Embed Size (px)
Citation preview

1
Advanced Carotid US
Interpretation
Leslie M. Scoutt, MD, FACR, FSRU, FAIUMProf of Diagnostic Radiology , Surgery & Cardiology
Vice Chair, Dept of Radiology & Biomedical Imaging
Medical Director, Non-Inv asiv e Vascular Lab
Yale School of Medicine
DISCLOSURES
• Educational consultant for Philips Healthcare
• Will discuss the use of IV US contrast to evaluate plaque, not FDA approved for vascular imaging
OBJECTIVES
• Understand the pathophysiology of stroke
– most strokes are embolic
– 20% due to disease at the carotid bifurcation
– begin by evaluating the plaque
OBJECTIVES
• While the chart is important…..
• Know when the charts don’t work– tortuous vessels, contralateral stenoses/occlusions
– tandem, long segment, near occlusive lesions
– high and low output states
– post intervention
• ALWAYS correlate spectral Doppler w/ grayscale, color Doppler, and waveforms– explain any discordance
OBJECTIVES
• Discuss the significance of abnormal carotid waveforms
– tardus parv us w aveform
– high resistance w av eform
VULNERABLE PLAQUE
• Risk of rupture + embolization related to
– v ascularity in plaque
– intra-plaque hemorrhage
– inflammation
– lipid content
– necrotic core
– thinning of fibrous cap
Courtesy Dr Ed Bluth

2
STABLE PLAQUE
• Hyalinized, fibrous, calcified plaque
– few er v essels
– less inflammation
– smooth surface
• Less likely to rupture
• Nothing for high velocity jet to knock off and embolize Courtesy Dr Ed Bluth
VULNERABLE PLAQUE:
What can you detect w/ US?
• Hemorrhagic plaque is typically hypoechoic• Irregularly surfaced plaque
– acts as a nidus for platelet aggregation
• The more plaque there is, the more likely it is to be friable
• Both ↑ vascularity and inflammation in plaque may be detectable with IV US contrast
PLAQUE: Echogenicity
• Hemorrhagic plaque is hypoechoic
– esp w orrisome if > 50%
PLAQUE: Echogenicity
• Extremely hypoechoic plaque may only be seen on color Doppler imaging
– signal v oid
PLAQUE: Echogenicity
• Hypoechoic plaque is a non-specific finding, esp if homogeneous
– hy alinized, fibrous, fatty plaque
PLAQUE: Echogenicity
• Extremely hypoechoic homogeneous plaque may represent thrombus/acute hemorrhage
– most unstable or “v ulnerable” plaque of all

3
PLAQUE: Surface Characteristics
• Irregular, fissured, undermined, ulcerated
• Often best evaluated with color or power Doppler
PLAQUE: Surface Characteristics
• Ulcers: US findings are non-specific
– histologic rather than morphologic diagnosis
– deeper than 2 mm, confirm in tw o planes
STABLE PLAQUE
• Echogenic, smooth surface
PLAQUE: How Much?
• Large plaques often hemorrhagic
• > 90% stenosis may have ↑ risk of stroke
• Large amount of plaque as assessed by 3D US assoc w/ elevated coronary artery calcium score on cardiac CT
Sillesen, JACC: 2012
PLAQUE: How Much?
• Before you start the spectral Doppler exam
– know w here the plaque is
– hav e a good sense of the degree of stenosis
• Helps guide & Q/A the spectral Doppler exam
– spectral Doppler findings should be concordant w ith amount
of plaque
Q/A DOPPLER EXAM

4
• Good for evaluation of plaque burden
– ov erestimate % stenosis c/w NASCET criteria
• Confirm findings on sagittal images
– make sure y ou are not off center, esp
if plaque is irregular
• Consider TRV cine clip of bulb
TRANSVERSE IMAGES TRANSVERSE IMAGES
• Incorrect gain– too low – plaque w ill look falsely hy poechoic
– too high – w ill miss hy poechoic areas
PLAQUE: Pitfalls PLAQUE: Pitfalls
• Color blooming may obscure plaque and underestimate stenosis
• Feinstein et al, J Am Coll Card: 2006
– early phase IV contrast enhanced US identified surface
ulcers and plaque neov ascularity
• Coli et al, J Am Coll Card: 2008
– CE of plaque correlated w / histologic density of
neov essels and hy poechoic plaque
• Giannoni et al, Eu J Vasc Endovasc Surg: 2008
– CE of plaque correlated w / Sx (acute neurologic ev ent)
PLAQUE: Vascularity
Copy right ©2006 Am eric an Col lege of Card io logy Foundation. Res tric tions m ay apply.
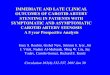
Feinstein et al, J Am Coll Cardiol
2006; 48: 236-243
Unenhanced (A) & contrast enhanced (B) US images of the carotid artery
Ulceration only seen on CE
image

5
Copy right ©2006 Am eric an Col lege of Card io logy Foundation. Res tric tions m ay apply.
Feinstein et al, J Am Coll Cardiol 2006; 48: 236-243
Copy right ©2006 Am eric an Col lege of Card io logy Foundation. Res tric tions m ay apply.
Photomicrograph: ↑ number of endothelial cells in carotid plaque
Feinstein et al, J Am Coll Cardiol 2006; 48: 236-243
• Microbubbles adhere to damaged epithelium and taken up by inflammatory cells
– monocy tes, macrophages
• Owen et al, Radiology: 2010
– ↑ late phase CE of plaque correlated w / Sx and
hy poechoic plaque
– believ e they are identify ing inflammatory plaque
PLAQUE: Inflammation
Non-CE image: Carotid lumen (white arrowhead), Carotid plaque (green arrowhead)
©2010 by Radio log ic a l Soc iety of North Am eric a
Owen DR et al, Radiology 2010; 255: 638-644
Late-phase CE image shows a lower density of contrast agent microbubbles in
the carotid lumen (white arrowhead) compared with that inside the carotid
plaque (green arrowhead)
Owen DR et al, Radiology 2010; 255: 638-644©2010 by Radio log ic a l Soc iety of North Am eric a
• Has been accepted as a good measure of CVD risk
• However, the jury is still out….
• New studies suggest that IMT assessment w/ US does not improve CVD risk stratification enough to be clinically significant
• Current thought is that MR might be better
– includes assessment of adv ential lay er and v asa v asorum
INTIMA-MEDIA THICKNESS

6
WHY DO WE GRADE CAROTID STENOSES?
• Patients with carotid stenosis derive a clear benefit, ↓ incidence of stroke, from carotid endarterectomy (CEA)– North American Sy mptomatic CEA Trial
(NASCET, 1991)
– Asy mptomatic Carotid Atherosclerosis Study (ACAS, 1995)
– European Carotid Surgery Trial (ECST, 1991)
– Asy mptomatic Carotid Surgery Trial (ACST, 2004)
SRU 2002 CONSENSUS CONFERENCE
Grant et al, Radiology: 2003
DISCORDANCE BTWN GRAYSCALE
& DOPPLER FINDINGS
• PSV elevated
• But no plaque!
– tortuous v essel
– contralateral occlusion/stenosis
TORTUOUS VESSEL
PSV = 163 cm/s
50-69% stenosis?
TORTUOUS VESSEL
• Velocity increases around a curve
• Difficult to assign correct Doppler angle as direction of blood flow changes rapidly
CONTRALATERAL HI-GRADE
STENOSIS/OCCLUSION
PSV = 260 cm/s< 50% stenosis

7
CONTRALATERAL HI-GRADE
STENOSIS/OCCLUSION
• ↑ PSV in CCA and ICA, esp at a stenosis
• Variable, unpredictable
• Correlation ↓ as contralateral stenosis ↑
• Use of PSVR may not compensate, but probably better than using PSV alone
Beckett, AJNR: 1990
AbuRahma, J Vasc Surg: 1995
Busuttil, Am J Surg: 1996
DISCORDANCE BTWN GRAYSCALE &
DOPPLER FINDINGS
• Plaque – LOTS!
• But velocity not as elevated as one would expect
– tandem lesions
– long segment stenosis
– > 95% stenosis
TANDEM LESIONS
• PSV < expected for a given % stenosis
LONG SEGMENT STENOSIS
LONG SEGMENT STENOSIS
• If plaque extends over more than 2 cm
– PSV w ill , diastolic v elocity usu remains high
• Likely due to increased in-flow resistance
– proportional to length of stenosis
TIGHT STENOSIS

8
Spencer and Reid, Stroke: 1979
CLUES TO A TIGHT STENOSIS
• diameter of lumen on grayscale and/or color images
• “Knocking”, “Thump”, or “Staccato” waveform proximally
• Tardus parvus waveform distally
TIGHT STENOSIS
Proximal CCA Distal ICA
TARDUS PARVUS WAVEFORM
• Delayed systolic upstroke
• Decreased PSV
• Rounded systolic peak
• Occurs distal to a high grade stenosis
• Pattern of distribution can help localize stenosis
• Rt CCA, Lt CCA & both VAs
TARDUS PARVUS WAVEFORM
• Note: ↓ PSV
• Seen in SEVERE Aortic Stenosis
TARDUS PARVUS WAVEFORM

9
TP in Rt CCA & ICA, Reversed flow Rt VA
Normal sharp upstroke in Lt CCA
Stenosis of Innominate Artery
TP in Lt CCA & Lt ICASharp upstroke on Rt and in both VAs
Stenosis at Origin of Lt CCA
• Low PSV
• Decreased, absent or reversed diastolic flow
• Occurs prox imal to an occlusion or high grade stenosis
“KNOCKING” WAVEFORM
• Asymmetry of Rt & Lt CCA waveforms
• ↓ diastolic flow in Lt CCA

10
• More pronounced in Lt ICA↓ PSV & EDV: RT CCA
↓ PSV & EDV: RT ICA RT MCA OCCLUSION
BILATERAL ↓ PSV & EDV in ICAs INCREASED INTRACRANIAL PRESSURE

11
74 YO FEMALE W/ STROKE BILATERAL DISTAL OCCLUSIONS
BILATERAL ↓ EDV in CCAs
• ↑ PSV
Severe Aortic Regurgitation
WATER HAMMER PULSE
• Severe aortic regurgitation
–sharp systolic upstroke
–normal to PSV
– reversed diastolic flow
–bilateral
–waveform normalizes distally
CCA PSV < 60 cm/s
• Low output states
– ↓ ejection fraction
cardiomyopathies, LV dysfunction, LV aneurysm, AS
– hy potension
– thoracic aortic aneury sm
LOW CARDIAC OUTPUT
• PSV in CCA = 35 cm/s
• When ICA PSV = 230 cm/s, PSVR will be > 6.5
• Relying on PSV will result in underestimation of ICA stenosis
• Grayscale, color Doppler, PSVR more reliable EF = 15%

12
CCA PSV > 100 cm/s
• High output states
– hy pertension
– hy perdy namic state
– aortic regurgitation
– thy rotox icosis
HIGH CARDIAC OUTPUT
• PSV will overestimate % stenosis
• Grayscale, color Doppler & PSVR more reliable
INTRA-AORTIC BALLOON PUMP
• Inflation of balloon causes 2nd peak of forw ard flow during
early diastole
• Flow rev ersal at end of diastole corresponds to deflation of
balloon
INTRA-AORTIC BALLOON PUMP
INTRA-AORTIC BALLOON PUMP
• PSV Lt ICA = 222 cm/s, but PSVR only 2.2
• What % stenosis?
INTRA-AORTIC BALLOON PUMP
• Choose 1st OR 2nd peak to measure PSV and be consistent
• PSVR may be a better Doppler criterion
• Look at grayscale and color Doppler
• May have to turn balloon off or decrease firing ratio

13
WEANING FROM IABP (1:2) LEFT VENTRICULAR ASSIST DEVICE
• Rx of severe heart failure, refractory to medical management
– bridge to my ocardial recov ery or cardiac transplantation
– final Rx for pts w ho are not candidates for cardiac transplant
• Blood diverted from Lt ventricular apex and propelled via pump through Dacron graft into aorta
LVAD
• Marked tardus parvus waveforms in all vessels
• ↓ PSV
– av erage = 32 cm/s
• Monophasic flow – no flow below the baseline
– rarely , nonpulsatile monophasic w av eform w /o perceptible
sy stolic peak
• Similar waveforms in subclavian, mesenteric, femoral arteries
LVAD: US Findings
Cervini, US Quarterly: 2010
LVAD

14
CONCLUSIONS
• Ev aluate plaque carefully
• Hy poechoic, irregularly surfaced plaque ↑ risk for
cerebrov ascular ev ents & more rapid progression
• Estimate % stenosis on gray scale and color Doppler before
the spectral Doppler ex am
– large plaques more often hemorrhagic and friable
– will help you interpret the PSV measurements & Q/A exam
• New techniques: CE, elastography, arterial w all stiffness,
v ector flow
• Standard charts don’t work for
- tortuous v essels, contralateral stenosis/occlusion
- tandem, long segment, near occlusiv e lesions
- high or low output states
- s/p interv ention
• ALWAYS correlate velocity measurements w/
grayscale/color Doppler images & waveforms
CONCLUSIONS CONCLUSIONS
• Waveforms should be symmetric Rt to Lt
• “Knocking” waveform pattern– distal occlusion/high grade stenosis
• Bilateral ↓ EDV but normal to ↑ PSV → AR• Tardus Parvus Waveform
– consider prox imal stenosis
– distribution w ill tell y ou w here bilateral, all v essels → severe AS
CONCLUSIONS
• Use a pattern recognition approach for complex waveform patterns
– often due to iatrogenic conditions
– w av eforms frequently bizarre, quite v ariable
– correlate w / gray scale and color Doppler imaging
DOPPLER CRITERIA
• Whatever criteria you choose,
– the closer y ou are to the cut off v alue, the more likely y ou
are to be w rong
– the farther aw ay you are, the more likely y ou are to be right
• F+ vs F- dependent on sens vs. spec of cut off value
• Consider correlative imaging if close to discriminatory thresholds
• As management algorithms change, so must the chart