Embed Size (px)
Citation preview
DISCUSSIONAs of 7/6/12
1

Outline• Background• What’s happening now• The treatment landscape• Options• Next steps
Proposal: Two options (private and public)
Preference: Private option
Position: Love and support either way
Process: Loved one to decide
2
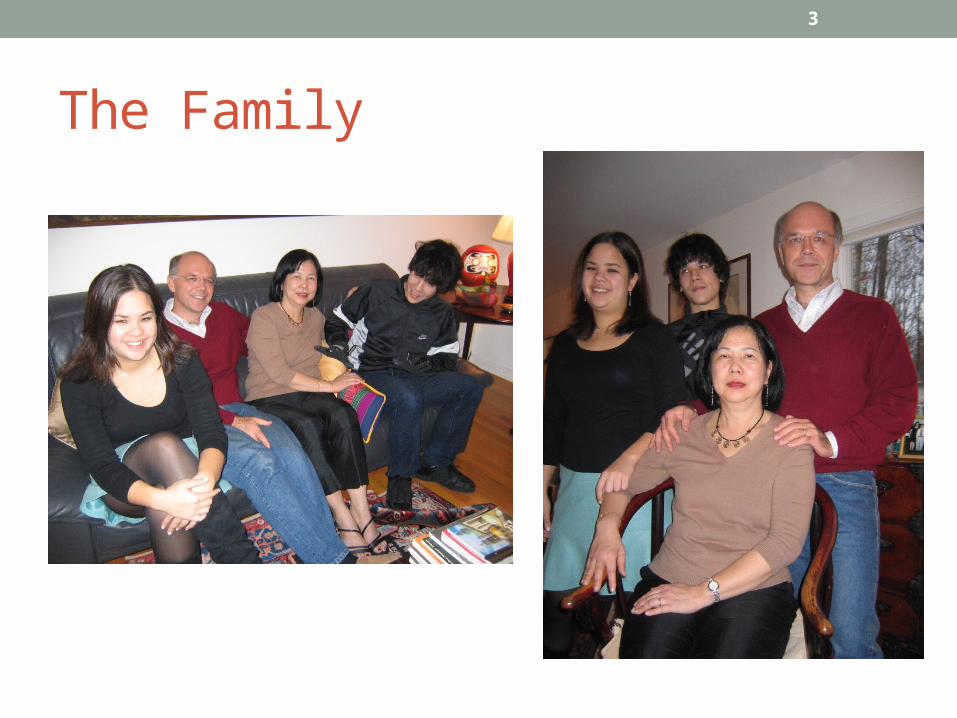
The Family
3

Philosophy
• Mind + body = 1, not 2• Not just biochemistry• Trauma: a huge factor
• Interdependence• Open dialogue• Inclusive. Collaborative.
• Psych Rehab
4
Preferred Approaches• Recovery model (EBP)
• Recovery = “finding new meaning”• Person-centered, self-defined & directed• Holistic. Based in hope.• Full supports, community-integration• Non-linear, time-unlimited• LT continuum of care
• Psychology• Reflective listening, CBT, motivational interviewing, etc.• Listen, Empathize, Accept, Partner (Amador)
• Medications• Judicious, minimalist
5

History
• 2003• Difficulties at Rutgers; withdrawals• DWI in two towns• Drug use in Worchester• Difficulties at Dynamy; withdraws
• 2005• Difficulties at Pratt; withdraws
• 2006• Community college for credits• Re-enters Rutgers; lives at home
• 2007• Difficulties at Rutgers; withdraws• 3/30/07: First psychotic episode• Carrier, Princeton House outpatient• Princeton House inpatient, outpatient
• 2008• Self confesses addictions to
amphetamines, marijuana• Second Nature Entrada• Difficulties at WestBridge; terminated• Princeton House inpatient• Pasadena Villa: admission refused
6

History, 2
• 2009, 2010• Walmart jobs, etc• D&D • ER visits• Lost while driving
• 2011• DWI• Princeton House detox• Difficulties at New Hope Foundation;
withdraws• Discharged to own apartment• Continuing visits to Dr. Steubben
7
More recently…• 9/17/11: Arrest after episode at Princeton University
• Inebriation Trespass Outburst at Muslim Students dinner• Arrested, charged with four crimes, including Class 4 bias felony• ALCOHOL
• 9/20/11: Call to county crisis center fails• 72 hour evaluation thwarted by Haldol, lack of HIPAA releases• Fuld releases to the street
• No referral, no discharge plan, no change in medications
• ALCOHOL
• 10/1/11: Involuntary commitment to Hampton House• ALCOHOL
8
…, 2• 10/18/11: Involuntary commitment overruled
• Judge orders release.
• 10/20/11: Botched discharge from Hampton House• Released to Mercer County PACT Team…• …without PACT’s knowledge.• 11 days without services
• 11/1/11: Admitted to Princeton House Outpatient• Dr. Stanley in charge• False start; leaves when hearing voices• Starts again; deemed “inappropriate for outpatient”
9
…, 3• 11/7/11: Enter Princeton House Inpatient (Voluntary)
• Doctors want faster meds change; resists proposed meds changes• Dr. Kazi’s compromise accepted: injectable for more time voluntary
• 11/11/11: Committed to Princeton House STCF (Involuntary) • Dr. Pahl in charge. Time limited.• Within 48 hours…
• Stripped off Zoloft; blasted with Thorazine, Invega, Lithium
• No family meeting; rushed decision before Thanksgiving• Dx on discharge: Schizoaffective; GAF = 20.
• 11/23/11: Transfer to TPH• Dr. Ghazili in charge (Drake Unit)• Dx upon admission: Bipolar I, GAF: 35
10
…, 4• 12/7/11: Leave TPH; Enter Princeton House Outpatient
• Dr. Stanley in charge• Lives with parents to support recovery, overcome institutional trauma
• January, 2012: ICMS engaged• Patty Crater
• 1/26/12: Court appearance: PTI approved.• 40 hours community service; completion of treatment plan
• February: Beck Institute engagement begins• 1x per week
• March: Step-down to Princeton House IOP
11
…, 5• April
• Leaves Princeton House• Engages APN Peter Njili at Greater Trenton• Begins weekly at Beck Institute (Dr. Cotterell in charge)
• May: Relapses (2 small episodes)• ALCOHOL
• 5/24/12: First family participation in Multi-Family Group
• 6/10/12: Enter Princeton Hospital ER• Voluntarily.• “Bored”• ALCOHOL
12

…, 6
• 6/12/12: Failed AAMH admission• “Can’t handle groups”
• 6/13/12: Enter Princeton Hospital ER (3 pm)• Massive relapse; 420 ml in 30 minutes; BAC: .38 (Lethal dose: 40)• $: CDs pilfered from home• Botched discharge
• Refused for Princeton House inpatient, released at 4 am. BAC ~ .20?
• ALCOHOL
• 6/17/12: Mother and sister to Singapore for a month.
13
…, 7 • 6/30/12: Enter Princeton Hospital ER
• 150 ml in one hour• $: cash pilfered from father’s wallet• ALCOHOL
• 7/1/12: Enter Princeton House Inpatient
• 7/17/12: Mother and sister to return from Singapore
14
What’s happening?
• Voices• Constant, loud, denigrating
• Depression• Desperate to avoid
• Discomfort with groups• Can’t discuss voices (AA)• Can’t discuss deeply
personal issues
• Anxiety about school
• Anxiety about self• Identity• Appearance
• Anxiety about life• No cash, no car• Uneasy with ADLs• Highly dependent on others
• “Bored”• Understimulated• Underappreciated• Uncertain
15
The recent crucible…
• Police• Arrest; overcharging• Inappropriate release• 5 encounters since September
• 72 hr. “crisis” watch (Fuld)• Sedated with Haldol• Released with no plan
• Hampton House• Involuntary• 3 unit changes in 18 days• Uncoordinated judicial ruling• Rushed, botched discharge
• PACT• Dropped handoff• 11 days without services
• Princeton House • OutPx: “Inappropriate for PHP”• InPx: Voluntary Involuntary• Major meds changes• But only 2 weeks…
• TPH• Different diagnosis• Overcrowding, fighting• Psychiatrist assaulted
16
…, 2
• Princeton House• “Why TPH only 2 weeks?”• PHP, IOP
• Greater Trenton• Depressing experience• No psychiatrist contact• Problems in adjusting meds
• Beck Institute• Long trips• Inconclusive results?
• Legal case• Stressful preparation• Court appearance• Community service• Reporting
• Job search• No support• No responses, except…• CVS’s response
• 3 ER visits in 2 weeks
• Family stress
17

In the last 10 months…
18
Police encounters 5Arrests 1Calls to Crisis Center 3Hospitalizations 10Outpatient programs 3Court appearances 1Prescribing psychiatrists/APNs 14Diagnoses 3Meds changes over 10Outside Therapists 2Group sessions InnumerableInstitutional case managers 12Ambulance rides 6
Result?...
19
VoicesFears of depressionAnxiety, DoubtUncertaintyUnresolved issuesNo controlSide effects
Police encountersLegal recordBotched transitionsChanging treatmentsHarsh medicatingLack of care continuumOscillating moodsNo available jobStigma
+
Trauma Pain Despair?
Recently expressed desires• A simple job• Good health and body• Music• Become a Mason• One on one counseling• Live at home• Esoterica
20
What these need…• Diligence• Consistency• Skills• Achievement
• Sobriety• Symptom control
21

How to get these?...• Reduce the voices…
• Medications carefully applied• Therapy mindfully engaged
• Arrest the drinking…• Supports firmly established• Temptations avoided (i.e., “Boredom”)
• Go at the right pace.
• Enhance skills, increase experience
• Grow more confidence
22
Best approach?...• Holistic approach (not just meds)• Full family and team support• Patience, consistency, steadiness, calm• Good resources and methods
• Time
23

A future vision
• In 5 years…• Five years sober• Fewer voices• Finishing school with B.A.• Working PT in music store• Member of Masonic lodge• Living in supported housing• Friendship group membership• Wellness training• Sharing with parents
• In 10 years…• 10 years sober• No voices• Assistant manager• FT job• Financially more secure• Working to exit SSI/SSD• Significant other• Wellness living• Helping parents
24
Optimal Tx Plan
25
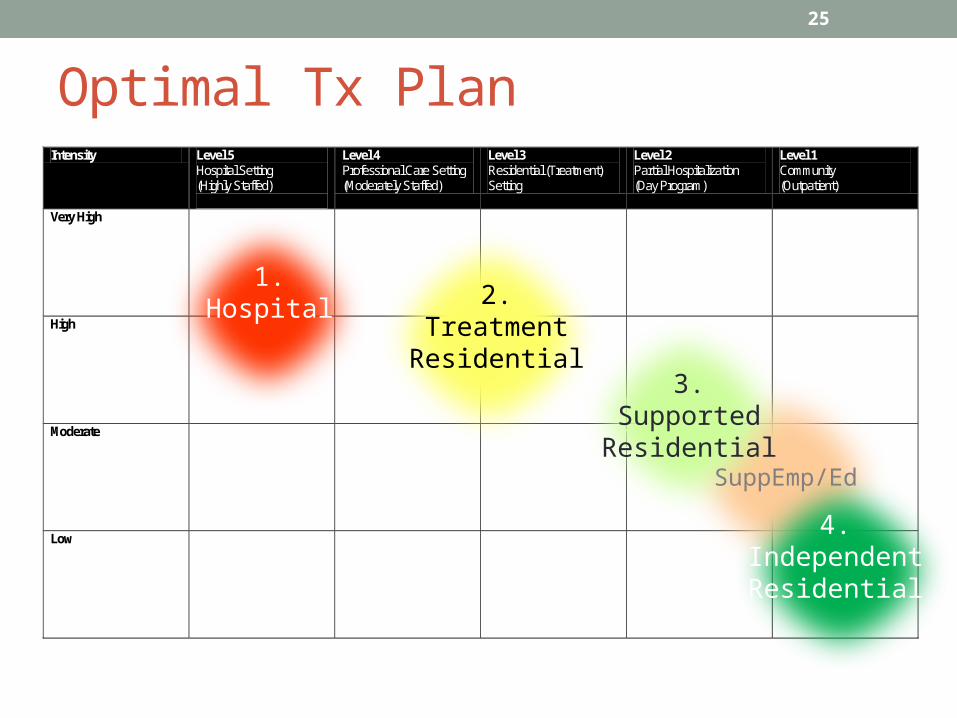
Intensity Level 5 Hospital Setting (Highly Staffed)
Level 4 Professional Care Setting (Moderately Staffed)
Level 3 Residential (Treatment) Setting
Level 2 Partial Hospitalization (Day Program)
Level 1 Community (Outpatient)
Very High
High
Moderate
Low
1.Hospital
Need(IDDT)
2.TreatmentResidential
3.SupportedResidential
4. IOP
4.IndependentResidential
SuppEmp/Ed

The Gap
26
Intensity Level 5 Hospital Setting (Highly Staffed)
Level 4 Professional Care Setting (Moderately Staffed)
Level 3 Residential (Treatment) Setting
Level 2 Partial Hospitalization (Day Program)
Level 1 Community (Outpatient)
Very High
High
Moderate
Low
Hospital
4.IndependentResidential
Gap(Integrated Dual
Disorder Treatment)
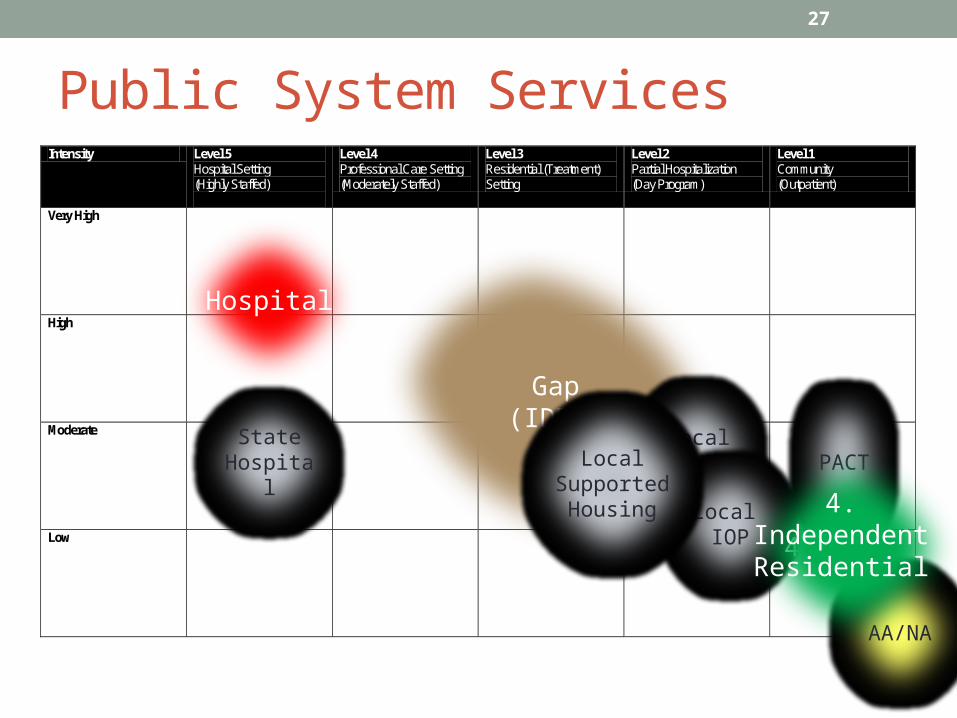
Public System Services
27
Intensity Level 5 Hospital Setting (Highly Staffed)
Level 4 Professional Care Setting (Moderately Staffed)
Level 3 Residential (Treatment) Setting
Level 2 Partial Hospitalization (Day Program)
Level 1 Community (Outpatient)
Very High
High
Moderate
Low
Hospital
Gap(IDDT)
PACTLocalPHP
Local IOP
State Hospital
Local Supported Housing
Hospital
AA/NA
4. IOP
4.IndependentResidential
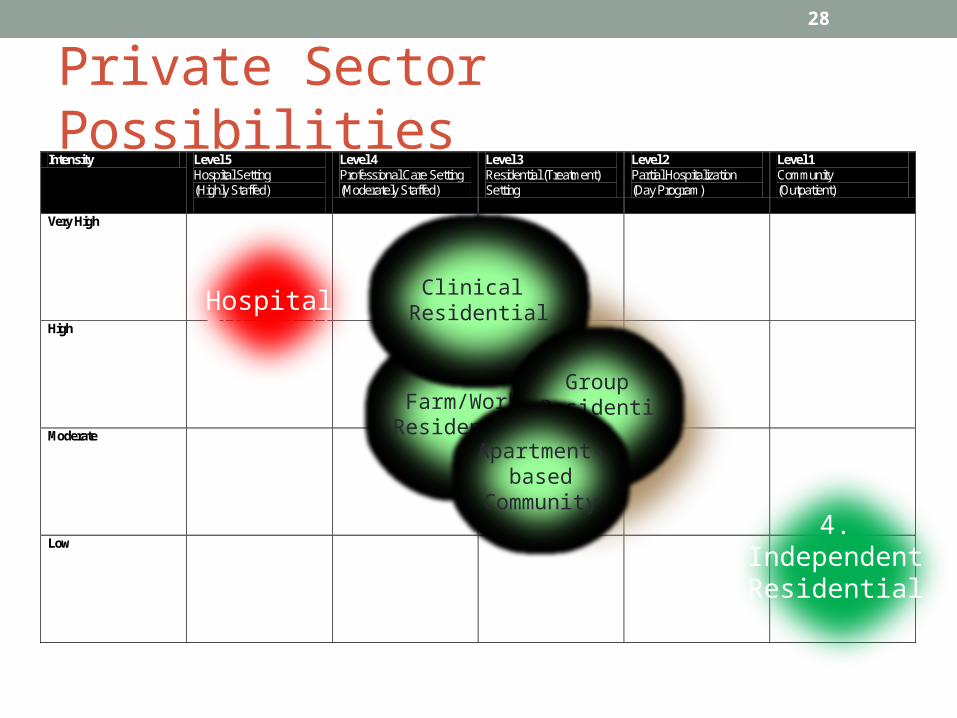
Private Sector Possibilities
28
Intensity Level 5 Hospital Setting (Highly Staffed)
Level 4 Professional Care Setting (Moderately Staffed)
Level 3 Residential (Treatment) Setting
Level 2 Partial Hospitalization (Day Program)
Level 1 Community (Outpatient)
Very High
High
Moderate
Low
Hospital
Need(IDDT)
Farm/Work Residential
Clinical Residential
HospitalHospital
4. IOP
4.IndependentResidential
GroupResidential
Apartment-based
Community

What Private Sector approaches?• Long term residential clinics
29

… 2• Private long-term residential therapeutic communities
30
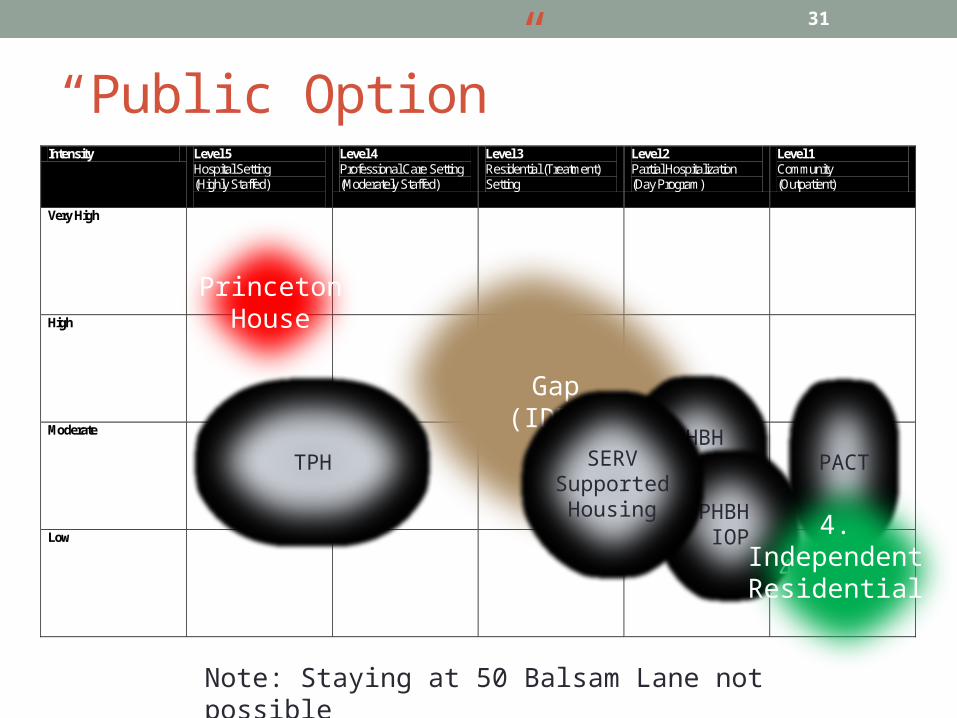
“Public Option”
31
Intensity Level 5 Hospital Setting (Highly Staffed)
Level 4 Professional Care Setting (Moderately Staffed)
Level 3 Residential (Treatment) Setting
Level 2 Partial Hospitalization (Day Program)
Level 1 Community (Outpatient)
Very High
High
Moderate
Low
Hospital
Gap(IDDT)
PACTPHBHPHP
PHBH IOP
TPH SERVSupported Housing
PrincetonHouse
4. IOP
4.IndependentResidential
Note: Staying at 50 Balsam Lane not possible
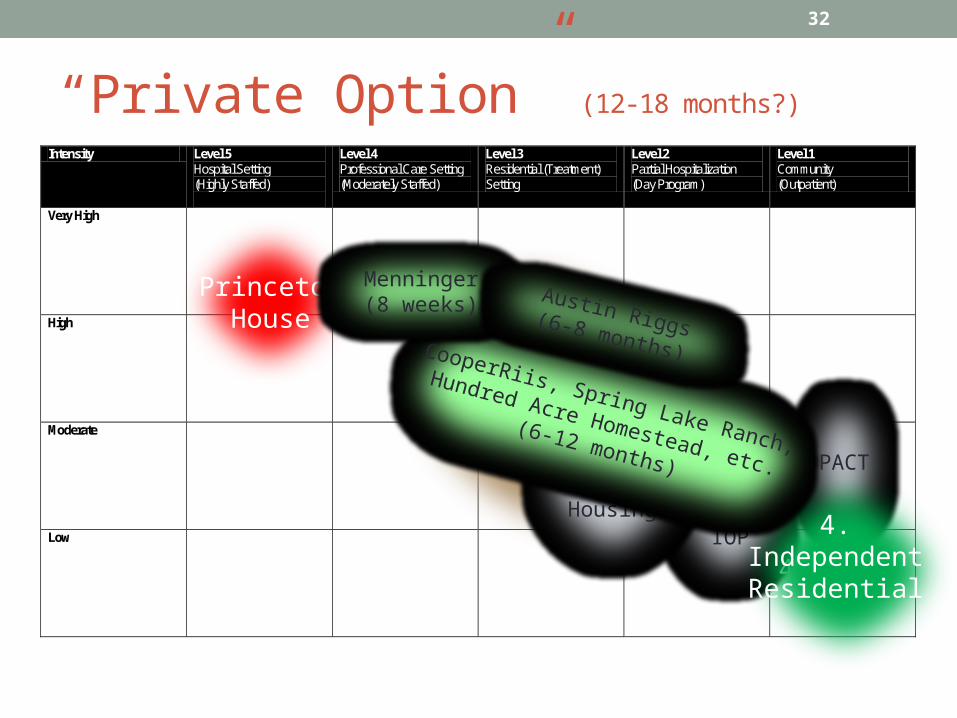
“Private Option” (12-18 months?)
32
Intensity Level 5 Hospital Setting (Highly Staffed)
Level 4 Professional Care Setting (Moderately Staffed)
Level 3 Residential (Treatment) Setting
Level 2 Partial Hospitalization (Day Program)
Level 1 Community (Outpatient)
Very High
High
Moderate
Low
Hospital
Gap(IDDT)
PACTPHBHPHP
PHBH IOP
SERVSupported Housing
PrincetonHouse
4. IOP
4.IndependentResidential
Need(IDDT)
CooperRiis, Spring Lake Ranch,
Hundred Acre Homestead, etc.(6-12 months)
Menninger(8 weeks) Austin Riggs(6-8 months)

Private Option requirements• 30 days of sobriety• No benzodiazepines• Interviews• Consultations• Documentation• Sizeable prepayments• Travel arrangements
• Research and clarification of options• Personal motivation
33
Future ways ahead• Private Option
• PH Therapeutic Clinic Therapeutic Community Transition Residential Local SuppHous and SuppEmp, etc. Independent Living
• At 50 Balsam Lane, if desirable
• Public Option
• PH PHP IOP Local SuppHous and SuppEmp, etc. Independent Living
• At Griggs Farm or elsewhere
34
Next Steps…• Think and talk about this… Take time to decide…• Timing: assure enough to bridge smoothly
• “Private option” is time-unlimited• But, likely only available once• What will be its “value”?
35

To do• ICMS
• Mobilize for public option• Supported housing, supported employment
resources, day programs
• Mobilize psychiatrist• Help integrate private and public options• Facilitate court reporting
• Princeton House• Provide bridging to transition• Accommodate preparation requirements of
private option• Assist loved one with one-to-one
counseling in the decision making• Facilitate loved one’s access to Family
Therapist and ICMS worker
• Family Therapist• Be available to loved one• Assist in consideration of options• Consult with PH and ICMS • Advise individuals and whole family
• Attorney• Facilitate PTI accommodation• Guard client against undue legal actions
• Family• Mobilize for private option• Support its loved one• Assist all possible ways
• Loved one• Be open minded; talk to others; state preferences• Choose
36