Embed Size (px)
Citation preview

10/13/2019
1
Pain and Addiction Treatment—Best Practices
Kirk Moberg, MD, PhD, FASAMUnityPlace Illinois Institute for Addiction Recovery
Clinical Professor of Internal Medicine and PsychiatryUniversity of Illinois College of Medicine
Appalachian Addiction and Drug Abuse ConferenceMorgantown, WVOctober 18, 2019
Disclosures
• Dr. Moberg has disclosed no conflicts ofinterest.
Objectives1- Case studies on best practices for indication of opioids in chronic paintreatment, general characteristics, including toxicities and drug interactions.2- Case studies on risk assessment and tools, examination and evaluation ofthe pain patient.3- Case studies on the initiation and ongoing management of chronic painpatient treated with opioid based therapies, including treatment objectives;monitoring and periodic review; referrals and consultations; informedconsent; prescription of controlled substance agreements, urine screens andpill counts; patient education on safe use, storage and disposal of opioids;discontinuation of opioids for pain due to lack of benefits or increased risks;documentation and medical records.4- Describe and explain the epidemiology of chronic pain and misuse ofopioids including the economic social impact5- To describe the tactics and behaviors of best practices of suspected doctorshopping, drug seeking and drug diversion.6- Understand best practice methods for working with patients suspected ofdrug seeking behavior, diversion and other aberrant behavior

10/13/2019
2
Agenda• Chronic pain• The opioid epidemics• Opioid addiction• Chronic pain treatment
Agenda
• Chronic pain• The opioid epidemics• Opioid addiction• Chronic pain treatment

10/13/2019
3
Pain—anotherco-existing disorder
“ Pain is viewed as a biopsychosocialphenomenon that includes sensory, emotional,cognitive, developmental, behavioral, spiritualand cultural components. ” (IASP website)
“ Pain is whatever the experiencing person saysit is, existing whenever he says it does. ”(McCaffrey 1968)
“ An unpleasant sensory and emotionalexperience associated with actual or potentialtissue damage or described in terms of suchdamage. ” (IASP 1994)
7 | © ASAM 2013
Pain classification
Acute pain Less than three months
Chronic pain Three months or greater
Treede et al. A Classification of Chronic Pain for ICD-11. Pain. 2015;156(6):1003-1007.
But more importantly
Chronic pain Lasts longer than thenormal healing time.
Serves no biologicpurpose.
Treede et al. A Classification of Chronic Pain for ICD-11. Pain. 2015;156(6):1003-1007.

10/13/2019
4
CategoryPain Persistence (Last3 Months)
Pain Bothersomeness (LastTime You Had Pain)
Pain free No pain in last 3 months Not applicable
Category 1 pain
Definition Some days A little pain
Category 2 pain
Definition 1 Most or every day A little pain
Or
Definition 2 Some days Between a little and a lot
Category 3 pain
Definition 1 Some days A lot
Or
Definition 2 Most or every day Between a little and a lot
Category 4 pain
Definition Most or every day A lot of pain
Nahin. Estimates of Pain Prevalence and Severity in Adults: United States, 2012. J Pain. 2015;16(8):769-80.
Pain Prevalence
Nahin. 2015.
Pain Prevalence

10/13/2019
5
Nahin. 2015.
Psychological Impact
Nahin. 2015.
Disability
Nahin. 2015..
Accessing the Health Care System

10/13/2019
6
Pain is costly
All figures in $billion/year in 2010 dollars
$560 – $635ComparisonsCardiovascular disease—$309Cancer—$243Injury and poisoning—$205Endocrine, Nutritional and Metabolic disease—$127Gastrointestinal disease—$112Respiratory disease—$112
Gaskin & Richard. The Economic Costs of Chronic Pain in the United States. J Pain. 2012;13(8):715-24.
Pain is costly
Incremental health care costs of pain—$261 - $300 billion
Lost productivity due to pain—$299 - $334 billion
Gaskin and Richard. 2012.

10/13/2019
7
Agenda
• Chronic pain• The opioid epidemics• Opioid addiction• Chronic pain treatment
A Triphasic Epidemic
PrescriptionOpioids
Heroin Fentanyl

10/13/2019
8
SOURCE: CDC, Prescription Opioid Data
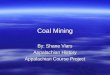
Prescription Opioids
Opioid Overdose US Prescribing Rate Maps. cdc.gov/drugoverdose/maps/rxrate-maps.html
<64.164.1-82.983-107.1>107.1
Prescriptions per 100 people—2016
126 96
47,600
WV
US2017
2014
81
Prescribing Rates (per 100 people)
2016 2017
Opioid Prescribing Rates & Overdose Deaths
833WV2017
https://www.cdc.gov/drugoverdosehttps://www.kff.org/state-category/health-status/opioids/
Opioid Overdose Deaths

10/13/2019
9
Past Year Misuse of Prescription Pain Reliever Subtypes amongPeople Aged 12 or Older: 2017
Bose et al. Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Surveyon Drug Use and Health. 2018. samhsa.gov/data/
Heroin then…
Ciccarone. Heroin in Brown, Black and White: Structural Factors and MedicalConsequences in US Heroin Market. Int J Drug Policy. 2009;20(3):277-82.
…and now

10/13/2019
10
McCance-Katz. The National Survey on Drug Use and Health: 2017. US Department of Health and Human Services.
Fentanyl
Armenian et al. Fentanyl, Fentanyl Analogs and Novel Synthetic Opioids: A Comprehensive Review.Neuropharmacology. 2018;134:121-132.

10/13/2019
11
Lethal dose
McDermott. N.H. Medical Examiner: At Least 10 Overdose Deaths in 2017 Traced to Carfentanil. New Hampshire PublicRadio, July 13, 2017. nhpr.org.Callejas. Opioid Epidemic Part 2: Stronger and Deadlier. July 29, 2017. inmaricopa.com.
Agenda• Chronic pain• The opioid epidemic?• Opioid addiction• Chronic pain treatment
Opioid Use Disorder in the Past Year among People Aged 12or Older, by Age Group: 2017
Bose et al. Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Survey onDrug Use and Health. 2018. samhsa.gov/data/

10/13/2019
12
The Cost of Opioid Addiction(2013 dollars)
$78.5 billion
Florence et al. The Economic Burden of Prescription Opioid Overdose, Abuse and Dependence In the United States.Medical Care. 2016;54(10):901-906.
The Economic Burden of Prescription Opioid Overdose, Abuse, and Dependence in the United States,2013.Florence, Curtis; Zhou, Chao; Luo, Feijun; Xu, LikangMedical Care. 54(10):901-906, October 2016.DOI: 10.1097/MLR.0000000000000625
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. Publishedby Lippincott Williams & Wilkins, Inc.
But it’s more than opioids

10/13/2019
13
The Addictions“Certain People Use Certain Substances
in Certain WaysThought at Certain Times
to Be Unacceptableby Certain Other People
for Reasons Both Certain and Uncertain.”
Burglass & Shaffer. Diagnosis in the Addictions I: Conceptual Problems. Adv Alc Subst Abuse. 1984;3(1-2):19-34.
Substance Use Disorders in Perspective
• Substance Use Disorder—20.1 million• Alcohol Use Disorder—15.1 million• Alcohol Related Deaths—100,000 per year• Past month tobacco use—63.4 million• Tobacco Related Deaths—450,000 per year• Opioid Use Disorder—2.1 million
Ahrnsbrak et al. 2017.Tobacco Related Mortality. 2016. cdc.gov.Alcohol Facts and Statistics. 2017. niaaa.nih.gov.
It’s your fault

10/13/2019
14
Agenda• Chronic pain• The opioid epidemic?• Opioid addiction• Chronic pain treatment
False dichotomies
…or else what?
OR

10/13/2019
15
Depression, Catastrophic ThinkingInfluence Pain
Pain catastrophizing:predictor of pain intensity and interference
Depression:predictor for perceived disability
based on physical functioningBaxter et al. The Role of Psychosocial Factors in the Pain Experience: the Relationship Between Depression, Catastrophizingand Chronic Pain. Pain. 2016;17(4S):S97-S98.
Non-pharmacologic techniques
Cognitive BehavioralTherapy
MotivationalInterviewing
Mindfulness RelaxationTechniques
Chronic pain is not monolithic

10/13/2019
16
Highly COX-1Selective
Relatively COX-1 Selective
EquallySelective
Relatively COX-2 Selectivee
Highly COX-2Selective
Flurbiprofen Fenoprofen Aspirin Diclofenac MK-966(Refecoxib)
Ketoprofen Piroxicam Ibuprofen Etodolac SC-58635(Celecoxib)
Sulindac Indomethacin Meloxicam L-743,337
Ketorolac Nabumetone NS-398
Naproxen Nimesulide SC-58125
Oxaprosin 6-MNA
Tenoxicam
Tolmetin
Table 3. General Ranges of COX Isoform Selectivity of Currently Available NSAIDsand of COX-2 Selective Inhibitors in Development
Cryer & Dubois. The Advent of Highly Selective Inhibitors of Cyclooxygenase—A Review. Prosta-glandins &Other Lipid Mediators. 1998;56:341-61.
Case Discussion: Jacob
Jacob, a 30 year old man who sufferswith fibromyalgia.
What is the best opioid for him?

10/13/2019
17
Name Substance Class Mechanism ofAction
RecommendedDosage
Grade ofRecommen-dation
Amitriptyline TCA Inhibition of NEand 5HTtransporter (1);*
10-50 mg/day Weak for
Cyclobenzaprine TCA derivative 1; ** 10-40 mg/day Weak for
Duloxetine SNRI 1 20-120 mg/day Weak for
Milnacipran SNRI 1 100-200 mg/day Weak for
Pregabalin Anti-convulsant Modulation ofa2d subunit ofpresynaptic Cachannel (2);
300-450 mg/day Weak for
Gabapentin Anti-convulsant 2; increasedGABA turnover
1200 mg/day Weak for
Tramadol Opioid m agonist; 1 150 mg/day Weak for
*5-HT2A, 5-HT2C, 5-HT6, 5-HT7 receptor antagonism**5-HT2A receptor antagonism
GRADE system for making recommendations
modified from Schmidt-Wilcke & Diers. 2017.
Case Discussion: Jacob
Jacob, a 30 year old man who sufferswith fibromyalgia.
What is the best opioid for him?
What if he suffers with alcohol use disorder?
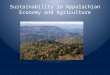
Gabapentin and Opioids
Low dose < 900 mg/dayModerate dose 900-1799 mg/dayHigh dose > 1800 mg/day
Gomes et al. Gabapentin, Opioids, and the Risk of Opioid-Related Death: A Population-Based Nested Case-ControlStudy. PLOS Medicine. 2017;14(10):e1002396.

10/13/2019
18
Gabapentin and Opioids
Low dose < 900 mg/dayModerate dose 900-1799 mg/day (1.56)High dose > 1800 mg/day (1.58)
Very high dose > 2500 mg/day (1.83)
Gomes et al. 2017.
Gabapentin and Opioids
Low dose < 900 mg/dayModerate dose 900-1799 mg/day (1.56)High dose > 1800 mg/day (1.58)
Very high dose > 2500 mg/day (1.83)
Age, opioid dose, other medications (pregabalin, SSRIs, other anti-depressants, benzodiazepines, other psychotropic drugs, long-actingopioids, methadone, buprenorphine), number of medications prescribed,alcohol use disorder, COPD, DM, Charlson index, number of opioidprescribers, number of pharmacies, NSAID use.
Gomes et al. 2017.

10/13/2019
19
Summary of 2016 CDC guidelines• Non-pharmacologic and non-opioid treatments preferred.• Establish treatment goals• Immediate release first• Lowest dose preferable; caution when exceeding 50
Morphine Milligram Equivalents• Avoid exceeding 90 MME• For acute pain only prescribe what is expected• Evaluate response to opioids one 1-4 weeks after initiation
for chronic pain• If benefits do not outweigh harms taper and discontinue
Frieden TR & Houry D. Reducing the Risks of Relief—The CDC Opioid-Prescribing Guideline. NEJM. 2016;374(16):1501-4.Dowell D, Haegerich TM, Chou R. CDC Guidelines for Prescribing Opioids for Chronic Pain-United States 2016. MMWRRecomm Rep. 2016;65(1):1-49.
Mitigate Risk
Refer for…
…Treatment

10/13/2019
20
Prescription Drug Monitoring Program
PDMP Outcomes
Opioid Prescribing Behavior (2/6)
Opioid Diversion and Supply (2/2)
Opioid Misuse (1/1)
Opioid Related Morbidity/Mortality (3/6)
Finley et al. Evaluating the Impact of Prescription Drug Monitoring Program Implementation: A Scoping Review. BMCHealth Serv Res. 2017;17(1):420.

10/13/2019
21
Non-fatal and Fatal Overdoses
Fink et al. Association Between Prescription Drug Monitoring Programs and Nonfatal and Fatal Drug Overdoses: ASystematic Review. Ann Int Med. 2018;168(11):783-790.
Evidence insufficient
even for heroin
Recent Use
Drug Screen ResultsOpiates present
A. FentanylB. MorphineC.NaltrexoneD.CodeineE. MethadoneF. BuprenorphineG.HydrocodoneH.MeperidineI. OxycodoneJ. 6-monoacetyl-morphineK.Propoxyphene

10/13/2019
22
Drug Screen ResultsOpiates present
A. FentanylB. MorphineC.NaltrexoneD.CodeineE. MethadoneF. BuprenorphineG.HydrocodoneH.MeperidineI. OxycodoneJ. 6-monoacetyl-morphineK.Propoxyphene
Case: Henry, UDT
Henry is 42 years old and was injured in an MVA several years ago.He underwent a THR with 2 revisions later on because of infectiouscomplications. He has been prescribed 40 mg oxycodone ER twice dailyand an “occasional diazepam.” He is switching primary care providers andpresents asking for an oxycodone refill.
He denies the use of any other drugs.
You order a UDT.
Case: Henry, UDT

10/13/2019
23
Case: Henry, UDT
He states,
“Your lab screwed up.It’s not my urine. I’ll doanother test right now.”
Case: Henry, UDT
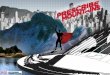
EXAMPLES OF OPIOIDMETABOLISM
*6-MAM=6-Monoacetylmorphine
CODEINE MORPHINE 6-MAM* HEROIN
HYDROCODONE HYDROMORPHONE
OXYCODONE OXYMORPHONE
T½=25 – 30 Min T½=3 – 5 Min
POPPY SEEDS

10/13/2019
24
“ OK, doc. I did use cocaine twice.Once on Jan 1 and once on Feb 1. Noother times.”
What is going on?
What do yourecommend?
Abuse deterrent opioids• Oxycodone/naloxone ER
– Targiniq ER®• Buprenorphine/naloxone
– Generic– Suboxone®– Zubsolv®– Bunavail®
• Morphine sulfate/naltrexone ER– Embeda®
• Oxycodone/naltrexone ER– Troxvca ER®

10/13/2019
25
Abuse deterrent opioids• Hydrocodone ER
– Hysingla ER®– Zohydro ER®– Vantrela ER®
• Hydromorphone ER– Embeda®
• Oxycodone ER* and IR**– *Oxycontin®– *Xtampza®– **Oxaydo®– **Roxybond® (4/20/2017)
• Morphine sulfate ER– Arymo ER®
2010
Cicero & Ellis. Abuse Deterrent Formulations and the Prescription Opioid Abuse Epidemic in the United States LessonsLearned from OxyContin. JAMA Psychiatry. 2015;72(5):424-430.
Deprescribing

10/13/2019
26
Deprescribing
Deprescribing
DeprescribingWithdrawal Treatment
Clonidine/LofexidineDicyclomine
AntihistaminesAntiemetics
AntidiarrhealsNSAIDS

10/13/2019
27
Loperamide
St. Louis. Addicts Who Can’t Find Painkillers turn to Anti-Diarrhea Drugs. New York Times, 5/10/2016Eggleston et al. Loperamide Abuse Associated with Cardiac Dysrhythmia and Death. Ann Emerg Med. 2017;69(1):83-86.Katselou et al. “Poor Man’s Methadone” Can Kill the Poor Man. Extra-medical Uses of Loperamide: A Review. ForensicToxicology. 2017;35(2):217-231.
KratomMitragyna speciosa
Summary
• Chronic pain is pervasive and complex.

10/13/2019
28
Summary
• Chronic pain is pervasive and complex.• Opioids are not first-line medications for
chronic pain.
Summary
• Chronic pain is pervasive and complex.• Opioids are not first-line medications for
chronic pain.• Opioids can be prescribed safely.
Summary
• Chronic pain is pervasive and complex.• Opioids are not first-line medications for
chronic pain.• Opioids can be prescribed safely.• Opioid addiction is part of a larger epidemic.

10/13/2019
29