Embed Size (px)
Citation preview

525
Differential Utilization of Eicosapentaenoic Acid and Docosahexaenoic Acid in Human Plasma Jason Hodge a, Kerrie Sanders a and Andrew J. Sinclairb, * aDepartment of Human Nutrition, Deakin University, Geelong 3217 and bDepartment of Applied Biology, Royal Melbourne Institute of Technology, Melbourne 3001, Victoria, Australia
It has recently been shown that the co3 fatty acid status in humans can he predicted by the concentration of eico- sapentaenoic (EPA) and docosahexaenoic {DHA) acids in plasma phospholipids [Bjerve, K.S., Brubakk, A.M., Fougner, K.J., John~en, H., Midjthell, K., and Vik, T. {1993) Am. J. Clin. Nutr., in press]. In countries with low intake of ~3 fatty acids, the level of EPA in plasma phospholipids is often only about one-fifth the concentration of DHA. The purpose of this study was to investigate whether this difference in the concentration of these two fatty acids was due to a selective loss of EPA relative to DHA or to a lower dietary intake of EPA. Seven female volunteers ingested four grams of MaxEPA daily for 2 wk and in the follow- ing 4 wk they ate a diet almost completely devoid of the long,chain co3 fatty acids. The concentrations of the c03 fatty acids in the plasma cholesteryl esters, triglycerides and phospholipids and the high density lipoprotein phos- pholipids were examined at weekly intervals throughout the study. There was a more rapid rise in the concentra- tion of EPA than in DHA levels in the supplementation period in all lipid fractions, but there was a dispropor- tionate rise in DHA relative to EPA in the plasma lipids compared with the ratio in the supplement. In the deple- tion phase there was a rapid disappearance of EPA from all fractions, such that pretrial levels were reached by one week post-supplementation. The disappearance of DHA was slower, particularly for the plasma phospholipids: at 4 wk post~supplementation, the DHA concentration in this fraction was stir 40% above the pre-trial value. It is sug- gested that the low plasma EPA values relative to DHA are the result of increased/~xidation of EPA and]or low dietary intake, rather than a rapid conversion of EPA to DHA. One practical result of this experiment is that, com- pared with DHA, the maintenance of increased EPA levels in plasma {and therefore tissues) would require constant inputs of EPA due to its more rapid loss from the plasma. Lipids 28, 525-531 (1993).
The oJ3 fatty acids are now recognized as important com- ponents of the human diet. Fonowing intense investigations during the last two decades, their role as modulators of the metabolism of arachidonic acid to eicosanoids (11, their im- portance in protecting against cardiovascular disease by a variety of actions 12) and their potential significance for the development of normal function of the retina and brain (3} has been establishecL
*To whom correspondence should be addressed at Department of Human Nutrition, Deak/n University, Geelong 3217, Victoria, Aus- trali~
Abbreviations: CE, cholesteryl esters; DHA, docosahexaenoic acid {22:6co3); DPA, docosapentaenoic add (22:5oJ3); EPA, eicosapentaenoic acid {20:5co3); GLC, gas-liquid chromatography; HDL, high density lipoproteins; LCP, long-chain polyunsaturated fatty acids; LDL, low density lipoproteLns; PL, phospholipid; PUFA, polyunsaturated fatty acids; TG, triglycerides.
The main co3 polyunsaturated fatty acids (PUFA) from the food chain are a-linolenic acid (from plant sources), eicosapentaenoic acid (20:5c03 or EPA), docosapentaenoic acid (22:5co3 or DPA) and docosahexaenoic acid (22:6co3 or DHA). These latter three fatty acids which can be found in high concentrations in marine foods, are often referred to as w3 long, chain PUFAs (LCP). The interest in these PUFA was stimulated by the observations on the low in- cidence of cardiovascular disease in Greenland Eskimos despite the high fat content of their diet (4).
There is general agreement that the level of ~3 PUFA should be increased in the Western diet, and various sug- gestions have been made regarding an appropriate level of co3 fatty acids in our current diet 15). In most Western coun- tries the level of ~3 PUFA in the diet is low relative to the oo6 PUFA [estimated at 1:11 based on world production figures (6), and a similar ratio for the United States, based on consumption figure~ (7)] and this is reflected in the balance of these fatty acids in plasma and certain tissues. The ratio of co3 to co6 PUFA in the diet in Australia is likely to be lower than that in the United States since many com- mon vegetable oils used in this country are low in a-linolenic acid (eg., significant sources of a-linolenic acid such as soy- bean oil and rapeseed oil have not been commonly used in the margarine and vegetable oil industry).
Bjerve et al (8) recently showed that plasma phospholipid (PL) concentrations of EPA and DHA can be used to assess the co3 PUFA status Within the dietary range of 0.1 to 0.6% of energy of total c03 PUFA (0.05 to 0.5 g per day of EPA and 0.1 to 0.8 g per day of DHA), there was a rectilinear association between plasma PL EPA and DHA levels and the dietary intake Previously, plasma fatty acid levels have only been considered as a short-term indicator of dietary intak~ whereas long-term intake was thought to be better judged from the fatty acid pattern of tissues or cells such as erythrocTtes or white blood cells (9).
The level of ~3 PUFA in tissues such as plasma, white cells and erythrocytes is low relative to the co6 PUFA in pe~ ple on typical Western diets (10-13). In addition, the EPA level is substantially lower than that of DHA an& in the case of the plasma PL, it is of the order of 0.2 X the DHA value (10,13). From these dat~ the following conclusions can be drawm (i) intake or absorption of EPA is substantially lower than that of DHA, (ii) there is a selective utilization of EPA and]or (iii) there is a selective retention of DHA.
Although it is recognized that dietary change can be as- sociated with rapid changes in the fatty acid composition of plasma lipids (13), the study of plasma lipids can pr~ vide useful information about fatty acid dynamics in the body since all dietary lipids pass through the plasma pool(s) before being incorporated in tissue lipids. The purpose of this investigation was to study the accumulation and loss of EPA and DHA in human plasma since it was believed that this might help explain why there was such a difference between the levels of these fatty acids in plasma in subjects on typical Western diets containing low levels of co3 PUFA.
The design of this experiment was to increase the levels of EPA and DHA in plasma over a two-week period, then
Copyright �9 1993 by the American Oil Chemists' Society LIPIDS, Vol. 28, na 6 (1993)

526
J. HODGE ET AL
to follow the washout of these PUFA from plasma during the next 4 wk when the subjects were on a diet with very low levels of LCP r thus ensuring that the disappearance from plasma was not confounded by an influx of r LCP from the diet. The fractions chosen for study were the plasma PL, triglycerides (TG) and cholesteryl esters (CE) and the high density lipoprotein (HDL) PL.
MATERIALS AND METHODS
Subjects. Seven healthy, female volunteers (mean age, 30.6 yrs; mean body mass index, 21.4) participated in the study. The protocol for this study was approved by the Deakin University Ethical Review Committee (Geelong, Australia) and informed consent was obtained from the volunteers, all of whom were staff members of the Depart- ment of Human Nutrition, De,kin University.
Experimentalprotocol. The study ran for six weeks. In the first two weeks (co3 supplementation phase) the sub- jects consumed their normal diet plus four 1-g capsules daffy of MaxEPA (Nature's Way | Nature's Way Health Products, Chadstone, Australia). Analysis of the oil by capillary gas-liquid chromatography (GLC) using an in- ternal standard of triheptadecanoin (Nu-Chek-Prep, Ely- sian, MN) established that the concentrations of EPA, DPA and DHA were 137, 21 and 98 mg/g oil, respective- ly (16.3, 2.5 and 12.1% of total fatty acids); thus the 4 g of fish oil provided 548 mg EPA and 392 mg DHA daily. In the remaining four weeks (r depletion phase), the sul~ jects were advised to reduce the ~3 PUFA content of their diet to a minimum by avoiding fish and other marine pro- ducts, and vegetable otis and margarines containing a- linolenic acid such as canola off, and walnuts, red meat and offal meats. They were allowed to consume one egg/week, three meals of lean pork and]or chicken (<100 g/serve) per week and were provided with four vegetarian meals weekly, consisting mainly of lentils and vegetables. The estimated maximum intakes of EPA, DPA and DHA in this latter phase were less than seven mg/d for each r LCP. These figures were calculated from our own data on the PUFA content of Australian foods (14,15). Blood samples were taken before the study began and at weekly intervals between 08:00 and 09:00 following a 10-h over- night fast.
Fatty acid analysis of plasma and HDL lipids. Fasting blood samples were collected in heparinized tubes, stored in ice immediately after collection and centrifuged at 3000 rpm (1700 • g, 15 min, 4~ in a Beckman TJ-6 centrifuge {Beckman Instruments Australia, P/L., Melbourne, Vic- toria, Australia). Plasma was collected for cholesterol and TG analysis, and aliquots were stored for subsequent lipid extraction. The HDL were separated from a 1.0 mL ali- quot of plasma within 2 h of blood collection from other plasma lipoproteins by precipitation with dextran sulfate (Dextralip 50, Sochibc~ Velizy Villacoublay, France).
Lipids of whole plasma and the HDL fraction were ex- tracted with chloroform/methanol (2:1, vol/vol) containing 10 mg/L of butylated hydroxytoluene (16). Internal stan- dards of diheptadecanoyl phosphatidylcholine (Sigma, St. Louis, MO), cholesteryl heptadecanoate and triheptadeca- noin (Nu-Chek-Prep) were added to the plasma samples and HDL samples prior to lipid extraction. The lipid ex- tracts were separated by thin-layer chromatography (16), and the fatty acid methyl esters of the PL, CE and TG
fractions were formed as described previously (16). The fatty acid methyl esters were analyzed by flame-ionization capillary GLC (model GC-9A, Shimadzu, Kyoto, Japan) using a 50 m X 0.32 mm i.d. fused silica (CPSil 88) capillary column (Chrompack, Middelburg, The Netherlands), programmed from 110~ for 3 min to 190~ at 8~ with helium as carrier gas at a flow rate of 5 mL/min. Fatty acids were identified by comparison with standard mixtures of fatty acid methyl esters, and the results were calculated using response factors derived from chromatography standards of known composition (GLC-68A and 63B, Nu-Chek-Prep).
Lipoprotein lipid analysis. Concentrations of cholesterol and triglyceride in fasting plasma were measured en- zymatically on an autoanalyzer (Hitachi Automatic Analyzer 705, Nissei Sangyo Ca Ltd., Tokyo, Japan) us- ing commercially available kits (Cholesterol CHOD-PAP; Triglyceride GPO-PAP; Boehringer Mannheim, Germany).
Statistical analyses. The results are presented as mean +_ SD. The experiment was designed to compare the in- crease in the r LCP values at week 2, achieved using the MaxEPA supplement, with the initial levels of these PUFA, and to compare the values at the end of the deple- tion phase (week 6) with the initial values. The statistical significances between means (week 2 vs. week 0, and week 6 vs. week 0) were analyzed using a paired t-test; signifi- cant results were taken as P < 0.05,
RESULTS
Plasma cholesterol and TG levels. There were no signifi- cant changes in the total plasma cholesterol and TG levels during the course of the experiment (Table 1), which is con- sistent with the results of a 20-wk study using similar low doses of w3 LCP (17).
Initial fatty acid data~ The pre-trial plasma PL fat ty acid concentrations of the seven subjects were within the normal range established in this laboratory (Table 2). The mean values for the plasma PL arachidonic acid, EPA and DHA were 9.3, 0.6 and 3.0 (as percent of phospholipid fat- ty acids), respectively; however, there was a spread of the values for the co3 LCP, indicating a variation in w3 intake of the seven subjects prior to the start of this experiment. The EPA values ranged from 0.3 to 1.0 mg/100 mL and the DHA concentrations from 2.0 to 4.5 rag/100 mL. There was no significant correlation between the EPA and DHA values (r 2 = 0.045), and the EPA-to-DHA ratio in the plasma PL varied from 0.11 to 0.38 (mean 0.22).
TABLE 1
Mean Concentration of Plasma Cholesterol and Triglyceride During Supplementation and Depletion of Diet with o~3 PUFA
Plasma Plasma Week cholesterol triglyceride 0 4.50 +__ 0.93 b 0.95 + 0.25 2 4.37 __+ 1.00 0.84 + 0.49 6 4.40 _____ 0.93 1.03 • 0.47 aResults are expressed as mean +_ SD deviation, o~3 Polyunsatur- ated fatty acid (PUFA) supplementation period during weeks 0 to 2; o:3 PUFA depletion period, weeks 3 to 6.
bmmol/L.
LIPIDS, Vol. 28, no. 6 (1993)

D I F F E R E N T I A L UTILIZATION OF EPA AND DHA IN PLASMA
TABLE 2
Mean Concentration of Fatty Acids in Plasma Phospholipids, Cholesteryl Esters, Triglycerides and High Density Lipoprotein Phospholipids During Supplementation and Depletion of Diet with o~3 PUFA a
Plasma b
Week HDL b
527
Phospholipid Cholesteryl ester Triglycerides Phospholipid
14:0 0 -- -- 1.6 +- 0.8 b -- 2 -- -- 1.4 • 0.7 -- 6 -- -- 1.4 • 0.8 --
16:0 0 31.8 • 6.0 10.0 • 3.2 16.3 • 4.5 16.3 • 2.8 2 30.8 • 5.7 10.3 • 3.0 16.8 • 10.0 14.0 • 2.3 6 31.3 • 8.6 8.8 • 1.9 15.6 +- 7.1 15.7 • 1.7
16:1 0 1.4 • 0.5 2.8 • 1.2 3.3 • 2.0 0.4 • 0.1 2 1.1 • 0.4 2.7 • 1.1 2.5 • 1.5 0.4 • 0.1 6 1.3 • 0.6 2.8 • 1.3 2.8 • 1.5 0.5 • 0.2
18:0 0 13.2 • 2.9 1.3 • 0.4 3.5 • 0.8 6.9 • 1.2 2 15.0 • 3.7 1.1 • 0.4 3.1 • 1.7 6.1 • 0.9 6 13.7 • 1.9 1.0 • 0.3 3.0 • 1.6 6.7 • 0.9
18:1 0 14.7 • 2.2 17.1 • 5.4 26.7 • 4.1 7.2 • 1.5 2 13.1 • 2.7 17.1 • 5.8 24.6 • 12.7 6.1 • 1.5 6 14.5 • 4.0 15.4 • 4.5 26.6 • 12.1 6.8 • 1.2
18:2r 0 29.6 • 5.7 53.2 + 15.3 10.7 • 4.0 15.4 • 3.1 2 28.0 • 6.8 52.6 • 17.4 10.2 • 6.1 12.6 + 0.9 6 32.2 • 6.8 51.0 • 12.6 11.4 • 5.2 14.6 • 1.5
18:3r 0 0.4 • 0.3 0.6 • 0.2 0.7 • 0.3 0.2 • 0.1 2 0.3 • 0.2 0.5 • 0.2 0.6 • 0.5 0.1 • 0.0 6 0.4 • 0.2 0.5 • 0.2 0.6 • 0.2 0.1 • 0.0
20:3r 0 3.8 • 1.1 0.7 • 0.3 0.2 • 0.1 2.1 • 0.2 2 3.3 • 1.5 0.6 • 0.2 0.2 + 0.1 1.3 • 0.2 6 4.3 • 1.5 0.6 • 0.2 0.2 • 0.1 2.0 • 0.4
20:4r 0 10.3 • 2.5 5.4 +-- 2.1 0.6 • 0.3 5.9 • 1.0 2 11.2 • 2.7 5.6 • 1.7 0.7 • 0.4 4.8 • 0.6 6 11.8 +_ 4.5 4.9 • 1.9 0.5 • 0.3 5.3 +-- 0.6
20:5r 0 0.7 • 0.3 0.6 • 0.1 0.1 • 0.0 0.5 • 0.3 2 2.9 • 0.3 1.9 • 0.5 0.3 • 0.2 1.4 • 0.3 6 0.8 • 0.3 0.4 • 0.1 0.1 • 0.0 0.4 • 0.1
22:4r 0 0.3 • 0.1 -- 0.2 • 0.1 0.2 • 0.0 2 0.3 • 0.2 -- -- 0.1 • 0.0 6 0.4 • 0.2 -- 0.1 • 0.1 0.2 +-- 0.0
22:5r 0 0.8 • 0.3 -- 0.2 • 0.1 0.6 • 0.2 2 1.4 • 0.5 -- 0.3 • 0.2 0.7 • 0.2 6 1.0 • 0.3 -- 0.2 • 0.1 0.5 • 0.2
22:6w3 0 3.3 • 1.0 0.5 + 0.1 0.3 • 0.2 2.4 • 0.7 2 6.3 • 1.9 0.7 • 0.2 0.7 • 0.6 3.2 • 0.7 6 4.7 • 1.3 0.4 • 0.1 0.3 • 0.2 2.4 • 0.5
aResults are expressed as mean + SD. oJ3 Polyunsaturated fatty acid (PUFA) supplementation period during weeks 0 to 2; ~o3 depletion period, weeks 3 to 6. Normal values (in 39 females) for 20:5, 1.5 • 1.0; 22:5, 1.4 • 0.5; 22:6, 5.8 • 2.9 • SD). HDL, high density lipoprotein.
bmg]100 mL.
PUFA (iilean
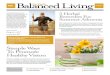
003 Supplementation phase. W i t h al l f r a c t i o n s s t u d i e d , t h e r e w a s a c o n s i s t e n t a n d r a p i d r i s e in t h e E P A concen - t r a t i o n a f t e r s u p p l e m e n t a t i o n s t a r t e d and , in m o s t f rac- t ions , t h e m a x i m u m i n c r e a s e h a d o c c u r r e d b y w e e k 1. T h e r e w a s a l e ss c o n s i s t e n t r e s p o n s e in t h e i n c r e a s e in D H A in t h e d i f f e r e n t f r a c t i o n s {Figs. 1-4). T h e i n c r e a s e s in t h e E P A a n d D H A c o n c e n t r a t i o n s b e t w e e n t h e s t a r t a n d w e e k 2 w e r e n o t r e l a t e d to t h e i n i t i a l E P A a n d D H A v a l u e s in t h e p l a s m a l i p id f r a c t i o n s .
T h e r e s u l t s for t h e p l a s m a P L s h o w e d t h a t t h e m a x - i m u m v a l u e s for E P A , D P A a n d D H A w e r e r e a c h e d a t 2 w k a f t e r s u p p l e m e n t a t i o n c o m m e n c e d (Fig. 1); t h e in- c r e a s e s in t h e c o n c e n t r a t i o n of t h e s e f a t t y a c i d s r e l a t i v e
t o t h e p ro - t r i a l v a l u e s w e r e 2.2, 0.6 a n d 3.0 m g / 1 0 0 m L p l a s m a for E P A , D P A a n d D H A , r e s p e c t i v e l y . T h e s e v a l u e s r e p r e s e n t e d i n c r e a s e s of 4.1, 1.7, 1 .9X t h e i n i t i a l va lues , r e s p e c t i v e l y ( P < 0.0001, 0.019, 0 .0024, respec- t ive ly) . T h e r e w a s a s t e p w i s e i n c r e a s e in t h e D H A leve l f r o m w e e k 1 t o w e e k 2 of t h e s u p p l e m e n t a t i o n p h a s e com- p a r e d w i t h t h e r i s e in E P A w h i c h h a d p l a t e a u e d b y t h e e n d of w e e k 1 o f t h e s u p p l e m e n t a t i o n .
S i m i l a r r e s u l t s w e r e s e e n for t h e p l a s m a C E E P A con- c e n t r a t i o n w h e r e t h e r e w a s a r a p i d r i s e b y w e e k 1 {Fig. 2); t h e i n c r e a s e in E P A in t h i s f r a c t i o n w a s b y a f a c t o r o f 3.4 Can i n c r e a s e o f 1.3 m g / 1 0 0 m L ) (P < 0.0003). T h e D H A in t h e C E f r a c t i o n a l so rose s i g n i f i c a n t l y {P < 0.019)
LIPIDS, Vol. 28, no. 6 (1993)

528
J. HODGE ET AL.
0 0
0
0 0 p-(
E
5 . 0 -
4.0-
3.0-
2.0-
1.0-
0.0 5.0
4.0-
3.0-
2.0-
1.0
0.0 7.0
6.0
5.0
4.0
3.0
20:5o33
I I I l I I
22:5co3
I I i I ! 1
m m
0.0 I , , , , 0 i 2 3 5 6
co3 supplement l,, co3 depletion I Week
FIG. 1. The concentration (mean +_ SD) of ~03 long-chain polyun- saturated fatty acids (PUFA) in plasma phospholipids during SUl~ plementation and depletion of diet with o~3 PUFA. Paired t-tests were conducted between the week 2 and week 0 samples, and between the week 6 and week 0 samples (*P< 0.05, **P < 0.01, ***P < 0.00D.
by 0.5 mg/100 mL, a factor of 1.5. There was no detectable DPA in the CE fraction.
In the plasma TG fraction, only the 22 carbon r LCP were evident and only at a low concentration (Table 2); the increases in these fatty acids during the supplementation period were not significant (Fig. 3).
The concentration of o03 LCP in the HDL PL was about 70% of the total plasma PL (o3 LCP concentration {Table 2). In contrast to the total plasma PL, the rise in all three r LCP in this fraction was maximal after 1 wk of sup- plementation (Fig. 4). The maximum increases in the con- centration of the (o3 LCP relative to the pre-trial values
LIPIDS, Vol. 28, no. 6 (1993)
E 0 0 p-4
0
2.0.
1.0.
0 . 0
2.0-
l.O �84
! I I I I I
22:66o3
. 0 I !
o i ; 5 6
Ico3 supplement I o)3 depletion
Week
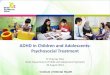
FIG. 2. The concentration (mean _+ SD) of ~3 long~hain polyun- saturated fatty acids (PUFA) in plasma eholesteryl esters during supplementation and depletion of diet with ~3 PUFA. Paired t-tests were conducted between the week 2 and week 0 samples, and bet- ween the week 6 and week 0 samples t*P < 0.05, ***P < 0.001).
were: EPA 1.3 mg/100 mL (P < 0.003), DPA 0.3 mg/100 mL (P < 0.0083), DHA 0.8 mg/100 mL (P < 0.0024).
0.)3 Depletion phase There was a rapid depletion of EPA and DPA in all of the total plasma and HDL fractions (Figs. 1-4), with the values returning to pre-trial levels within 1 wk.
In the case of DHA, there was a slower depletion than for the other two r LCP, particularly in the total plasma PL (Fig. 1). The DHA concentration had returned to pre- trial values by week 4 for the plasma CE and HDL PL and by week 5 for plasma TG. For the plasma PL there was a substantial drop in the DHA concentration in the first week of depletion (week 3), but no further fall in the remaining 3 wks. For six of the seven subjects examined, the DHA values did not return to the baseline values dur- ing the depletion phas~ In one subject it reached baseline in weeks 5 and 6. At the end of the experiment, the mean plasma PL DHA concentration was still 40% above the baseline figure {P < 0.02) {Fig. 1).
DISCUSSION
The results of this experiment indicate that there were differences in the rate of accumulation and decay of the

529
g
E
1,2 ~
g
22:50)3
1.0~ 0.8~
0.6~
0.4
0 . 2 '
0.0 1.2.
1.o- o.s: 0 . 6 -
0.4. 0 . 2
0.0 o i
O O
~ _ _ _ Z _ _ _ . ~ _ _ _ X '1" .I. i
! ! I I i I
! I
4 5 6
I0)3 supplement I 0)3 depletion
2 . 0 -
E
W e e k
FIG. 3. The concentration (mean __+ SD) of co3 bag-chain polynn- <> saturated fatty acids (PUFA) in plasma triglyeerides during sup-
plemeatation and depletion of diet with ~03 PUFA. Paired t-tests were "~ conducted between the week 2 and week 0 samples, and between the week 6 and week 0 samples.
three co3 LCP in the plasma lipids during the supplemen- tation and depletion phases, respectively. The EPA ac- cumulated in the plasma PL and CE more rapidly than DPA and DHA, and in the depletion phase the EPA and DPA decayed more rapidly compared with DHA, par- ticularly in the plasma PL. The EPA and DPA had return- ed to pre-trial values within one week in all plasma frac- tions whereas there was a slower decrease in the DHA con- centrations and, in the case of the plasma PL, the DHA still remained above the pretrial concentration 4 wk after the supplementation had finished. These results are consistent with those reported by
Bronsgeest-Schoute et al. (18), where volunteers were given different doses of fish oils {1.4-8.2 g/d of o~3 fatty acids) for 4 wk, and the effects of the plasma lipids were monitored during this period and for a further 2 wk after supplementation ceased. At the completion of the experi- ment for the three highest dose levels, the EPA, but not the DHA values, had returned to their pretrail levels in the plasma CE, TG and phosphatidylcholine fractions. Similar results have been reported by others for erythro- cytes and platelets {12,19). The slow return of erythrocyte DHA to baseline by comparison with EPA has been noted in particular by Brown et al. {20). They reported that 12 wk after fish plus fish oil supplementation had finished
1.0 �84
0.0 2 .0
1.0 �84
0.0 4 . 0
I I i I I I
3.0
: .
I I l I i I
22:50)3
DIFFERENTIAL UTILIZATION OF EPA AND DHA IN PLASMA
m
0.0 !
0 1 2 3 4 ~
Week FIG. 4. The concentration (mean _.+ SD) of co3 long~hain polyun- saturated fatty acids (PUFA) in high-density lipoprotein plasma phospholipids during supplementation and depletion of diet with ~03 PUFA. Paired t-tests were conducted between the week 2 and week 0 samples, and between the week 6 and week 0 samples **P< 0.0L
in eight volunteers, the degree of retention of erythrocyte EPA was 16% compared with a 44% retention of DHA (values expressed as a percent of the maximum increase on the fish plus fish oil diet). The present study differs from those discussed above, since in none of the previous studies was there a specific reduction in the dietary in- take of ~3 LCP during the "washout" phase, thus con- founding the possible interpretation of the results for the decay of the co3 fatty acids. There was an interesting difference between the disap-
pearance of the co3 fatty acids from HDL PL and total
LIPIDS, Vol. 28, no. 6 (1993)

530
J. HODGE ET AL.
plasma PL: in the former case, the DHA values returned to baseline within 2 wk whereas the disappearance from the total plasma was much slower. Although the interrela- tionships between the PLs in the different plasma lipopro- teins are a poorly understood area of study, these results suggest there may be different rates of metabolism for the acyl chains in the PLs of the plasma lipoproteins.
These results also showed differences in the distribu- tion of r LCP in the lipid classes of the plasma and a disproportional accumulation of DHA. Most of the EPA was incorporated into both the PL and CE fractions (44% in PL, 48% in CE), whereas DPA and DHA were mainly found in the PL fraction (86 and 83%, respectively). This partitioning of EPA and DHA into different plasma lipids has been noted previously (18) and might be explained by differences in the positional specificity of EPA and DHA in the chylomicron TG (21,22). There was also a dispropor- tional increase in the DHA in the plasma fipids. For ex- ample, at the end of the supplementation phase, the DHA- to-EPA ratio in the plasma lipids was 1.0 (expressed as the increase in DHA in the plasma lipid fractions, PL plus CE plus TG, over the 2-wk supplementation period/in- crease in EPA) compared with a ratio of 0.7 (DHA-to-EPA) in the supplementary fish off. The DPA-t~EPA ratio in the plasma lipids was 0.19 compared with 0.15 in the sup- plement, and the DPA-to-DHA ratio was 0.20 in both the plasma and the supplement. These calculations assume that most of the LCPw3 in the supplementation phase was derived from the fish oil supplement and not from other dietary sources such as fish. A disproportional increase in DHA into various tissues relative to EPA has been reported for rabbits and rats fed fish oils (23,24). In the former article, it was estimated that DHA was three times more likely to be incorporated into adipose tissue than was EPA: the authors speculated that EPA was diverted into alternative metabolic pathways such as oxidation or deposition in other tissues.
The results from this and other studies showing marked differences in the fate of EPA and DHA following inges- tion may allow an explanation of the low EPA levels in plasma lipids relative to the DHA levels. These data are consistent with the following possibilities: (i) that EPA is absorbed less effectively than DHA. This is not con- sistent with the data on the absorption of EPA and DHA from MaxEPA in the rat (22). (if) That EPA is rapidly removed from the plasma pools to other tissues. This is not consistent with data showing disproportional in- creases in DHA relative to EPA in a variety of tissues (fiver, muscle, adipose) (23,24). (iii) That EPA is E-oxidized faster than DHA. This is consistent with a preliminary report which indicated a more rapid in vitro/~-oxidation of EPA compared with DHA in rat liver and muscle (25), a significantly greater rate of acylcarnitine synthesis of EPA compared with DHA in rat fiver mitochondria (26) and an accelerated loss of a-linolenic acid and EPA com- pared with DHA in adipose tissue of human subjects undergoing weight loss (27). Gronn et al. (28) have in- dicated that the feeding of fish oil or purified w3 PUFA to rats stimulates fat ty acid oxidation in both mitochon- dria and peroxisomes and leads to an increased perox- isomal oxidation of (o3 PUFA. This report did not indicate whether there was any difference between the rate of ox- idation of EPA and DHA. Zhang et aL (29) have reported that in the perfused rat fiver, there is significantly less
EPA compared with DHA incorporated into very low den- sity lipoprotein lipids which is consistent with a greater of oxidation of EPA in the fiver. (iv) That there is a rapid conversion of EPA to DHA. There have been no experi- ments conducted in humans which have directly ad- dressed this issue Indirect evidence from experiments of several weeks' duration does not support the view that EPA is rapidly transformed to DPA and DHA in humans. These experiments involved a variety of dietary changes, such as feeding canola off or lean meat, which induced in- creases in EPA or EPA and DPA, respectively, in plasma or white cell lipids (13,30}. These data do not rule out the possibility of slow conversion or the possibility of any DPA and DHA formed being transferred from the plasma to a tissue such as adipose (27). There must be some con- version of a-linolenic acid to DHA in humans since vegan vegetarians have normal levels of EPA and DHA in their plasma lipids {10), although the direct measurement of metabolism of deuterated a-linolenic acid suggests that the process is very slow (31). (v) That there is a lower in- take of EPA than DHA in typical Western diets. Dietary sources of EPA and DHA in typical Western diets such as those consumed in Australia would include fish (EPA- rich for fatty fish and DHA-rich for lean fish, Ref. 32), lean red meat {which contains EPA plus DPA, Ref. 15), offal {which contains EPA, DPA, DHA) and eggs {which con- tain DHA) {14}. Furthermore some EPA and DPA may be produced by the slow conversion of dietary a-linolenic acid to EPA {30,31}. It is possible that the dietary intake of EPA is lower than that of DHA in some individuals (eg., diets containing fish low in fat and therefore DHA- rich, and eggs, which contain DHA but no EPA), but in general the EPA intake on a diet containing a variety of foods should be of the same order as that of DHA, as we have shown previously {13).
In conclusion, the relatively low levels of EPA compared with DHA in human plasma may be the result of a lower intake of EPA and an increased E-oxidation of EPA relative to DHA. One practical outcome of this data, especially for those with low levels of (o3 LCP, is that maintenance of increased EPA levels in plasma (and therefore tissues} would require constant inputs of EPA due to the relatively rapid loss of EPA from tissues.
ACKNOWLEDGMENTS The willing participation of the subjects is gratefully acknowledg- eel The authors also thank Miranda Hughes and Dr. Bob Gibson for constructive criticism of the manuscript.
REFERENCES 1. Budowski, P. (1988) Wld Rev. Nutr. Diet. 57, 214-274. 2. Kinsella, J.E., Lokesh, B., and Stone, R.A. (1990) Am. J. Clir~
Nutr. 52, 1-28. 3. Neuringer, M., Anderson, G.J., and Connor, W.E. (1988) Anr~ Rev.
Nutr. 8~ 517-541. 4. Dyerberg, J., and Jorgensen, K.A. (1982) Frog. Lipid Res. 21,
255-269. 5. Simopoulos, A.R (1989) J. Nutr. 119, 521-528. 6. Adam, O. (1989) in Dietary w6 and r Fatty Acids. Biological
Effects and Nutritional Essentiality (Galli, C., and Simopoulos, A.R, eds.) pp. 33-42, Plenum Press, New York.
7. Hunter, J.E. (1990) Am. J. Clin. Nutr. 51, 809-814. 8. Bjerve, K.K, Brubakk, A.M., Fougner, K.J., Johnsen, H., Mid-
jthell, K., and Vik, T. (1993) Am. J. Clin. Nutr., in press.
LIPIDS, Vol. 28, n~ 6 (1993)

531
DIFFERENTIAL UTILIZATION OF EPA AND DHA IN PLASMA
9. Glatz, J.F.C., Soffem, A.E.M.F., and Katan, M.B. (1989) Am. J. Clin. Nutr. 49, 269-276.
10. Phinney, S.D., Odin, R.S., Johnson, S.B., and Holman, R.T. (1990) Am. J. Clin. Nutr. 51, 385-392.
11. Cleland, L.G., James, M.J., Neumann, M.A., D'Angelo, M., and Gibson, R.A. (1992) Am. J. Clin. Nutr. 55, 395-399.
12. Brown, A.J., Pang, E., and Roberts, D.C.K. (1991) Prostaglan- dins Leukotrienes and Essential Fatty Acids 44, 103-106.
13. Sinclair, A.J., O'Dea, K., Dunstan, G., Ireland, P.D., and Niall, M. (1987) Lipids 22, 523-529.
14. Sinclair, A.J., and O'Dea, K. (1990) in Reducing Fat in Meat Animals (Wood, J.D., and Fisher, A.V., eds.) pp. 1-47, Elsevier, New York.
15. Sinclair, A.J., and O'Dea, K. (1987)Food Australia 39, 232-233. 16. Sinclair, A.J., McLean, J.G., and Monger, E.A. (1979) Lipids 14,
932-936. 17. Radack, K.L., Deck, C.C., and Huster, G.A. (1990) Am. J. Clin.
Nutr. 51, 599-605. 18. Bronsgeest~Schoute, H.C., van Gent, C.M., Luten, J.B., and Ruiter,
A. (1981) Am. J. Clin. Nutr. 34, 1752-1757. 19. Mori, T.A., Codde, J.P., Vandongen, R., and Beilin, L.J. (1987)
Lipids 22, 744-750. 20. Brown, A.J., Pang, E., and Roberts, D.C. (1991) Am. J. Clin. Nutz.
54, 668-673. 21. Nelson, G.J., and Ackman, R.G. (1988) Lipids 23, 1005-1014.
22. Chernenko, G.A., Barrowman, J.A., Kean, K.T., Herzberg, G.R., and Keough, ILM.W. {1989) Biochim. Biophys. Acta I(D~ 95-102.
23. Lin, D.S., and Connor, W.E. (1990)Am- J. Cli~ Nu~ 51, 535-539. 24. Sheppard, IL, and Herzberg, G.IL {1992)Nu~ Res. 12, 1405-1418. 25. Herzberg, G.R., Skinner, C., and Levy, R. {1992) in Third Inter-
national Conference on Essential Fatty Acids and Eicosanoids, Adelaide, Australia, Poster 31.
26. Gavino, G.R., and Gavino, V. (1991} Lipids 26, 266-270. 27. Phinney, S.D., Tang, A.B., Johnson, ~B., and Holman, R.T. {1990}
Lipids 25, 798-806. 28. Gronn, M., Christensen, E., Hagve" TA., and Christophersen, B.O.
{1992} Biochim. Biophys. Acta 1125, 35-43. 29. Zhang, Z.J., Wilcox, H.G., Elarn, M.B., Castellani, L.W., and
Heimberg, M. (1991} Lipids 26, 504-511. 30. Corner, E.J., Bruce, V.M., and McDonald, B.E. (1990} Lipids 25,
598-601. 31. Emken, E.A., Adlof, R.O., Rohwedder, W.K., and Gulley, R.M.
(1993} in Essential Fatty Acids and Eicosanoids {Sinclair, A.J., and Gibson, R.A., eds.) pp. 23-25, AOCS Press, Champaigru
32. Sinclair, A.J., Dunstan, G.A., Naughton, J.M., Sanigorski, A.J., and O'Dea, K. {1992} Aust. J. Nutr. Dieter. 49, 77-83.
[Received July 17, 1992, and in revised form March 31, 1993; Revision accepted April 7, 1993]
LIPIDS, Vol. 28, no. 6 (1993)