Embed Size (px)
Citation preview

Comparative Health Assessment Deficits and
FDA Regulatory Inefficiencies in Companion Diagnostics
by
Krishna Teja Yanamandra
A Paper Completed in Partial Fulfillmentof the Requirements for the Degree
Master of Science
Graduate Supervisor:Dr. Carl Yamashiro
Arizona State UniversityAugust 2015

INTRODUCTION
Personalized medicine as we know it
now is in its infancy relative to the hundreds
of years that traditional medical practices
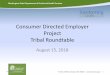
have been carried out. Figure 1 illustrates just
how new this approach is in the medical
realm. Treatment thus far has been
identification of a general disease or
condition followed by medicating the
patient group with whatever has been
found effective but not necessarily
effective for all patients with the disease or
condition. For decades, we have accepted risks from lethal side effects to a spectrum of results
when it comes to patient outcomes from very effective to not at all. Companion Diagnostics is
powerful as it now permits treatment of subgroups of patient with a certain illness with a
stratified approach that has proven to improve response rates versus traditional medicine.
Assuredly, what was once solely a method of identifying rare genetic diseases has since proven
to have a myriad of applications, from the characterization of tumors to the detection of
infectious agents [1][2][3].
The application of this approach towards stratification of patient populations via a
multitude of technologies is, then, useful in the evolution of treatment from the state that it is in
now. With targeted drugs being released monthly, the assay can not only test for the presence of
disease, but can direct medical professionals to better therapy options. Companion diagnostics
Figure 1- Contrast with Traditional Medicine. The figure shows the breakdown of the general diseased sub-group population into groups “A” and “B” based on response to a companion diagnostic. “A” is the positive response group and is likely to respond to targeted therapeutic treatment using the stratified approach. “B” is the negative response group and is unlikely to respond to targeted therapeutic treatment using the stratified approach. Source: Sarah K. Byron et al. Clin Cancer Res 2014;20:1469-1476

rely on this concept to co-develop a targeted drug and a diagnostic assay to identify suitable
subjects simultaneously [4].
As interest in personalized medicine in recent years has grown, so has the scientific clout
such that there is no denying that this is the future of treatment for many patients. This is
exemplified in the increase of the number of prominent personalized medicine drugs available
from 2006 to 2011, when the number of available examples ballooned from thirteen to seventy-
two. [5] PricewaterhouseCoopers has predicted personalized medicine will see an eleven percent
increase in the market year to year, with an estimate of $452 billion as the 2015 market value.
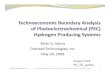
Figure 2 seeks to exemplify that the
market for personalized medicine has been
trending positively with regard to specialty
drug approvals from 2005 to 2014, with a
similar trend expected for 2015. In fact,
according to PwC’s Health Research Institute,
the specialty drug Viekira Pak, which is used
in the treatment of Hepatitis C, is estimated to
have three billion dollars in sales in 2016, a
number similar to the estimated revenue from the sale of the generic drug Lipitor for Pfizer. [6]
That is to say, the popular medication for high cholesterol with a target population of around 40
million adults, across the United States alone, is being matched in sales by a drug that has a
target population of about 2.4 million individuals. However, this estimation of sales becomes
more understandable as consideration is given to the fact that Viekira Pak is a curative treatment
in around 95% of users and thus, can command a greater price. The history of specialty Hepatitis
Figure 2- Number of specialty drug approvals year to year with orange representing approved traditional drugs and red representing specialty drug approvals. Source: PwC Health Research Institute

C drugs started with Boceprevir and Telaprevir, the first of the direct-acting antivirals that were
used clinically in the treatment of Hepatitis C; they illustrate the starting point in the steady
advancement in Hepatitis C treatment effectiveness in recent years. [7]
However, this example also illustrates the biggest pitfalls of personalized medicine with
regard to companion diagnostics. As the market for these treatments expands, the ready
acceptance of these drugs is becoming more and more reliant on dramatic results, such that
developers of specialty drugs receive proper attention. At the same time, regulation of the
necessary co-developed diagnostics by the Food and Drug Administration (FDA) is leagues
ahead of regulation of laboratory developed tests, with regard to evidence development of
efficacy. Even the July 2014 Consumer Health Information Report, released by the FDA,
claimed that because each companion diagnostic test is created as a companion to and is paired
with a specific drug, “the development of both products requires close collaboration between
experts in both FDA’s device center, which evaluates the test to determine whether it may be
cleared or approved, and FDA’s drug center, which evaluates the drug to determine whether it
may be approved.” Using the Genentech drug MPDL3280A, an engineered, anti-programmed
death ligand 1 (anti PD-L1) antibody as a case study, I will seek to show that not only does this
standard put unnecessary weight on solely the drug development party, but that there is currently
no way around the standard for companies.
To further understand efficiencies in the field of drug development, as well as its
financial and regulatory future in healthcare around the world, I will also seek to reflect upon the
types of models used by payers in various countries. One factor that dramatically differentiates
the US from other countries is the amount of money that can be injected into healthcare at any
one time. The United States has by far the highest per capita healthcare spending at $8362

current international dollars, as adjusted using the purchasing power parity. For this reason, there
has been a desire, but no real need, to change the underlying healthcare system to accommodate
for clinical or cost effectiveness. Using the UK and France as examples of different models that
could be used by payers as a clear standard from which reimbursement decisions can be better
made in the future, I will also illustrate that a more efficient regulatory system is not the reality
of the distant future, but rather that of a more proximal one.

MATERIAL AND METHODS
The project had two objectives. The first was to consolidate the regulatory environment
surrounding Laboratory Developed Tests (LDT) and the normal FDA 510(k) or PMN process by
which drug developers must obtain approval for the use of their diagnostic tests. This
information was for the most part completed using of the ASU library database from which
much of the information and articles of necessary information were excavated for use.
Furthermore, the case study of the Genentech and PD-L1 drug was conducted through interview
of Roche Tissue’s Market Access Leader Jim Armstrong, as well as Genentech publications. The
secondary objective was to review the requirements and considerations of the United Kingdom
and France’s healthcare oversight committees in order to identify key requirements. This was
done via ASU’s library database as well as the website for the French Health Assessment Board,
Haute Autorité de Santé (HAS).

RESULTS
Table 1. Population Coverage
Country Health Insurance Coverage Population Covered
United States[8]
Private Coverage 200 millionPublic Coverage 70-80 millionMedicare 44 million(Uninsured) 45 million
United Kingdom[9]
Private Coverage 500 thousandNationalized Healthcare 49.5 million
France [10] Mandatory Health Insurance (HI) System 63.9 million
Table 2. Technology Assessment Bodies / Decision Makers
Country Technology Assessment Bodies / Decision Makers
United States [8]MedicareMedicaidPrivate Payer
United Kingdom[9]
National Institute for Health and Care Excellence (NICE)National Coordinating Centre for Health Technology Assessment (NCCHTA)
France[10]Comité des Médicaments et des Dispositifs Médicaux Stériles (COMEDIMS), a subcommittee of the Hospital Medical Committee, Commission Médicale d’Etablissement (CME)
Technology Assessment Process in the United States
In the United States, private payers and Medicaid payers are the primary decision makers
regarding coverage for diagnostic tests. The decision is reached through an analysis of the
“expected volume of use, cost-impact to the organization, and concerns over data and/or clinical
utility of products.” Payers produce individual HTA reports to provide information regarding the
costs, effectiveness, and current/expected impacts of various healthcare tests and treatments.

Payers may also seek out expertise and HTA reports from third-party technology assessment
organizations, e.g., Hayes, ECRI, and BCBSTEC.
Source:
National Institutes of Health: National Information Center on Health Services Research and Health Care Technology
ECRI Institute website
Evaluation of Genomic Applications in Practice and Prevention website
Technology Assessment Process in the United Kingdom
In the United Kingdom, the National Coordinating Centre for Health Technology
Assessment (NCCHTA) is in charge of producing HTA reports to provide information to those
whom provide, receive, and plan care through the Nationalized Healthcare System (NHS). The
HTA report provides details regarding the costs, effectiveness, and current/expected impacts of
various healthcare tests and treatments [9].
The National Institute for Health and Care Excellence (NICE) is in charge of selecting
interventions for review based on a set of published guidelines:
1. “Is the technology likely to result in a significant health benefit, taken across the NHS as
a whole, if given to all patients for whom it is indicated?” [9]
2. “Is the technology likely to result in a significant impact on other health related
government policies (e.g. reduction in health inequalities)?” [9]
3. “Is the technology likely to have a significant impact on NHS resources (financial or
other) if given to all patients for whom it is indicated?” [9]

4. “Is the Institute likely to be able to add value by issuing national guidance? For instance,
in the absence of such guidance is there likely to be significant controversy over the
interpretation or significance of the available evidence on clinical and cost
effectiveness?” [9]
Technology Assessment Process in France
In France, a product’s medical benefit is determined by the use of five criteria: “efficacy
and safety; position of the medicine in the therapeutic strategy and the existence or absence or
therapeutic alternatives; severity of the disease; type of treatment: preventative, curative, or
symptomatic; and public health impact.” Based on these five criteria, one of five medical benefit
levels is assigned to the product by the Commission d’Evaluation des Médicaments (CEM):
insufficient to justify a reimbursement, weak, moderate, important, or major, in increasing
degrees of perceived benefit.
There are several different governmental bodies that oversee the technological
assessment process in France, each with a different responsibility in the overall process. The
Agence Française de Securité Sanitaire des Produits de Santé (AFSSAPS) oversees inspection of
industrial sites, controls laboratories and scientific evaluation, and controls advertising. The
Haute Autorité de Santé (HAS) oversees assessment of medical procedures, medications, and
medical devices, publishes guidelines, certifies doctors, and determines accreditation of
healthcare organizations. The Commission Nationale d’Evaluation des Dispositifs Médicaux et
des Technologies de Santé (CNEDiMTS) further assesses medical procedures that were
previously assessed by HAS [10].

DISCUSSION
The FDA has released guidelines on the regulation of the Biomedical Diagnostics test
that are made independently by LDTs [11][12][13]. However, the current regulatory system has
caused many to scratch their heads; the regulatory environment for companion diagnostics is
quite clear: in order for a targeted therapy drug to be approved, it must have an effective
diagnostic tool with which you can determine if a patient falls within certain, genetic or
otherwise, specifications for the use of the drug [12][14]. That concept is not hard to grasp and it is
quite logical to enforce the need to provide a companion diagnostic with the drug. This same
stringent scrutiny is not, however, afforded to LDTs. The current problem with LDTs is that
there is never any direct link to them and any kind of regulatory agencies. Laboratories that are
overseen by CLIA either are or are not allowed to perform certain tests, based on the complexity
of the test and the CLIA requirements the lab meets to prove their capability of doing high
complexity testing. If the laboratory passes the requirements laid out by CLIA, they can produce
any LDT with no oversight as to the efficacy of the test.
Jim Armstrong, the Market Access Leader at Ventana, first voiced these concerns
relaying that “there is no way to incentivize labs contracting to hospitals to use one assay over
another” (personal communication, June 26, 2015). For companies to even be able to market
their diagnostics, then, they need to make the antigen available to laboratories to train technicians
on the use of the assay and how to read it. Due to the fact that the product is held in the trials
phase, all diagnostics manufacturers have resorted to giving the raw components of the

diagnostic to labs for them to make their own tests. These raw materials, called Analyte Specific
Reagent (ASRs) are purchased by the lab and can be used for in-house LDTs. Any laboratory
that is capable of high complexity testing is then capable of running ASR based tests, and thus
can work around any restriction as to the regulation of LDTs. This is, in most cases,
economically prudent because it allowed labs to be ready to run a particular diagnostic for the
targeted therapeutic upon release of the drug thus eliminating the post release training period.
There is an increased prevalence of personalized medicine products available in the
market. In the case of oncology, this has many a time lead to not only competing drugs but
competing diagnostic assays that often use the same biomarker. Effectively, this means that
multiple diagnostic assays can, with different degrees of efficacy that will not be tested and
which are not necessarily developed hand-in-hand with the drug they are to be used with, can be
administered interchangeably and used to diagnose a non-small cell cancer variant that the
Genentech drug is effective in treating in lung and bladder instances of this cancer variant.
In the case of the Genentech drug MPDL3280A for example, the companion anti-
programmed death ligand 1 (anti PD-L1) diagnostic being co-developed and tested is going to be
competing with anti-PDL1 assays of two other companion diagnostic producers; Dako is making
the test for Merck and Bristol Myers Squibb. Whilst the Genentech drug and diagnostic is being
held for approval as both Roche products go through phase three trials, there is already no
guarantee that companies will go through the approval process the FDA requires and come out of
it being able to profit from their diagnostic products, each of which were a cost incurred in
research and development. This means that when MPDL3280A is approved for use, laboratories
will have three routes by which they can test for patients being positive for the PD-L1 antigen:

The Ventana assay, the Dako assays, and the LDTs that have been in the works since Ventana
Medical Systems released ASRs to labs that will be running the assay in the future.
Essentially, FDA oversight is thorough and ensures the production of a high quality
product. However, contrastingly, oversight of LDTs by CMS’ CLIA program at no point
addresses the clinical validity of any test. Testing for the analytical validity and putting it under
the trials, inspection, and scrutiny of the FDA whilst not ensuring that only the tests that have
been shown to have analytical validity be used to test for efficacy in the hospital is like asking
Pfizer to put in the research and development costs involved with Lipitor and then allowing
independent third parties to produce the same product with no proof of efficacy at a price
undercutting the pricing strategy that would be necessary to earn back the R&D dollars. The first
step to fixing the inefficiency of the current system, then, is to either have the FDA extend its
regulatory authority to include LDTs or expand the activities of CMS’ CLIA to include clinical
validity of individual test produced by laboratories in cases where the diagnostic is considered
high complexity. By including LDT review in a premarket capacity, the validity of these tests
can span beyond the doors of the laboratory in which they were developed.
Furthermore, it is important to consider that the US healthcare system is very much
decentralized and serves its citizens via three primary payor bodies. The first is private coverage,
which is by far the largest percentage of privately insured citizens among all three comparable
health care systems. As Table 1 shows, only about 1% of the UK population is privately covered
with 99% having nationalized healthcare. In France, the mandatory health insurance system
ensures that every member of the country of 63.9 million is covered by the government. The
other two insurers in the US are Public Coverage and Medicare with about 14.11 million

uninsured as of 2009, a number that has shrunk to 12.9% since the passing of the Affordable
Care Act.
The National Institute for Health and Care Excellence (NICE) and the National
Coordinating Centre for Health Technology Assessment (NCCHTA) in Britain and Comité des
Médicaments et des Dispositifs Médicaux Stériles (COMEDIMS), a subcommittee of the
Hospital Medical committee in France are the main technology assessment bodies that are the
decision makers. This presents us yet again with a rather large leap when it comes to the reality
of the gap in the assessment bodies. The whole of the decision making process is centralized to
these national bodies and some regional assessment boards while in the US, private payers,
whose actions are far more reliant on stakeholders in the long run make technology assessments.
Our assessment process is different than that of the UK and France because whereas
central bodies, often bound by EU regulations that allow for citizens of one country to get
benefits in another work in assessment committees with clear cut requirements from all
pharmaceutical producers, US payers can choose to outsource even their assessments to third
parties that will do all of their analysis for them. This process stems from the fact that unlike the
UK and France, any drug that has proven valid in the eyes of the FDA can and will be
reimbursed, even if begrudgingly. Here we can take a lesson from France, a country in which
drug approval is completely separate from reimbursement, which is done one a gradient
according to the medical benefit level. In this way, a company cannot simply rebrand a product
at the end of a patent (i.e. Lipitor) and sell what is essentially generic atorvastatin as an
expensive branded product because the new drug would not demonstrate a significant advantage.
The trend toward the idea of significant benefit exists even in the UK’s NICE model for
assessment and reimbursement. Drugs are given value if they are the yes tick mark to questions

regarding bridging the gap in inequality. The final change we can make in our assessment system
move away from risk-benefit analysis towards cost-effectiveness metrics as these will better
allow payers to assess what drug is the best value for the expenditure [13][15][16]. This doesn’t mean
that just because a drug is expensive, it shouldn’t be reimbursed. However, it does help bridge
the gap between cost and end of life procedures by bringing into questions of the opportunity
cost of treating an older individual already living beyond their life expectancy with drugs that are
more expensive and could reduce their quality of life in their last months; it will also allow for
many other qualitative measures like the drug’s anticipated effect [16]. That is you would expect
to pay more for a curative product than a pill you have to take for the rest of your life with regard
to monthly payments [13].
Ideally, the FDA has done a respectable job of being strict with its conditions. It is now
time to be fair with those conditions such that dramatic medical advances are no stunted by lack
of proper reimbursement and assurances that biologics developed alongside new drug receive a
fair chance to prove their value. By changing our approach to how we reimburse promising
technology and promoting a health assessment environment that allows for stand out drugs and
diagnostics to do just that, we will, if nothing else, make the medical environment simpler and
more efficient for all its stakeholders.

REFERENCES
1. Jameson, J. L., & Longo, D. L. (2015). Precision Medicine—Personalized, Problematic,
and Promising. New England Journal of Medicine.
2. Moore, M. W., Babu, D., & Cotter, P. D. (2012). Challenges in the codevelopment of
companion diagnostics. Personalized Medicine, 9(5), 485-496.
3. Euan, A., & Falk, C. V. R. B. (2015). The Precision Medicine Initiative A New National
Effort.
4. Whitfield, J. B. (2013). Genetics and molecular biology in laboratory medicine, 1963–
2013. Clinical Chemistry and Laboratory Medicine, 51(1), 113-117.
5. Pfizer's Projected $3B Drug: Name Will Shock You. (2013). Retrieved July 3, 2015.
6. Habersetzer F, Leboeuf C, Doffoël M, Baumert TF (2012). Boceprevir and personalized
medicine in hepatitis C virus infection. Pharmgenomics Pers Med. 2012;5:125-37. doi:
10.2147/PGPM.S24259.
7. U.S. Department of Health and Human Services, Food and Drug Administration, Center
for Devices and Radiologic Health. Public Meeting: Oversight of Laboratory Developed
Tests [LDTs] (2010).
8. Garfield, S. USA: In-Vitro Diagnostics. Retrieved June 26, 2015, from
http://www.ispor.org/htaroadmaps/USMD.asp#Diagram

9. Wilson, G. (2015). United Kingdom - Diagnostics. Retrieved June 26, 2015, from
http://www.ispor.org/htaroadmaps/UKDiagnostics.asp
10. Chicoye, A., & Levesque, K. France - Medical Devices. Retrieved June 26, 2015, from
http://www.ispor.org/htaroadmaps/FranceMD.asp
11. U.S. Department of Health and Human Services, Food and Drug Administration, Center
for Devices and Radiological Health, Center for Biologics Evaluation and Research, and
Center for Drug Evaluation and Research. Draft Guidance for Industry and Food and
Drug Administration Staff: In Vitro Companion Diagnostic Devices (2011).
12. U.S. Department of Health and Human Services, Food and Drug Administration. Drug-
Diagnostic Co-Development Concept Paper (2005).
13. Peabody, J. W., Shimkhada, R., Tong, K. B., & Zubiller, M. B. (2014). New Thinking on
Clinical Utility: Hard Lessons for Molecular Diagnostics. The American journal of
managed care, 20(9), 750-756.
14. Evans, B. J., Burke, W., & Jarvik, G. P. (2015). The FDA and genomic tests—getting
regulation right. New England Journal of Medicine.
15. Buchanan, J., Wordsworth, S., & Schuh, A. (2013). Issues surrounding the health
economic evaluation of genomic technologies. Pharmacogenomics,14(15), 1833-1847.
16. Atherly, A. J., & Camidge, D. R. (2012). The cost-effectiveness of screening lung cancer
patients for targeted drug sensitivity markers. British journal of cancer, 106(6), 1100-
1106.
17. Hodgson, D. R., Wellings, R., & Harbron, C. (2012). Practical perspectives of
personalized healthcare in oncology. New biotechnology, 29(6), 656-664.