-
8/9/2019 Disorders of Neural Tube Formation
1/32
DISORDERS OF NEURAL TUBE FORMATION
The neural tube usually fuses 18–26 days after ovulation.
Failure of closure maylead to anencephaly, encephalocele, spina
bifida or spina bifida occulta. Liveborn
anencephalic babies usually die in hours or days.
Epidemiology
Neural tube defects NT!s" are amon# the most common con#enital
abnormalitiesbut prevalence varies bet$een countries and races. The
prevalence of NT!s in%n#land and &ales fell from the 1'()s
on$ards to *ust under ).8+1))) total births by1''. -ome of the
decline $as due to antenatal dia#nosis but some is uneplained./n
the 0 anencephaly and spina bifida are of approimately eual
prevalence andto#ether ma3e up '45 of all NT!s.
Aetiology
ost NT!s result from a comple interaction bet$een several #enes
and poorlyunderstood environmental factors.
Genetic factor
NT!s occur in many syndromes and chromosome disorders. 7o$ever,
an NT! maybe the only anomaly in a member of a family in $hich case
the relatives have anincreased ris3 for all types of NT!.
En!ironmental factor
ericonceptual multiple vitamin supplements containin# folic acid
reduce theincidence of neural tube defects. /n %n#land it is
recommended that $omen plannin#pre#nancy ta3e )) 9# of folic acid
daily before conception and durin# the first 12$ee3s of the
pre#nancy. -ome dru#s ta3en durin# the pre#nancy may increase
theris3. These include sodium valproate and folic acid anta#onists
such as trimethoprim,triamterene, carbama:epine, phenytoin,
phenobarbitone, and primidone.
"renatal diagnoi
; Fetoprotein
-
8/9/2019 Disorders of Neural Tube Formation
2/32
Spinal dyrap#im
Spina $ifida cytica
This is a cystic lesion $hich in 8)–')5 is a myelomenin#ocele in
$hich the spinalcord is a component of the cyst $all. /t is
lumbosacral in about 8)5 of cases. Thereis usually a miture of
upper and lo$er motor neurone si#ns dependin# on the leveland there
is al$ays disturbance of bladder and bo$el function. -urvivin#
infantsreuire comple orthopaedic and urolo#ical support, includin#
sur#ery.
-
8/9/2019 Disorders of Neural Tube Formation
3/32
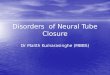
Syringomyelia
This is a tubular cavitation of the spinal cord $hich tends to
be in the cervical re#ion
but may involve the $hole cord. /t rarely becomes symptomatic in
children. -huntin#of the cavity is sometimes performed and
posterior fossa eploration may beunderta3en. /t is often associated
$ith the >hiari / malformation in $hich there isdo$n$ard
displacement of the lo$er cerebellum, includin# the tonsils fi#
1".
Fig%re &>hiari / malformation. -a#ittal T1 $ei#hted
ma#netic resonance ima#e sho$in# anenlar#ed cerebellar tonsil $hich
etends belo$ the level of the foramen ma#numarro$". The corpus
callosum is normal $ith the cin#ulate #yrus *ust above itcompare to
fi#ure 4". This 12 year old boy presented $ith headaches. The
>hiari /
malformation can be associated $ith hydrocephalus and
syrin#omyelia, $hich he didnot have.
DISORDERS OF REGIONALISATION
-
8/9/2019 Disorders of Neural Tube Formation
4/32
hypotelorism closely set eyes", a sin#le central incisor tooth
or the face may benormal.
DISORDERS OF 'ORTI'AL DE(ELO"MENT
Diorder of proliferation and differentiation
Microcep#aly
This is an abnormally small head circumference ? ).th centile on
occipito=frontalhead circumference charts", $hich is
disproportionately small in relation to the rest of the body.
The usual implication of this findin# is that brain #ro$th is not
normal.7o$ever, if a small head circumference is detected in the
neonatal period it isprudent to perform an ray of the s3ull to loo3
for evidence of early closure of all thecranial sutures total
craniosynostosis".
Genetic ca%e
There are familial cases $here the neurolo#ical problems are
relatively mild.7o$ever microcephaly is usually associated $ith
si#nificant abnormalities such aspyramidal tract si#ns and profound
learnin# difficulties. /t is part of more than 4)syndromes listed
in the @ford !ysmorpholo#y !atabase.
Non)genetic ca%e
These include ionisin# radiation in the first t$o trimesters of
pre#nancy, intrauterine
infections, dru#s and other chemicals, circulatory disturbance,
and perinatal hypoic=ischaemic events. &hen there is a
si#nificant perinatal insult to the brain the headcircumference may
be normal at birth $ith subseuent failure of #ro$th in the firstfe$
months of life. %ually in some types of #enetic microcephaly the
head si:e fallsoff as late as A2–A $ee3s of #estation or even after
birth, so prenatal dia#nosis byultrasound may be difficult.
Megalencep#aly
e#alencephaly is increased si:e of the brain itself. Lar#e heads
can run in normalfamilies but inherited me#alencephaly can be
associated $ith si#nificant learnin#
difficulties, neurolo#ical abnormalities, and sei:ures.
7emime#alencephaly isunilateral enlar#ement of one side of the
brain, sometimes the hemisphere only.
-
8/9/2019 Disorders of Neural Tube Formation
5/32
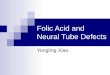
Agyria)pac#ygyria *liencep#aly+
There may be complete absence of #yri, in $hich case the terms
a#yria orlissencephaly Cree3D Esmooth brain" are used. achy#yria
describes a reducednumber of broadened and flat #yri $ith less
foldin# of the corte than normal. There
may be varyin# de#rees of a#yria+pachy#yria in the same brain
fi# 2".
Fig%re ,Type / lissencephaly. >oronal T1 $ei#hted ma#netic
resonance ima#e.
-
8/9/2019 Disorders of Neural Tube Formation
6/32
LIS1 #ene. utations in a second #ene on the H chromosome,
doublecortin DCX ",have also been sho$n to cause
lissencephaly.
Type II liencep#aly or -al.er)-ar$%rg yndrome
This is also called Ecobblestone lissencephaly and is a
different malformation fromtype / lissencephaly. The smooth corte
has a #ranular surface and is covered $ithmenin#es that are
thic3ened as a result of mesenchymal proliferation. The
clinicalfeatures include both nervous system and muscle
abnormalities. The infants are veryabnormal at birth. They have
abnormal eyes $ith retinal dysplasia, microphthalmia,and anomalies
of the anterior se#ment. There may be hydrocephalus or
sometimesmicrocephaly. 0sually there is necrosis of fibres in all
muscles, similar to that seen insevere muscular dystrophy, and
serum creatine 3inase is raised.
-
8/9/2019 Disorders of Neural Tube Formation
7/32
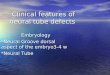
Fig%re 0Jilateral opercular polymicro#yria. >oronal T1
$ei#hted ma#netic resonance ima#e.These bilateral abnormalities
arro$s" are relatively subtle and $ere not identified ona computed
tomo#raphic eamination. /n the first year of life this boy
developed ri#htsided sei:ures and development $as delayed,
particularly in lan#ua#e. Later he had
poor ton#ue and pharyn#eal coordination and a ri#ht hemiple#ia.
!espite thelateralisation of some of his neurolo#ical si#ns, the
scan abnormalities $ere bilateral.
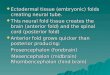
Diorder of cortical organiation
-ome patients have cortical microdys#enesisBmicroscopic
abnormalities of corticalarran#ement that have been described in
the brains of patients $ith epilepsy, autism,schi:ophrenia, and the
fetal alcohol syndrome. The etent to $hich these findin#seplain
abnormal brain function is an area of active research. @ther
patients haveareas of focal cortical dysplasia $hich are lar#e
enou#h to be seen on computedtomo#raphic or ma#netic resonance
ima#in# scans fi# ". These dysplasias are acause of early onset
sei:ures that may be focal or #eneralised. Iesection of
corticaldysplasias may improve sei:ure control.
-
8/9/2019 Disorders of Neural Tube Formation
8/32
Fig%re 1 >on#enital cortical malformation.
-
8/9/2019 Disorders of Neural Tube Formation
9/32
'OMBINED AND O(ERLA""ING 'EREBRAL MALFORMATIONS
There are distinct abnormalities that represent an overlap
bet$een different classes
of malformation. This is not surprisin#Bthe terato#enic periods
are so closelyspaced that overlaps are li3ely if there is an
environmental cause.
-
8/9/2019 Disorders of Neural Tube Formation
10/32
onset" sei:ures. allosal a#enesis is part of the fetal alcohol
syndrome and is seen inlactic acidosis and non=3etotic
hyper#lycinaemia.
&hen a#enesis of the corpus callosum is the only lesion
there may be no symptomsalthou#h tests of perception and lan#ua#e
may demonstrate disturbances ofinte#ration of hemispheric function.
7o$ever, some patients have mental retardation,sei:ures or cerebral
palsy.
renatal ultrasound allo$s dia#nosis from 2) $ee3s #estation.
&hen callosala#enesis is discovered on antenatal scan the
pro#nosis is difficult to assess because
the isolated lesion can be associated $ith normal development.
< decision toterminate the pre#nancy may depend on the
demonstration of associatedabnormalities.
"orencep#aly
The term porencephaly is often used for any cavity in a cerebral
hemisphere thatcommnunicates $ith a lateral hemisphere. 7o$ever, it
should probably be used onlyfor circumscribed hemispheric necrosis
that occurs in utero before the adult featuresof the hemisphere are
fully developed. The relatively early development of theselesions
is sho$n by their smooth $alls and by associated
developmentaldisturbances in the ad*oinin# corte such as
polymicro#yria or distortion of the #yralpattern. This is relevant
because unilateral or bilateral porencephalic cysts are foundin
children dia#nosed as havin# cerebral palsy and there is often
debate about thetimin# of the insult. Neuropatholo#ical tets debate
$hether or not there is adistinction bet$een porencephaly and
schi:encephaly, and some corticalabnormalities do not fit neatly
into any #roup fi# ".
Sc#i3encep#aly
This term is used by radiolo#ists to describe clefts $hich
traverse the full thic3ness of
the hemisphere, connectin# the ventricle to the subarachnoid
space. They aredescribed as type / or Efused=lip $hen the $alls of
the cleft are opposed, and type //or Eopen=lip $hen cerebrospinal
fluid separates the $alls. -ome of them are #eneticBfamilial cases
have been described and some sporadic cases are associated
$ithmutations in the homeobo #ene EMX2 . The clefts are
freuently bilateral and even$hen unilateral they are often combined
$ith cortical dysplasia of the oppositehemisphere.
%pilepsy is common and sometimes the only problem is isolated
partial sei:ures.There may be hemiple#ia, uadriple#ia, and learnin#
difficulties of variable de#ree. /f there is bilateral
involvement of both opercular re#ions there may be facial
apraia
and speech difficulties.
-
8/9/2019 Disorders of Neural Tube Formation
11/32
MALFORMATIONS OF "OSTERIOR FOSSA STRU'TURES
-
8/9/2019 Disorders of Neural Tube Formation
12/32
• /t is important to construct a three #eneration family tree,
if necessary $ith
eamination and investi#ation of close relatives for subtle
epression of adisorder, or evidence of carrier status.
• The aim is to establish a dia#nosis and #ive an accurate ris3.
/f it is not
possible to identify the precise aetiolo#y it is usually
possible to offer anempiric recurrence ris3 after eamination of the
parents.
"renatal diagnoi
• renatal dia#nosis and termination of affected pre#nancies is
only one of a
ran#e of reproductive options open to parents, but for many
couples it is theoption of choice.
• For the ma*ority of developmental disorders of the nervous
system, pre=
implantation #enetic dia#nosis is not yet feasible.
• For a condition follo$in# mendelian inheritance the option of
donor #ametes
could be discussed.
• For a condition $ith a stron# environmental component it is
imperative that
measures are ta3en to minimise the ris3 of eposure in a future
pre#nancy.For neural tube defects, periconceptual supplementation
$ith hi#h dose folatehas been sho$n to reduce the ris3 of
recurrence in future pre#nancies seeabove".
• &hen a specific dia#nosis has been made and a chromosomal
anomaly,
#enetic mutation or biochemical defect has been identified it is
usuallypossible to offer prenatal dia#nosis by chorion villus
samplin# at 11 $ee3s#estation in a future pre#nancy. /f this is not
the case, detailed ultrasoundscannin# may be helpful in some
instances.
•rovidin# accurate #enetic advice about developmental anomalies
of thenervous system is a challen#in# tas3. Referral for specialist
advice is stronglyrecommended .
Learning point
• Neural tube defects NT!s" are some of the most common
con#enital
abnormalities of the >N-, althou#h their prevalence in the 0
has fallen.Nevertheless it is still important to counsel $omen of
childbearin# a#e aboutthe need to ta3e dietary supplements
containin# folate before becomin#pre#nant
-
8/9/2019 Disorders of Neural Tube Formation
13/32
• There is an increased ris3 of NT!s in pre#nant $omen $ho are
ta3in# certain
dru#s
• %ven small midline abnormalities over the spinal cord should
be ta3en
seriously in case there is underlyin# spinal dysraphism
Learning point
• &hen assessin# children the head circumference should be
measured and
plotted on a centile chart. The current measurement should be
compared $ithprevious measurements to determine $hether or not
there has been apro#ressive chan#e $ith time
• -ome children $ith non=pro#ressive abnormalities of head si:e
are normal in
their development, but children $ith micro= or macrocephaly and
abnormal
development should probably have ma#netic resonance ima#in# of
the brain
Learning point
• The lissencephalies cause ma*or developmental problems and may
shorten
life
• /n type // lissencephaly the cerebral malformations may be
associated $ith
eye or muscle abnormalities so that a comprehensive assessment
isnecessary
• -ome of the less severe mi#rational and or#anisational
abnormalities may be
clinically silent. 7o$ever they may be associated $ith learnin#
difficulties orsei:ures. any $ill be discovered on ma#netic
resonance ima#in# of thebrain. 7o$ever some are microscopic, $hich
is relevant in the assessment ofsome patients $ith refractory
epilepsy
Learning point
• >ombined malformations may be found in infants $ith severe
developmental
and neurolo#ical problems
• 7o$ever, they may be present in patients $ith relatively minor
learnin#
difficulties or motor disability. atients $ith a#enesis of the
corpus callosummay have no neurolo#ical problems. /t is important
to be #uarded about thepro#nosis $hen such abnormalities are found
on scannin# in early life
4E5 REFEREN'ES
1. Aicardi J . Diseases of te nervo!s system in
cildood" 2nd ed. London#Mac $eit %ress" London"
1&&'.▸ This is a standard work, whichcontains an
excellent chapter on malformations of the nervous system.
-
8/9/2019 Disorders of Neural Tube Formation
14/32
2. Baraitser M . (1&&)*. +e genetics of
ne!rological disorders" ,rd ed. -xfordMonograps on Medical enetics.
,/. -xford# -xford 0niversity %ress" 1&&).▸ Another
standard reference book, which remains useful despite theevolution
of computerised neurogenetic databases.
A. Bar.o!itc# A6. %ediatric ne!roimaging , 2nd ed.
hiladelphiaD Lippincott=Iaven, 1''6.▸T#i compre#eni!e te7t$oo. #a a
%ef%l c#apter t#atincl%de can ill%trating t#e normal de!elopment of
t#e ner!o%ytem8 T#ere are alo c#apter on congenital a$normalitie of
t#e $rainand pine8
. Faer$er EN, ed. CS Magnetic resonance imaging in infants and
cildren.Clinics in Developmental Medicine o.1,/. LondonD ac eith
ress, 1''4.▸More %ef%l can of c#ildren 9it# de!elopmental
pro$lem8
4. Friede RL. Developmental ne!ropatology , 2nd revised and
epanded
edition. JerlinD -prin#er=erla#, 1'8'.▸T#i i a ne%ropat#ology
te7t$oo.dealing 9it# t#ee complicated de!elopmental a$normalitie8
It%pplement and %nderpin t#e more recent 9or.: 9#ic# i $aed moreon
imaging and genetic t%die t#an ne%ropat#ology8
6. leeson J " als C3. e!ronal migration disorders# from
genetic diseasesto developmental mecanisms. +rends in
e!roscience244452,#,627&.▸ Anexcellent recent review.
M>rossIef Medline M&eb of -cience
(. ovaert ! " de 8ries LS. 3n atlas of neonatal 9rain
sonograpy. Clinics inDevelopmental Medicine os. 1/171/2. London#
Mac $eit %ress" 1&&).▸"ltrasonography is now the means of
performing early and non# invasive examinations of the infant
brain so this is an importantreference work for those looking after
newborns.
httpD++*nnp.bm*.com+content+(+supplO1+iA.fullPsec=2
http://jnnp.bmj.com/external-ref?access_num=10.1016/S0166-2236(00)01607-6&link_type=DOIhttp://jnnp.bmj.com/external-ref?access_num=10.1016/S0166-2236(00)01607-6&link_type=DOIhttp://jnnp.bmj.com/external-ref?access_num=10906798&link_type=MEDhttp://jnnp.bmj.com/external-ref?access_num=10906798&link_type=MEDhttp://jnnp.bmj.com/external-ref?access_num=000088474900008&link_type=ISIhttp://jnnp.bmj.com/content/74/suppl_1/i3.full#sec-2http://jnnp.bmj.com/external-ref?access_num=10906798&link_type=MEDhttp://jnnp.bmj.com/external-ref?access_num=000088474900008&link_type=ISIhttp://jnnp.bmj.com/content/74/suppl_1/i3.full#sec-2http://jnnp.bmj.com/external-ref?access_num=10.1016/S0166-2236(00)01607-6&link_type=DOI
-
8/9/2019 Disorders of Neural Tube Formation
15/32
Birt# defect ) central ner!o% ytem
-ummary
Neural tube defects NT!s" include spina bifida, anencephaly and
encephalocele.
Folate deficiency and some epilepsy medications are ris3 factors
for these
conditions. Ta3in# folic acid before and durin# early pre#nancy
can si#nificantly
reduce the ris3 of neural tube defects. Tests in pre#nancy such
as ultrasound candia#nose these birth defects.
Jirth defects of the central nervous system are called neural
tube defects NT!s".
NT!s include conditions called spina bifida, anencephaly and
encephalocele. They
are all present at birth and are due to a problem $ith the
development of the brain
and+or spinal cord in the developin# baby fetus".
The brain and spinal cord of a #ro$in# fetus develop from a
simple structure called
the ne!ral t!9e. The neural tube Q:ips upR alon# its len#th to
close and protect thebrain and spinal cord. /f the neural tube
doesnRt close at any part alon# its len#th, the
-
8/9/2019 Disorders of Neural Tube Formation
16/32
baby $ill have a neural tube defect. The types of neural tube
defects spina bifida,
anencephaly and encephalocele" are due to the place alon# the
neural tube that
hasnRt closed, leavin# parts of the brain and+or spinal cord
eposed.
< ran#e of #enetic and environmental factors are
thou#ht to be responsible forNT!s, includin# the mother havin# not
enou#h of the vitamin folate and some
epilepsy medications. Ta3in# folate folic acid" before and
durin# early pre#nancy
can si#nificantly reduce the chance that a mother $ill have a
baby $ith this 3ind of
birth defect.
The central nervous system >N-"
The central nervous system consists of the brain and spinal
cord. Joth are $rapped
in a thin linin# called meninges and are surrounded by a
fluid called cere9rospinal
fl!id . The brain is attached to the spinal cord by the
brain stem, located at the baseof the brain. The spinal cord runs
the len#th of the bac3bone and is protected by the
bones vertebrae" of the spine. Nerves branch off from the spinal
cord into the parts
of the body.
!evelopment of the fetal >N-
The central nervous system of a #ro$in# fetus starts $ith a
simple structure called
the Qneural #rooveR that folds in to form the Qneural tubeR.
This then develops into the
spinal cord and brain. Jy day 28 after conception, the neural
tube should be closed
and fused. /f it doesnRt close, the result is a neural tube
defect./n many cases, these defects can be dia#nosed durin#
pre#nancy $ith ultrasound
scans and, rarely, $ith other tests such as amniocentesis
analysin# a sample of
amniotic fluid".
Iis3 factors and prevention of >N- birth defects
Neural tube defects are thou#ht to be caused by a ran#e of
#enetic and
environmental factors $or3in# in combination. -ome of these
factors includeD
• T#e mot#er #a a folate deficiency – if the mother is
lac3in# some nutrients,
especially the J=#roup vitamin called folate folic acid", the
chance of havin# ababy $ith a NT! is increased. /f folate is ta3en
$efore conception and atleast for the first four $ee3s of
pre#nancy, around seven out of 1) cases ofNT!s can be
prevented. Sou should tal3 to your doctor about ho$ much folateyou
should ta3e if you are thin3in# of becomin# pre#nant.
• Genetic – the eact #enetic association is unclear, but a
$oman is at
increased ris3 of havin# a baby $ith a neural tube defect if she
has a close
relative $ho has had a baby $ith the condition a family
history". < $oman
-
8/9/2019 Disorders of Neural Tube Formation
17/32
$ho has already #iven birth to a child $ith a neural tube defect
is also atincreased ris3 of havin# subseuent babies $ith a similar
condition.
• 7avin# a personal or family history of a NT! can influence the
amount of
folate needed to reduce the chance of havin# a baby $ith a
neural tube
defect. Sou should tal3 to your doctor about ho$ much folate you
should ta3eif you are thin3in# of becomin# pre#nant.
• /n some cases, ho$ever, there is evidence to su##est that some
forms of
neural tube defects are caused by specific #enetic chan#es
mutations" thatare not related to folate. /n these cases, the
neural tube defect is caused bythe baby inheritin# faulty #ene
copies from both parents. These faulty #enesprevent the baby from
ma3in# use of folate that is necessary to #ro$ anddevelop in
pre#nancy even if the folate is present in the ri#ht amount".
/nthese cases, ta3in# folate before and durin# pre#nancy $ill not
prevent thecondition.
• Medication – particular medications used to treat and
control epilepsy are
thou#ht to contribute to the ris3 of neural tube defect.
-pina bifida
/n a baby $ith spina bifida, the bones verte9rae" of the spine
fail to fuse. The spinal
cord and nerves protrude or Qpop outR" throu#h the #ap that has
been created due to
a failure of closure of the neural tube. This can affect the
nerves that spread from this
area into the abdomen and le#s. -pina bifida can occur any$here
alon# the len#th of
the spine, but more commonly appears in the lo$er bac3.
Nine out of 1) affected babies also have a build=up of
cerebrospinal fluid inside the
brain. This condition is called hydrocephalus and is sometimes
referred to as Q$ater
on the brainR. The incidence of spina bifida in ictoria is
around one in every 1,2A4
births.
-pina bifida can be mild, moderate or severe and is #raded
accordin# to the de#ree
of the defect intoD
• Occ%lta – the bones vertebrae" have not closed
completely, but the spinal
cord is unharmed. The characteristic soft lump may be missin#,
$hich is $hythis form of spina bifida is sometimes dia#nosed later
in life.
• Meningocele – the membrane menin#es" coverin# the spinal
cord protrudes
or bul#es out throu#h the #ap in the spine.
• Myelomeningocele – the menin#es, spinal cord and blood
vessels protrude
throu#h the #ap.
-pina bifida is incurable. The main form of treatment is sur#ery
to seal the #ap. /f the
baby has hydrocephalus, a shunt is inserted into the brain to
drain the ecess
cerebrospinal fluid.
-
8/9/2019 Disorders of Neural Tube Formation
18/32
-
8/9/2019 Disorders of Neural Tube Formation
19/32
entralOnervousOsystemVopenUWJirth defects = central nervous
system = Jetter 7ealth
>hannel?+aW?br+W
Neural tube defects NT!s" include spina bifida, anencephaly and
encephalocele.
Folate deficiency and some epilepsy medications are ris3 factors
for these
conditions. Ta3in# folic acid before and durin# early pre#nancy
can si#nificantly
reduce the ris3 of neural tube defects. Tests in pre#nancy such
as ultrasound can
dia#nose these birth defects.
httpD++$$$.betterhealth.vic.#ov.au+bhcv2+bhcarticles.nsf+pa#es+JirthOdefectsOcentral OnervousOsystem
HydrocephalusWater on the brain
Last reviewed: November 12, 2012.
Hydrocephalus is a buildup of fluid inside the skull that leads
to brain swellin.
Hydrocephalus means !water on the brain.!
Causes, incidence, and risk factors
Hydrocephalus is due to a problem with the flow of the fluid
that surrounds the brain. "his
fluid is called the cerebrospinal fluid, or #$%. &t
surrounds the brain and spinal cord, and
helps cushion the brain.
#$% normally moves throuh the brain and the spinal cord, and is
soaked into the
bloodstream. #$% levels in the brain can rise if:
• The ow of CSF is blocked
• It does not get absorbed into the blood properly
• Your brain makes too much of it
"oo much #$% puts pressure on the brain. "his pushes the brain
up aainst the skull and
damae brain tissue.
http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Birth_defects_central_nervous_systemhttp://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Birth_defects_central_nervous_systemhttp://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Birth_defects_central_nervous_systemhttp://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Birth_defects_central_nervous_system
-
8/9/2019 Disorders of Neural Tube Formation
20/32
Hydrocephalus may bein while the baby is rowin in the womb.
&t is common in babies
who have a myelomeninocele, a birth defect in which the spinal
column does not close
properly.
Hydrocephalus may also be due to:
• enetic defects
• Certain infections during pregnancy
&n youn children, hydrocephalus may be due to:
• Infections that a!ect the central ner"ous system #such as
meningitis orencephalitis$, especially in infants
•
%leeding in the brain during or soon after deli"ery #especially
in prematurebabies$
• In&ury before, during, or after childbirth, including
subarachnoidhemorrhage
• Tumors of the central ner"ous system, including the
brain or spinal cord
• In&ury or trauma
Hydrocephalus most often occurs in children. 'nother type,
called normal pressure
hydrocephalus, may occur in adults and the elderly.
Symptoms
$ymptoms of hydrocephalus depend on:
• 'ge
• 'mount of brain damage
• What is causing the buildup of CSF uid
&n infants with hydrocephalus, it causes the fontanelle
(soft spot) to bule and the head to be
larer than e*pected. +arly symptoms may also include:
• (yes that appear to ga)e downward
• Irritability
• Sei)ures
•
Separated sutures
http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001558/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A000752/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A000752/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A000752/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001558/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A000752/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A000752/
-
8/9/2019 Disorders of Neural Tube Formation
21/32
• Sleepiness
• *omiting
$ymptoms that may occur in older children can include:
• %rief, shrill, high+pitched cry
• Changes in personality, memory, or the ability to reason or
think
• Changes in facial appearance and eye spacing
• Crossed eyes or uncontrolled eye mo"ements
• i-culty feeding
• (.cessi"e sleepiness
• /eadache
• Irritability, poor temper control
• 0oss of bladder control #urinary incontinence$
• 0oss of coordination and trouble walking
• 1uscle spasticity #spasm$
• Slow growth #child 2 + 3 years$
• Slow or restricted mo"ement
• *omiting
Signs and tests
"he doctor or nurse will e*amine the baby. "his may show:
• Stretched or swollen "eins on the baby4s scalp
• 'bnormal sounds when the health care pro"ider taps lightly on
the skull,suggesting a problem with the skull bones
• 'll or part of the head may be larger than normal, usually in
the front part
• (yes that look 5sunken in5
• White part of the eye appears o"er the colored area, making it
look like a5setting sun5
• 6ee.es may be normal
-
8/9/2019 Disorders of Neural Tube Formation
22/32
-
8/9/2019 Disorders of Neural Tube Formation
23/32
ithout treatment, up to in 10 people with hydrocephalus will
die. "hose who survive have
different amounts of intellectual, physical, and neuroloical
disabilities.
"he outlook depends on the cause. Hydrocephalus that is not due
to an infection has the best
outlook. ersons with hydrocephalus caused by tumors usually do
very poorly.
3ost children with hydrocephalus that survive for 1 year will
have a fairly normal life span.
Complications
"he shunt may become blocked. $ymptoms of such a blockae include
headache and
vomitin. $ureons may be able to help the shunt open without
havin to replace it.
"here may be other problems with the shunt, such as kinkin, tube
separation, or infection in
the area of the shunt.
ther complications may include:
• Complications of surgery
• Infections such as meningitis or encephalitis
• Intellectual impairment
• 9er"e damage #decrease in mo"ement, sensation, function$
• :hysical disabilities
Calling your health care pro"ider
$eek immediate medical care if your child has any symptoms of
this disorder. 4o to the
emerency room or call 511 if emerency symptoms occur, which
include:
• %reathing problems
• (.treme drowsiness or sleepiness
• Feeding di-culties
• Fe"er
• /igh+pitched cry
• 9o pulse #heart beat$
• Sei)ures
• Se"ere headache
-
8/9/2019 Disorders of Neural Tube Formation
24/32
• Sti! neck
• *omiting
6ou should also call your health care provider if the child has
been dianosed with
hydrocephalus and the condition ets worse and you are unable to
care for him or her athome.
:re"ention
rotect the head of an infant or child from in7ury. rompt
treatment of infections and other
disorders associated with hydrocephalus may reduce the risk of
developin the disorder.
6eferences
;7 Saunders (lse"ier@ A2;;>chap 3B37;;7
A7 6osenberg '7 %rain edema and disorders of cerebrospinal
uidcirculation7 In> %radley W, aro! 6%, Fenichel 1, =anko"ic =,
eds7Neurology in Clinical Practice7 3th ed7 :hiladelphia, :a>
%utterworth+/einemann@ A22B>chap D7
8eview 9ate: 11122012.
8eviewed by: Neil ;. ;aneshiro, 39, 3H', #linical 'ssistant
rofessor ofediatrics, , $tephanie $lon, and Nissi an.
'77'717, isclaimer
'.9.'.3., &nc. is accredited by
-
8/9/2019 Disorders of Neural Tube Formation
25/32
constitute endorsementscof those other sites. A 155BC2011
'.9.'.3., &nc. 'ny duplication or
distribution of the information contained herein is strictly
prohibited.
Copyright E A2;D, '77'717, Inc7
MicrocephalyLast reviewed: November 1D, 2011.
3icrocephaly is a condition in which a persons head is
sinificantly smaller than normal for
their ae and se*, based on standardi>ed charts. Head si>e
is measured as the distance around
the top of the head.
Common Causes
3icrocephaly most often occurs because the brain fails to row at
a normal rate. $kull rowth
is determined by brain rowth. Erain rowth takes place while in
the womb and durin
infancy.
#onditions that affect brain rowth can cause microcephaly. "hese
include infections, enetic
disorders, and severe malnutrition.
4enetic conditions that cause microcephaly include:
• Cornelia de 0ange syndrome
• Cri du chat syndrome
• own syndrome
• 6ubinstein+Taybi syndrome
• Seckel syndrome
• Smith+0emli+pit) syndrome
• Trisomy ;B
• Trisomy A;
"hese additional conditions may indirectly cause
microcephaly:
• Gncontrolled phenylketonuria #:
-
8/9/2019 Disorders of Neural Tube Formation
26/32
• Congenital to.oplasmosis
• Congenital cytomegalo"irus #C1*$
• Gse of certain drugs during pregnancy, especially alcohol and
phenytoin
Call your health care pro"ider if
3icrocephaly is often dianosed at birth or durin routine
well-baby e*aminations when the
infants heiht, weiht, and head circumference is measured. &f
you suspect your infants head
si>e is too small or not rowin normally, consult your health
care provider.
What to e.pect at your health care pro"ider4s o-ce
3icrocephaly is usually discovered by the health care provider
durin routine e*amination.
Head measurements are part of all well-baby e*aminations up
to 1F months (loner in certain
circumstances). "hey are painless and take only a few seconds
while the measurin tape is
placed around the infants head.
9ocumentin microcephaly in detail may include:
• What is the head circumferenceH
• Is the head growing at a slower rate than the bodyH
• What other symptoms are thereH
Note: ' record of the head circumference should be
maintained over time.
'lthouh the health care provider maintains records on your baby,
it may be helpful to
maintain your own records, and brin them to the health care
providers attention if you
notice that the infants head rowth pattern seems to be
decreasin.
&f your health care provider dianoses your child with
microcephaly, you should note that in
your childs personal medical records.
6eferences
;7
A7 chap 3B37;27
8eview 9ate: 111D2011.
http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001360/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001343/http://www.ncbi.nlm.nih.gov/pubmedhealth/PMHT0001418http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001928/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001928/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001360/http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001343/http://www.ncbi.nlm.nih.gov/pubmedhealth/PMHT0001418http://www.ncbi.nlm.nih.gov/pubmedhealth/n/pmh_adam/A001928/
-
8/9/2019 Disorders of Neural Tube Formation
27/32
8eviewed by: 9avid #. 9udale, &&&, 39, rofessor of
3edicine, 9ivision of 4eneral
3edicine, 9epartment of 3edicine,
-
8/9/2019 Disorders of Neural Tube Formation
28/32
&t is most often caused by enetic abnormalities that
interfere with the rowth of the cerebral
corte* durin the early months of fetal development. &t
is associated with 9owns syndrome,
chromosomal syndromes, and neurometabolic syndromes. Eabies may
also be born with
microcephaly if, durin prenancy, their mother:
• abused drus or alcohol,
• became infected with a cytomealovirus,
• rubella (4erman measles), or varicella (chickenpo*) virus,
• was e*posed to certain to*ic chemicals, or
• had untreated phenylketonuria (;ures,
• difficulties with coordination and balance, and
• other brain or neuroloical abnormalities.
$ome children with microcephaly will have normal intellience and
a head that will row
bier, but they will track below the normal rowth curves
for head circumference.
Is there any treatment for microcephalyH
Comment on this Share Your Story
http://www.medicinenet.com/script/main/art.asp?articlekey=3573http://www.medicinenet.com/script/main/art.asp?articlekey=11490http://www.medicinenet.com/script/main/art.asp?articlekey=11490http://www.medicinenet.com/script/main/art.asp?articlekey=1936http://www.medicinenet.com/script/main/art.asp?articlekey=1936http://www.medicinenet.com/script/main/art.asp?articlekey=25825http://www.medicinenet.com/script/main/art.asp?articlekey=8709http://www.medicinenet.com/script/main/art.asp?articlekey=8709http://www.medicinenet.com/script/main/art.asp?articlekey=14092http://www.medicinenet.com/script/main/art.asp?articlekey=1985http://www.medicinenet.com/script/main/art.asp?articlekey=319http://www.medicinenet.com/script/main/art.asp?articlekey=1942http://www.medicinenet.com/script/main/submit-patient-comments.asp?questionid=1560http://www.medicinenet.com/script/main/art.asp?articlekey=20174http://www.medicinenet.com/script/main/art.asp?articlekey=38098http://www.medicinenet.com/script/main/art.asp?articlekey=3136http://www.medicinenet.com/script/main/art.asp?articlekey=11748http://www.medicinenet.com/script/main/art.asp?articlekey=11748http://www.medicinenet.com/script/main/submit-patient-comments.asp?questionid=1561http://www.medicinenet.com/script/main/art.asp?articlekey=3573http://www.medicinenet.com/script/main/art.asp?articlekey=11490http://www.medicinenet.com/script/main/art.asp?articlekey=11490http://www.medicinenet.com/script/main/art.asp?articlekey=1936http://www.medicinenet.com/script/main/art.asp?articlekey=25825http://www.medicinenet.com/script/main/art.asp?articlekey=8709http://www.medicinenet.com/script/main/art.asp?articlekey=14092http://www.medicinenet.com/script/main/art.asp?articlekey=1985http://www.medicinenet.com/script/main/art.asp?articlekey=319http://www.medicinenet.com/script/main/art.asp?articlekey=1942http://www.medicinenet.com/script/main/submit-patient-comments.asp?questionid=1560http://www.medicinenet.com/script/main/art.asp?articlekey=20174http://www.medicinenet.com/script/main/art.asp?articlekey=38098http://www.medicinenet.com/script/main/art.asp?articlekey=3136http://www.medicinenet.com/script/main/art.asp?articlekey=11748http://www.medicinenet.com/script/main/submit-patient-comments.asp?questionid=1561
-
8/9/2019 Disorders of Neural Tube Formation
29/32
"here is no treatment for microcephaly that can return a childs
head to a normal si>e or
shape. "reatment focuses on ways to decrease the impact of the
associated deformities and
neuroloical disabilities. #hildren with microcephaly and
developmental delays are usually
evaluated by a pediatric neuroloist and followed
by a medical manaement team. +arly
childhood intervention prorams that involve physical, speech,
and occupational therapistshelp to ma*imi>e abilities and
minimi>e dysfunction. 3edications are often used to control
sei>ures, hyperactivity,
and neuromuscular symptoms. 4enetic counselin may
help families
understand the risk for microcephaly in subse?uent
prenancies.
What is the prognosis for microcephalyH
$ome children will only have mild disability. thers, especially
if they are otherwise rowin
and developin normally, will have normal intellience and
continue to develop and meet
reular ae-appropriate milestones.
What research is being done on microcephalyH
"he National &nstitute of Neuroloical 9isorders and $troke
(N&N9$) conducts research
relatin to microcephaly in its laboratories at the National
&nstitutes of Health (N&H) and
supports additional research throuh rants to ma7or medical
institutions across the country. '
small roup of researchers studyin a rare neurometabolic syndrome
(D-49H), which
causes microcephaly, have successfully used amino
acid replacement therapy to reduce and
prevent sei>ures.
Defnition%y 1ayo Clinic sta!
3icrocephaly (my-kroh-$+%-uh-lee) is a rare neuroloical
condition in which an infants
head is sinificantly smaller than the heads of other children of
the same ae and se*.
$ometimes detected at birth, microcephaly usually is the result
of the brain developin
abnormally in the womb or not rowin as it should after
birth.
3icrocephaly can be caused by a variety of enetic and
environmental factors. #hildren with
microcephaly often have developmental issues. 4enerally theres
no treatment for
microcephaly, but early intervention may help enhance your
childs development and improve
?uality of life.
Coping and support%y 1ayo Clinic sta!
hen you learn your child has microcephaly, you may e*perience a
rane of emotions,
includin aner, fear, worry, sorrow and uilt. 6ou may not know
what to e*pect, and you
may worry about your childs future. "he best antidote for fear
and worry is information and
support. repare yourself:
http://www.medicinenet.com/script/main/art.asp?articlekey=4812http://www.medicinenet.com/script/main/art.asp?articlekey=4812http://www.medicinenet.com/script/main/art.asp?articlekey=4553http://www.medicinenet.com/script/main/art.asp?articlekey=4553http://www.medicinenet.com/script/main/art.asp?articlekey=34038http://www.medicinenet.com/script/main/art.asp?articlekey=34038http://www.medicinenet.com/script/main/art.asp?articlekey=2222http://www.mayoclinic.com/health/AboutThisSite/AM00057http://www.mayoclinic.com/health/AboutThisSite/AM00057http://www.medicinenet.com/script/main/art.asp?articlekey=4812http://www.medicinenet.com/script/main/art.asp?articlekey=4553http://www.medicinenet.com/script/main/art.asp?articlekey=34038http://www.medicinenet.com/script/main/art.asp?articlekey=2222http://www.mayoclinic.com/health/AboutThisSite/AM00057http://www.mayoclinic.com/health/AboutThisSite/AM00057
-
8/9/2019 Disorders of Neural Tube Formation
30/32
-
8/9/2019 Disorders of Neural Tube Formation
31/32
• &n anencephaly, the bones of the skull and brain do not
develop properly. Eabies with
anencephaly are missin lare areas of the brain and have an
incomplete skull.
• 'nencephaly affects about 1 out of every 1,000 prenancies, but
most cases end up as
miscarriaes. 'bout 1 out of every 10,000 babies in the
-
8/9/2019 Disorders of Neural Tube Formation
32/32
'nencephaly is a comple* condition that is likely caused by the
interaction of multiple
enetic and environmental factors. $ome of these factors
have been identified, but many
remain unknown.
#hanes in do>ens of enes may influence the risk of
anencephaly. "he best-studied of these
enes is 3"H%8, which provides instructions for makin a protein
that is involved in
processin the E-vitamin folate (also called folic
acid or vitamin E5). #hanes in other enes
related to folate processin and enes involved in the development
of the neural tube have
also been studied as potential risk factors for anencephaly.
However, none of these enes
appear to play a ma7or role in causin the condition.
8esearchers have also e*amined environmental factors that could
contribute to the risk of
anencephaly. ' shortae (deficiency) of folate appears to play a
sinificant role. $tudies have
shown that women who take supplements containin this
vitamin before they et prenant
and very early in their prenancy are sinificantly less
likely to have a baby with anencephalyor a related neural tube
defect. ther possible risk factors for anencephaly include
diabetes
mellitus, obesity, e*posure to hih heat (such as
a fever or use of a hot tub or sauna) in early
prenancy, and the use of certain anti-sei>ure
medications durin prenancy. However, it is
unclear how these factors may influence the risk of
anencephaly.
Reviewed on 10/23/2012
http://www.medicinenet.com/script/main/art.asp?articlekey=31304http://www.medicinenet.com/script/main/art.asp?articlekey=43991http://www.medicinenet.com/script/main/art.asp?articlekey=8899http://www.medicinenet.com/script/main/art.asp?articlekey=33915http://www.medicinenet.com/script/main/art.asp?articlekey=343http://www.medicinenet.com/script/main/art.asp?articlekey=343http://www.medicinenet.com/script/main/art.asp?articlekey=943http://www.medicinenet.com/script/main/art.asp?articlekey=943http://www.medicinenet.com/script/main/art.asp?articlekey=361http://www.medicinenet.com/script/main/art.asp?articlekey=361http://www.medicinenet.com/script/main/art.asp?articlekey=361http://www.medicinenet.com/script/main/art.asp?articlekey=31304http://www.medicinenet.com/script/main/art.asp?articlekey=43991http://www.medicinenet.com/script/main/art.asp?articlekey=8899http://www.medicinenet.com/script/main/art.asp?articlekey=33915http://www.medicinenet.com/script/main/art.asp?articlekey=343http://www.medicinenet.com/script/main/art.asp?articlekey=343http://www.medicinenet.com/script/main/art.asp?articlekey=943http://www.medicinenet.com/script/main/art.asp?articlekey=361