Embed Size (px)
Citation preview

Director of Infection Prevention and Control 2016-17

Directo
r of In
fection
Preven
tion
and
Co
ntro
l
2

Page
1. Executive Summary 4
2. Infection prevention and control arrangements 5
3. Healthcare Associated Infection Performance 6
3.1. Mandatory reporting 6
3.2. MSSA bacteraemia 6
3.3. MRSA bacteraemia 6
3.4. Clostridium difficile infection (CDI) 7
3.5. Hand hygiene 8
3.6. E coli bacteraemia 9
3.7. Outbreaks 9
4. Policies 11
5. Audit Programme 12
6. Antimicrobial Stewardship 13
7. Decontamination of the Environment and Equipment 15
8. Other significant issues 16
9. Conclusion 17
Appendix 1 Annual Programme 2017-18 18
Appendix 2 Annual Audit Report 24
Contents
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
3

1 Executive Summary
1.1 2016-17 was another challenging year in terms of healthcare associated infection. We were disappointed to not achieve our Clostridium difficile target for the second year, although this was always going to be difficult to achieve with an objective of no more than 13 cases. Our staff across all teams have worked hard to achieve reductions since 2007 when we reported 210 cases. E coli bacteraemia cases also saw an increase, although this was both in the cases attributed to the Trust and those that were non-Trust attributed. This reflects an increase in these infections seen across England which has prompted an initiative from the Secretary of State to reduce this type of infection by 50% by 2020-21. This year our performance for MSSA bacteraemia has improved which is encouraging, but there are still further improvements to be made. We have maintained the good performance for MRSA bacteraemia with significant reductions being seen since 2006.
1.2 The Trust has continued to implement measures to reduce the risk of infection, but has seen the impact of another very busy year in terms of hospital admissions and the number of very sick patients being admitted, along with vacancies for nurses and doctors, all of which research has shown to increase the risk of infection.
1.3 Infection Prevention and Control remains at the heart of good management and clinical practice in the Trust and the Board of Directors and staff in all areas have remained committed to maintaining high standards of care despite the challenges faced, particularly during the winter months.
1.4 For 2017-18 we will renew our focus on high quality care for our patients and will strive to achieve reductions in all infections, working with colleagues in other organisations to achieve improvements across the patient pathway.
Julie Lane Executive Director of Nursing, Quality and Patient Safety/ Director of Infection Prevention and Control
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
4

2 Infection Prevention and Control (IPC) Arrangements
2.1 The prevention and control of infections remains a high priority for the Trust and is discussed at each Board and Council of Governors meeting. Healthcare Associated Infection (HCAI) is a significant patient safety risk and impacts on our patient’s experience and outcomes. The Health and Social Care Act 2008, Code of Practice on prevention and control of infection and related guidance (2015) guides the activities carried out by the IPC team and is the basis of the annual work programme, which can be found at Appendix 1.
2.2 The constitution of the team includes:
• Director of Infection Prevention and Control
• Infection Control Doctor/ Consultant medical Microbiologist
• Assistant Director of Nursing and IPC
• Infection Prevention and Control Nursing staff
• Data and surveillance officer
• Secretarial and clerical staff
• The team works closely with:
• The Microbiology Laboratory Team
• Antimicrobial Pharmacist
• Decontamination Lead and team
The reporting arrangements for the IPC team are as below:
Fig 1 – IPC reporting arrangements
Trust Board
IPCT
Council of Governors
Patient Safety & Quality Standards Committee
Infection Control Committee
C difficile Improvement Group
HCAI Operational Group
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
5

3 HCAI Performance
3.1 Mandatory reporting
The Trust is required to report all cases of Methicillin resistant Staphylococcus aureus (MRSA) bacteraemia (blood stream infection), Methicillin sensitive Staphylococcus aureus (MSSA) bacteraemia, Escherichia coli (E coli) bacteraemia and Clostridium difficile infection (CDI) into a national data capture system administered by Public Health England on behalf of the Department of Health. National criteria are applied to establish whether cases of these infections are attributed to the reporting Trust or to another organisation. For bacteraemia cases when the sample is taken on the day of admission or the following day it is classed as non-Trust attributed and anything after that day is Trust attributed. For CDI if the sample is taken on the day of admission or the following two days it is non-Trust attributed but samples taken on subsequent days are classed as Trust attributed. National reduction trajectories are set for CDI and a zero tolerance approach is adopted for MRSA bacteraemia. There are no national trajectories set for MSSA and E coli bacteraemia but the Trust sets an internal target for each infection based on the performance in the previous year.
3.2 MSSA bacteraemia
3.2.1 Staphylococcus aureus is a bacterium commonly found on human skin, which can cause infection if there is an opportunity for the bacteria to enter the body. In serious cases it can cause blood stream infection. MSSA is a strain of these bacteria that can be effectively treated with many antibiotics.
3.2.2 In 2016-17 the Trust reported 21 Trust-attributed cases of MSSA bacteraemia (Fig 2). This is an improvement on the previous year when 24 cases were reported. The number of non-Trust attributed cases also reduced to 57 from 64 in the previous year. Root cause analysis is carried out on each Trust attributed case and action plans are formulated where learning is identified. No themes in terms of common sources of infection or practice related issues were identified from these investigations in 2016-17 and it was felt that 35% of cases were probably unavoidable.
Fig 2 MSSA bacteraemia cases 2008-17
3.3 MRSA bacteraemia
3.3.1 MRSA is a strain of Staphylococcus aureus, which is resistant to a large number of antibiotics and can cause infections such as wound infection, pneumonia and bacteraemia.
Apr
-08
Apr
-11
Apr
-14
Apr
-16
Jan-
11
Jan-
14
Oct
-10
Oct
-13
Jul-1
0
Jul-1
3
Oct
-08
Oct
-11
Oct
-14
Oct
-16
Jan-
17
Apr
-09
Apr
-12
Apr
-15
Oct
-09
Oct
-12
Oct
-15
Jul-0
8
Jul-1
1
Jul-1
4
Jul-1
6
Jan-
09
Jan-
12
Jan-
15
Jul-0
9
Jul-1
2
Jul-1
5
Jan-
10
Jan-
13
Jan-
16
Apr
-10
Apr
-13
0
1
2
3
4
No
of c
ases
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
6

3.3.2 The Trust reported one Trust-attributed case of MRSA bacteraemia in 2016-17 (Fig 3). This is an improvement on the previous year when 2 cases were reported. The post infection review of this case was carried out and as the patient had been previously known to be carrying MRSA and because the source of infection was the patient’s chest, which is very difficult to treat using decolonisation, the case was felt to have been not preventable.
3.3.4 The investigation was shared and agreed with commissioners at the quarterly Clinical Quality Review Group.
3.3.5 Two non-Trust cases were also reported. We assisted the commissioners with the investigation into these cases but no learning points for the Trust were identified.
Fig 3 Quarterly Trust MRSA bacteraemia cases 2006-17
3.4 E coli bacteraemia
3.4.1 Escherichia coli is a very common bacterium found in the human gut, which can cause serious infections such as blood poisoning.
3.4.2 A total of 50 cases of Trust-attributed cases of E coli bacteraemia were reported during 2016-17 (Fig 4). This is an increase on the 44 cases reported in 2014-15 and is likely to be a reflection of the increased activity, bed occupancy and acuity of patients along with an increased focus on early sampling in line with sepsis protocols. An increase in non-Trust cases was also seen with 267 cases compared to 224 in the previous year. Root cause analysis on Trust cases shows that the most common source of infection was the urinary tract (56%), and 57% of those cases had a urinary catheter in place however lapses in care were identified in only a small number of those patients. Other common sources of infection are hepatobiliary system, gastrointestinal system and chest infections. It is felt, following a review of cases that the majority of cases are considered to be unavoidable.
Apr
-Jun
08
Apr
-Jun
11
Jan-
Mar
08
Jan-
Mar
11
Jan-
Mar
14
Jan-
Mar
15
Jan-
Mar
16
Jan-
Mar
17
Apr
-Jun
16
Jul-S
ep 1
6O
ct-D
ec 1
6
Oct
-Dec
07
Oct
-Dec
10
Oct
-Dec
13
Oct
-Dec
14
Oct
-Dec
15
Jul-S
ep 0
7
Jul-S
ep 1
0
Jul-S
ep 1
3
Jul-S
ep 1
4
Jul-S
ep 1
5
Oct
-Dec
08
Oct
-Dec
11
Apr
-Jun
06
Apr
-Jun
09
Apr
-Jun
12
Oct
-Dec
06
Oct
-Dec
09
Oct
-Dec
12
Jul-S
ep 0
8
Jul-S
ep 1
1
Jan-
Mar
06
Jan-
Mar
09
Jan-
Mar
12
Jul-S
ep 0
6
Jul-S
ep 0
9
Jul-S
ep 1
2
Jan-
Mar
07
Jan-
Mar
10
Jan-
Mar
13
Apr
-Jun
07
Apr
-Jun
10
Apr
-Jun
13
Apr
-Jun
14
Apr
-Jun
15
0
1
2
3
4
5
6
7
8
No
of c
ases
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
7

Fig 4 E coli bacteraemia cases 2011 -17
3.5 CDI
3.5.1 Clostridium difficile is a bacterium that is found in the gut of around 3% of healthy adults. It seldom causes a problem as it is kept under control by the normal bacteria of the intestine. However certain antibiotics can disturb the bacteria of the gut and Clostridium difficile can then multiply and produce toxins which cause symptoms such as diarrhoea.
3.5.2 It is disappointing that following two years of excellent performance in reducing CDI the Trust has breached the trajectory of 13 cases for the second consecutive year, reporting 39 Trust-attributed cases in 2016-17 (Fig 5) which was also a deterioration from the previous year when 36 cases were reported. Consultant led root cause analysis is carried out within three days of notification for each case. These RCAs revealed that in the majority of cases although whole Trust level hand hygiene compliance and patient equipment cleaning scores have improved the individual ward scores were still below the Trust internal targets.
Fig 5 Trust attributed CDI 2007-17
Oct
-12
Oct
-14
Aug
-12
Aug
-14
Jun-
12
Jun-
14
Apr
-12
Apr
-14
Feb-
13
Feb-
15
Jun-
11
Jun-
13
Oct
-11
Oct
-13
Dec
-12
Dec
-14
Apr
-11
Apr
-13
Aug
-11
Aug
-13
Dec
-11
Dec
-13
Feb-
12
Feb-
14
Jun-
15
Oct
-15
Apr
-15
Aug
-15
Dec
-15
Feb-
16
Jun-
16
Oct
-16
Apr
-16
Aug
-16
Dec
-16
Feb-
16
0
5
Trust Attributed
Non-Trust Attributed
10
15
20
25
30A
pr-0
7
Jul-1
0
Jul-1
3
Apr
-10
Apr
-13
Jan-
10
Jan-
13
Jan-
16
Jan-
17
Oct
-09
Oct
-12
Oct
-15
Oct
-16
Oct
-07
Jan-
11
Jan-
14
Jul-0
8
Jul-1
1
Jul-1
4
Jan-
09
Jan-
12
Jan-
15
Jul-0
7
Oct
-10
Oct
-13
Jan-
08
Apr
-11
Apr
-14
Oct
-08
Oct
-11
Oct
-14
Apr
-09
Apr
-12
Apr
-15
Apr
-16
Jul-0
9
Jul-1
2
Jul-1
5
Jul-1
6
0
5
10
15
20
30
25
35
No
of c
ases
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
8

3.5.3 All Trust cases are subject to ribotyping (genetic typing) carried out by a regional microbiology laboratory. This testing helps to identify whether cases are linked and if so are likely to be a result of cross infection. The genetic testing suggests that cross infection has occurred on two occasions during the year. Other cases have been sporadic and unconnected. One ward had 12 positive patients during the 12 month period but none of these were found to match and work is underway to establish whether there is another source that has not been identified thus far.
3.5.4 The Trust recognised again at the beginning of the reporting year that it was unlikely to achieve the very challenging trajectory and established a group to develop an improvement plan for the year. However, despite all actions taken, the number of cases did not reduce.
3.5.5 The Trust participated in a national infection prevention and control collaborative programme facilitated by NHS Improvement. Clostridium difficile was the focus of our improvement project and involved measuring the impact of a new role to improve cleaning of patient equipment at ward level, utilising a member of staff with protected time and appropriate training. The outcome of the project was that the cleanliness scores on the pilot wards improved. A proposal for further roll out of the initiative will be developed as part of the actions to reduce C difficile in the Trust.
3.6 Hand hygiene
3.6.1 Monthly audits of hand hygiene practice are carried out in the Trust. This is a combination of independent observation, self-assessment and patient/carer feedback. The results are entered into a Safety, Quality and Infections dashboard where compliance by staff group and ward can be displayed. Table 1 shows overall Trust hand hygiene scores for the year but scores for individual wards form a RAG report which is used to provide feedback to clinical areas monthly, and is discussed at the HCAI Operational Group bimonthly and Infection Control Committee quarterly. In 2016-17 the Trust reached or exceeded the internal target of 95% compliance in 11 out of 12 months which is a significant improvement on previous years
Table 1 Hand hygiene % compliance 2015-16
Apr 16
May 16
Jun 16
Jul 16
Aug 16
Sept 16
Oct 16
Nov 16
Dec 16
Jan 17
Feb 17
Mar 17
95 96 97 97 96 96 97 98 97 98 95 97
3.6.2 A Hand Hygiene Champions network is in place with over 100 volunteers from all types of staff including the Chief Executive, staff nurses, healthcare assistants, domestics and corporate managers. These champions have a role in promoting good hand hygiene practice and challenging poor practice if they observe it. A programme of events for hand hygiene champions has been implemented, and a monthly ‘Champions Challenge’ has been utilised to raise awareness of different aspects of hand hygiene practice throughout the year,
3.7 Outbreaks
3.7.1 Each year there are a number of outbreaks which affect patients and staff both in hospital and in the community. There were 12 outbreaks of diarrhoea and/or vomiting in the Trust in 2016-17. These outbreaks affected 12 wards with 132 patients and 13 staff reporting symptoms. This represents a marked reduction in the number of both staff and patients affected compared to the previous year and the number of outbreaks overall, although some of the outbreaks were prolonged. The outbreaks lasted between 6 and 9 days, with one outbreak lasting 28 days in total, and in each case all or part of the ward was closed to prevent further spread of infection. Outbreaks can have an adverse impact on the business of the Trust because if a ward is closed it reduces the number of beds available to admit new patients into.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
9

3.7.2 Norovirus (winter vomiting bug) was identified as the causative agent in 4 of these outbreaks, and assumed to be the cause in the outbreaks where there were no positive samples, based on clinical symptoms. Adenovirus and Rotavirus were also identified as causative agents in 2 outbreaks, which has not been the case in previous years
3.7.3 Increased cleaning is implemented during an outbreak and the ward is deep cleaned before opening once an outbreak is declared closed. The pattern of outbreaks reflects those we are aware of in community settings such as care homes and schools.
Staff taking part in hand hygiene audits carried out by the infection prevention and control staff.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
10

4 Policies
4.1 The Trust has a programme for review and revision of core infection prevention and control policies as required by the Health and Social Care Act 2008 Code of Practice (2015). All policies are available to staff on the Trust Intranet site and many are available to members of the public on the external website. Compliance with policy is audited as part of the annual programme and an audit report published as described in section 5.
Policy Code Policy Title Status
IC1 Outbreak Policy For review December 2019
IC2 Hand Hygiene Policy For review April 2019
IC3 Infection Control Policy For review April 2019
IC5 CJD Policy For review October 2018
IC6 MRSA Policy For review March 2019
IC7 Management of Viral Haemorrhagic Fevers incl Ebola Policy
For review November 2017
IC11 Tuberculosis Policy For review June 2018
IC12 Local Decontamination of Medical Equipment Policy
For review June 2019
IC14 Clinical Specimen Policy Under review at time of reporting
IC15 Patient Isolation Policy For review December 2019
IC17 Standard Precautions Policy For review April 2018
IC18 Peripheral Cannulation Policy Under review at time of reporting
IC19 Clostridium difficile Policy For review May 2018
IC20 MRSA screening Policy For review March 2018
IC21 Theatre Policy For review September 2019
IC22 Management of Patients with Ectoparasitic Infestation Policy
For review December 2019
IC23 Infection Prevention and Control Surveillance Policy
For review April 2020
IC24 Management and Control of CPE Policy
For review August 2017
C56 Antibiotic Strategy For review April 2018
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
11

5 Audit Programme
5.1 An annual programme of audit is agreed as part of the annual IPC work programme. This audit programme is a combination of policy audits and general IPC audits carried out as part of an unannounced visit schedule. Each audit is collated and fed back to clinical departments and action planning requested as appropriate. The audits are presented to the Infection Control Committee and an annual report is produced summarising all of the audit activity and high-level findings. This report for 2016-17 can be found at Appendix 2.
5.2 In summary 2016-17 saw a slight reduction in compliance with MRSA policy and isolation policy, an improvement in compliance with the Clostridium difficile policy and peripheral cannulation policy, and maintenance of compliance with the basic practice audits.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
12

6 Antibiotic Stewardship
6.1 The core antibiotic audit programme is now being completed 4 monthly in all areas in line with audits carried out by junior doctors during their rotations. The prophylaxis and IV audits which form part of the programme are completed 6 monthly.
6.2 An antibiotic audit dashboard has been developed and is available to all Trust staff via the intranet site. This allows accurate and simple trend reporting to the Infection Control Committee via a RAG rating system which makes comparison of results more straightforward.
6.3 Audit results are reported to Audit and Clinical Effectiveness Committee twice yearly and discussed more frequently at the Antibiotic Group which is attended by clinical staff.
6.4 The role of the Antibiotic Champions has been reinvigorated and new champions have been nominated in some areas. The champions are responsible for overseeing antibiotic use in their directorates and for ensuring that audit results are shared and appropriate action plans are developed.
6.5 Defined daily dose (DDD) information is used to provide information to the Infection Control Committee (Fig 6). This information should be read with caution, as it does not consider bed occupancy.
Fig 6 Total antibiotic DDS per quarter
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
13

6.6 A CQUIN scheme around reduction of antibiotic consumption was introduced in 2016-17 and the Trust was successful in reducing use of carbapenems and pieracillin-tazobactam, but unfortunately saw a slight increase in overall antibiotic consumption, probably due to the acuity of patients being admitted who have required antibiotic treatments and the successful implementation of the sepsis bundle. The antimicrobial pharmacist has attended directorate meetings to raise awareness of this initiative and how individual specialities can assist with the reduction of antimicrobial prescribing.
6.7 Antibiotic ward rounds take place on the orthopaedic and critical care wards. This is an on-going development further wards will be added during the forthcoming year.
6.8 The Trust again participated in European Antibiotic Awareness Day, with the emphasis this year being on IV to oral switch. The Trust guidelines for this were updated prior to the event, as well as a new poster to get the message across in a clear and concise way.
6.9 Formal education sessions for medical staff continue and development of an eLearning package has been explored in line with the requirements of Start Smart Then Focus.
Audit North (now Audit One), completed a review of Antibiotic Stewardship in 2016 which made a number of recommendations. The actions identified are being led by a Deputy Medical Director and progress is reported to the Audit Committee.
European Antibiotic Awareness Day 2016
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
14

7 Decontamination of the environment and equipment
7.1 Decontamination is a process which removes or destroys infectious agents from furniture or medical equipment. Cleaning is always the first step in this process, which is usually then followed by disinfection or sterilisation depending on the circumstances in which the equipment is used. The Trust provides an in house sterile services department, reprocessing reusable medical devices. This is a fully validated and monitored process. Decontamination audits are carried out annually in departments when local decontamination is carried out and the IPC team are part of the audit team. Disposable items are used wherever possible and efficient.
7.2 The endoscope decontamination facilities on the endoscopy units on both sites are fully compliant with national requirements. An Authorising Engineer (Decontamination) has validated the annual reports as suitable for service. In addition the endoscope washer-disinfectors within the central sterile services department provide contingency support to the endoscopy unit facilities.
7.3 The provision of cleaning services in wards and departments is provided by a combination of in house staff and external contractors (some community premises). Performance management systems are in place with monitoring staff making checks of the environment and equipment in line with national standards.
7.4 In addition to routine cleaning the Trust has invested in enhanced cleaning services with a response team and a hygienist team responsible for touch point cleaning ( items frequently touched by staff and patients), deep cleaning, fogging with hydrogen peroxide, use of Ultra Violet light and a mattress decontamination facility.
7.5 During 2016-17 a decant ward to facilitate deep cleaning and fogging of a full ward was made available and a full programme of deep cleaning and fogging was achieved by November 2016. Reactive cleaning continues throughout the year in response to individual cases of infection or wards affected by outbreaks.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
15

8 Other significant issues
8.1 An increase in patients with samples positive for Pseudomonas aeruginosa was noted in Critical Care between September and November 2016. Control measures were implemented in line with national guidance, including decontamination of sinks and taps, additional hand hygiene measures and the use of sterile water for patient hygiene, and a number of incident meetings were held. Genetic typing revealed that the cases were not linked. Improved point of care practices have been implemented and will be continued, and a programme of screening and replacing taps has been agreed. Two recent cases are undergoing genetic typing but may be simply the sporadic cases that occur normally. The situation will be monitored and discussed at the regular Water Safety Meetings.
8.2 The same organism was isolated from water samples from the Birthing pool at University Hospital of Hartlepool. No patient infections have been identified that are linked with this environmental testing. The birthing pool was removed from use while investigations and enhanced decontamination took place. Following decontamination and tap replacement the testing was negative and the birthing pool was put back into use.
Staff in main outpatients at the University Hospital of North Tees doing health promotion on hygiene
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
16
9 Conclusion
9.1 2016-17 proved to be another challenging year in terms of levels of activity and acuity of patients. Although the Trust did not achieve the required reductions in Clostridium difficile infections we continuously strive to improve practice and keep our patients as safe as possible and protect them from preventable infections. We will continue to work with colleagues in national and local organisations to take a whole system approach to infection prevention.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
17
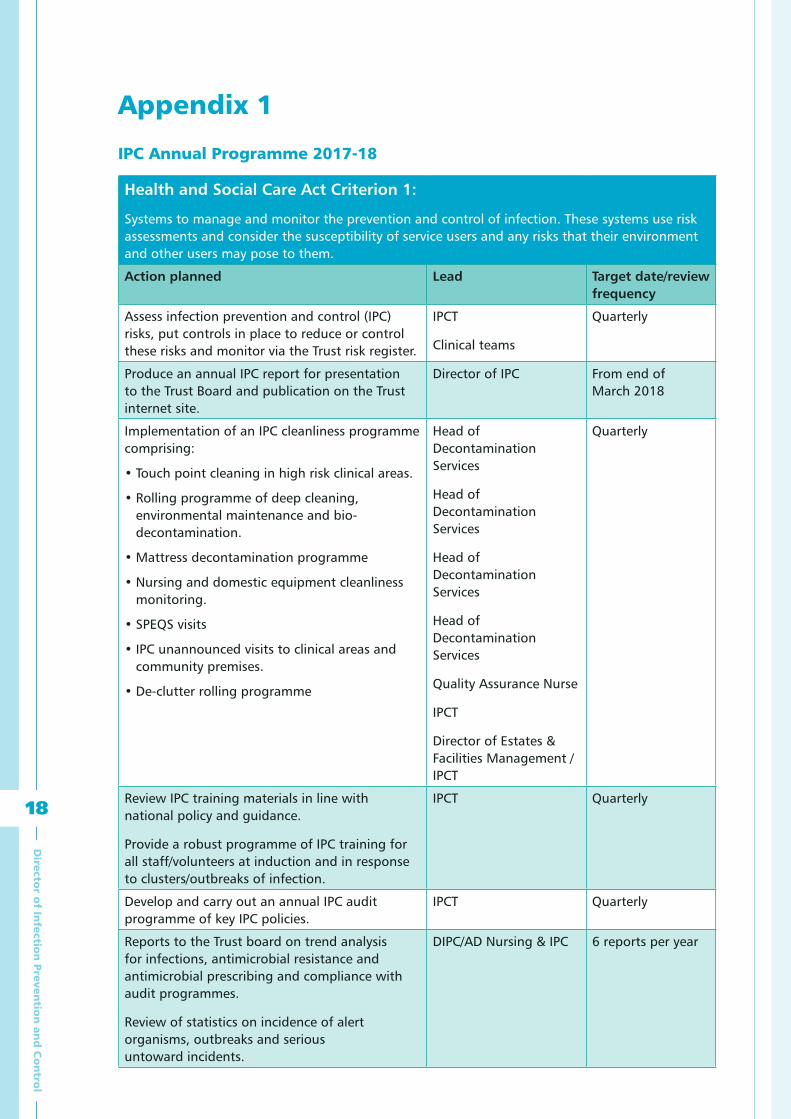
Appendix 1
IPC Annual Programme 2017-18
Health and Social Care Act Criterion 1:
Systems to manage and monitor the prevention and control of infection. These systems use risk assessments and consider the susceptibility of service users and any risks that their environment and other users may pose to them.
Action planned Lead Target date/review frequency
Assess infection prevention and control (IPC) risks, put controls in place to reduce or control these risks and monitor via the Trust risk register.
IPCT
Clinical teams
Quarterly
Produce an annual IPC report for presentation to the Trust Board and publication on the Trust internet site.
Director of IPC From end of March 2018
Implementation of an IPC cleanliness programme comprising:
• Touch point cleaning in high risk clinical areas.
• Rolling programme of deep cleaning, environmental maintenance and bio-decontamination.
• Mattress decontamination programme
• Nursing and domestic equipment cleanliness monitoring.
• SPEQS visits
• IPC unannounced visits to clinical areas and community premises.
• De-clutter rolling programme
Head of Decontamination Services
Head of Decontamination Services
Head of Decontamination Services
Head of Decontamination Services
Quality Assurance Nurse
IPCT
Director of Estates & Facilities Management /IPCT
Quarterly
Review IPC training materials in line with national policy and guidance.
Provide a robust programme of IPC training for all staff/volunteers at induction and in response to clusters/outbreaks of infection.
IPCT Quarterly
Develop and carry out an annual IPC audit programme of key IPC policies.
IPCT Quarterly
Reports to the Trust board on trend analysis for infections, antimicrobial resistance and antimicrobial prescribing and compliance with audit programmes.
Review of statistics on incidence of alert organisms, outbreaks and serious untoward incidents.
DIPC/AD Nursing & IPC 6 reports per year
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
18

Joint working with other health care workers and health care providers/organisations so that suitable and sufficient information on a service user’s infection status is provided upon admission, when patients move between departments and organisations and upon discharge.
IPCT/Care Home IPC Nurse/
SCMs/
Clinical teams
Quarterly
Develop a reporting tool for Essential Steps audits.
Quality Analyst Quarterly
Health and Social Care Act Criterion 2:
Provide and maintain a clean and appropriate environment in managed premises that facilitates the prevention and control of infections.
Action planned Lead Target date/review frequency
Monitor cleanliness standards and ensure that the environment is maintained in good physical repair and condition.
SCMs/Ward Matrons/Domestic Managers/Monitoring Officers/
Head of Decontamination Services
Quarterly
Hold/attend monthly cleaning standards group meetings and monitor cleaning scores.
Head of Decontamination Services/ IPCT/Monitoring Officers
Domestic Managers
SCMs
Quarterly
Hold/attend and contribute to decontamination group meetings ensuring that decontamination policies are in place and monitored.
Carry out/assist with decontamination audits.
SSD Lead IPCT/SCMs
SSD lead IPCT
Quarterly
Quarterly
Hold/attend and contribute to capital meetings.
Contribute to all Estates Department new build and refurbishment projects in terms of giving IPC advice.
Director of Estates & Facilities Management/ IPCT
IPCT
Quarterly
Quarterly
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
19

Have systems in place for the safe management of:
• Hand hygiene
• Water and air hygiene
• Pest control
• Drinkable and non drinkable water supplies
• Minimising the risk of Legionella
• Minimising the risk of pseudomonas
• Building and refurbishment
• Planned preventative maintenance
• Cleaning services
• Food service, including food hygiene
• Laundry arrangements
• Waste management
• Decontamination
IPCT
Director of Estates & Facilities Management
Head of Catering Services
Head of Portering Services
Head of Decontamination Services
Quarterly
Approve prepurchase procurement questionnaires for new equipment.
IPCT Quarterly
Health and Social Care Act Criterion 3:
Ensure appropriate antimicrobial use to optimise patient outcomes and to reduce the risk of adverse events and antimicrobial resistance.
Action planned Lead Target date/review frequency
Monitor adherence to the principles of Start Smart then Focus in all clinical areas.
Antibiotic Lead/ Antimicrobial Pharmacist
Annually
Manage the existing antibiotic stewardship programme.
Report antimicrobial stewardship activities to the Trust board via ICC
Antibiotic Lead/ Antimicrobial Pharmacist/ Medical Director
Quarterly
Review antibiotic audit programme to include the principles of Start Smart Then Focus.
Continue with antibiotic audit programme, providing feedback to CDs, SCMs, Antibiotic Champions and patient safety leads requesting action plans from them as appropriate.
Antibiotic Lead/ Antimicrobial Pharmacist
Annually
Review antibiotic consumption trends and explore the ability to report local antimicrobial susceptibility data.
Antibiotic Lead/ Antimicrobial Pharmacist/ Infection Control Doctor
Quarterly
Provide mandatory core training in prudent antibiotic use to all prescribers.
Antibiotic Lead/ Antimicrobial Pharmacist/ Infection Control Doctor/ Educators
Annually
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
20

Health and Social Care Act Criterion 4:
Provide suitable, accurate information on infections to service users, their visitors and any person concerned with providing further support or nursing/medical care in a timely fashion
Action planned Lead Target date/review frequency
Provide accurate and up to date IPC patient and staff information leaflets and awareness posters.
IPCT Quarterly
Provide accurate and up to date information for patients, the public and staff on the Trust website.
IPCT Quarterly
Work collaboratively with Healthcare User Group, Healthwatch and PALs as required.
IPCT Quarterly
Where possible, locally resolve informal complaints about IPC related incidents and investigate IPC related complaints.
IPCT
SCMs
Quarterly
Comply with national mandatory and voluntary surveillance programmes by reporting CDI/iGAS/E-coli, GRE, MRSA, MSSA bacteraemia & Norovirus outbreaks.
AD Nursing & IPC Quarterly
Participate in awareness initiatives including:
• European antibiotic awareness day
• WHO hand hygiene day
• World Sepsis day
• World Antibiotic week
• International Infection Control Week
IPCT
Antimicrobial Pharmacist
Quarterly
Health and Social Care Act Criterion 5:
Ensure prompt identification of people who have or are at risk of developing an infection so that they receive timely and appropriate treatment to reduce the risk of transmitting infection to other people.
Action planned Lead Target date/review frequency
Work collaboratively with Public Health England North East in order to manage outbreaks and occurrences of serious infection.
IPCT Quarterly
Undertake daily alert and targeted surveillance and act on results accordingly.
IPCT Quarterly
Feed back infection rate statistics via the Safety, Quality and Infections Dashboard and to Directorates via performance statistics.
IPCT Quarterly
Work collaboratively with Critical Care and NNU staff to assist with the implementation of the principles and best practice from the Matching Michigan project to reduce line related bloodstream infections.
IPCT/ Infection Control Doctor
Quarterly
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
21

Health and Social Care Act Criterion 6:
Systems to ensure that all care workers (including contractors and volunteers) are aware of and discharge
Their responsibilities in the process of preventing and controlling infection.
Action planned Lead Target date/review frequency
Include IPC and cleanliness in:
• Induction programmes for all staff, including volunteers
• Job descriptions of all staff
• Annual performance reviews of all relevant staff
IPCT All Managers All Matrons
Quarterly
Provide staff with training and assessment in IPC procedures prior to them being carried out independently.
IPCT/Ward Matrons/Clinical Educators
Quarterly
Co-ordinate the IPC link worker network and the hand hygiene Champions initiative.
Facilitate an annual link worker study day.
IPCNs Quarterly
Lead the post infection review for Trust attributed MRSA bacteraemias and participate in PIR of community acquired MRSA bacteraemias.
Initiate/participate in RCA for Trust attributed Toxin positive Clostridium difficile cases/ MSSA bacteraemia cases/E coli bacteraemias/Clostridium difficile related death.
AD Nursing & IPC IPCT IPCT Clinical teams
Quarterly
Directorate representatives to attend ICC and present an IPC report giving details of risks, actions taken and progress in reducing infections within their directorate.
General Manager, SCM, Clinical Director for each clinical directorate
Mar 2017
Provide information on infection prevention and control risks and responsibilities to contractors by written information or face to face session
IPCT Mar 2017
Health and Social Care Act Criterion 7:
Provide or secure adequate isolation facilities.
Action planned Lead Target date/review frequency
Work collaboratively with the Estates Dept to increase, where possible, the availability of isolation facilities.
Director of Estates & Facilities Management/ IPCT
Quarterly
Undertake risk assessment of patients with infection to ensure optimal use of isolation facilities.
IPCT
All Matrons
SCMs
Quarterly
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
22

Health and Social Care Act Criterion 8:
Secure adequate access to laboratory support as appropriate.
Action planned Lead Target date/review frequency
Work collaboratively with the Microbiology Laboratory staff in order to identify any shortfall in resources and escalate appropriately.
Infection Control Doctor Quarterly
Health and Social Care Act Criterion 9:
Have, and adhere to, policies designed for the individual’s care and provider organisations that will help to prevent and control infections.
Action planned Lead Target date/review frequency
Review all core IPC clinical policies by their review date. Policies to be available to all staff and the public.
Infection Control Doctor/ AD Nursing & IPC
Quarterly
Produce robust action plans in response to audit findings within the given timescale and review action plans to ensure that actions have been completed.
SCMs/ Heads of departments
Quarterly
Standardise aseptic technique and carry out an audit to monitor compliance.
AMs/IPCNs/Clinical Educators/Ward Matrons
March 17
Health and Social Care Act Criterion 10:
Providers have a system in place to manage the occupational health needs of staff in relation to infection.
Action planned Lead Target date/review frequency
Work collaboratively with the Occupational Health & Wellbeing Department in order to provide optimal advice on infection prevention and control related matters.
IPCT Quarterly
Monitor staff compliance with the Accidental exposure to bodily fluids policy and address instances of non compliance.
SCMs OH&WD H&S
Quarterly
Risk manage mucous membrane exposure and sharps injuries and incidents.
OH&WD Quarterly
Manage cases of occupationally acquired Dermatitis by providing treatment and advice.
OH&WD Quarterly
Provide guidance on glove use via the latex policy.
OH&WD Quarterly
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
23

Appendix 2
Infection Prevention and Control Department Annual Audit Programme Report - April 2016 to March 2017
Introduction
There are a number of Trust policies relating to infection prevention and control. Assurance continues to be required by the Care Quality Commission, as part of monitoring of the Health Act 2008, the National Health Service Litigation Authority, as part of the Risk Management Standards and NHS Improvement that these policies are being implemented and complied with. Audit is a means of measuring implementation and compliance. The Director of Infection Prevention and Control and the Healthcare Associated Infection (HCAI) Operational Group play a key role in the setting and monitoring of standards and challenging directorates to reach targets.
This report gives an overview of audit activity during 2016-17. All audits were carried out by the Infection Prevention and Control Team (IPCT). The audits include:
• Three core basic practice audits: hand hygiene, standard precautions and environmental cleanliness.
• Peripheral cannulation policy
• Clostridium difficile stool sampling
• MRSA screening audit
• MRSA emergency admission screening compliance
• Clostridium difficile policy
• Isolation policy
• MRSA policy
• Monthly hand hygiene observations
• Monthly urinary catheter record
• Monthly commode
• Outbreaks, including Acinetobacter outbreak
• Birthing pool
• Mortuary
Methodology
The programme of basic practice audits carried out by the IPCT as part of the annual unannounced visits programme has continued over 2016-17. The audit tools continue to be available on the Infection Prevention and Control Sharepoint site should Ward Matrons or link workers wish to use them.
The remaining policy audits carried out by the IPCT involve monitoring against standards set within each specific policy.
Percentage compliance is calculated based on the number of ‘yes’ answers for each audit. Results are fed back to clinical areas in a timely manner following each audit. Follow up of recommendations continues to be done through the HCAI Action Tracker database. Formal reporting and monitoring of progress is via the HCAI Operational Group and Infection Control Committee. Directorates must ensure that any required action is taken in a timely manner and dealt with promptly.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
24

ResultsUnannounced visits / Basic practice audits
Audit Overall Trust compliance 2016-17
Comparison to 2015-16
Hand hygiene 92% ê 93%
Standard Precautions(combined sharps safety & PPE) 90% é 88%
Environmental 81% ê 84%
Uniform 98% çè 98%
Overall compliance 90% çè 90%
All clinical areas are included in the unannounced visits programme. During 2016-2017 the IPCT completed all of the planned unannounced visits, there being 82 in total. As well as carrying out the three basic practice audits, the Assistant Matrons and Infection Prevention and Control Nurses continued to perform formal observations of practice, ad hoc training such as hand hygiene training and the following additional audits during unannounced visits:
• Uniform and personal appearance policy audit• Documentation checks (peripheral cannulation documentation)• Feedback from patients
Overall directorate compliance levels with the basic practice audits ranged from 63% to 100%, which is a reduction on the previous year’s audits. Total Trust compliance with the basic practice audits has remained at 90% compared to the previous year.
In summary:
• Hand hygiene: compliance with standards in the hand hygiene policy ranged from 56% to 100%. 53% of areas achieved 90% or above which is a slightly lower level of compliance compared to the 63% achieved in the previous year. Areas demonstrating sustained improvement included: good provision of recommended hand hygiene information, products and facilities. The main shortfall in compliance was once again, as highlighted in previous year’s reports, a need for improvement in the display of appropriate hand hygiene posters in some wards and also some empty hand cream dispensers. Missing posters were provided by the IPCT.
• Standard Precautions: scores ranged from 64% to 100%. 59% of areas achieved 90% or above, which is an improvement compared to 51% achieved in the previous year. Results demonstrate that there continues to be excellent availability of general personal protective equipment (gloves and aprons). Improvements in availability of FFP3 facemasks and face visors were recommended for a small number of wards/depts. A need for improvements in signage of arrest trolley sharps bins and post exposure prophylaxis was highlighted.
• Environment: scores ranged from 40% to 100%. 35% of areas scored 90% or above which is the same level of compliance achieved in the previous year. Areas demonstrating sustained improvements included: improvements in the general patient environment, such as communal facilities – toilets, bathrooms and general first impressions. However improvements were highlighted in several clinical areas regarding general damage to walls and flooring. Ward staff are encouraged to report issues for repair in a timely manner on Planet FM to enable estates staff to deal with such repairs. The deep clean programme has continued to be rolled out over the year and has allowed such repairs to take place. Some damaged patient equipment and furniture was highlighted in some areas, once again staff must report any damage for repair in a timely manner to ensure patient equipment is clean, intact and fit for purpose. Some Out of Hospital Care departments off site were noted have slightly poorer scores, generally due to cluttered storage areas and dusty equipment and furnishings, which has been addressed through action logs and the IPC action tracker system.
• Uniform: scores ranged from 67% to 100%. 91% of areas scored 90% or above which is a slight drop in compliance compared to the 96% achieved in the previous year. Although the majority of staff were compliant with the uniform and personal appearance policy, small numbers of staff in clinical areas were observed to be wearing stoned or additional rings, nail varnish or long sleeves. Compliance with the uniform and personal appearance policy is essential and this was discussed with non-compliant staff at the time of the audit and reported back to managers for continuous monitoring.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
25

Formal reporting was via the SCM, Ward Matron or Department Manager, with an action log for areas of improvement. Progress was monitored using the IPC action tracker database.
Isolation policy audit
This audit was carried out in April 2016 and a report circulated. Overall compliance with the total number of standards audited is as follows:
Overall compliance 2016-17 and comparison with previous year
Overall compliance 2015-16
92% ê (10 standards audited) 93% (10 standards audited)
In summary:
• 70 patients from all inpatient areas were included in the audit
• All patients who required isolation due to confirmed or suspected infection were included
• All patients with enteric infection (with the exception of 1 patient on a ward affected by a suspected Norovirus outbreak) were nursed in single rooms which demonstrates that risk assessments are being carried out effectively
• Full compliance noted with hand washing facilities
Recommendations included:
• Improved availability of correct colour coded aprons, disposable tourniquets and clinical waste bags must be available and in use at the point of care
• Isolation rooms must be kept free of excess equipment and clutter to facilitate adequate cleaning
A directorate action log was produced in response to the audit findings. Progress was monitored using the IPC action tracker.
Peripheral Cannulation Policy Audit
This audit was carried out in May. Full results are demonstrated in Appendix 3 with comparison to 2015-16 results. Overall compliance with the total number of standards audited is as follows:
Overall compliance 2016-17 and comparison with previous year
Overall compliance 2015-16
79% é (8 standards audited) 78% (8 standards audited)
In summary:
• 82 cannulae assessed
• Improvements were noted in five standards and three standards showed reduced compliance
• 93% of patients had a cannula record in their notes
• Slight reduction in overall completion of cannula record noted
Recommendations included:
• Attention needs to be paid to accurate completion of the Peripheral Intravenous Cannula Record regarding the position of the cannula or who had inserted it and documentation of inspection entries each shift
• Cannulation packs and needle-free connectors must be readily available in all wards/departments where cannulae are inserted and used for every cannula insertion
Directorate action plans were received in response to this audit. Progress was monitored using the IPC action tracker.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
26

MRSA Emergency Admission Screening compliance Audit
This audit was completed during June 2016. A random selection of 100 patients who were admitted as emergency admissions were included. Full results are demonstrated in Appendix 4. Overall compliance with the screening standard audited is as follows:
Overall compliance 2016-17
78%
Results were presented to the Infection Control Committee and progress was monitored using the IPC action tracker.
Clostridium difficile policy audit
This audit was carried out over a three month period, during June to August. Full results are demonstrated in Appendix 5 with comparison to 2015-16 results. Overall compliance with the total number of standards audited compared with the previous year is as follows:
Overall compliance 2016-17 (June-Aug 2016) and comparison with previous year
Overall compliance 2015-16 (July-Sept 2015)
93% é (17 standards audited) 91% (17 standards audited)
In summary:
• 41 patients included
• 12 standards showed either an improved level of compliance or 100% compliance
• One patient not isolated within the 2 hour agreed Trust timescale for isolation
• Compliance with door room closure showed a good improvement
Recommendations included:
Compliance with daily completion of the Clostridium difficile checklist remained at a consistent level but further improvement was highlighted in order to demonstrate that all of the necessary barrier precautions are in place and that all the required equipment is available for staff use
Improvement also highlighted around accurate and timely completion of Bristol stool charts in order to ensure infection prevention measures and treatment are appropriate
A directorate action log was produced in response to the audit findings. Progress was monitored using the IPC action tracker. Clostridium difficile awareness training has continued to be available for Trust staff on request, with intense training offered to wards with a period of increased incidence of cases.
Clostridium Difficile Stool Sampling Audit
This audit was carried out during September, to assess compliance with testing and health care workers knowledge of testing requirements, in line with requirements set out in the 2015-16 C difficile objectives. Full results are demonstrated in Appendix 6.
Overall compliance September 2016 Overall compliance November 2015
82% ê (4 standards audited) 85% (4 standards audited)
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
27

In summary:
• 16 inpatients from general wards met the criteria for inclusion
• Fewer patients had stool samples submitted promptly
• Awareness of the stool sampling flow chart and therefore compliance with guidance was reduced
Recommendations included:
• Improved staff awareness of sampling guidance and monitoring by Ward Matrons
• The IPCT have reviewed the current Bristol Stool chart to include information about when to send a stool specimen.
A directorate action log was produced in response to the audit findings. Progress was monitored using the IPC action tracker.
MRSA policy audit
This audit was performed during November and a report was circulated. Full results are demonstrated in Appendix 7 with comparison to 2015-16 results. Overall compliance with the total number of standards audited compared with the previous year is as follows:
Overall compliance 2016-17 and comparison with previous year
Overall compliance 2015-16
51% ê (11 standards audited) 63% (11 standards audited)
In summary:
• 30 patients included
• Seven standards showed increased compliance
• Full compliance noted in the correct prescription and prompt commencement of decolonisation and availability of hand rub dispensers. Noticeable improvement in door closure and admission screening.
Recommendations included:
• Recommended improvements included raised awareness of the completion of the elective MRSA screening/decolonisation record and evidence that perioperative antibiotic prophylaxis has been given. Improved awareness of completion of the MRSA care pathway and screening chart and appropriate completion of the MRSA risk assessment on admission were also highlighted.
A directorate action log was produced in response to the audit findings. Progress was monitored using the IPC action tracker. MRSA awareness training has continued to be available for staff on request.
MRSA Screening Policy Audit
This audit was carried out in January. A range of patients was selected to determine whether they had been screened for MRSA within 24 hours of emergency admission, or prior to their elective procedure. Full results are demonstrated in Appendix 8 with comparison to 2015-16 results. Overall compliance is as follows:
Overall compliance 2016-17 and comparison with previous year
Overall compliance 2015-16
80% é 77%
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
28

In summary:
• 40 patients included
• Patient groups included, orthopaedics/trauma, intensive care units, all patients previously identified as being colonised or infected by MRSA whether being admitted as an emergency or for elective care and all emergency admissions aged 60 or over.
Recommendations included:
• Admitting staff must be made aware of the guidance within the Trust MRSA screening policy relating to categories of patients who require screening for MRSA
• Ward / Dept Matrons to monitor their staff’s compliance with the policy
A directorate action log was produced in response to the audit findings. Progress was monitored using the IPC action tracker.
Monthly hand hygiene audits
The programme of unannounced monthly hand hygiene audits performed by the IPCT, using the Lewisham audit tool has continued over this last year. All inpatient wards have been included in the programme. This information continues to be available on the Safety, Quality and Infections Dashboard and is reported in the executive dashboard report each month. Self assessment of hand hygiene practice continues to be carried out by all other patient areas. Areas scoring below 95% are requested to perform weekly audits until the score is maintained at the Trust target of 95% or above. Repeat audits are carried out by the IPCT each month for clinical areas with the lowest scores. Formal reporting and monitoring of compliance is via the RAG report presented at the Infection Control Committee and HCAI Operational Group.
Outbreak audits
During 2016-17 the IPCT performed 12 audits of the management of gastro-intestinal outbreaks. Results and recommendations were cascaded to relevant Ward Matrons and SCMs at the time. Overall results show that stool samples were not submitted for every symptomatic patient during each of the audited outbreaks, although compliance has continued to improve. Audit results do however demonstrate that ward staff continue to report potential outbreak situations and instigate appropriate barrier precautions at an early stage. These prompt actions will have contributed to the containment of infection and prevention of spread to the wider community and are likely to have contributed to the decline in the overall numbers of outbreaks over this last year. Acute capacity management problems during one prolonged outbreak over winter months resulted in partial ward closure and it is likely that this pressure extended the outbreak situation.
As recommended in the investigation report for the outbreak of resistant Acinetobacter baumannii (2015), the final audit of respiratory practice was completed by the IPCT in July 2016. Overall compliance with the total number of standards audited is as follows:
Overall compliance July 2016 and comparison with previous audit
Overall compliance February 2016
Ward 25 50% ê
(8 standards audited)
Ward 25 67%
(8 standards audited)
Recommendations included:
• Hand wash sinks must be used for hand washing only and not for disposal of waste water or used for storage of patient toiletries
• Single use patient equipment must not be re-used
• Elephant tubing must be changed daily and a dated sticker applied to the tubing afterwards as evidence that this has been done
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
29

A directorate action log was produced in response to the audit findings and progress is being monitored using the IPC action tracker.
Birthing pool audits
These birthing pool-specific audits were carried out alongside the unannounced annual IPC visits in December 2016 (UHH) and February 2017 (UHNT) and reports were circulated. Overall compliance with the total number of standards audited compared with the previous year is as follows:
Compliance 2016-17 and comparison with previous year
Overall compliance 2015-16
Delivery Ward 100% ç è
Birthing Centre 100% é
Delivery Ward 100%
Birthing Centre 67%
(6 standards audited) (6 standards audited)
Both departments achieved full compliance with the audited standards this last year, which is excellent.
Mortuary Audits
Annual audits using ‘mortuary-specific’ audit tools were performed by the IPCT in conjunction with mortuary staff in January 2017. Both departments demonstrated an excellent full level of compliance with all audited standards, and comparison with the previous year is as follows:
Compliance 2016-17 and comparison with previous year
Overall compliance 2015-16
UHNT Mortuary 100% é
UHH Mortuary 100% ç è
UHNT Mortuary 97%
UHH Mortuary 100%
(32 standards audited) (32 standards audited)
Urinary catheter record audits
Monthly urinary catheter record audits continue to be carried out by the IPCT, in order to provide assurance that staff are documenting catheter insertions and on-going care appropriately. In order to provide a reasonable sample size, an audit continues to be carried out on each ward the IPCT visit when performing the monthly hand hygiene audits. Any deficits in documentation are addressed at the time of the audit with ward staff. Results are presented quarterly to the HCAI Operational Group and a summary is included in Appendix 9.
Commode audits
The programme of monthly commode audits has continued during 2016-17. An audit is carried out on each ward the IPCT visit when performing the monthly hand hygiene audits. Feedback is given to ward staff at the time of the audit and results reported monthly to the Senior Clinical Matrons and formally reported quarterly to the HCAI Operational Group. A summary of results is included in Appendix 10.
Decontamination audits
The IPCT have continued to be involved in the annual decontamination audits co-ordinated by the Decontamination/Sterilisation Manager. Audits have been carried out in areas such as Theatre, Day Case Unit, Outpatients, Endoscopy, Lung Health, Cardiac Investigations, Colorectal Unit, the One Life Centre, Peterlee Community Hospital and Community Dental premises.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
30

Service Level Agreements
A range of service level agreements are in place with some local GP practices, the Butterwick and Hartlepool Hospices, the Woodlands Hospital and Middlesbrough Council. Annual audit, led by the IPCT, of buildings and facilities is included for these establishments.
Recommendations • The three basic practice audit tools continue to be available on the IPC sharepoint site for link workers /
Ward Matrons to use as required, during episodes of increased incidence of infection or as part of good practice measures to ensure high standards of infection prevention and control practice within their clinical areas
• Progress with recommendations and action logs will continue to be monitored using the IPC action tracker, with overdue actions formally presented at the HCAI Operational Group and Infection Control Committee meetings
• Unannounced audits/observations of practice will continue to be carried out by the IPCT with all clinical areas visited at least once a year and more frequently if there is a concern about infection rates in the area or compliance with infection prevention and control policy
• The IPCT will continue to be available on request to support Ward Matrons to carry out additional audits within their own areas
• Ward Matrons must ensure results of unannounced visits and annual IPC audits, along with ward/department action logs to address shortfalls, are shared with ward staff at ward/department meetings and are readily available within their clinical area
Conclusion
As required by the Health Act, 2008, NHS organisations must be able to provide evidence of the actions they are taking to prevent and control infections and maintain patient safety. Audit remains a core requirement of the Code of Practice for the Prevention and Control of Healthcare Associated Infection and of the Risk Management Standards. Directorates continue to present their evidence of compliance and performance against the Trusts infection prevention and control annual programme to the Infection Control Committee; thereby demonstrating that infection prevention and control is part of everyday practice and that it is applied consistently by everyone. Actions highlighted from audit findings will continue to be formally monitored by the HCAI Action Tracker system and presented to the HCAI Operational Group and Infection Control Committee.
Overall reportable healthcare infection rates for the Trust have once again shown an increase over this last twelve month period. Good infection prevention is essential to ensure that people who use health care services receive safe and effective care. It is imperative that compliance with policy improves and action is taken promptly to address audit recommendations for improvement. Clinical areas must be maintained to a high standard by all staff in order to protect patients from avoidable infection and improve patient outcomes.
Staff have been welcoming and helpful during the IPCT audit visits. The IPCT would like to thank all Trust staff who have contributed to achieving improvements in patient care through their involvement in the audit process.
Directo
r of In
fection
Preven
tion
and
Co
ntro
l
31
www.nth.nhs.uk
Directo
r of In
fection
Preven
tion
and
Co
ntro
l





























