Embed Size (px)
Citation preview

Lecture: Direct Primary Care ‐Direct Primary Care Terminology, Legal,
and Legisla ve Issues ‐DPC: In the Trenches‐ Pu ng the Joy Back into
Family Medicine Philip Eskew, DO, JD, MBA
Brian Forrest, MD

ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as necessary.
Name of CME Activity: ACOFP 52nd Annual Convention and Scientific Seminars
Dates and Location of CME Activity: March 12-15, 2015, The Cosmopolitan Las Vegas, Nevada Lecture: Direct Primary Care -Direct Primary Care Terminology, Legal, and Legislative Issues (Eskew) -DPC: In the Trenches- Putting the Joy Back into Family Medicine (Forrest) Saturday, March 14, 2015 3:00-4:00pm
Name of Faculty/Moderator: Brian Forrest, MD
DISCLOSURE OF FINANCIAL RELATIONSHIPS WITHIN 12 MONTHS OF DATE OF THIS FORM
A. Neither I nor any member of my immediate family has a financial relationship or interest with any proprietary entity producing
health care goods or services.
x B. I have, or an immediate family member has, a financial relationship or interest with a proprietary entity producing health care
goods or services. Please check the relationship(s) that applies.
Research Grants x Stock/Bond Holdings (excluding mutual funds)
Speakers’ Bureaus* x Employment
x Ownership Partnership
x Consultant for Fee Others, please list:
Please indicate the name(s) of the organization(s) with which you have a financial relationship or interest, and the specific clinical area(s) that correspond to the relationship(s). If more than four relationships, please list on separate piece of paper:
Organization With Which Relationship Exists Clinical Area Involved
1. Access Healthcare Direct Network-CEO 1. Practice Transformation to DPC Model
2. DPCMH.org /DPCMH Association-President 2. Not For Profit providing information and resources on DPC
3. Access Healthcare, P.A.-Practicing Physician 3. Owner and Employee at Practice 4. Get Healthy Inc-Chief Practice innovation Officer 5. Twin Oaks Software Development-Consultant 6. NCAFP/AAFP/multiple state chapters
4. DPC Health Care and Wellness Portal and Software 5. DPC Membership Management software 6. Expert Faculty/Speaker on DPC
*If you checked “Speakers’ Bureaus” in item B, please continue: • Did you participate in company-provided speaker training related to your proposed Topic? Yes: No: x • Did you travel to participate in this training? Yes: No: x • Did the company provide you with slides of the presentation in which you were trained as a speaker? Yes: No: x • Did the company pay the travel/lodging/other expenses? Yes: No:x • Did you receive an honorarium or consulting fee for participating in this training? Yes: No: x • Have you received any other type of compensation from the company? Please specify: Yes: No: x • When serving as faculty for ACOFP, will you use slides provided by a proprietary entity for your presentation
and/or lecture handout materials? Yes: No:x • Will your Topic1 involve information or data obtained from commercial speaker training? Yes: No: x
DISCLOSURE OF UNLABELED/INVESTIGATIONAL USES OF PRODUCTS
____x__A. The content of my material(s)/presentation(s) in this CME activity will not include discussion of unapproved or
investigational uses of products or devices.
______B. The content of my material(s)/presentation in this CME activity will include discussion of unapproved or investigational
uses of products or devices as indicated below:
I have read the ACOFP policy on full disclosure. If I have indicated a financial relationship or interest, I understand that this information will be reviewed to determine whether a conflict of interest may exist, and I may be asked to provide additional information. I understand that failure or refusal to disclose, false disclosure, or inability to resolve conflicts will require the ACOFP to identify a replacement.
Signature: Date: 1/6/15
Brian Forrest, MD


2/27/2015
1
Direct Primary Care: Terminology, Legal, and Legislative Issues
Philip Eskew, DO, JD, MBA
Family Medicine Resident PGY-3
Heart of Lancaster Regional Medical Center
ACOFP Annual Convention - March 14, 2015
DPC Terminology, Legal & Legislative Issues
• Learning Objectives: • A) Obtain an understanding of common DPC Terminology
• B) Appreciate the diversity of DPC offices and locations across the US
• C) Medicare considerations – “opt out” vs “fee for non-covered service”
• D) Awareness of the “Business of Insurance” hurdles
• E) Review state and federal DPC regulatory & policy considerations

2/27/2015
2
Questions We Will Answer
• How may we define Direct Primary Care (DPC)?
• What about “Concierge” medicine?
• How many physician groups are really doing this?
• How does DPC interact with Medicare? (and Medicaid?)
• What are the legal hurdles?
• Which states have DPC legislation?
• Does the Affordable Care Act impact DPC practices?
Direct Primary Care Defined
• For a practice to be defined as DPC, it must be a:
• primary care practice that
• 1) charges a periodic fee for services,
• 2) not bill any third parties on a fee for service basis, and
• 3) any per visit charge must be less than the monthly equivalent of the periodic fee.

2/27/2015
3
Defining Direct Primary Care
• DPC = a periodic fee with no “double dipping”
• Concierge is synonymous with the fee for non-covered services model
Retainer Medicine / Membership Medicine
Direct Primary Care
Split / Hydbrid
Concierge / Boutique
Concierge Care Defined
• A primary care practice that
• 1) charges a periodic fee for “non-covered” services, and
• 2) continues to also bill third parties on a fee for service basis
• Concierge practices, such as MDVIP or MD2, continue to bill third parties in the traditional fee for service fashion in addition to the periodic fee

2/27/2015
4
DPC vs Concierge – Cost Differences
• Price is not a component of the definition
• Concierge fees are often much higher
• MD2 initially charged $20,000 per year for “non-covered” services
• DPC groups often charge around $1,000 per year for all services
• Overhead costs are unchanged in concierge practices
Many Groups Support DPC
• ACOFP – DPC Task Force
• Direct Primary Care Coalition
• American Academy of Family Physicians • DPC Interest Groups, Workshops, public policy endorsement
• American Academy of Private Physicians
• Family Medicine Education Consortium • Organized multiple DPC National Summits
• American Association of Physicians & Surgeons
• DPC United

2/27/2015
5
DPC Folks Think Differently
DPC Research Methods
• Located as many DPC practices as possible (100), recorded publicly available data from the practice website:
• Practice Fee Structure • Membership ranges (avg of high and low charges for pts > 29 years old)
• Any per visit fee (average of four visits per year)
• Any enrollment fee (divided by twelve for a monthly comparison)
• Practice Design (pure DPC or split)
• Medicare status (opt out vs accepting)
• Practice self description (DPC, “Direct,” Concierge, other)

2/27/2015
6
Results
• All Practice average monthly cost = $100.55 (range $35.67 to $562.50) • All Practice Median monthly cost = $79.00
• Self Described DPC average monthly cost= $80.68 • Self Described Concierge average monthly cost= $199.59 • Split practice average monthly cost= $89.57 • Opted Out practice average monthly cost= $100.47
• Enrollment Fee = $82.63 (only 24 of 81) (range $29 to $300) • Per Visit Fee = $16.85 (only 17 of 81) (range $5 to $35)

2/27/2015
7

2/27/2015
8
What’s in the Name?
• Only 44 of 100 practices located in the study referred to themselves using the term “Direct Primary Care”
• 17 did (inaccurately) self describe using the term “concierge,” which can lead to confusion for both patients and policy makers, although it did correlate with a higher membership price
• Many other adjectives were used to describe each DPC practice
• “If you have seen one DPC practice, you have seen one DPC practice”

2/27/2015
9
Charging a Per Visit Fee
• Approach used by only 17 out of 81 practices with price info
• Average of $16.85, Median of $20 with range of $5 to $35
• The fee does not appear to affect the number of in-office visits • Qliance and Access Healthcare data suggests an avg of slightly under four in-
office visits per year
• Other DPC docs report an avg of 1% of patient panel requires services daily, supporting an avg of slightly under four (3.65) office visits per year as well
Charging an Enrollment Fee
• Only used by 24 of 81 practices with price info
• Average of $82.63, Median $77.50
• Range of $29 to $300

2/27/2015
10
Limitations
• Complicated pricing structures
• Lack of price transparency among all websites
• Scope of practice variance
Summary Findings
• DPC is Affordable • Median $80 per month, Average $100 per month
• Over 90% of practices are small and independent
• Per visit fees are used by less than 1/4 of DPC practices
• Enrollment fees are used by less than 1/3 of DPC practices
• Public price perception is accurate • DPC – affordable
• Concierge - expensive
• Flexible geographic location – 36 states, rural or urban

2/27/2015
11
Medicare
• “Opting Out” • Must be actively renewed every two years
• Legally safer option (False Claims Act, Stark, etc.)
• Ideal for a “Pure” DPC practice
• “Non-covered Services” • Terminology game – must stay one step ahead of the government
• Moonlighting is less complicated
• More common in “Hybrid” practices
Medicaid and Traditional Insurance
• Do not sign any traditional third party contracts! • This would give insurance companies leverage to block your DPC efforts
• You can “go public” with denials of coverage (Brian Forrest has an example)
• Always have each patient sign an individual contract with your practice (even when brought to you by an employer or other group)
• The ONLY appropriate role of a third party in DPC is payment • These agreements should not have any effect on your documentation or price
• Medicaid managed care pilot (Qliance)
• Medicare Advantage (Iora)
• Eventually more patients via state run insurance exchanges

2/27/2015
12
The “Business of Insurance”
• State Insurance Commissioners argue that DPC is too much risk • Membership contract amounts to the “unlawful sale of insurance”
• No case law directly on point • Huff v St. Joseph’s Mercy Hospital of Dubuque Corporation
• IRS definition anticipated related to Health Savings Accounts • Would be additional persuasive evidence that DPC is not a “health plan”
• Each state may approach this issue independently • Six states have passed laws designed to address this concern
• Wise contract terminology will be your defense – minimize “risk”
States with DPC Laws
• The Good • Washington • Utah • Louisiana • Michigan
• The Bad • Oregon
• The Ugly • West Virginia
• The Irrelevant • Arizona
• Pending • Georgia • Idaho • Mississippi (SB 2687) • Missouri (HB 769) • New Hampshire (SB 176) • Oklahoma (SB 560) • Texas (HJR 109) • Florida

2/27/2015
13
State Washington West Virginia Oregon Utah Arizona Louisiana Michigan
Date Passed 2007 2006 2011 2012 2014 2014 2015
Title Direct Patient-Provider
Primary Health Care Preventive Care Pilot
Program
Requirements for Certification as
Retainer Medical Practice
Medical Retainer Agreements
Direct Primary Care Provider
Direct Primary Care Practice
Medical Retainer Agreements
Phrases Defined
Requires that a "direct fee" be charged on a
monthly basis, no definition or use of term periodic fee
"primary care" poorly defined using terms
basic and simple,
"primary care" = outpatient,
nonspecialist, "retainer medical fee" poorly
defined "Routine" health care
services
Poor definition of "DPC Provider Plan", Poor
definition of "Primary Care Provider"
failed to define periodic fee, vague definition of "direct
fee" "Routine" health care
services
"Not Insurance" Yes (& HMO) Yes
Unclear - the only time the phrase "not
insurance" is used is in the mandatory
disclosures section Yes Yes Yes Yes
Reporting Obligations Yes Yes - Severe Yes None No No No
Mandatory Disclosure Yes No
Yes (in both contracts and marketing
materials) Brief "not insurance" No Yes Brief "not insurance"
Discontinue Care Provision Yes No No None No Yes None
"Double Dipping" Prohibition No No No Yes No No Yes
Marketing Restrictions No Severe No, only via disclosure
requirements No No No No
Inadvertent Pilot/Exchange Ban Potentially No Likely Potentially No Potentially Potentially
Promotion of DPCMH in exchange No No No No No No No
Scope Mild restrict, primary
care is broadly defined Narow Narrow Broadly defined Broad Mild restrict, primary
care is broadly defined Broadly defined
Policing Authority
Must submit annual statements to the
insurance commissioner HCA & Ins Commish
Dept of Ins - may investigate and
subpoena, broad authority to adopt new
rules None None LA St Med Bd None
Separate License needed No Yes Yes No No No No
Discontinuing Care Provisions (WA, LA)
• Patient participates in fraudulent activity
• Patient fails to pay for services
• Patient is abusive and is an emotional/physical danger to DPC
• Patient “repeatedly fails to comply with the recommended txt plan”
• DPC discontinues operations as a DPC

2/27/2015
14
Required Disclaimer (Louisiana)
• “This agreement does not provide comprehensive health insurance coverage. It Provides only the health care services specifically described.” (WA, LA)
• Inform the patient of his financial rights & responsibilities to DPC
• Encourage patient to maintain insurance for non DPC services
• State that DPC will not bill a health insurance issues for DPC services
• Include contact information for the state medical board
West Virginia “Preventive Care Pilot Program”
• Initially limited to six sites
• Program expires (again) on June 30, 2016 (grandfathering available)
• Health Care Authority – full control of provider selection (Cert of Need)
• All fees, marketing materials, and forms are subject to prior approval from the insurance commissioner
• No marketing (except for known uninsured or known HDHP = $3,000)
• Mandatory 6 month wait for employer to purchase DPC conversion
• Must submit income tax returns to HCA
• http://www.hcawv.org/Pilot/AttchA.htm
• “Primary Care” defined using terms “basic” and “simple”

2/27/2015
15
State by State Summary
• Terminology problems continue • Only 3 of the 6 states with legislation even use the term DPC
• Any DPC definition (if provided) is poor • Only Washington, Louisiana, and Arizona offer some type of definition
• A broad definition is contained in the Affordable Care Act
• States where DPC could be more difficult • Vermont
• West Virginia
• Oregon
State Model Legislation Recommendations
• Define DPC using 3 part definition
• Should contain a clear “NOT Insurance” provision • This is consistent with the “not a health plan” language in the ACA
• Mandatory contract and advertisement “not insurance” disclaimers
• No separate state registration should be necessary
• Require an individual contract with each patient
• List recommended discontinuation of care contract language
• Broadly define primary care scope of practice
• Promote formation of “wrap around” insurance policies

2/27/2015
16
Affordable Care Act
• Sec 10104 HHS “shall permit a qualified health plan to provide coverage through a qualified direct primary care medical home plan that meets criteria established by the Secretary…”
Qualified Health Plan
• Essential Health Benefits • Ambulatory patient services • Emergency services (reduced) • Hospitalization (reduced) • Maternity and newborn care • Mental health / substance abuse / behavioral health • Prescription drugs (reduced) • Rehabilitative and habilitative services and devices • Laboratory services (reduced) • Preventive and wellness services and chronic disease management • Pediatric services including oral and vision care

2/27/2015
17
Federal Register HHS Rules
• “Direct primary care medical home plan” = an arrangement where a fee is paid by an individual, or on behalf of an individual, directly to a medical home for primary care services, consistent with the program in Washington
• “Primary care services” = routine health care services, including screening, assessment, diagnosis, and treatment for the purpose of promotion of health, and detection and management of disease or injury
Federal Register HHS Rules
• “We considered allowing an individual to purchase a direct primary care medical home plan and separately acquire wrap-around coverage. However DPCMHs are providers, not insurance companies… allowing a separate offering would require consumers to make two payments for full medical coverage, adding complexity…”

2/27/2015
18
Federal Register HHS Rules
• “While we recognize the importance of accreditation and quality assurance, we are not establishing that direct PCMHs be accredited in order to participate in QHP networks. We encourage QHP issuers to consider the accreditation, licensure, or performance of all network providers.”
• “We do not interpret that phrase as including providers of non-primary care services, such as specialists.”
• “We are not directing exchanges to create incentives for contracting with direct PCMHs. We encourage exchanges to promote, and QHP issues to explore, innovative models of delivery along the care spectrum.”
Top 3 Legal Advisements
• If you decide to start a DPC practice:
• Consider the “Business of Insurance”
• Opt out of Medicare • (and avoid signing standard Private Insurance and Medicaid contracts)
• Go “all in” • Hybrid practices are legally riskier
• Hybrid practices have higher overhead

2/27/2015
19
Broad Predictions
• DPC will grow exponentially over the next five to ten years
• IRS will change Health Savings Account interpretation
• Wrap-around “catastrophic” insurance plans will be offered
• Will likely represent over half of the primary care market in 10 years
• Increased interest in primary care, physician ratio will improve
• Litigated victories against initial insurance commissioner challenges
• Second series of suits will later be filed based upon scope
• Triple aim actually achieved!
Any Questions?
Email: [email protected]

2/27/2015
1
Brian R. Forrest, MD
Direct Primary Care in the Trenches: Meeting the Quadruple Aim
Copyright 2014 Access Healthcare Direct all rights reserved
What Keeps Family Physicians up at Night?
• Concern about Medicare RAC Audits
• Confusion about ACO implications
• Wondering if they will be able to be independent
• Uncertainty about viability of their practice
• ICD-10 and other bureaucratic changes ? costs ?
• SGR, RUC not working, workforce problems

2/27/2015
2
Physician Trends and Attitudes
• Survey of 1311 physicians nationwide by Physicians Practice 9/14
• 53% considering or already in Direct Primary Care • 35% considering or already working in Concierge Model • Only 20% in process or have achieved PCMH recognition
• 4.4% plan on entering ACO
• 3.9% plan to become PCMH
• 4% plan to become hospital employed
DPC-Direct Primary Care • Pro
– Significantly lower out of pocket costs for most – Quality improved due to more time (value- based instead
of volume-based care) – Complete price transparency – Lowers overhead/helps practices financially – Improved access for underinsured and poor
• Con – Major transition/disruptive – Recruiting patient panel (copay culture)
Adapted from Forrest, B.R. Physician’s Practice
Pearl 12/7/11 New Primary Care Models Can Change the Way You Practice Medicine

2/27/2015
3
Concierge and DPC-Similar and Different
• Both improve quality of care for patients
• Both improve physician experience/pay
• Concierge severely shrinks panel size
• DPC improves access for low income/uninsured whereas concierge worsens
• Workforce improved instead of compromised with DPC
What is the Difference Between Concierge and DPC?
• DPC generally affordable for the average person (Honda vs. Ferrari)
• DPC can be successful in rural and poor communities
• DPC can lower out of pocket costs and downstream costs
• DPC panel size is optimal

2/27/2015
4
Vision Realized-My Favorite Moment
How Access Healthcare Model Created: The Hypothesis: 1999My
Study Different Models(15 years ago)
-Data on 42 providers
• If You: Decrease Overhead (micropractice) and Have patients pay in full at time of service, monthly, or yearly (direct payment)
• Then you can: Reduce Fees, Increase Collections, And Focus on patient care-Improve Quality

2/27/2015
5
“You’re Crazy!”
“That will never work.”
“You won’t be able to afford to stay in practice.”
What People Said About This Idea
Traditional Our Model
$1.00 $1.00
x.65 collected (avg in US) x.99
----- -----
.65 .99
-60% overhead (avg in US) - 18%
----- -----
.26 left .81 left
Primary Care Math

2/27/2015
6
18%
65%
Overhead Dramatically Reduced

2/27/2015
7
Genius of the GYM
$5
$3
• Charge low per member per month directly to patient or their employer or their insurer* – nominal per visit fee to cover overhead costs
– Net profit double to triple per patient per year
• A La Carte Non-Member transparent pricing at 80% off typical rates for service
• 4 FTE equivalents in overhead costs saved per physician-mostly due to no “insurance related
staffing”
Access Healthcare: a D-PCMH Micropractice Model

2/27/2015
8
Medical Home Member “subscription/membership model”: patients charged affordable fee per month and a nominal fee per office contact- no extra charge for common labs, EKGs, U/As, etc. Patients who come in rarely only for acute complaints are not forced to be “members” and can have services from an “a la carte” menu posted in waiting room- typically 80% off most services A La Carte Model: patients who opt not to be members (usually young patients with occasional acute problems like UTIs) add up bill on a discounted price transparent menu with 80% discount
◦This makes out of pocket costs average less than a the least expensive individual cell phone plan per year (even the chronically ill multisystem patient-including labs, in office procedures, the entire basket of services in our office )
Affordable Care
• Lower patient charges-80% less (improves access for underinsured)
• Higher collections (99% for 12+ years) with overhead 15-22%
• More time with patients/less patient volume(even with similar panel)
• Not bound to insurance contracts - no insurance filed
• Less stress/Lower risk exposure/Decreases medical mistakes 1
• Allows better familiarity and firmer patient relationships thus
decreasing risk 1,2
• Allows time to coordinate all aspects of patient’s medical care to
truly be the patient’s medical home
1-O’Hare, Dennis C. et al. FPM.2/2004 Vol 11. No.2” The Outcomes of Open Access Scheduling.”
2-Linzer, Mark et al. Advances in Patient Safety Vol 1.”Organizational Climate, Stress, and Error in Primary Care: The MEMO Study.”
Summary of DPC Model for AH

2/27/2015
9
Kick the Payer out of the Exam Room -
Make the Physician-Patient Relationship a 2 Party affair
Medicaid patients?
Insured Patients (52%) ?
The 5/50 Paradox

2/27/2015
10
Increased
Quality
Access
Improved
Cost
Patient/Physician
QCAP-The Quadruple AIM
0
10
20
30
40
50
60
70
80
SBP
LDL
HDL
Traditional/PCMH Hybrid DPC Practice
COSEHC DATA 2014 www.cosehc.org

2/27/2015
11
DPC Practice
All Practices0
10
20
30
40
50
60
70
Patients attaining target goals who were not at control at baseline
SBP LDL ≤ 100 LDL≤ 130 A1c
COSEHC DATA 2014 www.cosehc.org
For a family physician with patient panel capacity of 1200 and a visit volume of 16 patients maximum per day incomes can be similar to specialists like cardiology or GI and better than general surgery and most of the other internal medicine subspecialties If you want to do packages for the extremely economically challenged and create a lower fee schedule or sliding scale that is reduced by another 50%(as compared to average DPC practice fee), this can still net 50% more in salary for a family physician even if their entire panel was in this demographic.(works for rural communities or low median income areas)
Physician Income Expectations

2/27/2015
12
ACCESS HEALTHCARE, PA
Chronic Disease Management and Valuing Trust
Does Trust Matter?
• How much trust is built in a 35-minute visit versus an 8-minute visit?
• Research shows the cost of litigations when the patient and doctor spend more
time together and have more trust is significantly lower1,3
• The average primary care doctor pays $11,000/yr. in malpractice premiums.
• Two physicians at Access Healthcare together pay less than $4000 per year2.
• Also the decreased volume of 30 patients vs. 12 patients, means that you are
2.5 times less likely to be sued just based on volume.
1A study of sued and non-sued obstetricians found that patients who saw obstetricians with the most
frequent number of prior lawsuits were significantly more likely to report spending less than 10 minutes
with their physician during each visit; 2 Dr. Brian Forrest, Access Healthcare
3Kristin E. Schleiter, JD; Difficult Patient-Physician Relationships and the Risk of Medical Malpractice
Litigation
AMA Journal of Ethics. March 2009, Volume 11, Number 3: 242-246.
ACCESS HEALTHCARE, PA
Management of Chronic Disease in a DPC Model
• Only 50% of patients nationally with high BP who are
seeing a doctor and are being treated for high BP
have their BP under control1
• 80% of patients at goal in a review of 3 DPC
physicians2
1 NHANES 2007-2010 data
2 Access Healthcare Direct patient data 2011-2013

2/27/2015
13
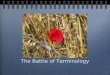
200 220
45 25
0
50
100
150
200
250
300
Baseline Follow-up
ATGOAL NOT ATGOAL
Access Healthcare Direct Diastolic Blood Pressure
Nu
mb
er o
f p
ati
ents
www.cosehc.org
82% ATGOAL 90% ATGOAL
JNC 7 Goal Attainment: < 90 mm Hg; < 80 mm Hg diabetic
8%
US vs. World vs. Access Healthcare Direct Practices
All Patient Out-of-Pocket costs per year including insurance premiums in DPC Model with High Deductible
Plan
ACCESS HEALTHCARE, PA
http://www.oecd.org/els/health-systems/oecdhealthdata2013-frequentlyrequesteddata.htm
The Organization for Economic Co-operation and Development (OECD)
© OECD. All rights reserved

2/27/2015
14
Two DPC physicians, One Quarter – 2Q2013 Results reflect a traditional profile…
ACCESS HEALTHCARE, PA
Access Healthcare1:
• In a full quarter, doctors
provide about 600
diagnoses.
• This equates to about 200 a
month or 50 a week.
• Most patients have more
than one ailment.
• Patient population is
demographically and
diagnosis code c/w NC
averages-except higher
portion of uninsured
1Access Healthcare Review of patient visit data 2011-2013
Access Healthcare LLC, All rights reserved
ACCESS HEALTHCARE, PA
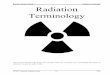
Doctor and Patient Experience Compared:
• In the AHC model, patients get more minutes, and are charged less leading to more favorable outcomes.
8
35
0
5
10
15
20
25
30
35
40
Traditional Care Access Healthcare
Doctor minutes for patient
20
140
0
20
40
60
80
100
120
140
160
Traditional Care Access Healthcare
Total Doctor-Patient Minutes/Year

2/27/2015
15
Observation Traditional DPCMH
Patients per day 30 12
Doctor minutes available 15 45
Doctor minutes for non-patient-facing work
7.5 10
Doctor min. average for patient interface
8 35
Typical Per Patient Insurance out of pocket costs for premiums
$2500 Employee Plan1 $ 33% less 2
Typical Visits per Year 2.5 4
Total Doctor time 20 140
Hospitalizations per 1000 pt/yr 11 4
ACCESS HEALTHCARE, PA
Patient Experience Compared:
• In the DPC model, patients get more minutes, and are charged less leading to more
favorable outcomes.
1 Various leading plans were reviewed including BCBS and UHC, this figure represents the approximate employee-based out-
of-pocket from those plans, per person covered.
2 Review of a 2013 BCBS plan with high deductible and catastrophic health coverage
8
35
0
5
10
15
20
25
30
35
40
Traditional Care Access Healthcare
Doctor minutes for patient
• Primary-care physicians with rising overhead, more paperwork, and packed waiting rooms are propelling ever-greater numbers to shed insurance and charge a retainer- up to 33% by 2016 according to Accenture Survey
• In 2011 the average American medical practice spent $82,975 per doctor just dealing with insurers, according to the Commonwealth Fund.
• In 2010, patients in this model visited emergency rooms 65 percent less than similar patients. Thirty-five percent fewer of them needed to be hospitalized. They required 66 percent fewer specialist visits.
• In 2012 the average premium for an employer-provided insurance policy for a family of four climbed to a record high of $20,728, according to Milliman, a health-care consultancy.
Interesting Tid Bits

2/27/2015
16
• Financial viability of independent practices (overhead can be <20%)
• Physician burnout- med students often say it seems like we are on vacation
• Work force recruitment-med students see hope in this model-being able to make as much as other specialists helps
• GME bottleneck-private residency programs can be self funding
• Access to primary care for most
• Practice determines reimbursement/payment rates
• Malpractice risk decreased
• Non-clinical bureaucracy/paperwork decreased
• Quality metrics and value based care are built in with measured practices exhibiting top tier chronic disease management
Key Problems the Model Solves:
Why Medical Students Should Be Excited About Direct Primary Care(excerpt from blog published on DPCMH.org, KevinMD and Primary Care Progress)-By Brian
Lanier
Direct primary care makes me incredibly optimistic about the
future. I will avoid the hamster wheel and provide the kind of
care I envisioned, while building deep, rich connections with
my patients. I will be offering a level of care previously only
available to the rich that almost anyone can afford. I will be
taking meaningful steps towards true, primary-care driven
and patient-centered health reform, and I won’t have to wait
for the “system” to figure it out. I will be able to provide the
majority of care my patients require instead of having time
only for refills and referrals. In short, I will be part of the
solution, both for my patients and for the system as a whole.
Brian Lanier is a fourth-year medical student at the University of North Carolina and a future family physician. Follow him on Twitter at @lanierbrian.
One Medical Student’s Thoughts-

2/27/2015
17
AAFP Response:DPC The AAFP recently created a document with frequently asked questions(4 page
PDF) to accompany the Academy's newly created policy on direct primary care
(DPC), a model in which practices charge patients a flat monthly or annual fee in
exchange for access to a broad range of primary care services.
"The AAFP supports the physician and patient choice to, respectively, provide and
receive health care in any ethical health care delivery system mode, including the
DPC practice setting," says the policy. It notes that the model is structured to
"emphasize and prioritize" the physician/patient relationship to improve health
outcomes and lower costs and is consistent with the AAFP's advocacy of both
the patient-centered medical home and a blended payment model.
According Glen Stream, M.D., M.B.I., of Spokane, Wash., "There is more than one
way to build a patient-centered medical home (PCMH)." He noted that the number of
AAFP members developing DPC practices was increasing.
"The model eliminates the insurance middleman and provides revenue directly
to the practice to innovate in both customer service and quality of care for the
patients they serve," said Stream.
-Employers-low cost option for employers, ACA has a section discussing that this
qualifies as insurance with HBE qualified plan as approved by HHS-section 1301 A 3
-Patients-higher satisfaction and better outcomes at lower out of pocket costs with
complete price transparency
-Medscape article reports explosive growth of this model and in conjunction with
Concierge practices represents currently 12% of primary care- expected to be 30-40%
of market by 2016
-Summit in St. Louis last October –Washington D.C., New Orleans, Miami, AZ- AAFP to
hold 3 regional workshops at the end of the year and Annual Assembly
-Insurers-products launching now to integrate into HBE eligible plans-including
Medicaid and Medicare Advantage
-Large Companies like Expedia.com, Freelancers Union, Whole Foods, Grove Park
Inn, Huntington Bank, McDonalds, and Taco Bell/Long John Silver’s already looking
to or currently contracting with DPC practices.
Significance of Direct Primary Care in 2013-2014

2/27/2015
18
Medicaid and DPC looks promising -In Washington State, Coordinated Care has partnered with 5 DPC practices to provide primary care for Medicaid Patients -With the initial 40,000+ enrollees: ER visits are down 60%, hospitalization and re-admission down 65%, and overall costs for this Medicaid population is 30% less for 2013 than the non-DPC pilot practices -Opportunity exists to do this in any state (like NC). It would make Medicaid a preferred payer by many family physicians- double the net revenue per patient of fee for service is possible (and payment is upfront every month-no waiting on delayed reimbursements) -In Washington State, participating physicians getting $50+ per member per month -This can really make practicing in rural and low income communities sustainable and recruit needed workforce into those areas
Access Healthcare Direct Network Practice
Practices Using our model/software including hybrid practices
Last updated 6/14

2/27/2015
19
Sprey, E. Physicians Practice “New Practice Models are Gaining Acceptance” 9/14 Forrest, B.R. Physicians Practice Pearl “New Primary Care Models Can Change the Way You Practice Medicine” 12/11 Forrest, B.R. Medical Economics Cover Story “Cutting Edge” 5/25/11 Mescia, Tony. Weekly Standard “Cash for Doctors Revisited” 4/11 Mescia, Tony. Weekly Standard Cover Story “Cash for Doctors” 5/23/10 Morgan, Lewis. Medical Economics Cover Story “Keeping it Simple” 1/22/10 Forrest, B.R. Physicians Practice. July 2008. “Cash and Carry Healthcare Still Works.” Forrest, B.R. Family Practice Management. June 2007. “Breaking Even on 4 Patients per Day.” Forrest, B.R. Physicians Practice. June 2007. “Cash and Carry Health Care.” Forrest, BR. NC Medical Journal May 2005. Innovations in Primary Care. “The Access Healthcare Model” Backer, Leigh Ann. Family Practice Management. February 2006. “2500 Cash Paying Patients and Growing”
Twitter @innovadoc (just starting to use this but giving regular DPC updates now) http://www.physicianspractice.com/pearls/new-primary-care-models-can-change-way-you-practice-medicine (link to first article above) http://newsle.com/BrianForrest source of compilation of 20+ articles on the DPC model www.accesshealthcaredirect.com website for DPC network practices. Undergoing renovation and updates www.DPCMH.org free membership for students and residents- website for members only
Where to Learn More