Embed Size (px)
Citation preview

Disordered Eating and Unhealthy Weight Reduction Practices amongAdolescent Females
MARGARET GRIGG, M.MED.SCI.,* JENNY BOWMAN, PH.D.,† AND SALLY REDMAN, PH.D.‡
*The Royal Australian College of General Practitioners Training Program, North Ryde, Sydney, New South Wales 2113; †Faculty ofMedicine and Health Sciences, University of Newcastle, Newcastle, New South Wales 2308; and ‡Cancer Screening Unit, NSW Cancer
Council, Kings Cross, Sydney, New South Wales 2011, Australia
Background. Dissatisfaction with body weight andthe use of unhealthy weight reduction practices havebeen reported among adolescent females. There is aneed for methodologically rigorous studies using largerepresentative samples of adolescent females to accu-rately assess the prevalence of these behaviors andattitudes.Methods.Eight hundred sixty-nine Australian school
girls ages 14–16 years were administered a self-reportquestionnaire to determine the prevalence of disor-dered eating behaviors, unhealthy dieting practices,and distorted body image. Anthropometric (heightand weight) data were collected on each of these ado-lescent females.Results. The prevalences of disordered eating, un-
healthy dieting, and distorted body image were 33, 57,and 12%, respectively. Over one-third (36%) of the totalsample had used at least one ‘‘extreme’’ dietingmethod in the past month, i.e., ‘‘crash’’ dieting, fasting,slimming tablets, diuretics, laxatives, and/or ciga-rettes to lose weight. Of the total sample, 77% wantedto lose weight and 51% had tried to lose weight in thepast month. Motivating factors for disordered eatingand unhealthy dieting behaviors were peer pressure,media pressure, and the perception that extreme diet-ing strategies were harmless.Conclusion. The prevalence of disordered eating and
dieting behaviors among adolescent females shown bythis study suggests the need for preventive programsencouraging appropriate eating and dieting behav-iors. © 1996 Academic Press, Inc.
Key Words: Adolescent; dieting; weight reduction;disordered eating; eating disorder; body weight.
INTRODUCTION
Overseas and Australian studies show that manynormal-weight adolescents, especially females, are dis-satisfied with their weight [1,2]. They want to be thin-ner [1,2]. Extreme weight control strategies, such as
fasting, vomiting, diet pills, laxatives, cigarettes, anddiuretics were reported in a substantial proportion ofadolescent females [3,4]. In the United States Killen etal. [4] found that 11% of female adolescents (n 4 823)reported the regular use of self-induced vomiting. Afurther 13% reported regularly using some form ofpurging behavior such as vomiting, laxatives, and/ordiuretics for weight control [4]. In Australia Wertheimet al. [5] surveyed 606 adolescent females. They foundthat 9% reported vomiting, 6% used diet pills, a further6% used laxatives, and 3% used diuretics regularly tocontrol their weight. Eleven percent of these girls re-ported using at least one extreme weight loss behavior(i.e., fasting, ‘‘crash’’ dieting, diet pills, laxatives, anddiuretics) at least weekly [5].Adolescents who diet even when they have normal
body weight can threaten their nutritional status.They may deny their bodies important nutritional com-ponents at a time when they are most needed [6]. Iflarge amounts of fat are lost, amenorrhoea, ketosis,reduced body mass, reduced lean muscle tissue, re-duced basal metabolic rate, fatigue, irritability, insom-nia, lack of concentration, and growth failure can re-sult [7]. Furthermore, intermittent dieting may con-tribute to obesity in adolescents by decreasing basalenergy needs [8] and making subsequent weight lossmore difficult.Eating disorders such as anorexia nervosa and bu-
limia nervosa are usually preceded by dieting [6]. Con-sequently, dieting is regarded as an important risk fac-tor for the development of an eating disorder [9]. Onestudy estimated that at 15 years of age, the relativerisk of dieters becoming disordered eaters is eighttimes that of nondieters [10]. Anorexia nervosa has itshighest incidence in girls at the beginning of adoles-cence and bulimia nervosa has its highest incidence atthe end of adolescence [9].Australian data regarding the prevalence of disor-
dered eating behaviors and unhealthy weight reduc-tion practices among adolescents is limited to severalstudies that have used relatively small and selectivesamples. Abraham et al. [11], Huon et al. [12], andHuon et al. [13] used small sample sizes of less than
Address reprint requests to Margaret Grigg, 1/134 Ramsgate Ave.,Bondi, Sydney, NSW 2026, Australia.
PREVENTIVE MEDICINE 25, 748–756 (1996)ARTICLE NO. 0115
748
0091-7435/96 $18.00Copyright © 1996 by Academic Press, Inc.All rights of reproduction in any form reserved.

150 girls. Ben-Tovim et al. [14], Paxton et al. [2], andWertheim et al. [5] used larger sample sizes (356, 341,and 606 girls, respectively) but sampled from eitherone school or only a few selected schools.International data about the prevalence of disor-
dered eating behaviors and unhealthy weight reduc-tion practices among adolescents suffer similar samplesize and sampling procedure limitations. In particular,few studies using school populations have addressedthe issue of clustering [15]. In addition, many studieshave not used objective assessments of body size(height and weight) to evaluate the ‘‘appropriateness’’of weight concerns and dieting behaviors reported byadolescents in questionnaires.The present study overcomes these methodological
problems. It assesses the prevalence of disordered eat-ing behaviors, unhealthy weight reduction practices,and distorted body image in a large random sample ofAustralian school girls ages 14–16 years. The studyalso investigates the relationship between dietingpractices and a range of demographic and psychosocialvariables to identify possible strategies for interven-tion.
METHODOLOGY
First, an initial sample of 32 government highschools was randomly selected from within one regionof New South Wales, Australia. Of these 32 schools, 8were ineligible as they were already participating inother research projects, 3 were nonconsenting (partici-pation was at the discretion of the principal) and 1became a pilot school, leaving a final sample of 20schools to give a school consent rate of 87.5%. Second,from each school three classes were randomly selectedproviding students between 14 and 16 years of age.This two-stage cluster sampling approach, while con-venient, had the disadvantage of reducing the effectivesample size. Individuals within a cluster (studentswithin classes in the chosen schools) were more likelyto have similar knowledge, attitudes, and behaviorscompared with individuals selected at random. Indi-viduals within a cluster do not act independently anddecrease their contribution to the sample size. This re-duction in sample size was taken into account in thesample size calculations.Only nongraded classes were included to avoid bias
concerning academic ability. All female students in theselected classes who gave their own consent and hadtheir parents’ consent were eligible to participate inthe study. Participants completed an anonymous ques-tionnaire administered to each class separately duringone school lesson (35–50 min depending on the school).After the questionnaire was administrated, anthro-
pometric (height and weight) data were collected oneach participant. Height was measured to the nearest0.5 of a centimeter on a Harpenden stadiometer.
Weight was measured to the nearest 0.5 of a kilogramon a standard, calibrated platform scale. The studentswere measured in light clothing and without shoes.The BMI (body weight in kilograms divided by theheight in meters squared) was calculated to assess theactual body size of each person. BMIs were then as-signed to one of five categories, i.e., very underweight,underweight, normal, overweight, or very overweight.The questionnaire developed for this project was de-
signed to measure the prevalence of disordered eating,weight control practices, and distorted body image. Inaddition, the questionnaire investigated several pos-sible correlating variables such as demographics, ac-tual body size, current dieting, acceptance of the thinfemale stereotypes promoted by the media, social in-fluence, knowledge of dieting, and exercise levels.Adolescent females were considered ‘‘disordered eat-
ers’’ if they reported doing one or more of the followingthree behaviors in the past month: (a) binge eatingthree or more times, (b) vomiting after a meal forweight control, or (c) trying to lose weight, when theywere already very underweight (BMI < 18). Binge eat-ing was described in the questionnaire as ‘‘pigged-outor gone on an eating binge where you have overeaten oreaten lots of food in a short space of time.’’ These be-haviors are among the major symptoms of eating dis-orders according to the DSM-III criteria [16].Adolescent females were considered ‘‘unhealthy di-
eters’’ if they reported practicing one or more of thefollowing weight control methods in the past month: (a)inappropriately cutting out foods (dairy, meat, and/orcereal products) and not compensating with a balanceddiet (for example, a balanced vegetarian diet), (b) skip-ping meals, (c) using inappropriate or ‘‘fad’’ diets (forexample, ‘‘the Scarsdale diet, the Grape Fruit diet, orthe Hip and Thigh diet’’), (d) crash dieting (described inthe questionnaire as ‘‘where small amounts of food oronly drinks are allowed to be taken’’), (e) fasting (de-scribed in the questionnaire as ‘‘gone without food for aday or longer to help you lose weight’’), or (f) using dietaids (slimming drinks and biscuits), slimming tablets,laxatives, diuretics, or cigarettes to lose weight.Adolescent females reporting any one of the more
extreme and potentially dangerous weight controlmethods (fasting, crash dieting, laxatives, slimmingtablets, diuretics, and cigarettes) [2,4,10] were consid-ered ‘‘extreme dieters.’’Students were asked to report only those behaviors
that related specifically to losing weight.The BMI category of each participant was compared
with their perceived weight category (very under-weight, underweight, normal, overweight, and veryoverweight). If perceived and actual BMI differed bytwo or more categories, the participant was classifiedas having a distorted body image [17].Demographic characteristics were reported by stu-
dents and consisted of age, school year, and parents’
UNHEALTHY WEIGHT REDUCTION AMONG ADOLESCENT FEMALES 749

occupational status. Parents’ occupational status waslater assessed by the researcher using a slightly modi-fied Congalton scale of occupation [18]. This scale wasused to divide the respondents into three broad socio-economic categories (high: 1, 2, 3; medium: 4, 5; andlow: 6, 7, 8).Actual body size was determined by each partici-
pant’s categorized BMI. BMI is considered a reliableindicator of body fat [19] and is suitable for use withchildren [20]. BMI was categorized according to theAustralian National Health and Medical ResearchCouncil (NH&MRC) [21] standards (>30, obese or veryoverweight; 25–30, overweight; 20–25, acceptable; <20,underweight) and the Australian Nutrition Founda-tion which suggests a very underweight group forBMIs < 18 [22]. For subsequent analyses these catego-ries were collapsed into three groups, ‘‘overweight,’’‘‘normal,’’ and ‘‘underweight.’’Participants were asked to report whether they were
currently trying or had previously tried to lose weight(in the last year and in the last month).Social influences were assessed by several questions
(using a ‘‘Yes,’’ ‘‘No,’’ and ‘‘Does not apply’’ responseformat) regarding:
(a) Approval of current body weight by family, peers,and others. Students were asked whether parents,other family members, female friends, male friends,and other people had suggested to them that they wereover- or underweight.
(b) Family dieting. Students were asked whetherany family members (apart from themselves) had di-eted to lose weight in the past month.
(c) Acceptance of the thin female stereotypes promotedby the media. Students were asked to rate the bodysize of the ‘‘typical, attractive female body shape pro-moted by mass media’’ on a 7-point scale ranging from‘‘very overweight’’ to ‘‘very underweight.’’ They werethen asked to compare this typical attractive mediaideal with their own weight status on a 7-point scaleranging from ‘‘heavier than you’’ to ‘‘lighter than you.’’Finally, participants were asked to gauge ‘‘how much’’they personally desired to have the ‘‘typical attractivefemale body shape promoted by mass media’’ on a3-point response scale (‘‘Yes, I would really like thatbody shape,’’ ‘‘Yes, I would quite like that body shape,’’and ‘‘No, I don’t really wish to have that body shape’’).The knowledge of dieting comprised three sections.
First, students were asked 11 questions concerning thesafety of several dieting methods. Second, studentswere asked 5 questions concerning the severity of beingvery overweight, overweight, or very underweight orhaving anorexia nervosa and bulimia nervosa. Third,students were given a series of true–false questions toassess their knowledge of the health effects of being
very overweight or very underweight or having an-orexia nervosa and bulimia nervosa.Students were asked to report how frequently they
exercised vigorously. Vigorously was defined in thequestionnaire as ‘‘exercise which makes you breatheharder or puff and pant and includes activities likeswimming, tennis, netball, athletics, bicycle riding,aerobics, rowing, football, soccer, and running.’’ Re-sponse categories on a 5-point scale ranged from ‘‘none’’to ‘‘seven or more times a week.’’The external reliability of the questionnaire was as-
sessed at the pilot stage using a test–retest method. Asample of 51 students from the pilot school was askedto complete the questionnaire on two occasions, 1 weekapart. The completed questionnaires were then ana-lyzed using tests of weighted k [23–25] for dichotomousdata. Of the 57 individual items kept from the pilotedquestionnaire and assessed for test–retest reliability,65% gave k coefficients indicating strong agreement,28% gave k coefficients indicating fair to good agree-ment, and 7% gave k coefficients indicating poor agree-ment. The multi-item Likert scale behavioral questionsgave k coefficients in the range 0.42–1.00. This showsthat substantial agreement exists between test–retestitems and indicates that the questionnaire is reliable[26]. Items showing poor agreement on test–retest (n4 4) were modified to improve clarity.
RESULTS
Statistical analysis was undertaken using the SASprogram [27]. Proportions and corresponding 95% CIswere calculated for disordered eaters, unhealthy diet-ers, extreme dieters, and students with a distortedbody image. The effects of clustering were taken intoaccount at this stage, affecting prevalence data CIwidth [15]. Clustering was assumed to occur mainly atthe class level: students in the same class were morelikely to possess similar knowledge, attitudes, and be-haviors. Inflation factors (IF) and intraclass correla-tions (IC) were calculated for disordered eating (IF 41.8, IC 4 0.06), unhealthy (IF 4 4.9, IC 4 0.28), andextreme dieting (IF 4 1.7, IC 4 0.05) using prevalenceestimates obtained from pilot data. An IF was also cal-culated for distorted body image; however, very littlecorrelation existed within classes, that is, the relation-ship between perceived weight and actual weight foreach class member was independent of other classmembers. The variance for each 95% CI calculation fordisordered eating and unhealthy and extreme dietingwas multiplied by the corresponding IF to account forclustering. Subsequent to these calculations all datawere analyzed with the units of measurement viewedas individuals and not class groups. The clustering ef-fect was not taken into account when the relationshipsbetweendietingpractices and correlates (associated fac-tors) were investigated, as it would not significantly
GRIGG, BOWMAN, AND REDMAN750

alter the outcomes. Correlates were then constructed,the majority being categorical with the exception of theknowledge scores. Knowledge scores were continuousand approximately Gaussian in distribution [28]. Totest for any statistically significant associations be-tween each outcome variable and each categorical cor-relate the x2 test, Yates corrected where appropriate,was used. Analysis of variance was used to test for anystatistically significant associations between each ofthe outcome variables and the continuous predictorvariable [28]. The main measure of association forthese tests was the odds ratio and 95% CI. Statisticalsignificance was determined at a conservative level ofP 4 0.01 to allow for multiple univariate testing.A total of 869 girls ages 14–17 years took part in this
survey (88% consent rate), with a mean of 44 femalestudents per school and 15 female students per class.Of the sample, 26.6% were 14-year-olds, 35.5% were15-year-olds, 30.0% were 16-year-olds, and the remain-ing 7.5% were 17 to 18 years of age.The mean and standard deviation for height and
weight of all the females was 1.636 m (±0.064) and 59.3kg (±10.7), respectively.According to the NH&MRC [21] and Australian Nu-
trition Foundation [22] categorization of BMI, 3.8% ofthe girls were considered obese (BMI greater than 30)and 12.0% overweight (BMI equal to 30 but greaterthan 25), while 54.6% were in the acceptable range(BMI 20–25), and 29.7% were underweight (BMI < 20).Of the total sample of girls, 5.9% had a BMI < 18 asshown in Fig. 1.Of the total sample, 27.4% reported monthly binge
eating, 8.0% monthly vomiting, and 0.4% dieting whenthey were actually very underweight. Overall, 33% ofthe sample reported at least one disordered eating be-havior (95% CI 28.8, 37.2).At the time of this survey, 47% of the total sample (n
4 398/845) were currently trying to lose weight. Thatis, 19% of the actual underweight students (n 449/252), 56% of the actual normal-weight students (n4 256/461), and 71% of the actual overweight students(n 4 93/132) were trying to lose weight. Of all thestudents, 64% reported having tried to lose weight inthe past year and 51% had tried to lose weight in thepast month, regardless of their body weight. Further-more, 77% of the total sample (n 4 673/869) reportedthat they had wanted to lose weight in the past year.A large proportion of females reported exercising
more (77%, 95% CI 70.8, 83.2) and eating less fatty,sugary foods (71%, 95% CI 64.3, 77.7) to lose weight.However, only 26% (95% CI 19.4, 32.6) reported usingeither exercising and/or eating less fatty, sugary foodsas the only methods to reduce weight. These acceptablemethods for losing weight were more often used in con-junction with other unhealthy methods of weight lossas shown in Table 1. Overall, 57% of the sample wereclassified as practicing ‘‘unhealthy dieting’’ (95% CI49.7, 64.2) and 36% as practicing extreme dieting (i.e.,crash dieting, fasting, slimming tablets, diuretics,laxatives, and cigarettes) (95% CI 31.8, 40.2).When subjects were asked to characterize their cur-
rent weight, 63.0% perceived themselves to be over-weight (15.8% of the total sample were actually over-weight according to their BMI), 28.3% perceived them-selves to be ‘‘just right’’ (54.6% were actually of normalweight according to their BMI), and 8.7% perceivedthemselves to be underweight (29.7% were actually un-derweight according to their BMI). Figure 2 shows therelationship between perceived body weight and actualbody weight.A person was classified as having a distorted body
image if their perceived weight category and their ac-tual BMI category differed by two or more. Overall,12% of the sample had a distorted body image (95% CI
FIG. 1. Body size in adolescent girls. BMIs were categorized as follows: very overweight, BMI > 30; overweight, BMI ø 30 but >25;normal, BMI 20–25; underweight, BMI < 20 but ù18; very underweight, BMI < 18.
UNHEALTHY WEIGHT REDUCTION AMONG ADOLESCENT FEMALES 751

10.2, 14.6). x2 analysis showed that of the studentswith a distorted body image, almost half were disor-dered eaters (xc
2 4 5.735, df 4 1, P 4 0.017, OR 1.7,95% CI 1.1, 2.6) and over two-thirds practiced un-healthy dieting methods (xc
2 4 5.184, df 4 1, P 40.023, OR 1.7, 95% CI 1.1, 2.6) (Fig. 3).Multiple logistic regression analyses, using the
BMDP statistical package [29], were employed to testfor relationships between the correlating variables andthe outcome variables. x2 analyses were used to selectvariables for the logistic regression models. Variableswere included in the models if their P values were<0.25 from the bivariate analyses.The five variables which significantly correlated
with disordered eating behaviors by regression analy-sis were female friends suggesting the girl was over-weight, male friends suggesting the girl was over-weight, the desire to have the slender media-promoted
‘‘ideal’’ body shape, currently trying to lose weight, andlower knowledge of dieting, weight, and eating prob-lems. Table 2 reports the logistic regression results. Italso includes all variables which were found to be sig-nificant on x2 analyses and then entered into themodel.The seven variables which significantly correlated
with unhealthy dieting behaviors by regression analy-sis were the desire to have the slender media-promoted‘‘ideal’’ body shape, currently trying to lose weight,family members other than parents suggesting the girlwas overweight, other people suggesting the girl wasoverweight, being 15 years of age, being normal- oroverweight, and lower knowledge scores (i.e., knowl-edge of weight, weight reduction methods, and eatingproblems).The six variables which significantly correlated with
extreme dieting behaviors by regression analysis werethe desire to have the slender media-promoted ‘‘ideal’’body shape, male friends suggesting the girl was un-derweight, currently trying to lose weight, familymembers other than parents suggesting the girl wasoverweight, other people suggesting the girl was over-weight, and being normal- or overweight. Table 3 re-ports the logistic regression results. It also includes allvariables which were found to be significant on x2
analyses and then entered into the model.The five variables which significantly correlated
with distorted body image by regression analysis werebeing underweight, currently trying to lose weight, thedesire to have the slender media-promoted ‘‘ideal’’ bodyshape, students’ perception of the media-promoted‘‘ideal’’ body shape as normal- or overweight, being inschool year 9.
DISCUSSION
This study found the prevalence of disordered eating,unhealthy dieting, and distorted body image among
TABLE 1Prevalence of Unhealthy and Extreme Weight
Reduction Practices
Behavior (monthly) Prevalence % (95% CI)
No dairya (n 4 861) 16 (10.5, 21.4)No meatsa (n 4 860) 18 (12.3, 23.6)No starchy foodsa (n 4 862) 13 (8.0, 17.9)Slimming biscuit use (n 4 858) 15 (9.7, 20.3)Slimming drink use (n 4 857) 11 (6.4, 15.6)Skipping meals (n 4 862) 46 (38.6, 53.4)Fad dieting (n 4 858) 14 (8.9, 19.2)‘‘Crash’’ dietingb (n 4 861) 22 (18.3, 25.7)Fastingb (n 4 859) 21 (17.4, 24.6)Slimming tablet useb (n 4 861) 5 (3.1, 6.9)Diuretic useb (n 4 860) 2 (0.8, 3.2)Laxative useb (n 4 862) 5 (3.1, 6.9)Cigarette useb (n 4 862) 12 (9.1, 14.9)
a These foods were cut out and not compensated for with a balanced diet (forexample, a balanced vegetarian diet).
b Extreme dieting was defined as ‘‘crash’’ dieting, fasting, or use of slimmingtablets, diuretics, laxatives, and cigarettes.
FIG. 2. Body size perception and actual body size in adolescent girls.
GRIGG, BOWMAN, AND REDMAN752

Australian school girls ages 14–16 years to be 33, 57,and 12%, respectively. Twenty-seven percent reportedmonthly binge eating and 8% reported monthly vomit-ing. Similar levels of monthly binge eating [30] andmonthly vomiting have been reported among female
adolescents in the United States. These U.S. studieshave reported higher (11%) [4] and lower (2%) [31] lev-els of vomiting. Two recent Australian studies withsmaller and more selective samples than the presentstudy have reported slightly higher levels of regularvomiting (9–11%) and lower levels of regular binge eat-ing (17%) [2,14]. The discrepancy in the reportedprevalence of binge eating may be due, in part, to dif-ferent criteria for defining the frequency of binge eat-ing.Over half of the females surveyed in this study used
at least one unhealthy weight reduction method in thepast month, most commonly skipping meals (46%).Paxton et al. also found the same proportion of skip-ping meals to lose weight [2]. The practice of skippingmeals can be problematic with adolescents if they ‘‘fillup’’ on nonnutritious snack foods high in fat, sugar,and salt. This practice can lower their intake of essen-tial nutrients and may lead to obesity.In this study significant proportions of females (be-
tween 10 and 20%) also used a variety of other un-healthy weight reduction practices which may restrictnutrient and energy intakes. These included cuttingout all meats (rich sources of iron and zinc), all dairyfoods (rich sources of calcium), or all starchy foods (richsources of energy and fiber) and not compensating witha balanced diet (for example a balanced vegetariandiet); fad dieting; and using special dietary aids and/ormeal replacement products. If such undesirable dietingefforts were superimposed upon eating patterns whichwere poor to begin with, they might lead to suboptimalor marginal nutrition in some adolescents [32,33].Weight-loss attempts and dietary restriction in adoles-cents have also been associated with a variety of symp-toms including fatigue, anxiety, menstrual irregulari-ties, impaired concentration, listlessness, and poorschool performance [34].
TABLE 2Results of Model Building Logistic Regression for
Correlates of Disordered Eatinga
Variables NbOddsratio
95% CI ofodds ratio
Friends who are female suggesting overweightNoc 652Yes 35 3.27 1.49, 7.18d
Friends who are male suggesting overweightNo
c595
Yes 92 2.40 1.45, 3.96d
Wish to have ‘‘ideal’’ body shapeNoc 90Yes, quite 307 1.18 0.65, 2.15Yes, really 290 2.00 1.08, 3.71d
Currently trying to lose weightNoc 363Yes 324 1.57 1.08, 2.28d
Knowledge 0.95 0.91, 0.98d
Other family members suggesting overweightNoc 530Yes 157 0.67 0.43, 1.04
Goodness of fit x2 (Hosmer–Lemeshow) 4 3.809, df 4 8, P 4 0.87.
a Disordered eating was defined as undertaking any one or more ofthe following behaviors in the past months: (i) binge eating three ormore times, (ii) vomiting after a meal for weight control, or (iii) tryingto lose weight, when already very underweight (BMI < 18).
b For each item, the sample size varied depending on the numberof incomplete data which were excluded.
c Reference group.d Significant odds ratio compared with reference group.
FIG. 3. Distorted body image and actual body size in adolescent girls.
UNHEALTHY WEIGHT REDUCTION AMONG ADOLESCENT FEMALES 753
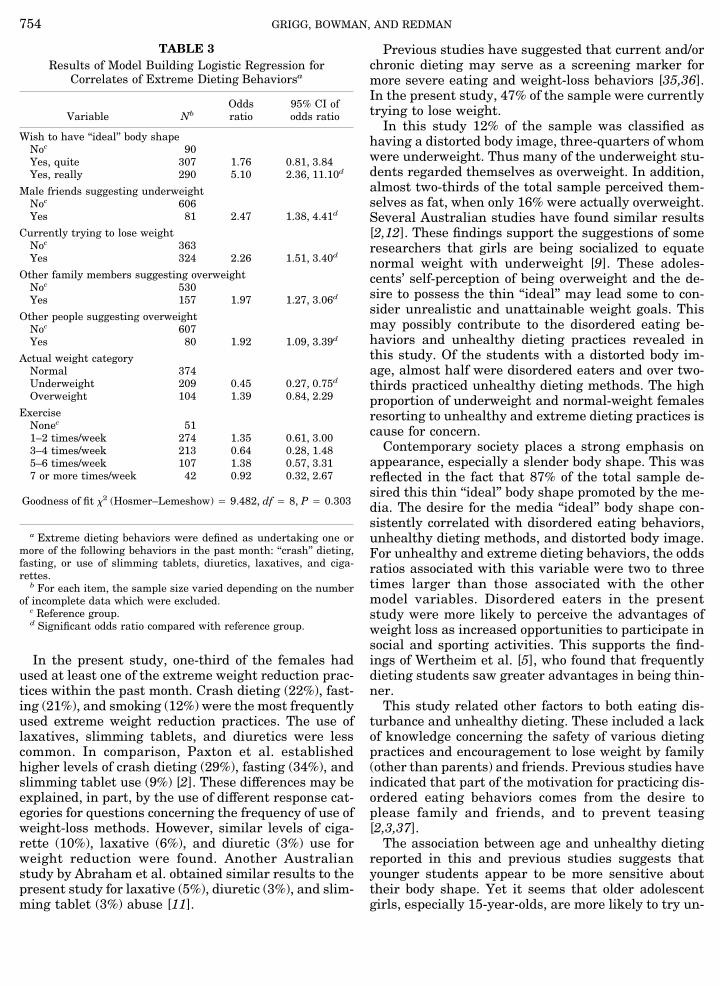
In the present study, one-third of the females hadused at least one of the extreme weight reduction prac-tices within the past month. Crash dieting (22%), fast-ing (21%), and smoking (12%) were the most frequentlyused extreme weight reduction practices. The use oflaxatives, slimming tablets, and diuretics were lesscommon. In comparison, Paxton et al. establishedhigher levels of crash dieting (29%), fasting (34%), andslimming tablet use (9%) [2]. These differences may beexplained, in part, by the use of different response cat-egories for questions concerning the frequency of use ofweight-loss methods. However, similar levels of ciga-rette (10%), laxative (6%), and diuretic (3%) use forweight reduction were found. Another Australianstudy by Abraham et al. obtained similar results to thepresent study for laxative (5%), diuretic (3%), and slim-ming tablet (3%) abuse [11].
Previous studies have suggested that current and/orchronic dieting may serve as a screening marker formore severe eating and weight-loss behaviors [35,36].In the present study, 47% of the sample were currentlytrying to lose weight.In this study 12% of the sample was classified as
having a distorted body image, three-quarters of whomwere underweight. Thus many of the underweight stu-dents regarded themselves as overweight. In addition,almost two-thirds of the total sample perceived them-selves as fat, when only 16% were actually overweight.Several Australian studies have found similar results[2,12]. These findings support the suggestions of someresearchers that girls are being socialized to equatenormal weight with underweight [9]. These adoles-cents’ self-perception of being overweight and the de-sire to possess the thin ‘‘ideal’’ may lead some to con-sider unrealistic and unattainable weight goals. Thismay possibly contribute to the disordered eating be-haviors and unhealthy dieting practices revealed inthis study. Of the students with a distorted body im-age, almost half were disordered eaters and over two-thirds practiced unhealthy dieting methods. The highproportion of underweight and normal-weight femalesresorting to unhealthy and extreme dieting practices iscause for concern.Contemporary society places a strong emphasis on
appearance, especially a slender body shape. This wasreflected in the fact that 87% of the total sample de-sired this thin ‘‘ideal’’ body shape promoted by the me-dia. The desire for the media ‘‘ideal’’ body shape con-sistently correlated with disordered eating behaviors,unhealthy dieting methods, and distorted body image.For unhealthy and extreme dieting behaviors, the oddsratios associated with this variable were two to threetimes larger than those associated with the othermodel variables. Disordered eaters in the presentstudy were more likely to perceive the advantages ofweight loss as increased opportunities to participate insocial and sporting activities. This supports the find-ings of Wertheim et al. [5], who found that frequentlydieting students saw greater advantages in being thin-ner.This study related other factors to both eating dis-
turbance and unhealthy dieting. These included a lackof knowledge concerning the safety of various dietingpractices and encouragement to lose weight by family(other than parents) and friends. Previous studies haveindicated that part of the motivation for practicing dis-ordered eating behaviors comes from the desire toplease family and friends, and to prevent teasing[2,3,37].The association between age and unhealthy dieting
reported in this and previous studies suggests thatyounger students appear to be more sensitive abouttheir body shape. Yet it seems that older adolescentgirls, especially 15-year-olds, are more likely to try un-
TABLE 3Results of Model Building Logistic Regression for
Correlates of Extreme Dieting Behaviorsa
Variable NbOddsratio
95% CI ofodds ratio
Wish to have ‘‘ideal’’ body shapeNoc 90Yes, quite 307 1.76 0.81, 3.84Yes, really 290 5.10 2.36, 11.10d
Male friends suggesting underweightNoc 606Yes 81 2.47 1.38, 4.41d
Currently trying to lose weightNoc 363Yes 324 2.26 1.51, 3.40d
Other family members suggesting overweightNoc 530Yes 157 1.97 1.27, 3.06d
Other people suggesting overweightNoc 607Yes 80 1.92 1.09, 3.39d
Actual weight categoryNormal 374Underweight 209 0.45 0.27, 0.75d
Overweight 104 1.39 0.84, 2.29
ExerciseNonec 511–2 times/week 274 1.35 0.61, 3.003–4 times/week 213 0.64 0.28, 1.485–6 times/week 107 1.38 0.57, 3.317 or more times/week 42 0.92 0.32, 2.67
Goodness of fit x2 (Hosmer–Lemeshow) 4 9.482, df 4 8, P 4 0.303
a Extreme dieting behaviors were defined as undertaking one ormore of the following behaviors in the past month: ‘‘crash’’ dieting,fasting, or use of slimming tablets, diuretics, laxatives, and ciga-rettes.
b For each item, the sample size varied depending on the numberof incomplete data which were excluded.
c Reference group.d Significant odds ratio compared with reference group.
GRIGG, BOWMAN, AND REDMAN754

healthy dieting methods [38,39]. Longitudinal investi-gation would add to our knowledge of how the factorsmeasured in the present study develop and changewith age.
CONCLUSION
While this study overcame many of the methodologi-cal constraints of previous research, a number of fac-tors should be acknowledged as limitations. First, inconducting such a study, it was difficult to be certain ofthe representativeness of the sample, although thehigh consent rate (88%) suggests that the possible ef-fects of selection bias would be minimal. Second, pri-vate schools were not included in the sample. Onemight expect a higher than average socioeconomic sta-tus among this group and possibly higher levels of theoutcome measures [40]. Third, self-report instrumentsassume that subjects will respond accurately. As sub-jects with disordered eating and unhealthy dietingpractices often display significant denial [41], some un-derreporting may be expected. Fourth, the definitionfor ‘‘disordered eating’’ used in this study is less rigidthan many of the ‘‘all-or-none’’ type of definitions usedto identify severe cases of eating disorders and doescontribute to the high prevalence reported. However,the purpose of a more liberal definition is to representthe entire spectrum of the disordered-eating con-tinuum, from the less severe ‘‘indicators’’ present in thepopulation in the absence of a true eating disorder tothe clinical extreme of bulimia nervosa and anorexianervosa. Regardless of the type or severity of the eatingdisorder, the medical consequences of inappropriateeating practices and unhealthy dieting behaviors canbe quite severe [4,32,33].This study indicates that a significant proportion of
adolescents is engaged in disordered eating behaviorsand unhealthy dieting practices. These practices aloneor combined with a distorted body image, or a strongdesire to attain the thin ‘‘ideal’’ female body shape, mayplace these young people at considerable risk. As a re-sult they may develop eating disorders or other seriousnutrition-related problems. For many of the adoles-cents in this study, their motivation to diet seemed tohave little to do with their actual body weight. Media,family (other than parents), and peer pressure to at-tain the ‘‘ideal’’ body shape provided much of the in-centive to diet. In particular a strong correlation ex-isted between media images and adolescent dieting.The need for longitudinal studies to investigate eat-
ing and dieting behaviors in adolescent populations isclear. We need to know whether the disordered andunhealthy behaviors persist over time, develop intomore severe conditions, or disappear. Interventionstudies are needed to evaluate the effects of education-al strategies targeting young adolescent females andtheir families and friends. The development of a
simple, easily administered screening device with goodpredictive validity for disordered eating and unhealthydieting behaviors is needed. This would enable theidentification of at-risk adolescents and the early de-tection of those with eating disorders. Identifying anddirecting educational activities to those at risk hasbeen suggested by Killen et al. [42].Educational interventions targeting younger at-risk
adolescents may be more likely to reduce the problembut while society (and in particular the media) stillattaches a stigma to obesity and rewards restrictiveeating/dieting practices, the problem will remain. Ide-ally, adolescents should be made to feel accepted andrespected regardless of their physical appearance.
REFERENCES
1. Wardle J, Beales S. Restraint, body image and food attitudes inchildren from 12 to 18 years. Appetite 1986;7:209–17.
2. Paxton SJ, Wertheim EH, Gibbons K, Szmukler GI, Hiller L,Petrovich J. Body image satisfaction, dieting beliefs and weightloss behaviours in adolescent girls and boys. J Youth Adolesc1991;20(3):361–79.
3. Hendren RL, Barber JK, Sigafoos A. Eating-disordered symp-toms in a nonclinical population: a study of female adolescents intwo private schools. J Am Acad Child Psychiatry 1986;25(6):836–40.
4. Killen JD, Taylor CB, Telch MJ, Saylor KE, Maron DJ, RobinsonTN. Self-induced vomiting and laxative and diuretic abuseamong teenagers. J Am Med Assoc 1986;255:1447–9.
5. Wertheim EH, Paxton SJ, Maude D, Szmukler GI, Gibbons K,Hiller L. Psychological predictors of weight loss behaviors andbinge eating in adolescent girls and boys. Int J Eating Disord1992;12(2):151–60.
6. Polivy J, Herman CP. Dieting and binge eating. Am Psychol1985;40:193–201.
7. Mallick MJ. Health hazards of obesity and weight control inchildren: a review of the literature. Am J Public Health 1983;73:78–82.
8. Steen SN, Opplinger RA, Brownell KD. Metabolic effects of re-peated weight loss and regain in adolescent wrestlers. J AmMedAssoc 1988;260:47–50.
9. Striegel-Moore RH, Silberstein LR, Rodin J. Towards an under-standing of risk factors for bulimia. Am Psychol 1986;41:246–63.
10. Patton GC, Johnson-Sabine E, Woods K, Mann AH, Wakeling A.Abnormal eating attitudes in London schoolgirls: outcome attwelve month follow-up. Psychol Med 1990;20:383–94.
11. Abraham SF, Mira M, Beumont PJV, Sowerbutts TD, Llewellyn-Jones D. Eating behaviours among young women. Med J Aust1983;2:225–8.
12. Huon G, Brown LB. Attitude correlates of weight control amongsecondary school boys and girls. J Adolesc Health Care 1986;7:178–82.
13. Huon G, Brown LB. Psychological correlates of weight controlamong AN patients and normal girls. Br J Med Psychol 1984;57:61–6.
14. Ben-Tovim DI, Subbiah N, Schuetz B, Morton J. Bulimia: symp-toms and syndromes in an urban population. Aust N Z J Psy-chiatry 1989;23:73–80.
15. Donner A, Birkett N, Buck C. Randomisation by cluster: samplesize requirements and analysis. Am J Epidemiol 1981;114:906–14.
16. American Psychiatric Association. Diagnostic and statistical
UNHEALTHY WEIGHT REDUCTION AMONG ADOLESCENT FEMALES 755

manual of mental disorders: DSM-III. 3rd ed. Washington: Am.Psychiatric Assoc., 1980.
17. Mellin LM, Irwin CE, Scully S. Prevalence of disordered eatingin girls: a survey of middle-class children. J Am Diet Assoc1992;92(7):851–3.
18. Congalton AA. Status and prestige in Australia. Melbourne:Cheshire, 1969.
19. Bray GA. Definition, measurement and classification of the syn-dromes of obesity. Int J Obes 1978;2:99–112.
20. Rolland-Cachera M, Sempe M, Guilloud-Bataille M, Patois E,Pequignot-Guggenbuhl F, Fautrad V. Adiposity indices in chil-dren. Am J Clin Nutr 1982;36:178–84.
21. National Health and Medical Research Council. Report of the98th Session, Canberra, October 1984. Canberra: AustralianGov. Publ. Services, 1985:429.
22. Australian Nutrition Foundation. Aim for the healthy weightrange. Sydney: Australian Nutrition Found., 1993:1.
23. Cohen J. A coefficient of agreement of nominal scales. Educ Psy-chol Measure 1960;20:37–46.
24. Cohen J. Weighted kappa: nominal scale agreement with provi-sion for scaled disagreement of partial credit. Psychol Bull 1968;70:213–20.
25. O’Connell D, Dobson A. General observer-agreement measureson individual subjects and groups of subjects. Biometrics 1984;40:973–83.
26. Fleiss JL. Statistical methods for rates and proportions. Sydney:Wiley, 1981.
27. SAS Institute, Inc. SAS [computer program] release 6.03 for theIBM PC. Cary (NC): SAS Inst., 1988.
28. Bland M. An introduction to medical statistics. London: OxfordUniv. Press, 1987.
29. Dixon WJ. BMDP statistical software. Los Angeles: Univ. ofCalifornia Press, 1985.
30. Johnson C, Lewis C, Love I, Stuckey M. Incidence and correlates
of bulimic behavior in a female high school population. J YouthAdolesc 1984;13(1):15–27.
31. Moses N, Banilivy MM, Lifshitz F. Fear of obesity among ado-lescent girls. Pediatrics 1989;83(3):393–8.
32. Lifshitz F, Moses N. Nutritional dwarfing: growth, dieting andthe fear of obesity. J Am Coll Nutr 1988;7:367–76.
33. Pugliese M, Lifshitz F, Grad G, Fort P, Marks-Katz M. Fear ofobesity: a cause of short stature and delayed puberty. N Engl JMed 1983;309:513–8.
34. Nylander I. The feeling of being fat and dieting in a school popu-lation: epidemiologic, interview investigation. Acta SociomedScand 1971;3:17–26.
35. Maloney MJ, McGuire J, Daniels SR, Specker B. Dieting behav-iour and eating attitudes in children. Pediatrics 1989;84:482–7.
36. Story M, Rosenwinkel K, Himes JH, Resnick M, Harris LJ, BlumRW. Demographic and risk factors associated with chronic diet-ing in adolescents. American Journal of Diseases in Children1991;145:994–8.
37. Fabian LJ, Thompson JK. Body image and eating disturbance inyoung females. Int J Eating Disord 1989;8(1):63–74.
38. Davies E, Furnham A. The dieting and body shape concerns ofadolescent females. J Child Psychol Psychiatry 1986;27(3):417–28.
39. Richards MH, Casper RC, Larson R. Weight and eating concernsamong pre- and young adolescent boys and girls. J AdolescHealth Care 1990;11:203–9.
40. Crisp AH, Palmer RL, Kalucy RS. How common is AN? A preva-lence study. Br J Psychiatry 1976;128:549–54.
41. Vanderdeycken W, Vanderlinden J. Denial of illness and the useof self-reporting measures in anorexia. Int J Eating Disord 1983;1:47–60.
42. Killen JD, Hammer LD, Barr Taylor C, Litt I, Wilson DM, RichT, et al. An attempt to modify unhealthful eating attitudes andweight regulation practices of young adolescent girls. Int J Eat-ing Disord 1993;13(4):369–84.
GRIGG, BOWMAN, AND REDMAN756