Embed Size (px)
Citation preview


Kei Muro, MD.
Department of Clinical Oncology
Aichi Cancer Center Hospital
Nagoya, JAPAN
Where Are We with Check-Point Inhibitors
in Gastric Cancer?
21 June 2018, Barcelona
Session VII: Metastatic Gastric Cancer

Disclosure
Research Funding:
Gilead Sciences, Merck Serono, MSD, Daiichi Sankyo, Sanofi,
Ono, Shionogi, Medisience Planning, Pfizer, and Kyowa Hakko Kirin
Lecture Fee:Chugai, Eli Lilly, Takeda, Ono, Taiho, and Bayer
Kei Muro, MD.

Hayakawa Y, et al. Nature Reviews Cancer 16: 305-318, 2016
Molecular Subtypes of Gastric Cancer

T cell activation
OFF
T cell activation
OFF
Suppression of T cell activation by PD-1/PD-L1(or PD-L2) interaction3)
Escape from immune
surveillance3) Tumor cell
inactivated T cell
Attack against
tumor cells
OFF
Attack against
tumor cells
OFF
tumor cell inactivated T cell
PD-L2
PD-L1
PD-1
antigen-presenting cell(dendritic cells etc.)
1) Chen DS et al. Immunity 39: 1-10, 2013
2) Mellman I et al. Nature 480: 480-489, 2011
3) Pardoll DM. Nat Rev Cancer 12: 252-264, 2012
antigen
presentation1,2)
naïve T cell
Lymph node
tumor-specific antigen
Migration and infiltration of T cells into tumors2)
Editorial supervision:
Division of Cellular Signaling Institute for Advanced Medical Research,
Keio University School of Medicine, Prof. Yutaka Kawakami
Escape from Immune Surveillance

T
cellsactiva
tion
OFF
T
cellsactiva
tion
OFF
Suppression of T cell activation
by PD-1/PD-L1(or PD-L2)
interaction 2,3)
Anti-PD-1 therapy
PD-L2PD-L1
tumor cell
PD-1
activated T cell
PD-L2
PD-L1
PD-1
Anti-PD-1 Therapy
Killing of tumor cells
by reactivation of T
cells5)
Tumor cell
inactivated T cell
Attack against
tumor cells
Attack against
tumor cells
antigen-presenting cell(dendritic cells etc.)
antigen
presentation 1,2)
naïve T cell
reactivation of T cells by suppression of PD-1/PD-L1(or PD-L2) interaction3,4)
Lymph node
tumor-specific antigen
Editorial supervision:
Division of Cellular Signaling Institute for Advanced Medical Research,
Keio University School of Medicine, Prof. Yutaka Kawakami
Cancel of Immunity Suppression
by Anti PD-1 Therapy
1) Chen DS et al. Immunity 39: 1-10, 2013; 2) Mellman I et al. Nature 480: 480-489, 2011
3) Pardoll DM. Nat Rev Cancer 12: 252-264, 2012; 4) Postow MA et al. J Clin Oncol 33: 1974-1982, 2015
5) Topalian SL et al. Curr Opin Immunol 24: 207-212, 2012

Line Study Agent Tested Targeting Control Arm Primary EP
1st ToGA (HER2) trastuzumab HER2 XP/FP OS
LOGiC(HER2) lapatinib HER2 XELOX OS
JACOB (HER2) pertuzumab HER2 XP + trastuzumab OS
AVAGAST bevacizumab VEGF XP OS
AVATAR bevacizumab VEGF XP OS
EXPAND cetuximab EGFR XP PFS
REAL-3 panitumumab EGFR EOX OS
RILOMET-1, 2 rilotumumab MET ECX, XP OS
METGastric onartuzumab MET mFOLFOX6 OS
RAINFALL ramucirumab VEGFR2 XP PFS (OS)
KEYNOTE 062 pembrolizumab PD-1 XP/FP PFS, OS
ATTRACTION-04 nivolumab PD-1 SOX/CapeOX PFS, OS
CheckMate-649 nivolumab,nivo+ipilimumab PD-1 FOLFOX/CapeOX OS in PD-L1+
GS-5745 (Gilead) andecaliximab MMP9 mFOLFOX6 OS
1st maintenance JAVELIN GASTRIC 100 avelumab PD-L1 FOLFOX/CapeOX PFS, OS
2nd TyTAN (HER2) lapatinib HER2 weekly paclitaxel OS
GATSBY (HER2) TDM-1 HER2 weekly paclitaxel OS
RAINBOW ramucirumab VEGFR2 weekly paclitaxel OS
REGARD everolimus mTOR BSC (Placebo) OS
ENRICH nimotuzumab EGFR irinotecan OS
GRANITE2 everolimus mTOR weekly paclitaxel PFS
GOLD olaparib PARP weekly paclitaxel OS
BRIGHTER BBI-608 STAT3 weekly paclitaxel OS
KEYNOTE 061 pembrolizumab PD-1 weekly paclitaxel PFS, OS in PD-L1+
2nd / 3rd GRANITE1 everolimus mTOR BSC (placebo) OS
3rd JAVELIN GASTRIC 300 avelumab PD-L1 Irinotecan/taxane OS
Apatinib Study (China only) apatinib VEGFR2 BSC (placebo) OS
3rd~ ANGEL apatinib VEGFR2 BSC (placebo) OS
ATTRACTION-02 nivolumab PD-1 BSC (placebo) OS
Global RCTs with
Molecular Targeting
Agents (Including PD-(L)1
Ab) for Metastatic GC

Line Study Agent Tested Targeting Control Arm Primary EP
1st ToGA (HER2) trastuzumab HER2 XP/FP OS
LOGiC(HER2) lapatinib HER2 XELOX OS
JACOB (HER2) pertuzumab HER2 XP + trastuzumab OS
AVAGAST bevacizumab VEGF XP OS
AVATAR bevacizumab VEGF XP OS
EXPAND cetuximab EGFR XP PFS
REAL-3 panitumumab EGFR EOX OS
RILOMET-1, 2 rilotumumab MET ECX, XP OS
METGastric onartuzumab MET mFOLFOX6 OS
RAINFALL ramucirumab VEGFR2 XP PFS (OS)
KEYNOTE 062 pembrolizumab PD-1 XP/FP PFS, OS
ATTRACTION-04 nivolumab PD-1 SOX/CapeOX PFS, OS
CheckMate-649 nivolumab,nivo+ipilimumab PD-1 FOLFOX/CapeOX OS in PD-L1+
GS-5745 (Gilead) andecaliximab MMP9 mFOLFOX6 OS
1st maintenance JAVELIN GASTRIC 100 avelumab PD-L1 FOLFOX/CapeOX PFS, OS
2nd TyTAN (HER2) lapatinib HER2 weekly paclitaxel OS
GATSBY (HER2) TDM-1 HER2 weekly paclitaxel OS
RAINBOW ramucirumab VEGFR2 weekly paclitaxel OS
REGARD everolimus mTOR BSC (Placebo) OS
ENRICH nimotuzumab EGFR irinotecan OS
GRANITE2 everolimus mTOR weekly paclitaxel PFS
GOLD olaparib PARP weekly paclitaxel OS
BRIGHTER BBI-608 STAT3 weekly paclitaxel OS
KEYNOTE 061 pembrolizumab PD-1 weekly paclitaxel PFS, OS in PD-L1+
2nd / 3rd GRANITE1 everolimus mTOR BSC (placebo) OS
3rd JAVELIN GASTRIC 300 avelumab PD-L1 Irinotecan/taxane OS
Apatinib Study (China only) apatinib VEGFR2 BSC (placebo) OS
3rd~ ANGEL apatinib VEGFR2 BSC (placebo) OS
ATTRACTION-02 nivolumab PD-1 BSC (placebo) OS
Global RCTs with
Molecular Targeting
Agents (Including PD-(L)1
Ab) for Metastatic GC

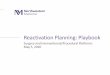
Treatment Pathways Currently under Evaluation
for Gastric Cancer
EGFR: epidermal growth factor receptor; STAT3: signal transducer and activator of transcription 3
Extensively Modified from Shah MA. J Clin Oncol 33:1760–1769, 2015
STAT3 ×STAT3 ×
Immune Checkpoint Inhibitor (Nivolumab ○)Immune Checkpoint Inhibitor (Nivolumab ○)
Angiogenesis (BEV ×, AFL×, RAM ○, <Apatinib ○>)Angiogenesis (BEV ×, AFL×, RAM ○, <Apatinib ○>)
EGFR ×EGFR ×
MET ??MET ??
>5,000 patients are planned to be enrolled in 19 ongoing studies,
with additional studies being planned
>5,000 patients are planned to be enrolled in 19 ongoing studies,
with additional studies being planned
FGFR ??FGFR ??
HER-2 (Tmab ○, T-DM1 ×, Lapatinib ×, Pertuzumab ×)HER-2 (Tmab ○, T-DM1 ×, Lapatinib ×, Pertuzumab ×)

Predicted ORR Across Tumor Types in 2L All-Comers
PFS Across Tumor Types in 2L All Comers
A Meta-Analysis to Indirectly Compare The Efficacy Profiles of Anti-PD-1/PD-L1
Monotherapy across Solid Tumors Using A Bayesian Hierarchical Model
Koneru M, et al. ASCO 2018

ORR PFS OS
Kang YK, et al. Lancet 2017

ORR PFS OS
Fuchs CS, et al. JAMA Oncol 2018

Patient,n
Events,n
mOS, months (95%CI)
12-month OS rate (95%CI)
Nivo.
330 2255.32(4.63, 6.41)
26.6(21.1, 32.4)
PLB.
163 1414.14(3.42, 4.86)
10.9(6.2, 17.0)
OS
0
0 2 4 6 8 10 12 14 16 18 20 22
Time, months
Pro
ba
bili
ty o
f su
rviv
al, %
100
80
60
40
20
HR 0.63 (95%CI 0.50, 0.78)
p<0.0001
Kang Y-K, et al. ASCO-GI, 2017
ORR: 11.2% (95% CI; 7.7-15.6)
ATTRACTION-02 (Nivolumab) KEYNOTE-059 (Pembrolizumab)
0
0
10
20
30
40
50
60
70
80
90
100
2 4 6 8 10 12
Overa
ll S
urv
ival, %
14 16 18 20 22Time, months
Median OS(95% CI), mos
12-month OS rate, %
All patients (n=259) 5.5 (4.2-6.5) 23.4
Fuchs CS, et al. ASCO, 2017
Wainberg ZA, et al. ESMO, 2017
OS
ORR: 11.6% (95% CI; 8.0-16.1)
Anti-PD-1 Antibody Monotherapy: Later Line for GC
N=330 N=259
N=163
Fuchs CS, et al. JAMA Oncology 2018

Q: Which is better, in earlier or later line
in case of using anti-PD-(L)1 antibody
for G/GEJ Cancer?
A: Probably earlier line is better
in terms of efficacy (ORR, OS).

Hui R. ASCO 2016
Brahmer JR, et al. WCLC 2017
KEYNOTE-001
KEYNOTE-024 Study Design
Reck M, et al. N Engl J Med 2016
Hui R, et al. ASCO 2016
Garon EB, et al. N Engl J Med 2015
OS ORR
Lessons from NSCLC
OS

KN-59 cohort 3N = 31
KN-59 cohort 1N = 259
ATTRACTION-02N = 330
Line 1L 3L or later 3L or later
PD-L1 + All comer + - All comer + -
ORR 26% 11.6% 16% 6% 11.2% - -
DCR 36% 27% 34% 19% 40.3%
mPFS 3.3m 2.0m 2.1m 2.0m 1.61m - -
mOS 20.7m 5.5m 5.8m 4.6m 5.3m 6.1m 5.2m
AE (Any) 77% 61% 43%
AE ( G3)≧ 23% 18% 11%
ORR And Waterfall in KEYNOTE-059 & Attraction-02
24 patients (77%) experienced
a reduction in target lesion size
Best Percentage Change in All Patients (n = 31)
–100
–80
–60
–40
–20
0
20
40
60
80
100
Ch
ange F
rom
Baselin
e, %
20% increase in tumor size
95 patients (42%) experienced
a reduction in target lesion size
Best Percentage Change in All Patients (n = 224)
Wainberg ZA, et al. ESMO, 2017 Fuchs CS, et al. JAMA Oncol 2018 Kang YK, et al. Lancet 2017

Phylogenetic Tree Analyses: Clonal And Subclonal Neoantigen
Heterogeneous tumors are composed of multiple subclones and under selection pressures, such as
chemotherapy, subclones with either intrinsic or acquired resistance can be selected for, allowing these
subclones to dominate a tumor mass and potentially drive disease progression.
Primary tumors consist of different subclones with shared and private somatic alterations. Alterations shared
by all tumor cells (A) occur early in tumorigenesis, represented by the blue trunk of the phylogenetic tree;
alterations shared by tumor cells present in some regions of the tumor but not all (B and C) occur later in
tumorigenesis, represented by the yellow branches of the tree; and private alterations (D–F) present in only
one region of the tumor also occur later in tumorigenesis, represented by the red branches of the tree.
Jamal-Hanjani M, et al. Clin Cancer Res 21:1258-1266, 2015

Clonal Neoantigens Elicit T cell Immunoreactivity
And Sensitivity to Immune Checkpoint Blockade
McGranahan N, et al. Science 351:1463-1469, 2016
A relationship between clonal neoantigen burden and overall
survival in primary lung adenocarcinoma was observed.
Sensitivity to PD-1 blockade in patients with advanced NSCLC
was enhanced in tumors enriched for clonal neoantigens.
T cells recognizing clonal neoantigens were detectable
in patients with durable clinical benefit.
Cytotoxic chemotherapy–induced subclonal
neoantigens, contributing to an increased mutational
load, were enriched in certain poor responders.

Q: What is a biomarker of anti-PD-(L)1
therapy in G/GEJ cancer?
A: 1) PD-L1 expression may be, but has not
been established robustly
2) MSI-H without doubt
3) TMB probably YES, but few data in GC

Shitara K, et al. Lancet 2018
KEYNOTE-061: Overall Survival, CPS 1%≧

Mok TS, et al. N Engl J Med 2009
IPASS: PFS, Gefitinib vs. CP

Is PD-L1 Expression Definite Biomarker in Anti-PD-1 Ab for GC?
Mok TS, et al. N Engl J Med 2009
IPASS (n=1218), PFS
KN-061, CPS 1% (n=395, 67%), ≧ OSCPS 10%≧
MSI-H
n=261 (21%)
n=108 (27%,18% )ITT population, n=592
n=27 (4.6% )
Shitara K, et al. Lancet 2018

0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
0
10
20
30
40
50
60
70
80
90
100
Pro
bab
ility
of
Su
rviv
al (
%)
Overall Survival by PD-L1 Expression <1% vs ≥1%
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
0
10
20
30
40
50
60
70
80
90
100
PD-L1 <1% PD-L1 ≥1%
Hazard ratio, 0.58
(95% CI, 0.24–1.38)
Median OS, months (95% CI)
Nivolumab (n=16) 5.2 (2.8–9.4)
Placebo (n=10) 3.8 (0.8–5.0)
Ove
rall
Su
rviv
al
(%)
114100
75 56 49 42 37 24 15 11 7 4 3 1 0
52 40 27 22 16 14 11 6 5 4 3 2 2 2 0
16 15 10 7 5 4 4 2 2 0 0 0 0 0 0
10 8 4 2 1 1 1 0 0 0 0 0 0 0 0
Nivolumab
Placebo
Months MonthsNo. at Risk
Median OS, months (95% CI)
Nivolumab (n=114) 6.1 (4.8–8.6)
Placebo (n=52) 4.2 (3.0–6.9)
Hazard ratio, 0.71
(95% CI, 0.50–1.01)
Boku N, et al. ESMO 2017
Evaluable for PD-L1 expression, n (%)≥1% vs <1%≥5% vs <5%
Nivo: 130 (39)16 (12) vs 114 (88)10 (8) vs 120 (92)
Placebo: 62 (38)10 (16) vs 52 (84)7 (11) vs 55 (89)
Among PD-L1–evaluable patients, baseline characteristics between nivolumab and placebo arms were similar
ATTRACTION-02: Nivolumab

Hellmann MD, et al. N Engl J Med. 2018
Low TMB 1Y-PFS MST 95%CI
Nivo + Ipi 26% 3.2 M 2.7-4.3
Chemotherapy 17% 5.5 M 4.3-5.6
HR 1.07 (95%C.I. 0.84-1.35)High TMB: defined as 10MT/Mb by Foundation One
HR 0.58 (95%C.I. 0.41-0.81)
p<0.001
High TMB 1Y-PFS MST 95%CI
Nivo + Ipi 42.6% 7.2 M 5.5-13.2
CTx 13.2% 5.5 M 4.4-5.8
No. at risk
IPI+NIVO
CTx
PFS
NSCLC
CTx naïve
No genetic alteration
PD-L1 1%≧
N=1189
PD-L1 + 1%
N=550
IPI+NIVO
(N=139)
CTx
(N=160)
Lessons from NSCLC (TMB)
CheckMate-227

Janjigian YY, et al. Cancer Discovery, 2018
MSI-H TMB

Megan G, et al. #4056, ASCO 2018
TMB for G/GEJ Cancer, ASCO 2018MSK-IMPACTTM (468-gene platform)
Cut off 7.3 MT/megabases
N=120 (MSI-H, N=7)
‘SCRUM JAPAN’ by OCP panel (143-gene platform)
Panel is possible instead of WES,
but optimal ‘cut off’ is not established
Panel is possible instead of WES,
but optimal ‘cut off’ is not established
cf: 5.0 in Foundation One Panel
Nakamura Y, et al. #12094, ASCO 2018

Q: Are there any substantial rationales
regarding IO-combo therapy?
A: 1) IO + cytotoxic agents (chemotherapy)
2) IO + IO
3) IO + anti-angiogenic inhibitor (including
other molecular targeting agents)
4) IO + radiotherapy

Combined with Chemotherapy
- Is It Good or Evil?
Gandhi L, et al. AACR 2018

Emens LA, et al. Cancer Immunol Res 2015
Cytotoxic Agents Enhances Immunological Reaction
around Tumor and Tumor Microenvironment

Tumor cells can upregulate
expression of immune target
molecules such as Fas and
MHCI following irradiation.
Irradiation can also
normalize dilated and chaotic
blood vessels to enable T
cells to access tumors.
The Effects of Chemotherapy And Radiotherapy
on The Tumor Microenvironment
Kershaw MH, et al. OncoImmunology, 2013
Ox can also lead to an increased proportion of proinflammatory, M1,
macrophages relative to alternatively activated, M2, macrophages.
Anthracyclines can recruit APCs and enhance their differentiation to
an activated phenotype, better able to present antigen to lymphocytes.
Ox can induce immunogenic cell
death, which can lead to the release
of tumor antigens for uptake and
processing by antigen presenting
cells (APC).
Gem, Ox and Pacli
can reduce the
frequency of
MDSC and/or Treg
infiltrating tumors,
thereby reducing
their immuno-
suppressive
effects.
Increases in
intratumoral T cells
can also be achieved
using antibodies
against VEGF.

Attraction-04 Part 1 Efficacy
Kang YK et al. ESMO, 2017

KN 059-Cohort 2: Best Percentage Change and
Longitudinal Change in Target Lesion Size
aOnly patients with measurable disease per RECIST v1.1 by central review at baseline who had ≥1 postbaseline assessment were included (n = 25); assessment was nonevaluable for 1 patient.bLongitudinal change in the sum of the longest target lesion diameters from baseline in patients with ≥1 postbaseline assessment (n = 25).+No progressive disease at last disease assessment.
24 patients (96%) experienced a reduction in target lesion size
–100
–80
–60
–40
–20
0
20
Ch
an
ge
Fro
m B
as
eli
ne
, %
PD-L1 positive
PD-L1 expression unknown
PD-L1 negative Ch
an
ge
Fro
m B
as
eli
ne
, %
Best Percentage Change in All Patients (n=25)a
Cohort 2
No prior therapy
PD-L1 positive or
negative
Cohort 2
No prior therapy
PD-L1 positive or
negative
Pembrolizumab 200 mg Q3W +
Cisplatin 80 mg/m2 Q3W +
5-FU 800 mg/m2 Q3W or
Capecitabine 1000 mg/m2 BID Q3Wa
Pembrolizumab 200 mg Q3W +
Cisplatin 80 mg/m2 Q3W +
5-FU 800 mg/m2 Q3W or
Capecitabine 1000 mg/m2 BID Q3Wa
aCapecitabine was administered only in Japan
Study Design
Wainberg ZA, et al. ESMO, 2017
ORR:
17/25 (68%)
mOS:
13.8 mo

Janjigian YY, et al. ASCO 2017
Primary endpoint:
• ORR per RECIST v1.1
Secondary endpoints:
• OS, PFS, TTR, DOR• Safety
Exploratory endpoint:
• PD-L1 tumor expression (Dako 28-8 pharmDx assay)
Primary endpoint:
• ORR per RECIST v1.1
Secondary endpoints:
• OS, PFS, TTR, DOR• Safety
Exploratory endpoint:
• PD-L1 tumor expression (Dako 28-8 pharmDx assay)
Checkmate 032 EG Cohort
DOR, duration of response; EG, esophagogastric (including gastric/esophageal/gastroesophageal junction
cancer); TTR, time to response.
* Nivolumab + ipilimumab administered for 4 cycles followed by nivolumab 3 mg/kg IV Q2W. † Time from first dose to data cut-off; follow-up was shorter for patients who died prior to data cut-off.
Nivolumab 3 mg/kg +
Ipilimumab 1 mg/kg IV
Q3W*
(NIVO 3 + IPI 1)
Nivolumab 3 mg/kg +
Ipilimumab 1 mg/kg IV
Q3W*
(NIVO 3 + IPI 1)
Nivolumab 1 mg/kg +
Ipilimumab 3 mg/kg IV
Q3W*
(NIVO 1 + IPI 3)
Nivolumab 1 mg/kg +
Ipilimumab 3 mg/kg IV
Q3W*
(NIVO 1 + IPI 3)
Nivolumab 3 mg/kg IV Q2W
(NIVO 3)
Nivolumab 3 mg/kg IV Q2W
(NIVO 3)
Western patients with advanced/metastatic EG cancer
with progression on ≥1 prior chemotherapy
N = 160
Western patients with advanced/metastatic EG cancer
with progression on ≥1 prior chemotherapy
N = 160
Median (range)
follow-up, mo†:28 (17 to 35) 24 (21 to 33) 22 (19 to 25)

* Investigator review.
# Patients with confirmed response (complete or partial response).† Patients with 0% best reduction in target lesion, including 3 patients with PD-L1 ≥1%
(NIVO 3, n=2; NIVO 3 + IPI 1, n=1) and 1 patient with PD-L1 <1% (NIVO 1 + IPI 3).change truncated to 100%
†
##
#
#
#
#
# #
## #
100
75
50
25
0
-25
-50
-75
-100
Be
st
Red
uc
tio
n f
rom
Bas
eli
ne i
n T
arg
et
Le
sio
ns
* (%
)
#
#
##
#
100
75
50
25
0
-25
-50
-75
-100
Be
st
Red
uc
tio
n f
rom
Ba
seli
ne i
n T
arg
et
Les
ion
s*
(%)
†
PD-L1 < 1% PD-L1 ≥ 1% PD-L1 not evaluable/missing
100
75
50
25
0
-25
-50
-75
-100
Be
st
Red
ucti
on
fro
m B
as
eli
ne i
n T
arg
et
Le
sio
ns
* (%
)
#
#
#
#
#
#
#
† †
Best Reduction in Target Lesions
Responses were observed regardless of PD-L1 expression
ORR: 12%
Janjigian YY, et al. ASCO 2017
ORR: 24% ORR: 8%
NIVO 1 + IPI 3PD-L1–evaluable patients, 38 of 42
NIVO 1 + IPI 3PD-L1–evaluable patients, 38 of 42
NIVO 3PD-L1–evaluable patients, 38 of 53
NIVO 3PD-L1–evaluable patients, 38 of 53
NIVO 3 + IPI 1PD-L1–evaluable patients, 34 of 41
NIVO 3 + IPI 1PD-L1–evaluable patients, 34 of 41

KEYNOTE-062 (1L)Checkmate-649 (1L)
Attraction-04 (1L)
Ongoing 1L-Combination Trials
Any PD-L1
1st-line
N=1266 Primary Endpoint: OS (PD-L1+)
PD-L1+
1st-line
N=750
Primary Endpoint: PFS, OS
Primary Endpoints: PFS, OS
Any PD-L1
1st-line
N=650

JVDF/KN-098 Phase 1a/b Study DesignRAM + Pembro
J. Exp. Med. 2015 Vol. 212 No. 2 139–148
Herbst RS, et al. ASCO 2018

Phase 1 StudyRAM + Durvalumab
Golan T, et al. WCGC 2017

Nivo + Ram as IIT-PII
Takahari D et al. ASCO 2018

PTX + Ram + Nivo as IIT-PII
Nishina T, et al. ASCO 2018

Loi S, et al. SABCS 2017
Catenacci D VT, et al. ASCO 2018
G/GEJC (Pembro+margetuximab)
BC (Pembro+trastuzumab)
Stagg J et al. PNAS 108 : 7142-7147, 2011
Anti-HER2 Therapy for BC, G/GEJC
Pretreated Trastuzumab

IO Combinations: Others
Anti-PD-(L)1 Inhibitor +
Bevacizumab: NSCLC, HCC..
Lenbatinib: H&N, HCC, RCC, EC..
Axitinib: RCC..
BBI-608: CRC..
IDO Inhibitor: TNBC, Melanoma↓..
LAG-3 Inhibitor: multi-type of cancer..
CCR-4 Inhibitor: HCC, PC, NSCLC, SCLC,
E/G/GEJC..
M7824 (TGF-β+(avelumab)): E/G/GEJC…

Ngwa W, et al. Nat Rev Cancer 18:313-322, 2018 Sato H, et al. Nature Commun 24::1751, 2017
Durvalumab (Lung : PACIFIC trial) Nivo+SBRT (H&N)
Mcbride SM, et al. ASCO 2018Antonia SJ, et al. N Engl J Med 377: 1919-1929, 2017
TAA
Abscopal Effect RT upregulates PD-L1
IO + RT

PembrolizumabPTX
Niv olumabplacebo
pembrolizumab
pembrolizumab+XP/FP
pembrolizumab
Ipilimumabplacebo
Olaparib+PTXOlaparib
Ev erolimusPlacebo
ECX+rilotumumabECX
FOLFOX+onartuzumabFOLFOX
Irinotecan+nimotuzumabIrinotecan
EOC+panitumumabEOC
XP+cetuximabXP
ApatinibPlacebo
PTX+RamcirumabPTX
RamucirumabPlacebo
Ramcirumab+XP/FPXP/FP
XP+Bev acizumabXP+placebo
T-DM-1PTX or DTX
PTX + LapatinibPTX
CapeOX + lapatinibCapeOX
FP/XP+trastuzumabFP/XP
FP/XP+trastuzumab+perutsuzumabFP/XP+trastuzumab
0 5 10 15 20 25
target Study Line ph OS Treatment
HER2
JACOB 1 3 ×
ToGA 1 3 +
Logic 1 3 ×
TyTAN 2 3 ×
GATSBY 2 3 ×
VEGF/VEGFR
AVAGAST 1 3 ×
RAINFALL 1 3 ×
REGARD 2 3 +
RAINBOW 2 3 +
Apatinib 3 3 +
EGFR
EXPAND 1 3 ×
REAL-3 1 3 ×
ENRICH 2 3 -
HGF RILOMET1 1 3 ×
MET METGastric 1 3 ×
mTOR GRANITE-1 2/3 3 ×
PARP GOLD 2 3 ×
CTLA-4 maintenance 1 2 ×
PD-1
KN59 ch3 1 2 -
KN59 ch2 1 2 -
KN59 ch1 3 + 2 -
ATTRACTION-02 3 + 3 +
KN61 2 3 ×
Extensively Modified from Shitara K, Gastric Cancer 2017
OS Data from Global Trials against GC/GEJC

Summary
• Anti-PD-1 antibody monotherapy (Pembrolizumab and Nivolumab)
are both active and having similar efficacy in late line of G/GEJC,
but the efficacy (such as long survival) is limited to few populations.
• Anti-PD-1 antibody combined with other agents (cytotoxic,
molecular targeting agent such as anti-angiogenic, and other
immuno-oncological agent) demonstrates encouraging efficacy and
may promise the position of earlier line therapy for G/GEJC.
• The role of PD-L1 expression and relationship between PD-L1
expression and efficacy are needed to be further investigated in
G/GEJC.
• Many clinical trials in any line or any combinations are now
ongoing, and these results will be confirmed as definite therapy for
G/GEJC.

Acknowledgment

Thank you