Embed Size (px)
Citation preview
DISCUSSION OF PRESENTATION BY DRS BARRY WEPMAN AND JULES BAUM
GEORGE 0. WARING ill, MD DAVIS, CALIFORNIA
DocTORS Wepman and Baum have filled a void in the ophthalmic literature by documenting that the corneal complications of Bell's palsy are limited to transient punctate epithelial keratopathy in about half the patients.
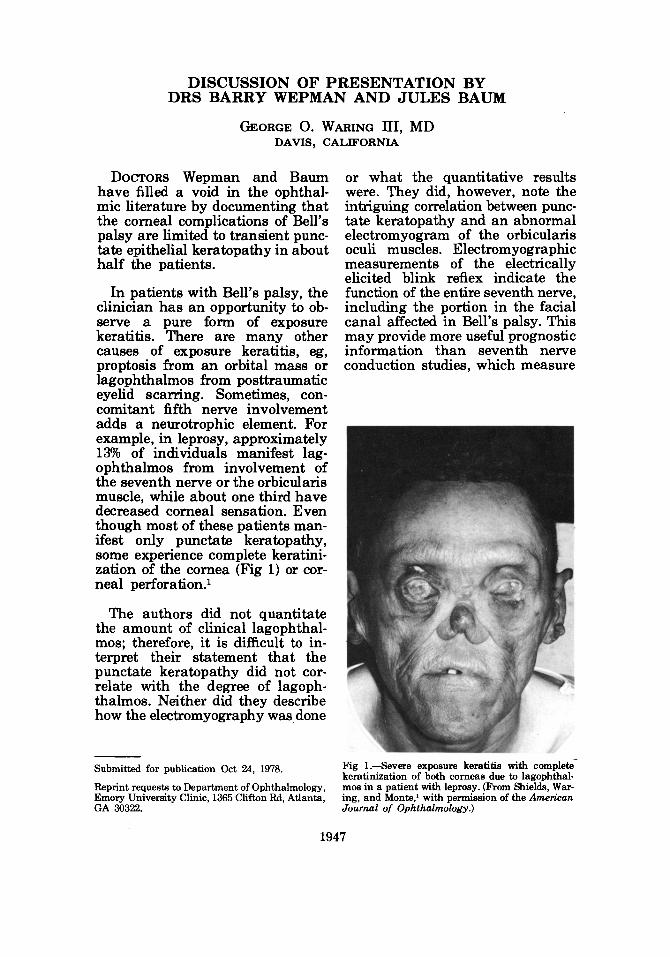
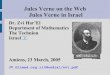
In patients with Bell's palsy, the clinician has an opportunity to observe a pure form of exposure keratitis. There are many other causes of exposure keratitis, eg, proptosis from an orbital mass or lagophthalmos from posttraumatic eyelid scarring. Sometimes, concomitant fifth nerve involvement adds a neurotrophic element. For example, in leprosy, approximately 13% of individuals manifest lagophthalmos from involvement of the seventh nerve or the orbicularis muscle, while about one third have decreased corneal sensation. Even though most of these patients manifest only punctate keratopathy, some experience complete keratinization of the cornea (Fig 1) or corneal perforation.1
The authors did not quantitate the amount of clinical lagophthalmos; therefore, it is difficult to interpret their statement that the punctate keratopathy did not correlate with the degree of lagophthalmos. Neither did they describe how the electromyography was done
Submitted for publication Oct 24, 1978.
Reprint requests to Department of Ophthalmology, Emory University Clinic, 1365 Clifton Rd, Atlanta, GA 30322.
or what the quantitative results were. They did, however, note the intriguing correlation between punctate keratopathy and an abnormal electromyogram of the orbicularis oculi muscles. Electromyographic measurements of the electrically elicited blink reflex indicate the function of the entire seventh nerve, including the portion in the facial canal affected in Bell's palsy. This may provide more useful prognostic information than seventh nerve conduction studies, which measure
Fig 1.-Severe exposure keratitis with completekeratinization of both corneas due to lagophthalmos in a patient with leprosy. (From Shields, Waring, and Monte, 1 with permission of the American Journal of Ophthalmology.)
1947
1948 GEORGE 0. WARING III OPHTH AAO
A 8
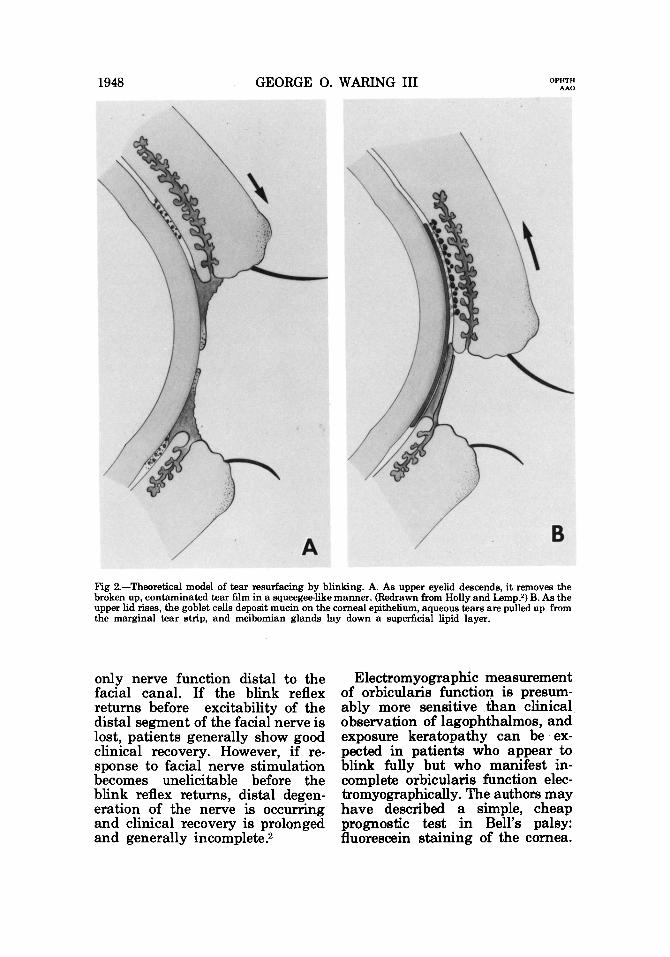
Fig 2.-Theoretical model of tear resurfacing by blinking. A. As upper eyelid descends, it removes the broken up, contaminated tear film in a squeegee-like manner. (Redrawn from Holly and l..emp.2) B. As the upper lid rises, the goblet cells deposit mucin on the corneal epithelium, aqueous tears are pulled up from the marginal tear strip, and meibomian glands lay down a superficial lipid layer.
only nerve function distal to the facial canal. If the blink reflex returns before excitability of the distal segment of the facial nerve is lost, patients generally show good clinical recovery. However, if response to facial nerve stimulation becomes unelicitable before the blink reflex returns, distal degeneration of the nerve is occurring and clinical recovery is prolonged and generally incomplete.2
Electromyographic measurement of orbicularis functiol) is presumably more sensitive than clinical observation of lagophthalmos, and exposure keratopathy can be expected in patients who appear to blink fully but who manifest incomplete orbicularis function electromyographically. The authors may have described a simple, cheap prognostic test in Bell's palsy: fluorescein staining of the cornea.
VOLUME 86 NOVEMBER 1979
DISCUSSION 1949
What is the physiology of normal blinking and what is the pathogenesis of exposure keratopathy in Bell's palsy? The preocular tear film does not flow from the lacrimal gland across the globe to the lacrimal punctae. A blink must mechanically spread tears over the globe. The preocular tear film remains stable in the absence of blinking for about 30 seconds. Between blinks, according to the current model of tear film function,3 the superficial lipid layer seeps into the aqueous layer and contaminates the deep mucin layer, which is responsible for adsorbing the aqueous tears to the hydrophobic corneal epithelium. This raises the sur-
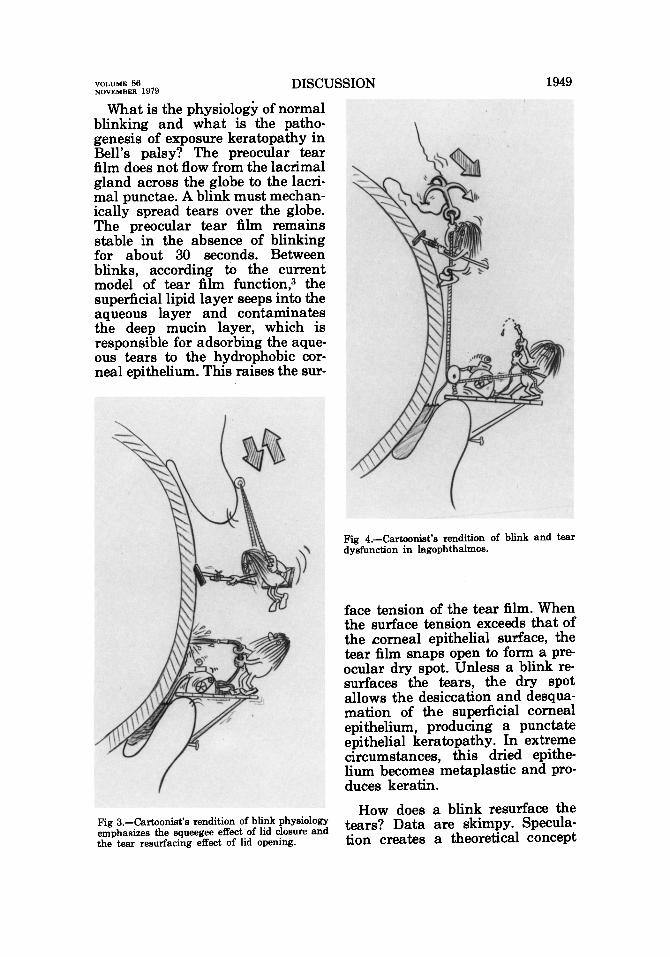
Fig a.-Cartoonist's rendition of blink physiology emphasizes the squeegee effect of lid closure and the tear resurfacing effect of lid opening.
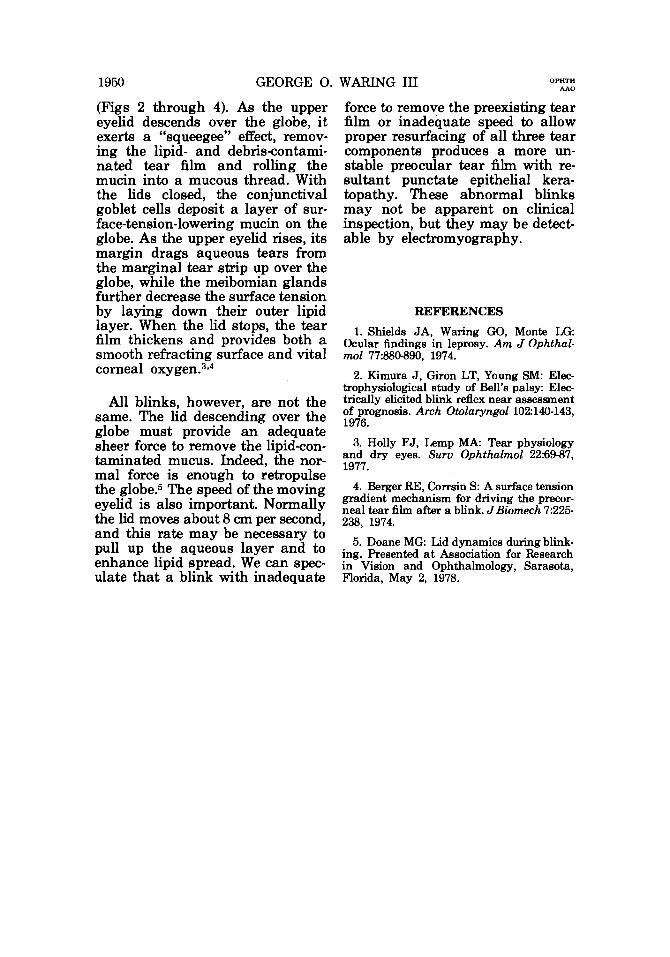
Fig 4.-Cartoonist's rendition of blink and tear dysfunction in lagophthalmos.
face tension of the tear film. When the surface tension exceeds that of the .corneal epithelial surface, the tear film snaps open to form a preocular dry spot. Unless a blink resurfaces the tears, the dry spot allows the desiccation and desquamation of the superficial corneal epithelium, producing a punctate epithelial keratopathy. In extreme circumstances, this dried epithelium becomes metaplastic and produces keratin.
How does a blink resurface the tears? Data are skimpy. Speculation creates a theoretical concept
1950 GEORGE 0. WARING III OPHTH AAO
(Figs 2 through 4). As the upper eyelid descends over the globe, it exerts a "squeegee" effect, removing the lipid- and debris-contaminated tear film and rolling the mucin into a mucous thread. With the lids closed, the conjunctival goblet cells deposit a layer of surface-tension-lowering mucin on the globe. As the upper eyelid rises, its margin drags aqueous tears from the marginal tear strip up over the globe, while the meibomian glands further decrease the surface tension by laying down their outer lipid layer. When the lid stops, the tear film thickens and provides both a smooth refracting surface and vital corneal oxygen. 3•4
All blinks, however, are not the same. The lid descending over the globe must provide an adequate sheer force to remove the lipid-contaminated mucus. Indeed, the normal force is enough to retropulse the globe.5 The speed of the moving eyelid is also important. Normally the lid moves about 8 em per second, and this rate may be necessary to pull up the aqueous layer and to enhance lipid spread. We can speculate that a blink with inadequate
force to remove the preexisting tear film or inadequate speed to allow proper resurfacing of all three tear components produces a more unstable preocular tear film with resultant punctate epithelial keratopathy. These abnormal blinks may not be apparent on clinical inspection, but they may be detectable by electromyography.
REFERENCES
1. Shields JA, Waring GO, Monte LG: Ocular findings in leprosy. Am J Ophthalmol 77:880-890, 1974.
2. Kimura J, Giron LT, Young SM: Electrophysiological study of Bell's palsy: Electrically elicited blink reflex near assessment of prognosis. Arch Otolaryngol102:140-143, 1976.
3. Holly FJ, Lemp MA: Tear physiology and dry eyes. Surv Ophthalmol 22:69-87, 1977.
4. Berger RE, Corrsin S: A surface tension gradient mechanism for driving the precorneal tear film after a blink. J Biomech 7:225-238, 1974.
5. Doane MG: Lid dynamics during blinking. Presented at Association for Research in Vision and Ophthalmology, Sarasota, Florida, May 2, 1978.
























![[Baum Whiteman] 2013trends](https://img.pdfslide.us/doc/110x75/5451d6cbb1af9f7a248b4aba/baum-whiteman-2013trends.jpg)


