Embed Size (px)
Citation preview

CASE REPORT
Dihydrolipoamide dehydrogenase (DLD) deficiencyin a Spanish patient with myopathic presentationdue to a new mutation in the interface domain
Ester Quintana & Mercé Pineda & Aida Font &Maria Antonia Vilaseca & Frederic Tort &Antonia Ribes & Paz Briones
Received: 13 May 2010 /Revised: 30 June 2010 /Accepted: 1 July 2010# SSIEM and Springer 2010
Abstract We present a 32-year-old patient who, from age7 months, developed photophobia, left-eye ptosis andprogressive muscular weakness. At age 7 years, she showednormal psychomotor development, bilateral ptosis andexercise-induced weakness with severe acidosis. Basalblood and urine lactate were normal, increasing dramati-cally after effort. PDHc deficiency was demonstrated in
muscle and fibroblasts without detectable PDHA1 muta-tions. Ketogenic diet was ineffective, however thiaminegave good response although bilateral ptosis and weaknesswith acidosis on exercise persisted. Recently, DLD geneanalysis revealed a homozygous missense mutation, c.1440A>G (p.I480M), in the interface domain. Both parents areheterozygous and DLD activity in the patient’s fibroblastsis undetectable. The five patients that have been reportedwith DLD-interface mutations suffered fatal deteriorations.Our patient’s disease is milder, only myopathic, moresimilar to that due to mutation p.G229C in the NAD+-binding domain. Two of the five patients presentedmutations (p.D479Vand p.R482G) very close to the presentcase (p.I480M). Despite differing degrees of clinicalseverity, all three had minimal clues to DLD deficiency,with occasional minor increases in α-ketoglutarate andbranched-chain amino acids. In the two other patients,hypertrophic cardiomyopathy was a significant feature thathas been attributed to moonlighting proteolytic activity ofmonomeric DLD, which can degrade other mitochondrialproteins, such as frataxin. Our patient does not havecardiomyopathy, suggesting that p.I480M may not affectthe DLD ability to dimerize to the same extent as p.D479Vand p.R482G. Our patient, with a novel mutation in theDLD interface and mild clinical symptoms, further broadensthe spectrum of this enzyme defect.
AbbreviationsDLD Dihydrolipoamide dehydrogenasePDHc Pyruvate dehydrogenase complexKGDC α-Ketoglutarate dehydrogenase complexBCKDC Branched-chain α-keto acid dehydrogenase
complex
Communicated by: Garry Brown
References to electronic databases: Dihydrolipoamide dehydrogenasedeficiency: OMIM 238331. Lipoamide dehydrogenase: EC 1.8.1.4.
Competing interest: None declared.
E. Quintana :A. Font : F. Tort :A. Ribes : P. BrionesSección de Errores Congénitos del Metabolismo,Servicio de Bioquímica y Genética Molecular, Hospital Clínic,Instituto de Bioquímica Clínica,Barcelona, Spain
M. Pineda :M. A. VilasecaServicios de Bioquímica y Neurología Pediátrica,Hospital Sant Joan de Deu,Barcelona, Spain
M. Pineda : F. Tort :A. Ribes : P. BrionesCIBER de Enfermedades Raras (CIBERER),Barcelona, Spain
P. BrionesConsejo Superior de Investigaciones Científicas,Barcelona, Spain
P. Briones (*)Instituto de Bioquímica Clínica,Edificio Helios III, c/ Mejia Lequerica s/n,08028 Barcelona, Spaine-mail: [email protected]
DOI 10.1007/s10545-010-9169-4J Inherit Metab Dis (201 ) 3 (Suppl 3):S315–S3190 3
/Published online: 21 July 2010

Introduction
Mammalian dihydrolipoamide dehydrogenase, known asE3 (dihydrolipoamide:NAD+ oxidoreductase, EC 1.8.1.4),is the common flavoprotein component of the threemitochondrial α-keto acid dehydrogenase multienzymecomplexes: pyruvate dehydrogenase complex (PDHc), α-ketoglutarate dehydrogenase complex (KGDC) andbranched-chain α-keto acid dehydrogenase complex(BCKDC), where it catalyses the third stage of the reaction(Patel and Roche 1990; Cameron et al. 2006). E3 is also acomponent of the glycine cleavage system (Kikuchi andHigara 1982), another mitochondrial enzyme complex,where it is known as protein L.
The active enzyme is a homodimer of 51 kDa subunitswith four distinctive subdomain structures (FAD binding,NAD+ binding, central and interface domains; Hong et al.1997). The DLD gene, located on chromosome 7q31–32, isapproximately 20 kb long and contains 14 exons (Grafakouet al. 2003).
In this report, we describe a Spanish patient with PDHcdeficiency and a myopathic presentation attributable to anew mutation in the interface domain of DLD.
Materials and methods
Patient
The patient is a girl born in 1977 and first investigated byour group at 7 years of age. There is a strong family historyof consanguinity, and her parents are second cousins. Anaunt died at 8 years of age with ptosis, photophobia andwalking difficulties; a cousin suffers from convulsive crisesand mental retardation, and the patient’s mother has ptosis.In addition, the patient’s brother has mental retardation andcerebral palsy, attributable to neonatal seizures.
The perinatal history was unremarkable: she sat at6 months, walked at 9 months, and controlled sphinctersat 14 months. From the 7th month she developedphotophobia and ptosis of the left eye. By 3 years of age,the ptosis was bilateral and she had developed fatigabilityon exercise that increased to the point where she wasalmost unable to walk alone. This was associated withgeneralised muscular weakness and cramps. Limb muscleswere normal at rest, but tone and strength diminishedmarkedly on exercise.
At 7 years of age, she was of normal weight and height.She had bilateral ptosis, brisk reflexes and normal strengthat rest, however after walking 50 m, strength was reducedto 3/5 and she developed severe acidosis. EEG, EMG,nerve conduction velocity and cardiological studies werenormal. Her cognitive level was good, but cranial MRI
showed bilateral hyperintensity of the pallidum on T2-weighted images, with slight abnormality of periventricularwhite matter.
Blood lactic acid concentration at rest was 1.93 mmol/Land increased after effort to 5.30 (controls: 0.55–1.80);pyruvic acid concentration was 0.074 mmol/L under basalconditions and 0.098 after effort (controls: 0.030–0.100). Inurine, lactic acid at rest was 65–288 mmol/mol creatinine(controls: 37–50), and after effort it increased to4,926 mmol/mol creatinine. Muscle and skin biopsies wereperformed for enzyme determinations, which led to thediagnosis of PDHc deficiency.
A ketogenic diet was tried, without benefit. Withthiamine supplementation there was a good response,however at present, aged 32 years, slight bilateral ptosispersists, although there is much less fatigability andacidosis after exercise. She continues to receive high dosesof thiamine (2,700 mg/day) and carnitine (3 g/day).
Enzyme studies
PDHc activity was determined in muscle and/or fibroblastsby measuring 14CO2 production from [1-14C]-pyruvate afteractivation with Ca++ and Mg++ and addition of carnitineand cytochrome C (Sperl et al. 1990, modified as describedin Guitart et al. 2009).
Substrate oxidation by intact fibroblasts was alsoevaluated by measuring 14CO2 production with [1-14C]-and [2-14C]-pyruvate, [1-14C]-leucine and [14C]-glutamate(Willems et al. 1978).
Western blotting
Western blotting was performed to test for the presence ofthe PDHc subunits. Protein homogenate was resolved in a10% polyacrylamide/SDS gel and then transferred to anitrocellulose membrane, incubated with primary rabbitantibody against subunits of the complex (kindly providedby Dr Ruitenbeek, Radboud University Nijmegen MedicalCentre, Nijmegen, The Netherlands), and finally detectedby chemiluminescence using the ECL system (AmershamBiosciences, Piscataway, NJ, USA).
Molecular analysis
Total RNA was extracted from patient and control fibro-blasts using QIAshredder and RNeasy kits (Qiagen, Hilden,Germany). Single-stranded cDNA was obtained usingoligo-dT primers and M-MLV Reverse Transcriptase,RNase H Minus, Point Mutant (Promega, Madison, WI,USA) according to the manufacturer’s protocol.
Standard PCR techniques were employed with self-designed specific primers (sequences available on request).
J Inherit Metab Dis (201 ) 3 (Suppl 3):S315–S3190 3 S316

The amplified products were analysed by electrophoresis in2% agarose gels. The same PCR primers were used forsequencing.
To confirm the change observed in cDNA, thecorresponding sections of the gene were also sequenced ingenomic DNA. Nucleotide numbering is according to thereference sequence Genbank RefSeq NM_000108.
Results and discussion
We describe a new patient with DLD deficiency and a mildclinical presentation. The patient, first daughter of consan-guineous parents, had an unremarkable perinatal history.She developed her first symptoms at 7 months of age, withphotophobia and ptosis in the left eye. Neuromuscularsymptoms increased, with ptosis of the right eye, walkingdifficulties and generalised muscular weakness developingby 6 years of age. Her psychological development wasnormal and she performed well at school.
Biochemical analysis showed episodic increases in bloodlactate (up to 9.5 mmol/L) and pyruvate (up to 0.156 mmol/L)concentrations, but only after exercise tests. There weremild sporadic increases in plasma branched-chain aminoacids and urinary α-ketoglutarate excretion, unrelated tothe exercise tests. Muscle respiratory chain activitiesshowed normal results (data not shown), while fibroblastPDHc activity was mildly decreased, with PDH-E1activity in the lower control range (Table 1). The ratesof [1-14C]- and [2-14C]-pyruvate and [1-14C]-glutamateoxidation by her fibroblasts were decreased to 71, 46 and70% of the lowest control respectively. Western blotanalysis showed no alterations of PDHc components (datanot shown).
As PDH-E1α is the most commonly affected subunit inPDHc deficiency (Robinson 2001) and slight deficienciescan have pathological significance (Patel and Harris 1995),mutation analysis of the PDHA1 gene was performedwithout detecting any abnormality.
Following the diagnosis of PDHc deficiency, a ketogenicdiet was introduced at the age of 7 years, however this wassoon stopped because of lack of response and poorcompliance. The patient also received a trial of cofactors,with very good response to thiamine. A ketogenic diet wastried on two further occasions, again without additionalbenefit, while thiamine has been clearly beneficial since itsintroduction.
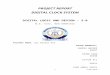
We recently performed a general review of our PDH-deficient patients without mutations in PDHA1. To achievea diagnosis, we have implemented mutation analysis of theother genes of the PDHc (PDHB, DLAT, DLD and PDHX).In this patient we detected a homozygous change c.1440A>G (p.I480M) in the DLD gene, which is located in theinterface domain (see Fig. 1). The change was confirmed byanalysis of exon 13 in genomic DNA. It was not present in104 control alleles, and both parents were shown to beheterozygous carriers. Neither the patient’s younger sisternor brother carry the mutation. Mental retardation andcerebral palsy in the brother have been attributed toneonatal seizures, although other autosomal genes maywell be involved given the high degree of familialconsanguinity.
Once the mutation was identified, we analysed E3(dihydrolipoamide dehydrogenase) activity in the patient’sfibroblasts and found it undetectable (see Table 1); unfor-tunately muscle tissue was unavailable for this investiga-tion. We also analysed the rate of leucine oxidation byfibroblasts, which was clearly deficient (40% of the lowestcontrol).
To our knowledge, five other patients with DLDdeficiency and mutations located in the interface domainhave been reported. All were severely affected, and threedied before the 3rd year of life (Odièvre et al. 2005; Liu etal. 1993; Hong et al 1996). A fourth patient was reported atage 9 months with severe neurodegenerative disease (Shanyet al. 1999), and the last patient (Grafakou et al. 2003), afteran uneventful 1st year of life, presented with failure tothrive, developmental delay and regression at the age of
Patient Controls
Enzyme activities (nmol min−1 mg−1 protein)
Pyruvate dehydrogenase 0.33 0.34–2.60
Pyruvate decarboxylase (PDH-E1 component) 0.05 >0.04
Lipoamide dehydrogenase (PDH-E3 component) Undetectable 20–97
Citrate synthase 24 11–29
Substrate oxidation rates (nmol h−1 mg−1 protein)
1-14C-Pyruvate 6 8–36
2-14C-Pyruvate 1.3 2.8–24.0
1-14C-Glutamate 4.0 5.7–25.0
1-14C-Leucine 0.2 0.5–1.2
Table 1 Enzymatic studies inpatient’s fibroblasts
S317J Inherit Metab Dis (201 ) 3 (Suppl 3):S315–S3190 3

2 years associated with stroke-like episodes, Leigh syn-drome and spastic tetraparesis. Our patient is now 32 yearsold and is much less severely affected; her symptomsstarted at 7 months of age with ptosis and weakness andresulted in exercise intolerance with extreme fatigue, butwith a good response to thiamine. A similar clinical picturewith exertional fatigue and without neurological involve-ment was described for a group of Ashkenazi Jewishindividuals homozygous for mutation p.G229C (Shaag etal. 1999).
Two of the reported patients with mutations in the interfacedomain (Fig.1) have homozygous changes, p.D479V(Shany et al 1999) and p.R482G (Odièvre et al. 2005),in amino acid residues which are very close to that of ourpatient (p.I480M). In these patients, in spite of severeclinical deterioration and lactic acidemia, there were onlyoccasional increases in levels of α-ketoglutarate andbranched-chain amino acids. It has been proposed thatthe lack of significant evidence of BCKDC and KGDCdeficiency is due to differences in the interaction of E3with PDC and KGDC or BCKDC (Odièvre et al. 2005).In our patient, biochemical clues to DLD deficiency were
also minimal, with elevations of lactate only after an effortand very sporadic and minor increases in α-ketoglutarateand branched-chain amino acids. It is of note that the twopatients reported earlier presented with hypertrophiccardiomyopathy, while our patient has never had anycardiac abnormalities. This may be because the p.I480Mmutation does not affect DLD as severely as p.D479V orp.R482G. In fact the change of the non-reactive hydro-phobic isoleucine to methionine, another hydrophobicamino acid, does not constitute a substantial change andmay not dramatically alter the interface interactionsbetween the E3 monomers.
With this report we describe a new DLD-deficientpatient with a novel homozygous mutation in theinterface domain of DLD. Her relatively mild clinicalsymptoms extend the spectrum of clinical features of thisdeficiency.
Acknowledgements We are grateful to the patient and her family fortheir kind collaboration. We acknowledge the expert technicalassistance of Sonia Moliner. This research was supported in part bySpanish Ministerio de Sanidad (FIS) grants PI 08/0307.
Patient Heterozygous father Heterozygous mother Healthy brother
5’ 3’
p.G229C# p.E375K
p.I480M #,*
p.D479V #
p.P488L
p.R495G
MTS FAD NAD central interface
p.Y35X
p.I47Tp.K72E
p.G136delc.875+1G>A
p.M361Vp.I393T
p.R482G#
a
b
c
Fig. 1 a Genomic DNA sequence of the DLD gene from the patient,her parents and her brother. The frame indicates the position of thechange. b Alignment of the DLD gene between species and the changein our patient. Data obtained from http://www.ncbi.nlm.nih.gov/. c
Previously published mutations in DLD; mutations marked with hashsymbol (#) have been found in homozygous form, and the asteriskdenotes the mutation identified in this study. (The figure is modifiedfrom Cameron et al. 2006)
J Inherit Metab Dis (201 ) 3 (Suppl 3):S315–S3190 3 S318

References
Cameron JM, Levandovskiy V, MacKay N et al (2006) Novelmutations in dihydrolipoamide dehydrogenase deficiency in twocousins with borderline-normal PDH complex activity. Am JMed Genet 140:1542–1552
GrafakouO, Oexle K, van den Heuvel L et al (2003) Leigh syndrome dueto compound heterozygosity of dihydrolipoamide dehydrogenasegenemutations. Description of the first E3 splice site mutation. Eur JPediatr 162:714–718
Guitart M, Andreu AL, García-Arumi E et al (2009) Fatp1 localizes tomitochondria and enhances pyruvate dehydrogenase activity inskeletal myotubes. Mitochondrion 9:266–272
Hong YS, Kerr DS, Craigen WT, Tan J, Pan Y, Lusk M, Patel MS(1996) Identification of two mutations in a compound heterozygouschild with dihydrolipoamide dehydrogenase deficiency. Hum MolGenet 5:1925–1930
Hong YS, Kerr DS, Liu TC, Lusk M, Powell BR, Patel MS (1997)Deficiency of dihydrolipoamide dehydrogenase due to twomutant alleles (E340K and G101del). Analysis of a family andprenatal testing. Biochim Biophys Acta 1362:160–168
Kikuchi G, Higara K (1982) The mitochondrial glycine cleavagesystem. Unique features of the glycine decarboxylation. Mol CellBiochem 45:137–149
Liu TC, Kim H, Arizmendi C, Kitano A, Patel MS (1993)Identification of two missense mutations in a dihydrolipoamidedehydrogenase-deficient patient. PNAS 90:5186–5190
Odièvre MH, Chretien D, Munnich A et al (2005) A novel mutation inthe dihydrolipoamide dehydrogenase E3 subunit gene (DLD)resulting in an atypical form of α-ketoglutarate dehydrogenasedeficiency. Hum Mutat 25:323–324
Patel MS, Harris RA (1995) Mammalian α-keto acid dehydrogenasecomplexes: gene regulation and genetic defects. FASEB J9:1164–1172
Patel MS, Roche TE (1990) Molecular biology and biochemistry ofpyruvate dehydrogenase complexes. FASEB J 4:3224–3233
Robinson BH (2001) Lactic acidemia: disorders of pyruvate carbox-ylase and pyruvate dehydrogenase. In: Scriver CR, Beaudet AL,Sly WS, Valle D (eds) The metabolic and molecular bases ofinherited disease. McGraw-Hill, New York, pp 2275–2295
Shaag A, Saada A, Berger I et al (1999) Molecular basis of lipoamidedehydrogenase deficiency in Ashkenazi Jews. Am J Med Genet82:177–182
Shany E, Saada A, Landau D, Shaag A, Hershkowitz E, Elpeleg ON(1999) Lipoamide dehydrogenase deficiency due to novelmutation in the interface domain. Biochem Biopys Res Commun262:163–166
Sperl W, Ruitenbeek W, Kerkhof CM et al (1990) Deficiency of thealpha and beta subunits of pyruvate dehydrogenase in a patientwith lactic acidosis and unexpected sudden death. Eur J Pediatr149:478–492
Willems HL, Dekort TFM, Trijbels FJM, Monnens LAH, VeerkampJH (1978) Determination of pyruvate oxidation rate and citricacid cycle activity in intact human leukocytes and fibroblasts.Clin Chem 24:200–203
S319J Inherit Metab Dis (201 ) 3 (Suppl 3):S315–S3190 3