Embed Size (px)
Citation preview

Diffuse Biliary Tract Injury After Orthotopic Liver Transplantation
Shujun Li, MD, Robert J. Stratta, MD, Alan N. Langnas, Do, R. Patrick Wood, MD, Wagner Marnjo, MD, Byers W. Shaw, Jr., MD, Omaha, Nebraska
An unusual type of diffuse biliary tract injury after liver transplantation that is characterized by multi- ple intrahepatie biliary strictures, duetal dilatations, fluid collections, or intrahelmtie abscesses has been identified. Over a 5-year period, a total of 10 pa- tients (2%) developed diffuse intrahepatie biliary injury with established vascular pateney and no ob- vious source for their biliary tract pathology. All patients received livers preserved in University of Wisconsin solution with a mean preservation time of 16 hours. This biliary tract injury was associated with the presence of severe preservation injury and Roux limb biliary reconstruction. Of the 10 pa- tients, 5 were treated nonoperatively with multiple stricture dilations and stent placements, 3 under- went retransplantation, 1 was treated operatively with hepaticojejunostomy, and 1 died of sepsis. This study suggests that this complication appears to be related to preservation injury and that the eti- ology may be ischemic in origin.
From the Department of Surgery, University of Nebraska Medical Center, Omaha, Nebraska.
Requests for reprints should be addressed to Robert J. Stratta, MD, Department of Surgery, University of Nebraska Medical Center, 600 South 42nd Street, Omaha, Nebraska 68198-3280.
Presented at the 44th Annual Meeting of the Southwestern Surgi- cal Congress, Seottsdale, Arizona, April 26-29, 1992.
B iliary tract complications are a continuing source of morbidity after orthotopic liver transplantation.
However, in the last few years, several centers have noted a reduction in biliary complications after liver transplan- tation, with the incidence ranging from 13% to 25% [1=7]. The genesis of a biliary tract complication is multi- factorial but most often related to vascular, technical, or immunologic considerations.
It is well established that hepatic artery thrombosis may cause biliary complications, such as intrahepatie ductal strictures, biliary sepsis or abscesses, and extra- hepatic biliary leak or stricture due to ischemia [8-11]. In addition, immunologic phenomena, such as rejection [12,13] and ABO blood group incompatibility [14,15], may lead to biliary strictures, presumably due to arterio- pathy and/or direct biliary epithelial injury. However, diffuse intrahepatie biliary tract injury in the absence of these conditions has not been well described previously. In addition, the effect of severe preservation injury [16-20] on the biliary tract is likewise ill defined.
With the introduction of extended preservation with the University of Wisconsin (UW) solution into clinical liver transplantation [21,22], we have identified an un- usual type of diffuse intrahepatic biliary tract injury in the absence of vascular or immune etiologies. The pur- pose of this study was to: (1) define the incidence and severity of this lesion in liver transplant recipients; (2) determine its etiology and pathogenesis; (3) characterize the clinical presentation and methods of diagnosis; and (4) describe treatment options and outcome.
PATIENTS AND METHODS Study population and design: From July 1985 to
July 1990, a total of 406 consecutive patients received 468 liver transplants at the University of Nebraska Medi- cal Center. During this 5-year period, data from all recip- ients were retrospectively analyzed for this study. The minimum length of follow-up was 1 year.
Of the 406 patients, 258 (64%) liver recipients were adults, with a mean age of 45 4- 12 years (range: 18 to 68 years). The remaining 148 patients (36%) were children, with a mean age of 4 4- 4 years (range: newborn to 17 years). A total of 62 retransplants were performed, in- eluding 56 second and 6 third transplants.
Recipient selection and management: Recipient se- lection was based primarily on ABO blood type compati- bility, size considerations, medical urgency, and length of time on the waiting list, according to United Network for Organ Sharing guidelines. No attempt was made to per- form HLA matching or prospective lymphocytotoxie crossmatehing. A total of 23 transplants involving ABO-
536 THE AMERICAN JOURNAL OF SURGERY VOLUME 164 NOVEMBER 1992

BILIARY TRACT INJURY AFTER TRANSPLANTATION
incompatible patients (5%) were performed, usually for urgent indications. During the period of study, uniform protocols for donor management, organ retrieval, trans- plantation, and immunosuppression were followed, with the exception of the use of cold storage preservation solu- tion [22]. Over a 32-month interval extending from July 1985 to March 1988, 163 procured livers were flushed and stored in Euro-Collins solution with cold ischemia not exceeding 8 hours. During the next 28 months from March 1988 through June 1990, 305 donor livers were stored in UW solution with liberal use of extended preser- vation. Donor hepatectomy was performed by standard techniques in conjunction with multiple organ retrieval [23]. Recipient hepatectomy and hepatic replacement were performed by standard techniques with venous by- pass in recipients weighing more than 40 kg [24]. Biliary reconstruction was accomplished with either a choledo- chocholedochostomy over a T-tube stent or Roux-en-Y choledochojejunostomy over an internal stent [7].
All patients were treated with combination cyclospor- ine-steroid immunosuppression, as described previously [25]. Duplex ultrasonography was performed on the first postoperative day to check for vascular patency [26]. Subsequently, this technique was applied liberally to any patient with evidence of allograft dysfunction, particular- ly in the early postoperative period. Arteriography was used to confirm and delineate hepatic artery or portal vein thrombosis. In patients with a T-tube, cholangiogra- phy was performed for allograft dysfunction and prior to T-tube removal (usually at 3 to 6 months after transplan- tation). Hepatic function was assessed by serial monitor- ing of liver enzymes, prothrombin time, serum bilirubin, mental status, and overall clinical condition.
Definitions: Severe preservation injury was defined as serum aspartate aminotransferase (AST) or alanine aminotransferase (ALT) levels above 2,000 IU/L within 72 hours of liver transplantation in the absence of vascu- lar thrombosis [17]. Diffuse biliary tract injury was de- fined as a nonanastomotic intrahepatic biliary lesion with: (1) two or more sites of either stricture formation and/or biliary dilatation or (2) multiple intrahepatic flu- id collections or abscesses.
Statistical analysis: Data are expressed as mean 4- standard deviation (SD). Univariate analysis was per- formed by the Student's t-test for continuous variables, the X 2 for categorical variables, and Fisher's exact test when data were sparse. A multivariate analysis was not performed. A p value of less than 0.05 was considered significant.
RESULTS A total of 64 patients (16%) developed biliary tract
complications after orthotopic liver transplantation. In 17 of these patients, a pattern of diffuse intrahepatic biliary injury was identified. Seven of these patients had docu- mented hepatic artery thrombosis, whereas the remain- ing 10 had established vascular patency and no obvious source for their biliary pathology.
The incidence of diffuse intrahepatic biliary injury was similar in the adult and pediatric age groups and also
after both primary transplantation and retransplantation. In addition, there was no predilection according to pri- mary disease, donor and recipient cytomegalovirus sero- logic status, HLA-matching, or T-cell crossmatching re- sults. However, the incidence of this lesion was higher in patients receiving ABO-incompatible grafts (2 of 23 or 9% versus 8 of 445 or 2%, p = 0.08).
A total of 163 donor livers were preserved in Euro- Collins solution with a mean preservation time of 5 4- 2 hours. The remaining 305 donor livers were flushed and preserved in cold storage in UW solution with a mean preservation time of 13 4- 4 hours (p <0.001). There were no documented cases of diffuse intrahepatic biliary injury in the absence of vascular thrombosis with Euro-Collins preservation. In contrast, all 10 patients with diffuse bil- iary tract injury and vascular patency received livers pre- served in UW solution with a mean preservation time of 16 4- 3 hours. The incidence of this lesion was much higher with the use of UW preservation (10 of 305 or 3% versus 0 of 163 or 0%, p = 0.01). Furthermore, in livers preserved in UW solution, the incidence of this lesion was higher with preservation times of 14 hours or greater (9 of 155 or 6% versus 1 of 150 or 1%, p = 0.01).
In order to correlate this diffuse type of biliary pathol- ogy with donor liver preservation injury, we reviewed the posttransplant liver function tests in all patients who re- ceived livers preserved in UW solution. In 103 transplants (34%), a marked elevation in serum transaminase levels (AST or ALT greater than 2,000 IU/L) occurred within 72 hours of transplantation. The 1-month graft survival rate was decreased in the setting of severe preservation injury in the UW era (66% versus 95% in the absence of severe preservation injury, p <0.001). Thirty-five of these patients either had retransplantation or died within 1 month. Of the remaining 68 patients, 8 (12%) had diffuse biliary tract injury within 3 months of transplantation. In contrast, only two patients (1%, p <0.01) developed dif- fuse biliary injury in the absence of both hepatic artery thrombosis and an early marked elevation in serum trans- aminase levels.
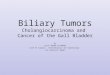
Patients usually presented with jaundice, hepatic allo- graft dysfunction, or cholangitis. Laboratory values early after transplant (peak), and before and after initial treat- ment, are illustrated in Table L The mean time to diagno- sis was 50 4- 30 days after transplant. The diagnosis was usually suggested by ultrasonographic findings and con- firmed by biliary visualization techniques (Figure 1) or computerized tomography. Initial management usually consisted of biliary decompression by percutaneous trans- hepatic techniques and intravenous antibiotic therapy. Subsequent management included dilation of strictures, drainage of fluid collections, and internal stenting via percutaneous or endoscopic techniques. Of the 10 pa- tients with diffuse biliary tract injury, 5 were treated nonoperatively with multiple stricture dilations and stent placements, 3 underwent retransplantation (1 died dur- ing attempted retransplantation), 1 was treated opera- tively with hepaticojejunostomy, and 1 died of biliary sepsis. Patient and graft survival rates are 80% and 60%, respectively, after a mean follow-up of 20 4- 10 months.
THE AMERICAN JOURNAL OF SURGERY VOLUME 164 NOVEMBER 1992 537

LI ET AL
TABLE I Laboratory Values After Transplant and Before and After Treatment
No. Total Alkaline of Bilirubin AST ALl- GGTP Phosphatase
Patients (mg/dL) (IU/L) (IU/L) (IU/L) (IU/L)
Peak level in first 72 hr after transplant 10 6.7 _+ 3.6 3,672 _+ 5,000 1,832 _+ 2,210 268 _+ 192 244 __ 205 Value at time of diagnosis of diffuse biliary injury 10 4.5 • 2.9 172 • 105 288 • 206 1,129 -- 297 576 ___ 353 Value after initial treatment (usually stenting) 10 1.5 • 0.8* 46 • 20* 83 - 64* 386 • 360* 239 • 111 * Current levels in surviving allografts 6 1.3 -+ 0.8 59 -+ 44 54 _+ 51 345 • 505 237 __ 100
GGTP = ~/glutamyl transpeptidase; AST = aspartate aminotrensferase; ALT = alanine aminotransferase. �9 p <0.01 versus pre-treatrnent level.
F lgu re 1. C h o l a n g i o g r a m Showing mul t ip le in t rahepat ic strictures and a t ranshepa t i c s ten t th rough the R o u x - e n - Y cho ledocho je ju - nos tomy .
Liver function in the six surviving livers with early diffuse biliary injury is shown in Table I. Four patients continue to have stable allograft function, whereas two have developed chronic (ductopenic) rejection. Another patient underwent retransplantation for chronic rejection superimposed on recurrent strictures. Episodic cholangi- tis with sludge formation and stent obstruction was a short-term but not a long-term problem.
COMMENTS A spectrum of biliary tract complications may occur
after liver transplantation and are usually related to tech- nical errors or local pathologic processes. However, pathologic conditions of the intrahepatic bile ducts of the hepatic allograft are unusual and may be due to: (1) hepatic artery or portal vein thrombosis [8-11]; (2) im- munologic phenomena such as acute or chronic rejection [12,13,27]; (3) ABO incompatibility [14,15]; (4)
"shock" liver; (5) recurrent primary biliary tract disease such as sclerosing cholangitis [28]; (6) primary or recur- rent viral hepatitis [29]; (7) reflux cholangitis associated with Roux limb reconstruction; and (8) ischemia-reper- fusion injury [16-20].
In this study, we identified 10 cases of diffuse biliary tract injury characterized by multiple intrahepatic biliary strictures, ductal dilatations, fluid collections, or intrahe- patic abscesses in the presence of vascular patency. The cholangiographic features of this lesion are similar to those described in nontransplanted patients with hepatic artery ligation [30] and transplanted patients with hepat- ic artery thrombosis [8-11], suggesting a vascular etiolo- gy. In addition to technical problems resulting in throm- bosis, it has been postulated that allograft rejection may cause arteriopathy and lead to biliary tract ischemia [31]. Other proposed mechanisms of intrahepatic biliary pa- thology include immunologic, infectious, or chemical in- jury directed at the biliary epithelium.
This pattern of diffuse, intrahepatic, multi-focal bil- iary tract injury in the absence of vascular thrombosis is unusual and has only recently been recognized [32]. In two cases, ABO-incompatible grafts were transplanted. In this setting, direct immunologic injury to either the biliary epithelium or vascular endothelium can be impli- cated as having a causative effect. In two other cases, reoperations were performed on the hepatic artery for low flow. Regardless of whether or not these cases represent ischemia due to poor inflow or high resistance to outflow from preservation injury or rejection [17,18], a vascular etiology is suggested. Animal studies have suggested that extended preservation of the donor liver may lead to a high hepatic arterial resistance [18] and severe microcir- culatory disturbances [19,20]. Since the biliary tract is solely dependent on hepatic artery inflow, the injury of extended preservation may result in biliary pathology in the absence of either hepatic artery thrombosis or pri- mary nonfunction.
In another five cases, allograft rejection preceded the onset of diffuse biliary injury. Three of these patients developed chronic rejection. Our overall incidence of chronic rejection after liver transplantation is 8%, sug- gesting that this lesion predisposes to or is an early mani- festation of ductopenic rejection. Whether this is indica- tive of primarily an immune etiology or perhaps a
538 THE AMERICAN JOURNAL OF SURGERY VOLUME 164 NOVEMBER 1992

BILIARY TRACT INJURY AFTER TRANSPLANTATION
manifestation of preservation injury on superimposed re- jection [17] is largely unknown.
The most striking finding in this study was the rela- tionship between diffuse biliary injury not only with the duration of cold ischemia in UW solution but also with the degree of preservation injury as quantitated by trans- aminase elevation. The absence of this entity in livers preserved with Euro-Collins solution is probably related to shorter cold ischemia and a higher incidence of pri- mary nonfunction with longer cold ischemia in the Euro- Collins era. The exclusivity of this lesion to livers with extended preservation in UW solution certainly suggests an ischemia-reperfusion pathogenesis, especially when considering the correlation with the degree of preserva- tion injury. However, even in the highest risk setting (extended preservation in UW solution for 14 hours or more with a Roux limb reconstruction), 90% of patients did not develop this lesion, thus underscoring the multi- factorial etiology of preservation injury and its effect on the biliary epithelium and microvasculature.
The natural history of this lesion is variable and ap- pears to be dependent not only on the severity of the initial insult but also on co-existent factors such as rejection, sludge formation, and cholangitis [13,17,28,32]. Al- though six patients were successfully managed by me- chanical interventions (stents, dilations, lithotripsy, oper- ative drainage), two subsequently developed chronic rejection. Three other patients required extirpative proce- dures (hepatic resections, retransplantation), with one eventually having a retransplantation for chronic rejec- tion. The final patient died of unresolved (and unrecog- nized) biliary sepsis.
In summary, we have identified an unusual type of diffuse intrahepatic biliary injury that occurs early after liver transplantation in the absence of vascular thrombo- sis. This study suggests that this complication may be related to preservation injury and that the etiology may be ischemic in origin.
REFERENCES 1. Iwatsuki S, Shaw BW Jr, Starzl TE. Biliary tract complications in liver transplantation under cyclosporine-steroid therapy. Trans- plant Proc 1983; 15: 1288-91. 2. Krom RAF, Kingma LM, Haagsma EB, et al. Choledechocho- ledochostomy, a relatively safe procedure in orthotopic liver trans- plantation. Surgery 1985; 97: 552-6. 3. Vicente E, Perkins JD, Sterioff S, et al. Biliary tract complica- tions following orthotopic liver transplantation. Clin Transplant 1987; 1: 138-42. 4. Hiatt JR, Quinones-Baldrich W J, Ramming KP, Brems J, Bu- suttil RW. Operations upon the biliary tract during transplantation of the liver. Surg Gynecol Obstet 1987; 165: 89-93. 5. Lerut J, Gordon RD, Iwatsuki S, et al. Biliary tract complica- tions in human orthotopic liver transplantation. Transplantation 1987; 43: 47-51. 6. Wilson B J, Marsh JW, Makowka L, et al. Biliary tract compli- cations in orthotopic adult liver transplantation. Am J Surg 1989; 158: 68-70. 7. Stratta R J, Wood RP, Langnas AN, et al. Diagnosis and treat- ment of biliary tract complications after orthotopic liver transplan- tation. Surgery 1989; 106: 675-84. 8. Tzakis AG, Gordon RD, Shaw BW Jr., Iwatsuki S, Starzl TE.
Clinical presentation of hepatic artery thrombosis after liver trans- plantation in the cyclosporine era. Transplantation 1985; 40: 667-71. 9. Zajko AB, Campbell WL, Logsdon GA, et al. Cholangiographic findings in hepatic artery occlusion after liver transplantation. A JR Am J Roentgenol 1987; 149: 485-9. IO. Hesselink EJ, Schilfgaarde R Van, Grond J, et al. Hepatic artery thrombosis after orthotopic liver transplantation: clinical presentation and possible etiologic factors. Clin Transplant 1988; 2: 306-11. 11. Langnas AN, Marujo W, Stratta R J, et al. Hepatic allograft rescue following arterial thrombosis: role of urgent revasculariza- tion. Transplantation 1991; 51: 86-90. 12. Mazzaferro V, Esquivel CO, Makowka L, et al. Hepatic artery thrombosis after pediatric liver transplantation: medical or surgical event? Transplantation 1989; 47: 971-7. 13. Oguma S, Belle S, Starzl TE, Demetris AJ. A histometric analysis of chronically rejected human liver allografts: insights into the mechanisms of bile duct loss: direct immunologic and ischemic factors. Hepatology 1989; 9: 204-9. 14. Sanchez-Urdazpal L, Sterioff S, Janes C, et al. Increased bile duct complications in ABO incompatible liver transplant recipients. Transplant Proc 1991; 23: 1440-1. 15. Gugenheim J, Samuel D, Reynes M, Bismuth H. Liver trans- plantation across ABO blood group barriers. Lancet 1990; 336: 519-23. 16. McKeown CMB, Edwards V, Philips M J, et al. Sinusoidal lining cell damage: the critical injury in cold preservation of liver allografts in the rat. Transplantation 1988; 46: 178-91. 17. Howard TK, Klintmalm GB, Cofer JB, et al. The influence of preservation injury on rejection in the hepatic transplant recipient. Transplantation 1990; 49: 103-7. 18. Ikeda T, Yanaga K, Lebeau G, et al. Hemodynamic and biochemical changes during normothermic and hypothermic san- guinous perfusion of porcine hepatic grafts. Transplantation 1990; 50: 564-7. 19. Momii S, Koga A. Time-related morphological changes in cold-stored rat livers: a comparison of Euro-Collins solution with UW solution. Transplantation 1990; 50: 745-50. 20. Manner M, Shult W, Senninger N, Machens G, Otto G. Evaluation of preservation damage after porcine liver transplanta- tion by assessment of hepatic microcirculation. Transplantation 1990; 50: 940-3. 21. Kalayoglu M, Sollinger HW, Stratta R J, et al. Extended pres- ervation of the liver for clinical transplantation. Lancet 1988; 1: 617-9. 22. Stratta R J, Wood RP, Langnas AN, et al. The impact of extended preservation on clinical liver transplantation. Transplan- tation 1990; 50: 438-43. 23. Starzl TE, Hakala TR, Shaw BW Jr, et al. A flexible procedure for multiple cadaveric organ procurement. Surg Gynecol Obstet 1984; 158: 223-30. 24. Starzl TE, Iwatsuki SI, Van Thiel DH, et al. Evolution of liver transplantation. Hepatology 1982; 2: 614-36. 25. Wood RP, Shaw BW Jr, Williams L. The use of OKT3 rescue therapy after orthotopic liver transplantation: the University of Nebraska Medical Center experience. Transplant Proc 1988; 20: 254-9. 26. Sayage LH, Husberg BS, Klintmalm GB, Goldstein RM, Gonwa TA. Vascular complications in adult liver transplant pa- tients: value of post-operative Doppler ultrasound screening and the surgical management of hepatic arterial thrombosis. Clin Trans- plant 1989; 3: 344-8. 27. Ludwig J, Weisner RH, Batts KP, Perkins JD, Krom RAF. The acute vanishing bile duct syndrome (acute irreversible rejec- tion) after orthotopic liver transplantation. Hepatology 1987; 7:
THE AMERICAN JOURNAL OF SURGERY VOLUME 164 NOVEMBER 1992 539

LI ET AL
476-83. 28. Lerut J, Demetris A J, Steiber AC, et aL Intrahepatic bile duct strictures after human orthotopic liver transplantation: recurrence of primary sclerosing cholangitis or unusual presentation of allo- graft rejection? Transplant Int 1988; 1: 127-30. 29. Portmann B, Neuberger JM, Williams R. Intrahepatic bile duct lesions. In: Calne RY, editor. Liver transplantation. New York: Grune and Stratton, 1983: 279-87. 30. Terblanche J, Allison HF, Northover JM. An isehemic basis for biliary strictures. Surgery 1983; 94: 52-7. 31. Bauman J, Campbell WL, Demetris A J, Zajko AB. Intrahepa- tic cholangiographie abnormalities in liver transplants: correlation with biopsy evidence of rejection and other disorders. A JR Am J Roentgenol 1989; 152: 275-9. 32. Sanchez-Urdazpal L, Gores G J, Ward EM, et al. Ischemie- type biliary complications after orthotopic liver transplantation. Hepatology 1992; 16: 49-53.
DISCUSSION Romano Delcore (Kansas City, KS): You have de-
scribed an uncommon but troublesome biliary injury that occurs early after orthotopic liver transplantation. Inter- estingly, the UCLA group described seven patients with a similar injury earlier this year at the American Surgical Association meeting. All of their patients had received grafts preserved with University of Wisconsin (UW) so- lution, and, in every patient, the cold ischemic time ex- ceeded 12 hours.
You have presented evidence that this rare lesion may be due to ischemic injury as suggested by the fact that, of 17 patients, 7 had documented arterial thrombosis and 2 required early arterial anastomotic revisions. In the re- maining eight patients, diffuse intrahepatic biliary injury occurred in the absence of vascular thrombosis. There- fore, you suggest that preservation injury may have had an important etiologic role. In order to correlate diffuse biliary injury with donor liver preservation injury, you have reviewed the incidence of liver function test abnor- malities in all patients receiving livers preserved with UW solution. I have three questions relating to this aspect of the study: (1) Did preservation injury, as defined by your study, occur in the Euro-Collins solution group, and, if so, what was the incidence compared with that found in the UW solution group? (2) You defined preservation injury as a transaminase level elevated above 2,000 IU/L within 72 hours of transplantation. Was preservation injury con- firmed by liver biopsy in the 10 patients presented here with diffuse biliary injury? (3) What was the incidence of the elevation of transaminase level above 2,000 IU/L in the UW solution group with ischemic times of less than 14 hours? In other words, how often did preservation injury as defined by your study occur in organs that were transplanted within less than 14 hours?
This is an important paper, which defines an unusual lesion that may be identified with increasing frequency in the future. The continued improvement of preservation solutions has led to a relative complacency with respect to cold ischemic times. As a result, transplant centers, in- cluding our own, are now more likely to utilize commer- cial flights instead of charter planes for organ delivery and to schedule transplants for early the next morning rather than to operate in the middle of the night. There- fore, based on the results of this study, should transplant centers now pay more careful attention to cold ischemic times, and furthermore, should organs over 14 hours old continue to be utilized routinely?
John Brems (San Diego, CA): We have been using prostaglandin El in these patients, especially in those with long ischemia times, in order to improve microcirculation and possibly prevent some of the strictures you've seen. Please comment on the use of prostaglandins in your patients.
Shujun Li (closing): Dr. Delcore, I believe that pres- ervation injury is quite a subtle concept. We didn't per- form any biopsies to prove preservation injuries. The se- lection of a 2,000-IU/L transaminase level as significant is somewhat arbitrary. It appears that most of the pa- tients with UW solution preservation have elevated trans- aminase levels within 72 hours after transplantation, but levels above 2,000 IU/L are rather high. About 30% of patients develop marked elevation of transaminase levels postoperatively (greater than 2,000 IU/L). When Euro- Collins solution was used, the incidence was about the same. However, in this study, no patients whose trans- planted livers were preserved in Euro-Collins solution developed a diffuse type of biliary tract injury. That is why there may be a strong correlation with preservation injury, but apparently the preservation injury is not the cause of the diffuse type of biliary tract injury. In regard to the question about the timing of transplantation, my belief is that liver transplantation should not be delayed beyond 14 hours. Some institutions have adopted a new policy to transplant as soon as possible. In our series, there were several patients who had the maximum preservation time of 24 hours, and the patients did well with no diffuse type of biliary tract injury. So for this question, my an- swer is that, although we should perform transplant as early as possible, if there is a delay beyond 14 hours, the transplant should still be performed.
Dr. Brems, in Omaha, we administered prostaglandins in several patients postoperatively; however, we did not make a study of the use of prostaglandins. Our impression is that the administration of prostaglandins made little difference to the elevation of the transaminase levels. Most of this work, I believe, has been done by a Canadian physician who has shown a lower incidence of nonfunc- tioning grafts, but we did not have that experience.
540 THE AMERICAN JOURNAL OF SURGERY VOLUME 164 NOVEMBER 1992