Embed Size (px)
Citation preview

Diseases of the Abdomen and PelvisDiagnostic Imaging and Interventional Techniques

J. Hodler • G.K. von Schulthess • Ch.L. Zollikofer (Eds)
DISEASES OF THE ABDOMENAND PELVIS
DIAGNOSTIC IMAGING AND INTERVENTIONALTECHNIQUES
38th International Diagnostic Coursein Davos (IDKD)Davos, April 1-7, 2006
including thePediatric Satellite Course ‘Kangaroo’Davos, April 1-2, 2006
presented by the Foundation for the Advancement of Education in Medical Radiology, Zurich

J. HODLER G. K. VON SCHULTHESS
Department of Radiology UniversitätsspitalUniversity Hospital Balgrist NuklearmedizinZurich, Switzerland Zurich, Switzerland
CH. L. ZOLLIKOFER
KantonsspitalInstitut für RadiologieWinterthur, Switzerland
Library of Congress Control Number: 2006922660
ISBN-10 88-470-0470-5 Springer Milan Berlin Heidelberg New YorkISBN-13 978-470-0470-2 Springer Milan Berlin Heidelberg New York
This work is subject to copyright. All rights are reserved, whether the whole or part of the material isconcerned, specifically the rights of translation, reprinting, re-use of illustrations, recitation,broadcasting, reproduction on microfilms or in other ways, and storage in data banks. Duplication ofthis publication or parts thereof is only permitted under the provisions of the Italian Copyright Lawin its current version, and permission for use must always be obtained from Springer. Violations areliable for prosecution under the Italian Copyright Law.
Springer is a part of Springer Science+Business Media
springer.com
© Springer-Verlag Italia 2006
The use of general descriptive names, registered names, trademarks, etc., in this publication does notimply, even in the absence of a specific statement, that such names are exempt from the relevantprotective laws and regulations and therefore free for general use.
Product liability: The publisher cannot guarantee the accuracy of any information about dosage andapplication contained in this book. In every individual case the user must check such information byconsulting the relevant literature.
Cover design: Simona Colombo, Milan, ItalyTypesetting: C & G, Cremona, ItalyPrinting and binding: Grafiche Porpora, Cernusco sul Naviglio (Mi), Italy
Printed in Italy

Preface
The International Diagnostic Course in Davos (IDKD) offers a unique learningexperience for imaging specialists in training as well as for experienced radiolo-gists and clinicians wishing to be updated on the current state of the art and thelatest developments in the fields of imaging and image-guided interventions.
This annual course is focused on organ systems and diseases rather than onmodalities. This year’s program deals with diseases of the abdomen and pelvis.During the course, the topics are discussed in group seminars and in plenary ses-sions with lectures by world-renowned experts and teachers. While the seminarspresent state-of-the-art summaries, the lectures are oriented towards future devel-opments.
Accordingly, this Syllabus represents a condensed version of the contents pre-sented under the 20 topics dealing with imaging and interventional therapies in ab-dominal and pelvic diseases. The topics encompass all the relevant imaging modal-ities including conventional X-rays, computed tomography, nuclear medicine, ul-trasound and magnetic resonance angiography, as well as image-guidedinterventional techniques.
The Syllabus is designed to be an ‘aide-mémoire’ for the course participants sothat they can fully concentrate on the lecture and participate in the discussionswithout the need of taking notes.
Additional information can be found on the IDKD website: www.idkd.ch
J. HodlerG.K. von Schulthess
Ch.L. Zollikofer
IDKD 2006

Table of Contents
Seminars
Emergency Radiology of the Abdomen: The Acute AbdomenB. Marincek, J.P. Heiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Trauma of the Abdomen and Pelvis IP.J. Kenney . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Trauma of the Abdomen and Pelvis IIS. Ledbetter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Variants and Pitfalls in Body Imaging. Abdomen and PelvisA. Shirkhoda, K. Mortele . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
An Approach to Imaging the Acute Abdomen in PediatricsA. Daneman, U. Willi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Impairments of Swallowing: Diagnosis by CineradiographyW. Brühlmann . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
Diseases of the EsophagusM.S. Levine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Diseases of the Stomach and Duodenum: Basics of Radiologic-Pathologic CorrelationJ.E. Lichtenstein, F.J. Scholz . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Small Bowel ImagingN. Gourtsoyiannis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Essentials and Clinical Applications of CT EnteroclysisD.D. Maglinte . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Imaging of the Colon and Rectum: Inflammatory and Neoplastic DiseasesR.M. Gore, J. Stoker . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
CT ColonographyM. Macari, C.D. Johnson . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
Imaging of Liver DiseasesE. Rummeny, R. Baron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
Diseases of the Pancreas, Part I: PancreatitisT. Helmberger . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
IDKD 2006

Diseases of the Pancreas, Part II: TumorsR.F. Thoeni . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
Imaging of Diseases of the Bile Ducts and Gallbladder C.D. Becker . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 112
Differential Diagnosis of Diseases of the Gallbladder and Bile DuctsA.D. Levy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
Imaging the Adrenal GlandsR.H. Reznek, G.P. Krestin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122
Radiologic Approach to Solid and Cystic Renal MassesS.G. Silverman, D.S. Hartman . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127
Urinary Tract Obstruction and InfectionR.J. Zagoria, J.R. Fielding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 132
Diseases of the Female Genital Tract IS.M. Ascher . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 136
Diseases of the Female Genital Tract IIR.A. Kubik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
Imaging of the Male PelvisJ.O. Barentsz, B.J. Wagner, E. Abouh-Bieh . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
Spread of Metastatic Disease in the AbdomenJ.A. Brink, T. Hany . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 174
Abdominal Vascular MRAT.M. Grist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181
Abdominal Vascular Imaging Including Mesenteric IschemiaM. Prokop . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
Abdominal InterventionsJ. Lammer, D. Vorwerk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 195
Pediatric Satellite Course “Kangaroo”
The Fetal Abdomen: From Normal to Abnormal. From Ultrasound to MR ImagingF.E. Avni, M. Cassart, A. Massez . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 207
Genitourinary Sonography in the ChildI. Gassner, T.E. Geley . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 211
Intussusception: An Approach to ManagementA. Daneman . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218
Imaging the Child with an Abdominal MassU.V. Willi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 224
VIII Table of Contents

List of Contributors
Abouh-Bieh E., 153Ascher S.M., 136Avni F.E., 207Barentsz J.O., 153Baron R., 90Becker C.D., 112Brink J.A., 174Brühlmann W., 40Cassart M., 207Daneman A., 33, 218Fielding J.R., 132Gassner I., 211Geley T.E., 211Gore R.M., 74Gourtsoyiannis N., 60Grist T.M., 181Hany T., 174Hartman D.S., 127Heiken J.P., 3Helmberger T., 98Johnson C.D., 84Kenney P.J., 10Krestin G.P., 122
IDKD 2006
Kubik R.A., 146Lammer J., 195Ledbetter S., 17Levine M.S., 45Levy A.D., 118Lichtenstein J.E., 52Macari M., 84Maglinte D.D., 66Marincek B., 3Massez A., 207Mortele K., 26Prokop M., 188Reznek R.H., 122Rummeny E., 90Scholz F.J., 52Shirkhoda A., 26Silverman S.G., 127Stoker J., 74Thoeni R.F., 106Vorwerk D., 195Wagner B.J., 153Willi U.V., 33, 224Zagoria R.J., 132

SEMINARS

Introduction
The term ‘acute abdomen’ defines a clinical syndromecharacterized by a history of hitherto undiagnosed ab-dominal pain lasting less than one week. A large numberof disorders, ranging from benign, self-limited diseasesto conditions that require immediate surgery, can causeacute abdominal pain. Eight conditions account for over90% of patients who are referred to hospital and are seenon surgical wards with acute abdominal pain: acute ap-pendicitis, acute cholecystitis, small bowel obstruction,urinary colic, perforated peptic ulcer, acute pancreatitis,acute diverticular disease, and non-specific, non-surgicalabdominal pain (‘dyspepsia’, ‘constipation’).
Imaging Techniques
Clinical assessment of acute abdomen is often difficultbecause of the often non-specific findings of physical ex-amination and laboratory investigations. In many centersplain radiographs of the abdomen, despite significant di-agnostic limitations, serve as the initial radiological ap-proach. Two views are usually taken, one supine and oneerect. If the patient is unable to stand, a left lateral decu-bitus view is performed. For a systematic film analysis itis helpful to follow the mnemonic ‘gas, mass, stones andbones’ for the detection of (1) signs of mechanical bow-el obstruction or paralytic ileus; (2) gas outside the bow-el lumen in the peritoneal cavity (pneumoperitoneum),retroperitoneum, bowel wall, portal veins, or biliary tract;(3) mass or fluid collections, displacement of organs orbowel loops; (4) abnormal calcifications and/or calculi;(5) skeletal pathology.
The need for plain abdominal radiographs has de-clined due to the impact of cross-sectional imaging.The traditional indications for plain abdominal radiog-raphy – pneumoperitoneum, bowel obstruction, and thesearch for ureteral calculi – are better evaluated by un-enhanced helical computed tomography (CT). A num-ber of authors have shown that CT is clearly superior toplain radiography for diagnosing pneumoperitoneum,detecting a bowel obstruction, and for identifying
ureteral calculi. The major obstacles to replacing plainabdominal radiography with unenhanced CT are itshigher cost, more limited availability, and higher radia-tion dose.
Although ultrasonography (US) has gained wide-spread acceptance for evaluating the gallbladder in af-fected patients and the pelvis in children and women ofreproductive age, CT is considered to be one of the mostvalued tools for triaging patients with acute abdominalpain. This is because it can provide a global perspectiveof the gastrointestinal (GI) tract, mesenteries, peri-toneum, and retroperitoneum, inhibited by the presenceof bowel gas and fat. Over recent years, most emergencycenters have been equipped with newer helical CT scan-ners that permit imaging procedures to be performed inless time, with greater accuracy, and with less patientdiscomfort. The introduction of multidetector CT (MD-CT) technology, with advances in contrast dynamics andhigh-resolution volumetric data acqusition, has furtherenhanced the utility of CT in abdominal imaging. Imageinterpretation with helical CT and particularly with MD-CT is primarily performed at a workstation by manuallypaging or continuously scrolling up and down throughthe stack of reconstructed images. Additionally, multi-planar reformation (MPR) using coronal, sagittal, andcurved planes, has evolved as a routine supplement tothe axial images.
Three-dimensional volume rendered and maximumintensity projection (MIP) images are also easily pro-duced from MDCT data sets. Inquiry about the site ofabdominal pain facilitates the choice of imaging tech-nique. For practical reasons, it is helpful to discuss theimaging strategies for acute pain localized in an ab-dominal quadrant separately from acute abdomen withdiffuse pain and acute abdomen with flank or epigastricpain.
Acute Pain in an Abdominal Quadrant
Acute abdomen with pain localized in an abdominalquadrant can be classified as pain in the right upper, leftupper, right lower, and left lower abdominal quadrant.
IDKD 2006
Emergency Radiology of the Abdomen: The Acute Abdomen
B. Marincek1, J.P. Heiken2
1 Institute of Diagnostic Radiology, University Hospital Zurich, Zurich, Switzerland2 Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO, USA

Right Upper Quadrant
Acute cholecystitis is by far the most common disease inthe right upper quadrant. Other important diseases thatresemble acute cholecystitis are pyogenic or amebic liverabscess, spontaneous rupture of a hepatic neoplasm (usu-ally hepatocellular adenoma or carcinoma), hepatitis, andmyocardial infarction.
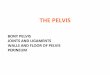
US is the preferred imaging method for evaluating pa-tients with acute right upper abdominal pain. It is a reliabletechnique for establishing the diagnosis of acute calculouscholecystitis. The primary criterion is the detection of gall-stones. Secondary signs include the sonographic Murphysign, gallbladder wall thickening by 3 mm or more, andpericholecystic fluid. Typically, a calculus obstructs thecystic duct in acute calculous cholecystitis. The trappedconcentrated bile irritates the gallbladder wall, causing in-creased secretion, which in turn leads to distension andedema of the wall. Rising intraluminal pressure compress-es the vessels, resulting in thrombosis, ischemia, and sub-sequent necrosis and perforation of the wall. Gallbladderperforation and complicating pericholecystic abscessestypically occur adjacent to the gallbladder fundus becauseof the sparse blood supply. CT may be useful for confir-mation of the sonographic diagnosis. Emphysematouscholecystitis is a rare complication of acute cholecystitisand is associated with diabetes mellitus. US or CT demon-stratation of gas in the wall and/or lumen of the gallblad-der imply underlying gangrenous changes (Fig. 1).Acalculous acute cholecystitis accounts for approximatelyonly 5% of cases of acute cholecystitis. It is especiallycommon in intensive care unit patients. Prolonged bile sta-sis results in increased viscosity of the bile that ultimatelyleads to functional cystic duct obstruction.
US and CT are both accurate techniques for diagnos-ing liver abscesses. US usually reveals a round or oval hy-poechoic mass with low-level internal echoes. Althoughthe lesion may mimic a solid hepatic mass, the presenceof through transmission is a clue to its cystic nature.Normally, pyogenic liver abscesses are the result of seed-ing from appendicitis or diverticulitis, or direct extensionfrom cholecystitis or cholangitis. Amebic abscesses resultfrom primary colonic involvement with seeding throughthe portal vein. In most cases, pyogenic and amebic ab-scesses are indistinguishable by US appearance. The CTappearances of pyogenic and amebic abscesses also showsubstantial overlap. Amebic abscesses are low attenuationcystic masses. An enhancing wall and a peripheral zoneof edema surrounding the abscess are common but notuniversally present. Extrahepatic extension of the amebicabscess with involvement of chest wall, pleura, or adja-cent viscera is a frequent finding. Whereas amebic ab-scesses are usually solitary and unilocular, pyogenic ab-scesses may be multiple or multiloculated and maydemonstrate an irregular contour.
Spontaneous rupture of a hepatocellular carcinomaand subsequent hemoperitoneum represent a frequentcomplication found in countries with a high incidence of
4
this tumor, but uncommon in Western countries.Subcapsular localization and tumor necrosis have beenimplicated in pathogenesis. US, and especially CT, arethe most useful techniques for diagnosing a ruptured he-
B. Marincek, J.P. Heiken
a
b
Fig. 1. A 74-year-old man with known diabetes mellitus presents withacute abdominal pain in the right upper quadrant. a Plain abdominalradiograph shows a fluid-gas level in the distended gallbladder andgas in the gallbladder wall (open arrow). b MDCT depicts the dilat-ed gallbladder with intramural gas (open arrow), indicative of em-physematous cholecystitis. In addition, extraluminal/extramural gasis present due to walled-off gallbladder perforation (arrow).Hydronephrosis and parenchymal atrophy of the left kidney

patocellular carcinoma, which appears as a peripheral orsubcapsular mass. Spontaneous hemorrhage within a he-patocellular adenoma occurs most commonly in womentaking oral contraceptives. Capsular rupture with subse-quent hemoperitoneum is an uncommon complication.On CT, high-density intraperitoneal fluid confirms the di-agnosis of hemoperitoneum, and extravasation of contrastmaterial is indicative of active bleeding.
Left Upper Quadrant
Acute abdomen with left upper quadrant pain is not fre-quent. Splenic infarction, splenic abscess, gastritis, andgastric or duodenal ulcer are the most important causes.US is usually used for screening, and CT enables accuratefurther evaluation. The diagnosis of gastric pathology is es-tablished by endoscopy, with imaging playing a minor role.
Common causes of splenic infarction include bacteri-al endocarditis, portal hypertension, and underlyingsplenomegaly. Pancreatitis that extends into the splenichilum can also result in infarction. Splenic infarction maybe focal or global. Typical focal splenic infarcts appear asperipheral wedge-shaped defects, hypoechoic at US andhypodense at CT, respectively. Most splenic abscesses areassociated with hematogenous dissemination of infec-tion, such as bacterial endocarditis or tuberculosis.Intravenous drug abusers are predominantly affected.Both US and CT are sensitive, but specificity is low. OnUS, most abscesses appear as hypo- or anechoic, poorlydefined lesions; on CT, they typically appear as rounded,low-density lesions with rim enhancement.
Right Lower Quadrant
Acute appendicitis is not only the most frequent cause ofacute right lower quadrant pain, but also the most com-monly encountered cause of acute abdomen. Other diseasesmanifesting acute right lower quadrant pain include acuteterminal ileitis (Crohn’s disease), acute typhlitis, right sidedcolonic diverticulitis and, in women, pelvic inflammatorydisease, complications of ovarian cyst (hemorrhage, torsionand leak), endometriosis, or ectopic pregnancy.
Most patients with typical clinical findings of acute ap-pendicitis undergo immediate surgery without preoperativeimaging. Since diagnosis is uncertain in up to one third ofpatients because of atypical symptoms, many centers todayrequest appendiceal imaging for clinically equivocal pa-tients. Although plain radiography continues to play a rolein evaluating patients with acute right lower quadrant pain,its role is quite limited. Less than 50% of patients with ap-pendicitis show an abnormality on plain radiographs. Themost specific finding is the presence of an appendicolith,which is usually calcified, solitary, and rounded.
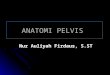
US has become an important imaging option in the eval-uation of suspected acute appendicitis, particularly in chil-dren, pregnant women, and women of reproductive age.The prime sonographic criterion is the demonstration of aswollen, non-compressible appendix greater than 7 mm in
diameter with a target configuration (Fig. 2). Generally, thenormal appendix cannot be defined with US, thus, clear vi-sualization of the appendix is suggestive of inflammation.
Advantages of US include lack of ionizing radiation,relatively low cost, and widespread availability. On theother hand, US requires considerable skill and is difficultto perform in obese patients, patients with severe pain,and patients likely to have a complicating periappen-diceal abscess. When the sonographic findings are un-clear, CT can provide a rapid and definitive diagnosis.
Emergency Radiology of the Abdomen: The Acute Abdomen 5
a
b
Fig. 2. A 25-year-old man presented with acute abdominal pain inthe right lower abdominal quadrant. Physical examination and lab-oratory tests revealing elevated white blood cell counts, raised thesuspicion of acute appendicitis. Longitudinal (a) and perpendicu-lar (b) graded compression US shows an enlarged appendix (cur-sors, diameter > 10 mm) with edematous thickening of the appen-dical wall, confirming the diagnosis of acute appendicitis

CT has emerged in many centers as the primary imagingmodality for patients with suspected acute appendicitisdue to its exceptional accuracy. In the case of mild dis-ease, the findings include a dilated, fluid-filled appendixwith a calcified appendicolith or inflammatory changesof the mesenteric fat (Fig. 3). An inflammatory mass oran abscess may develop with disease progression andperforation.
Diverticulitis rarely manifests itself as a right-sidedcondition. Right-sided colonic diverticula are often con-genital, solitary and true diverticula, unlike sigmoid di-verticula. The normal appendix should be visible in right-sided diverticulitis. If the appendix cannot be identified,right-sided omental infarction or epiploic appendagitismust be considered in the differential diagnosis.
Left Lower Quadrant
Diverticulitis is the most common cause of acute abdom-inal pain in the left lower quadrant. Diverticulitis occursin up to 25% of patients with known diverticulosis andtypically involves the sigmoid colon. CT has replacedbarium enema examinations because it is very sensitiveand approaches 100% specificity and accuracy in the di-agnosis or exclusion of diverticulitis. CT is also very use-ful in establishing the presence of pericolic complicationsand differentiating sigmoid diverticulitis from carcinoma– a major differential diagnostic consideration.
Superimposed on diverticulosis, the CT diagnosis ofacute diverticulitis is based on the identification of seg-mental colonic wall thickening and pericolic inflammato-ry changes, such as fat stranding, inflammatory mass, gasbubbles, abscess, or free fluid (Fig. 4). Occasionally, pa-tients with diverticulitis may manifest pneumaturia be-cause of a complicating enterovesical fistula.
6
Acute Abdomen with Diffuse Pain
Any disorder that irritates a large portion of the GI tractand/or the peritoneum will cause diffuse abdominal pain.The most common disorder is gastroenterocolitis. Otherimportant disorders are bowel obstruction, ischemic bow-el disease, and GI tract perforation.
Bowel Obstruction
Bowel obstruction is a frequent cause of abdominal painand accounts for approximately 20% of surgical admis-sions for acute abdominal conditions. The small bowel isinvolved in 60-80% of cases. Frequent causes of smallbowel obstruction are adhesions resulting from priorsurgery, hernias, and neoplasms. In the large bowel, me-chanical obstruction is commonly due to diverticular dis-ease or colorectal carcinoma. 5-10% of cases of largebowel obstruction are caused by volvulus, which is mostcommonly in the sigmoid, followed by the cecum.
The diagnosis of bowel obstruction is established onclinical grounds and usually confirmed with plain abdom-inal radiographs. Because of the diagnostic limitations ofplain films, CT is increasingly used to establish the diag-nosis, identify the site, level, and cause of obstruction anddetermine the presence or absence of associated bowel is-chemia. CT can be useful for differentiating between sim-ple and closed loop obstruction. Closed loop obstruction isa form of mechanical bowel obstruction in which twopoints along the course of the bowel are obstructed at asingle site. It is usually secondary to an adhesive band ora hernia. A closed loop tends to involve the mesentery andis prone to produce a volvulus, thus representing the most
B. Marincek, J.P. Heiken
b
Fig. 3. 45-year-old man with elevated white blood cells and acute painin the right lower abdominal quadrant. US examination was unableto identify the appendix. a Sagittal MDCT depicts marked enlarge-
ment of the retrocecal appendix(arrow in a and b), with wallthickening, mural enhancement,and adjacent fat stranding. bTransverse MDCT shows twoappendicoliths within the appen-dical lumen. The US-diagnosisof acute appendicitis is difficultto establish in a retrocecal ap-pendix
Fig. 4. 55-year-old man with known diverticular disease and acuteabdominal pain in the left lower quadrant. MDCT shows a nar-rowed segment of the sigmoid colon with wall thickening, pericol-ic inflammatory changes, and an adjacent fluid-collection withmarked peripheral enhancement (arrow), indicating an abscess af-ter walled-off perforation in acute diverticulitis
a

common cause of strangulation. However, only volvulus ofthe large bowel is associated with classic features on plainabdominal radiographs. The sigmoid volvulus produces adistended loop, with the twisted mesenteric root pointingto the origin of the volvulus, i.e., to the sigmoid.
CT is particularly reliable in higher grades of bowelobstruction. It has proved useful for characterizing bow-el obstruction from various causes, including adhesions,hernia, neoplasm, extrinsic compression, inflammatorybowel disease, radiation enteropathy, intussusception,gallstone ileus, or volvulus. The essential CT finding ofbowel obstruction is the delineation of a transition zonebetween the dilated and decompressed bowel. Careful in-spection of the transition zone and luminal contents usu-ally reveals the underlying cause of obstruction.However, the presumed point of transition from dilatedto non-dilated bowel can be difficult to determine in theaxial plane. MDCT facilitates this task by providing theradiologist with a volumetric data set that can be viewedin the axial, sagittal, or coronal plane or any combina-tion of the three. These MPR views centered on the an-ticipated transition point help to determine the site, lev-el, and cause of obstruction.
Mechanical obstruction has to be differentiated fromparalytic ileus. Numerous causes exist for both diffuseand localized paralytic ileus. Paralytic ileus is a commonproblem after abdominal surgery. It may be secondary toischemic conditions, inflammatory or infectious disease,abnormal electrolyte, metabolite, drug or hormonal lev-els, or innervation defects. A massively dilated colon witha thickened wall (‘thumbprinting’) caused by wall edemaand inflammation is seen with toxic megacolon inpseudomembranous colitis. Toxic megacolon is the radi-ological manifestation of a paralytic ileus.
Ischemic Bowel Disease
Arterial or venous occlusion or thrombosis and hypoper-fusion are predominant causes of bowel ischemia. Usually,a combination of these factors is observed. The predomi-nance of one factor determines the outcome and the find-ings on CT. Diminished bowel wall enhancement is theonly direct sign of vascular impairment of the bowel andhas been reported in predominantly arterial disease, suchas infarction, as well as in predominantly venous diseases,such as strangulation. Other CT findings are direct visu-alization of the thrombus in the superior mesenteric arteryor vein. Bowel distention and bowel wall edema are non-specific findings and can be seen with inflammatory orinfectious causes. Bowel distention reflects the interrup-tion of peristaltic activity in ischemic segments.
In closed loop bowel obstruction the closed loop canbecome strangulated, i.e., ischemic, although the pro-gression of a closed loop obstruction to a strangulatedone is not inevitable. The reported prevalence of strangu-lating obstruction ranges from 5-40%. Strangulation is apredominantly venous disease. The most frequent abnor-mality seen on CT is bowel wall thickening. The thick-ened bowel wall is sometimes associated with the targetsign, alternating layers of high and low attenuation with-in the thickened bowel wall, which results from submu-cosal edema and hemorrhage. The bowel segment proxi-mal to an obstruction can become ischemic due to severebowel distention. CT findings that suggest subsequent in-farction include non-enhancement of the bowel wall, gasin the bowel wall, mesenteric or portal veins, edema/he-morrhage in the mesentery adjacent to thickened and/ordilated bowel loops, and ascites (Fig. 5).
Emergency Radiology of the Abdomen: The Acute Abdomen 7
a b
Fig. 5. 76-year-old man with acute diffuse abdominal pain and with a history of abdominal surgery performed five weeks previously. aTransverse MDCT demonstrates mesenteric edema and infarction of the distal ileum (arrowhead) with intramural gas. b Transverse MD-CT at a level below depicts thickening of the bowel wall with irregular mucosal enhancement (arrow) indicative of bowel ischemia.Intraoperatively, a strangulating small bowel volvulus secondary to adhesion of the distal ileum was identified

GI Tract Perforation
Pneumoperitoneum usually starts with localized pain andculminates in diffuse pain after peritonitis has developed.It may result from a variety of causes. Gastroduodenalperforation associated with peptic ulcer or necrotic neo-plasm has become less frequent in the last few decadesdue to earlier diagnosis and improved therapy. At thesame time, the incidence of gastroduodenal perforationsresulting from endoscopic instrumentation has increased.Perforation of the small bowel is relatively uncommon.Spontaneous rupture of the large bowel is more frequentand can occur in a markedly dilated colon proximal to anobstructing lesion (tumor, volvulus) or when the bowelwall is friable (ischemic or ulcerative colitis, necroticneoplasm). Over the last decades, fiberoptic endoscopyhas been increasingly performed for evaluation and biop-sy of colorectal lesions, as well as for polypectomy; theseprocedures cause perforation in 0.5-3% of patients.
Pneumoperitoneum can be recognized by the presence ofsubdiaphragmatic gas on an erect chest radiograph or anerect or left lateral decubitus radiograph of the abdomen.An abundant pneumoperitoneum is indicative of a perfora-tion complicating large bowel obstruction, and moderatequantities of free gas are seen in the perforation of the stom-ach. Only small quantities of gas escape with perforation ofthe small bowel, because the small bowel does not usuallycontain gas. Detection of subtle pneumoperitoneum is oftendifficult. CT is far more sensitive than conventional radi-ography for the detection of a small pneumoperitoneum,and it has thus become the modality of choice in cases thatare unclear on a conventional radiograph. To enhance thesensitivity of CT for extraluminal gas, the images are alsoviewed at ‘lung window’ settings. On CT, small amounts ofgas around the stomach and the liver are seen mainly aftergastroduodenal or small bowel perforation.
Retroperitoneal perforations (duodenal loop beyondthe bulbar segment, appendix, posterior aspect of as-cending and descending colon, rectum below the peri-toneal reflection) tend to be contained locally and remainclinically silent for several hours or days. Retroperitonealgas has a mottled appearance and may extend along thepsoas muscles. In contrast to intraperitoneal gas,retroperitoneal gas does not move freely when the pa-tient’s position is changed from supine to upright forplain abdominal radiographs.
Acute Abdomen with Flank or Epigastric Pain
Acute flank or epigastric pain is commonly a manifestationof retroperitoneal pathology, especially urinary colic, acutepancreatitis, or leaking abdominal aortic aneurysm.
Urinary Colic
For several decades, intravenous urography has been theprimary imaging technique used in patients with flank
8
pain thought to be caused by urinary colic. Abdominal ra-diograph and US are considered useful for those patientswith contraindications to irradiation or contrast media.However, because of the low sensitivity of abdominal ra-diographs and US for urinary tract calculi, the role of un-enhanced CT has grown rapidly. On CT, virtually allureteral stones are radiopaque, regardless of their chemi-cal composition. Uric acid stones have attenuation valuesof 300-500 Hounsfield units (HU), and calcium-basedstones have attenuation values > 1,000 HU. In addition tothe direct demonstration of a ureteral stone, secondarysigns of ureterolithiasis may be seen, including hy-droureter, hydronephrosis, perinephric stranding, and re-nal enlargement (Fig. 6). Perinephric stranding and ede-ma result from reabsorbed urine infiltrating the per-inephric space along the bridging septa of Kunin. Themore extensive the perinephric edema as shown on unen-hanced CT, the higher the degree of urinary tract ob-struction. Focal periureteral stranding resulting from lo-cal inflammatory reaction or irritation and induced by thepassage of a stone helps localize subtle calculi. MDCT is
B. Marincek, J.P. Heiken
a
bFig. 6. 46-year-oldman with right-sided flank pain.Coronal MDCT re-construction (a) andtransverse MDCTafter intravenouscontrast administra-tion (b) demonstratean obstructing stoneat the uretero-pelvicjunction (arrow)with dilatation ofthe renal pelvis andof the calices

favored over single-detector CT because it provides coro-nal MPRs, which often portray the urinary tract more ef-fectively than axial images.
When no stone is detected, a search for an alternativediagnosis should be performed. Non-calculus urinarytract abnormalities causing symptoms of colic includeacute pyelonephritis, renal cell carcinoma, acute renalvein thrombosis and renal infarction. Extraurinary dis-eases, such as appendicitis, diverticultis, small bowel ob-struction, pancreatitis, and retroperitoneal hemorrhagemay also simulate acute urinary colic. Occasionally, re-peating the CT examination with intravenous, oral, orrectally administered contrast material may be required.
Acute Pancreatitis
Acute pancreatitis is an important disease causing epi-gastric pain. US is helpful for the demonstration of gall-stones as a cause of acute pancreatitis and for the follow-up of known fluid collections. CT has become the imag-ing modality of choice to stage the extent of disease andto detect complications because CT findings correlatewell with the clinical severity of acute pancreatitis.Pancreatic enlargement due to interstitial parenchymaledema may progress to pancreatic exudate collecting inthe anterior pararenal space, the transverse mesocolon,the mesenteric root, and the lesser sac. The pancreaticparenchyma may undergo necrosis or hemorrhage.Severe pancreatitis is often complicated by thrombosis ofthe splenic and portal vein.
Acute pancreatic and peripancreatic fluid collectionsmay evolve into pseudocysts. Pseudocysts exhibit de-fined capsules. A pseudocyst can erode peripancreaticvessels, resulting in bleeding or formation of a pseudoa-neurysm. Larger aneurysms can be diagnosed by CT orsonographically with Doppler; angiography may be nec-essary to diagnose small pseudoaneurysms (< 1 cm).
Leaking Aneurysm of Abdominal Aorta or Iliac Artery
One of the most life-threatening alternative diagnoses inacute flank pain is a leaking aneurysm of the abdominalaorta or iliac artery. When a patient with suspected rup-ture of an abdominal aortic aneurysm is hemodynami-cally unstable, US is the initial imaging technique used.The examination can be performed rapidly usingportable equipment in the emergency room. However,the diagnosis of para-aortic hemorrhage by US is poor.
In hemodynamically stable patients non-contrast-en-hanced CT is the initial imaging test of choice. Non-contrast CT can almost always demonstrate a para-aor-tic hematoma if present and may show additional find-ings helpful in establishing the diagnosis, such as ahigh-attenuating crescent sign. If the non-contrast CTfindings are equivocal or if endoluminal stent graft re-pair of the aorta is planned, contrast-enhanced CTshould be performed.
Conclusions
The practice of radiology in imaging patients with acuteabdomen has changed dramatically in the last few years.The time-honored plain abdominal radiographs havebeen largely replaced with US and CT. In particular, he-lical CT and more recently, MDCT permit the examina-tion to be performed in less time, with greater diagnosticaccuracy, and with less patient discomfort. The topo-graphic classification of pain (i.e., localized pain in oneof the four abdominal quadrants, diffuse abdominal painand flank or epigastric pain) facilitates finding the answerto specific questions. Therefore, close co-operation withthe referring physician prior to imaging remains essentialfor rapid and accurate diagnosis.
Suggested ReadingBhalla S, Menias CO, Heiken JP (2003) CT of acute abdominal
aortic disorders. Radiol Clin N Am 41:1153-1169Freeman AH (2001) CT and bowel disease. Br J Radiol 74:4-14Gore RM, Miller FH, Pereles FS et al (2000) Helical CT in the
evaluation of the acute abdomen. AJR Am J Roentgenol174:901-913
Macari M, Megibow A (2001) Imaging of suspected acute smallbowel obstruction. Seminars in Roentgenology XXXVI:108-117
Mindelzun RE, Jeffrey RB (1997) Unenhanced helical CT for eval-uating acute abdominal pain: a little more cost, a lot more in-formation. Radiology 205:43-47
Novelline RA, Rhea JT, Rao PM, Stuk JL (1999) Helical CT inemergency radiology. Radiology 213:321-339
Smith RC, Varanelli M (2000) Diagnosis and management of acuteureterolithiasis. AJR Am J Roentgenol 175:3-6
Taourel P, Kessler N, Lesnik A et al (2003) Helical CT of largebowel obstruction. Abdom Imaging 28:267-275
Urban BA, Fishman EK (2000) Tailored helical CT evaluation ofacute abdomen. Radiographics 20:725-749
Wiesner W, Khurana B, Ji H, Ros PR (2003) CT of acute bowel is-chemia. Radiology 226:635-650
Emergency Radiology of the Abdomen: The Acute Abdomen 9

Introduction
Trauma has become a significant health problem, in partdue to high velocity transportation and the use of pene-trating weapons, especially firearms. Not only the young,but also the elderly and pregnant women are affected.Improvements for those affected include more rapid res-cue, better organization of trauma centers, and advancesin treatment. There are three recent trends: the increasedtendency for non-operative care, the resulting increasedneed for accurate non-invasive imaging diagnosis, and adesire for cost-effective use of imaging. One aspect of thetrend towards non-operative care is the desire to avoidnon-therapeutic surgery; this is possible if imaging canidentify those patients who require surgery. Another as-pect is the realization that non-operative care can resultin better long-term outcome, such as salvaging splenicand renal function. Lastly, imaging evaluation with a highnegative predictive value may allow for discharge of trau-ma victims directly from the Emergency Department,avoiding hospital admission for observation.
CT versus Ultrasound
Controversy exists about the appropriate use of CT ver-sus ultrasound (US). Each has advantages and disadvan-tages [1-3]. In general, CT has been shown to have thebest statistical accuracy for detecting, characterizing andexcluding injuries. If the volume of trauma justifies it,CT can be located in the trauma suite such that even un-stable patients can be examined quickly and withoutcompromise. This has been done in our institution andthere is heavy reliance on CT for rapid accurate diagno-sis, avoiding diagnostic peritoneal lavage and non-thera-peutic laparotomies. CT is more reliable at excluding in-jury in those who may be discharged home, avoiding ob-servation in hospital.
However CT may be overused – in one study onlythree of 100 patients had an alteration in clinical man-agement after follow-up CT [4]. Sonography can detectsignificant injuries that can be treated; conversely, lowrisk patients with normal sonograms may be observed
and possibly avoid CT [2, 3]. One of the strengths of USis its ability to detect peritoneal fluid, a significant but non-specific finding indicative of abdominal injury. However,abnormal US often requires further evaluation by CT. In alarge study, US had 86% sensitivity and 98% specificity,with 43 false negative and 23 indeterminate studies, in-cluding six splenic, one liver, one renal, one pancreatic andone bowel injury [3]. Although the incidence of significantinjury in the absence of free intraperitoneal fluid is low, itdoes occur. A multi-institutional study found a 28% inci-dence of splenic and hepatic injury in patients with no orminimal free fluid on CT [5]. In patients with seat beltmarks, where bowel and mesenteric injury are common,US has been reported to miss up to 78% of significant in-juries [6].
The advent of multidetector CT (MDCT) for traumahas allowed some improvements, although routine traumaCT of the abdomen has changed little. Use of MDCT al-lows for more rapid acquisition of high quality images ofmultiple body parts, such as examination of the head,neck, chest, abdomen and pelvis. It allows for better re-formatting of images, with either thinner slice recon-structions, or other planes. In addition, if clinical circum-stances warrant, a CT angiogram can be performed im-mediately followed by routine trauma imaging.
In traumatized pregnant women, US should be the firstexamination. It can evaluate the pregnancy, documentingfetal viability. US is nearly as accurate in detecting ab-normal fluid in pregnant, as in non-pregnant patients [7].If US shows fluid or other injury, CT is justified to ob-tain the best evaluation (Fig. 1). The best outcome for thefetus is assured by the best care of the mother. The radi-ation risk is reasonable if there is life-threatening injury,necessitating prompt diagnosis and treatment [8].
Urinary Tract
Installation of CT in the Trauma unit, and nearly univer-sal use of CT, has altered our assessment of urinary tracttrauma. While significant hematuria has been shown tobe the best indicator of urinary tract injury, presently thedecision to perform CT has little to do with presence or
IDKD 2006
Trauma of the Abdomen and Pelvis I
P.J. Kenney
University of Alabama Medical Center, Birmingham, AL, USA

Trauma of the Abdomen and Pelvis I 11
absence of hematuria. CT is a primary investigation, af-ter standard radiographs, for those patients with signifi-cant mechanism of injury or any signs or symptoms ofsignificant injury. While intravenous urography (IVU)can detect renal injuries, it is less sensitive than CT, notaccurate for grading the renal injury and cannot assessother organ systems (Fig. 2). US has a limited ability toevaluate renal injury [9]. Although screening US has val-
ue in trauma in general, it has severe limitations in de-tecting genitourinary (GU) injury. Free intraperitonealfluid may not result from renal injury; although it mayfrom bladder rupture, US cannot diagnose bladder injury.In a study of 4,320 trauma patients who had undergoneUS, 33 of 99 patients with urologic injury had false neg-ative US. The sensitivity was only 56% for those with iso-lated urologic injury [10]. US is also not capable of grad-ing renal injuries.
CT has excellent negative predictive value for renal in-jury. Presence and type of renal injury can be accuratelyindicated [11]. Renal contusion demonstrates ill-defined
a
b
c
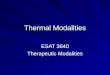
Fig. 1. Pregnant female who suffered high speed motor vehicle col-lision. a US demonstrates intrauterine fetus (heart motion docu-mented) and free pelvic fluid. b US shows perisplenic fluid withhypoechoic defect. c CT confirms splenic laceration; note higherdensity of perisplenic hematoma compared to rim of fluid aboutliver (sentinel clot sign)
a
b
Fig. 2. Hematuria and left upper quadrant pain after football injury.a IVU shows no abnormality. b Subsequent CT for persistent painshowed free fluid in pelvis and extensive splenic laceration withextensive ‘blush’. Surgery confirmed grade 4 splenic injury

12 P.J. Kenney
regions of diminished enhancement. Segmental renal in-farction is identified as a wedge shaped, well-defined areaof non-enhancement, and renal artery occlusion can be ac-curately diagnosed by its complete lack of enhancement orexcretion by the kidney, usually with little to no associatedhematoma. Angiography is thus not needed, and conserva-tive therapy is now most often used. Most renal injuries arelacerations, with simple laceration limited to the cortex,and deep laceration extending into the collecting system,which may show extravasation. Scans delayed between 2and 10 minutes aid in demonstrating or excluding extrava-sation (Fig. 3), although in most cases small amounts ofextravasation will resolve with conservative therapy.Subcapsular hematoma is delimited by the renal cortex andmay deform the renal surface; perinephric hematoma ex-tends from the renal surface to fill Gerota’s space, but doesnot deform renal contours, although it may displace thekidney. CT is excellent at demonstrating the extent of
hematoma, and evaluating enlargement on follow-up scans[11]. Renal fracture indicates a single complete fractureplane, often extending through the collecting system; mul-tiple planes of disruption are seen with shattered kidney.CT can also diagnose ureteropelvic junction (UPJ) avul-sion or ureteral injury, demonstrating lack of opacificationof the ureter, retroperitoneal water attenuation collectionsadjacent to pelvis or ureter, and possibly extravasation ofcontrast on delay scans [11].
Although the American Association for Surgery ofTrauma (AAST) Organ Injury Severity Scale for the kid-ney includes lesions with a different appearance in eachcategory (1: contusion, small subcapsular hematoma, 2:< 1 cm laceration without extravasation, 3: > 1 cm lacer-ation without extravasation, 4: deep laceration with ex-travasation or main renal artery or vein injury, 5: shat-tered kidney or UPJ avulsion), it has been shown to cor-relate with need for surgery and outcome [12].
Urethral injuries are predominantly seen in males.Anterior urethral ruptures are most commonly seen dueto straddle injury. Posterior urethral ruptures most oftenare due to compressive force and resultant pubic bonefractures, although both anterior and posterior urethral in-jury can result from penetrating injury. Retrograde ure-thrography is the only accurate diagnostic imaging pro-cedure. If a urethral injury is strongly suspected, a ure-throgram should be performed before passage of acatheter (Fig. 4). However, in patients with moderate risk,a urethral catheter may be gently passed and the patientmay go on to CT. A pericatheter urethrogram may then beperformed after other injuries are stabilized. Urethral in-
a
b
Fig. 3. Hematuria after fall from power line. a Initial CT shows leftrenal laceration with perinephric hematoma. b Delay image showsno leak from collecting system
Fig. 4. Blunt trauma resulted in pubic rami fractures. Retrogradeurethrogram reveals type 3 posterior urethral rupture

Trauma of the Abdomen and Pelvis I 13
juries may be classified as Type 1: posterior urethrastretched but intact, Type 2: tear of membranous urethraabove urogenital diaphragm, Type 3: tear of posterior ure-thra above and below urogenital diaphragm, Type 4: blad-der neck injury and Type 5: anterior urethral injury [13].
Although urethrography remains the standard, CTfindings have been described in urethral injury, whichmay be useful if CT is performed as the initial study.Obscuration of normal periurethral landmarks, in partic-ular distortion or obscuration of urogenital diaphragmfat planes and hematoma of the ischiocavernosus mus-cle, are commonly seen in those with urethral injury[14]. Alternatively, completely normal perineal anatomymay exclude significant injury, but further investigationis needed.
Bladder injuries, which consist of contusions and rup-tures, are most commonly extraperitoneal, less common-ly intraperitoneal, or are combined in about 5% of cas-es. They have classically been detected with standard ra-diographic cystography (Fig. 5). While CT with only in-travenous contrast may fail to identify extravasationfrom a ruptured bladder, several studies have shown veryhigh accuracy for CT cystography, which is now ourstandard (Fig. 6). In those with suspected bladder rupture(primarily those with gross hematuria, over 25 red bloodcells per high power field [rbc/hpf] with pelvic fractures,or unexplained pelvic fluid), we perform standard CTwith the bladder catheter clamped. If there is no ex-travasation, the bladder is drained then refilled with 300-500 cc of dilute contrast and the pelvis is rescanned.Bladder ruptures are virtually always associated with flu-id or hematoma in the pelvis, but such blood or fluid
may be due to splenic or other injuries, or pelvic frac-ture. Extravasation low in the pelvis, not outlining bow-el loops (and which may extend up the retroperitoneum)indicates extraperitoneal rupture that most often can bemanaged conservatively. Extravasation high near thedome outlining bowel loops or extending to the guttersor higher indicates intraperitoneal rupture, and is moreoften managed surgically [15].
Bowel and Mesenteric Injury
Bowel and mesenteric injury are found in about 5% ofpatients having surgery for trauma, seen in 0.7% of trau-matized patients [1, 16]. Mechanism of injury is directcompressive force, including from seatbelts, although de-celeration may play a role. Morbidity and mortality canoccur if peritonitis and resulting abscess are missed.Clinical signs and symptoms are non-specific. Althoughpositive diagnostic peritoneal lavage (DPL) or free fluidon sonography may be due to bowel or mesenteric injury,these findings are non-specific [2].
Although some have commented on the difficulty ofcorrect diagnosis by CT, CT is the most accurate diag-nostic modality, with a reported sensitivity of 88-96%and a specificity of 80-99% [16-20]. Use of oral contrast,
a
b
Fig. 6. Gross hematuria following motor vehicle collision resultingin extensive pelvic fractures. a Standard CT shows pelvic fluid butno extravasation. b CT cystogram documents extraperitoneal blad-der rupture (note clot in bladder)
Fig. 5. Gross hematuria after gunshot wound to pelvis. Standard cys-togram shows extraperitoneal rupture (X, entry site; O, exit)

14 P.J. Kenney
and early scanning after rapid injection of high volumeintravenous contrast allows detection of extravasation[21]. Active bleeding is seen as a focal collection with at-tentuation similar to the aorta at the same level and dif-ferent from the adjacent organ. Contrast extravasation,whether intravenous contrast from a mesenteric vessel ororal contrast from the bowel lumen, is the most specificsign of mesenteric or bowel injury, but is not common –it was seen in only seven of 26 patients with bowel injury[17]. Free air is thought to be a good sign of perforatedbowel, but in fact it has limited value; it is infrequentlyseen in those patients with bowel injury, and may in factrepresent air tracking into the peritoneum from thoracicinjuries. Free air was seen in only 28% of true positiveCT scans, but in 2% of false positive scans [16]. Thecommonest finding was unexplained free fluid, eventhough 70% of those with only unexplained free fluid hadno bowel injury. Other findings, such as focal bowel wallthickening, interloop fluid, mesenteric stranding or frankhematoma are often seen (Fig. 7). If a single finding isseen, likelihood of injury is low; a combination of find-ings, particularly free fluid without an obvious source incombination with focal bowel wall thickening and/ormesenteric stranding is very suggestive of bowel injuryand such patients should be further explored or followedvery carefully.
Oral contrast presents a risk, although low, of adverseevents, including aspiration pneumonia. Given this andthe low rate of visible bowel contrast leak, some havequestioned the use of oral contrast to detect bowel injury.One study of 1,000 patients [22] and another of 500 [23]showed similar accuracy to previous reports with oralcontrast – with a sensitivity of 82-95%, and a specificityof 99%. At our institution, the use of oral contrast hasbeen discontinued in trauma patients with no recognizedill effect.
Splenic Injuries
The spleen is the most frequently injured abdominal or-gan in blunt trauma. There may be signs of blood loss, orleft upper quadrant pain, but the diagnosis largely restson imaging or surgical exploration. A trend towards non-operative management is supported by evidence thatlong-term health is better in those who have had splenicfunction preserved. This necessitates accurate non-invasive diagnosis, and is aided by signs predictive ofsuccess or failure of conservative management.
Splenic injuries can cause free fluid, perisplenically orelsewhere, which can readily be detected by sonography.Splenic injury may alter echo texture: lacerations may beanechoic if there is rapid bleeding, but are more com-monly more echogenic than normal spleen [2]. With suchfindings on sonography, the decision whether to furtherevaluate with CT or to proceed to surgery can be madeon clinical grounds (Fig. 1). Splenic injuries may bemissed by sonography, particularly if not associated withfree fluid. In one large study, there were 43 false negativesonograms, including six splenic ruptures that requiredsurgery [3].
CT is quite sensitive for the detection of splenic injuries[24]. Subcapsular hematoma is seen as a crescentic low at-tenuation peripheral rim, and intraparenchymal hematomais seen as a rounded area within the spleen with low at-tenuation and no enhancement. Lacerations are common,seen as linear or branching low attenuation lesions whichoften extend to the surface, often associated withperisplenic or free fluid (Fig. 1, 2). Hemoperitoneumtends to be higher attenuation close to the source of thebleeding; thus when the spleen is the source, the collec-tion adjacent to the spleen may be higher in attenuationthan elsewhere (Fig. 1), the sentinel clot sign. Lacerationsmay involve the vasculature. There can be devasculariza-tion of the spleen by hilar injury. There may be active ex-travasation into the peritoneal cavity or a confined area ofextravasation – a pseudoaneurysm (Fig. 2). Both types ofextravasation indicate that non-operative managementmay not succeed, although angiographic embolizationmay control the bleeding and allow splenic salvage [25].
A number of schemes have been devised to gradesplenic injury on CT in an attempt to predict outcome,with variable correlation with need for surgery [1]. Oneof the commonest is the AAST scoring system. In a largestudy, failure of non-operative management correlatedwith splenic injury grade: less than 10% failed withgrades 1 or 2, while one-third of grade 4 and three-quar-ters of grade 5 injuries required surgery [26]. Never-theless, for the individual patient, occasional cases oflow-grade injury suffer delayed rupture, and some high-grade injuries are successfully conservatively managed.The additional finding of traumatic pseudoaneurysm oractive extravasation (which does not confer to a specificstage in the AAST scoring system) increased the likeli-hood of failure of non-operative management, whateverthe grade [27]. No CT findings are accurate predictors of
Fig. 7. Motor vehicle collision. Focal hematoma and thickening ofcecum; cecal laceration was found at surgery

the need for intervention. Angiographic embolization hassimilar outcomes and less morbidity compared withsurgery [28].
Hepatic Injuries
The liver is the second most frequently injured abdom-inal organ, accounting for about 20% of abdominal in-juries [1, 24]. The right lobe is more often affected thanthe left, with the posterior right lobe being the most fre-quently injured segment. Hepatic injuries may be asso-ciated with intraperitoneal hemorrhage, but injury maybe confined to the liver, or hemorrhage limited by anintact capsule. Laceration of the bare area is associatedwith extraperitoneal fluid [1]. US may show liver lac-erations, which appear similar to splenic injuries, butUS has a limited sensitivity of 67%, compared to 93%for CT [29]. This is in part because of the large size ofthe liver, and the difficulty in clearly imaging all por-tions by US.
Injuries to the liver include contusion, seen on CT asan ill-defined area of low attenuation; subcapsularhematoma, a crescentic collection limited by the capsule;and intraparenchymal hematoma, a collection of bloodwithin a liver laceration. Laceration is the most common,with linear or branching low attenuation regions, some-times with jagged margins, that can extend to surface orto vessels. Periportal low attenuation is usually due toedema, but it may represent blood tracking along portalveins. Rarely, this is the only sign of liver injury [1, 24].The most severe, and rare, injury is avulsion of the he-patic pedicle [30].
Liver injuries may require surgery, but 50-90% can bemanaged non-operatively. The liver, with a dual bloodsupply, is relatively resistant to infarction, and has con-siderable functional reserve. No CT signs or gradingschemes have been shown to be reliable predictors ofwhich patients will require intervention. However, activeextravasation may predict a need for surgery or angioem-bolization. The presence of hepatic arterial extravasationor extension of injury into hepatic veins correlates withthe need for surgery [31]. Subclassification of extravasa-tion can be useful: extravasation into the peritoneal cavi-ty is highly correlated with the need for surgery, intra-parenchymal extravasation with significant hemoperi-toneum may require surgery, while extravasation limitedwithin a hepatic hematoma without hemoperitoneum canusually be managed conservatively [21].
References
1. Novelline RA, Rhea JT, Bell T (1999) Helical CT of abdomi-nal trauma. RCNA 37:591-612
2. McKenney KL (1999) Ultrasound of blunt abdominal trauma.RCNA 37:879-893
3. Dolich MO, McKenney MG, Varela JE et al (2001) 2576Ultrasounds for blunt abdominal trauma. J Trauma 50:108-112
Trauma of the Abdomen and Pelvis I 15
4. Shapiro MJ, Krausz C, Durham RM et al (1999) Overuse ofsplenic scoring and computed tomographic scans. J Trauma47:651-658
5. Ochsner MG, Knudson MM, Pachter HL et al (2000)Significance of minimal or no intraperitoneal fluid visible onCT associated with blunt liver and splenic injuries: a multi-center analysis. J Trauma 49:505-510
6. Stassen NA, Lukan JK, Carillo EH et al (2002) Abdominalseat belt marks in the era of focused abdominal sonography fortrauma. Arch Surg 137:718-722
7. Goodwin H, Holmes JF, Wisner DH (2001) Abdominal ultra-sound examination in pregnant blunt trauma patients. J Trauma50:689-693
8. Lowdermilk C, Gavant ML, Qaisi W et al (1999) Screeninghelical CT for evaluation of blunt traumatic injury in the preg-nant patient. Radiographics 19:S243-S255
9. McGahan JP, Richards JR, Jones CD et al (1999) Use of ul-trasonography in the patient with acute renal trauma. JUM18:207-213
10. McGahan PJ, Richards JR, Bair AE et al (2005) Ultrasound de-tection of blunt urological trauma: a 6 year study. Injury36:762-770
11. Kawashima A, Sandler CM, Corl FM et al (2001) Imaging ofrenal trauma: a comprehensive review. Radiographics221:557-574
12. Santucci RA, McAninch JW, Safir M et al (2001) Validationof the American Association for the Surgery of Trauma organinjury severity scale for the kidney. J Trauma 50:195-200
13. Goldman SM, Sandler CM, Corriere JN et al (1997) Blunt ure-thral trauma: a unified anatomical mechanical classification. JUrol 157:85-89
14. Ali M, Safriel Y, Sclafani SJA et al (2003) CT signs of urethralinjury. Radiographics 23:951-963
15. Morgan DM, Nallamalla LK, Kenney PJ et al (2000) CT cys-tography: radiographic and clinical predictors of bladder rup-ture. AJR Am J Roentgenol 174:89-95
16. Malhotra AK, Fabian TC, Katsis SB et al (2000) Blunt boweland mesenteric injuries: the role of screening CT. J Trauma48:991-998
17. Dowe MF, Shanmuganathan K, Mirvis SE et al (1997) CTfindings of mesenteric injury after blunt trauma. AJR Am JRoentgenol 168:425-428
18. Butela ST, Federle MP, Chang PJ et al (2001) Performance ofCT in detection of bowel injury. AJR Am J Roentgenol176:129-135
19. Sharma OP, Oswanski MF, Singer D et al (2004) The role ofcomputed tomography in diagnosis of blunt intestinal andmesenteric trauma. J Emergency Med 27:55-67
20. Elton C, Riaz AA, Young N et al (2005) Accuracy of comput-ed tomography in the detection of blunt bowel and mesentericinjuries. Br J Surgery 92:1024-1028
21. Fang J-F, Chen R-J, Wong Y-C et al (2000) Classification andtreatment of pooling of contrast material on CT scan of blunthepatic trauma. J Trauma 49:1083-1088
22. Stuhlfaut JW, Soto JA, Lucey BC et al (2004) Blunt abdomi-nal trauma: performance of CT without oral contrast material.Radiology 233:689-694
23. Allen TL, Mueller MT, Bonk T et al (2004) Computed tomo-graphic scanning without oral contrast for blunt bowel andmesenteric injuries in abdominal trauma. J Trauma 56:314-322
24. West OC (2000) Intraperitoneal abdominal injuries. In: WestOC, Novelline RA, Wilson AJ (eds) Emergency and TraumaRadiology Categorical Course Syllabus, pp 87-98
25. Davis KA, Fabian TC, Croce MA et al (1998) Improved suc-cess in nonoperative management of blunt splenic injuries:embolisation of splenic artery pseudoaneurysms. J Trauma44:1008-1013
26. Peitzman AB, Heil B, Rivera L et al (2000) Blunt splenic in-jury in adults: multi-institutional study of the EasternAssociation for the Surgery of Trauma. J Trauma 49:177-187

16 P.J. Kenney
27. Gavant ML, Schurr M, Flick PA et al (1997) Predicting clini-cal outcome of nonsurgical management of blunt splenic in-jury: using CT to reveal abnormalities of splenic vasculature.AJR Am J Roentgenol 168:207-212
28. Wahl WL, Ahrns KS, Chen S et al (2004) Blunt splenic injury:operation versus angiographic embolization. Surgery 136:891-899
29. Richards JR, McGahan JP, Pali MJ et al (1999) Sonographicdetection of blunt hepatic trauma. J Trauma 47:1092-1097
30. Romano L, Giovine S, Guidi Guido et al (2004) Hepatic trau-ma: CT findings. Eur J Radiol 50:59-66
31. Poletti PA, Mirvis SE, Shanmuganathan K et al (2000) CT cri-teria for management of blunt liver trauma. Radiology216:418-427

Introduction
Computed tomography (CT) is the established methodfor the imaging evaluation of traumatic injury to the ab-domen and pelvis. This role has been galvanized in theera of multidetector CT (MDCT) because of the greaterspeed and flexibility afforded by this modality. MDCTcan now image the head, entire spine and torso, often inless time than would be typical for obtaining a standardthree-view radiographic trauma series (portable chest, lat-eral C-spine and AP pelvis). When coupled with its ac-curacy for detecting multisystem injuries, CT has becomethe indispensable means by which prompt diagnosis andtriage is undertaken for the stable trauma patient.Additionally, the high quality image data sets now ob-tained from MDCT permit the routine use of post pro-cessing techniques such as multiplanar reformation(MPR), maximum intensity projection (MIP) and three-dimensional (3D) image display for improving evaluationand communication of diagnostic results.
MDCT Imaging Techniques
Since most traumatic injury is not isolated to a singleanatomic region, abdominal and pelvic imaging is usual-ly undertaken in the context of a complete system evalu-ation of the multitrauma patient that often includes imag-ing of the head, entire spine and torso. As previously pub-lished by several authors, following a head CT withoutintravenous contrast material (IVCM), scanning is per-formed from the circle of Willis, or alternatively, from thethoracic inlet to the symphysis pubis following the intra-venous administration of nonionic IVCM (100-150 ml of300 mg iodine/mL, Ultravist 300) using an injection rateof at least 3 cc/s. Imaging through the abdomen shouldbe timed so that it commences during the portal venousphase of homogeneous parenchymal enhancement. Earlyor delayed scanning may falsely simulate injury or de-crease conspicuity of true injury. At our institution, theemergency radiologist immediately reviews a trauma pa-tient’s scans while the patient is on the CT table. Wheninjury is present, delayed imaging is generally performed
approximately 3 minutes after the initial IVCM injection,or during the pyelographic phase. Delayed imaging is notperformed if no significant injury is detected, thereby re-ducing radiation exposure for these patients. If immedi-ate review of the initial scan is not an option based on ra-diologist’s availability, or if the incidence of injury is highamong a given institution’s trauma population, routine ac-quisition of a delayed scan in every patient may prove amore efficient means of operating procedure. An unen-hanced CT is performed in patients with known renal in-sufficiency or severe contrast allergy, though sensitivityfor detecting injury is reduced.
Oral contrast material (OCM) is not routinely used atour trauma center at the time of the initial CT evaluation.Though the use of OCM has been shown to be safe, theperception of providers at our institution is that it delaystransit to CT, results in the otherwise unnecessary place-ment of a nasogastric tube in many patients, and owing tothe speed of MDCT, is increasingly of little benefit hav-ing rarely progressed beyond the stomach to typical areasof injury by the time CT is performed in most patients.Instead, once immediate life-threatening injuries havebeen excluded by an initial CT scan, patients with sus-pected bowel injury based on clinical grounds or resultsof the initial scan are reimaged after administration ofwater soluble OCM and a relatively short time for boweltransit, usually about 1 hour.
Rectal contrast material should be administered in allpatients with penetrating injuries to the abdomen orflank. Approximately 50 cc of Ultravist 300 (or anyIVCM of similar iodine concentration) is injected into aliter of warm saline for use as contrast material.Adequate colonic distention generally involves adminis-tration of approximately 500 cc rectal contrast materialwith the patient in a left lateral decubitus position forsuspected left colonic injury, or up to a liter of contrastmaterial with the patient in a right lateral decubitus po-sition for suspected right colonic injury. Use of intra-venous, oral and rectal contrast material (i.e., triple con-trast CT) has been shown to be a highly accurate meansof excluding peritoneal violation in the setting of pene-trating trauma to the flank. Additionally, among thosepatients with peritoneal violation, CT has been reported
IDKD 2006
Trauma of the Abdomen and Pelvis II
S. Ledbetter
Division of Emergency Radiology, Brigham and Women’s Hospital, Boston, MA, USA

to accurately predict the need for laparotomy with 100%sensitivity, 96% specificity, 100% negative predictivevalue, and 97% accuracy.
When bladder injury is suspected, CT cystography isperformed. Antegrade filling of the bladder from renalexcretion of IVCM is insufficient for excluding bladderinjury. Bladder contrast is easily obtained by mixing 50cc Ultravist 300 in a liter of warm saline. Following theinitial scan of the abdomen and pelvis with IVCM, theFoley catheter is unclamped, permitting completedrainage of excreted contrast material. A closed system isused to connect the liter of saline to the indwelling Foleycatheter and contrast is instilled in a retrograde fashionwith the saline bag approximately 40 cm above the heightof the patient’s bladder (i.e., the height of the CT table).Bladder contrast is instilled until one of the following: 1)contrast flow stops, 2) 350 to 400 cc of contrast havebeen instilled, or 3) the patient no longer tolerates con-trast instillation. Adequate retrograde distention of thebladder is critical for its proper evaluation. Furthermore,CT cystography should not be performed until after theinitial CT scan through the abdomen and pelvis withIVCM. This allows easy discrimination between arterialextravasation and bladder contrast extravasation, both ofwhich are encountered in the setting of pelvic fractures.
Splenic Injury
The spleen is the most commonly injured solid organ inthe setting of blunt abdominal trauma, representing ap-proximately 25% of all blunt injuries to the abdominalviscera. The spleen is a highly vascular organ that weighsapproximately 75-100 grams in the average adult, con-tains approximately one unit of blood at any given timeand circulates approximately 350 liters of blood per day.With greater recognition of its important immunologicroll, there has been a progressive trend toward the con-servative, nonoperative management of splenic injuryamong hemodynamically stable patients. Today, morethan half of all patients with splenic injury are managednonoperatively.
Splenic injury may be manifest on CT as parenchymalcontusion, intraparenchymal or subcapsular hematomas,intrasplenic lacerations, vascular injuries includingpseudoaneurysms and arteriovenous fistulas, and activearterial hemorrhage. Parenchymal contusions are seen aspoorly defined areas of decreased parenchymal enhance-ment. Subcapsular hematomas are generally seen as welldefined elliptical or crescentic collections of blood thatreside immediately below the splenic capsule, may com-press the subjacent splenic parenchyma and are of lowerattenuation than the enhancing splenic parenchyma.Presence of parenchymal compression helps differentiatesubcapsular hematoma from perisplenic hematoma.Intrasplenic lacerations are seen as linear or complex andbranching areas of low attenuation coursing through thenormally enhancing splenic parenchyma, whereas intra-
18
parenchymal hematomas are seen as intrasplenic low at-tenuation collections. Active hemorrhage, pseudoa-neurysms and arteriovenous fistulas appear as areas of in-creased density relative to the normally enhancingsplenic parenchyma and are of similar attenuation valueto an adjacent major artery, generally within 10Hounsfield units (HU) (i.e., contrast blush [CB]).Traumatic injury may also result in segmental or com-plete splenic devascularization.
Relying on CT appearance alone to accurately predictthose patients requiring splenectomy versus those whocan be managed nonoperatively would be highly advan-tageous. Unfortunately, despite a number of CT gradingsystems, none has proven reliable in predicting outcomefor nonoperative management. Using logisitic regression,Schurr et al. showed that CT splenic injury grade had nopredictive value for nonoperatively-managed patients.Other studies have shown that CT often underestimatesthe severity of splenic injury. There is also significant in-terobserver variability among radiologists in their grad-ing of splenic injury. Despite these limitations, CT hasnonetheless greatly facilitated the trend toward nonoper-ative management, if for no other reason than its contri-bution toward excluding other injuries that would requiresurgical exploratory laparotomy.
More recent radiology literature suggests that someCT findings may have strong predictive values for failednonoperative management. These include: 1) active he-morrhage, 2) post-traumatic pseudoaneurysm, and 3) ar-teriovenous fistula. All three of these lesions may beseen as a ‘contrast blush’ on the initial phase of CT scan-ning. The latter two splenic vascular injuries cannot befurther differentiated on contrast-enhanced CT.However, the latter two can be differentiated from activehemorrhage on delayed scanning, at which time the ar-terial attenuation ‘blush’ typically decreases to becomeisodense or minimally hyperdense compared to the nor-mally enhancing splenic parenchyma. Conversely, the ar-terial ‘blush’ persists during delayed scanning with ac-tive hemorrhage since the contrast material has ex-travasated from vascular structures and therefore doesnot ‘wash-out’. Furthermore, whereas the splenic vascu-lar injuries of post-traumatic pseudoaneurysm and arte-riovenous fistula are always intrasplenic, active hemor-rhage may be intrasplenic, subcapsular or freely in-traperitoneal (Fig. 1) (Tab. 1).
Among those managed nonoperatively, the majority offailures will occur within 24 hours of admission. Gavantand colleagues reported an 82% failure rate among pa-tients with contrast extravasation or intrasplenic vascularinjury (pseudoaneurysm or arteriovenous fistula) whowere managed nonoperatively. Other investigators haveshown that patients with a CB by CT are 9.2 times morelikely to require surgical laparotomy or angiographic em-bolization. In effect, a CB at CT has a high correlationwith failure of nonoperative management. However, todate this finding has not been included in any of thewidely used splenic injury grading criteria.
S. Ledbetter