF-α inhibitors and corticosteroids.
Clinical presentation is extremely variable and is dependent upon the route of infection and the bacterial load in lesions. Exogenous inoculation often causes a tuberculous chancre or TB verrucosa cutis, while endogenous spread causes scrofuloderma, miliary TB or lupus vulgaris. Tuberculids are reactive conditions, which include papulonecrotic lesions, lichen scrofulosorum and erythema induratum. Tuberculous cellulitis, as our patient developed, is an uncommon presentation and does not fit neatly into the aforementioned categories.
Diagnosis of cutaneous TB is multifaceted and often includes a combination of the following modalities: PPD, interferon-γ release assay, tissue culture, PCR for mycobacterial DNA and tissue culture and/or biopsy with special staining techniques, such as Auramine-Rhodamine (highly sensitive fluorescent study), Ziehl-Neelsen or Wade-Fite stain. The histopathological findings vary depending on the type of infection, however CTB is characteristically described as a mixed inflammatory reaction of the dermis and subcutis comprised of neutrophils, multinucleate giant cells and epithelioid histiocytic granulomas, which may display some caseation necrosis.
Treatment of CTB is primarily antibiotic therapy, based upon the culture and sensitivities of the isolated strain of M. tuberculosis due to the rise in multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB).
This patient represents an interesting case of cutaneous tuberculosis from endogenous spread, presenting as a recalcitrant “cellulitis” that deteriorated to an uncommon ulceronecrotic form of the disease. Typically ulceronecrotic cases are due to tuberculid reactions, however in this case, the isolation of bacilli on tissue culture favors this to be an active cutaneous infection from hematogenous spread. There are fewer than ten reported cases of tuberculous cellulitis in the literature, seven of which reported systemic corticosteroid use, similar to our patient. Studies estimate approximately 20% of patients with CTB may have concomitant pulmonary TB as in our patient’s case. This case is relevant to dermatologists, because it increases awareness of cutaneous TB as the presenting symptom of disseminated tuberculosis infections in immunocompromised patients. It also serves as a reminder to maintain a high index of suspicion for such opportunistic infections, specifically in cases of resistant cellulitides and to complete a thorough patient work-up.
References:1 TaguchiR,NakanishiT,ImanishiH,etal.Acaseoftuberculouscellulitis.Clinical Medicine Insights: Case reports.2015;(8):11-12.2 DiasM,QuaresmaM,AzulayD,etal.Updateoncutaneoustuberculosis.An Bras Dermatol.2014;89(6):925-938.3 Daido-HoriuchiY,KikuchiY,KobayashiS,etal.Tuberculouscellulitisinapatientwithchronickidneydiseaseandpolymyalgia
rheumatica.Intern Med.2012;51:3203-3206.4 MahmudT,PaulHK,ZakariaASM,etal.Studyonassociationofcutaneoustuberculosiswithpulmonarytuberculosis.Bangladesh
Med Res Counc Bull. 2010;36:57-60.5 KobaS,OkawaT,MisagoN,etal.Acaseoftuberculouscellulitislackingepithelioidgranuloma.Acta Derm Venereol.
2013;93:596-597.
© 2015 Lehigh Valley Health Network
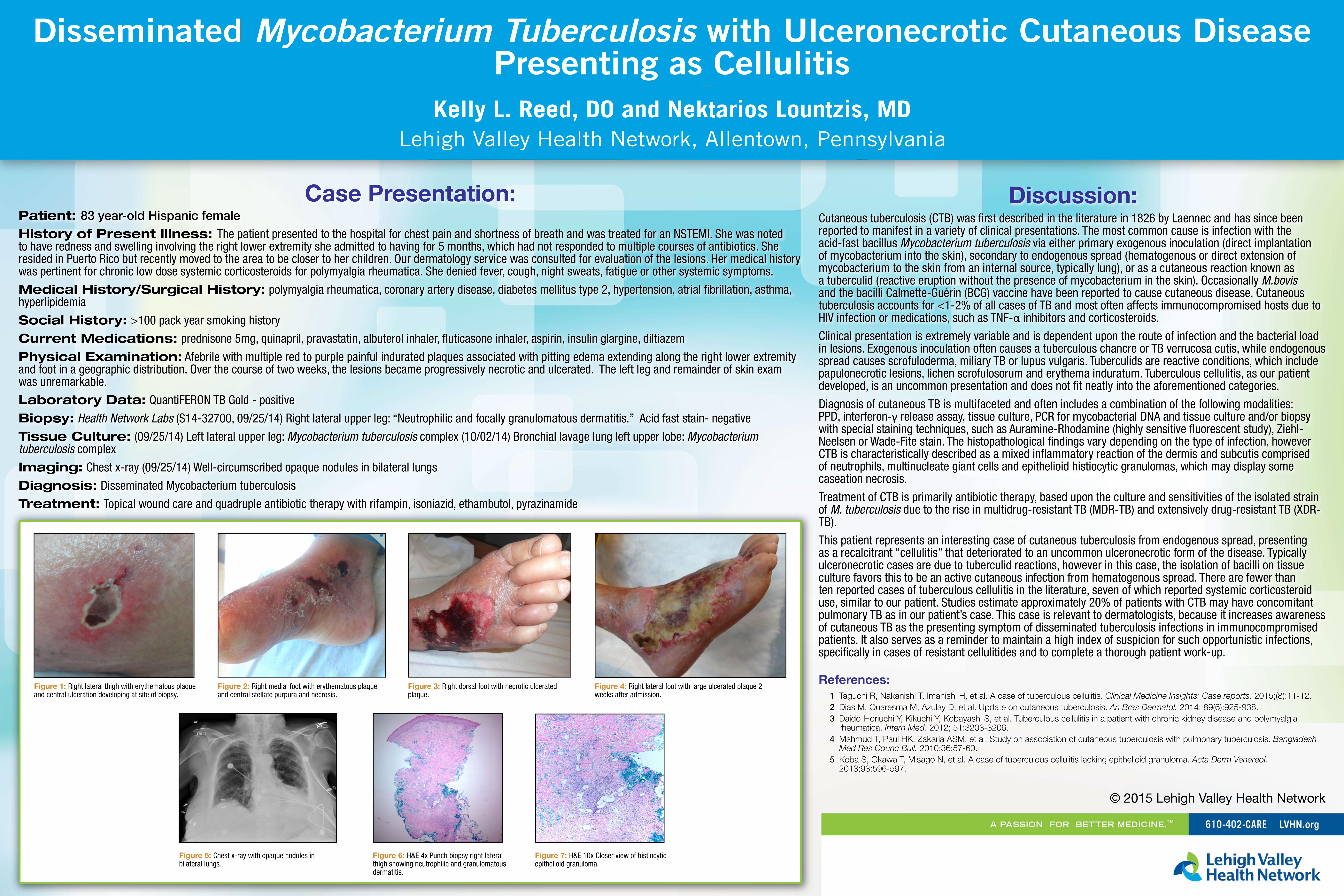
Patient: 83 year-old Hispanic female
History of Present Illness: The patient presented to the hospital for chest pain and shortness of breath and was treated for an NSTEMI. She was noted to have redness and swelling involving the right lower extremity she admitted to having for 5 months, which had not responded to multiple courses of antibiotics. She resided in Puerto Rico but recently moved to the area to be closer to her children. Our dermatology service was consulted for evaluation of the lesions. Her medical history was pertinent for chronic low dose systemic corticosteroids for polymyalgia rheumatica. She denied fever, cough, night sweats, fatigue or other systemic symptoms.
Medical History/Surgical History: polymyalgia rheumatica, coronary artery disease, diabetes mellitus type 2, hypertension, atrial fibrillation, asthma, hyperlipidemia
Social History: >100 pack year smoking history
Current Medications: prednisone 5mg, quinapril, pravastatin, albuterol inhaler, fluticasone inhaler, aspirin, insulin glargine, diltiazem
Physical Examination: Afebrile with multiple red to purple painful indurated plaques associated with pitting edema extending along the right lower extremity and foot in a geographic distribution. Over the course of two weeks, the lesions became progressively necrotic and ulcerated. The left leg and remainder of skin exam was unremarkable.
Laboratory Data: QuantiFERON TB Gold - positive
Biopsy: Health Network Labs (S14-32700, 09/25/14) Right lateral upper leg: “Neutrophilic and focally granulomatous dermatitis.” Acid fast stain- negative
Tissue Culture: (09/25/14) Left lateral upper leg: Mycobacterium tuberculosis complex (10/02/14) Bronchial lavage lung left upper lobe: Mycobacterium tuberculosis complex
Imaging: Chest x-ray (09/25/14) Well-circumscribed opaque nodules in bilateral lungs
Diagnosis: Disseminated Mycobacterium tuberculosis
Treatment: Topical wound care and quadruple antibiotic therapy with rifampin, isoniazid, ethambutol, pyrazinamide
Figure 3: Right dorsal foot with necrotic ulcerated plaque.
Figure 4: Right lateral foot with large ulcerated plaque 2 weeks after admission.
Figure 5: Chest x-ray with opaque nodules in bilateral lungs.
Figure 6: H&E 4x Punch biopsy right lateral thigh showing neutrophilic and granulomatous dermatitis.
Figure 1: Right lateral thigh with erythematous plaque and central ulceration developing at site of biopsy.
Figure 2: Right medial foot with erythematous plaque and central stellate purpura and necrosis.
Figure 7: H&E 10x Closer view of histiocytic epithelioid granuloma.

















![[Micro] mycobacterium tuberculosis](https://img.pdfslide.us/doc/110x75/55d6fc67bb61ebfa2a8b47ea/micro-mycobacterium-tuberculosis.jpg)









