Embed Size (px)
Citation preview

Dilatation and Dysfunction of the Right VentricleImmediately After Ultraendurance Exercise
Exploratory Insights From Conventional Two-Dimensional and SpeckleTracking Echocardiography
David Oxborough, MSc; Robert Shave, PhD; Darren Warburton, PhD; Karen Williams, MSc;Adele Oxborough, BSc; Sarah Charlesworth, PhD; Heather Foulds, MSc; Martin D. Hoffman, MD;
Karen Birch, PhD; Keith George, PhD
Background—Running an ultramarathon has been shown to have a transient negative effect on right ventricular (RV) andleft ventricular (LV) function. Additionally, recent findings suggested that ultraendurance athletes may be more at riskof developing a RV cardiomyopathy. The standard echocardiographic assessment of RV function is problematic;however, the introduction of ultrasonic speckle tracking technology has the potential to yield a comprehensiveevaluation of RV longitudinal function, providing new insights into this phenomenon. Thus, the primary aim of thisexploratory study was to evaluate comprehensively RV structure and function after a 161-km ultramarathon andestablish whether changes in the RV are associated with alterations in LV function.
Methods and Results—Myocardial speckle tracking echocardiograms of the RV and LV were obtained before and immediatelyafter a 161-km ultramarathon in 16 healthy adults. Standard echocardiography was used to determine RV size and functionand LV eccentricity index. Speckle tracking was used to determine the temporal evaluation of indices of RV and LV function.RV size was significantly increased postrace (RV outflow, 32 to 35 mm, P�0.002; RV inflow, 42 to 45 mm, P�0.027) withan increase in LV eccentricity index (1.03 to 1.13, P�0.006). RV strain (�) was significantly reduced postrace (�27% to�24%, P�0.004), but there was no change in the rates of �. Peak � in all planes of LV motion were reduced postrace(longitudinal, �18.3 to �16.3%, P�0.012; circumferential, �20.2% to �15.7%, P�0.001; radial, 53.4% to 40.3%,P�0.009). Changes in RV size and function correlated with diastolic strain rates in the LV.
Conclusions—This exploratory study demonstrates RV dilatation and reduction in function after an ultramarathon. Furtherresearch is warranted to elucidate the mechanisms responsible for these findings. It is not clear what clinical impactmight result from consecutive bouts of postexercise RV dysfunction. (Circ Cardiovasc Imaging. 2011;4:253-263.)
Key Words: ventricles � echocardiography � imaging � exercise � cardiac output � fatigue
The effects of prolonged strenuous exercise on cardiac functionduring the early stages of recovery have been relatively well
explored, with substantive descriptive evidence supporting a tran-sient reduction in left ventricular (LV) systolic and diastolic func-tion.1 Interest in the impact of prolonged exercise on right ventric-ular (RV) function was likely stimulated by case reports of 2athletes presenting with pulmonary edema and right-side heartfailure after a 90-km ultramarathon race.2 Subsequently, a smallnumber of exercise studies (using conventional 2D echocardio-graphic indices) have shown a reduction in RV function during therecovery period.3–7 Using tissue Doppler echocardiography-derivedstrain (�) technology, Neilan and colleagues8 described a reduction
in RV free wall deformation in athletes after completion of theBoston Marathon. In a recent study by our group, a transientdepression in both LV and left atrial (LA) function was reported inathletes after running a marathon, with a link postulated between apostrace reduction in LA deformation and RV function.9 This study
Clinical Perspective on p 263
demonstrated reduced RV function using echocardiographic-derived RV fractional area change (RVFAC), which may wellhave had a consequent impact on LA preload and subsequentdistension. Taken together, these previous reports suggest RVinvolvement after prolonged exercise; however, at present, a
Received November 4, 2010; accepted March 2, 2011.From the Faculty of Medicine and Health, University of Leeds, Leeds, UK (D.O.); Cardiff School of Sport, Cyncoed Campus, Cyncoed, Cardiff, Wales,
UK (R.S.); Centre for Sport Medicine and Human Performance, Brunel University, Uxbridge, London, UK (R.S.); Cardiovascular Physiology andRehabilitation Laboratory, Physical Activity and Chronic Disease Prevention Unit and Experimental Medicine Program, University of British Columbia,Vancouver, British Columbia, Canada (D.W., S.C., H.F.); Research Institute for Sport and Exercise Sciences, Liverpool John Moores University,Liverpool, UK (K.W., K.G.); Spire Hospital, Leeds, UK (A.O.); Department of Physical Medicine and Rehabilitation, Department of Veterans Affairs,Northern California Health Care System, and University of California Davis Medical Center, Sacramento, CA (M.D.H.); and MultidisciplinaryCardiovascular Research Centre, University of Leeds, Leeds, UK (K.B.).
Correspondence to David Oxborough, University of Leeds, Woodhouse Ln, Leeds LS2 9JT, UK. E-mail [email protected]© 2011 American Heart Association, Inc.
Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.110.961938
253
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

comprehensive evaluation of RV structure and functionbefore and after prolonged exercise has not been attempted.
The significance of RV impairment after prolonged strenuousexercise is the subject of some speculation. Exercise-inducedRV damage has been proposed as a potential mechanism for RVarrhythmias in some ultraendurance athletes,10 and a recentstudy by La Gerche and colleagues11 highlighted the potential
for developing an arrhythmogenic RV cardiomyopathy pheno-type through prolonged bouts of intense endurance exercise. Inview of this, it is tempting to speculate that acute changes to RVstructure and function after a bout of intense endurance exercisemay contribute to this chronic phenomenon.
The assessment of RV systolic function with 2D echocar-diography, particularly the calculation of volumes and, thus,
Figure 1. Myocardial speckle tracking dem-onstrating region of interest along the rightventricular lateral wall and subsequentoffline analysis of right ventricular strain andstrain rate. AVC, aortic valve closure.
254 Circ Cardiovasc Imaging May 2011
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

function, is extremely problematic because of the geometry,location, and excess trabeculation of the RV.12 Myocardialspeckle tracking (MST) is a relatively new technique that hasbeen applied to the assessment of LV13 and, more recently,LA function.14 Unlike other techniques, such as tissue Dopp-ler echocardiographic imaging of velocities or �,8 MST-derived � is free from angle dependency15 and has beenshown to be reliable and valid in providing circumferential,radial, and longitudinal deformation indices.16 Because of theadvantages of the technique in overcoming some of thegeometric ultrasound limitations, MST recently has beenapplied successfully to the assessment of the RV.17
In view of the development in ultrasound technology andthe possible clinical significance of RV dysfunction afterintense exercise, we sought to provide in this exploratorystudy a comprehensive evaluation of RV structure and func-tion after a 161-km ultraendurance trail run and to establishwhether any changes are associated with alterations in LVfunction. We proposed the following hypothesis: A 161-kmultramarathon will negatively affect RV function, and postex-ercise changes in LV filling will be related to altered RVfunction.
MethodsParticipantsSixteen (12 male) competitors in the 161-km 2009 Western StatesEndurance Run (Squaw Valley, CA, to Auburn, CA) aged 42�8years (range, 25 to 60 years) volunteered to participate in the study.All participants were healthy and free from known cardiovasculardisease, had no early family history of cardiovascular disease, andwere not currently taking any form of prescribed medication. Allwere endurance runners with a broad range of experience demon-strated by the number of previously completed ultramarathon races(mean, 69�117 races; range, 7 to 500 races) and years training(15�12 years; range, 2 to 46 years). Also documented was the
training status of the cohort in terms of miles per week (mean,65�22 miles/week; range, 40 to 120 miles/week) and hours perweek (mean, 14�4 hour/week; range, 8 to 24 hours/week). Allsubjects provided written informed consent to participate, and thestudy was granted approval by the ethics committee at BrunelUniversity as well as complied with the Declaration of Helsinki.
Experimental ProceduresEchocardiograms were performed �24 hours before starting therace, and postrace echocardiograms were completed within 1 hour ofrace completion. Body mass was measured with the same scalepreceding each echocardiogram. All subjects refrained from vigor-ous training for 24 hours and avoided alcohol and caffeine for 4hours before the prerace assessment. During the race, participantswere permitted to consume food and fluid ad libitum. On the day ofthe race, the event started at 0500 hours. Over the race period (30hours), temperature recorded at course temperature stations rangedfrom 4°C to 37°C.
Figure 2. Temporal graphical representation of RV strain beforeand after an ultramarathon competition. PVC indicates pulmo-nary valve closure; RV, right ventricular.
Table 1. RV Indices Before and After the Ultramarathon Competition
Prerace Postrace
Parameter Mean�SE Range Mean�SE Range P
RV end-diastolic area, cm2 23�0.8 16 to 28 25�0.9 20 to 30 0.010
RV end-systolic area, cm2 13�0.6 7 to 17 15�0.7 12 to 22 0.007
RVFAC, % 43�0.02 30 to 60 38�0.02 26 to 48 0.028
RV outflow, mm 32�1.0 27 to 40 35�1.1 25 to 41 0.002
RV inflow, mm 42�1.1 36 to 50 45�1.2 38 to 53 0.027
RV acceleration time, cm/s 1.6�0.24 0.6 to 3.1 1.7�0.27 0.6 to 3.1 0.677
RV IVCT, ms 77�4.7 60 to 100 80�5.8 60 to 110 0.496
RV IVRT, ms 47�7.0 20 to 80 57�8.0 30 to 110 0.049
LVEI 1.03�0.01 0.91 to 1.18 1.13�0.03 0.92 to 1.50 0.006
RA volume, mL 65�4.9 38 to 114 67�5.6 32 to 110 0.535
RV �, % �27�1.5 �17 to �36 �24�1.8 �12 to �37 0.004
RV SRs� �1.66�0.09 �1.14 to �2.38 �1.67�0.13 �1.06 to �3.19 0.948
RV SRe� 2.14�0.19 0.94 to 3.48 1.94�0.21 0.29 to 3.41 0.381
RV SRa� 1.58�0.14 0.72 to 2.55 1.50�0.15 0.72 to 2.40 0.580
RV SRe�/SRa� 1.48�0.15 0.49 to 2.62 1.46�0.19 0.32 to 2.94 0.930
� indicates strain; IVCT, isovolumic contraction time; IVRT, isovolumic relaxation time; LV, left ventricular; LVEI, LVeccentricity index; RA, right atrial; RV, right ventricular; RVFAC, RV fractional area change; SRa�, strain rate lateventricular diastole; SRe�, strain rate early ventricular diastole; SRs�, strain rate during ventricular systole.
Oxborough et al Right Ventricular Function After an Ultramarathon 255
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Echocardiographic AssessmentsAfter a full explanation of procedures, participants lay supine for 5minutes before echocardiographic examination. Heart rate was takenfrom the ECG inherent to the ultrasound system, and resting brachialartery blood pressure was recorded using standard auscultation. Allechocardiographic images were acquired with a commercially avail-able ultrasound system (Vivid I; GE Medical; Horten, Norway) witha 1.5- to 4-MHz phased-array transducer. All images were acquiredby 2 experienced sonographers with the subject lying in the leftlateral decubitas position and recorded to DVD in a raw digitalimaging and communications in medicine format. Acquisition andanalysis were performed by a single experienced sonographer. Alldata were analyzed off line with commercially available software(EchoPac version 7.0; GE Medical), and a minimum of 3 cardiaccycles were averaged for all peak indices.
Conventional EchocardiographyStandard 2D, pulsed-wave and pulsed tissue Doppler echocardio-graphic parameters were obtained from parasternal and apicalacoustic windows. All settings were optimized to obtain maximumsignal-to-noise ratio and 2D images to provide optimal endocardialdelineation. RV size was measured at end diastole from the outflowtract using a parasternal long-axis view and at the inflow from anapical 4-chamber orientation as previously described.18 RV end-di-astolic area and end-systolic area were calculated by tracing aroundthe endocardium from a modified apical 4-chamber orientation, andRVFAC was calculated as [(RV end-diastolic area�RV end-systolicarea)/RV end-diastolic area]. An LV end-diastolic eccentricity index(LVEI) also was calculated as a measure of interventricular septaldisplacement. A parasternal short-axis orientation at midlevel (pap-illary muscle) was used. LV diameter was measured in end diastolefrom inferior to anterior wall and from septum to posterolateral walland the LVEI was calculated as the ratio of the two measurements.19
Right atrial volume was measured using an apical 4-chamberorientation and calculated using Simpsons method at end systole. RV
isovolumic contraction and relaxation times were calculated frompulsed-wave tissue Doppler echocardiographic imaging traces with a2-mm sample volume placed in the tricuspid annulus to ensure thebest alignment between wall motion and the ultrasound beam.
LV end-diastolic dimension, LV end-diastolic volume (LVEDV),LV end-systolic volume, LA anterior-posterior diameter, and LAvolume at end systole were measured in accordance with recommen-dations from the American Society of Echocardiography.20 Allvolumes were derived using Simpsons biplane methodology, and LVejection fraction was calculated. LV stroke volume was calculated asthe difference of LVEDV and LV end-systolic volume, and cardiacoutput was subsequently calculated as the product of stroke volumeand heart rate. LV diastolic function was assessed using pulsed-waveDoppler echocardiographic recordings from apical 4-chamber and3-chamber orientations. A 4-mm sample volume was placed at thetips of the mitral leaflets in diastole, and transmitral flow wasacquired to obtain peak early (E) and atrial (A) flow velocities.21 Forthe tissue Doppler echocardiographic assessment of early diastolicmyocardial velocity (E�), the apical 4-chamber orientation was used,and a 2-mm sample volume was positioned at the septal aspect of themitral valve annulus. Peak E� tissue myocardial velocity wasrecorded, and E/E� was calculated.
Two-Dimensional Myocardial Speckle TrackingFor the acquisition of RV functional data, the apical 4-chamberorientation was used, with the region of interest placed around theRV lateral wall from base to apex (Figure 1). LV radial andcircumferential � and strain rate (SR) were derived from a paraster-nal short-axis view at the base, defined as at the tips of the mitralvalve. The calculation of torsion also required the acquisition of anapical short-axis view at the level immediately above that of systoliccavity obliteration.22 LV and LA longitudinal � and SR data wereobtained from an apical 4-chamber view only. In all orientations,frame rates were acquired as high as possible, but not �90frames/second, with the focal point positioned at the midlevel of the
Figure 3. Significant RV structural parameters for individual participants. Abbreviation as in Figure 2.
Figure 4. Significant RV functional parameters for individual participants. LV indicates left ventricular; LVEI, LV eccentricity index;RVFAC, right ventricular fractional area change. Other abbreviation as in Figure 2.
256 Circ Cardiovasc Imaging May 2011
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

cavity of interest to minimize the impact of beam divergence. Allimages were optimized with gain, compression, and dynamic rangeto enhance myocardial definition, whereas depth, frequency, andinsonation angle were standardized from all acquisitions to reducethe impact of variability.23
Offline analysis allowed the assessment of peak data of the RVlateral wall, and a global value was obtained as the average of thebase, mid, and apical wall segments. Indices obtained included peakRV � and SR during ventricular systole and during early and lateventricular diastole and their calculated ratio (Figure 1). For theassessment of circumferential and radial LV function, basal paraster-nal short-axis segments provided data from the inferoseptum; an-teroseptum; and anterior, lateral, posterior, and inferior walls, and amean value was obtained representing global �. The apical4-chamber orientation provided longitudinal data from the basal,mid, and apical septum and basal, mid, and apical lateral walls, andagain, a mean value of all myocardial segments was obtained. Allmyocardial segments were considered acceptable and included in theanalysis. Peak basal and apical rotation and rotation rate wereobtained, and torsion was calculated as the net difference betweenapical and basal rotation. Peak LV circumferential, radial, and
longitudinal systolic and diastolic function were assessed, providing� and SR in ventricular systole, early diastole, and late diastole. AllRV and LV data are presented as peak values, but temporal data alsowere obtained, providing � and SR from throughout the entirecardiac cycle. The raw data were exported to a spreadsheet (Mi-crosoft Excel 2003) and were normalized to the percentage durationof systole and diastole, and then to allow comparisons amongsubjects, the data were further exported to GraphPad Prism 5software. All data points underwent cubic spline interpolation toprovide 300 data points for both systole and diastole as previouslydescribed.24 Net torsion was calculated at each of the normalizedpoints, allowing for a direct comparison of torsion throughout thecardiac cycle. Time to peak RV � and time to pulmonary valveclosure also was calculated from the raw data. LA data from thelateral wall was obtained, providing peak and temporal indices ofdeformation during ventricular systole, ventricular diastole, andatrial contraction as previously described.9
Data collected by our group before the present study havedemonstrated acceptable intraobserver variation in all peak LVand LA � and SR data.9 A further 20 subjects with 2 separateacquisitions were analyzed for RV intraobserver variation, giving
Figure 5. A and B, Two-dimensionalimage demonstrating increase in rightventricular size from 40 to 47 mm takenat end diastole as defined as the framefollowing closure of the atrioventricularvalve.
Oxborough et al Right Ventricular Function After an Ultramarathon 257
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from
coefficients of variation of 5%, 10%, 8%, and 8% for RV �, SRin ventricular systole, SR in early diastole, and SR in late diastole,respectively.
Statistical AnalysisAlthough predominantly an exploratory study, echocardiographicdata were analyzed for normality of distribution using aKolmogorov-Smirnov test, and then prerace versus postrace datawere compared using Student paired t tests. For all functional indicesthat were significantly altered postrace, bivariate correlational anal-ysis was used to establish the nature of any relationship to exercise-related changes in heart rate and preload (LVEDV) as well asassessed any correlation to training status, previous experience(ultramarathon races completed), and finishing times. Furtherchanges in RV structure and function were correlated with changesin LV and LA parameters. All statistical tests were applied usingcommercially available software (SPSS version 16), and a critical Pvalue was set to �0.05.
ResultsThe 16 participants completed the 161-km ultramarathonwith a mean�SD finishing time of 24:32�3:20 (range, 19:53to 29:46). Postrace body mass was reduced (69�12 to 67�12kg, P�0.001), heart rate was increased (58�7 to 72�7beats/min, P�0.001), and LVEDV was reduced (129�19 to119�19 mL, P�0.02). Systolic and diastolic blood pressures
were reduced postrace (118�14 to 107�9 mm Hg, P�0.009,and 76�7 to 72�8 mm Hg, P�0.042, respectively).
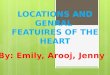
RV Structure and FunctionPrerace and postrace data for RV structural and functionalparameters are shown in Table 1. Postrace increases in RVcavity dimension at the RV outflow, inflow, and diastolicarea were 9% (P�0.002), 7% (P�0.027), and 9% (P�0.01).There was a 12% reduction in RVFAC (P�0.028), an 18%elevation in RV isovolumic relaxation time (P�0.04), and asignificant increase in LVEI (10%, P�0.006) postrace. PeakRV � was reduced by 12% postrace (P�0.004), whereas RVSR during early and late diastole were reduced but notsignificantly. Prerace time to peak RV � occurred at 106% ofsystole, whereas postrace peak RV � occurred later at 112%of systolic duration (ie, prerace peak RV � occurred 35 msafter pulmonary valve closure, whereas postrace peak RV �occurred 60 ms after pulmonary valve closure, suggesting inreal terms a 25-ms delay (P�0.045). Figure 2 shows thetemporal nature of RV � throughout the cardiac cycle beforeand after completion of the ultramarathon, further demon-strating the reduction in peak RV � with a slight delay inreaching maximum deformation.
The significant reduction in peak RV � was apparent acrossthe cohort (Figures 3 and 4). Individual plots in Figures 3 and4 highlight the fact that some subjects demonstrated morepronounced changes. Specifically 2 demonstrated exagger-ated increases in right-side heart cavity size, with the RVinflow increasing from 40 to 47 mm and 46 to 50 mm and RVdiastolic area increasing from 21 to 25 cm2 and 23 to 30 cm2
(Figure 5A and 5B). In these 2 subjects, the LVEI also wassignificantly elevated, with clear visual diastolic flattening ofthe septum (Figure 6). RV � also was dramatically alteredpostrace, reducing from 27% to 23% and 28% to 16% (Figure7). Importantly, removing these cases did not diminish thesignificant changes in the entire cohort.
LV and LA FunctionPostrace LV ejection fraction and stroke volume were re-duced by 8% (P�0.027) and 14% (P�0.004), respectively;transmitral E was reduced by 14%; E/A was reduced by 16%
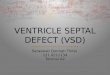
Figure 6. Two-dimensional image in the same patient. The image on the left demonstrates the circular left ventricular cavity and,hence, highlights the appropriate orientation, and the image on the right demonstrates septal flattening on the following cardiac cycle.
Figure 7. Temporal graphical representation from a single casedemonstrating an extreme reduction in RV strain after the ultra-marathon competition. Abbreviations as in Figure 2.
258 Circ Cardiovasc Imaging May 2011
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

(P�0.021); and E� was reduced by 18% (P�0.004), whereas Edeceleration time was increased by 15% (P�0.014) (Table 2).All LV and LA � data are presented in Table 3. Peak LVcircumferential, radial, and longitudinal � all were signifi-cantly reduced postrace (22%, 25%, and 11%, respectively)(Figure 8). Circumferential systolic SR and circumferentialearly diastolic SR were reduced by 9% and 27%, respec-tively. No significant change in radial and longitudinal SRdata were noted. LV torsion was reduced by 25% postrace asa consequence of reduction in basal (19%) and apical rotation(26%), although these results did not quite reach statisticalsignificance (Figure 8). Postrace, there was an 18% reductionin LA distension, a 13% reduction in conduit deformation,and a 10% increase in atrial contractility.
Correlation AnalysisA reduction in RVFAC and increased RV isovolumic relax-ation time were partially associated with an increase in heartrate at the postrace assessment (r�0.63, P�0.01, andr�0.69, P�0.03, respectively); however, we did not observesimilar correlations for any of the other changes in RVstructure and function. The reduction in LVEDV (as asurrogate for preload) correlated with a reduction in transmi-tral E velocity (r�0.653, P�0.01), E/E� (r�0.53, P�0.03),and radial � (r�0.61, P�0.01). Finishing time and thenumber of completed ultramarathons inversely correlatedwith the increase in RV inflow dimension and diastolic area(Table 4). Training status, as defined as the number of milesrun per week, inversely correlated with changes in LVEI(r�0.541, P�0.030). There was a lack of any other signifi-
cant correlations of training and performance to other LV orRV functional indices.
A decrease in RV � was correlated with decrements in LVlongitudinal early diastolic SR (r�0.56, P�0.024) and cir-cumferential early diastolic SR (r�0.482, P�0.05) postrace,suggesting a relationship between RV systolic function andLV diastolic function. Changes in LVEI also were moderatelyassociated with a reduction in RVFAC (r�0.457, P�0.034)and RV SRs (r�0.466, P�0.042). All significant correlationsare presented in Table 4.
DiscussionThe current exploratory study provides a comprehensiveevaluation of RV function immediately after ultraenduranceexercise. The key findings of an increase in RV size postraceas demonstrated by increased diameters at the outflow andinflow and an increase in diastolic area, a reduction in RVfunction postrace as identified by both standard 2D and MSTindices, an increase in LVEI postrace that suggests anincrease in RV pressure and volume, and the significantcorrelation between RV � and LV diastolic deformation helpto support the notion of an RV-LV interaction after prolongedexercise.
Previous evidence to support an increase in RV sizepostexercise is limited; however, Davila-Roman and col-leagues4 demonstrated marked RV dilatation and increasedpulmonary hypertension after a 161-km ultramarathon ataltitude; similarly, an increase in RV size also was shownafter the Hawaii Ironman Triathlon3 and Boston Marathon.8
In contrast, other investigators have not shown an increase inRV size after Ironman triathlon6 or marathon9 competitions.
Table 2. Standard Two-Dimensional and Doppler LV and LA Indices Before and After theUltramarathon Competition
Prerace Postrace
Parameter Mean�SE Range Mean�SE Range P
Heart rate, beats/min 58�1.8 43–72 72�1.8 60–83 �0.001
E velocity, m/s 0.76�0.03 0.44–0.94 0.65�0.04 0.43–0.91 0.004
A velocity, m/s 0.5�0.02 0.32–0.64 0.5�0.02 0.4–0.61 0.920
E/A ratio 1.57�0.11 0.85–2.50 1.32�0.08 0.80–1.73 0.021
E decel, ms 190�9.2 145–292 223�11.8 144–332 0.014
IVRT, ms 78�4.6 39–109 85�5.1 48–115 0.187
LVDd, mm 52�1.1 45–60 51�0.8 47–58 0.170
LVDs, mm 33�1.1 23–38 34�0.9 29–44 0.232
LA, mm 37�1.5 29–46 36�0.8 30–41 0.123
LA vol ES, mL 56�3.8 37–75 50�3.2 38–86 0.150
LV vol d, mL 129�4.8 95–155 119�4.8 83–144 0.002
LV vol s, mL 46�2.5 29–61 47�2.1 31–61 0.626
EF, % 65�1.0 58–71 60�1.6 48–72 0.027
SV, mL 83�2.8 66–104 71�3.9 48–103 0.004
CO, L/min 4.77�0.18 3.70–5.93 5.15�0.29 3.57–7.53 0.152
E�, cm/s 10.9�0.64 6.9–17.2 9.4�0.56 5.8–14.3 0.001
E/E� 7.3�0.29 5.2–9.4 7.1�0.41 5.4–11.7 0.724
A, atrial; CO, cardiac output; E, early diastolic flow velocity; E=, early diastolic myocardial velocity; EF, ejectionfraction; LA, left atrial; LV, left ventricular; LVDd, LV end-diastolic dimension; LVDs, LV end-systolic dimension; SV, strokevolume; vol ES, volume end systole; vol d, volume diastolic; vol s, volume systolic.
Oxborough et al Right Ventricular Function After an Ultramarathon 259
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Regardless of this disparity in the observed structural changesin the RV, all these studies report a negative impact on RVfunction. There is limited evidence to support the transient orpersistent nature of these changes. Many of these studies onlyevaluated subjects immediately after endurance exercise, withthe exception of La Gerche and colleagues6 and Neilan andcolleagues,25 who both demonstrated some residual changesat 1 week and 3 to 4 weeks postexercise, respectively.
Uniquely, the present study evaluated LVEI, which wassignificantly increased postrace across the cohort. This find-ing is consistent with increased RV pressure and volume, andfurthermore, the increased RV isovolumic relaxation timesupports a potential increase in RV afterload. A recent studyevaluating RV and LV ultrasound indices in patients withknown pulmonary arterial hypertension26 demonstrated stan-dard RV changes along with a reduction in LV torsion, LVcircumferential �, and LV longitudinal �. All these indiceswere reduced in the present study, and although this could bea consequence of an intrinsic impairment in LV function, it ispertinent to note that these also could be a consequence ofincreased RV afterload. Our data also support that of Neilanand colleagues,8 who demonstrated an increased pulmonary
artery pressure and RV dilatation after marathon running,although there was no measurable relationship between RVindices and LV filling. Assessment of pulmonary arterypressure has demonstrated consistently higher resting pulmo-nary pressures in an athletic population than in a controlgroup.27 The conventional measures of pulmonary hyperten-sion28 use the tricuspid regurgitant signal to estimate pulmo-nary artery pressure, but unfortunately, because of the trivialnature and inadequate continuous wave signal, this wasunable to be assessed in the present cohort.
In conjunction with seeing a reduction in peak RV �, wealso observed a slight delay in time to peak � relative topulmonary valve closure. This finding is interesting andconsistent with other work in this area. Chan Dewar andcolleagues29 demonstrated an increase in time to peak myo-cardial velocities from both the LV and RV after an 89-kmultramarathon, whereas other work demonstrated increasedtime to peak LV twist and untwist after prolonged exer-cise.9,13 From these data, it is difficult to speculate whetherany mechanism underpins this delay; however, both anintrinsic delay in contractility and response to an elevated RVafterload possibly could generate these findings.
Table 3. Peak LV and LA Strain Data Before and After the Ultramarathon Competition
Prerace Postrace
Parameter Mean�SE Range Mean�SE Range P
Circ �, % �20.2�1.0 �13.2 to �27.4 �15.7�0.9 �7.1 to �21.1 0.001
Circ SRs� �1.23�0.05 �0.84 to �1.62 �1.12�0.06 �0.88 to �1.61 0.022
Circ SRe� 1.87�0.13 1 to 2.92 1.37�0.11 0.47 to 2.02 0.018
Circ SRa� 0.59�0.05 0.28 to 0.99 0.61�0.06 0.28 to 1.14 0.800
Circ SRe�/SRa� 3.34�0.23 1.76 to 5.07 2.67�0.26 0.68 to 7.21 0.176
Basal rotation �6.5�0.70 �1.6 to �11.8 �5.24�0.70 �0.79 to �10.62 0.119
Apical rotation 10.24�2.09 3.4 to 34.5 7.57�1.14 2 to 15.5 0.235
Basal rotation rate S� �68.4�2.84 �48.8 to �93.9 �2.9�5.24 �35.3 to �107.6 0.507
Basal rotation rate E� 82.6�6.20 30 to 107.5 54.3�8.33 12.1 to 146.5 0.005
Apical rotation rate S� 65�7.26 27.9 to 132.8 61.8�6.28 21.3 to 99 0.581
Apical rotation rate E� �68.1�9.44 �20.8 to �171.7 �71.6�10.71 �21 to �175.7 0.782
Torsion 15.4�2.31 4.7 to 42 11.5�1.28 2.9 to 21.6 0.129
Radial �, % 53.4�3.6 19.3 to 78.3 40.3�3.5 26 to 67.2 0.009
Radial SRs� 1.97�0.14 1.35 to 3.26 1.91�0.09 1.48 to 2.74 0.723
Radial SRe� �1.92�0.18 �0.75 to �3.12 �1.76�0.17 �0.84 to �3.04 0.469
Radial SRa� �1.21�0.09 �0.52 to �1.84 �1.65�0.13 �0.81 to �2.51 0.007
Radial SRe�/SRa� 1.78�0.25 0.68 to 3.46 1.22�0.18 0.41 to 2.88 0.024
Long �, % �18.3�0.5 �13.7 to �21.7 �16.3�0.6 �12.3 to �19.7 0.012
Long SRs� �0.95�0.03 �0.72 to �1.18 �0.99�0.05 �0.64 to �1.41 0.419
Long SRe� 1.26�0.07 0.61 to 1.62 1.17�0.09 0.77 to 2.16 0.345
Long SRa� 0.68�0.04 0.41 to 0.95 0.70�0.03 0.50 to 0.94 0.707
Long SRe�/SRa� 1.92�0.13 1.03 to 3.24 1.74�0.18 0.82 to 3.60 0.354
LA �, % 45.2�3.9 21.1 to 67.7 36.9�3.9 15.8 to 67.4 0.047
LA SRs� 2.58�0.21 1.47 to 4.32 2.34�0.21 1.27 to 3.87 0.429
LA SRe� �2.62�0.22 �0.89 to �4.87 �2.27�0.16 �1.13 to �3.61 0.184
LA SRa� �2.22�0.26 �0.38 to �4.32 �2.48�0.26 �1.05 to �4.64 0.440
circ, circumferential; E=, early diastolic myocardial velocity; LA, left atrial; S=, systolic rotation rate. Otherabbreviations as in Table 1.
260 Circ Cardiovasc Imaging May 2011
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

The consistent findings across the cohort (with somemore-extreme cases) of changes to RV structure and functionfurther support the theory that the relative increase in strokework during endurance exercise is greater in the RV than inthe LV partly because of a proposed smaller rate of decreasein pulmonary resistance than in the systemic circulation.30 Arecent study by La Gerche and colleagues31 demonstratedincreased wall stress measured in the RV compared with theLV during endurance exercise, providing further evidence to
support RV adaptation in endurance athletes. Correlationanalysis in the present study that addressed the impact oftraining status, experience, and finish time provided interest-ing findings. The inverse correlations suggest that athleteswho had completed more ultramarathons and trained a greaternumber of miles per week had fewer changes in RV size andLVEI. We can speculate that experience and increasedtraining status may provide some physiological adaptationsthat may protect these athletes from negative RV changes inresponse to increased wall stress.
It is important to note that there was a positive, yet inversecorrelation between finishing time and changes in RV size,suggesting that a better finish time results in a greatermagnitude of RV enlargement. Although there is some debatepertaining to the impact of duration1 or intensity32 on cardiacchanges after prolonged exercise, the present findings supporta predominant effect from intensity and workload. Althoughthis correlation provides some evidence in support of thiseffect, changes in indices of RV function or LVEI did notdemonstrate similar significant correlations. It is clear thatfurther work on larger sample sizes may help to shed morelight on the chronic and acute nature of RV remodeling inendurance athletes.
Clinical PerspectiveThere is strong evidence to suggest that people who aregenerally physically active have increased life expectancy.33
Further, it is extremely important to note that all the athletes
Figure 8. Temporal representation of LV functional parameters. Abbreviations as in Figures 1 and 4.
Table 4. Major Significant Bivariate Correlations
BivariateCorrelation
Parameter r P
RV �:long SRe� 0.560 0.024
RV �:circ SRe� 0.482 0.050
LVEI:RVFAC �0.457 0.034
LVEI:RV SRs� �0.466 0.042
Finishing time:RV inflow �0.637 0.008
Finishing time:RV diastolic area �0.604 0.017
No. ultramarathons:RV inflow �0.577 0.002
No. ultramarathons:RV diastolic area �0.529 0.035
Training status:LVEI �0.541 0.030
RVFAC:heart rate �0.630 0.010
RVIVRT:heart rate 0.690 0.030
Abbreviations as in Tables 1 and 3.
Oxborough et al Right Ventricular Function After an Ultramarathon 261
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

in this study had completed numerous ultraendurance eventsbefore the competition studied, and resting RV structure andfunction was considered normal. The changes in RV and LVfunction after prolonged exercise are likely transient,9 repre-senting a “cardiac fatigue” process from which well-trainedathletes recover. Despite these important points, both theshort-term and the long-term effects of training and compet-ing in ultraendurance athletics has received little clinicalattention. Clearly, more work is needed to address any minorconcerns that arise from data such as that presented in thisarticle and in other similar studies.6,8,13
La Gerche and colleagues11 postulated a link betweenultraendurance exercise and an arrhythmogenic RV cardio-myopathy phenotype consistent with an “RV cardiomyopa-thy.” They suggested that repeated bouts of ultraenduranceexercise may well provide consecutive and repeated bouts ofRV dilatation and dysfunction that may “weaken the intersti-tial matrix of the RV,” providing a substrate for arrhythmo-genic origin. The present study demonstrates the markedimpact a single endurance event can have on RV structure andfunction and, therefore, may provide additional support to thepossible long-term outcomes of RV remodeling and fibro-sis.34,35 Direct evidence that this process of events happenscumulatively in ultraendurance athletes is still missing, butthis and other recent evidence36 suggest that we shouldinvestigate the long-term health consequences of ultraendur-ance activity.
LimitationsThis exploratory study was carried out on a relatively smallsample of mainly male subjects and compared changes inmultiple variables. Therefore, it is important to identify thepossible chance of statistical error and limited statisticalpower of the study. In view of this, the study has beenidentified as exploratory, and there is clear scope to developthis work in a larger sample with more-specific foci ofinterest. The changes were only observed immediately afterthe ultramarathon competition, and it would be of interest toestablish whether these were transient in nature. There issome conflicting evidence with regard to this issue9,25;therefore, follow-up echocardiograms may be warranted infuture work. Another important limitation is the inability toaccurately evaluate pulmonary artery pressure because of thelack or minimal amount of tricuspid regurgitation bothpreexercise and postexercise in all the subjects. It is clear thatto validate the findings of this study and to shed light on thepossible mechanism behind the RV changes, a more thoroughevaluation of pulmonary artery pressure is required. Futurestudies may use an ultrasound contrast agent or agitatedsaline to improve the quality of the tricuspid regurgitantsignal and, hence, reliability and accurate detection.37
ConclusionsFinishing a 161-km ultramarathon is associated with RVdilatation and dysfunction in recovery as demonstrated by2D, Doppler, and MST echocardiography. The causes of thisimpairment are unclear but could include the relative increasein RV afterload or an intrinsic reduction in myocardialfunction. LV systolic and diastolic function also is impaired
after an ultramarathon, and this is likely to be a consequenceof a combination of intrinsic reduction in function and RVinteraction. In view of the exploratory nature of this study, itis clear that the findings observed provide a justification forthe development of further work in this area.
AcknowledgmentsWe thank GE Medical and Dr Jack Taunton for their support of thisproject.
Sources of FundingThis work was supported by the Western States Endurance RunFoundation, Liverpool John Moores University, University of Leeds,Brunel University, University of British Columbia, the CanadaFoundation for Innovation, the Natural Sciences and EngineeringResearch Council of Canada, the Canadian Institutes of HealthResearch, and the Michael Smith Foundation for Health Research.
DisclosuresNone.
References1. Oxborough D, Birch K, Shave R, George K. “Exercise-Induced Cardiac
Fatigue”—a review of the echocardiographic literature. Echocardiogra-phy. 2010;27:1130–1140.
2. McKechnie J, Leary W, Noakes T, Kallmeyer J, MacSearraigh E, OliverL. Acute pulmonary oedema in two athletes during a 90-km running race.SA Med J. 1979;56:261–265.
3. Douglas PA, O’Toole M, Hiller W, Reichek N. Different effects ofprolonged exercise on the right and left ventricles. J Am Coll Cardiol.1990;15:64–69.
4. Davila-Roman V, Guest TM, Tuteur PG, Rowe WG, Ladenson JH, JaffeAS. Transient right but not left ventricular dysfunction after strenuousexercise at high altitude. J Am Coll Cardiol. 1997;30:468–473.
5. Carrio I, Serra-Grima R, Berna L, Estorch M, Martinez-Duncker C,Ordonez J. Transient alterations in cardiac performance after a six-hourrace. Am J Cardiol. 1990;65:1471–1474.
6. La Gerche A, Connelly KA, Mooney DJ, MacIsaac AI, Prior DL. Bio-chemical and functional abnormalities of left and right ventricularfunction following ultra-endurance exercise. Heart. 2008;94:860–866.
7. Oxborough D, Shave R, Middleton N, Whyte G, Forster J, George K. Theimpact of marathon running on ventricular function as assessed by 2D,Doppler and tissue Doppler echocardiography. Echocardiography. 2006;23:635–641.
8. Neilan TG, Januzzi JL, Lee-Lewandrowski E, Ton-Nu TT, Yoerger DM,Jassal DS, Lewandrowski K, Siegel AJ, Marshal JE, Douglas PS, LawlorD, Picard MH, Wood MJ. Myocardial injury and ventricular dysfunctionrelated to training levels among nonelite participants in the BostonMarathon. Circulation. 2006;114:2325–2333.
9. Oxborough D, Whyte G, Wilson M, O’Hanlon R, Birch K, Shave R,Smith G, Godfrey R, Prasad S, George K. A depression in left ventriculardiastolic filling following prolonged strenuous exercise is associated withchanges in left atrial mechanics. J Am Soc Echocardiogr. 2010;23:968–976.
10. Heidbuchel H, Hoogsteen J, Fagard R, Vanhees L, Ector H, Willems R,Van Lierde J. High prevalence of right ventricular involvement inendurance athletes with ventricular arrhythmias. Role of an electrophysi-ologic study in risk stratification. Eur Heart J. 2003;24:1473–1480.
11. La Gerche A, Robberecht C, Kuiperi C, Nuyens D, Willems R, de RavelT, Matthijs G, Heidbuchel H. Lower than expected desmosomal genemutation prevalence in endurance athletes with complex ventriculararrythmias of right ventricular origin. Heart. 2010;96:1268–1274.
12. Bleeker GB, Steendijk P, Holman ER, Yu C, Breithardt OA, KaandorpTA, Schalij MJ, van der Wall EE, Nihoyannopoulos P, Bax JJ. Assessingright ventricular function: the role of echocardiography and comple-mentary technologies. Heart. 2006;92:i19–i26.
13. Nottin S, Doucende G, Schuster I, Tanguy S, Dauzat M, Obert P.Alteration in left ventricular strains and torsional mechanics afterultralong duration exercise in athletes. Circ Cardiovasc Imaging. 2009;2:323–330.
262 Circ Cardiovasc Imaging May 2011
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

14. Vianna-Pinton R, Moreno C, Baxter C, Lee K, Tsang T, Appleton C.Two-dimensional speckle-tracking echocardiography of the left atrium:feasibility and regional contraction and relaxation differences in normalsubjects. J Am Soc Echocardiogr. 2009;22:299–305.
15. Grabskaya E, Spira C, Hoffmann R, Altiok E, Ocklenburg C, Hoffman R,Becker M. Myocardial rotation but not circumferential strain is transducerangle dependent: a speckle echocardiography study. Echocardiography.2010;27:809–814.
16. Korinek J, Wang J, Sengupta PP, Miyazaki Y, Kjaergaard J, McMahon E,Abraham TP, Belohlavek M. Two-dimensional strain—a Doppler-independent ultrasound method for quantitation of regional deformation:validation in vitro and in vivo. J Am Soc Echocardiogr. 2005;18:1247–1253.
17. Kalogeropoulos AP, Georgiopoulou VV, Howell S, Pernetz MA, FisherMR, Lerakis S. Evaluation of right intraventricular dyssynchrony bytwo-dimensional strain echocardiography in patients with pulmonary ar-terial hypertension. J Am Soc Echocardiogr. 2008;21:1028–1034.
18. Ho S, Nihoyannopoulos P. Anatomy, echocardiography, and normal rightventricular dimensions. Heart. 2006;92(suppl I):i2–i13.
19. Ryan T, Petrovic O, Dillon J, Feigenbaum H, Conley M, Armstrong W.An echocardiographic index for separation of right ventricular volumeand pressure overload. J Am Coll Cardiol. 1985;5:918–927.
20. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, PellikkaPA, Picard M, Roman M, Seward J, Shanewise J, Solomon S, Spencer K,St John Sutton M, Stewart W. Recommendations for chamber quantifi-cation: a report from the American Society of Echocardiography’sGuidelines and Standards Committee and the Chamber QuantificationWriting Group, developed in conjunction with the European Associationof Echocardiography, a branch of the European Society of Cardiology.J Am Soc Echocardiogr. 2005;18:1440–1463.
21. Garcia MJ, Thomas JD, Klein AL. New Doppler echocardiographicapplications for the study of diastolic function. J Am Coll Cardiol.1998;32:865–875.
22. Opdahl A, Helle-Valle T, Remme EW, Vartdal T, Pettersen E, Lunde K,Edvardsen T, Smiseth OA. Apical rotation by speckle tracking echocar-diography: a simplified bedside index of left ventricular twist. J Am SocEchocardiogr. 2008;21:1121–1128.
23. Sivesgaard K, Christensen SD, Nygaard H, Hasenkam JM, Sloth E.Speckle tracking ultrasound is independent of insonation angle and gain:an in vitro investigation of agreement with sonomicrometry. J Am SocEchocardiogr. 2009;22:852–858.
24. Burns A, La Gerche A, Prior D, MacIsaac A. Left ventricular torsionparameters are effected by load. Echocardiography. 2010;27:407–414.
25. Neilan TG, Yoerger DM, Douglas PS, Marshall JE, Halpern EF, LawlorD. Persistent and reversible cardiac dysfunction among amateur marathonrunners. EurHeart J. 2006;27:1079–1084.
26. Puwanet S, Park M, Popovic Z, Wilson Tang W, Farha S, George D,Sharp J, Puntawangkoon J, Loyd J, Erzurum S, Thomas J. Ventriculargeometry, strain and rotational mechanics in pulmonary hypertension.Circulation. 2010;121:259–266.
27. D’Andrea A, Naeije R, D’Alto M, Argiento P, Golia E, Cocchia R,Riegler L, Scarafile R, Limongelli G, Di Salvo G, Citro R, Caso P, RussoM, Calabro R, Bossone E. Range of pulmonary artery systolic pressureamong highly trained athletes: pulmonary artery systolic pressure inathletes. Chest. 2011;139:788–794.
28. Milan A, Magnino C, Veglio F. Echocardiographic indexes for the non-invasive evaluation of pulmonary haemodynamics. J Am Soc Echocardiogr.2010;23:225–239.
29. Chan Dewar F, Oxborough D, Shave R, Gregson W, Whyte G, Noakes T,George K. Evidence of increased electromechanical delay in the left andright ventricle after prolonged exercise. Eur J Appl Physiol. 2010;108:581–587.
30. Gurtner H, Wasler P, Fassler B. Normal values for pulmonary haemody-namics at rest and during exercise in man. Prog Resp Res. 1975;9:295–315.
31. La Gerche A, Heidbuchel H, Burns A, Mooney D, Taylor A, Pfluger H,Inder W, MacIsaac A, Prior D. Disproportionate exercise load and remod-elling of the athlete’s right ventricle. Med Sci Sports Exerc. 2011. [Epubahead of print].
32. Banks L, Sasson Z, Busaro M, Goodman J. Impaired left and rightventricular function following prolonged exercise in young athletes:influence of exercise intensity and responses to dobutamine stress. J ApplPhysiol. 2010;108:112–119.
33. Blair S, Kampert J, Kohl H, Barlow C, Macera C, Paffenbarger R,Gibbons L. Influences of cardiorespiratory fitness and other precursors oncardiovascular disease and all-cause mortality in men and women. JAMA.1996;276:205–210.
34. Harper R, Motram P. Exercise-induced right ventricular dysplasia/cardio-myopathy—an emerging condition distinct from arrythmogenic right ven-tricular dysplasia/cardiomyopathy. Heart Lung Circ. 2008;18:233–235.
35. La Gerche A, Prior DL, Heidbuchel H. Clinical consequences of intenseendurance exercise must include assessment of the right ventricle. J AmColl Cardiol. 2010;15:1263–1264.
36. Wilson M, O’Hanlon R, Prasad S, Deighan A, MacMillan P, OxboroughD, Godfrey R, Smith G, Sharma S, George K, Whyte G. Diverse patternsof myocardial fibrosis in lifelong, veteran endurance athletes. J ApplPhysiol. 2011. [Epub ahead of print].
37. Chahal N, and Senior R. Clinical applications of left ventricular opacifi-cation. J Am Coll Cardiol Img. 2010;3:188–196.
CLINICAL PERSPECTIVEIt is well established that exercise has a significant benefit on an individual’s health and longevity. The results of this studysuggest a negative impact on right ventricular morphology and function after a prolonged bout of extreme exercise, whichappears to influence changes in left ventricular filling. The acute changes are unlikely to require clinical intervention,particularly in view of their previously reported transient nature. That aside, the physiological adaptations identified in thisstudy could help to elucidate the recently observed long-term right ventricular adaptations observed in the ultraenduranceathlete. In view of this, there are 2 key points that the clinician may take from this study: (1) The findings should notinfluence any advice given to patients regarding the general health benefit of undertaking moderate, regular exercise, and(2) with the ever-increasing participation in extreme ultraendurance exercise, it is important in sports cardiology that theclinician is aware of these acute effects. These points provide greater insight that could influence patient managementduring and after such events, if required.
Oxborough et al Right Ventricular Function After an Ultramarathon 263
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Charlesworth, Heather Foulds, Martin D. Hoffman, Karen Birch and Keith GeorgeDavid Oxborough, Robert Shave, Darren Warburton, Karen Williams, Adele Oxborough, Sarah
Tracking EchocardiographyExercise: Exploratory Insights From Conventional Two-Dimensional and Speckle
Dilatation and Dysfunction of the Right Ventricle Immediately After Ultraendurance
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2011 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.110.9619382011;4:253-263; originally published online March 18, 2011;Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/4/3/253World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 29, 2018http://circim
aging.ahajournals.org/D
ownloaded from