Embed Size (px)
Citation preview

Unlocking the Cellular Secrets of DiseaseAPPLICATION NOTE
Direct quantification of pharmaceutical effects on cardiac action potentials in human stem cell-derived cardiomyocytes
INTRODUCTIONEach heartbeat results from a transient electrical depolarization, or cardiac action potential (Figure 1), that begins in the sinoatrial node and propagates through the heart to contract the cardiac muscle cells (cardiomyocytes). Since the 1990’s, many FDA-approved drugs (e.g., cisapride, used to treat gastric reflux1) have been linked to action potential arrhythmias and sudden cardiac deaths. Many proarrhythmic drugs inhibit potassium flux through the Kv11.1 channel (aka the human Ether-à-go-go-Related Gene, or hERG), encoded by the KCNH2 gene.2 These drugs prolong the cardiac action potential, the related QT interval, and the time required for cardiomyocyte repolarization (Figure 1). These side effects increase the incidence of Torsade de Pointes, a dangerous arrhythmia that can result in sudden cardiac death.
The US FDA and other regulatory agencies now require intensive testing of all drug candidates for proarrhythmic effects prior to human clinical trials.3 Current preclinical cardiosafety testing systems use electrophysiological methods to test compounds for effects on cardiac action potentials in intact hearts, tissue fragments, cardiomyocytes isolated from rabbits or dogs, or non-cardiac cell lines engineered to express the hERG channel.4,5 However, non-human model systems and non-cardiac cell lines incompletely model the physiology of human cardiomyocytes and may fail to predict proarrhythmic effects in the clinic.
Cardiomyocytes differentiated from human stem cells (hSC-CMs) exhibit the contractile phenotype of human ventricular cardiomyocytes6,7 and represent a new human model system for cardiosafety testing. Previous studies using Vala’s Kinetic Image Cytometer® (KIC®)—an automated, high-throughput digital microscopy workstation designed to record images at high frame rates—identified compounds that prolong cardiac action potentials in hSC-CMs loaded with Fluo-4, a fluorescent intracellular calcium indicator. This calcium transient
Figure 1. The relationship between the cardiac action potential
duration, hERG channel conductance, Torsades de Pointes (from
Grilo et al., 2010).
APPLICATION NOTE
Page 2
data predicted the clinical proarrhythmic effects of test compounds better than non-human in vitro systems and rivaled the predictive value of data obtained by administering the compounds to living canines.6–9
In this pilot study, we tested if Vala’s IC200 KIC® and CyteSeer® (Vala’s cell image analysis software) can directly quantify effects of compounds on the duration of cardiac action potentials in hSC-CMs loaded with FluoVoltTM, a molecular voltage sensor that increases
in fluorescence when cells depolarize.10 We tested two compounds with known effects on cardiac action potentials: dofetilide, which prolongs cardiac action potentials by inhibiting potassium flux through hERG; and nifedipine, which shortens cardiac action potentials by inhibiting calcium flux through L-type calcium channels. Our results demonstrate that Kinetic Image Cytometry® can quantify action potential duration from hundreds of hSC-CMs. This method enables high-throughput, accurate, and cost-effective cardiosafety testing.
METHODShSC-CMs (NCardia, Cor.4U Cardiomyocytes) were thawed and cultured in accordance with the protocols suggested by the cell manufacturer in 96-well plates featuring optically clear well bottoms (Cat. No. 655090, Greiner, Monroe, NC, USA) and maintained at 37°C and 5% CO2 for 6 days prior to imaging in culture media from the cell manufacturer. hSC-CMs displayed spontaneous beating within 48 hours of thawing. The cells were loaded with FluoVoltTM (Thermo Fisher) as per the manufacturer instructions in a loading buffer of 20 mM HEPES in HBSS that contained 200 ng/mL Hoechst 33342, a live cell nuclear stain.
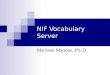
Cells were loaded for 30 minutes at 37°C. The cells were rinsed and test drugs dissolved in DMSO (final DMSO concentration: 0.1%) were applied: nifedipine at doses of 0.001, 0.01, 0.1, and 1 μM and dofetilide at does of 0.33, 1.0, 3.2, and 10 nM (Figure 2). Overall, 10 wells were treated with 0.1% DMSO alone and 5 wells were treated with each dose of dofetilide or nifedipine. The hSC-CMs were incubated with test compounds for 20 minutes prior to being imaged (incubation and imaging were done at 37°C). Image acquisition was with a 20x NA 0.75 objective.
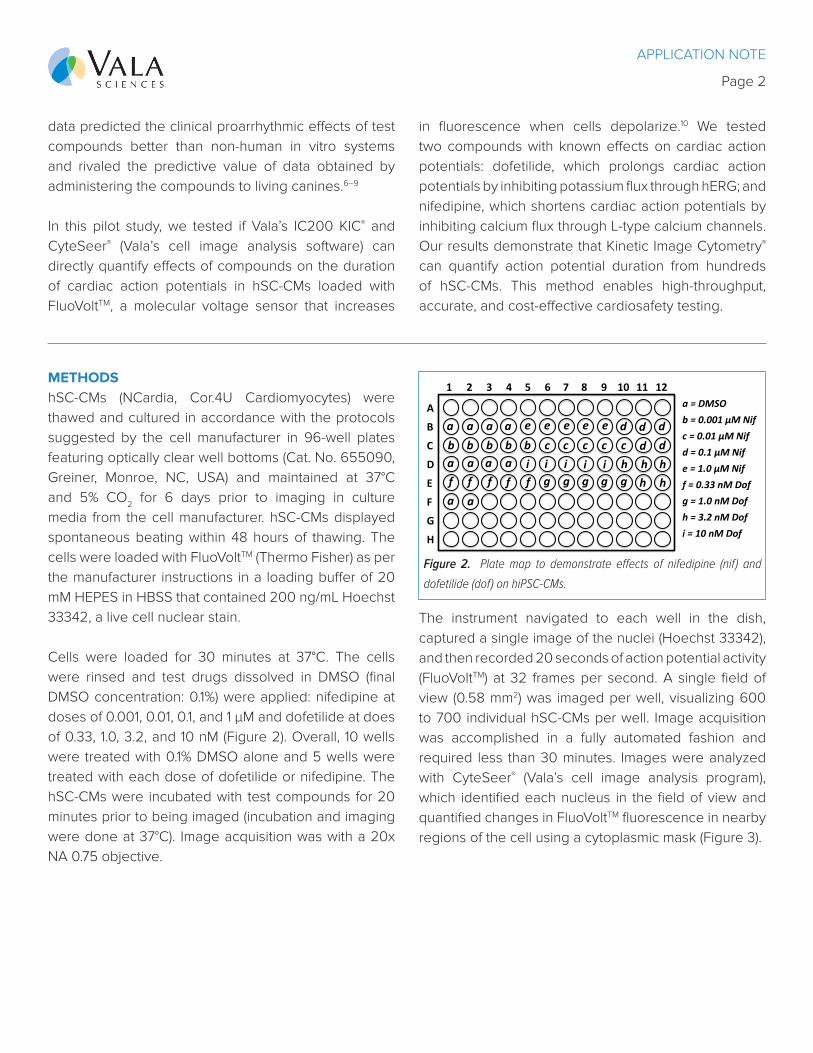
The instrument navigated to each well in the dish, captured a single image of the nuclei (Hoechst 33342), and then recorded 20 seconds of action potential activity (FluoVoltTM) at 32 frames per second. A single field of view (0.58 mm2) was imaged per well, visualizing 600 to 700 individual hSC-CMs per well. Image acquisition was accomplished in a fully automated fashion and required less than 30 minutes. Images were analyzed with CyteSeer® (Vala’s cell image analysis program), which identified each nucleus in the field of view and quantified changes in FluoVoltTM fluorescence in nearby regions of the cell using a cytoplasmic mask (Figure 3).
a=DMSOb=0.001µMNifc=0.01µMNifd=0.1µMNife=1.0µMNiff=0.33nMDofg=1.0nMDofh=3.2nMDofi=10nMDof
A
B
C
D
E
F
G
H
1 2 3 4 5 6 7 8 9 10 11 12
a a a a
aa a a
a a
b b b b b c c c c cd d d
dd
e e e e e
f f f f f g g g g gh h h
h hi i i i i
Figure 2. Plate map to demonstrate effects of nifedipine (nif) and
dofetilide (dof) on hiPSC-CMs.
APPLICATION NOTE
Page 3
Figure 3. Identifying iPSC-CMs
in the field of view. iPSC-CMs
were seeded in a 96-well dish
and loaded with FluoVolt (green)
and Hoechst 3342 (blue). A, Full
field of view. B, Cytoplasmic
mask and cell ID numbers
assigned by CyteSeer® (area in
A at higher magnification).
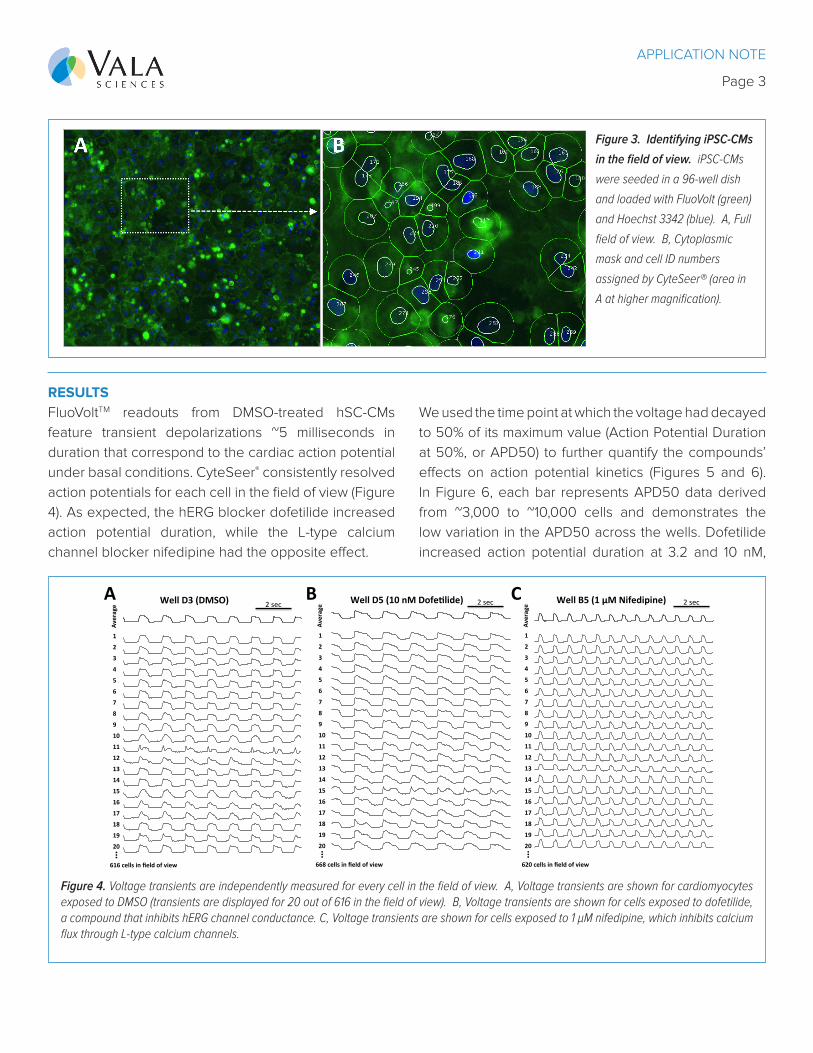
RESULTSFluoVoltTM readouts from DMSO-treated hSC-CMs feature transient depolarizations ~5 milliseconds in duration that correspond to the cardiac action potential under basal conditions. CyteSeer® consistently resolved action potentials for each cell in the field of view (Figure 4). As expected, the hERG blocker dofetilide increased action potential duration, while the L-type calcium channel blocker nifedipine had the opposite effect.
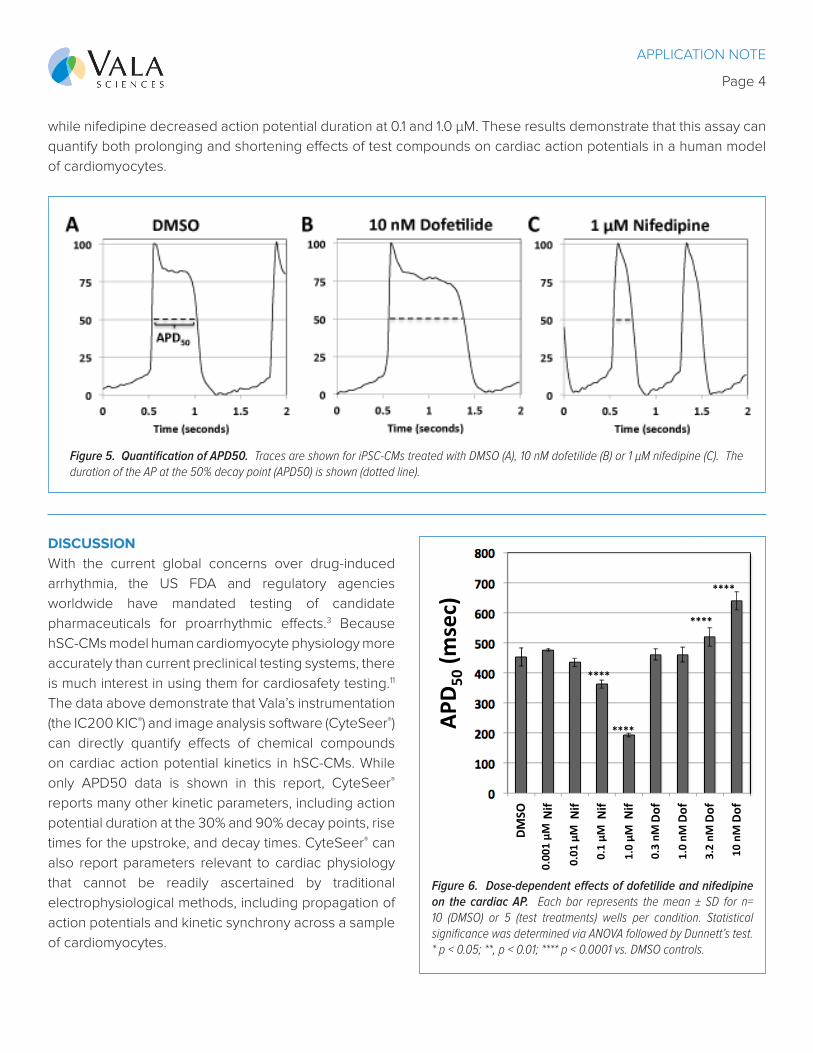
We used the time point at which the voltage had decayed to 50% of its maximum value (Action Potential Duration at 50%, or APD50) to further quantify the compounds’ effects on action potential kinetics (Figures 5 and 6). In Figure 6, each bar represents APD50 data derived from ~3,000 to ~10,000 cells and demonstrates the low variation in the APD50 across the wells. Dofetilide increased action potential duration at 3.2 and 10 nM,
0
500
1000
1500
2000
2500
3000
0 1 2 3 4 5 6 7 8 9 10
Average
1
2
3
4
5
6
7
13
9
8
10
12
11
14
15
16
17
18
19
20
…
668cellsinfieldofview
WellD5(10nMDofeAlide) 2sec
0
500
1000
1500
2000
2500
3000
0 1 2 3 4 5 6 7 8 9 10
Average
1
2
3
4
5
6
7
13
9
8
10
12
11
14
15
16
17
18
19
20
…
620cellsinfieldofview
WellB5(1µMNifedipine) 2sec
0
500
1000
1500
2000
2500
3000
0 1 2 3 4 5 6 7 8 9 10
Average 2sec
1
2
3
4
5
6
7
13
9
8
10
12
11
14
15
16
17
18
19
20
…
616cellsinfieldofview
WellD3(DMSO)A B C
Figure 4. Voltage transients are independently measured for every cell in the field of view. A, Voltage transients are shown for cardiomyocytes exposed to DMSO (transients are displayed for 20 out of 616 in the field of view). B, Voltage transients are shown for cells exposed to dofetilide, a compound that inhibits hERG channel conductance. C, Voltage transients are shown for cells exposed to 1 µM nifedipine, which inhibits calcium flux through L-type calcium channels.
APPLICATION NOTE
Page 4
while nifedipine decreased action potential duration at 0.1 and 1.0 μM. These results demonstrate that this assay can quantify both prolonging and shortening effects of test compounds on cardiac action potentials in a human model of cardiomyocytes.
Figure 5. Quantification of APD50. Traces are shown for iPSC-CMs treated with DMSO (A), 10 nM dofetilide (B) or 1 µM nifedipine (C). The duration of the AP at the 50% decay point (APD50) is shown (dotted line).
DISCUSSIONWith the current global concerns over drug-induced arrhythmia, the US FDA and regulatory agencies worldwide have mandated testing of candidate pharmaceuticals for proarrhythmic effects.3 Because hSC-CMs model human cardiomyocyte physiology more accurately than current preclinical testing systems, there is much interest in using them for cardiosafety testing.11 The data above demonstrate that Vala’s instrumentation (the IC200 KIC®) and image analysis software (CyteSeer®) can directly quantify effects of chemical compounds on cardiac action potential kinetics in hSC-CMs. While only APD50 data is shown in this report, CyteSeer® reports many other kinetic parameters, including action potential duration at the 30% and 90% decay points, rise times for the upstroke, and decay times. CyteSeer® can also report parameters relevant to cardiac physiology that cannot be readily ascertained by traditional electrophysiological methods, including propagation of action potentials and kinetic synchrony across a sample of cardiomyocytes.
DMSO
0.00
1Nif
0.01
0Nif
0.10
Nif
1.00
Nif
0.00
03Dof
0.00
1Do
f
0.00
32Dof
0.01
0Do
f
Dof(0.0030)
APD50(msec)
****
****
****
****
*
0.00
30Dof
APD 5
0(msec)
0.00
1µM
0.01
µM
0.1µM
1.0µM
0.3nM
1.0nM
3.2nM
10nM
Figure 6. Dose-dependent effects of dofetilide and nifedipine on the cardiac AP. Each bar represents the mean ± SD for n= 10 (DMSO) or 5 (test treatments) wells per condition. Statistical significance was determined via ANOVA followed by Dunnett’s test. * p < 0.05; **, p < 0.01; **** p < 0.0001 vs. DMSO controls.
APPLICATION NOTE
Page 5
CONCLUSIONSThis report demonstrates that Vala’s IC200 KIC® and CyteSeer® can measure voltage transients in hSC-CMs loaded with FluoVoltTM, which is relevant for cardiosafety testing. Vala’s technology can also measure voltage in hSC-CMs derived from individuals with mutations in cardiac ion channels that cause prolonged action potentials. Previous studies have applied Vala’s technology to elucidate the role of microRNAs in cardiac calcium transients during heart failure12 and to identify FSTL1 as an endogenous cardiac protein with proliferative effects that could be targeted to treat infarctions.13 Vala’s IC200 KIC® can also quantify action potentials and calcium transients in adult cardiomyocytes and other excitable cells such as neurons or skeletal muscle to derive data relevant to research in neurodevelopment, neurodegeneration, or muscular dystrophies. Thus, the IC200 KIC® is a versatile automated microscopy workstation with broad applications across biomedical and cell biology research.
CONTACT USPlease contact Vala Sciences, Inc (www.valasciences.com/contact) for more information about purchasing an instrument, which includes a copy of CyteSeer®. We also provide drug discovery or safety screening services using our technologies.
REFERENCES
1. Mohammad, S., Zhou, Z., Gong, Q. & January, C. T. Blockage of the HERG human cardiac K+ channel by the gastrointestinal prokinetic agent cisapride. American Journal of Physiology-Heart and Circulatory Physiology 273, H2534–H2538 (1997).
2. Grilo, L.S., Carrupt, P.A. & Abriel, H. Stereoselective Inhibition of the hERG1 Potassium Channel. Front. Pharmacol. 1, (2010).
3. Turner, J. R. et al. Drug-induced Proarrhythmia and Torsade de Pointes: A Primer for Students and Practitioners of Medicine and Pharmacy. The Journal of Clinical Pharmacology 58, 997–1012 (2018).
4. Berridge, B. R., Schultze, A. E., Heyen, J. R., Searfoss, G. H. & Sarazan, R. D. Technological Advances in Cardiovascular Safety Assessment Decrease Preclinical Animal Use and Improve Clinical Relevance. ILAR J 57, 120–132 (2016).
5. Gintant, G., Sager, P. T. & Stockbridge, N. Evolution of strategies to improve preclinical cardiac safety testing. Nature Reviews Drug Discovery 15, 457–471 (2016).
6. Pfeiffer, E. R., Vega, R., McDonough, P. M., Price, J. H. & Whittaker, R. Specific prediction of clinical QT prolongation by kinetic image cytometry in human stem cell derived cardiomyocytes. Journal of Pharmacological and Toxicological Methods 81, 263–273 (2016).
7. Lu, H. R. et al. High Throughput Measurement of Ca++ Dynamics in Human Stem Cell-Derived Cardiomyocytes
by Kinetic Image Cytometery: A Cardiac Risk Assessment Characterization Using a Large Panel of Cardioactive and Inactive Compounds. Toxicol Sci 148, 503–516 (2015).
8. Cerignoli, F. et al. High throughput measurement of Ca2+ dynamics for drug risk assessment in human stem cell-derived cardiomyocytes by kinetic image cytometry. Journal of Pharmacological and Toxicological Methods 66, 246–256 (2012).
9. Pfeiffer, E. R. et al. Kinetic Image Cytometry for Predicting Arrhythmias Using Human Stem Cell-Derived Cardiomyocytes. in Stem Cell-Derived Models in Toxicology (eds. Clements, M. & Roquemore, L.) 153–171 (Springer New York, 2017). doi:10.1007/978-1-4939-6661-5_8
10. Miller, E. W. et al. Optically monitoring voltage in neurons by photo-induced electron transfer through molecular wires. PNAS 109, 2114–2119 (2012).
11. Gintant, G., Fermini, B., Stockbridge, N. & Strauss, D. The Evolving Roles of Human iPSC-Derived Cardiomyocytes in Drug Safety and Discovery. Cell Stem Cell 21, 14–17 (2017).
12. Wahlquist, C. et al. Inhibition of miR-25 improves cardiac contractility in the failing heart. Nature 508, 531–535 (2014).
13. Wei, K. et al. Epicardial FSTL1 reconstitution regenerates the adult mammalian heart. Nature 525, 479–485 (2015).





















![Dealing with community conflict, (lsp 0.010 [dwcc])](https://img.pdfslide.us/doc/110x75/5583625ed8b42afe418b553b/dealing-with-community-conflict-lsp-0010-dwcc.jpg)