Embed Size (px)
Citation preview
TECHNICAL NOTE
Direct electrical stimulation of the optic radiation in patientswith covered eyes
Andrej Šteňo & Vladimír Hollý & Martin Fabian &
Matúš Kuniak & Gabriela Timárová & Juraj Šteňo
Received: 8 February 2014 /Accepted: 9 February 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Direct electrical stimulation (DES) of the opticradiation (OR) during an awake tumor resection has beenrepeatedly reported. In all cases, visual function monitoringwas performed in patients with open eyes which were lookingat a picture. We report a new modification of the standardmethod, OR stimulation in patient with closed and coveredeyes. To the best of our knowledge, this method was notpresented before. According to our first experience, this meth-odology may be in some cases a potentially more sensitiveform of neuromonitoring than the OR stimulation in patientswith open eyes, as the phosphenes elicited by DES may bemore distinct in patients with covered eyes. The technique isdiscussed, and a literature review on intraoperative identifica-tion of the OR is presented as well. However, a future pro-spective study is needed to confirm the relevance of ourfinding.
Keywords Low-grade glioma . Awake resection . Opticradiation . Direct electrical stimulation . Intraoperativeultrasound
Introduction
Optic radiation (OR) stimulation during awake resection ofbrain tumors has been repeatedly reported; however, the dataare still sparse [2, 8, 10, 21]. In all cases, visual functionmonitoring was performed in patients with open eyes whichwere looking at a picture. We report a new modification of thestandard method, OR stimulation in patient with closed andcovered eyes. According to our first experience, this method-ology may be in some cases a potentially more sensitive formof neuromonitoring than the OR stimulation in patients withopen eyes.
Illustrative clinical report
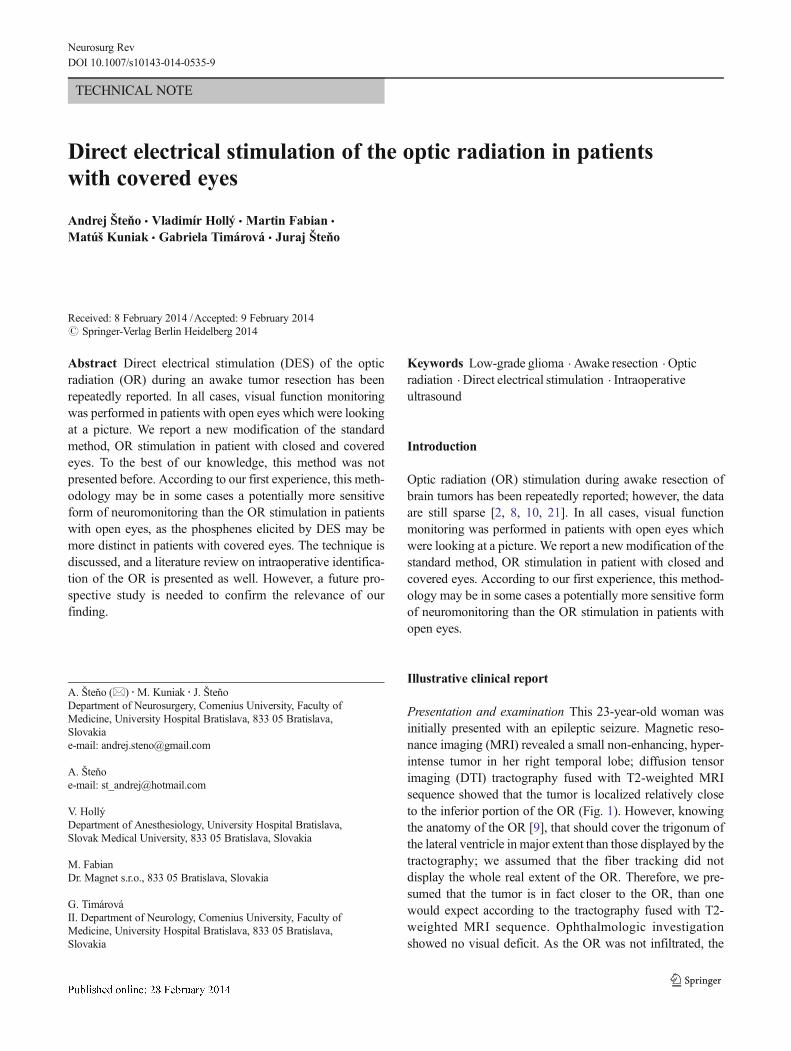
Presentation and examination This 23-year-old woman wasinitially presented with an epileptic seizure. Magnetic reso-nance imaging (MRI) revealed a small non-enhancing, hyper-intense tumor in her right temporal lobe; diffusion tensorimaging (DTI) tractography fused with T2-weighted MRIsequence showed that the tumor is localized relatively closeto the inferior portion of the OR (Fig. 1). However, knowingthe anatomy of the OR [9], that should cover the trigonum ofthe lateral ventricle in major extent than those displayed by thetractography; we assumed that the fiber tracking did notdisplay the whole real extent of the OR. Therefore, we pre-sumed that the tumor is in fact closer to the OR, than onewould expect according to the tractography fused with T2-weighted MRI sequence. Ophthalmologic investigationshowed no visual deficit. As the OR was not infiltrated, the
A. Šteňo (*) :M. Kuniak : J. ŠteňoDepartment of Neurosurgery, Comenius University, Faculty ofMedicine, University Hospital Bratislava, 833 05 Bratislava,Slovakiae-mail: [email protected]
A. Šteňoe-mail: [email protected]
V. HollýDepartment of Anesthesiology, University Hospital Bratislava,Slovak Medical University, 833 05 Bratislava, Slovakia
M. FabianDr. Magnet s.r.o., 833 05 Bratislava, Slovakia
G. TimárováII. Department of Neurology, Comenius University, Faculty ofMedicine, University Hospital Bratislava, 833 05 Bratislava,Slovakia
Neurosurg RevDOI 10.1007/s10143-014-0535-9
planned surgical result was gross total tumor removal withoutany postoperative visual disturbance. To make the surgery assafe as possible, an awake resection with intraoperative visualfunctions monitoring was performed.
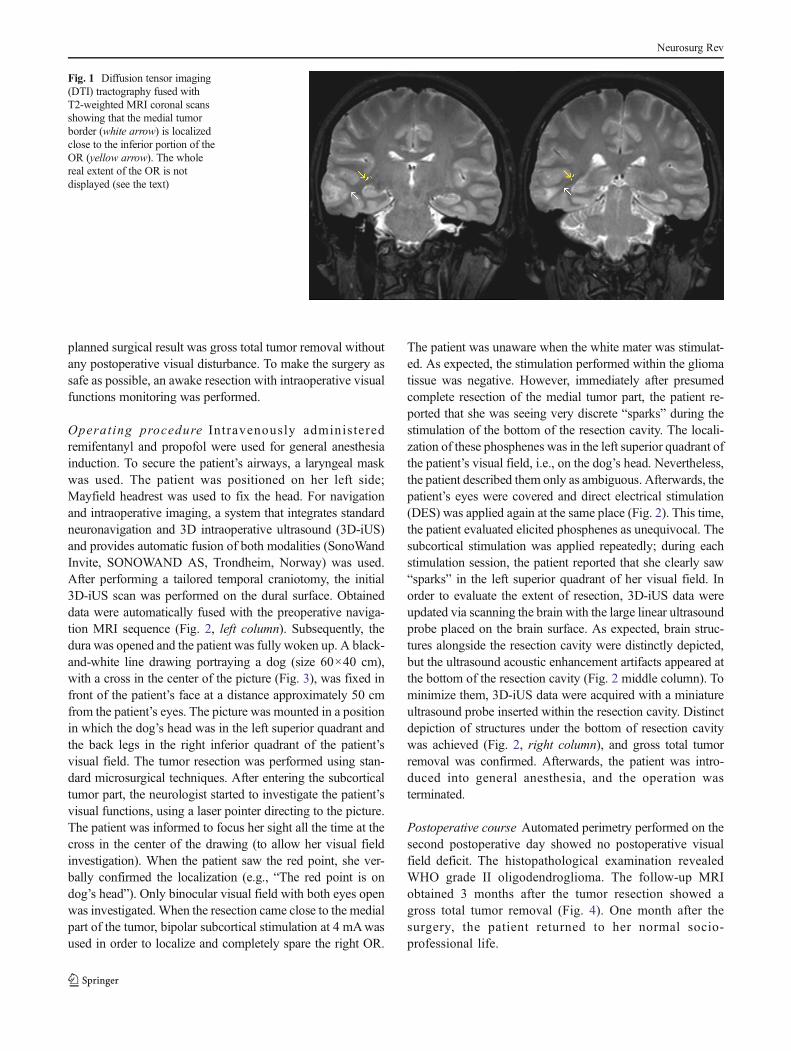
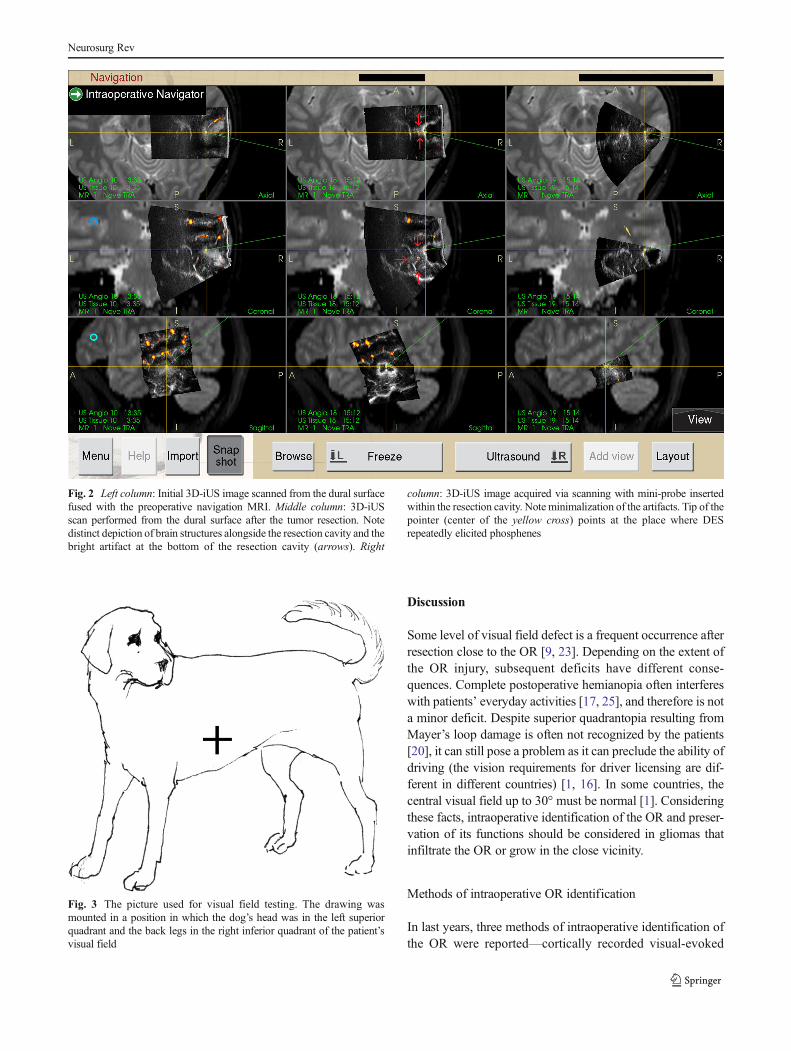
Operating procedure Intravenously administeredremifentanyl and propofol were used for general anesthesiainduction. To secure the patient’s airways, a laryngeal maskwas used. The patient was positioned on her left side;Mayfield headrest was used to fix the head. For navigationand intraoperative imaging, a system that integrates standardneuronavigation and 3D intraoperative ultrasound (3D-iUS)and provides automatic fusion of both modalities (SonoWandInvite, SONOWAND AS, Trondheim, Norway) was used.After performing a tailored temporal craniotomy, the initial3D-iUS scan was performed on the dural surface. Obtaineddata were automatically fused with the preoperative naviga-tion MRI sequence (Fig. 2, left column). Subsequently, thedura was opened and the patient was fully woken up. A black-and-white line drawing portraying a dog (size 60×40 cm),with a cross in the center of the picture (Fig. 3), was fixed infront of the patient’s face at a distance approximately 50 cmfrom the patient’s eyes. The picture was mounted in a positionin which the dog’s head was in the left superior quadrant andthe back legs in the right inferior quadrant of the patient’svisual field. The tumor resection was performed using stan-dard microsurgical techniques. After entering the subcorticaltumor part, the neurologist started to investigate the patient’svisual functions, using a laser pointer directing to the picture.The patient was informed to focus her sight all the time at thecross in the center of the drawing (to allow her visual fieldinvestigation). When the patient saw the red point, she ver-bally confirmed the localization (e.g., “The red point is ondog’s head”). Only binocular visual field with both eyes openwas investigated. When the resection came close to the medialpart of the tumor, bipolar subcortical stimulation at 4 mAwasused in order to localize and completely spare the right OR.
The patient was unaware when the white mater was stimulat-ed. As expected, the stimulation performed within the gliomatissue was negative. However, immediately after presumedcomplete resection of the medial tumor part, the patient re-ported that she was seeing very discrete “sparks” during thestimulation of the bottom of the resection cavity. The locali-zation of these phosphenes was in the left superior quadrant ofthe patient’s visual field, i.e., on the dog’s head. Nevertheless,the patient described them only as ambiguous. Afterwards, thepatient’s eyes were covered and direct electrical stimulation(DES) was applied again at the same place (Fig. 2). This time,the patient evaluated elicited phosphenes as unequivocal. Thesubcortical stimulation was applied repeatedly; during eachstimulation session, the patient reported that she clearly saw“sparks” in the left superior quadrant of her visual field. Inorder to evaluate the extent of resection, 3D-iUS data wereupdated via scanning the brain with the large linear ultrasoundprobe placed on the brain surface. As expected, brain struc-tures alongside the resection cavity were distinctly depicted,but the ultrasound acoustic enhancement artifacts appeared atthe bottom of the resection cavity (Fig. 2 middle column). Tominimize them, 3D-iUS data were acquired with a miniatureultrasound probe inserted within the resection cavity. Distinctdepiction of structures under the bottom of resection cavitywas achieved (Fig. 2, right column), and gross total tumorremoval was confirmed. Afterwards, the patient was intro-duced into general anesthesia, and the operation wasterminated.
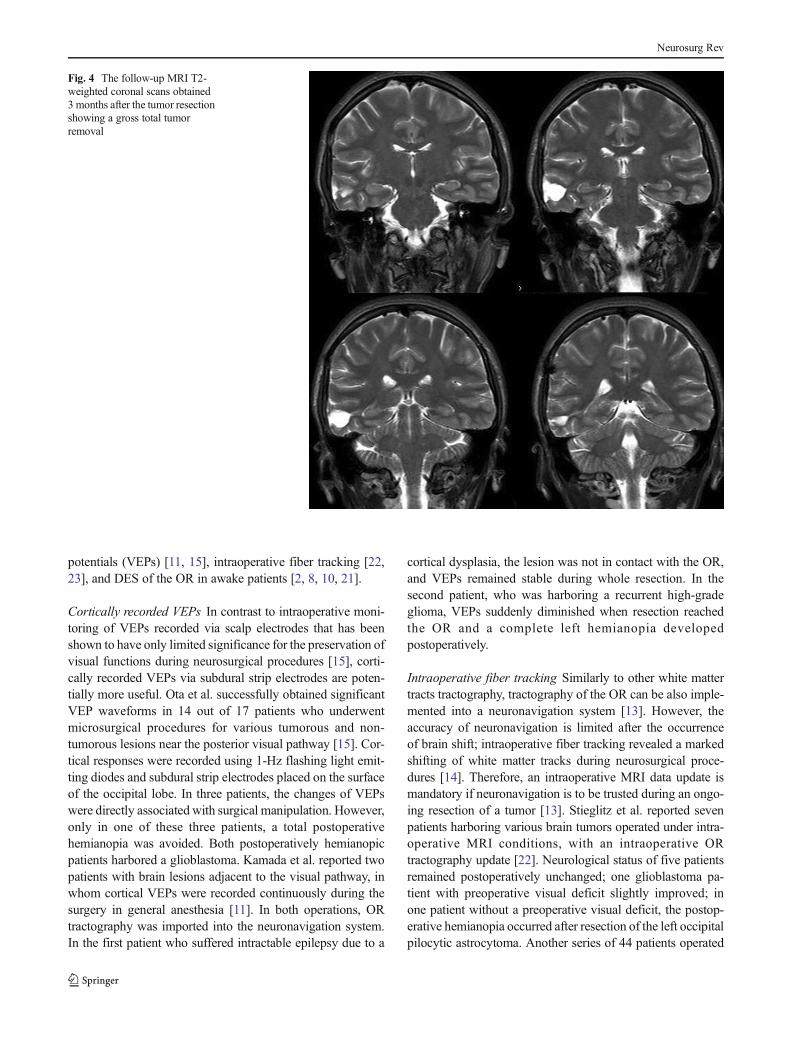
Postoperative course Automated perimetry performed on thesecond postoperative day showed no postoperative visualfield deficit. The histopathological examination revealedWHO grade II oligodendroglioma. The follow-up MRIobtained 3 months after the tumor resection showed agross total tumor removal (Fig. 4). One month after thesurgery, the patient returned to her normal socio-professional life.
Fig. 1 Diffusion tensor imaging(DTI) tractography fused withT2-weighted MRI coronal scansshowing that the medial tumorborder (white arrow) is localizedclose to the inferior portion of theOR (yellow arrow). The wholereal extent of the OR is notdisplayed (see the text)
Neurosurg Rev
Discussion
Some level of visual field defect is a frequent occurrence afterresection close to the OR [9, 23]. Depending on the extent ofthe OR injury, subsequent deficits have different conse-quences. Complete postoperative hemianopia often interfereswith patients’ everyday activities [17, 25], and therefore is nota minor deficit. Despite superior quadrantopia resulting fromMayer’s loop damage is often not recognized by the patients[20], it can still pose a problem as it can preclude the ability ofdriving (the vision requirements for driver licensing are dif-ferent in different countries) [1, 16]. In some countries, thecentral visual field up to 30° must be normal [1]. Consideringthese facts, intraoperative identification of the OR and preser-vation of its functions should be considered in gliomas thatinfiltrate the OR or grow in the close vicinity.
Methods of intraoperative OR identification
In last years, three methods of intraoperative identification ofthe OR were reported—cortically recorded visual-evoked
Fig. 2 Left column: Initial 3D-iUS image scanned from the dural surfacefused with the preoperative navigation MRI. Middle column: 3D-iUSscan performed from the dural surface after the tumor resection. Notedistinct depiction of brain structures alongside the resection cavity and thebright artifact at the bottom of the resection cavity (arrows). Right
column: 3D-iUS image acquired via scanning with mini-probe insertedwithin the resection cavity. Note minimalization of the artifacts. Tip of thepointer (center of the yellow cross) points at the place where DESrepeatedly elicited phosphenes
Fig. 3 The picture used for visual field testing. The drawing wasmounted in a position in which the dog’s head was in the left superiorquadrant and the back legs in the right inferior quadrant of the patient’svisual field
Neurosurg Rev
potentials (VEPs) [11, 15], intraoperative fiber tracking [22,23], and DES of the OR in awake patients [2, 8, 10, 21].
Cortically recorded VEPs In contrast to intraoperative moni-toring of VEPs recorded via scalp electrodes that has beenshown to have only limited significance for the preservation ofvisual functions during neurosurgical procedures [15], corti-cally recorded VEPs via subdural strip electrodes are poten-tially more useful. Ota et al. successfully obtained significantVEP waveforms in 14 out of 17 patients who underwentmicrosurgical procedures for various tumorous and non-tumorous lesions near the posterior visual pathway [15]. Cor-tical responses were recorded using 1-Hz flashing light emit-ting diodes and subdural strip electrodes placed on the surfaceof the occipital lobe. In three patients, the changes of VEPswere directly associated with surgical manipulation. However,only in one of these three patients, a total postoperativehemianopia was avoided. Both postoperatively hemianopicpatients harbored a glioblastoma. Kamada et al. reported twopatients with brain lesions adjacent to the visual pathway, inwhom cortical VEPs were recorded continuously during thesurgery in general anesthesia [11]. In both operations, ORtractography was imported into the neuronavigation system.In the first patient who suffered intractable epilepsy due to a
cortical dysplasia, the lesion was not in contact with the OR,and VEPs remained stable during whole resection. In thesecond patient, who was harboring a recurrent high-gradeglioma, VEPs suddenly diminished when resection reachedthe OR and a complete left hemianopia developedpostoperatively.
Intraoperative fiber tracking Similarly to other white mattertracts tractography, tractography of the OR can be also imple-mented into a neuronavigation system [13]. However, theaccuracy of neuronavigation is limited after the occurrenceof brain shift; intraoperative fiber tracking revealed a markedshifting of white matter tracks during neurosurgical proce-dures [14]. Therefore, an intraoperative MRI data update ismandatory if neuronavigation is to be trusted during an ongo-ing resection of a tumor [13]. Stieglitz et al. reported sevenpatients harboring various brain tumors operated under intra-operative MRI conditions, with an intraoperative ORtractography update [22]. Neurological status of five patientsremained postoperatively unchanged; one glioblastoma pa-tient with preoperative visual deficit slightly improved; inone patient without a preoperative visual deficit, the postop-erative hemianopia occurred after resection of the left occipitalpilocytic astrocytoma. Another series of 44 patients operated
Fig. 4 The follow-up MRI T2-weighted coronal scans obtained3 months after the tumor resectionshowing a gross total tumorremoval
Neurosurg Rev

with iMRI-updated OR tractography was presented by Sunet al. [23]:36 patients harbored a glioma, 6 patients hadcavernous or arteriovenous malformation, and 2 patients hada metastatic brain lesion. Thirteen patients had the lesion indirect contact with the OR; in 31 cases, the OR was in thedistance of several millimeters (0.9–14). Five patients im-proved after the lesion resection: four of them harbored aglioma and one patient had a cavernous malformation. In threecases, a homonymous hemianopia developed postoperatively;however two of these three patients were not intact preopera-tively—they had a preoperative quadrantopia; all three post-operatively hemianopic patients harbored a glioma. Neurolog-ical status of all other patients remained unchanged after thesurgery.
DES of the OR in awake patients Subcortical stimulation ofthe OR in an awake patient was first time published by Duffauet al. [8]. The resected lesion was a low-grade glioma; the ORconstituted the posterior and deep functional boundary of theresection. The identification of the OR helped the surgeon toavoid the complication of a postoperative hemianopia in spiteof an asymptomatic quadrantopia. Another patient in whomthe OR was intraoperatively localized by DES during anawake tumor resection was reported by us [21]. The patientwas harboring a temporal low-grade glioma which infiltratedthe right OR. A total of 97 % resection was achieved; a smalltumor portion involving the ORwas intentionally left in place.Functional result was partial quadrantanopia instead of moreprofound visual deficit, which would follow gross-total resec-tion. The first series of 14 patients in whom an intraoperativesubcortical stimulation of the OR was performed during anawake surgery was presented by Gras-Combe et al. [10]. Allpatients suffered a glioma involving the OR; no patient hadpreoperative visual deficit. One patient remained unchangedafter the surgery, and one had a postoperative permanenthemianopia. All other patients had a postoperativequadrantopia. The authors concluded that subcortical ORstimulation is an effective and reliable method, allowingavoidance of permanent postoperative hemianopia. Chan-Seng et al. [2] recently presented DES of the OR in fivepatients; in all of them, hemianopia was avoided and thefunctional result was superior quadrantopia. Mapping of vi-sual functions in awake patients without stating whether visualcortex or visual pathwayswere stimulatedwas documented bySerletis and Bernstein [18] and by Shinoura et al. [19]; DES ofvisual cortex during an awake tumor resection was publishedby Danks et al. [3] and Nguyen et al. [12].
Because of limited amount of data, the comparison ofeffectiveness of aforementioned methods of intraoperativeOR identification is problematic. Differences between pre-sented series make the evaluation even more challenging.For example, in the series presented by Chan-Seng et al. [2]and Gras-Combe al. [10], all gliomas involved the OR, while
in the series presented by Sun et al. [23], the lesions were notin direct contact with the OR in majority of patients (31 out of44). In the series published by Ota et al., only three patientshad changes in VEPs that was directly associated with surgicalmanipulation [15]. This implies that only in minority of pre-sented cases, the OR was infiltrated by the tumor (the infor-mation about tumor border to OR distance was lacking in thepaper; the authors defined the location of the lesions as “nearOR”). While in some series, non-tumorous and tumorous(low- and high-grade) lesions were included [11, 15, 22, 23];other authors included only patients with gliomas [2, 10].Therefore, a responsible evaluation and comparison of effec-tiveness of different methods is not possible at the moment,and further studies are needed. However, two facts can bestated. Firstly, despite small number of patients included, nomethod was able to avoid the permanent hemianopia in allcases. Secondly, both intraoperatively updated ORtractography and subcortical OR stimulation in awake patientenabled the prevention of permanent hemianopia in majorityof patients with infiltrated OR or with the tumor growing inclose vicinity of the OR.
Presented case
In all previously published papers [2, 8, 10, 21], DES of theOR was always performed in patients looking at a picture.This methodology was also used in our previously presentedpatient in whom we were not able to preserve whole visualfield, despite we left in place a small piece of tumor thatinfiltrated her OR; the functional result was incomplete hom-onymous quadrantopia (unrecognized by the patient). Weconcluded that the reason for the deficit was late use of DES(after the opening of the lateral ventricle) after the OR hadalready been interrupted.
In present patient, considering the small size of the tumorand the fact that the ORwas not infiltrated, the only acceptablepostoperative result was gross total removal and no permanentvisual deficit. In order to achieve our goal, we started tostimulate the tissue early after beginning of subcortical resec-tion. As no visual (or any other eloquent) cortex was ap-proachable for DES, the standard procedure of the currentintensity setting (i.e., progressive increasing of the currentamplitude until a functional response is elicited) was notpossible. Therefore, we selected the current intensity accord-ing to the data published by Gras-Combe et al., who stimulat-ed the OR at the current intensity level of 4 mA in a patientwith no postoperative visual field deficit [10], and accordingto our own previous experience with a successful OR stimu-lation at 4 mA [21]. The tumor resection was stopped imme-diately after the patient reported the occurrence of very dis-crete phosphenes. However, after the patient closed her eyes(which we completely covered with a woven surgical drape),repeated DES at the same place at the bottom of the resection
Neurosurg Rev

cavity elicited phosphenes so unambiguously that we weresure that we really stimulated a part of the OR. As the 3D-iUSre-scan confirmed gross total removal, we terminated theresection. We hypothesize two reasons why the phospheneswere more distinct when DESwas applied during the patient’seyes were closed. First, the picture we used for visual func-tions testing was a black-and-white drawing, with majority ofthe image area being in fact white. It seems logical that thepatient could have problems to “see” bright phosphenes on awhite area. Interestingly, other authors [10, 12] also usedpictures with majority of the image area being white. Inaddition, we presume that the daylight itself could cause thatthe elicited phosphenes were less contrast, i.e., less distinct.Second, as the important condition of intraoperative visualfield investigation in patient with opened eyes is staring at thecross in the image center, it is natural that lack of her concen-tration could probably also influence the result (similarly, aspatient’s fatigue can negatively influence the result of intra-operative speech and language function testing) [5]. Indeed,we had to repeatedly remind our patient that she must keepstaring at the cross in the image center.
On the other hand, we do not recommend to replace thestandard method of visual testing with opened eyes with thepresented methodology. In fact, we are convinced that there isan important reason for regular performance of standard test-ing with open eyes during every procedure: in the seriespresented by Gras-Combe et al., the most common symptomelicited by DER of the ORwas blurring of the vision [10]. It isvery questionable if these patients would have any symptomsif they would have closed eyes during the stimulation. There-fore, we recommend to use the stimulation with closed eyes asan adjunct to the standard methodology and not as a solemethod.
Optimization of so-called “onco-functional” balance, i.e.,balance between the extent of resection and preservation ofthe quality of the patient’s life [4, 7, 10], is an important issuethat has to be always taken into consideration during resectionof gliomas growing close to or within the visual structures [7,10]. Patients harboring a residual low-grade glioma smallerthan 10 cm3 have in general better prognosis than the patientswith less extensive resection [6]. Considering the fact thatquadrantopia (especially when incomplete) is not a majordeficit, it can be evaluated as an acceptable functional result,if resection with a significant impact on patient prognosiswould otherwise not be possible. In numerous cases,quadrantopic patients are allowed to drive cars [2, 7, 10].However, as in some countries, the rules for driver licensingdo not allow car driving in patients with completequadrantopia [1, 16]; it is necessary to discuss any voluntarilygenerated visual field deficit with the patient preoperatively.On the other hand, even hemianopia can be considered asacceptable in patients with occipital lobe involvement, inwhom a minor resection would not have a positive impact
on prognosis [24]. Nevertheless, in tumors which grow in theclose vicinity to the OR but do not infiltrate it, every effortshould be made not to cause an unnecessary postoperativevisual field deficit. We presume that our method can beparticularly beneficial in such patients.
Conclusions
DES of the OR in patients with closed eyes maybe in somecases a potentially more sensitive form of neuromonitoringthan the OR stimulation with in patients with open eyes. Tothe best of our knowledge, this method was not presentedbefore. A future prospective study is needed to confirm therelevance of our finding. As the phosphenes are not the onlypossible symptom elicited by DES of the OR and blurring ofthe vision could remain unnoticed, we recommend to use thestimulation with closed eyes as an adjunct to the standardmethodology and not as a sole method.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Bron AM, Viswanathan AC, Thelen U, de Natale R, Ferreras A,Gundgaard J, Schwartz G, Buchholz P (2010) International visionrequirements for driver licensing and disability pensions: using amilestone approach in characterization of progressive eye disease.Clin Ophthalmol 4:1361–1369. doi:10.2147/OPTH.S15359
2. Chan-Seng E,Moritz-Gasser S, Duffau H (2014) Awakemapping forlow-grade gliomas involving the left sagittal stratum:anatomofunctional and surgical considerations. J Neurosurg. Jan31. [Epub ahead of print]
3. Danks RA, Aglio LS, Gugino LD, Black PM (2000) Craniotomyunder local anesthesia and monitored conscious sedation for theresection of tumors involving eloquent cortex. J Neurooncol 49:131–139
4. Duffau H (2009) Surgery of low-grade gliomas: towards a ‘functionalneurooncology’. Curr Opin Oncol 21:543–549. doi:10.1097/CCO.0b013e3283305996
5. Duffau H, Capelle L, Denvil D, Sichez N, Gatignol P, Taillandier L,Lopes M, Mitchell MC, Roche S, Muller JC, Bitar A, Sichez JP, vanEffenterre R (2003) Usefulness of intraoperative electrical subcorticalmapping during surgery for low-grade gliomas located within elo-quent brain regions: functional results in a consecutive series of 103patients. J Neurosurg 98:764–778
6. Duffau H, Lopes M, Arthuis F, Bitar A, Sichez JP, Van Effenterre R,Capelle L (2005) Contribution of intraoperative electrical stimula-tions in surgery of low grade gliomas: a comparative study betweentwo series without (1985–96) and with (1996–2003) functional map-ping in the same institution. J Neurol Neurosurg Psychiatry 76:845–851
7. Duffau H, Mandonnet E (2013) The “onco-functional balance” insurgery for diffuse low-grade glioma: integrating the extent of resec-tion with quality of life. Acta Neurochir 155:951–957. doi:10.1007/s00701-013-1653-9
Neurosurg Rev

8. Duffau H, Velut S, Mitchell MC, Gatignol P, Capelle L (2004) Intra-operative mapping of the subcortical visual pathways using directelectrical stimulations. Acta Neurochir 146:265–269
9. Ebeling U, Reulen HJ (1988) Neurosurgical topography of the opticradiation in the temporal lobe. Acta Neurochir 92:29–36
10. Gras-Combe G, Moritz-Gasser S, Herbet G, Duffau H (2012)Intraoperative subcortical electrical mapping of optic radiations inawake surgery for glioma involving visual pathways. J Neurosurg117:466–473. doi:10.3171/2012.6.JNS111981
11. Kamada K, Todo T, Morita A, Masutani Y, Aoki S, Ino K, Kawai K,Kirino T (2005) Functional monitoring for visual pathway using real-time visual evoked potentials and optic-radiation tractography.Neurosurgery 57(1 Suppl):121–127
12. Nguyen HS, Sundaram SV, Mosier KM, Cohen-Gadol AA(2011) A method to map the visual cortex during an awakecraniotomy. J Neurosurg 114:922–926. doi:10.3171/2010.11.JNS101293
13. Nimsky C, Ganslandt O, Fahlbusch R (2006) Implementation offiber tract navigation. Neurosurgery 58(4 Suppl 2):ONS-292–ONS-303
14. Nimsky C, Ganslandt O, Hastreiter P, Wang R, Benner T, SorensenAG, Fahlbusch R (2005) Preoperative and intraoperative diffusiontensor imaging-based fiber tracking in glioma surgery. Neurosurgery56:130–137
15. Ota T, Kawai K, Kamada K, Kin T, Saito N (2010) Intraoperativemonitoring of cortically recorded visual response for posterior visualpathway. J Neurosurg 112:285–294. doi:10.3171/2009.6.JNS081272
16. Pathak-Ray V, Ray A, Walters R, Hatfield R (2002) Detection ofvisual field defects in patients after anterior temporal lobectomy formesial temporal sclerosis-establishing eligibility to drive. Eye (Lond)16:744–748
17. Romano JG (2009) Progress in rehabilitation of hemianopic visualfield defects. Cerebrovasc Dis 27(Suppl 1):187–190. doi:10.1159/000200458
18. Serletis D, Bernstein M (2007) Prospective study of awake craniot-omy used routinely and nonselectively for supratentorial tumors. JNeurosurg 107:1–6
19. Shinoura N, Suzuki Y, Yamada R, Tabei Y, Saito K, Yagi K (2010)Relationships between brain tumor and optic tract or calcarine fissureare involved in visual field deficits after surgery for brain tumor. ActaNeurochir 152:637–642. doi:10.1007/s00701-009-0582-0
20. Sincoff EH, Tan Y, Abdulrauf SI (2004)White matter fiber dissectionof the optic radiations of the temporal lobe and implications forsurgical approaches to the temporal horn. J Neurosurg 101:739–746
21. Šteňo A, KarlíkM,Mendel P,ČíkM, Šteňo J (2012) Navigated three-dimensional intraoperative ultrasound-guided awake resection oflow-grade glioma partially infiltrating optic radiation. ActaNeurochir 154:1255–1262. doi:10.1007/s00701-012-1357-6
22. Stieglitz LH, Lüdemann WO, Giordano M, Raabe A, Fahlbusch R,Samii M (2011) Optic radiation fiber tracking using anteriorlyangulated diffusion tensor imaging: a tested algorithm for quickapplication. Neurosurgery 68:1239–1251. doi:10.1227/NEU.0b013e31820b52e1
23. Sun GC, Chen XL, Zhao Y, Wang F, Hou BK, Wang YB, Song ZJ,Wang D, Xu BN (2011) Intraoperative high-field magnetic resonanceimaging combined with fiber tract neuronavigation-guided resectionof cerebral lesions involving optic radiation. Neurosurgery 69:1070–1084. doi:10.1227/NEU.0b013e3182274841
24. Viegas C, Moritz-Gasser S, Rigau V, Duffau H (2011) OccipitalWHO grade II gliomas: oncological, surgical and functional consid-erations. Acta Neurochir (Wien) 153:1907–1917. doi:10.1007/s00701-011-1125-z
25. WarrenM (2009) Pilot study on activities of daily living limitations inadults with hemianopsia. Am J Occup Ther 63:626–633
Comments
Hugues Duffau, Montpellier, FranceIn this report, Šteňo et al. describe the case of a 23-year-old woman
that underwent an awake surgery for a WHO grade II oligodendrogliomalocated in the posterior part of the right temporal lobe, near the opticradiation (OR). Using intraoperative subcortical direct electrical stimula-tion (DES), they were able to identify and preserve the visual pathwayswhile performing a gross-total resection of the tumor, as demonstrated onthe postsurgical MRI. Interestingly, during DES, although the patientdescribed ambiguous phosphenes with open eyes (she looked at a pic-ture), after the patient’s eyes were covered, the phosphenes elicited wereunequivocal. Therefore, the authors recommend to use DES with closedeyes as an adjunct to the standard method of visual testing with open eyes,in order to increase the sensitivity of OR mapping.
First of all, Šteňo and colleagues have to be congratulated for theirexcellent result. Indeed, by optimizing the technique of OR detection,they avoided postoperative visual field deficit and they removedcompletely the glioma. It is puzzling to note that mapping of visualpathways has received less attention in the neurosurgical literature. Yet,whereas quadrantanopia is usually not recognized by the patients,hemianopia may have serious consequence on the quality of life, espe-cially with regard to driving. Therefore, OR mapping should be moresystematically considered for tumor near or within optic pathways.
To this end, intraoperative imaging is definitely not reliable enough incomparison with DES. For example, using intraoperative MRI and fibertract neuronavigation, Sun et al. [5] generated three hemianopias in aseries of 13 patients (23%) who had a lesion in direct contact with the OR(31 patients in this experience had a lesion distant from the OR). It isworth noting that, using DES, Gras-Combes et al. [4] induced permanenthemianopia in only one case out of 14 diffuse gliomas involving the OR(7 %)—no hemianopia in Chan-Seng et al.’ series [1]. Nonetheless, asstated by Šteňo et al., DES does not allow to prevent hemianopia in 100%of cases, probably because OR mapping is based on the patient’s subjec-tivity (in contrast to other functions that can be mapped more objectively,as language or semantic processing [2]). As a consequence, the additionalmethod reported by Šteňo et al., which consists in performing DES of theOR not only with open eyes but also with closed eyes, might represent amore sensitive form of visual neuromonitoring which deserves to bevalidated in further series. On the other hand, the “closed eyes technique”cannot replace the standard testing with open eyes, which remains crucial,especially in the left dominant hemisphere to map language simulta-neously [1]—or even in the right hemisphere to test visual recognition[3]—due to the close proximity of the OR and inferior longitudinalfascicle/inferior fronto-occipital fascicle in the temporo-occipital junctionand sagittal stratum [1].
References1. Chan-Seng E,Moritz-Gasser S, Duffau H (2014) Awakemapping for
low-grade gliomas involving the left sagittal stratum: anatomofunctionaland surgical considerations. J Neurosurg. Jan 31. [Epub ahead of print]
2. Coello AF, Moritz-Gasser S, Martino J, Martinoni M, Matsuda R,Duffau H (2013) Selection of intraoperative tasks for awake mappingbased on relationships between tumor location and functional networks. JNeurosurg 119:1,380–94.
3. Coello AF, Duvaux S, De Benedictis A, Matsuda R, Duffau H(2013) Involvement of the right inferior longitudinal fascicle in visualhemiagnosia: a brain stimulation mapping study. J Neurosurg 118:202–5
4. Gras-Combe G, Moritz-Gasser S, Herbet G, Duffau H. Intraoper-ative subcortical electrical mapping of optic radiations in awake surgeryfor glioma involving visual pathways (2012) J Neurosurg 117:466–73.
5. Sun GC, Chen XL, Zhao Y, Wang F, Hou BK, Wang YB, Song ZJ,Wang D, Xu BN (2011) Intraoperative high-field magnetic resonanceimaging combined with fiber tract neuronavigation-guided resection ofcerebral lesions involving optic radiation. Neurosurgery 69:1,070–84.
Neurosurg Rev





























