Embed Size (px)
Citation preview

WM CalOMS Discharge Questionnaire
Unicare IDWM Diisschcharargege
Left before completion with satisfactory progress
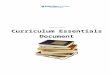
Discharge Reason (Choose one)
Discharge Date
- -
* Specify Drug NamePPPage 1 oage 1 oage 1 of 3
Primary Substance Use Route of Admin
Substa
nce
Drug N
ame
Past
#3
D0 a
Dy
as
ys
Age U a
st
eO
First
ral Sm Io
nk
hi
ang
Inl
ja
et
ci
to in
Oton
her
None
Heroin o o o o oAlcohol o o o o oBarbiturates* o o o o oOther Sedatives or Hypnotics* o o o o oMethamphetamine o o o o oOther Amphetamines* o o o o oOther Stimulants* o o o o oCocaine / Crack o o o o oMarijuana / Hashish o o o o oPCP o o o o oOther Hallucinogens* o o o o oTranquil izers (Benzodiazepine)* o o o o oOther Tranquil izers* o o o o oNon-Prescription Methadone o o o o oOxycodone / OxyContin o o o o oOther Opiates or Synthetics* o o o o oInhalants* o o o o oOver-the-Counter* o o o o oEcstasy o o o o oOther Club Drugs* o o o o oOther* o o o o o
AOD use during past 30 days
Rev. 1.0, 1/7/2020, KC, PRC

WM Discharge
PPage 2 oage 2 of 3
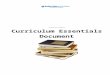
AOD use during past 30 days
Unicare ID
Secondary Substance Use Route of Admin
Substa
nce
Drug N
ame
Past 3
0 Day
s
# Day
s
Age at
First
Use Oral Smokin
g
Inhalatio
n
Injection
Other
None
Heroin o o o o oAlcohol o o o o oBarbiturates* o o o o oOther Sedatives or Hypnotics* o o o o oMethamphetamine o o o o oOther Amphetamines* o o o o oOther Stimulants* o o o o oCocaine / Crack o o o o oMarijuana / Hashish o o o o oPCP o o o o oOther Hallucinogens* o o o o oTranquil izers (Benzodiazepine)* o o o o oOther Tranquil izers* o o o o oNon-Prescription Methadone o o o o oOxycodone / OxyContin o o o o oOther Opiates or Synthetics* o o o o oInhalants* o o o o oOver-the-Counter* o o o o oEcstasy o o o o oOther Club Drugs* o o o o oOther* o o o o o
* Specify Drug Name
Rev. 1.0, 1/7/2020, KC, PRC

WM Discharge
Page 3 of 3
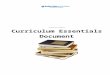
(Ask next question only if primary, secondary drug is not alcohol)
Number of days in the past 30 days client used Alcohol? .........................................................................days
Unicare ID
(0 -30)None/Not Applicable
Were you pregnant at any time during the treatment? ......................... Yes No Not Sure
What type of disability/disabilities do you have?None Visual Hearing SpeechMobility Mental Developmentally Disabled Other Disability (not AOD)Declined to State Unable to answer
(Check all that apply)
Ever been diagnosed with a mental illness? ..................................................................... Yes No Not Sure
How many days, in the past 30 days, have you participated in any social support recovery activities (such as 12-step meetings, other self help meetings, religious/faith recovery meetings, meetings of ..........an organization other than those listed above, interactions with family members and/or friend forsupport of your recovery)?
days(0 -30)
Current living arrangements:
Homeless No stable arrangements Transitional Housing/Residential
Parents Family Friends
Sexual partner alone Sexual partner & children Children alone
Alone Board & Care
Are you currently enrolled in school?
If enrolled, how many days in the past 30 days have you missed school? ...................................................
Employment Status Employed Full time (35 hours or more) Unemployed, not in the labor force (not seeking)
Employed Part time (less than 35 hrs.) Not in the labor force (Not seeking)
Unemployed, looking for work
Yes No Declined to State Unable to answer
(0 -30)days
How many days in the past 30 days ..............................................................................................................have you had serious conflicts with your family?
How many times have you been arrested in the past 30 days? ....................................................................Unable to Answer
Declined to Answer Unable to Answerdays(0 -30)
(0 -30)days
Name of data entry staff:
Rev. 1.0, 1/7/2020, KC, PRC