Embed Size (px)
Citation preview

Direct 3D segmentation of carotid plaques from 3Dultrasound images
Jieyu Cheng, Yanyan Yu and Bernard Chiu*Department of Electrical Engineering
City University of Hong Kong, Hong Kong, ChinaEmail: [email protected] (*Corresponding author)
Abstract—A direct 3D segmentation method is proposed tosegment carotid plaques from 3D ultrasound images. A 3D level-set evolution approach was applied to refine the initial plaquesurface constructed by an algorithm described in this paper.Compared with the previously described 2D slice-by-slice segmen-tation approach method, this direct 3D segmentation approachtook into account the continuity of the plaque geometry along thelongitudinal direction. Experimental results (total plaque volume(TPV) difference: 3D 4.5±9.8% vs. 2D 13.3±23.2; Dice similaritycoefficient (DSC): 84.4± 5.8% v.s. 83.7± 5.4%) suggest that theproposed 3D method outperforms the 2D slice-by-slice approach.
I. INTRODUCTION
Automatic segmentation of the carotid plaques from 3Dultrasound images is required for monitoring progression andregression of carotid atherosclerosis [1]. While several algo-rithms for carotid plaque segmentation from ultrasound imageshave been proposed, a majority of these methods segmentedplaques from 2D longitudinal carotid image. A comprehensivereview on the recent progress was given in Loizou [2]. Loizouet al. [3] segmented plaques in longitudinal images usingvarious snake models with initialization based on Dopplerblood flow images. Delsanto et al. [4] combined gradient-basedsegmentation, a snake method, and a fuzzy K-means algorithmto segment plaque-plus-vessel complex in longitudinal images.Destrempes et al. [5] adopted motion estimation and Bayesianframework to perform segmentation of plaques using RF infor-mation from longitudinal images. An integrated segmentationframework was proposed to segment atherosclerotic carotidplaque in ultrasound videos of the CCA based on video framenormalization, speckle reduction filtering, M-mode state-basedidentification, parametric active contours, and snake segmenta-tion [6], [7]. Since in carotid US images the contrast is lower atboundaries parallel to the US beam than boundaries orthogonalto the US beam, the applicability of those techniques to 3Dultrasound is unclear. Although segmentation approaches from2D ultrasound transverse images have been described, theysegmented the initima-media complex (IMC) instead of theplaque [8]–[11]. Plaque measurement is a more direct indicatorof stroke risk.
Our previous work [12] used outer wall and lumen segmen-tations as prior knowledge in a level-set framework to segment2D transverse slices extracted from 3D ultrasound images.First, for each vertex on outer wall contour, the one-to-one cor-respondence between the lumen and outer wall contours wasestablished using the modified symmetric correspondence [13].Then, initial points were identified. We connected these initialpoints to form a closed initial contour, which was subsequently
deformed using a 2D level-set approach. However, there aretwo main limitations associated with this approach:
1) The result of the level-set approach is sensitive tothe initial plaque contour constructed by our algorithm. Inour previous method, the prior wall and lumen boundariesespecially wall restricted the searching range for initial points,sometimes leading to inaccurate initialization of the plaquecontour. The inaccurate wall delineation would cause theaccumulation in error.
2) The previous approach segmented each transverse sliceindependently, without taking advantage of the continuity ofthe plaque geometry along the longitudinal direction.
Here, we propose a direct 3D carotid plaque segmentationframework. The contributions of this work are summarized asfollows:
1) The 2D curve evolution in previous work was extendedto 3D surface evolution, incorporating the longitudinal infor-mation.
2) We utilized a trust level to the prior knowledge, whichreduces the impact of the inaccurate wall delineations.
3) The proposed method was performed on the wholescanned carotid arteries, including external carotid artery(ECA) and internal common artery (ICA).
II. METHODOLOGY
The proposed method consists of 3 main steps: 2D initial-ization on transverse slices with fixed inter-slice distance, 3Dinitial surface generation by triangulation and 3D surface evo-lution using sparse field level-set. Figure 1 gives the flowchartof the proposed method.
A. Initialization
First we initialize on a stack of 2D slices with inter-slice distance of 1mm. To improve robustness to segmentationvariations of outer wall, a local intensity change map [14] iscomputed to determine the suspicious points on wall boundary.Chiu et al. [15] has examined the relationship of arterial walland lumen segmentation variability with the local intensitychange [14]. Hence, for those suspicious points, the searchingrange for initial points is extended by moving the wall pointoutwards in the direction of wall-lumen correspondence linefor 0.5mm. Searching criterion of the initial point for eachcorrespondence line can refer to our previous method [12].
978-1-5090-2959-4/16/$31.00 2016 IEEE 123

Fig. 1. Schematic diagram of the proposed method.
After 2D initialization, we obtain a stack of 2D initialcontours. These 2D contours are then triangulated to generatea 3D surface mesh which is considered as the initial surface,i.e. the input for 3D level-set evolution. The 2D initial pointselection is merely based on the intensity profile of the linesegment linking points on outer wall and lumen withoutconsidering the information of neighbor initial points, thusthe generated 2D contour on each slice might be unsmooth.The following 3D level-set incorporates the smoothness termwith image data- and high-level knowledge-based terms, thusrefining the initial surface at the same time keeping it in acertain extent of smoothness.
B. 3D Level-sets
Sparse field level-set method [16] is adopted to iterativelyevolve the initial 3D surface to achieve the local optimum ofthe objective energy function. Each image is represented asI : Ω ⊂ R3, where R defines the image domain. The evolvingsurface is represented implicitly as a level set of a 4D scalarfunction - referred to as the level set function Φ(x) : Ω→ R,and x ∈ R is a voxel within the image domain. The evolvingsurface is specified as the set of x with Φ(x) = 0 . During thesegmentation process, the function Φ(x) is iteratively evolved.In our implementation, Φ(x) is initially defined as a signeddistance function of the initial surface obtained in the previousinitialization step.
The designed objective function consists of four differentterms, i.e. smoothness energy Es, distance restriction energyEd [17], local region-based energy El [18] and global intensitypdf energy Eg [19].
E = λsEs + λlEl + λdEd + λgEg (1)
Where λs, λl, λd and λg are their weights which controlthe influence of these energy terms. Their values used inthe experiment were determined by evolutionary strategy (ES)algorithm [20].
Es controls the smoothness of the evolving surface whichonly considers the geometry of the evolving surface. Thedefinition is given below:
Es =
∫Ω
|∇H(Φ(x))| dx (2)
where H(·) is regularized Heaviside function.
Distance restriction energy Ed is based on high-level priorknowledge to keep the evolving surface and outer wall surfacein a reasonable distance [17]
Ed =
∫Ω
δ(Φ(x))P (x)dx (3)
where P (x) =
0 ‖x,MAB‖ ≤ MSD1 otherwise
, ‖x,MAB‖ repre-
sents the Euclidean distance between x and the MAB (outerwall). δ(·) denotes the Delta function.
Local region-based energy El and global intensity pdfenergy Eg are image intensity-based terms. El is used tocapture the weak edge between healthy vessel tissue andplaque [18].
El =
∫Ω
δ(Φ(x))
∫Ω
BL(x, x)[H(Φ(x))(I(x)− ux)2
+ (1−H(Φ(x)))(I(x)− vx)2]dx dx
(4)
where BL(x, x) defines a Gaussian kernel centered at voxel xwith radius of r. ux and vx represent the intensity means ofvoxels within the kernel region of voxel x inside and outsidethe evolving surface respectively.
Eg makes use of the Bhattacharyya distance of the proba-bility density functions (PDFs) as a measure of the differencein the intensity pattern [19].
Eg = B(Φ(x)) =
∫z
√P−(z|Φ(x))P+(z|Φ(x))dz (5)
where P− and P+ are two smoothed PDFs computed fromthe global interior and exterior regions of the surface usingz intensity bins. The Bhattacharyya coefficient B serves as ameasure representing the similarity of the two PDFs.
The computation of all these energy terms takes into ac-count the longitudinal information compared with 2D level-set.The evolution will stop when meeting the stopping criterion(changing volume less than 1.0mm3 between two adjacentiteration) or after a certain iteration number (here we set it to1000 iterations). The voxels between the final evolving surfaceand lumen surface are regarded as our algorithm output, i.e.plaque region.
C. Image Acquisition and Evaluation
Both previous 2D method and direct 3D method wereperformed on 10 3DUS images obtained from 8 subjects withcarotid stenosis ≥ 60% (according to carotid Doppler flowvelocities). Subjects provided written informed consent to thestudy protocol, which was approved by The University ofWestern Ontario Standing Board of Human Research Ethics.All subjects were recruited from The Premature Atherosclero-sis Clinic and The Stroke Prevention Clinic at University Hos-pital (London Health Sciences Centre, London, ON, Canada)
124

and the Stroke Prevention and Atherosclerosis Research Centre(Robarts Research Institute, London, ON, Canada). The 3DUS system used in our study has been described in detailelsewhere and is summarized as follows [1], [21]. The 3D USimages were acquired using an ATL HDI 5000 US machine bytranslating a 50 mm L12-5 transducer (ATL-Philips, Bothell,WA, USA) . The transducer was mounted on a linear motorassembly, which was moved along the lateral side of the neckat a constant speed of 3 mm/s for approximately 4.0 cm. Theacquired 2D images were parallel to each other with a pixelsize of 0.1×0.1mm2 and separated by 0.2 mm. Then these 2Dimages were reconstructed to a 3D image with the resolutionof 0.1× 0.1× 0.2mm3.
Manual segmentations were used as reference for theevaluation of segmentation accuracy and obtained by oneexpert blind to the subject information manually delineatingthe plaque boundaries according to the criterion described inLandry [22]. 2D method was performed on already resliced2D transverse images and compared with manual 2D bound-aries. To offer direct comparison with previous algorithm, 3Dalgorithm-generated plaque surfaces were also resliced at 1mm intervals and compared with corresponding manual bound-aries. Similar to the 2D method, three different types of metricsincluding volume-, region- and distance-based metrics wereused for accuracy evaluation. In this experiment, total plaquevolume (TPV) is defined for individual plaque. We calculatedthe absolute TPV difference (∆TPV mm3) and relative TPVdifference (%) as volume-based metrics. Region-based metricsinclude the absolute plaque area (PA) difference (∆PAmm2),relative PA difference (∆PA%) and dice similarity coefficient(DSC). DSC measures the overlap of two regions:
DSC =|Rm ∩Ra||Rm|+ |Ra|
(6)
where operator | · | here means the area of region. Distance-based metrics are calculated after the establishment of cor-respondence two contours using modified symmetric corre-spondence method [13]. Then mean absolute distance (MAD),maximum absolute distance (MAXD) and average distance(AVD) were computed.
III. RESULTS
Both 2D and proposed 3D methods were performed on10 3DUS images including CCA and two branches (ECAand ICA) with 13 plaques ranging from 9.5 to 458.0 mm3.Figure 2 gives a slice-by-slice comparison between manual andalgorithm results for two example arteries. We also comparesthe generated surface using manual and algorithm methods inFigure 3. As shown in Table 1, the proposed method exhibitshigher accuracy than 2D method.
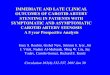
In addition, since total plaque volume (TPV) is a clinicallysignificant indicator of carotid atherosclerosis, we carried outthe Bland-Altman analysis and Pearson correlation analysis.As shown in Figure 4, there is a mean bias of 6.6mm3
in quantification of TPV using our method. High correlationcoefficient (r = 0.985) revealed the high linear relationship be-tween estimated TPVs using proposed method and manually-generated TPVs.
Fig. 2. Slice-by-slice comparison of manual and algorithm segmentations
Fig. 3. surface comparison of manual and algorithm segmentations
IV. CONCLUSION
In conclusion, we proposed a direct 3D method to segmentcarotid plaques from 3D US images. Experimental results sug-gest that the proposed method is more robust to segmentationsof outer wall and achieve higher segmentation accuracy thanthe previous 2D method.
Fig. 4. Bland-Altman plot for total plaque volumes (TPVs) generated by 3Dalgorithm and manual methods.
125

Fig. 5. Pearson correlation analysis between manual TPV (MTPV) andalgorithm TPV (ATPV).
TABLE I. COMPARISON OF 2D AND 3D METHODS IN SEGMENTATIONACCURACY.
Metrics 2D method 3D method∆TPV (mm3) 11.4± 23.1 6.6± 21.3∆TPV (%) 13.3± 23.2 4.5± 9.8|∆TPV |(mm3) 13.3± 19.9 15.7± 15.3|∆TPV |(%) 14.3± 22.5 9.2± 5.1∆PA(mm2) 1.0± 3.9 1.3± 3.6∆PA(%) 5.0± 18.7 6.6± 15.8|∆PA|(mm2) 2.7± 3.0 2.6± 2.8|∆PA|(%) 13.0± 14.2 13.6± 14.5DSC (%) 83.7± 5.4 84.4± 5.8MAD (mm) 0.30± 0.12 0.23± 0.11MAXD (mm) 1.78± 1.67 1.78± 1.49AVD (mm) −0.01± 0.16 −0.01± 0.17
REFERENCES
[1] C. D. Ainsworth, C. C. Blake, A. Tamayo, V. Beletsky, A. Fenster, andJ. D. Spence, “3D ultrasound measurement of change in carotid plaquevolume: a tool for rapid evaluation of new therapies,” Stroke, vol. 36,no. 9, pp. 1904–1909, Sep 2005.
[2] C. P. Loizou, “A review of ultrasound common carotid artery imageand video segmentation techniques,” Medical & biological engineering& computing, vol. 52, no. 12, pp. 1073–1093, 2014.
[3] C. P. Loizou, C. S. Pattichis, M. Pantziaris, and A. Nicolaides, “An in-tegrated system for the segmentation of atherosclerotic carotid plaque,”IEEE Trans. Inf. Technol. Biomed., vol. 11, no. 6, pp. 661–667, Nov2007.
[4] S. Delsanto, F. Molinari, P. Giustetto, W. Liboni, S. Badalamenti,and J. S. Suri, “Characterization of a completely user-independentalgorithm for carotid artery segmentation in 2-d ultrasound images,”Instrumentation and Measurement, IEEE Transactions on, vol. 56, no. 4,pp. 1265–1274, 2007.
[5] F. Destrempes, J. Meunier, M.-F. Giroux, G. Soulez, and G. Cloutier,“Segmentation of plaques in sequences of ultrasonic b-mode images ofcarotid arteries based on motion estimation and a bayesian model,”Biomedical Engineering, IEEE Transactions on, vol. 58, no. 8, pp.2202–2211, 2011.
[6] C. P. Loizou and M. Pantziaris, “An integrated system for the completesegmentation of the common carotid artery bifurcation in ultrasoundimages,” Journal of Biomedical Engineering and Informatics, vol. 1,no. 1, p. p11, 2015.
[7] C. P. Loizou, T. Kasparis, C. Spyrou, and M. Pantziaris, “Integratedsystem for the complete segmentation of the common carotid arterybifurcation in ultrasound images,” in Artificial Intelligence Applicationsand Innovations. Springer, 2013, pp. 292–301.
[8] E. Ukwatta, J. Awad, A. D. Ward, D. Buchanan, J. Samarabandu,G. Parraga, and A. Fenster, “Three-dimensional ultrasound of carotid
atherosclerosis: semiautomated segmentation using a level set-basedmethod.” Med Phys, vol. 38, no. 5, pp. 2479–2493, May 2011.
[9] E. Ukwatta, J. Yuan, D. Buchanan, B. Chiu, J. Awad, W. Qiu,G. Parraga, and A. Fenster, “Three-dimensional segmentation of three-dimensional ultrasound carotid atherosclerosis using sparse field levelsets,” Medical physics, vol. 40, no. 5, p. 052903, 2013.
[10] A. Zahalka and A. Fenster, “An automated segmentation method forthree-dimensional carotid ultrasound images.” Phys Med Biol, vol. 46,no. 4, pp. 1321–1342, Apr 2001.
[11] M. M. Hossain, K. AlMuhanna, L. Zhao, B. K. Lal, and S. Sikdar,“Semiautomatic segmentation of atherosclerotic carotid artery wallvolume using 3d ultrasound imaging,” Medical physics, vol. 42, no. 4,pp. 2029–2043, 2015.
[12] J. Cheng, H. Li, F. Xiao, A. Fenster, X. Zhang, X. He, L. Li,and M. Ding, “Fully automatic plaque segmentation in 3-d carotidultrasound images,” Ultrasound in medicine & biology, vol. 39, no. 12,pp. 2431–2446, 2013.
[13] B. Chiu, M. Egger, J. D. Spence, G. Parraga, and A. Fenster, “Quan-tification of carotid vessel wall and plaque thickness change using 3dultrasound images,” Medical physics, vol. 35, no. 8, pp. 3691–3710,2008.
[14] D. Shen, Y. Zhan, and C. Davatzikos, “Segmentation of prostateboundaries from ultrasound images using statistical shape model,” IEEETrans. Med. Imaging, vol. 22, no. 4, pp. 539–551, Apr 2003.
[15] B. Chiu, A. Krasinski, J. D. Spence, G. Parraga, and A. Fenster, “Three-dimensional carotid ultrasound segmentation variability dependence onsignal difference and boundary orientation.” Ultrasound Med Biol,vol. 36, no. 1, pp. 95–110, Jan 2010.
[16] R. T. Whitaker, “A level-set approach to 3d reconstruction from rangedata,” International journal of computer vision, vol. 29, no. 3, pp. 203–231, 1998.
[17] O. Gloger, M. Ehrhardt, T. Dietrich, O. Hellwich, K. Graf, andE. Nagel, “A threestepped coordinated level set segmentation methodfor identifying atherosclerotic plaques on mr-images,” Communicationsin Numerical Methods in Engineering, vol. 25, no. 6, pp. 615–638,2009.
[18] S. Lankton and A. Tannenbaum, “Localizing region-based active con-tours,” Image Processing, IEEE Transactions on, vol. 17, no. 11, pp.2029–2039, 2008.
[19] O. Michailovich, Y. Rathi, and A. Tannenbaum, “Image segmentationusing active contours driven by the bhattacharyya gradient flow,” ImageProcessing, IEEE Transactions on, vol. 16, no. 11, pp. 2787–2801,2007.
[20] H.-G. Beyer and H.-P. Schwefel, “Evolution strategies–a comprehensiveintroduction,” Natural computing, vol. 1, no. 1, pp. 3–52, 2002.
[21] A. Fenster, D. B. Downey, and H. N. Cardinal, “Three-dimensionalultrasound imaging,” Phys. Med. Biol., vol. 46, no. 5, pp. R67–99, May2001.
[22] A. Landry, J. D. Spence, and A. Fenster, “Measurement of carotidplaque volume by 3-dimensional ultrasound,” Stroke, vol. 35, no. 4,pp. 864–869, Apr 2004.
126