Embed Size (px)
Citation preview

DISEASES OF WHITE DISEASES OF WHITE BLOOD CELLS BLOOD CELLS
Premed 3Premed 3 Dr RoopaDr Roopa

What Is Leukemia?What Is Leukemia?
Cancer of the white blood cellsCancer of the white blood cells Acute or ChronicAcute or Chronic Affects ability to produce normal Affects ability to produce normal
blood cellsblood cells Bone marrow makes abnormally Bone marrow makes abnormally
large number of immature white large number of immature white blood cells called blastsblood cells called blasts

HistoryHistory
Means “white blood” in GreekMeans “white blood” in Greek
Discovered by Dr. Alfred Velpeau in Discovered by Dr. Alfred Velpeau in France, 1827France, 1827
Named by pathologist Rudolf Virchow Named by pathologist Rudolf Virchow in Germany, 1845in Germany, 1845

LeukemiasLeukemias
↑ ↑ leukocytesleukocytes
Acute leukemiasAcute leukemias
1. Acute 1. Acute Lymphoblastic Lymphoblastic Leukemia (ALL)Leukemia (ALL)
2. Acute Myelogenous 2. Acute Myelogenous Leukemia (AML)Leukemia (AML)
Chronic leukemiasChronic leukemias
1.Chronic 1.Chronic LLymphoblastic ymphoblastic Leukemia (CLL)Leukemia (CLL)
2. Chronic Myelogenous 2. Chronic Myelogenous Leukemia (CML)Leukemia (CML)


Treatment may involve some combination of chemotherapy, radiation therapy, targeted therapy, and bone marrow transplant, in addition to supportive care and palliative care as needed.

The success of treatment depends on the type of leukemia and the age of the person.

Acute LeukemiasAcute Leukemias
Blast predominateBlast predominate Child or elderChild or elder Short & drastic courseShort & drastic course ALL – Lymphoblasts (pre-B or pre-T)ALL – Lymphoblasts (pre-B or pre-T) AML – MyeloblastsAML – Myeloblasts

Chronic LeukemiasChronic Leukemias
More mature cellsMore mature cells Middle ageMiddle age Longer & less devastating courseLonger & less devastating course CLL – LymphocytesCLL – Lymphocytes CML – Myeloid stem cellsCML – Myeloid stem cells

Acute LeukemiasAcute Leukemias
accumulation of blasts in the marrowaccumulation of blasts in the marrow

Acute Lymphoblastic Leukemia Acute Lymphoblastic Leukemia (ALL)(ALL)
ChildrenChildren Lymphoblasts (pre-B or pre-T)Lymphoblasts (pre-B or pre-T) Neoplastic transformation of theNeoplastic transformation of the
lymphoid stem cellslymphoid stem cells
• • Progressive accumulation of Progressive accumulation of Lymphoblasts in the bone marrowLymphoblasts in the bone marrow
•• Suppression of normal Suppression of normal hemopoiesishemopoiesis

ALLALL

• • Primarily a disease of Primarily a disease of childrenchildren and old ageand old age
• • B-cell subtypeB-cell subtype (80%)(80%)
• • T-cell subtypeT-cell subtype (20%)(20%)


ALL - PathogenesisALL - Pathogenesis
•• Etiology unknownEtiology unknown•• Genetic predisposition (some)Genetic predisposition (some)
Down syndromeDown syndrome•• Translocations (Translocations (worseworse prognosis) prognosis)
t(4;11)t(4;11) t(12;21)t(12;21) t(9;22)t(9;22)

Signs &SymptomsSigns &Symptoms
AnemiaAnemia InfectionInfection BleedingBleeding Bone painBone pain ArthritisArthritis SplenomegalySplenomegaly LymphadenopathyLymphadenopathy CNS involvementCNS involvement

ALLALL
Prognosis:Prognosis:•• Age 3-7, pre-B, L1 :Age 3-7, pre-B, L1 :
> 90% - CR> 90% - CR ( 2/3 - cure )( 2/3 - cure )•• Adults, mature B and T-ALL:Adults, mature B and T-ALL:
Less favorableLess favorable
Therapy: Therapy: Chemotherapy ( w/CNS Chemotherapy ( w/CNS prophylaxis ),prophylaxis ),
supportive care, BMTsupportive care, BMT

ACUTEACUTE MYELOGENOUS MYELOGENOUS
LEUKEMIA ( AML )LEUKEMIA ( AML )
- AdultsAdults- MyeloblastsMyeloblasts- monoblasts, eosinoblasts, monoblasts, eosinoblasts,
megakarioblasts, proerythroblasts, megakarioblasts, proerythroblasts, basophiloblastsbasophiloblasts
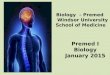
- Auer rods in the cytoplasm of the cellsAuer rods in the cytoplasm of the cells- Very rapidly progressive malignancyVery rapidly progressive malignancy

AMLAML

Auer rods in AMLAuer rods in AML

AML - PathogenesisAML - Pathogenesis
Environmental factors:Environmental factors:
High-dose radiation exposureHigh-dose radiation exposure
Myelotoxic agents (benzene, Myelotoxic agents (benzene, alkylating agents)alkylating agents)
Genetic abnormalities:Genetic abnormalities:
Down syndrome, Down syndrome, Immunodeficiency diseasesImmunodeficiency diseases

Differentiation from ALL may be Differentiation from ALL may be made by microscopy – presence of made by microscopy – presence of Auer Rods.Auer Rods.
Clinical features based onClinical features based on Marrow failure –anemia, bleeding, Marrow failure –anemia, bleeding,
DIC, infection…DIC, infection… Leukemic infiltration – bone pain, Leukemic infiltration – bone pain,
CNS signs, hepatosplenomegaly, CNS signs, hepatosplenomegaly, lymphadenopathy…lymphadenopathy…
Constitutional upset -- malaise, fever, Constitutional upset -- malaise, fever, weakness, polyarthritis.weakness, polyarthritis.

Course:Course:
•• Rapidly fatal if untreated (< 2 mo )Rapidly fatal if untreated (< 2 mo )
•• Median survival - 3 years after Median survival - 3 years after chem..chem..
•• Adverse prognostic factors:Adverse prognostic factors:
Age > 60Age > 60
t(9;21), t(9;21),
Previous chemotherapyPrevious chemotherapy
Leukocytosis > 100,000 /ulLeukocytosis > 100,000 /ul
Therapy:Therapy: Chemotherapy, supportive, BMTChemotherapy, supportive, BMT

***Remember this*** ***Remember this*** For Acute leukemiasFor Acute leukemias
acute leukemias = too many acute leukemias = too many blastsblasts in the in the marrowmarrow
2 broad categories: AML vs. ALL2 broad categories: AML vs. ALL a hematologic urgencya hematologic urgency prognosis is poor in adults; but good prognosis is poor in adults; but good
in kids with ALL.in kids with ALL.

CHRONIC LYMPHOCYTIC LEUKEMIA (CLL)CHRONIC LYMPHOCYTIC LEUKEMIA (CLL)
A monoclonal lymphoproliferative A monoclonal lymphoproliferative
disorder characterized by disorder characterized by lymphocytosis(>4000/cu.mm),lymphocytosis(>4000/cu.mm),
lymphadenopathylymphadenopathy and and splenomegalysplenomegaly
B - CLL > 95%B - CLL > 95%T - CLLT - CLL

CLL CLL
•• Most commonMost common adult leukemia in adult leukemia in
Western society (30% of all Western society (30% of all leukemias)leukemias)
•• Monoclonal proliferation of the Monoclonal proliferation of the small lymphocytes… small lymphocytes…
•• AgeAge > 40 > 40 M:F / 2:1M:F / 2:1

CLLPB and BM



CLL - PathologyCLL - Pathology
Blood:Blood:•• LymphocytosisLymphocytosis
( > 10,000 u/L - diagnostic )( > 10,000 u/L - diagnostic )•• (+) Coombs test (+) Coombs test (20%)(20%)•• Hypogammaglobulinemia Hypogammaglobulinemia (50-70%)(50-70%)•• Anemia, thrombocytopenia, neutropeniaAnemia, thrombocytopenia, neutropenia
Bone marrow:Bone marrow:•• nodular / interstitial infiltratesnodular / interstitial infiltrates•• diffuse - obliteration of normal diffuse - obliteration of normal hemopoiesishemopoiesis
Lymphadenopathy,Lymphadenopathy, HepatosplenomegalyHepatosplenomegaly (50-60%)(50-60%)
CLL - Clinical courseCLL - Clinical course
Initially:Initially: asymptomatic asymptomatic
Advanced disease:Advanced disease:
•• bacterial infections, bacterial infections, hemorrhagehemorrhage
Prognostic factors:Prognostic factors:
•• extent of tumor burdenextent of tumor burden
•• pattern of marrow infiltrationpattern of marrow infiltration
•• chromosomal abnormalitieschromosomal abnormalities
Median survival:Median survival: ~ 6 years~ 6 years

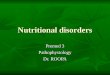
Smudge cells - CLLSmudge cells - CLL

CLLCLL
One more peripheral blood findings One more peripheral blood findings
in CLL is Presence of in CLL is Presence of Smudge Smudge cellscells
( parachute cells). ( parachute cells). Along with increased number of Along with increased number of
normal appearing lymphocytes.normal appearing lymphocytes.

8/12/2009 35
Chronic Myelogenous Leukemia Chronic Myelogenous Leukemia (CML)(CML)
Excessive development of mature Excessive development of mature neoplastic granulocytes in the bone neoplastic granulocytes in the bone marrowmarrow Move into the peripheral blood in Move into the peripheral blood in
massive numbersmassive numbers Ultimately infiltrate the liver and spleen Ultimately infiltrate the liver and spleen
8/12/2009 36
Chronic Myelogenous LeukemiaChronic Myelogenous Leukemia
Philadelphia chromosomePhiladelphia chromosome 9 and 22 translocation almost specific 9 and 22 translocation almost specific
to CMLto CML Produces BCR/c-abl fusion oncogeneProduces BCR/c-abl fusion oncogene
The chromosome abnormality that causes The chromosome abnormality that causes chronic myeloid leukemia (CML) (9 &22)chronic myeloid leukemia (CML) (9 &22)
Genetic markerGenetic marker Chronic, stable phase followed by Chronic, stable phase followed by
acute, aggressive (blastic) phaseacute, aggressive (blastic) phase

i.e – mainly uncontrolled proliferation i.e – mainly uncontrolled proliferation of myeloid cells.of myeloid cells.
Males more than femalesMales more than females
Splenomegaly – sometimes massive.. Splenomegaly – sometimes massive..


**Philadelphia chromosome****Philadelphia chromosome** Hybrid chromosome with Hybrid chromosome with
translocation between the long arm translocation between the long arm of chr. 9 and long arm of chr.22 . --- of chr. 9 and long arm of chr.22 . --- t(9:22).t(9:22).
May be present in granulocyte, RBC May be present in granulocyte, RBC or platelet precursors in more than or platelet precursors in more than 95% of CML..95% of CML..

CML - PathologyCML - PathologyBone marrow:Bone marrow:
• • Hypercellular / predominant Hypercellular / predominant granulocytic hyperplasiagranulocytic hyperplasia
• • Increased megakaryocytes (small forms)Increased megakaryocytes (small forms)
• • Normal to decreased erythroid precursorsNormal to decreased erythroid precursors
Peripheral blood:Peripheral blood:
• • GranulocytosisGranulocytosis (>25,000/cmm), with (>25,000/cmm), with immature cells,immature cells,
• • Basophilia,Basophilia, eosinophilia, eosinophilia,
Extramedullary hemopoiesis:Extramedullary hemopoiesis: Spleen, Spleen, liver, lymph nodes liver, lymph nodes

CML - Clinical FeaturesCML - Clinical Features
15 - 20% of all leukemias; age 25-6015 - 20% of all leukemias; age 25-60
Symptoms:Symptoms:
- non-specific- non-specific
- related to hypermetabolism (high cell turnover)- related to hypermetabolism (high cell turnover)
- related to splenomegaly- related to splenomegaly
Course:Course:
- chronic phase (mean survival, 3-4y)- chronic phase (mean survival, 3-4y)
- accelerated phase- accelerated phase
- blast crisis / - blast crisis / myeloid or lymphoidmyeloid or lymphoid (survival, < (survival, < 1y)1y)
Therapy:Therapy: chemotherapy; chemotherapy; BMTBMT

Hodgkin’s lymphomaHodgkin’s lymphoma
a lymphoid neoplastic disorder of B cell a lymphoid neoplastic disorder of B cell originorigin
A disease marked by chronic enlargement A disease marked by chronic enlargement of the lymph nodes, often local at the of the lymph nodes, often local at the onset and later generalized.onset and later generalized.
characterized by the presence of Reed-characterized by the presence of Reed-Sternberg cells (or variants of RS cells) in Sternberg cells (or variants of RS cells) in the affected tissuesthe affected tissues
Enlargement of the spleen and often of Enlargement of the spleen and often of the liver is also present.the liver is also present.
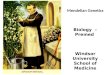
Reed-Sternberg cellsReed-Sternberg cells Considered to be a malignant Considered to be a malignant
neoplasm of lymphoid cells of neoplasm of lymphoid cells of uncertain origin. uncertain origin.
Owl – Eye appearanceOwl – Eye appearance
These cells have mirror-image nuclei.These cells have mirror-image nuclei.
Young adults and elderlyYoung adults and elderly


Signs & SymptomsSigns & Symptoms
Enlarged painless nodes – mostly neck Enlarged painless nodes – mostly neck & axilla& axilla
Fever, wt.loss, pruritis & night sweats.Fever, wt.loss, pruritis & night sweats. Pel – Ebstein Fever – fever alternating Pel – Ebstein Fever – fever alternating
with long periods (15-28days).with long periods (15-28days). AnemiaAnemia CachexiaCachexia HepatosplenomegalyHepatosplenomegaly
Hodgkin’s disease: SummaryHodgkin’s disease: Summary
a lymphoid neoplasm of B cell origina lymphoid neoplasm of B cell origin characterized histologically by Reed characterized histologically by Reed
Sternberg cells (or variants)Sternberg cells (or variants) commonly presents with commonly presents with
lymphadenopathy or mediastinal mass lymphadenopathy or mediastinal mass in young adultsin young adults
treatment modality depends on stagetreatment modality depends on stage curable in mostcurable in most
Non Hodgkin's LymphomaNon Hodgkin's Lymphoma
These include all lymphomas without These include all lymphomas without Reed-Sternberg cells.Reed-Sternberg cells.
Most are B-cell proliferationsMost are B-cell proliferations Extra nodal involvement is there.. Extra nodal involvement is there..

Signs & SymptomsSigns & Symptoms
Often symptomlessOften symptomless Lymphadenopathy, wt.loss..Lymphadenopathy, wt.loss.. Extra nodal spread – skin, bone, gut, Extra nodal spread – skin, bone, gut,
CNS, lung..CNS, lung.. Pancytopenia may be therePancytopenia may be there Infections are very common.Infections are very common. Fatigue, unexplained fever, sweatsFatigue, unexplained fever, sweats Enlarged Tonsils and adenoidsEnlarged Tonsils and adenoids

FOLLICULAR LYMPHOMAFOLLICULAR LYMPHOMA
Follicular lymphoma’s – most common in USFollicular lymphoma’s – most common in US Derived from B lymphocytesDerived from B lymphocytes t (14:18)t (14:18) Affects middle ageAffects middle age Not very aggressive – mean survival 7-10 Not very aggressive – mean survival 7-10
yrsyrs Rarely they may transform in to aggressive Rarely they may transform in to aggressive
type of lymphomastype of lymphomas

Burkitt’s LymphomaBurkitt’s Lymphoma A Lymphoblastic lymphoma mainly in A Lymphoblastic lymphoma mainly in
African children.African children. Mostly associated with EBV infection.Mostly associated with EBV infection. Involves facial bones ( Jaw), ovaries, and Involves facial bones ( Jaw), ovaries, and
abdominal lymph nodes.abdominal lymph nodes. Undifferentiated stem cells with scattered Undifferentiated stem cells with scattered
pale macrophages containing nuclear debris. pale macrophages containing nuclear debris. Isolated histiocytes on background of Isolated histiocytes on background of
abnormal lymphoblasts (STARRY SKY abnormal lymphoblasts (STARRY SKY APPERANCE)APPERANCE)
t (8:14)t (8:14) High incidence in AIDS pt’s High incidence in AIDS pt’s



Burkitts lymphomaBurkitts lymphoma