Embed Size (px)
Citation preview

Eur Radiol (2007) 17: 3031–3037DOI 10.1007/s00330-007-0717-8 MAGNETIC RESONANCE
Petra MürtzCarsten KrautmacherFrank TräberJürgen GiesekeHans H. SchildWinfried A. Willinek
Received: 27 November 2006Revised: 7 May 2007Accepted: 15 June 2007Published online: 24 July 2007# Springer-Verlag 2007
Diffusion-weighted whole-body MR imaging
with background body signal suppression:
a feasibility study at 3.0 Tesla
Abstract The purpose was to providea diffusion-weighted whole-bodymagnetic resonance (MR) imagingsequence with background body sig-nal suppression (DWIBS) at 3.0 Tesla.A diffusion-weighted spin-echo echo-planar imaging sequence was com-bined with the following methods offat suppression: short TI inversionrecovery (STIR), spectral attenuatedinversion recovery (SPAIR), andspectral presaturation by inversionrecovery (SPIR). Optimized se-quences were implemented on a 3.0-and a 1.5-Tesla system and evaluatedin three healthy volunteers and sixpatients with various lesions in theneck, chest, and abdomen on the basisof reconstructed maximum intensityprojection images. In one patient withmetastases of malignant melanoma,DWIBS was compared with 18
F-fluorodeoxyglucose positron emis-
sion tomography (FDG-PET). Goodfat suppression for all regions anddiagnostic image quality in all casescould be obtained at 3.0 Tesla with theSTIR method. In comparison with 1.5Tesla, DWIBS images at 3.0 Teslawere judged to provide a better lesion-to-bone tissue contrast. However,larger susceptibility-induced imagedistortions and signal intensity losses,stronger blurring artifacts, and morepronounced motion artifacts degradedthe image quality at 3.0 Tesla. A goodcorrelation was found between themetastases as depicted by DWIBS andthose as visualized by FDG-PET.DWIBS is feasible at 3.0 Tesla withdiagnostic image quality.
Keywords Diffusion magneticresonance imaging . Whole bodyimaging . High field . 3.0 Tesla
Introduction
Recently, a new magnetic resonance (MR) technique calledDWIBS (diffusion-weighted whole-body imaging withbackground body signal suppression) has been introducedfor 1.5-Tesla MR scanners by Takahara et al. [1]. In theDWIBS approach, multiple thin axial slices with a highnumber of signal averages are acquired during freebreathing, and STIR (short TI inversion recovery) fatsuppression is used. It has been reported that image qualityobtained by DWIBS at 1.5 Tesla allows three-dimensional(3D) reconstructions like maximum intensity projection(MIP), on which 3D distributions of disseminated tumors,lymph nodes or abscesses can be recognized [1].
The clinical evaluation of the DWIBS method at 1.5Tesla is still a subject of research. Initial studies withpreliminary results focused on tumor detection [2, 3], lymphnode imaging [4], and imaging of bone metastases [5].
Up to now, the DWIBS technique has only beendescribed for MR systems operating at 1.5 Tesla. At 3.0Tesla, only first applications of conventional diffusion-weighted imaging (DWI) have been performed to parts ofthe body [6, 7]. Conventional DWI, where SPIR (spectralpresaturation by inversion recovery) fat suppression is usedand the images are acquired either during breath-hold or incombination with respiratory triggering, partly withadditional cardiac triggering [8], is not applicable forwhole-body scanning. The aim of this work was the
P. Mürtz (*) . C. Krautmacher .F. Träber . J. Gieseke . H. H. Schild .W. A. WillinekDepartment of Radiology,University of Bonn,Sigmund-Freud-Straße 25,53105 Bonn, Germanye-mail: [email protected].: +49-228-28714496Fax: +49-228-28716093
J. GiesekePhilips Medical Systems,P.O. Box 10000, 5680 DABest, The Netherlands
P. MürtzRadiologische Klinik der UniversitätBonn,Sigmund-Freud-Straße 25,53105 Bonn, Germany

implementation and first evaluation of a DWI sequence,which is suitable for whole-body scanning at 3.0 Tesla.
Materials and methods
Subjects
This study was performed after approval of the localinstitutional review board. Written informed consent wasobtained from all participants. Three healthy volunteerswithout a history of disease of the head/neck, chest, andabdomen (one female, two male; 23–40 years) and sixpatients (three female, three male; 45–76 years) wereincluded in this study. Patients were suspected of havingmetastases of neuroendocrine carcinoma (n=1), bronchialcarcinoma (n=1), non-Hodgkin lymphoma (n=3) andmelanoma (n=1).
MR imaging
At 3.0 Tesla, theMR imagingwas performed on awhole-bodysystem (Achieva, Philips Medical Systems, Quasar Dualgradient system: 80 mT/m maximum amplitude, 0.16 msminimal rise time, 200 T/m/s maximum slew rate) using six-and eight-element phased array surface coils (SENSE-cardiac,SENSE-NV-8). At 1.5 Tesla, a whole-body system (Intera,PhilipsMedical Systems, gradient system: 30mT/mmaximumamplitude, 0.2 ms minimal rise time, 150 T/m/s maximumslew rate) was used with eight- and sixteen-element phasedarray surface coils (SENSE-body, SENSE-NV-16).
With both scanners, a diffusion-weighted (DW) single-shot spin-echo (SE) echo-planar imaging (EPI) sequence(parameters see Table 1) was implemented in order toacquire image series of 60 transversal slices during freebreathing containing one image without diffusion weight-ing and three images with diffusion gradients in orthogonaldirections for each slice. Additionally, an isotropic DWimage was provided for each slice by the scanner calculatedfrom the three different DW images by pixelwise averagingof the signal intensities. At both field strengths, parallel
imaging with reduction (SENSE) factor 2 was used to reducethe echo train length. Depending on the gradient system, at3.0 Tesla shorter values of echo time TE, diffusion gradientduration δ and distance Δ, and bandwidth in EPI frequencydirection could be reached (see Table 1).
The DWI sequences from both scanners were combinedwith STIR, SPAIR (spectral attenuated inversion recovery),and SPIR fat suppression techniques. SPIR and SPAIR usefrequency selective inversion pulses aligned to the reso-nance frequency of fat. In contrast to SPIR, for SPAIR theinversion pulse is of adiabatic shape and with adjustabledelay time TI, which makes SPAIR relatively insensitive toradio frequency (B1) inhomogenities. However, bothmethods are sensitive to B0 inhomogenities, which maybe a problem for regions with strong susceptibility differ-ences. STIR is an inversion recovery method with aninversion time (TI), at which the longitudinal magnetizationof fat reaches zero, which is obtained for TI=ln2×T1 (forTR>>T1), where T1 is the spin lattice relaxation time of fat.Therefore, STIR is relatively insensitive against magneticfield inhomogenities, but yields lower signal-to-noise ratios(SNR), and signals from other substances with short T1relaxation are also suppressed. Thus, STIR should be notused after gadolinium contrast agent supply. However, theadditive T1- and T2-weighting of the images may have thefollowing advantage: most lesions have increased freewater content and thus show prolonged T1 and T2relaxation times [9], whereas signals of the intestines aresuppressed due to their short T1 relaxation times. Theoptimum values of TI for the multislice STIR and SPAIR fatsuppression have been determined in a previous experimenton abdominal imaging of four healthy volunteers (unpub-lished data). The obtained TI values are given in Table 2,together with the repetition times (TRs) and the acquisitiontimes. At 3.0 Tesla, TR and as a consequence theacquisition times are considerably longer than at 1.5 Tesladue to specific absorption rate (SAR)-related restrictions.
The data of each image series were transferred to acommercially available postprocessing workstation (ViewForum, Philips Medical Systems). A MIP reconstructionfollowed by gray scale inversion was carried out for theisotropic DW images. In the following, these inverted MIP
Table 1 Parameters of the useddiffusion-weighted single-shotSE-EPI sequence at 1.5 and 3.0Tesla
1.5 Tesla 3.0 Tesla
Field of view/orientation 400×314 mm/transversal
Number of slices/thickness/gap 60/4 mm/0 mm
Matrix/resolution 112×86/3.6×3.7 mm
Echo time (TE)/repetition time (TR) 65 ms/>4,900 ms 41 ms/>7,000 ms
EPI-/half-Fourier-/SENSE-factor 47/0.6/2
Bandwidth in EPI frequency direction 2,688 Hz 3,176 Hz
Number of diffusion gradients 3 (orthogonal directions)
b-values (number of averages) 0 s/mm2 (NSA=2) and 1,000 s/mm2 (NSA=6)
Diff. gradient duration δ/distance Δ 24.2 ms/32.1 ms 10.0 ms/19.6 ms
3032

images are referred to as DWIBS images. In the DWIBSimages, dark areas appear for restricted diffusion, corre-sponding to low values of the apparent diffusion coefficient(ADC), or for long T1 and/or T2 relaxation times.
Comparison of DWI sequences with STIR, SPAIRand SPIR fat suppression at 3.0 Tesla
The DW-SE-EPI sequences with different methods of fatsuppression (STIR, SPAIR, and SPIR) were tested at 3.0Tesla on one healthy volunteer (male, 40 years) and twopatients (one female, 54 years; one male, 49 years) in thehead/neck region, chest, and abdomen. Fat suppression ofDWIBS images was judged by two readers (P.M., W.W.) inconsensus making use of a three-point scale rating thedegree of fat suppression as “good”, “fair” or “poor”.“Good” means that marginal fat signal on original DWimages was so well suppressed that central parts of the bodyinDWIBS images were clearly visible. “Fair”means that fatsuppression on DW images was not optimal. Image qualityof DWIBS was reduced by residual fat signal superimposedon other parts of the anatomy impairing its visibility. “Poor”means that fat signal on DW images was not adequatelysuppressed or even undesired suppression of non-fattytissue occurred. DWIBS images were in this case of non-diagnostic image quality, because central objects were fullyobscured or of diminished signal intensity.
Comparison between 3.0 Tesla and 1.5 Tesla
In two healthy volunteers (one female, 40 years; one male,23 years) and two patients (male, 49 and 71 years), DWimages were acquired both at 3.0 Tesla and at 1.5 Tesla byusing STIR fat suppression. In the isotropic DW images, aquantitative analysis of the contrast between lymph nodesand adjacent fatty tissue was performed by determinationof (SIlym-SIfat)/(SIlym+SIfat), where SIlym is the averagesignal intensity within a region of interest placed in alymph node and SIfat is the average residual/unsuppressedsignal intensity within a ROI placed in the fatty tissueadjacent to the lymph node (both ROIs of the same size).Moreover, the reconstructed DWIBS images were com-
pared in three ways. First, the contrast between lesions andbones (vertebral bodies and ribs) was judged by visualscoring of two readers (P.M., W.W.) in consensus using thefollowing scale: “3” for higher, “2” for similar, and “1” forlower contrast at 3.0 Tesla compared with 1.5 Tesla.Second, all DWIBS images were rated by the two readers(P.M., W.W.) in consensus with respect to susceptibilityartifacts (such as signal loss and geometric distortion),blurring artifacts, and motion artifacts on a three point scalecategorizing the degree of artifacts as weak (“3”), medium(“2”), and strong (“1”). Third, in order to investigatesensitivity to small lesions we measured the diameters ofsmall lesions discernable at the DWIBS images at 1.5 Teslaand explored their detectability at 3.0 Tesla.
Clinical applications
Six patients (three female, three male; 45–76 years) withvarious lesions in the neck, chest, and abdomen wereexamined with DWIBS at 3.0 Tesla to evaluate feasibility.Image quality was judged by the two readers (P.M., W.W.)in consensus with respect to fat suppression, blurring, andmotion and susceptibility artifacts. The readers decidedwhether DWIBS images were of diagnostic (score “2”) ornon-diagnostic quality (score “1”). In one patient, 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) images were available for intraindividual comparisonwith the DWIBS images.
Results
Comparison of DWI sequences with STIR, SPAIRand SPIR fat suppression at 3.0 Tesla
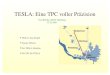
DWIBS images acquired by using STIR showed “good” fatsuppression and the contours of all investigated regions,head/neck region, chest, and abdomen, were clearly visible.The use of SPAIR and SPIR at 3.0 Tesla resulted in DWIBSimages with “poor” fat suppression in the head/neckregion, “fair” fat suppression in the chest and “good” fatsuppression in the abdomen (see Fig. 1). For the furtherexperiments, we used STIR fat suppression.
Table 2 Values of inversion recovery times (TI) and repetition times (TR) used for the different fat suppression methods and differentacquisition times of the sequences for 1.5 and 3.0 Tesla
1.5 Tesla 3.0 Tesla
STIR: TI 180 ms 260 ms
TR/acquisition time 4,961 ms/3:38 min 9,799 ms/7:11 min
SPAIR: TI/SPAIR TR 65 ms/166 ms 75 ms/242 ms
TR/acquisition time 4,990 ms/3:39 min 7,245 ms/5:18 min
SPIR: TR/acquisition time 4,983 ms/3:39 min 7,247 ms/5:18 min
3033

Comparison between 3.0 Tesla and 1.5 Tesla
The contrast between the lymph nodes and the surroundingfatty tissue in the isotropic DW images was 0.67±0.12 at1.5 Tesla and 0.75±0.09 at 3.0 Tesla and the factor ofimprovement was 1.14±0.15 (mean value ±standarddeviation, n=8). The judgment of the DWIBS imageslead to the following results. First, the contrast betweenlesions and vertebral bodies or ribs was higher for 3.0 Teslathan for 1.5 Tesla (score “3”) in all cases (see for exampleFig. 2). The lesions in the mediastinum are better depictedon the DWIBS image at 3.0 Tesla (Fig. 2a). Second,
artifacts on DWIBS images of the chest were judged to bestronger at 3.0 Tesla (medium, score “2”) than at 1.5 Tesla(weak, score “3”). Geometric distortion artifacts and signalloss due to susceptibility differences in the vicinity of thelungs are more pronounced at higher field strength(Fig. 2b). Moreover, motion artifacts were increased at3.0 Tesla which could be recognized by the streakyappearance of the spleen and of lesions located close to theheart or to highly pulsatile vessels (especially the aorta).The degree of artifacts in the head/neck region was juged asweak (score “3”) for both field strengths and in all cases.Third, the smallest lesion diameter detectable on the 1.5
Fig. 1 DWIBS images of thehead/neck region (a–c), chest(d–f), and abdomen (g–i) ob-tained at 3.0 Tesla by acquisitionof diffusion-weighted single-shot SE-EPI sequences withSTIR (a, d, g), SPAIR (b, e, h),and SPIR (c, f, i) fat suppres-sion. On all DWIBS imagesobtained by using STIR fatsuppression, body fat is ade-quately suppressed and centralparts of the body are clearlyvisible. Moreover, the intestinesare suppressed in the imagesobtained by using STIR (g) butnot by using SPAIR (h) or SPIR(i) due to their short T1 relax-ation times
Fig. 2 Coronal (a, c) and sag-ittal (b, d) DWIBS imagesobtained by using STIR fatsuppression of a patient withmultiple lymph node metastasesat 3.0 Tesla (a, b) and 1.5 Tesla(c, d). On the sagittal view, thestronger susceptibility-inducedgeometric distortions and signallosses around the lung (air/softtissue interface) at 3.0 Tesla (b)compared with 1.5 Tesla (d) canbe seen. On the coronal views, abetter lesion-to-bone (vertebralbodies and ribs) contrast can benoted on the image obtained at3.0 Tesla (a) compared with 1.5Tesla (c)
3034

Tesla DWIBS images was 4 mm. All lesions discernable onDWIBS images at 1.5 Tesla were also detectable at 3.0Tesla.
Clinical applications
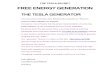
In all six patients, DWIBS imaging at 3.0 Twas feasible. In allcases, images were of diagnostic quality (score “2”). Theintraindividual comparison of DWIBS and FDG-PET isdisplayed in Fig. 3. A good correlation between DWIBS andFDG-PETwas found in the patient withmultiplemetastases ofa melanoma. Metastases to the right parotid gland and to theright adrenal gland arewell depicted on theDWIBS image andconfirmed by FDG-PET. The bilateral pulmonary metastases,however, are not as clearly depicted on the DWIBS image ason FDG-PET, most likely due to pronounced susceptibilityartifacts at the air/soft tissue interface.
Discussion
Diffusion-weighted MR imaging of extracranial organswas first attempted many years ago [10], but image qualityand accuracy of quantitative ADC analysis were limited inthis early work. With the advances in MR technology, suchas high-performance gradient hardware, parallel imagingtechniques, and phased array receiver coils, image qualityimproved [11] and an increasing number of studies focusedon DWI of extracranial organs during the last few years[12]. Especially, increasing interest in oncological pro-blems can be noted [13–17]. Conventional DWI was
applied with the aim of accurate ADC determination inorder to discriminate between benign and malignantlesions. Reports show that the ADC is reduced inmalignancy compared with normal tissue due to largercell diameters and denser cellularity [18–20] and is relatedto the cellular density of a tumor [21–23] and to itshistological architecture [18]. The DWIBS method intro-duced by Takahara [1] at 1.5 Tesla provides the possibilityof whole-body screening. However, sensitivity and spec-ificity of the DWIBS images for tumor detection are stillunder investigation.
Up to now, at 3.0 Tesla only a few studies have beenpublished about applying conventional DWI to parts of thebody [6, 7]. However, no attempts have been describedabout the implementation of DWIBS at 3.0 Tesla. In ourwork, we intended to provide an appropriate sequence forDWIBS at 3.0 Tesla. Three methods of fat suppression wereinvestigated. With STIR, a good fat suppression wasachieved for all investigated regions by using an inversiontime TI of 260 ms (TR ≥5,000 ms). This TI is considerablylonger than the optimum TI of 180 ms at 1.5 Tesla, which isin accordance with the increased longitudinal relaxation rateT1 of fat at 3.0 Tesla (382±13 ms [24], 371±8 ms [25])compared with the T1 at 1.5 Tesla (288±8ms [25], 266±2ms[26]). With the frequency-specific fat suppression methodsSPIR and SPAIR, we could not obtain good results for allregions. However, for the abdomen the fat suppression wasgood. Thus, for examinations of the abdomen, SPIR orSPAIR might be favored over STIR due to the advantage ofhigher SNR. For whole-body examinations with DWIBSimage reconstructions, the STIR fat suppression method hasto be used.
The tissue appearance in the DWIBS images at 3.0 Teslais similar to that at 1.5 Tesla: vessels, muscles, fat, and mostorgans appear white or light gray, whereas spleen, kidneys,tonsils, lymph nodes, peripheral nerves, ribs, vertebralbodies and spinal cord are medium gray. Pathologicaltissues like tumor were depicted as dark gray areas (highsignal intensity in the DW images). Instead of signal-to-noise or contrast-to-noise ratios, which vary from pixelto pixel in parallel imaging [27], we investigated thecontrast between lymph nodes and adjacent fatty tissue,which has low signal intensities due to the fat suppression.We found a contrast improvement of about 14% at 3.0Tesla. Moreover, we found an improved contrast at 3.0Tesla between lesions and bones like ribs and vertebralbodies, which seems to be caused by a lower signal-to-noise ratio of bone marrow at 3.0 Tesla. This may beexplained to some extent by higher susceptibility artifactsleading to stronger signal intensity losses at the bone/tissueinterfaces at 3.0 Tesla. Additionally, the T2 time reductionat 3.0 Tesla may lead to markedly lower signal intensitiesof bone marrow despite the fact of using a sequence with alower TE value (see Table 1), because only the hemato-poietic component of bone marrow with its very short T2relaxation time contributes to the signal intensity as a
Fig. 3 Intraindividual comparison between DWIBS and FDG-PETin a 59-year-old patient with multiple metastases of a melanoma. aCoronal DWIBS image obtained by using STIR fat suppression at3.0 Tesla and b gray scale inverted coronal MIP image of FDG-PETimages. Metastases to the right parotid gland and to the right adrenalgland are well depicted on both images (see arrows). Visualizationof bilateral lung metastases is impaired on the DWIBS image due tosusceptibility-induced signal loss at the air/soft tissue interface
3035

consequence of the fat suppression. The sensitivity to smalllesions was found to be equal at both magnetic fieldstrengths, but may be reduced at 3.0 Tesla when lesionsoccur in regions with large magnetic susceptibility differ-ences (bone/tissue or air/tissue interfaces).
It could be demonstrated that DWIBS is feasible at 3.0Tesla, with image quality sufficient for diagnostic pur-poses, but the advantages compared with 1.5 Teslapredominate not unambiguously. As disadvantages, wefound: longer acquisition times (SAR limits), increasedsusceptibility-induced geometric distortions and signallosses, and increased motion artifacts, which may be partlydue to the longer acquisition time. Thus, further investiga-tions concerning DWIBS at 3.0 Tesla should be under-taken. Improvements of DWIBS at 3.0 Tesla may beachieved,for example, by using higher reduction (SENSE)factors (>2). Nevertheless, it is already known that higherreduction factors may reduce not only susceptibility-induced and blurring artifacts but also SNR.
The following general limitations of the DWIBS tech-nique are also worth mentioning. (1) The DWIBS methodis sensitive to motion influences, which may lead toartifacts in the DWIBS images, and in case of quantitativeanalysis to less accurate ADC values [8, 28]. Less accurateADC values may hamper discrimination between benignand malignant lesions. A large number of signal averages
are performed in DWIBS, with the result that many DWimages are acquired during relatively motionless periods ofthe cardiac and respiratory cycle. However, a small, but notnegligible number of the DW images suffer from signalloss due to cardiac and respiratory motion. This influencevaries for different anatomic locations and for differentacquisitions. Thus, for areas with strong motion, stripes arediscernable on coronal and sagittal MIP images, especiallyif lesions extend over multiple slices. The effect is alsoclearly seen in the spleen, which is regularly depicted withhigh signal intensity on DWIBS images. This effect isstronger at higher magnetic field strength. This point has tobe investigated in further experiments at both magneticfield strengths. (2) Signal averaging during free breathingmay lead to pixel misregistrations, which limits the spatialresolution [29]. (3) DWIBS images may have limitedspecificity for tumor detection due to possible T1 and/or T2shine-through effects. (4) DWIBS images do not provideaccurate identification of the anatomical position of thelesions. Thus, for clinical applications, image fusion ofDWIBS images and, for example, T2-weighted images isnecessary.
In conclusion, we implemented DWIBS at 3.0 Tesla anddemonstrated its feasibility. This work opens the door tofurther investigate DWIBS at high magnetic field strengthsin the context of whole-body MRI in oncology.
References
1. Takahara T, Imai Y, Yamashita T, YasudaS, Nasu S, Van CM (2004) Diffusionweighted whole body imaging withbackground body signal suppression(DWIBS): technical improvement usingfree breathing, STIR and high resolution3D display. Radiat Med 22:275–282
2. Sakurada A, Takahara T, Nasu S, HorieT, van Cauteren M, Imai Y (2006)Clinical significance of diffusion-weighted image in staging esophagealcancer. 14th Scientific Meeting andExhibition, ISMRM: Abstracts, p 2226
3. Komori T, Narabayashi I, MatsumuraK, Matsuki M, Kawachi M, YamamotoM (2005) Comparison of radiography,FDG-PET/CT and body diffusion-weighted imaging for tumor evaluationin cancer patients on the same day.RSNA 2005, abstract
4. Zhang Y, Liang B, Gao L (2005)Preliminary study of a lymph nodesimaging: diffusion-weighted MRI withSTIR-EPI. RSNA 2005, abstract
5. Goudarzi B, Kishimoto R, YoshikawaK, Kandatsu S, Komatsu S, IshikawaH, Shahnazi M, Tsujii H (2006) Thediagnostic ability of diffusion-weightedimaging with background body signalsuppression (DWIBS) in bone metas-tasis. 14th Scientific Meeting and Ex-hibition, ISMRM: Abstracts, p 548
6. Gibbs P, Pickles MD, Turnbull LW(2006) Diffusion imaging of the prostateat 3.0 tesla. Invest Radiol 41:185–188
7. Chiu FY, Jao JC, Chen CY, Liu GC,Jaw TS, Chiou YY, Hsu FO, Hsu JS(2005) Effect of intravenous gadolini-um-DTPA on diffusion-weighted mag-netic resonance images for evaluationof focal hepatic lesions. J ComputAssist Tomogr 29:176–180
8. Mürtz P, Flacke S, Träber F, van denBrink JS, Gieseke J, Schild HH (2002)Abdomen: diffusion-weighted MR im-aging with pulse-triggered single-shotsequences. Radiology 224:258–264
9. Kawai Y, Sumi M, Nakamura T (2006)Turbo short tau inversion recovery im-aging for metastatic node screening inpatients with head and neck cancer.AJNR Am J Neuroradiol 27:1283–1287
10. Müller MF, Prasad P, Siewert B,Nissenbaum MA, Raptopoulos V,Edelman RR (1994) Abdominal diffu-sion mapping with use of a whole-bodyecho-planar system. Radiology190:475–478
11. Chow LC, Bammer R, Moseley ME,Sommer FG (2003) Single breath-holddiffusion-weighted imaging of the ab-domen. J Magn Reson Imaging18:377–382
12. Thoeny HC, De KF (2007) Extracranialapplications of diffusion-weightedmagnetic resonance imaging. EurRadiol [Epub ahead of print]
13. Abdel Razek A, Soliman NY, ElkhamaryS, Alsharaway MK, Tawfik A (2006)Role of diffusion-weighted MR imagingin cervical lymphadenopathy. Eur Radiol16:1468–1477
14. Koh DM, Scurr E, Collins DJ, PirgonA, Kanber B, Karanjia N, Brown G,Leach MO, Husband JE (2006) Colo-rectal hepatic metastases: quantitativemeasurements using single-shot echo-planar diffusion-weighted MR imaging.Eur Radiol 16:1898–1905
3036

15. Hayashida Y, Yakushiji T, Awai K,Katahira K, Nakayama Y, ShimomuraO, Kitajima M, Hirai T, Yamashita Y,Mizuta H (2006) Monitoring therapeu-tic responses of primary bone tumorsby diffusion-weighted image: initialresults. Eur Radiol 16:2637–2643
16. Kozlowski P, Chang SD, Jones EC,Berean KW, Chen H, Goldenberg SL(2006) Combined diffusion-weightedand dynamic contrast-enhanced MRIfor prostate cancer diagnosis-correla-tion with biopsy and histopathology. JMagn Reson Imaging 24:108–113
17. Rubesova E, Grell AS, De MV, MetensT, Chao SL, Lemort M (2006) Quan-titative diffusion imaging in breastcancer: a clinical prospective study. JMagn Reson Imaging 24:319–324
18. Squillaci E, Manenti G, Cova M, DiRM, Miano R, Palmieri G, Simonetti G(2004) Correlation of diffusion-weighted MR imaging with cellularityof renal tumours. Anticancer Res24:4175–4179
19. Kim T, Murakami T, Takahashi S, HoriM, Tsuda K, Nakamura H (1999)Diffusion-weighted single-shot echo-planar MR imaging for liver disease.AJR Am J Roentgenol 173:393–398
20. Issa B (2002) In vivo measurement ofthe apparent diffusion coefficient innormal and malignant prostatic tissuesusing echo-planar imaging. J MagnReson Imaging 16:196–200
21. Guo Y, Cai YQ, Cai ZL, Gao YG, AnNY, Ma L, Mahankali S, Gao JH(2002) Differentiation of clinically be-nign and malignant breast lesions usingdiffusion-weighted imaging. J MagnReson Imaging 16:172–178
22. Guo AC, Cummings TJ, Dash RC,Provenzale JM (2002) Lymphomas andhigh-grade astrocytomas: comparisonof water diffusibility and histologiccharacteristics. Radiology 224:177–183
23. Gauvain KM, McKinstry RC,Mukherjee P, Perry A, Neil JJ,Kaufman BA, Hayashi RJ (2001)Evaluating pediatric brain tumor cellu-larity with diffusion-tensor imaging.AJR Am J Roentgenol 177:449–454
24. de Bazelaire CM, Duhamel GD, RofskyNM, Alsop DC (2004) MR imagingrelaxation times of abdominal and pel-vic tissues measured in vivo at 3.0 T:preliminary results. Radiology230:652–659
25. Gold GE, Han E, Stainsby J, Wright G,Brittain J, Beaulieu C (2004) Muscu-loskeletal MRI at 3.0 T: relaxationtimes and image contrast. AJR Am JRoentgenol 183:343–351
26. Träber F, Block W, Layer G, BrauckerG, Gieseke J, Kretzer S, Hasan I, SchildHH (1996) Determination of 1H relax-ation times of water in human bonemarrow by fat-suppressed turbo spinecho in comparison to MR spectro-scopic methods. J Magn Reson Imaging6:541–548
27. Reeder SB, Wintersperger BJ, DietrichO, Lanz T, Greiser A, Reiser MF,Glazer GM, Schoenberg SO (2005)Practical approaches to the evaluationof signal-to-noise ratio performancewith parallel imaging: applicationwith cardiac imaging and a32-channel cardiac coil. Magn ResonMed 54:748–754
28. Nasu K, Kuroki Y, Sekiguchi R,Kazama T, Nakajima H (2006) Mea-surement of the apparent diffusioncoefficient in the liver: is it a reliableindex for hepatic disease diagnosis?Radiat Med 24:438–444
29. Nasu K, Kuroki Y, Sekiguchi R,Nawano S (2006) The effect of simul-taneous use of respiratory triggering indiffusion-weighted imaging of the liver.Magn Reson Med Sci 5:129–136
3037