Embed Size (px)
Citation preview
i
Disability in Afghanistan:
Taking a Capabilities Approach to look atResearch Challenges and Policy Implications
ii
Abstract
This article presents an example of the operationalization of the capabilities approach into relevant
research tools and policy recommendations. The National Disability Survey in Afghanistan (NDSA)
was elaborated within this framework, looking at the interaction between the individual and the
collective to define relevant tools and methods to look at disability. It relies on a definition of
disability that encompasses the different models of disability: the medical, social and ICF bio-
psychosocial models. The NDSA was launched due to scarcity of knowledge on disability leading to
implementation of services on a groundless basis. It is a national multistage, cluster, population-
based survey of 38320 household members, 1013 disabled and 1683 non disabled respondents
aged 5 or above conducted from December 2004 to July 2005. It relies on the capabilities
approach to look at persons with disabilities, in order to understand the individual as part of a
family, a community and a society and to make policy recommendations. At the policy level we
argue that while the definition of human development had evolved considerably, through works of
scholars such as Sen and Nussbaum, the translation of this change often remains at the level of
objectives. One of the main reasons for this gap that separates the goals and their translation into
policies is the paucity of knowledge.
Key Words: Disability, Policy development, Potentiality, Research, Vulnerability.
Biographical details:JF Trani, PhD, economist, NDSA project manager for Handicap-International and invitedprofessor at the Center for Economics and Ethics for the Environment and theDevelopment, University of Versailles .P Bakhshi, PhD, psychologist. Consultant for Handicap International.A. A. Noor, MD MPH, USAID, Health, Disaster and Complex Emergency AssistanceAdvisor.A. Mashkoor, MD, consultant for the Health Management Information Systems of theMinistry of Public Health, Afghanistan.S. Helseth, United Nations Mine Action Centre for Afghanistan.D. Lopez, statistician, European Monitoring Center for Drugs and Drug Addiction; Scientificcoordination unit.S. Schwarz, Handicap International.L. Lavasani, Handicap International.
iii
Jean Francois Trani
Project Manager, NDSA, Invited Professor UVSQ, [email protected]
Parul Bakhshi
Researcher, NDSA, [email protected]
Ayan Ahmed Noor
USAID, Health, Disaster and Complex Emergency Assistance Advisor.
Ashraf Mashkoor
Health Management Information Systems, National Consultant,
Ministry of Public Health, Afghanistan,
4
Introduction
The National Disability Survey in Afghanistan (NDSA) is the first household survey on disability that
attempt to utilize the capabilities approach. This survey aims to determine the prevalence of
disabilities in Afghanistan and provide a cross-cutting overview of the situation of persons with
disabilities by collecting reliable information about their needs, and promoting integration of their
concerns into the programmes and policies of the government. This study carried out between
December 2004 and July 2005 by Handicap International in collaboration with the Ministry of
Martyrs and Disabled and Social Affairs (MMDSA), the Ministry of Public Health (MoPH) and the
Central Statistic Office (CSO), provides relevant essential information for policy makers, both
development actors and the Government, and a better understanding of the condition of
vulnerable groups in order to effectively prioritise, define and implement policies for their welfare.
This article highlights the difficulties that often divide academic and somewhat idealised definitions
from their actual operationalization and raises the following questions; how to move from
theoretical and philosophical considerations to a methodology that will serve as the basis for
collecting data? How to look at the disability picture in Afghanistan through a capabilities lens?
Going beyond and encompassing existing models, the use of the Capabilities Approach is a rather
innovative way of assessing disabling situations. A void exists between the overall aims that have
been defined by the government of Afghanistan and the lack of policies and programmes to
achieve these goals. The overall goal of the national disability strategy is to improve livelihood and
social protection of persons with disabilities in Afghanistan, eradicate poverty and fight for the
recognition of their rights [Italian Cooperation, 2003, UNDP, 2004, Trani, 2004]. These problems
are, for a great part, explained by the absence of relevant knowledge about field realities as they
stand today and the needs, aspirations and living conditions of vulnerable groups in general.
However whereas no services exist in rural areas, those that prevail in urban areas are not always
adapted to the needs. Employment and income generation activities are non-existent and
education and health facilities remain inaccessible.
5
The article discusses the political implications of this type of survey, as well as the factors that may
jeopardize the efficient translation of its results and findings into relevant policies in the very
unstable context prevalent at the state level. How do we transform the knowledge gained into
relevant public action? The capabilities approach can be operationalized in research methodology
and tools from the perspective of the individual. It can also be a valid space for the thinking and
defining of collective public policies.
Defining and conceptualizing impairment and disability
Disability has been defined using several paradigms, each of them focusing on a specific facet of
disability. The NDSA research project relies on the Capabilities Approach of Amartya Sen and
others. Such an approach is comprehensive as it includes the medical and the social model
[Burchardt, 2004, Mitra, 2003].
Overview of models
The medical and social models of disability have been presented as being opposed in their
approach. The medical view, based on the individual and his/her impairment, considers the
physical or mental ‘problem’ that a person has [Pfeiffer, 2001, Amundson, 2000, Marks, 1999].
Thus, disability is at first a deficit in the body. Disability is the situation of persons with disabilities,
defined by any restriction or lack, resulting from impairment, of ability to perform an activity in a
manner or within the range considered normal for human beings [WHO, 1980]. Impairment, in the
traditional medical approach, relates to individually based bio-physical conditions. As a result,
quantitative research based exclusively on this model needs to establish a medical diagnosis of the
health situation of the person. Not only is this unfeasible in a country like Afghanistan where
medical capacity is limited [Ventevogel et al., 2006] but more importantly it is not required to fulfill
some of the aims of the survey: namely to provide scientific knowledge for public policies.
This view, which looks at disability by focusing on the individual, has been held as biased by
disability activists and organizations, especially in the British approach [Hunt, 1966, Finkelstein,
1981, Barnes, 1991, Oliver, 1996]. The Physically Impaired Against Segregation (UPIAS) were the
first to make the distinction between impairment and disability [Barnes, 1997]. Disability is due to
the exclusion of persons with disability from mainstream society. The social model put forward the
6
argument that persons are ‘disabled’ because of the structure of the society in which they live,
which does not accommodate their impairment. Thus it is the environment, both physical and
social, that makes a person with impairment, a person with disability [Shakespeare, 2001]. This
approach, which has been put forward by a number of disabled persons’ organizations, looks at the
barriers that exist within the social context and prevent a person from achieving the same level of
functioning than a non-disabled person. In this perspective it is society that needs to be
redesigned in order to take into account the disabled person’s needs [Olivier, 1996]. However, the
individualistic rights -based approach to empowerment at the basis of the social model raises many
questions as it fails to take into account the family factor in the decision-making process [Lang,
2001].
Going a step further, the World Health Organization has formulated the ICF, the International
Classification of Functioning, Disability and Health, which provides guidelines for data collection
and other information gathering [WHO, 2001]. The ICF looks at disability as a combination of
individual, institutional and societal factors that define the environment within which a person with
impairment evolves. In ICF, the term functioning refers to all the “body functions, activities and
participation, while disability is similarly an umbrella term for impairments, activity limitations and
participation restrictions” [WHO, 2001, p. 3].
This definition is limited to 2 main concepts:
1. Body functions and structures (these take into account attributes specific to an individual).
2. Activities and participation (this refers to the environmental factors, including the physical
environment, the social environment and the impact of attitudes).
This definition is potentially compatible with the capabilities approach [Seddon et al. 2001]. But the
ICF approach presents certain limitations. First of all it focuses on the body, individual limitations
and participation and does not stress on the interaction between individual and society in its
definition of disability, thus does not offer a broader perspective for defining policies [Terzi, 2004].
This approach does not take into account the diversity of situations of individuals and the socio-
cultural contexts in which the phenomenon of disability is considered. A disabling situation in
Afghanistan (i.e. a farmer with a missing leg not having access to a device) can be completely
7
overcome in Australia because the difficulty is addressed: the farmer will be equipped with an
artificial leg and will use a tractor for the farm work. Considering the disabling situation itself can
lead to a division between persons with disabilities and non-disabled persons considered as
“normal”, thus encouraging stigma and marginalization where mainstreaming and participation are
sought.
The Capabilities approach to disability: going beyond the medical, social and bio-psychosocial models of disability
The capabilities approach places the definition of disabilities within the wider spectrum of human
development. The focus is not anymore on the disabling situation but on the equality in terms of
choices offered to an individual. It provides further insight into the issues related to disability since
it highlights not what a person actually does (functioning) but the range of possibilities that he/she
chooses that specific functioning from – this is the capabilities set [Sen A., 1999]. While
elaborating research aimed at defining policy, it is relevant to take into consideration certain
aspects that come into play in socially sustainable human development.
The capabilities approach applied to disability complements the medical model by considering the
individual as a person with linkages to her/his environment. The social and the ICF models do also
consider the environment but by overstressing its insufficiencies. The capabilities approach adds to
the ICF and the social model by stressing on the following dimensions. In the first place looking at
capabilities of persons with disabilities from a policy point of view entails considering ways of
reducing vulnerability. Vulnerability can be defined as “the probability of having his/her own
situation worsen when facing a dramatic event” [Dubois & Rousseau, 2001, p.1]. Poverty reduction
policies require taking into consideration vulnerable groups and building preventive policy. Within
this framework, policies need to aim at reducing vulnerability and enhancing capabilities, viewed as
composed of ability and potentiality. While the former looks at what a person can do and be in a
given context, the latter refers to the ability to cope over time, in a sustainable manner.
Secondly, the capabilities’ perspective looks at the interplay between individual characteristics and
social restrictions and proposes to measure outcomes in terms of the expanding of people’s
choices and thus freedoms. Limiting the definition to merely a quantitative one, or gathering
information on income and institutional access, and trying to categorize different types of disability
8
into broad groups as the ICF does, would be ignoring the dynamics that exist between the
individual and the community. The capabilities approach takes into consideration the individual
with the social groups that he/she belongs to, as well as the institutional factors that may influence
his/her choices. To what extent do the social and cultural dynamics of the context contribute to
expanding or impeding the spectrum of choices of the individual?
Thirdly, the value given by this approach to human diversity and the interactions between
disability, gender, cultural and ethnic dynamics and religious implications is also particularly
important in view of the research carried out in Afghanistan. “The difference entailed by these
variations has to be accounted for, when addressing the demands of equality” [Terzi, 2004, p. 12].
The burden of physical disability on men injured during the war is considerably less than that of
the same disability on a young unmarried woman disabled at birth.
Finally, the agency of the individual in the capability approach looks at if and to what extent, the
person considers her/himself as the main actor and decision maker in her/his own life. This
element is linked with seeing oneself as the main actor in defining a positive outcome for the
future, and is close to the concept of “power” or “agency” developed by Sen as a person’s “ability
to form goals, commitments, values etc.” It is recognizing a person as “someone who acts and
brings about change, and whose achievements can be judged in terms of her/his own values and
objectives, whether or not we assess them in terms of some external criteria as well” [Sen, 1999,
p. 19].
Disability in the post-conflict Afghan context
When the Ministry of Martyrs and Disabled, the Ministry of Public Health, the Central Statistic Office
of Afghanistan asked Handicap International to carry out a quantitative household survey on
disability, no scientific knowledge was available to comprehend the social and economic conditions
of persons with disabilities in Afghanistan.
Lack of reliable knowledge
To date all of the quantitative knowledge was limited to estimation data of prevalence. For
instance, UNDP/UNOPS estimations in 1999 were of 700,000 Afghans with a disability, or 3% of
9
the population [UNDP/UNOPS, 1999]. In 2003, The Italian Cooperation estimated that 4% of the
population, 800.000 people were disabled in Afghanistan [Italian Cooperation, 2003]. While
hundreds of thousands of Afghans were disabled by war and landmines, many more have
impairments from birth, inadequate healthcare, congenital disabilities, accidents or/and
malnutrition and preventable diseases such as polio or tuberculosis. A high rate of birth
complications, especially in undernourished women with inadequate maternal care, causes
disabilities. Large numbers of people who were psychologically traumatized have received minimal
services, if any. Nevertheless, a 2002 survey of the Center for Disease Control and Prevention
(CDC), the United Nations Children’s Emergency Fund, and Vietnam Veterans of America
Foundation, in collaboration with the MoH and the MMD, and non governmental organizations
estimates that about 67.7% of Afghans have been affected by mental disorders or psychosocial
stress such as depression, anxiety and psychosomatic problems [Cardozo et al 2004, Scholte et al
2004]. This survey targeted Afghans above the age of 15 and was limited to 50 clusters. Moreover
it did not account for village level population. In its National Policy for Action on Disability the MMD
still indicate that estimated number of persons with disabilities range from 80.000 to 2 million of
the total estimated 25 million Afghans [MMD/UNDP, 2005]. This was the latest of many other
estimates.
Thus, the limited body of work that did exist consisted mostly of qualitative experiences
[Turmusani, 2004, Miles, 1990], very small scale studies limited to a region and children in school
[GVC, 2003], limited to a certain topic, the social perception of disability [Thakkar et al., 2004], or
limited on both aspects, geographic coverage and topic for the survey on mental distress in
Afghanistan [Cardozo et al., 2004]. Whenever disability was included in a quantitative national
household survey, it was not the main topic. As a result questions relating to disability consisted in
one or two queries aimed mostly at defining categories of persons with disabilities within more
general surveys [WFP et al. 2004, UNICEF et al. 2003]. The surveys and research that addressed
the situation of persons with disabilities in Afghanistan provide few figures. Among youth, the 2003
Italian Cooperation survey in 65 schools of Kabul showed that congenital disability accounts for
over 30% of overall causes of disability [GVC, 2003]. The National Risk and Vulnerability
10
Assessment (NRVA) estimated the rate of prevalence in Afghanistan at 2% for physical disability
and 1% for mental disability [WFP et al., 2004].
The NDSA was the first survey carried out in 2005 in Afghanistan which focused specifically and
solely on all aspects of disability. It was commissioned at a time when much required attention was
been paid to the needs of the most vulnerable in the country. All elements (the experts, the
funding, the Government will) were set in place to define a strategy based on scientific evidence.
However, gathering the data on the field to provide useful information necessitated tools and
methods based on a good understanding of the socio-cultural construction of disability in the
Afghan context.
Socio-cultural construction: stereotypes, prejudice and discrimination
Disability is by social and cultural norms defined, and this is why what is considered “disability” in a
given context is not necessarily the case in another [Lang, 2001]. In Afghan culture, disability is
perceived differently according to gender differences, traditional or ethnic attitudes and religious
motives, and even the person’s economic status. They are different beliefs about persons with
disabilities considered as a group or several distinct groups. Therefore, persons with disabilities are
facing different prejudices and thus are more or less vulnerable in day-to-day life. In this matter,
Afghanistan differs from other culture where prejudice against persons with disabilities is
generalized [Shakespeare, 1994, Douglas, 1966, Murphy, 1987]. They do not however constitute a
homogeneous group, but various sub-groups facing diverse needs and opportunities.
Understanding the notion of ‘disability’ within this context is not simple. This requires an in depth
analysis of the religious, cultural, economic and social realities.
A study carried out on the perceptions of disability in Afghanistan [Thakkar et al., 2004] showed a
complex picture of the beliefs, knowledge and attitudes related to different types of disability and
the level of discrimination that different groups encounter. A very complex set of social
representations are linked to the term ‘disability’ and persons with disabilities are valorized or
shunned, admired or hidden in accordance with the cause. Disability in Afghanistan has been
linked with the issue of martyrdom [Italian Cooperation, 2003]. There is a common belief that the
war related disabled men be viewed as heroes, courageous and having made a sacrifice for their
country. The landmine/UXO/IED survivors also enjoy a particular image within society, viewed as
11
being the first victims of a conflict/post-conflict situation and receive sympathy and often pity from
the community. Thus, the war-disabled men and the landmine/UXO/IED survivors are very
respected and visible in the Afghan society, whereas other types of disabled suffer from
discrimination. These persons not only form a socially visible group, but constitute a strong political
pressure group. They have a high level of visibility and have access to a number of rehabilitation
and physiotherapy centers in major towns of the country. They also head major organizations of
persons with disabilities in Kabul and other provinces. Some of their prominent figures have been
elected or nominated by the President as members of Parliament. The men disabled because of
the war are also the persons with disabilities with the easiest access to the labor market (see
below Table I).
Table I: Level of activity of Afghans aged 15-64
Approximately here.
Yet, access to labor market, because it provides an income and the ability to take care of oneself
and moreover contribute to the family welfare is essential for consideration and respect [Thakkar
et al., 2004, Coleridge, 1998]. This is the reason why persons with disabilities who are
economically a burden on the family suffer from stigmatization. Thus, a major aspiration for
persons with disabilities, notably in developing countries, is to gain employment, and thus be in a
position to make a financial contribution to the household [Erb and Harriss-White, 2001, Lang,
2001]. Policy makers must therefore develop employment support and vocational training policies
as employability is deeply linked to respectability.
Lack of awareness and strong cultural beliefs lead the population to consider other causes of
disabilities, especially congenital ones, as shameful. Most often though, mental illness and
intellectual disability are perceived as a curse in Afghanistan: diwana is the colloquial term that
refers to any impairment related to asab (mind). It is used as much for people with mental illness
as for people with intellectual disability. The diwanas are the most stigmatize and face great
difficulties in terms of integrating within their families and society [Thakkar et al., 2004]. Mocking
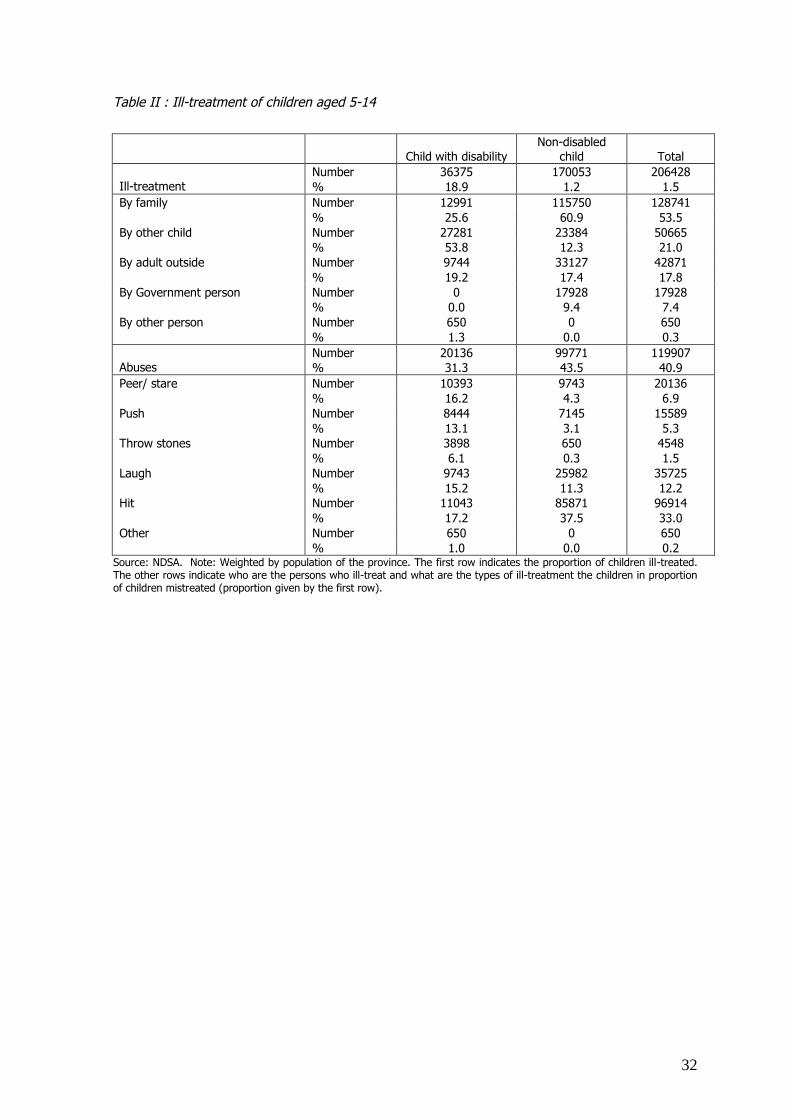
and teasing of children with disability are frequently observed (18.9% of children with disability are
ill-treated, table II), often by other children: 60.7% of ill-treated children are ill-treated by other
12
children or other pupils in class [Miles, 2002c]. Some of them are ill-treated by their own family
(25.6%), and some by different people outside home (19.2%). Forms of ill-treatment observed are
most frequently abuses (31.3%), but can be also laughing (15.2%), peering (16.2%), hitting
(17.2%) or pushing (13.1%), and even throwing stones (6.1%).
Table II: Ill-treatment of children aged 5-14
Approximately here.
Mental retardation is commonly denied and considered as a Post Traumatic Stress Disorder (PTSD)
resulting from past bomb attacks children may have been exposed to. However, this parental
attitude may be due to the fact that the presence of a person with disability not only constitutes an
obstacle to a normal marriage and family life for him or her, but might affect the marriage
opportunities of other members of the family. This lack of awareness leads to stigmatization.
Disability, especially those that result from congenital problems, disease and cannot be attributed
to a clear-cut cause, is often considered as a problem brought on by divine punishment or a
person’s bad luck. In the case of epilepsy, Miles [2002b] has shown that Afghan people think that
all people with epilepsy have a djinn or spirit.
The challenge for the survey was to have a framework that would encompass all these differences.
Focusing on at the activities and participation of an individual allows for a more comprehensive
view that looks at the various aspects of the disabling situation.
Disability in the Afghan policy process since 2001
The need for bridging research and policy has been recently emphasized by many authors [Court
and Maxwell, 2005, Carden, 2004, Ryan and Garrett, 2003]. We discuss the political dynamics that
strongly influence the use of the recommendations put forward: once the knowledge is available,
who is responsible for translating it into sustainable public action? How can we ensure that the will
to expand choices and freedoms is a priority from the conception of research to the
implementation of policies?
Paucity of services, poor coordination, necessity for empowerment of persons with
disabilities
13
Since 2001, a patchwork of services (physical rehabilitation, community based rehabilitation…) has
been organised independently mainly by NGOs, UNDP Comprehensive Disabled Afghans’
Programme (CDAP)i and the MMD in Afghanistan. These are characterised by incomplete
geographical coverage, deficient services (nothing on mental health for instance), little
coordination, and lack of mainstreaming. This is largely due to the scarcity of human and financial
means, but above all to the lack of knowledge of the needs of persons with disabilities.
Programmes have been set up and implemented on unfounded and unchecked assumptions about
needs and living conditions of persons with disabilities as well as a lack of comprehension
regarding their positions and function within the family and the community. The various
stakeholders recognize the necessity to collect information on vulnerable groups. Research became
a priority of the National Program for Action on Disability [UNDP, 2004] and the first sub-
programme of the planned National Vulnerability Program which remained at the state of project
as a prerequisite to the defining of priorities and designing of policies. This is the overall goal of
the NDSA.
In a capability approach to disability, the public policies concerning persons with disabilities would
aim at increasing assets, strengthening potentialities, and enhancing capabilities of individuals,
thus decreasing their vulnerability [Bakhshi et al., 2004]. Understanding of the situation of persons
with disabilities is therefore a prior necessity. The political context is largely responsible for the lack
of knowledge. However, the collapse of the CDAP which sub-contracted all field activities to NGOs,
and the Government’s decision to launch a National Vulnerability Programme (NVP), highlighted a
major need for knowledge-based evidence to direct programme decisions.
The case of the Health Policy
In a capabilities approach perspective applied to the health sector, the main functionings would be
‘to be healthy and well nourished’, thus interpreting the approach as promoting the capabilities of
an individual to achieve the valuable functionings of being healthy and well nourished. If this is the
approach one takes, then in Afghanistan, which has survived over twenty years of conflict and
instability, the dismal health statistics are a reflection of the lack of health infrastructure which has
impeded the individuals to achieve their maximal capabilities.
14
Since the end of 2001, real progress has been made by the Afghan government and people to
secure peace, stability and to rehabilitate the devastated infrastructure. Despite these efforts
Afghanistan remains one of the poorest and least developed countries in the world with some of
the worst health statistics. Maternal mortality rate is reported to be 1600 per 100,000 live births;
the under-five mortality is estimated as 257 per 1000 births and infant mortality as 165 per 1000
births [Ministry of Public Health, 2004]. In addition to poor health statistics, there is no information
on the numbers of Afghans with disabilities and mental health impairments. When it comes to
mental health, a survey conducted by the CDC showed that there was an overall prevalence 67.7%
and 71.7% of non-disabled and disabled respondents with symptoms of depression. When it
comes to symptoms of anxiety, the prevalence rates were 72.2% and 84.6% for non-disabled and
disabled respondents, respectively [Cardozo et al., 2004]. These numbers signify many years of
conflict and a disjointed and dysfunctional health care system and Ministries of Health without
coherent vision and policies.
Into this arena, Ministry of Health (MoH) was keen to adopt a wide vision as the corner stone of all
health policies. The MoH and the subsequent Ministry of Public Health (MoPH), established after
the presidential elections in 2004, embarked on the development of the health sector with the goal
of developing better health for all Afghans in order to contribute to economic and social
development. The MoPH strategy focused on the development of the foundations for the delivery
of equitable health services to all Afghans with a specific focus on the limited resources available
and the use of evidence to base policies. Health sector research became a priority in the Ministry
with the motto of ‘evidence based decision making’. The MoPH with the help of UNICEF embarked
on the Multiple Indicator Cluster Survey (MICS) in 2003 and with the assistance of Management
Sciences Health carried out the National Health Resources Assessment (NHRA) that same year.
These surveys were undertaken in order to gain knowledge of the status of health care and
services in Afghanistan.
When it came to the fields of mental health and disabilities the knowledge gap was even greater.
No nationally representative survey had been carried out in Afghanistan, which outlined the
prevalence of mental health illnesses and enumerated the numbers and types of persons with
disabilities, which existed. The ‘Mental Health, Social Functioning, and Disability Survey’ of the
15
CDC, which provided prevalence rates for mental health illnesses such as depression and anxiety,
however fell short of providing information of the functionalities and social challenges faced by
persons with mental illness and disabilities [Cardozo et al., 2004, Scholte et al., 2004].
Furthermore, it did not provide national level prevalence rates of types of disabilities present in the
population, nor any information on the coping strategies and stigmatisation of persons with
disabilities. Finally, respondents to this survey might have a tendency to aggravate their symptoms
in the hope to receive some assistance [Ventevogel, 2005].
Supported by the donors, WHO, UNICEF, and other development partners, the MoPH in 2002
developed a national package of health services, the Basic Package of Health Services (BPHS),
which addressed the greatest health needs of the population. The focus was placed on providing
cost effective services, which would have the greatest impact on the major health problems in both
rural and urban settings. This document was the first product of the new Ministry in the post-
Taliban era and it was and still is the basis for implementation in the health sector. The BPHS
covers 7 health categories, which are felt to be of priority in Afghanistan. These categories are
maternal and newborn health, child health and immunization, public nutrition, communicable
diseases, with concentration on Tuberculosis and Malaria, mental health, disabilities, and finally the
supply of essential drugs. All categories are considered first tier priorities since the review of the
BPHS in 2004 [MoPH, 2005].
In 2005, when it came to the revision of the BPHS, and the elaboration of services for Afghans
with mental health impairments, the lack of data available in these two fields became quickly
evident. Thus, the MoPH became a partner in the NDSA, which turned out to be the first to
attempt to address the severe knowledge gap in mental health and disability. This void has
contributed to the inability of the MoPH to develop a cohesive strategy on providing mental health
services and health care to persons with disabilities.
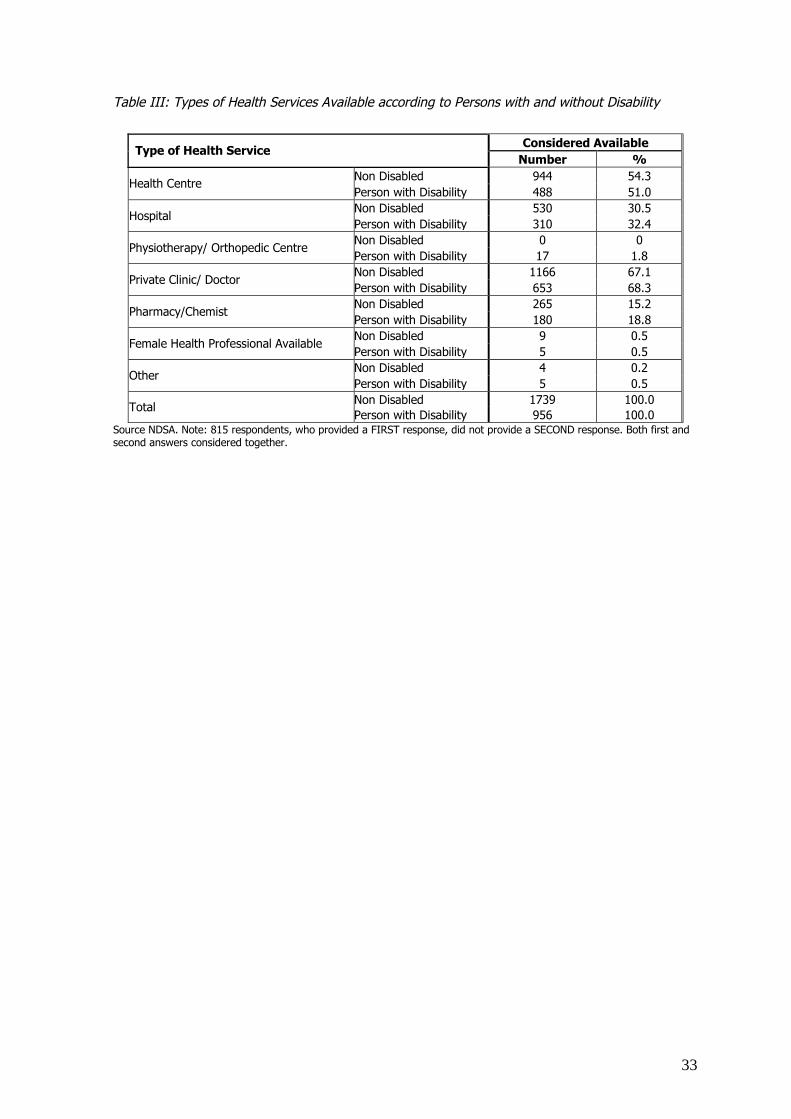
Table III: Types of Health Services Available according to Persons with and without Disability
The BPHS is supposed to establish health facilities on the entire territory with adequate staff and
drugs supply [MoPH, 2005]. For the time being, the situation is still challenging, and many villages
are out of reach of health facilities and health workers. People indifferently use modern medicine
16
and traditional cures such as Tibbi or Tabi Unani, bonesetter, Mullahs, pilgrimage… Table 3 reports
the responses of the persons with disabilities and the non-disabled to the types of health services
available. The respondent was asked to rate answers by order of importance. The importance that
the respondent gives was left to his/her decision. It might be efficiency, distance, and cost-
effectiveness. In case of request, the surveyor was told to precise: “Where do you go, first, in case
of a health need? In second choice?”. The results show that the persons with disabilities and non-
disabled have similar first rank responses: 51% of persons with disabilities and 54.3% of non-
disabled report having a health center available; 68.3% and 67.1% respectively report having a
private clinic or doctor available; 32.4% and 30.5% respectively report having a hospital available.
The objectives of covering the entire territory with health facilities adequately staffed and with
sufficient drugs supply remains unmet [MoPH and JHUBSPH, 2005].
In the mental health and disabilities categories, very few services are covered. In the field of
mental health the only two services that are covered are community based mental health
management and health facility based mental health treatment of outpatients and inpatients with
limited anti-psychotic medications and antidepressants. In disability, the services covered under
the BPHS are limited to physiotherapy which is integrated into Primary Health Care (PHC) services
and orthopaedic services expanded to the hospital level. Early on, the designers of the BPHS
recognized that mental health and disability were of importance in the health sector, however
these topics have been limited to second tier priorities of the BPHS until 2004 largely due to lack of
available resources and capacity to integrate these services fully [Ventevogel et al., 2006].
In essence the lack of enumeration of persons with mental health impairments and/or disabilities
has created limited opportunity for the challenges faced by these persons to be addressed. Lack of
information here clearly translated to lack of appropriate policies and strategies to provide this
segment of the afghan population the chance to fully achieve their maximum functionings.
Since the presidential elections in 2004 and the subsequent cabinet change, including
administrative changes in the MoPH, there has been limited change in the position of disabilities
and mental health in the policies and strategies of the ministry. The new administration has been
keener to integration of these two categories in the national dialogue. For the first time, disabilities
17
and mental health had their own policy statements, however limited capacity and information on
the magnitude of these categories has been cited for lack of action to interpret the policy into
action plans.
With the emergence of the National Program for Action on Disabilities (NPAD), headed by the
UNDP, the MoPH has been one of the ministries targeted to have a disability advisor. In mid 2005,
the MoPH National Disability Advisor has been hired and end of 2006, two international advisors
have also been recruited. They are tasked with the integration of disability and mental health
issues into the policies and programmes of the ministry. Convincing the donors, implementing
partners and the administration of the MoPH to expand the BPHS from its focus on women and
children to integrate persons with mental impairments and disabilities as a national priority even
now having data available is a daunting task. This is compounded by the fear of the budgetary
implications on the health sector of such an expansion of services.
The foundation of a disability strategy in Afghanistan
If we consider, on the basis of Sen’s theory, that “disability can be understood as a capability or a
functioning deprivation that results from the interaction of (i) an individuals personal characteristics
(e.g., age, impairment) and (ii) his or her basket of available goods (assets and income) and (iii)
the environment (social, economic, political and cultural)” [Mitra, 2003, p. 4], then public policies
should be aiming at increasing assets of the persons with disabilities and modifying the
environment to better include them in mainstreaming livelihood and society.
The MMD which was established in the beginning of the Soviet influence in Afghanistan with the
aim to pay welfare pensions to families of those killed in war and to war disabled people.. The
ministry still provides now pensions to a recipient base that has been expanded in 2003 to include
those who have lost more than 30% of mobility, sight or hearing. Intellectual impairment is not
included as there is no expertise to assess it. Furthermore there has been a distinct lack of
information in Afghanistan on the enumeration of Afghans with disabilities levels and types of
disabilities and the challenges faced by them. This divergence between the perceived role of the
MMD as the principle actor championing the causes of persons with disabilities and the reality that
has till now functioned as a pension agency is largely due to the limited definition of disability to
18
the ‘war disabled’. This lack of vision and exclusiveness has lead to the necessity of developing
inclusive programmes run by other actors: delivering services, representing persons with
disabilities, defining a strategy are assumed and carried out by national programs implemented by
MMD partners such as the UNDP and NGOs.
In 1995, UNDP set up the Comprehensive Disabled Afghans Program (CDAP). The CDAP was
designed as a comprehensive model of services for and with persons with disabilities, based on
Community Based Rehabilitation (CBR) in 50 districts. During the period 1995-2001 there was no
effective government, and the CDAP managed the coordination of activities in disability among the
relevant agencies and NGOs from Pakistan. The CDAP was acting essentially as a direct service
provision component of the MMD. After the end of the Taliban regime and exile in Pakistan, the
CDAP management moved back to Afghanistan. This close physical proximity could have led to an
integration of the CDAP staff into the MMD. However, this did not occurred, even in 2002, when
the CDAP was newly mandated to reinforce the capacity of the MMD considered as a weak ministry
by all actors [Italian Cooperation, 2003]. An evaluation of the needs of the Ministry by the CDAP
showed the necessity to launch a structural reform of procedures and increase the capacity of the
staff to meet their obligations. CDAP continued to be a completely independent structure with
specific staff and offices in the provinces, providing services for persons with disabilities. At the
Ministry level, the CDAP team in charge of following the different activities (special education,
physical rehabilitation, employment support and outreach programme) were providing feedback
only to the Minister. The only concrete interaction was the capacity building officer of CDAP efforts
who achieved the modernization of the welfare pension system in 2003/04. No real synergies
existed, leading to the paralleled functioning of two structures, one providing mainly pensions and
creating a list of persons with disabilities benefiting from the welfare pension system, and the
other, the CDAP, implementing services.
The idea of creating a National Disability Commission was launched by the CDAP, the MMD and
different donors at the beginning of 2003 to overcome these difficulties. It was an attempt to
coordinate actors by giving the leadership to the Government and having a strong back-up from
UNDP staff and other experts [Italian Cooperation 2003]. But this project was dropped, essentially
19
because a Ministry is politically more visible than a Commission, even when linked directly to the
President. Political considerations were put before technical efficiency.
In 2003, after an external evaluation, the CDAP program was revamped. Direct service provision
was eliminated, emphasis was placed on NGO sub-contracting and the program was limited to
“focus much more strongly on policy definition, development and wider institutional reform with
the Government of Afghanistan to establish appropriate structures and processes for the
coordination of the disability sector” [UNDP, 2004, p. 6]. This restructuring led the way to the
development of the National Program for Action on Disability (NPAD) based and funded through
UNDP in early 2005. This program is designed to be the central coordination body, which provides
support to selected Ministries to push for the inclusion of persons with disabilities into the national
dialogue and policies. The strategy of NPAD has been to place advisors within key ministries,
mainly MoPH, Ministry of Education, and the new Ministry of Martyrs and Disabled and Social
Affairs, providing technical support.
While NPAD has been structured to assume the role of policy definition and coordination of the
disability sector in close collaboration with the MMDSA, the program has suffered the same
limitations of its predecessor CPAD. This is largely due to the limited capacity of all actors to
comprehend the needs of persons with disabilities in Afghanistan. Without this key information
disability stakeholders have been unable to develop comprehensive policies working towards
improving the capabilities of persons with disabilities. Therefore, knowledge based on research
might be the way to improve the coordination of actors and the legitimacy of policies and
programmes.
The National Disability Survey of Afghanistan (NDSA): A CapabilityPerspective on Disability
In this context, the decision to launch the NDSA was undertaken to meet the need of a national
disability strategy aiming at mainstreaming persons with disabilities into existing public policy,
coordinating actors and answering existing needs. The research was steered by the expectations
and queries of stakeholders who would use the results and findings.
Objectives of the survey
20
For the NDSA the main aim was to provide a comprehensive picture of disability in Afghanistan,
prevalence rates and information regarding all major issues concerning access to public services,
livelihoods and social participation of persons with disabilities. However, the objectives were also
dependent on the demands of the funding agencies as well as the political partners. Although the
overall goal of the survey seemed clear, its political implications and consequences were less
explicit. The results of the survey would impact the disability scene by putting forward findings that
would not always be in line with the beliefs that programmes and policies have been based on to
date. The study was aimed at providing insights and recommendations for the Government even
though other organisations would also benefit from it. However from a research perspective the
objectives were clear:
1. To measure prevalence of disability by type of disability;
2. To provide insight into the needs and opportunities of persons with disabilities in Afghanistan.
These may include needs in terms of rehabilitation, education, employment, vocational
training, social integration and political participation;
3. To identify barriers, difficulties and stigmatisation that persons with disabilities face in
everyday life;
4. To provide strategic guidelines on how to overcome these difficulties.
The NDSA contributes to the mainstreaming of disability issues into development studies looking at
livelihoods of persons with disability [Seddon et al. 2001]. The methodology adopted was based on
these research purposes.
Operationalizing definitions
Based on the abundance of literature that exists on the concept of disability, the NDSA had
adopted a functional definition keeping in mind:
1. Firstly, the need to be functional in order to be able to design a questionnaire that takes into
account individual, institutional and societal factors and their interrelations;
2. Secondly, the view on disability needs to be relevant to the Afghan context and take into
account gender, cultural, ethnic and social factors.
21
“Disability is thus the condition that results from the interaction between an individual impairment
in functioning and the community and social resources, beliefs and practices that enable or prevent
a person from participating in all spheres of social life and taking decisions that are relevant to
his/her own future” [Bakhshi et al., 2006].
There are evidently similarities between the various definitions of disability used by the ICF, the
medical and the social model [Burchardt, 2004]. For the NDSA, emphasis is put on the interplay
between the individual and the collective. Within the human development perspective, the
definition of disability devised for the NDSA needed to take into account diverse aspects:
1. The individual’s potentialities and vulnerabilities;
2. The opportunities offered by the environment the individual lives in;
3. The agency role of the individual or communities, which looks at the extent to which the
person (or the group) considers him/herself as the main actor and decision maker in his/her
own life.
The elaboration of the tool is the result of the above choices made by the authors. Disability
matters are examined in a comprehensive manner using the capabilities approach and looking at
the various factors that contribute to the quality of life of individuals. To comprehend the cultural
norms and beliefs, open discussions regarding cultural practices, religious beliefs, and ways of life
using basic qualitative methods (life stories, focus group discussions, open-ended interviews) have
been conducted.
For the NDSA, being well aware of the importance of the detection of disability, we adopted a
screening tool composed of 27 questions in 4 sections: physical, psychological, intellectual and
relational difficulties. Questions are looking at the functionings of the individual, relate to the
concept of what is disabling and constitutes an impediment to living a fulfilling life within the
community and society. The answers were cross-checked with 13 possible categories identified by
the interviewer him/herself in the checklist. Correspondence between the 2 classifications was
further verified by the Master Trainer/ Monitor (MTM) who met the person in case of doubt. This
way of categorising disabilities allows cross-table analysis and multidimensional analyses [Benzecri,
1992].
22
Disability being a complex social phenomenon, a great number of questions are needed to depict
its various facets [Altman, 2001]. The questionnaire is composed of different units offering
elements of knowledge and persons with disabilities’ opinions on the following topics [Bakhshi et
al., 2006]: family and demographic characteristics, health, education, activity, unemployment,
underemployment, livelihood, income, social participation. Firstly, the questionnaire identifies the
resources (family, community and state level) that are available. Secondly, it assesses the access
to these resources. It then detects the existing barriers that prevent persons with disabilities from
accessing these resources. These can be physical, social and/or psychological. It explores schemes
used by persons with disabilities to overcome these barriers, and the range (or limitations) of
choices that the persons with disabilities perceive as open to them. Finally, the questionnaire looks
at ways to enhance persons with disabilities’ capabilities, by defining strategies that expand real
choices. Finally, questions were designed to reflect the prejudice and discrimination faced, and go
into arrangements to bring about long-term changes. In a context where state structures are
scarce, the community constitutes the essential resource system to rely upon. It has developed
certain mechanisms that include/exclude individuals according to perceptions and beliefs.
Survey Methodology
The NDSA funded by UNDP/UNOPS/UNMACA, European Union, France, Swiss Cooperation,
Voluntary Trust Fund and Handicap International is a probability proportional to size, three stage
random sample survey. The first stage of sampling is the district. Two sources of population data
were used to define the district population frame. For 30 provinces, the 2003-2004 population pre-
census figures were available. As a result the districts were ordered based on the population size.
For the remaining 4 provinces, which were not covered due to security issues, the Central Statistics
Office provided projections calculated based on the 1979 census and the same ordering was done.
The required number of districts to be included in the survey was then selected. As a result the
NDSA was carried out in 175 districts throughout the country and including all provinces.
The second stage of sampling is to locate the village or section of town. All sections of towns and
villages in a district were listed and then one or more were randomly selected. At the third stage, a
constant number of 30 households per cluster were randomly selected for a total of 5250. The
23
sample size allows for estimation of a disability rate that is 8% or greater with 95% confidence and
15% precision when considering a design effect of 2.
In each cluster, the team proceeded to the center of the cluster indicated by the Mullah or another
authority. It chose a direction by spinning a pointer. It numbered the houses from 1-30 in that
direction. One household between 1 and 30 was randomly selected. That first household, and the
nearest 29 were selected for interview. The next 29 households of the cluster were chosen using
the “nearest front door” method.
All the persons with disabilities older than 4 years old were interviewed. The detection of persons
with disabilities was done through the screening questionnaire mentioned earlier. The head of
household answered the screening questions regarding all the members of his household. Each
question refers to the term difficulty or ability to do, avoiding stigma and negative stereotypes. The
NDSA made the choice to use the term “difficulty” or mushkel in Dari. This term is less threatening
and constitutes less of a ‘label’ for the persons concerned.
In order to better comprehend living conditions and coping strategies of persons with disabilities, a
control group was interviewed. Thus, we determine whether a given problem is specifically linked
to disability, or whether the family or the community as a whole shares this problem. Two sub-
groups without disability have been interviewed. One is composed of persons without disability
within the household of a person with disability matching her/him in terms of sex and age. The
second sub-group is composed of persons living in households where no person with disability
lives. This control person is randomly selected among persons aged more than age 4 within every
fifth household where there is no person with disability. This allows a comparison at the individual
level but also at the household level to see how disability impacts the family as a functioning
entity.
The NDSA training was more than a month long. The NDSA surveyors were trained to explain the
objectives of the survey. Special emphasis was given to the fact that the survey team needed the
help of the people to gather information. These training sessions were elaborated with the help of
a number of experts working in the field of disability and with the participation of persons with
disabilities. The training looked at sensitization pertaining to the concept of disability; it worked on
24
existing prejudice and attitudes [Bakhshi et al., 2006]. The rest of the training focused on survey
tools and interview techniques. Finally, field tests were organized for the survey teams.
Strict ethical guidelines were followed. Respondents were systematically informed that no direct
benefit will be provided and it was stated at the beginning of the questionnaire.. Likewise
provincial and district officials were notified of the presence of the survey teams and permission
sought to enter clusters. Furthermore, permission was gathered from the village leaders, abob, or
mullahs. Household consent was obtained from the head of the household for those individuals
interviewed verbally.
During the fieldwork the teams faced a range of challenges, mainly geographical conditions and
security problems. For instance, in a village of Nangarhar province in eastern Afghanistan, the
villagers met the team with extreme skepticism because they feared the data would be given to
the Afghan National Army (ANA). As the team learned, the villagers were at conflict with the
security commander responsible for the district. Moreover, about a week before, the commander
sent two soldiers to this village who were subsequently killed by the villagers and their uniforms
hanged on a tree by the entrance to the village. The team leader however explained the purpose
of the survey and reassured the villagers about confidentiality. Afghanistan’s demanding geography
also obliged to plan the fieldwork according to seasons. During the winter time many clusters were
not accessible due to snow and remoteness. The team in some case had to hike through the
mountains to reach the village. These are few example of challenges met during the fieldwork.
Conclusion informing poverty and vulnerability policy via the NDSA: Lookingbeyond numbers
A unique perspective, which has emerged in the interaction between research in the disability field
and policy development, has been the use of research in determining government agencies
standing and future role in the disability field. Before the launching of the NDSA, research and
studies attracted few resources. Additionally, since many years, the CDAP included research in
both its provisional budget and in its strategic papers. However, until the NDSA was launched after
8 years of programme, the only study funded by CDAP was an awareness qualitative study. Yet,
this was an important start: as Peter Coleridge, former CDAP coordinator, stated, disability is a
25
rights issue and one can only start to tackle this issue if one deals with people's attitudes
[Coleridge, 2003].
Research is asserted as being a priority in the expected key outcomes of NPAD strategic planning
document: an accessible national knowledge bank created on disability based on information in-
country and international information gained from surveys, research and lessons learnt from
programme implementation [UNDP, 2004].
With the NDSA, the capabilities approach has been translated into practical field research in one of
the most dynamic and fast moving policy settings. Afghanistan is now 5 years post-conflict and has
been in the throes of rapid policy and infrastructure development. With the NDSA providing data
and analysis in the field of disabilities, one must stop to ask, where does the UN agencies and
other international partners fall to carry the mantle of the information from research to policy?
Now, who takes on the responsibility for translating this information to action? Does this fall on the
researchers or on the policy developers and implementers? One may argue that the limited
capacity of the Government in this field precludes them from taking the more active role in the use
of this data, but that the UN agencies and international partners, who have an understanding of
the field of human development which is derived from the capabilities approach, should carry forth
this function. Since the Government has the ultimate responsibility for the development of
sustainable and practical solutions to the problems inherited after over 20 years of conflict one
could easily argue that it is they who have the burden of carrying this research forward to program
and policy development in partnership with the development partners.
Gathering of knowledge on livelihood, vulnerability, risks and poverty provides understanding,
information and insights necessary for policy formulation and strategic planning in the area of
disability. A national disability strategy framework based on such principles as empowerment and
mainstreaming aims at increasing access for persons with disabilities to social and economic
opportunities. Designs of policies and strategies have to rely on scientific based knowledge and on
participation of persons with disabilities themselves in the elaboration process [Abberley, 1997,
Morris, 1993].
26
This view, which has been put forward by a number of disabled persons’ organisations, tends to
look at the barriers that exist within the social context and that prevent a person from achieving
the same level of functioning as that of a non-disabled person. In this perspective it is society that
needs to be redesigned in order to take into account the disabled persons’ needs. Mainstreaming
persons with disabilities is a progressive way of reshaping society in order to better include them.
Equalisation of opportunities is a major goal put forward by the new United Nations Convention on
the Rights of Persons with Disabilities adopted by the General Assembly on the 13th December
2006.
27
References
Abberley, P. (1997) ‘The limits of classical social theory in the analysis and transformation ofdisablement’, in Barton L. and Oliver M. (Eds.), Disability Studies: Past Present and Future, Leeds:The Disability Press, pp. 25 – 44.
Alkire, S. (2003) Valuing Freedoms: Sen’s Capability Approach and Poverty Reduction, OxfordUniversity Press, Oxford.
Altman, B. M. (2001) ‘Definitions of disability and their operationalization, and measurement insurvey data: an update’, In Altman Barbara M., Barnatt Sharon N. (Eds), Exploring Theories andExpanding Methodologies: Where we Are and Where we Need to Go, Elsevier Jai, Oxford, vol. 2,pp. 77-100.
Amundson, R. (2000) ‘Against normal function’. Studies in History and Philosophy of Biological andBiomedical Sciences, 31, 33-53.
Bakhshi, P., Rolland, C., and Trani, J. F. (2006) Conducting Surveys on Disability a ComprehensiveToolkit, Handicap-International, Lyon, http://www.handicap-international.org/dans-le-monde/nos-pays-dintervention/programmes/afghanistan/afghanistan-toolkit-on-disability/index.html
Bakhshi, P., Dubois, J.-L. and Trani J.-F. (2004) ‘Enhancing security and social sustainability:strengthening capabilities: the case of persons with disabilities in Afghanistan’, 4th InternationalConference on the Capability Approach: Enhancing Human Security, 5-7 September 2004,University of Pavia, Italy.
Barnes, C. (1997) ‘A legacy of oppression: a history of disability in western culture’ in Barton L. and
Oliver M. (Eds.), Disability Studies: Past Present and Future, Leeds: The Disability Press, pp. 3 –24.
Barnes, C. (1991) Disabled People in Britain and Discrimination. London, Hurst and Co.
Benzecri, J.P. (1992) Correspondence Analysis Handbook, New York: Marcel Dekker.
Burchardt, T. (2004) ‘Capabilities and disability: the capabilities framework and the social model ofdisability’, Disability and Society, 19 (7): 735-751. 2004.Cardozo, B.L., Bilukha, O.O., Crawford, C.A., Shaikh I., Wolfe, M.I., Gerber, M.L., Anderson, M.(2004) ‘‘Mental health, social functioning, and disability in post-war Afghanistan’, Journal ofAmerican Medical Association, 4.
Civic Voluntary Group (2003) ‘Survey results on access to education for disabled in Kabul’,Submitted to the Italian Cooperation Educational Sector, April–July 2003, Draft.
Coleridge, P. (2003) ‘Comprehensive Disabled Afghan Programme’, Radio Netherlands report ondisability in Afghanistan, http://www2.rnw.nl/rnw/en/features/humanrights/disability001127.html.
Coleridge, P. (2002) ‘Community based rehabilitation in a complex emergency: study ofAfghanistan’, in M. Thomas, and M.J. Thomas (eds), Selected Readings in CBR - Series 2: Disabilityand Rehabilitation Issues in South Asia, National Printing Press, Bangalore, pp. 35-49.
Coleridge, P. (1998) ‘Development, Cultural Values and Disability: The Example of Afghanistan’, inStones M. (ed.), Disability and Development, The Disability press, Leeds.
Court, J. and Maxwell, S. (2005) ‘Policy entrepreneurship for poverty reduction: bridging researchand policy in international development’, Journal of International Development, 17, 713-725.
Douglas, M. (1966) Purity and Danger, London, Routledge & Kegan Paul. ed.
Dubois, J-L., and Rousseau, S. (2001) ‘Reinforcing household’s capabilities as a way to reducevulnerability an prevent poverty in equitable terms’, Justice and Poverty: Examining Sen’sCapability Approach, 1st Conference on the Capability Approach, Cambridge University 5th-7thJune 2001.\

28
El Harizi, K. (2006) ‘Empowering the rural poor under volatile policy environments in the near eastand north Africa region research project: Sudan case study’, final report, IFPRI-DGSD, March 2006,London.
Erb, S. and Harriss-White, B. (2001) ‘Disability and Incapacity’, in Harriss-White B. and JanakarajanS. (eds) Reforms And Development: Essays On Long Term Village Change And RecentDevelopment Policy In South India, India.
Finkelstein, V. (1981) ‘To deny or not to deny disability’, in A Brechin et al. (Eds), Handicap in aSocial World, Sevenoaks: Hodder and Stoughton.
Government of Afghanistan, Asian Development Bank, United Nations Assistance Mission forAfghanistan, United Nations Development Programme and World Bank, (2004) SecuringAfghanistan’s Future: Accomplishment and the Strategic Path Forward, Kabul.
Harriss-White, B. (1996) ‘The Political Economy of Disability and Development: With SpecialReference to India’, Discussion Paper No. 73, United Nations Research Institute for SocialDevelopment, Geneva.
Hunt, P. (1966) 'A critical condition' in Hunt, P. (ed.) Stigma: The Experience of Disability, London,Geoffrey Chapman, pp. 145-164.
Italian Cooperation (2003), The Comprehensive National Disability Policy in Afghanistan submittedTo Minister of Martyrs and Disabled, Kabul, October, 2003.
Lang, R. (2001) ‘Understanding disability fro a south Indian perspective’, paper presented at theAnnual Conference of the Society for Disability Studies, June 20th to 23rd, 2001, Winniped,Manitoba, Canada, http://www.ee.umanitoba.ca/~kinsner/sds2001/proceed/pdocs/htms/22.HTM.
Marks, D. (1999) Disability: Controversial Debates and Psychosocial Perspectives. London,Routledge.
Miles, M. (2002a) ‘Formal and informal disability resources for afghan reconstruction’. WorldQuarterly Vol. 23, pp. 945-959.
Miles, M. (2002b) ‘Epilepsy in the Afghan village’. At:http://www.disabilityworld.org/01-03_02/arts/afghan.shtml
Miles, M. (2002c) ‘Disability in the Afghan school’. At:http://www.disabilityworld.org/01-03_02/arts/afghan.shtml
Miles M. (2001) ‘Disabled Afghans in the cross-fire of cultures’, http://www.disabilityworld.org/09-10_01/news/afghan.shtml.
Miles, M. (1997) ‘Afghan children and mental retardation: information, advocacy and prospects’,Disability & Rehabilitation, 19: 496-500.
Miles, M. (1990) ‘Disability and Afghan reconstruction: some policy issues’. Disability, Handicapand Society, 5/3: 257-267.
Ministry of Martyrs and Disabled and United Nations Development Programme (2005), NationalProgram for Action on Disability, Kabul.
Ministry of Martyrs and Disabled (2003), Profile and History,http://www.disabilityafghanistan.org/profile.htm.
Ministry of Public Health, (2005) Basic Package of Health Services, Ministry of Public HealthPublication, Kabul.
Ministry of Public Health, (2004) Afghanistan Health Statistics, Ministry of Public Health Publication,Kabul.
Ministry of Public Health and Johns Hopkins University Bloomberg School of Public Health (2005),Report on Health Seeking Behaviour, Health Expenditures, and Cost Sharing Practices inAfghanistan, Kabul, 60 pp.
29
Mitra, S., (2003) “The capability approach of disability”, From Sustainable Development toSustainable Freedom, 3rd Conference on the Capability Approach, 7th-9th September 2003,University of Pavia, Italy.
Morris, J. (1993) Independent Lives - Community Care and Disabled People, London: Macmillan.
Murphy, R. (1987) The Body Silent, New York, Henry Dolt.
Nussbaum, M. (2000) Women and Human Development: The Capabilities Approach, CambridgeUniversity Press, Cambridge.
Oliver, M. (1996) Understanding Disability: from Theory to Practice, Basingstoke, Macmillan.
Pfeiffer, D. (2001) ‘The Conceptualisation of disability’, In Altman, Barbara M., Barnatt, Sharon N.(Eds), Exploring Theories and Expanding Methodologies: Where we Are and Where we Need to Go,Elsevier Jai, Oxford, vol. 2, pp. 29-52.
Ryan, J. G. and Garrett, J. L. (2003) ‘The impact of economic policy research: lessons onattribution and evaluation from IFPRI’, Impact Assessment Discussion Paper no. 20, InternationalFood Policy Research Institute, October 2003, http://www.ifpri.org/impact/iadp20.pdf.
Scholte, W.F., Olff M., Ventevogel, P., Vries (De), G. J., Jansveld, E., Cardoso, B.L., and GotwayCrawford C.A. (2004) ‘Mental health symptoms following war and repression in easternAfghanistan’, Journal of the American Medical Association, 2004, 292:585-593.
Schütte S. (2004) ‘Urban vulnerability in Afghanistan: case studies from three cities’, AfghanistanResearch and Evaluation Unit, AREU Working Papers, Kabul.
Seddon, D., Lang R., Daines, V. (2001) ‘Mainstreaming disability issues into development studies –in theory and practice’, paper presented at the Annual Conference of the Society for DisabilityStudies, June 20th to 23rd, 2001, Winniped, Manitoba, Canada,http://www.ee.umanitoba.ca/~kinsner/sds2001/proceed/pdocs/htms/27.HTM.
Sen, A. (1992) Inequality Re-examined, Oxford University Press, Oxford.
Sen, A. (1999) Development as Freedom, Oxford University Press, Oxford.
Shakespeare, T. (2001) ‘The social model of disability: an outdated methodology?” In AltmanBarbara M., Barnatt Sharon N. (Eds), Exploring Theories and Expanding Methodologies: Where weAre and Where we Need to Go, Elsevier Jai, Oxford, vol. 2.Shakespeare, T. (1994) `Cultural Representations of Disabled People: Dustbins for Disavowal'Disability and Society No. 9, Vol. 3. pp. 283-301.
Thakkar, M., Cerveau, T., and Davin, E., (2004) ‘Afghan perception on disabilities, a researchproject on the perceptions and practices regarding disability in Afghanistan, to Inform aCommunication Strategy’, Study carried out by ALTAI Consulting for UNICEF, UNOPS, UNDP,Kabul.
Terzi L., (2003) ‘A Capability perspective on impairment, disability and special needs: towardssocial justice in education’, paper presented at the 3rd Conference on the Capability Approach,From Sustainable Development to Sustainable Freedom, 7th-9thSeptember 2003, University ofPavia, Italy.
Trani, J. F. (2004) A new Structure in the Government of Afghanistan for the Promotion of theRights of Persons with Disabilities: The National Disability Commission, Report to the Minister ofMartyrs and Disabled, Kabul, www.disabilityafghanistan.org, September 2004.
Turmusani M. (2004) ‘Disabled people and education in Afghanistan’, Disability World, no. 23,April–May2004.
Turmusani, M. (2003) ‘Poverty and disabled people in development context: examples from Jordanand Afghanistan’. Paper presented at the Conference ‘Staying Poor: Chronic Poverty andDevelopment Policy’, Manchester, April 2003.http://www.chronicpoverty.org/pdfs/conferencepapers/Turmusani.pdf
United Nations Development Programme (2004) National Program for Action on Disability, Theexpected outcome, Kabul.
30
United Nations Development Programme /United Nations Operation Programme Services (1999)‘Comprehensive disabled Afghan’s program: integrating disabled and marginalized people inAfghanistan’. Journal of Mine Action, Fall 1999-Volume3, No.3.
United Nations International Children and Education Fund and Central Statistics Office ofAfghanistan (2003) Multiple Indicators Cluster Survey, Kabul.
Ventevogel, P., Azimi, S., Jalal, S., and Kortmann F. (2002) ‘Mental health care reform inAfghanistan’, Journal of Ayub Medical College, Abbotabad, December 2002, 14 (4):1-3.
Ventevogel P., Nassery R., Azimi S., and Faiz H. (2006) « Psychiatry in Afghanistan », CountryProfile, International Psychiatry Bulletin of the Board of International Affairs of the Royal College ofPsychiatrists, volme 3, number 2, april 2006, 36:38.
Ventevogel, P. (2005) ‘The psychiatric epidemiological studies in Afghanistan: a critical review ofliterature and future directions’, Journal of Pakistan Psychiatric Society, Abbotabad, January 2005,Volume 2 Number 1:9-12.
Vulnerability Analysis and Mapping Unit of the World Food Programme and the VulnerabilityAnalysis Unit of The Ministry of Rural Rehabilitation and Development (2004), Reports on Findingsfrom the 2003 National Risk and Vulnerability Assessment (NRVA) in Rural Afghanistan, December2004, 123 p., http://www.mrrd.gov.af/vau/.
Wardak, A. and Turmusani, M. (2003) ‘Development agenda in Afghanistan: disability model’.Japanese Journal of Trade and Industry, November/December 2003.
Wardak, A., Faiz I.M., and Turmusani, M. (2003) Disability policy development in Afghanistan:towards barriers free society. UNESCAP, Bangkok.
World Health Organization (1987) International Classification of Impairments, Activities andParticipation, WHO, Geneva.
World Health Organization (2001) International Classification for Functioning, Disability and Health,Geneva.
Yeo, R. (2001) ‘Chronic Poverty and Disability’, Action on Disability and Development, Backgroundpaper number 4, august 2001.

31
Table I: Level of Activity of Afghans Aged 15-64
Landmine/UXOSurvivors
Other WarSurvivors
Other Causes:Disease,
Accident...
Non-Disabled
Total
Number 15589 16888 68853 1260131 1361461notworking % 46.2 37.1 47.3 22.4 23.3
Number 18187 28580 76647 4361093 4484507working
% 53.8 62.9 52.7 77.6 76.7
Male
Total Number 33776 45468 145500 5621224 5845968
Number 3248 5846 141602 5389334 5540030notworking % 100.0 90.0 96.9 93.3 93.3
Number 0 650 4547 389731 394928working
% 0.0 10.0 3.1 6.7 6.7
Female
Total Number 3248 6496 146149 5779065 5934958
Source: NDSA. Note: Weighted by population of the province.
32
Table II : Ill-treatment of children aged 5-14
Child with disabilityNon-disabled
child Total
Number 36375 170053 206428Ill-treatment % 18.9 1.2 1.5
By family Number 12991 115750 128741
% 25.6 60.9 53.5
By other child Number 27281 23384 50665% 53.8 12.3 21.0
By adult outside Number 9744 33127 42871
% 19.2 17.4 17.8
By Government person Number 0 17928 17928% 0.0 9.4 7.4
By other person Number 650 0 650
% 1.3 0.0 0.3
Number 20136 99771 119907Abuses % 31.3 43.5 40.9
Peer/ stare Number 10393 9743 20136
% 16.2 4.3 6.9
Push Number 8444 7145 15589
% 13.1 3.1 5.3Throw stones Number 3898 650 4548
% 6.1 0.3 1.5
Laugh Number 9743 25982 35725
% 15.2 11.3 12.2Hit Number 11043 85871 96914
% 17.2 37.5 33.0
Other Number 650 0 650
% 1.0 0.0 0.2Source: NDSA. Note: Weighted by population of the province. The first row indicates the proportion of children ill-treated.The other rows indicate who are the persons who ill-treat and what are the types of ill-treatment the children in proportionof children mistreated (proportion given by the first row).
33
Table III: Types of Health Services Available according to Persons with and without Disability
Considered AvailableType of Health Service
Number %
Non Disabled 944 54.3Health Centre
Person with Disability 488 51.0
Non Disabled 530 30.5Hospital
Person with Disability 310 32.4
Non Disabled 0 0Physiotherapy/ Orthopedic Centre
Person with Disability 17 1.8
Non Disabled 1166 67.1Private Clinic/ Doctor
Person with Disability 653 68.3
Non Disabled 265 15.2Pharmacy/Chemist
Person with Disability 180 18.8
Non Disabled 9 0.5Female Health Professional Available
Person with Disability 5 0.5
Non Disabled 4 0.2Other
Person with Disability 5 0.5
Non Disabled 1739 100.0Total
Person with Disability 956 100.0Source NDSA. Note: 815 respondents, who provided a FIRST response, did not provide a SECOND response. Both first andsecond answers considered together.

34
i The Comprehensive Disabled Afghans’ Programme started in 1995 as a UNDP/UNOPS initiative to addressthe needs of people with disabilities in Afghanistan. CDAP had three principal areas of work until its shuttingdown in 2004:- Community-based physical and socio-economic rehabilitation activities in 48 districts of 16 provinces.-Capacity building of the Ministry of Martyrs and Disabled (MMD) and welfare reform.- Policy development.