Embed Size (px)
Citation preview

Direct Measures of Physical Factors Contributing to Work-Related Musculoskeletal Pain among
Diagnostic Medical Sonographers: A Pilot Study
Lauren Selhorst, RDMS
Radiologic Sciences and Therapy Division
Presented in Partial Fulfillment of the Requirements for Graduation With Distinction from
The School of Allied Medical Professions
Graduation with Distinction Committee Members Kevin D. Evans, PhD Shawn C. Roll, MS Terri Bruckner, MA
The Ohio State University
2011
1

Abstract
Diagnostic medical sonographers are very often exposed to factors that contribute to
workplace injury which have been categorized as work-related musculoskeletal
disorders (or WRMSD). This problem has become increasingly common as the number
of sonographic exams increases. A study to determine the height of the sonographers,
dimensions of the workspace, and other factors would be helpful to obtain a better
understanding of the potential for work-related injuries among sonographers. Survey
research has only provided indirect information and these reports need to be directly
verified. This undergraduate research project is an effort to better understand workplace
injury risk by directly observing sonographers while scanning and evaluated their
postures and positions. The measurements of posture and position are based on a
Rapid Upper Limb Assessment (RULA) scoring form. Direct measures were taken of the
sonographers' heights, exam table heights, and the dimensions of the machine. An
analysis will be completed to determine a potential relationship between the direct
measures (independent variables) and the individual sonographers' pain scores at the
beginning and end of each day. It is predicted that the pain scores will be in some way
related to the RULA scores, the sonographer heights, and the exam table heights. This
study begins to capture workplace factors that may plague sonographers and contribute
to WRMSD. Future work should be directed to modify these factors in order to prevent
these injuries from occurring.
2

Acknowledgements
I would like to thank my advisor, Dr. Kevin Evans, for all the work and support he has provided during the research process. He spent many hours meeting with me, editing my writing, applying for IRB approval, and supplying me with many helpful tips and advice. Without his guidance, this project would not have been possible.
I would also like to thank Shawn Roll for providing education on the RULA tool and advice on how to analyze the data.
A thank you is also extended to The Ohio State University East Hospital and all the sonographers in the Non-Invasive Vascular Lab and to Barbara Montgomery, RDMS, for allowing me to evaluate their scanning techniques.
3

Table of Contents
Abstract.. . .. . ... . .. ... ... . .. . . . . .. . .. . .. . .. ... ... . .. .. . .. ............................................ . .......... Page 2
Acknowledgements .......................................................................................... Page 3
Chapter 1
a. Problem Statement.. ...................................................................................... Page 5
b. Related Research .......................................................................................... Page 6
c. Objectives of the Study ................................................................................. Page 13
Chapter 2
a. Procedures ................................................................................................. Page 14
b. Design ....................................................................................................... Page 14
Chapter 3
a. Results ....................................................................................................... Page 17
Chapter 4
a. Discussion .................................................................................................. Page 20
References .................................................................................................... Page 27
Appendices
a. Appendix A... .. . .. .. . . .. . . . . .. . .. .. . ....................................................................... Page 28
b. Appendix 8 .................................................................................................. Page 30
c. Appendix C ................................................................................................. Page 33
d. Appendix D ................................................................................................. Page 34
e. Appendix E ................................................................................................. Page 34
4

Chapter 1
Problem Statement
Diagnostic medical sonographers are very often exposed to factors that contribute to workplace
injury which have been categorized as work-related musculoskeletal disorders (WRMSD).
WRMSD have become increasingly common in the field of sonography as a 2000 survey found
that "more than 80% of sonographers are scanning in pain during a study and 20% of these
professionals eventually experience a career-ending injury".' Even more recently, another
survey was conducted yielding the greatest participant sample to date with 2963 respondents.
This new survey revealed a 9% increase in the number of sonographers scanning in pain since
the 2000 survey, which implies that WRMSD are increasingly being reported in the field. 2
Obtaining a quality sonographic image can sometimes prove to be challenging and demands
odd angles and increased pressure on the hand and wrist. This can lead to scanning practices
that can contribute to WRMSD. Some scanning practices in the sonography field that have
been linked to WRMSD include: tightly gripping the transducer, sustained shoulder abduction,
twisting and bending of the wrist, maintaining poor posture for long periods of time, and
increased workload.' Other factors that have been linked to WRMSD include height, age, and
gender differences among sonographers. 3 Certain risk factors, such as level of personal
stress, the number of examinations performed per day, the length of time each examination
requires, the sonographer's physical and mental status, behavior such as work/rest cycles,
awkward postures, and physiological factors, have also been identified as contributing to
5

WRMSO. 3 The increased risk ofWRMSO has necessitated extensive research in the work
habits and environments of sonographers internationally.
Related Research
WRMSO are increasing among diagnostic medical sonographers (OMS) and previous research
efforts have been executed to better understand the burden attached to the delivery of this
diagnostic service. This literature reviewed is organized in a chronologic manner to capture the
work that has evolved over time.
One of the earlier studies was conducted by Brown et al. to address the problem of
musculoskeletal disorders as a broad topic over a time span of three hundred years.
Throughout history, scribes, clerks, and telegraphers have all been documented as having
musculoskeletal disorders related to their occupations. Phrases such as writer's cramp and
scrivener's palsy were coined to refer to these disorders. The increased prevalence of these
disorders in the last several years, not only in diagnostic medical sonography, is described as
an epidemic and a 20th century health disaster' There is currently a lack of consensus on what
to call these musculoskeletal disorders because these disorders can arise as a result of a
variety of activities. Research is made difficult by the variety of the disorders. Because the
cause of the disorders can be ambiguous, the authors preferred that the disorders not be called
injuries. The term injury applies only if the cause of the tissue damage is known. 2
Brown et al.'s work takes a biopsychosocial approach to determining the cause of
musculoskeletal disorders. Physical factors were combined with psychological and social
factors in an attempt to find a link to the disorders. Factors were categorized as predisposing
factors, precipitating factors, and perpetuating factors. Predisposing physical factors include
6

poor posture and short arms, while predisposing psychosocial factors include history of anxiety,
depression, job dissatisfaction, and emotional or physical trauma 2 Precipitating physical factors
include minor trauma, change of routine, and long hours of work, while precipitating
psychosocial factors include personal problems or current negative life events 2 Perpetuating
physical factors include poor ergonomics, abduction of the arm, tool design, poor health, and
deficiency conditions (i.e. iron, thyroid, vitamin 812), while perpetuating psychosocial factors
include chronic anxiety or depression, fatigue, financial issues, and attitudes 2
PHYSICAL PSYCHOSOCIAL
Predisposing Factors Poor posture History of anxiety or depression Short arms Job dissatisfaction
Emotional or physical trauma
Precipitating Factors Minor trauma Personal problems Change of routine Current negative life events LonQ work hours
Perpetuating Factors Poor ergonomics Chronic anxiety or depression Abduction of the arm Fatigue Tool design Financial issues Poor health Attitudes Deficiency problems
Sonographers with chronic regional pain were specifically interviewed by researchers; spinal
segmental dysfunction, active myofascial trigger pOints (a hyperirritable spot in skeletal muscle)
on the transducer side, subacromial rotator cuff impingement, and dysfunctional movement of
the scapulothoracic joint were consistently found on the transducer side 2
Electromyography was used to demonstrate the amount of time it takes to fatigue muscles
during arm abduction-"30 degrees of abduction is 60 minutes, 20 minutes when held at 60
degrees, 10 minutes when held at 90 degrees, and 5 minutes when held at 120 degrees.,,2
When scanning, sonographers are sometimes forced to use a variety of these angles, but it is
7

important for them to understand that the greater the angle of abduction the shorter the time to
muscle fatigue and to avoid the greater angles as much as possible to prevent dysfunction.
Primary, secondary, and tertiary prevention methods need to be incorporated into the practice of
all DMS to reduce the risk ofWRMSD.
In a study by Muir et aI., a questionnaire was developed by an occupational health physician, an
occupational health nurse, an ergonomic engineer, an athletic therapist, and a
sonographer/nurse to record indirect incidence of WRMSD and related factors to the practice of
sonography. Sixty-seven members of the Canadian Society of Diagnostic Medical
Sonographers completed the Sonographers Work Health and Ergonomics Survey. Most DMS
worked in general clinical settings, performing a variety of 20 to 45 minute ultrasound exams
respondents had an average work experience of 9.82 years.3
When asked to rate present health status, 62% of DMS answered good, 34% excellent, and 3%
fair. 64% of DMS exercised for a minimum of 20 minutes three times a week, and 63%
exercised their shoulders, back, neck, or arms. Pain was reported in 15% of sonographers
within six months of employment, 45% after three years, and 72% after ten years. Several DMS
experienced changes in home life, work responsibilities, sleep patterns, and psychosocial well
being due to their pain. Shoulders, neck and upper back were found to be the most common
sites of pain. Treatment of WRSMD, either currently or in the past, was obtained by 85% of
DMS. 67% of DMS scaned five to seven hours per day and only 45% took breaks of ten
minutes or longer more than three times per day. Ergonomic education was received by only
66% of DMS within the previous two years at work. Workers responded that they would like to
have adjustable ultrasound equipment and increased exam room space, which they believed
would assist them to perform their work. A mean score of 4 (agree) was found when DMS were
asked if they felt like their own health is compromised because of their profession. 3
8

A survey conducted by David concentrated on the importance of DMS self-reporting WRMSD,
and provided descriptive data during the time frame that the disorders are reported.
Respondents also provided information about barriers that prevent reporting injuries and
administrative responses to WRMSD. Many times, DMS believe that WRMSD is part of their
job and that they need to deal with the situation on their own instead of reporting it. David cited
a 2002 international conference which was held to discuss prevention and corrections that could
combat the increasing prevalence of WRMSD. "Steps that were recommended included
incorporating musculoskeletal injury prevention in sonography educational curricula, including
question related to prevention on credentialing examinations, and requiring prevention
processes for laboratory accreditation.'" Prevention is not only important for the well-being of
the individual DMS, but also for the well-being of the institution. Financially, the loss of one full
time DMS resulted in $21,153 lost in revenue for only one week'it also amounts to more stress
on co-workers and longer wait times for patients'
Additional indirect information was collected using open-ended questions focusing on the
reporting of WRMSD. Some qualitative responses included:
The administrators skeptically sent the sonographer for an examination and testing,' 'the
administrators refused to believe that the injury could occur on the job and forced the
sonographer to scan with the opposite hand the sonographer was using,' 'the workers'
compensation process is daunting,' and 'WRMSD is just part of the job.""
The study by David has limited ability to be generalized, due to its qualitative nature and that the
participants were all from the University of Oklahoma Health Sciences Center. However, it
uncovered some of the reasons that WRMSDs may go unreported.
9

A pilot study was conducted in 2009 that recorded direct measurements on five DMS after
completing four portable neonatal neurosonographic scans in a NICU. Researchers proposed
that specific risk factors involved in performing neonatal neurosonography examinations
contributed to musculoskeletal distress of the wrist and hands. While conducting a portable
neonatal scan, sonographers were forced to maneuver through lines and tubes while wearing
protective gloves and scanning in compromised positions because these premature infants
must remain inside their isolettes at all times. The Rapid Upper Limb Assessment (RULA) tool,
a scoring system that analyzes musculoskeletal postures and positions, was used to evaluate
the sonographers' positions during each exam. Immediately following each examination, a
musculoskeletal sonogram of the DMS' elbows and wrists was also taken in order to evaluate
physiologic changes. Anterior-posterior and length measurements were made of the median
nerve while Power and Spectral Doppler were utilized to record hypervascularization. Lastly,
each DMS was given a visual analog scale (VAS) to self report the level of discomfort in the
neck, shoulder, and wristS
The mean age of the DMS in this study was 43 and mean work experience was 16.7 years.
RULA scores ranged from 1 to 7 with a "1" indicating a low strain posture and a "7" being a
hazardous position. Total RULA scores on the first session were 4.0 and 3.8 at the end of the
fourth session; these results were minimal. The researchers suggested that "comparative
studies using other gold standards are necessary to make any claim for the use of Doppler in
studying WRMSD and CTS more credible."s
Additional indirect information was recorded using a survey of a random and convenient sample
of 5200 registered DMS which returned 2963 respondents. This survey indicated that 90.4% of
DMS were scanning in pain. Shoulder pain was the most common in all groups, while finger,
hand, and wrist pain occurred most often in the older, more experienced groups. Cross-
10

tabulation and Chi-square analysis involving age, gender, height, experience, and full-time or
part-time status were used to analyze the data. These data analyses found that location of pain
varied across the groups. "Aching" was the most common word to describe pain in all groups,
anti-inflammatory medicine was the most common prescribed treatment to treat injuries. There
was no difference in discomfort levels between full-time and part-time employees B
This survey was voluntary, therefore it produced a skewed response population, with most
respondents being over the age of 50 with 20 or more years of experience, a majority under 5'4"
in height, and a majority performing 9 to 11 sonographic examinations per day. Nearly all
participants indicated that they were able to adjust the positions of the examination table and
chair, but few were able to adjust their PACS workstations. Of all respondents, 48% have been
diagnosed with a musculoskeletal injury. The researchers suggested that OMS be followed
over longer periods of time to look at acute verses chronic pain. They recommended that future
studies be performed, and that education be offered to OMS about ergonomic practices to break
bad scanning habits and possibly decrease the prevalence of WRMSOB
In a study on comparing anthropometric measurements and the prevalence of musculoskeletal
injuries, research involved distributing another questionnaire focusing on job strain, obtaining
anthropometric measurements (including height, weight, waist circumference, functional forward
reach, hand breadth, hand length, hand spread), performing grip strength testing, and
evaluating occupational health records. The results indicated that shoulder pain was most
common, occurring in 73% of OMS reporting injury. The lower back followed with 69%, and
pain in the wrist and hand occurred in 54% of OMS. The researchers found that differences in
hand strength did not significantly affect the wrist and hands, but OMS who hold two or more
credentials have an increased risk of having injury in the wrist and hands. Musculoskeletal
11

disorders were less likely to occur in those OMS who were physically larger, had more favorable
job strain scores, and spent less time standing 7
The authors of the article concluded that these results were only descriptive due to the small
sample size. It is suggested that transducers be made customized to different body types of
individual OMS. The authors also provided equipment design changes that could potentially
decrease the risk of musculoskeletal disorders. Height adjustable keyboards, monitors, chairs,
and examination tables, lightweight transducers, and voice-activated controls may improve the
ergonomic risk within sonography.7 A study to determine the relationship of the height of OMS,
dimensions of the workspace, and other factors would be helpful in better understanding the
potential for work-related injuries among OMS.
12

Objectives of the Study
A gap in the literature exists with recording direct measurements of many of the factors that may
be contributory to WRMSO among OMS. Survey research has only provided indirect
information and these reports need to be directly verified. This research project proposed to
better understand these workplace issues by addressing this research question: What direct
measures taken among DMS and the work station and equipment contribute to their level of
discomfort upon completing their daily work?
13

Chapter 2
Procedures
A direct observation of DMS in the work place was used to better investigate factors that may
increase their individual risk of WRMSD. To accomplish this direct observation of DMS at work,
the student researcher obtained consent during clinical rotations in Franklin County area
imaging centers. The researcher was in the site for a ten week period and was able to monitor
conditions over time. Exams were selected for observation based on the competency of the
researcher. The posture and position of the DMS was observed and recorded.
This study is an extension of research being conducted to evaluate equipment modifications to
prevent WRMSD in DMS. The protocol for this portion of the research was approved by the
Institutional Review Board.
Design
This descriptive research project was conducted over a period of five months. Direct
measurements of the following variables were collected:
Independent- Height of the DMS, Dimension of the ultrasound machine, Exam table heights,
and RULA scores for common ultrasound exams. (See attached images and sample RULA
worksheet in Appendix B).
Oependent- VAS pain scores taken before and after each work shift. (See attached VAS pain
scale in Appendix C).
The Rapid Upper Limb Assessment tool (RULA) was used to score the posture and position of
the DMS, for each scan. The RULA provides the opportunity to gather data and compute both a
sub-score and a total score for each subject evaluated. Sub-scores are computed for the
14

following parts of the worker's body: upper arm position, lower arm position, wrist position, wrist
twist, neck position, trunk position, legs, and muscle and force/load scores for both the upper
and lower limbs. The values for these sub-scores are referenced to a chart and combined to
form scores for the arm and wrist position and the neck, trunk, and leg position. These two
scores are again referenced in another chart and combined to form an overall RULA score for
the exam. Referencing the RULA, an acceptable score for an exam is a 1 or a 2, a score of a 3
or a 4 requires further investigation, a 5 or 6 should be further investigated and changed soon,
and a 7 should be investigated and changed immediately· The process of conducting a RULA
evaluation was rigorously practiced.
The visual analog scale (VAS) is a self-rated score provided to the DMS, allowing them indicate
their level of pain, at the beginning and the end of each work shift. Descriptive statistics were
used to analyze the data set. The DMS were asked to provide a VAS score at the beginning of
their work shift and at the end of their work shift, for each day that was evaluated. The VAS
scoring chart is rated from 0 to 10-0 being "no pain" and 10 being "agonizing." An
occupational therapist provided periodic checks for scoring to insure reliability of the data with
both the RULA and the VAS.
The height of each sonographer in centimeters was self-reported. The height of the exam table
that was selected by the sonographer for each individual exam was measured in centimeters by
the researcher. A height ratio was calculated by taking the exam table height and dividing it by
the sonographer height.
The RULA and VAS both have published reliability measures that make them the best choice
for this kind of data collection. The researcher received training on how to obtain data with
these instruments. The anticipated statistics are reported as both frequencies and means for
the group of 5 DMS. Although statistical power was not achieved due to a lower than
15

anticipated N, the hope had been to perform a statistical correlation to determine which of the
variables might be the most contributory to OMS's self-reported pain scores.
Variable Level of Measurement
RULA score (independent) Ordinal
OMS height (independent) Ratio
Table height (independent) Ratio
VAS score (dependent) Ordinal
Preliminary data was collected to determine feasibility of this project (See Appendix 0).
16

Chapter 3
Results
Work-related musculoskeletal disorders have been identified as a problem among Diagnostic
Medical Sonographers (OMS). The objective of this study was to obtain direct measures of OMS
in an attempt to find a comparison between their posture and position during each exam and their
level of pain for each day. A total of five OMS were involved in this study, and a total of twenty-
five scores were obtained during a variety of ultrasound examinations.
Descriptive Statistics
The most frequently observed ultrasound observed examinations, in this study, were a carotid
duplex, obstetrical ultrasound (OBITVS), and a lower extremity venous Doppler (Right, Left, or
Bilateral LEV). Table 1 includes mean RULA sub-scores and overall scores and is provided
below. A table of all the RULA scores for ultrasound examinations can be found in the appendix
(Appendix D).
Table 1. Mean RULA sub-scores and overall scores for frequently observed exams.
Expected Sub-score for Sub-score for Neck, Trunk, Overall Score ArmlWrist & Legs RULA Score
RLEV 1-2 4.33 2.33 3.33 BLEV 1-2 3.86 3.29 3.43 Carotid 1-2 4.00 4.17 . 4.50 OBITVS 1-2 3.83 4.83 4.83
The height of each OMS was collected and compared with the height of an adjustable
examination table used for the patient's ultrasound examination (Note: OMS 10 #5's exam table
was not adjustable). Table 2 includes the examination table heights, OMS height, and overall
RULA scores and is provided below:
17

Table 2. Comparison of the DMS heights, exam table heights, and RULA scores.
DMS Height Exam Table Height Height Ratio RULA Score (in cm) (in cm)
1 170 BLEV 94 1.81 3 BLEV 96 1.77 3 BLEV 90 1.89 3 LUEV 64 2.66 7
2 158 RLEV 64 2.47 3 BLEV 64 2.47 3
CAROTID 132 1.20 4 3 161 RLEV 76 2.12 3
BLEV 75 2.15 3 BLEV 72 2.24 3 BLEV 70 2.3 6
CAROTID 64 2.52 3 CAROTID 92 1.75 3
RUEV 72 2.24 3 4 173 RLEV 70 2.47 4
CAROTID 90 1.92 3 CAROTID 60 2.9 7 CAROTID 60 2.9 7
LUEV 70 2.47 5 5 175 OBITVS 81 2.16 3
OBITVS 81 2.16 5 OBITVS 81 2.16 7 OBITVS 81 2.16 4 OBITVS 81 2.16 4 OBITVS 81 2.16 6
The VAS scores for all the DMS are provided in Table 3.
Table 3. VAS scores taken daily among all DMS evaluated in the study.
Sonographer Exam Pre Score Post Score Difference
1 0 1 1
0 1 1
0 2 2
0 3 3
18

2 01/25/11 RLEV o o o o 1 1
3 2
1
3
3 02/19/11
3 03/10/11 4 4 02/15/11 CAROTID 0 0
4 02/18/11 CAROTID 0 3 3 4 02/25/11 RLEV 0 2 2
4 02/28/11 LUEV 0 0 0
4 03/01/11 CAROTID 0 2 2
5 04/05/11 OBITVS 2 4 2
5 04/07/11 OBITVS 2 4 2
5 04/08/11 OBITVS 2 4 2
A table is provided that lists some of the more frequently evaluated sonographic examinations and
the associated sub-scores, overall scores, and height ratios of the DMS.
Table 4. Most frequently evaluated sonographic exams and associated DMS data.
DMS Exam Location Trunk Score Leg Score RULA Height
19

Chapter 4
Discussion
The prevalence of work-related musculoskeletal disorders (WRMSD) among diagnostic medical
sonographers (DMS) and vascular technologists (VT) is increasing. A recent study reported a 9%
increase in the amount of sonographers scanning in pain, raising the total to 89% experiencing a
WRMSD B The challenging nature of obtaining a quality sonographic examination is responsible
for this high rate of injury; awkward posture, shoulder abduction, and bending and twisting of the
wrist are only a few contributing factors. The objective of this study was to obtain direct measures
of DMS in an attempt to find a comparison between their posture and position during each exam
and their level of pain for each day. The RULA tool and the VAS scale were used to score
scanning technique and rate the daily pain level. Unfortunately, none of the sample sonographers
achieved an acceptable score of 1 or 2 on the RULA. Therefore, this pilot study illuminates the
need for further investigation.
Oescriptive Statistics
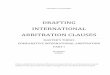
The obstetrical transvaginal (OBITVS) exam yielded the highest mean overall RULA score. This
exam requires using a long transducer with a handle and scanning transvaginally. Most
sonographers reach over the patient's leg in the stirrup causing the shoulder of the scanning hand
to abduct; the sonographer must then reach toward the machine with their free hand to work the
controls. The sonographer must angle the probe up, down, and side to side to get the proper
images causing bending and twisting of the hand and wrist. (See Fig.1)
20

Figure 1. Demonstration of scanning on a phantom, illustrating the angulation of the DMS wrist.
The carotid exam yielded the second highest mean overall RULA score. This exam requires
using a linear transducer with a footprint of approximately 3 to 4 centimeters. This small footprint
forces the sonographer to use a pinch grip to hold the transducer. Most sonographers stand on
the right side of the patient when scanning, so he or she must reach over the patient in order to
scan the left carotid artery. This places the shoulder of the scanning hand in abduction.
Sometimes sonographers have to reach so far to the side of the cart that it causes the DMS feet
to become unbalanced. The DMS tends to bend the trunk and twist the neck. (See Fig. 2)
Figure 2. Demonstration of carotid scanning, illustrating the unbalanced posture, bent trunk and
twisted neck.
The lower extremity venous (LEV) exams yielded the lowest mean overall RULA score, averaging
1-1 Y, points lower than the osrrvs and the carotid. The LEV exam requires the sonographer to
compress the vein to check for thrombus causing the sonographer to apply a lot of force and put
21

stress on the scanning arm. Like the carotid exam, the sonographer is forced to reach over the
patient to scan the left leg causing the same issues as mentioned above. (See Fig. 3)
Figure 3. An illustration of a sonographer pushing downward with the transducer, which causes a pinch grip.
Exams done portably at the patient's bedside consistently had a higher overall RULA score than
comparable exams done in the department, as all three portable exams evaluated scored a 6 or 7
on the RULA. Three exams done in the department also scored a 6 or a 7, but nineteen other
exams done in the department did not score as high. A study by Patel et al. evaluated the
efficiency of portable ultrasound examinations. Overall exam time for portable exams is 17.7
minutes longer than exams done in the department, exposing sonographers to prolonged
scanning'" Typically, portable patients are unstable and unable to travel to the department. These
examinations require a greater amount of physical work by the DMS. During a portable
examination, the DMS is required to push an ultrasound machine (>300 Ibs) from the department,
to the patient's bedside, and back. The Patel study also reported sub-optimal images obtained in
less-than-ideal environments. 9 While at the patient's bedside, the DMS is expected to work around
various medical equipment, which doesn't promote proper ergonomics during the ultrasound
scanning process.
22

A study by Pawaskar et al. compared the workflow and efficiency of conventional mobile
ultrasound scanners (full-size ultrasound machine on wheels) and the fairly new portable
ultrasound scanners (compact, lightweight, laptop-style ultrasound scanners). This study reported
that "portable testing represents 18% of the total volume of studies in large vascular labs."'° This
means that sonographers are exposed to less than ideal conditions that produce higher RULA
scores approximately one-fifth of the work shift. Researchers saw no significant difference in the
overall exam time required to perform a bedside exam with either machine. It may be beneficial
to look further into the ergonomic advantages, if any, of using laptop ultrasound equipment rather
than the larger versions. Patel et al. advocated the use of portable ultrasound scanners being
used to increase efficiency and reduce OMS exposure to WRMSO.
Bedside exams have been proven to decrease efficiency of ultrasound labs and have been
attributed to an increase in WRMSO. Reasons to avoid such exams include a performance trade
off, repetitive stress injuries, and the wear and tear of equipment. 9 These portable exams should
only be utilized when the patient is incapable of travel (i.e. a patient that is on a ventilator).
Anthropometric Data
The heights of sonographers were obtained along with the heights of exam tables selected for the
patient having a sonographic exam. The ratio of sonographer height to exam table height was
calculated, but no trends in the data could be visualized. Given this sample, however, it was
feasible to collect this information in the clinical site.
A 2009 study by Hill et al. gathered anthropometric data as well as the prevalence of WRMSO.
They reported that "larger" females "may be protected against the development of overuse
syndromes of the shoulder, low back, and hand/wrist," while also suggesting that larger hand size
may also be protective?
23

Visual Analog Scale
The VAS tool provided a means of self-reported pain scores from the sonographers. Many exams
scoring high on the RULA also showed an increase in the pre and post VAS scores. This could
suggest that exams yielding high RULA scores could contribute to a increase in pain levels.
Although, the pilot data obtained could indicate that a high score on RULA could contribute to a
painful day for the sonographer, more data is needed in order to determine if the association does
exist.
The Evans et al. study demonstrated no significant difference in the experience of pain from
different age groups. Most sonographers described their pain as "aching" in their study.6
Additional work reported by Evans analyzed pain in the wrist, hand, and fingers specificaliy. The
researchers reported that sonographers experiencing wrist, hand, or finger pain had "similar
descriptions of symptoms regardless of the area of practice or years of experience.,,11
A major problem is that most injuries go either unreported or underreported; forty-three percent of
respondents in the Evans study related their pain to their occupation, but only twenty-six percent
put in a formal report. " When pain is allowed to go unrecognized it is more likely to progress to an
even more serious injury. Again, an indirect report is valuable, but has increased credibility when
compared to direct measures of sonographers in the workplace.
24

Limitations
The main limitation of this study is attributed to the fact that data was obtained during the student
researcher's clinical rotation. The student researcher had other obligations to complete during the
rotation in addition to data collection for this study so she was unable to follow each sonographer
through the entire workday to better determine which exams contributed most to their level of
pain. The student researcher was scanning patients as well, so the patient workload was less
than that of a regular workday for the sonographer, possibly skewing the VAS scores. It could be
expected that the VAS scores would be higher if the sonographer had taken on the full patient
workload.
The VAS was taken at the beginning and at the end of the workday instead of the beginning and
the end of each exam, so it cannot be implied that a single exam score contributed to a certain
level of pain. It is difficult to say how reliable the VAS tool itself is, because it involves self
reported pain levels; however, the face to face self-reporting obtained in this study is thought to be
more accurate than that of online submissions to report pain utilized in past research.
This study had an N of only 5 DMS, and only 25 ultrasound exams evaluated in total. The N was
too low to make any statistically significant conclusions. Sonographers from only two facilities
were used, and only eight different exams were evaluated. The clinical examinations were
evaluated based on the prevalence for certain types of examination that were requested of these
laboratories. The data reported represents only those DMS observed for those examinations
preformed in these specific clinical sites. This data is only representative of these workers in the
context of these examinations.
If the proper time and resources were available, a more controlled study could be completed. The
student researcher could have repeatedly followed several sonographers for entire work shifts
25

until a statistically significant number of exams were evaluated. Sonographers from a variety of
scanning environments should be recruited (i.e. various vascular labs, obstetrical settings, and
radiology departments). A greater variety of exams should be evaluated in addition to those
included for this study, such as abdominal exams, renal exams, thyroid exams, and arterial
exams.
During each shift, every exam ordered should be evaluated. VAS scores should be recorded
before and after each exam as well as an overall VAS score at the beginning and end of each
work shift. If this were done, each RULA score and VAS score could be compared with each
other, and a correlation of problematic exams could possibly be made. The pushing and the
pulling of the ultrasound machine to and from the patient's bedside on portable exams would have
been included in the evaluation. A two person team of evaluators would have been utilized, and
the RULA scores would have been averaged to acquire a more accurate score.
Conclusions
This pilot study has objectively measured some of possible factors that contribute to WRMSD that
have been subjectively reported through past research. WRMSD among DMS and vascular
technologists are a serious issue that requires direct evaluation. The methods used in this pilot
study have been proven feasible; Future research that is executed on a larger scale may help to
truly pinpoint the risks related to WRMSD among sonographers.
26

References
1. SDMS speaks out for sonographers at OSHA hearings on ergonomic injury rules. 2000-2001. http://www.sdms.org/msilosha.asp.
2. Evans KD, Roll SC, Baker J: Work-related musculoskeletal disorders (WRMSD) among registered diagnostic medical sonographers and vascular technologists: a representative sample. J Diagn Med Sonography 2009; 25:287-299.
3. Evans KD, Roll SC, Li X, Sammet S: A holistic evaluation of risk factors for work-related musculoskeletal disorders among asymptomatic sonographers performing neurosonology. J Diagn Med Sonography 2009.
4. Brown G, Fhgi A, Baker J: Work-related musculoskeletal disorders in sonographers. J Diagn Med Sonography 2004; 20:85-93.
5. David S: Importance of sonographers reporting work-related musculoskeletal injury: a qualitative view. J Diagn Med Sonography 2005; 21 :234-237.
6. Muir M, Hrynkow P,. Chase R, Boyce D, McLean D: The nature, cause, and extent of occupational musculoskeletal injuries among sonographers: recommendations for treatment and prevention. J Diagn Med Sonography 2004; 20:317-325.
7. Hill JJ, Slade MD, Russi MB: Anthropometric measurements, job strain, and prevalence of musculoskeletal symptoms in female medical sonographers. Work 2009; 33:181-189.
8. McAtamney C, Corlett N: RULA: rapid upper limb assessment tool. http://www.rula.co.uk/brief.html. Accessed March 2, 2010.
9. Patel D, Satiani B, Mong R, Baetz L, Spiezio K: Appropriate resource utilization in portable noninvasive vascular studies: the role of disruptive technology. J Vasc Ultrasound 2006; 30(1):35-38.
10. Pawaskar M, Balkrishnan R, Kiser D, Gray M, Satiani B: Work flow analysis: evaluation of conventional mobile versus portable ultrasound scanners in the noninvasive vascular laboratory. J Vasc Ultrasound 2008; 32(2):85-88.
11. Evans KE, Roll SC, Hutmire C, Baker JP: Factors that contribute to wrist-hand-finger discomfort in diagnostic medical sonographers and vascular technologists. J Diag Med Sonographer 2010.
27

Appendix A. Ultrasound equipment in the clinical sites.
Zonare
Length: 76 em Width: 60 em Cord Length: 404 em Height (lowest): 80 em Height (highest): 99 em
28

Length: 107 em
Philips HD 11
Height: 56em Cord Length: 337.5em
29

Length: 87 em
GE Logiq 9
Height: 61 em Cord Length: 332.5 em
30

Appendix B. Rapid Upper Limb Assessment tool
Client:
Right Side:
E .:e
RAPID UPPER LIMB ASSESSMENT
Date/time:
100"+
Assessor:
o Working across the
midline of the body or out
tothe side
==9')) ~ ~~1 bent'lway from midH..,e
SELECT ONLY ONE OF THESE: v
'" ~ .E o No resistance ~ less than 2kg intermittent load or force TI TI . ~ 'l
'" ~ o 2-lOkg intermittent load or force
~ ~
"
D Shoulder is raised
D Upper arm is abducted
D Leaning or supporting
the weight of the arm
o Wrist is bent away
from midline
~ o 2-lOkg static load' 2-lOkg repeated loads or forces + lOkg or more intermittent load or force
Muscle Use
Left Side:
E .:e
o Posture is mainly static, e.g. held for longer than 1 minute or repeated more than 4 times per minute
4S"-90"
o Working across the
midline of the body or out
to the side
o Shoulder is raised
o Upper arm is abducted
o Leaning or supporting
the weight of the arm
31

Muscle Use
~ u . Z
] ~ u . Z
fj . .8
~ .. " ~ 3 ~
" :e . ." " oc
"
SELECT ONLY ONE OF THESE:
o No resistance + less than 2kg intermittent load or force
o 2-10kg intermittent load or force
o Wrist is bent away
from midline
o 2-10kg static load. 2-lOkg repeated loads or forces· lOkg or more intermittent load or force
o Posture is mainly static, e.g. held for longer than 1 minute or repeated more than 4 times per minute
I!"___... ..... 20·
-'" '~.'.".'.".".".'." ••.. ' .•. ' .. " .•.. ' .. '.' ()~
© 2001
till" ..
)1
32

, ,
t ,
" (l \'1
~ ~
Force & Load forthe neck, trunk
and legs
Muscle Use
~ '(;
Legs and feet are well Legs and feet are
supported and in an NOT evenly balanced and
evenly balanced posture.
v (". supported.
SELECT ONLY ONE OF THESE:
o No resistance. less than 2kg intermittent load Of force
o 2-10kg intermittent load or force
o 2-1Qkg static load· 2-10kg repeated loads or forces. lOkg or more intermittent load or force
o lOkg static load' lOkg repeated loads or forces • Shock or forces with rapid buildup
o Posture is mainly static, e.g. held for longer than 1 minute or repeated more than 4 times per minute
Whilst COPE Occupational Health and Ergonomic Services Ltd (COPE) and Osmond Group Limited (Osmond) have taken every care in preparing this resource, it must be used according to the guidelines based on the original article~ by Prof E.N. Corlett and Dr L. McAtamney.
No responsjbility will be taken by COPE or Osmond in the use of this resource.
RULA provides a score of a snapshot of the activity as part of a rapid screening tool. The user should refer to the original article* to check the detail of the scoring and correct use of RULA scores. Further investigation and actions may be required.
For further information on methodology, please refer to our on-line guidance at www.ergonomics.co.uk or: McAtamney, Land Conel!. EN. Reducing the risks of work related upper limb disorders - A guide and methods. Published by: Institute for Occupational Ergonomics, University of Nottingham, Nottingham NG7 2RD, UK. (1992). Tel: +44 (0)115 9514005 for details
*McAtamney, L. and Corlett, EN. "RULA -: A survey method for investigation of work-related upper limb disorders Applied Ergonomics 1993, 24(2), 91-99
Appendix C. The Visual Analog Pain Scale
!?' -?y .!f!
~@ c:: ,g (j '< :t'
Unbearable Distress
Task
;S § &
r:'f
.!f! til
1::: </2
! §
'" .f;; if '" ff §
'< <:
No Distress
Date ______ Start ___ End __ _
Osmond® Ergonomic Office Solutions
33

Appendix D. RULA Assessment Data
Appendix E. Pilot data collected for Drs. Sommerich and Evans in one clinical site.
Pelvis-Transabdominal
Sonographer A (65 inches)
• Table height: 26 inches, 66 em
• Thigh height to sonographer
• Sat while scanning
• Chair height: 26 in, 66 em
Sonographer B (63.5 in)
• Table height: 27 in, 68.5 em
• Thigh height
• Sat while scanning
• Chair height: 26 in, 66 em
Pelvis-Transvaginal
Sonographer A
• Table height: 30 in, 76.2 em
• Hip height to sonographer
34

• Sat while scanning
• Chair height: 26 in, 66 em
• Rests elbow on foot stool with handle
• Stool handle height: 35 in, 89 em
Sonographer B
• Table height: 31 in, 78.5 em
• Hip height to sonographer
• Stood while scanning
RUQ
Sonographer A
• Table height: 26 in, 66 em
• Thigh height to sonographer
• Sat while scanning
• Chair height: 26 in, 66 em
Thyroid
Sonographer C (63 in)
• Table height: 26 in, 66 em
• Thigh height to sonographer
• Sat while scanning
• Chair height: 20.5 in, 52 em
Lower Extremity
Sonographer D (70 in)
• Table height: 28.5 in, 72 em
35

• Sat while scanning
Lower Extremity (portable)
Sonographer D
• Table height: 36.5 in, 92 cm
• Stood while scanning
36
![NICU Database Appendices - CPQCC NICU Appendices.pdf2020 NICU Appendices| 4 1101 [K. oxytoca, K. pneumoniae and others] including Carbapenem-resistant Klebsiella and Cephalosporin-resistant](https://img.pdfslide.us/doc/110x75/5f0e96fb7e708231d43ff847/nicu-database-appendices-cpqcc-nicu-2020-nicu-appendices-4-1101-k-oxytoca.jpg)