Embed Size (px)
Citation preview
Differential Diagnosis of Dementias
George T. Grossberg, MD
Samuel W. Fordyce Distinguished Professor
Director, Geriatric Psychiatry
Department of Neurology & Psychiatry
St Louis University School of Medicine

2
Disclosures
• None for this presentation

3
Differential Diagnosis of Dementias
Presentation Overview
Clinical evaluation for dementia
Cognitive assessment tools
Profiles of common dementias
Imaging the different dementias
Neuropsychiatric symptoms in dementias
4
Common Types of Neurodegenerative
Dementia1
Alzheimer’s dementia (AD)
Parkinson’s disease dementia (PDD)
Dementia with Lewy bodies (DLB)
Vascular dementia (VaD)
Frontotemporal dementia (FTD)
Mixed (multiple pathologies/etiologies) dementia
Lewy Body
Dementia
Spectrum2
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR®.) Washington, DC: American
Psychiatric Association; 2000.
2. Lewy Body Dementia Association, Inc. 2010. Caregiver Burden in Lewy Body Dementias: Challenges in Obtaining Diagnosis and Providing Daily Care. Atlanta, GA:
Lewy Body Dementia Association; 2010.
5
The Typical Dementia Scenario
• Patients may not seek medical care for symptoms
• Lack of insight common
• Patient denies problem, family/friends express
concerns
• Caregivers may gradually compensate and cover
up symptoms for the patient, "masking" the true
magnitude of the deficits
• Delayed diagnosis until moderate stage
Agronin ME. Alzheimer disease and other dementias : a practical guide. 2nd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.
6
Core features of degenerative dementia
• Deficits in cognitive domains that may include
memory
• Usually progressive deterioration
• Cognitive impairment interferes with social or
occupational function
• Not attributable to another disorder
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR®.) Washington, DC:
American Psychiatric Association; 2000.

7
Clinical Evaluation for Dementia1
History
Physical,
Neurologic,
Mental Status
Examinations
Laboratory,
Psychiatric, and
Neuropsych Tests
• Obtain medical and psychiatric history, along
with current symptoms
• Include collateral source such as family or
other informant
• Identify neurologic deficits
• Conduct general screen for cognitive
impairment
• Identify reversible causes of cognitive
impairment
• Build on mental status examination, and
provide clearer picture of pattern and degree
of cognitive impairment
Agronin ME. Alzheimer disease and other dementias : a practical guide. 2nd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.

8
The “Dementia Workup”
• Detailed history from patient & reliable informant
• Head to toe physical & neurological examination
• Bloodwork(if not done recently)-
CMP;CBC;TSH;B12/Folate; ?vit
D;?CRP;?Homocysteine
• RPR, HIV testing(if indicated)
• Plain CT/MRI(one time);?FDG-PET;?amyloid-
PET
• UA;CXRY(if indicated);EKG
• EEG,LP- not part of routine workup
9
Delirium is a Reversible Cause of Cognitive
Impairment
Dehydration
Electrolyte/Endocrine disorder
Lack of oxygen
Injury/Impaction
Rule out psychiatric disorder
Infection
Urinary retention/Unfamiliar environment
Medications
Desai AK, Grossberg GT. Psychiatric consultation in long-term care : a guide for health care professionals. Baltimore: Johns Hopkins University Press; 2010.

10
Delirium, Dementia, and Depression1,2
Delirium Dementia Depression
Onset Sudden Insidious Recent or recurrent
Duration Minutes to
days Months to years Weeks to months
Progression
Reversible –
resolves with
treatment
Irreversible Reversible, relapses
common
Consciousness Fluctuating Generally alert Generally alert,
possibly withdrawn
History of
depression
Usually
negative Usually negative Usually positive
Visuospatial Preserved Often abnormal Preserved
Mood – Sadness/
Guilt/Worthlessness Absent Usually absent Usually Present
1. Cefalu C, Grossberg GT. Leawood, KS: American Academy of Family Physicians; 2001. 2. American Psychiatric Association. DSM-IV-TR®.
Washington, DC: American Psychiatric Association; 2000.

11
Examples of Cognitive Assessment Tools
for the Office Setting
• Mini-Mental State Examination (MMSE)1
• AD8 informant interview2
• Mini-Cog assessment3
• Montreal Cognitive Assessment (MoCA)4
• St Louis University Mental Status (SLUMS)
Examination5
1. Folstein MF et al. J Psychiatr Res. 1975;12:189-198. 2. Galvin JE et al. Neurology. 2005;65:559-564. 3. Borson S et al. Int J Geriatr Psychiatry.
2000;15:1021-1027. 4. Nasreddine ZS et al. J Am Geriatr Soc. 2005;53:695-699. 5. Tariq SH et al. Am J Geriatr Psychiatry. 2006;14:900-910.
Note. These are assessment tools, and are not fully diagnostic of dementia.
12
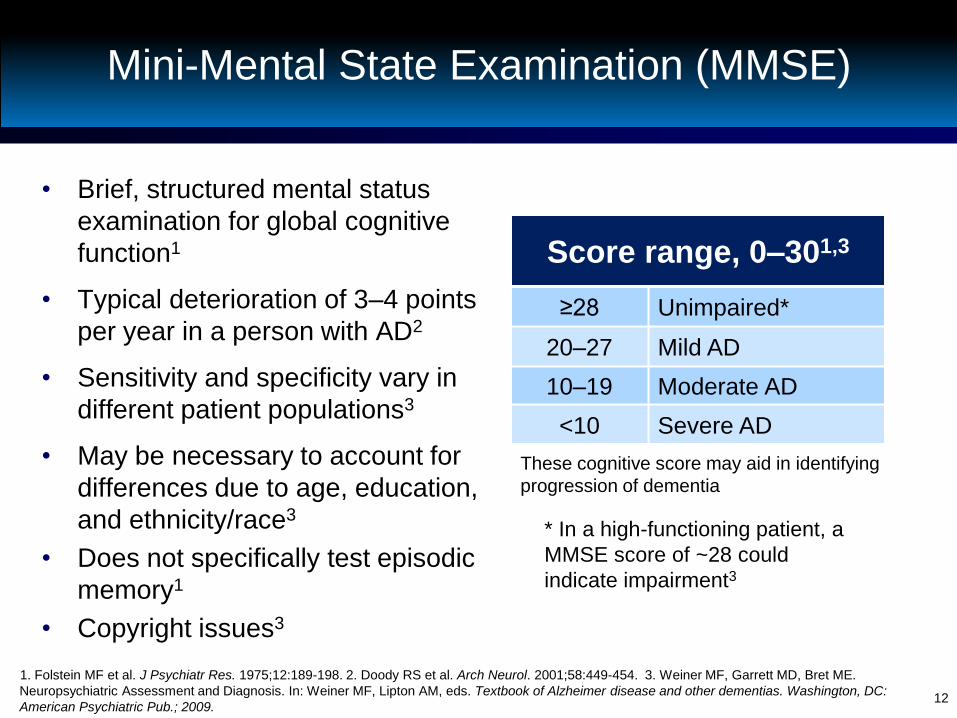
Mini-Mental State Examination (MMSE)
• Brief, structured mental status
examination for global cognitive
function1
• Typical deterioration of 3–4 points
per year in a person with AD2
• Sensitivity and specificity vary in
different patient populations3
• May be necessary to account for
differences due to age, education,
and ethnicity/race3
• Does not specifically test episodic
memory1
• Copyright issues3
1. Folstein MF et al. J Psychiatr Res. 1975;12:189-198. 2. Doody RS et al. Arch Neurol. 2001;58:449-454. 3. Weiner MF, Garrett MD, Bret ME.
Neuropsychiatric Assessment and Diagnosis. In: Weiner MF, Lipton AM, eds. Textbook of Alzheimer disease and other dementias. Washington, DC:
American Psychiatric Pub.; 2009.
Score range, 0–301,3
≥28 Unimpaired*
20–27 Mild AD
10–19 Moderate AD
<10 Severe AD
These cognitive score may aid in identifying
progression of dementia
* In a high-functioning patient, a
MMSE score of ~28 could
indicate impairment3
13
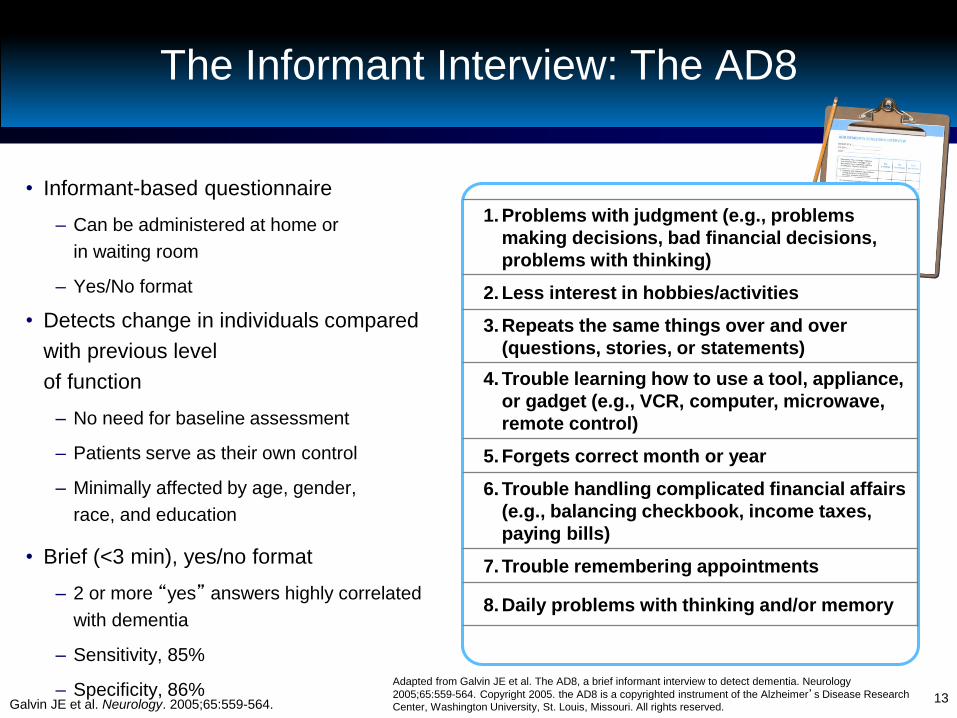
1. Problems with judgment (e.g., problems
making decisions, bad financial decisions,
problems with thinking)
2. Less interest in hobbies/activities
3. Repeats the same things over and over
(questions, stories, or statements)
4. Trouble learning how to use a tool, appliance,
or gadget (e.g., VCR, computer, microwave,
remote control)
5. Forgets correct month or year
6. Trouble handling complicated financial affairs
(e.g., balancing checkbook, income taxes,
paying bills)
7. Trouble remembering appointments
8. Daily problems with thinking and/or memory
The Informant Interview: The AD8
• Informant-based questionnaire
– Can be administered at home or
in waiting room
– Yes/No format
• Detects change in individuals compared
with previous level
of function
– No need for baseline assessment
– Patients serve as their own control
– Minimally affected by age, gender,
race, and education
• Brief (<3 min), yes/no format
– 2 or more “yes” answers highly correlated
with dementia
– Sensitivity, 85%
– Specificity, 86% Galvin JE et al. Neurology. 2005;65:559-564.
Adapted from Galvin JE et al. The AD8, a brief informant interview to detect dementia. Neurology
2005;65:559-564. Copyright 2005. the AD8 is a copyrighted instrument of the Alzheimer’s Disease Research
Center, Washington University, St. Louis, Missouri. All rights reserved.

14
Rapid Screen for
Cognitive Impairment: Mini-Cog
• Rapid screen for cognitive
impairment
– 5 minutes to administer
• 3-word registration
• Simple clock-drawing test
• 3-item recall
• Not influenced by education
level or language
• Sensitivity, 99%
• Specificity, 93%
Borson S et al. Int J Geriatr Psychiatry. 2000;15:1021-1027.
Abnormal Clock Normal Clock
Demented
Nondemented Demented
Nondemented
Recall 0 Recall 1-2 Recall 3
Mini-Cog
Adapted from Borson S et al. Int J Geriatr Psychiatry. 2000;15:1021-1027; with permission.
15
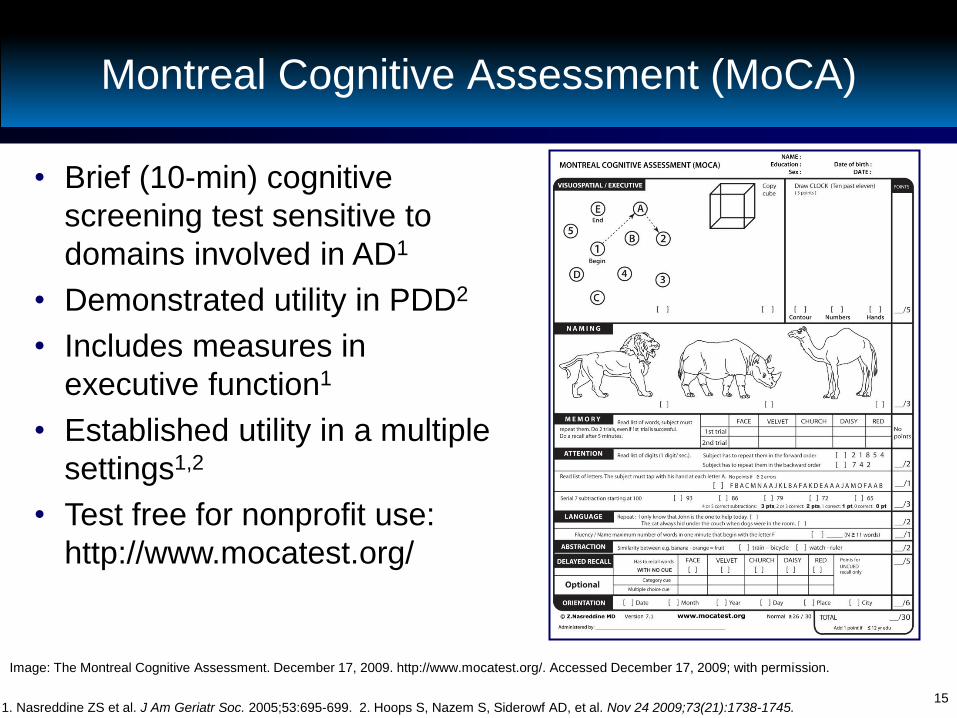
Montreal Cognitive Assessment (MoCA)
1. Nasreddine ZS et al. J Am Geriatr Soc. 2005;53:695-699. 2. Hoops S, Nazem S, Siderowf AD, et al. Nov 24 2009;73(21):1738-1745.
Image: The Montreal Cognitive Assessment. December 17, 2009. http://www.mocatest.org/. Accessed December 17, 2009; with permission.
• Brief (10-min) cognitive
screening test sensitive to
domains involved in AD1
• Demonstrated utility in PDD2
• Includes measures in
executive function1
• Established utility in a multiple
settings1,2
• Test free for nonprofit use:
http://www.mocatest.org/

16
Saint Louis University Mental Status
Examination
• Designed to improve screening for mild neurocognitive disorder (MNCD)
• 11-item, clinician-scored scale
• Study of SLUMS vs MMSE (N = 705)
– DSM-IV-TR® criteria used to diagnose MNCD or dementia
– Patients assessed by MMSE and SLUMS
– Sensitivity and specificity
• Dementia: similar for MMSE and SLUMS
• MNCD: SLUMS appears superior to MMSE
Tariq SH et al. Am J Geriatr Psychiatry. 2006;14:900-910.
High School
Education
Less Than High
School Education
Normal 27–30 25–30
MNCD 21–26 20–24
Dementia 1–20 1–19

17
Rapid Brief Cognitive Screens:
Pros and Cons
Screening Test Pros Cons
MMSE1,2
Widely used, validated, reliable
Adjustments for age, education, and
race may be necessary
Copyright issues
AD8 informant
interview3 Reliable, sensitive, specific, rapidly administered Knowledgeable informants may not be
readily available
Mini-Cog
assessment4 Superior to MMSE in prediction of dementia
status, rapidly administered, produces a visible
performance indicator
Clock-drawing test scoring is vulnerable
to varying interpretations
MoCA5,6 Useful in patients with scores >25 on MMSE,
strong executive function component Conclusions regarding validity in PDD
restricted to specialty clinic setting
SLUMS
examination7 Potentially superior to MMSE for early detection of
cognitive impairment
Research needed to confirm applicability
beyond initial study group
Note: insufficient information is available to determine whether any one screening tool is superior to another. Positive
screening results should be followed by complete neurologic and medical examinations.
1. Folstein MF et al. J Psychiatr Res. 1975;12:189-198. 2. Weiner MF, Garrett MD, Bret ME. Neuropsychiatric Assessment and Diagnosis. In: Weiner
MF, Lipton AM, eds. Textbook of Alzheimer disease and other dementias. Washington, DC: American Psychiatric Pub.; 2009. 3. Galvin JE et al.
Neurology. 2005;65:559-564. 4. Borson S et al. Int J Geriatr Psychiatry. 2000;15:1021-1027. 5. Nasreddine ZS et al. J Am Geriatr Soc. 2005;53:695-
699. 6. Zadikoff C et al. Mov Disord. 2008;23:297-299. 7. Tariq SH et al. Am J Geriatr Psychiatry. 2006;14:900-910.

Profiles of Dementias

19
Alzheimer’s Dementia
• Multiple cognitive deficits, consisting of
memory impairment and ≥11
– Aphasia
– Apraxia
– Agnosia
– Executive function
• Each deficit causes significant impairment
in social or occupational functioning1
• Difficulty learning and remembering
new information2
• Repetitiveness, anomia2
• Poor orientation to time2
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR®.) Washington, DC: American
Psychiatric Association; 2000. 2. Geldmacher D. Alzheimer’s Disease. In: Weiner MF, Lipton AM, eds. Textbook of Alzheimer disease and other dementias. 1st ed.
Washington, DC: American Psychiatric Pub.; 2009. 3. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. In: Weiner MF, Lipton AM,
eds. Textbook of Alzheimer disease and other dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.
Co
re
Clin
ica
l
AD largely
involves
temporal-
parietal deficits3
Praxis
Language
Gnosis

20
Parkinson’s Disease Dementia
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR®.) Washington, DC: American Psychiatric
Association; 2000. Emre M, Aarsland D, Brown R, et al. Mov Disord. Sep 15 2007;22(12):1689-1707; quiz 1837. 3. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and
other Synucleinopathies. In: Weiner MF, Lipton AM, eds. Textbook of Alzheimer disease and other dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.
Co
re
Clin
ica
l
• Develops in the context of established PD (>2
years)1
• Cognitive and motor slowing with significant
impairments in:1,2
– Executive function
– Memory retrieval
• A decline from premorbid levels, with deficits
sufficient to impair function1,2
• Slowing of cognitive processes/processing
speed2
• Fluctuating attention deficits2
• Difficulties with abstraction and visuospatial
skills2
PDD affects the
basal ganglia
first, and
disrupts
ascending
subcortical
circuits3
21
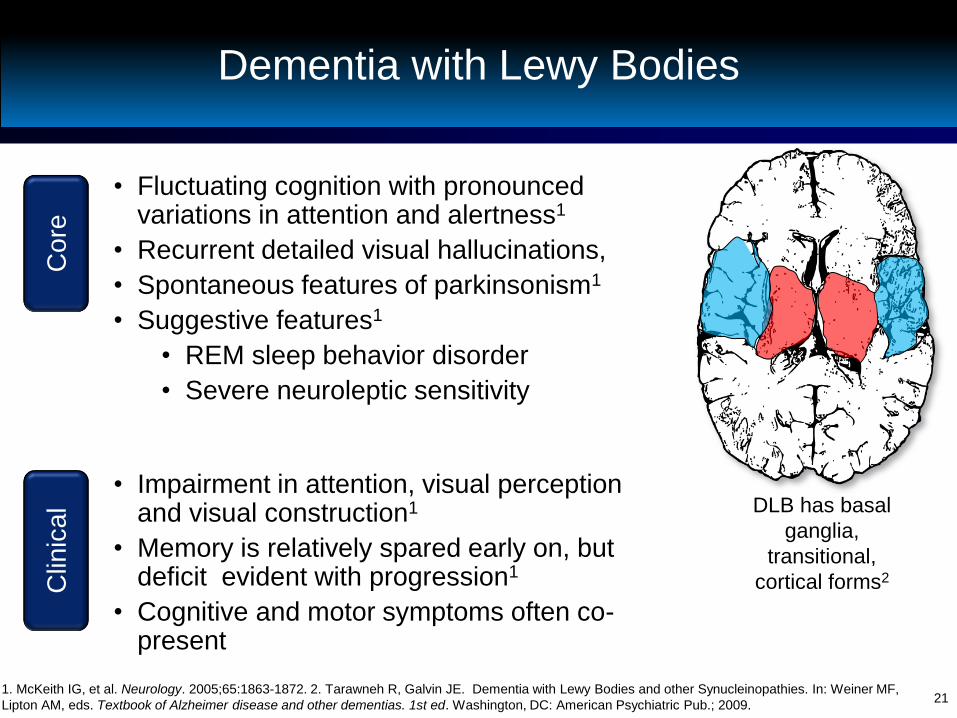
Dementia with Lewy Bodies C
ore
C
linic
al
• Fluctuating cognition with pronounced variations in attention and alertness1
• Recurrent detailed visual hallucinations,
• Spontaneous features of parkinsonism1
• Suggestive features1
• REM sleep behavior disorder
• Severe neuroleptic sensitivity
• Impairment in attention, visual perception and visual construction1
• Memory is relatively spared early on, but deficit evident with progression1
• Cognitive and motor symptoms often co-present
1. McKeith IG, et al. Neurology. 2005;65:1863-1872. 2. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. In: Weiner MF,
Lipton AM, eds. Textbook of Alzheimer disease and other dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.
DLB has basal
ganglia,
transitional,
cortical forms2

22
Vascular Dementia
• Decline in cognitive function from a
prior baseline and a deficit in
performance in ≥21
– Executive/attention
– Memory (may not always be impaired)2
– Language
– Visuospatial function
• Evidence of cerebrovascular
disease via neuroimaing1,3,4
• Focal neurological signs that
may relate to vascular lesion
location1,3,4
• Cognitive deficits may occur in
a stepwise fashion1,3,4
1. Gorelick PB, Scuteri A, Black SE, et al. Stroke. Sep 2011;42(9):2672-2713. 2. Szoeke CE, Campbell S, Chiu E. Vascular Cognitive Disorder. In: Weiner MF,
Lipton AM, eds. Textbook of Alzheimer disease and other dementias. Washington, DC: American Psychiatric Pub.; 2009. 3. American Psychiatric Association.
Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition. Text Revision. (DSM-IV-TR®.) Washington, DC: American Psychiatric Association; 2000.
4. Roman GC, Tatemichi TK, Erkinjuntti T, et al. Neurology. Feb 1993;43(2):250-260.
Co
re
Clin
ica
l

23
Frontotemporal Dementia
• FTD may be classified into various subtypes1,2
– Primary progressive aphasia (PPA)
• Progressive nonfluent aphasia
• Logopenic variant
• Semantic dementia (SD)
– Behavioral Variant (bvFTD)
• PPA primarily affects language early, whereas
bvFTD may be classified as an early behavioral
disorder1
• FTD variants may overlap later in the disease
course1,2 1. Lipton AM, Boxer A. Frontotemporal Dementia. In: Weiner MF, Lipton AM, eds. Textbook of Alzheimer disease and other dementias. Washington, DC:
American Psychiatric Pub.; 2009.2. Gorno-Tempini ML, Hillis AE, Weintraub S, et al. Neurology. Mar 15 2011;76(11):1006-1014.
24
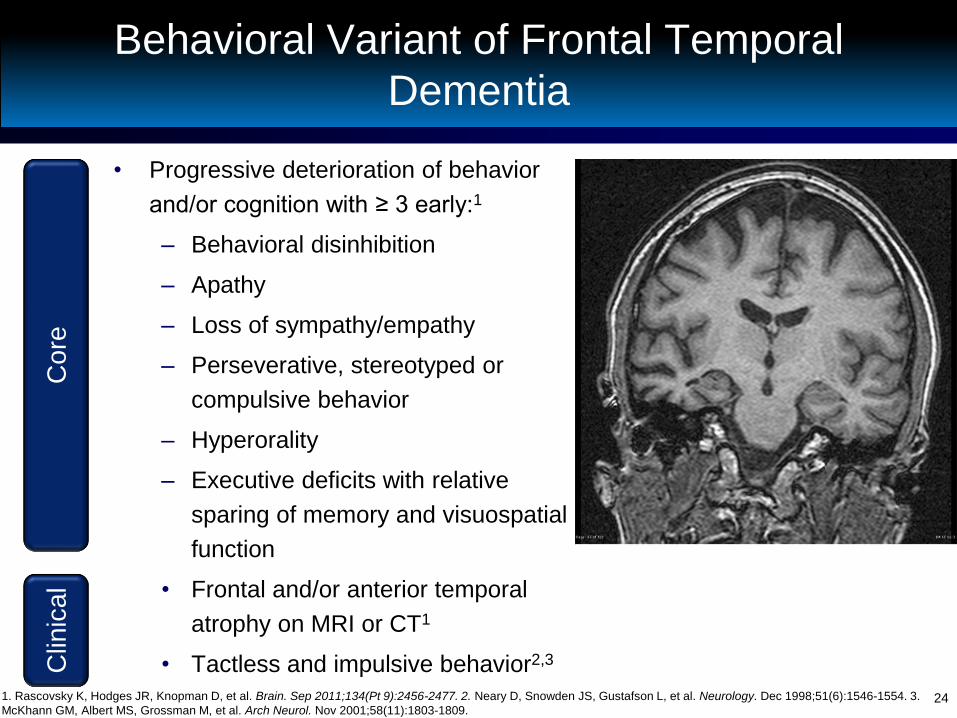
Behavioral Variant of Frontal Temporal
Dementia
• Progressive deterioration of behavior
and/or cognition with ≥ 3 early:1
– Behavioral disinhibition
– Apathy
– Loss of sympathy/empathy
– Perseverative, stereotyped or
compulsive behavior
– Hyperorality
– Executive deficits with relative
sparing of memory and visuospatial
function
• Frontal and/or anterior temporal
atrophy on MRI or CT1
• Tactless and impulsive behavior2,3 1. Rascovsky K, Hodges JR, Knopman D, et al. Brain. Sep 2011;134(Pt 9):2456-2477. 2. Neary D, Snowden JS, Gustafson L, et al. Neurology. Dec 1998;51(6):1546-1554. 3.
McKhann GM, Albert MS, Grossman M, et al. Arch Neurol. Nov 2001;58(11):1803-1809.
Co
re
Clin
ica
l
25
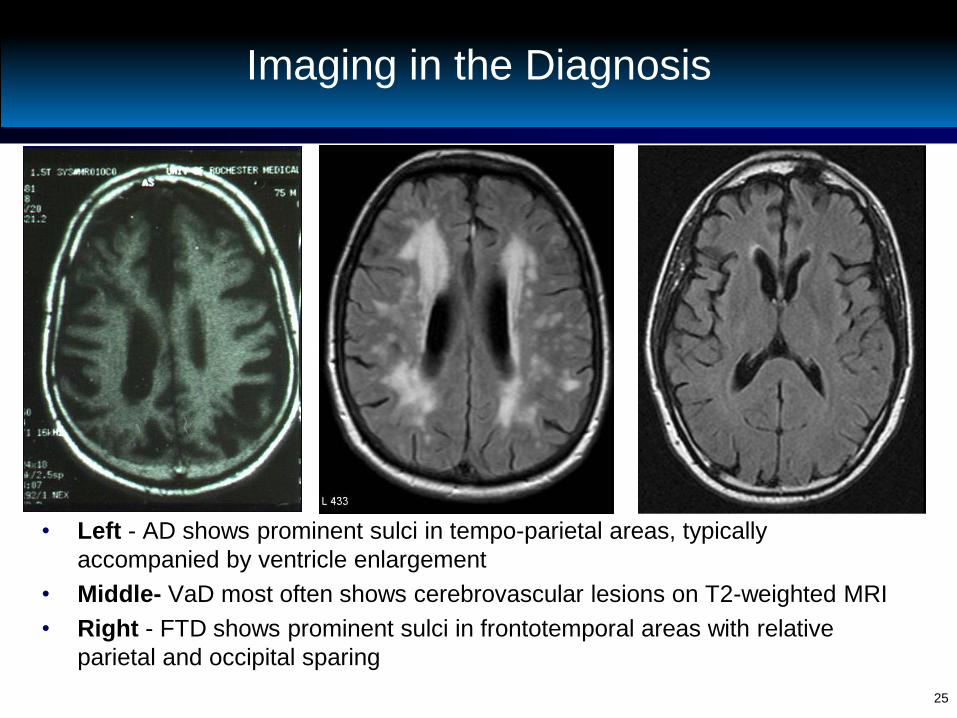
Imaging in the Diagnosis
• Left - AD shows prominent sulci in tempo-parietal areas, typically
accompanied by ventricle enlargement
• Middle- VaD most often shows cerebrovascular lesions on T2-weighted MRI
• Right - FTD shows prominent sulci in frontotemporal areas with relative
parietal and occipital sparing
26
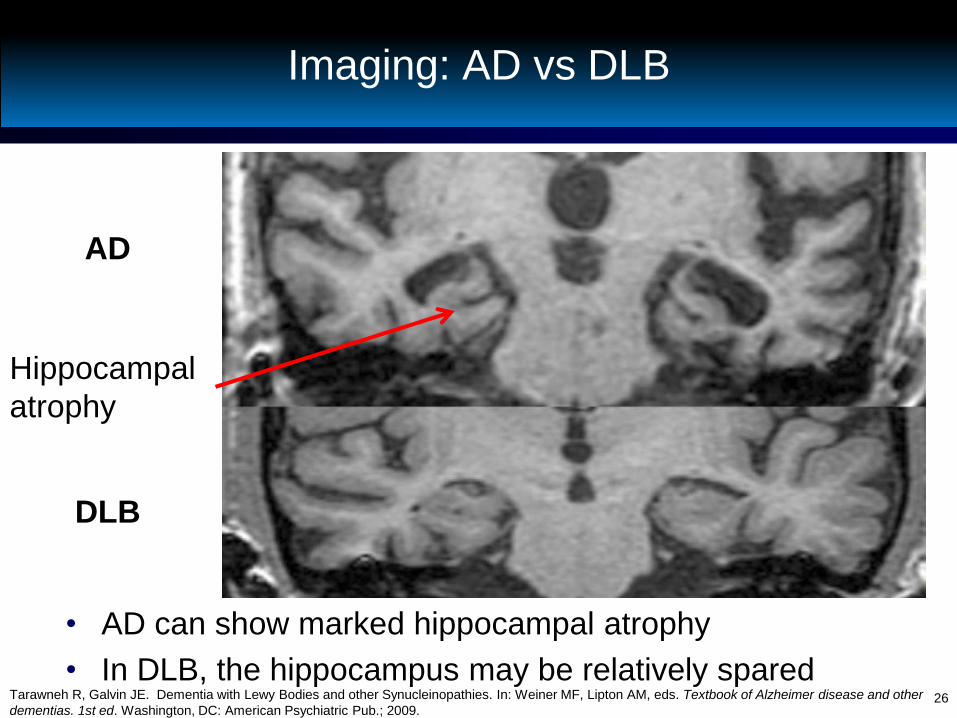
Imaging: AD vs DLB
• AD can show marked hippocampal atrophy
• In DLB, the hippocampus may be relatively spared
Hippocampal
atrophy
AD
DLB
Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. In: Weiner MF, Lipton AM, eds. Textbook of Alzheimer disease and other
dementias. 1st ed. Washington, DC: American Psychiatric Pub.; 2009.

27
Neuropsychiatric Symptoms in Dementias
NPI Item AD PDD DLB VaD FTD
Delusions ● ● ●● ● -
Hallucinations - ●●● ●● ● -
Agitation ●● ●● ●●● ●●● ●●●
Depression ●● ●●● ●●● ●● ●●●
Anxiety ●● ●●● ●●● ●● ●
Apathy ●●● ●●● ●●●● ●●● ●●●●
Disinhibition - - ● ● ●●●●
Irritability ●● ● ●●● ●● ●●●
Sleep ● ● ●●● ●● ●●
- 0-14% ● 15-29% ●● 30-44% ●●● 45-59% ●●●●
≥ 60%

28
Pathologic Profiles of Dementias
Pathologic Signs AD PDD DLB VaD bvFTD
Neuritic plaques ●●● ● ●● - -
NFTs ●●● ● ●● - -
Cortical Lewy bodies ● ● ●● - -
Subcortical Lewy bodies ● ●●● ●●● - -
Ischemic damage ●● - - ●●● -
Tau or TDP-43 inclusions - - - - ●●●
Biochemical Deficit AD PDD DLB VD FTD
Cholinergic ●●● ●●●● ●●● -/● -
Dopaminergic ● ●●● ●●● - -
- Generally absent ● Infrequent ●● Typical ●●● Hallmark Feature ●●●● Severe Deficit 1. Stahl SM. Stahl's essential psychopharmacology: neuroscientific basis and practical applications. 3rd ed, Fully rev. and expanded. ed. Cambridge ; New York: Cambridge
University Press; 2008. 2. Geldmacher D. Alzheimer’s Disease. Textbook of Alzheimer disease and other dementias. 1st ed. Weiner MF, Lipton AM, eds. Washington, DC:
American Psychiatric Pub.; 2009. 3. Tarawneh R, Galvin JE. Dementia with Lewy Bodies and other Synucleinopathies. Textbook of Alzheimer disease and other dementias. 1st
ed. Weiner MF, Lipton AM, eds. Washington, DC: American Psychiatric Pub.; 2009. 4. Bird TD, Miller BL. Alzheimer’s disease and other dementias. Harrison’s Principles of
Internal Medicine. 16th ed. Kasper DL, Braunwald E, Fauci, AS, et al., eds. New York, NY: McGraw-Hill; 2005. 5. Szoeke CE, Campbell S, Chiu E et al, Vascular Cognitive
Disorder. Textbook of Alzheimer disease and other dementias. 1st ed. Weiner MF, Lipton AM, eds. Washington, DC: American Psychiatric Pub.; 2009. 6. Rascovsky K, Hodges
JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. Sep 2011;134(Pt 9):2456-2477. 7. Bohnen NI, Kaufer
DI, Ivanco LS, et al. Cortical cholinergic function is more severely affected in Parkinsonian dementia than in Alzheimer disease: an in vivo positron emission tomographic study.
Arch Neurol. 2003;60:1745-1748.

29
Current FDA-Approved Therapies
1. Fortinash KM, Holoday-Worret PA. Psychiatric Mental Health Nursing. 3rd ed. St. Louis, MO: Mosby; 2004. 2. Boyd M Psychiatric Nursing: Contemporary
Practice. 4th ed. Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008. 3. Reisberg B et al. N Engl J Med. 2003;348(14):1333-1341.
AD PDD
Number of Acetylcholinesterase Inhibitors1 4 1
Number of NMDA Antagonists1 1 0
• AD symptoms correlate with disruption of cholinergic circuits2
• PDD is characterized by a larger cholinergic deficit than AD3
• There are no FDA-approved medications of any class to treat
DLB, VaD, or FTD

30
The Importance of Making an Early
Diagnosis
• Identify and treat reversible causes
• Help explain presence of troublesome behaviors
• Allow the patient to make critical life decisions
• Identify and treat psychiatric symptoms
• Maximize patient safety
• To provide treatment
• Allow caregiver early access to support and
community resources
Agronin ME. Alzheimer disease and other dementias : a practical guide. 2nd ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.
31
Caregiver Challenges in Different Types of Dementias
• AD – typically older onset, with frequent co-
morbidities
• PDD – prominent motor symptoms leading to
falls
• DLB – frequent and sometimes severe
neuropsychiatric symptoms
• VaD – depression and continuing risk factors for
stroke
• FTD - younger onset, predominant behavioral
and language symptoms

32
Summary
• Diagnosis of dementia begins with recognizing
cognitive impairment (CI) in the patient
– Cognitive assessment tools can be valuable
• Reversible causes of CI should be ruled out via
the dementia workup
– Delirium must be ruled out, or if present, treated
accordingly
• Key clinical features of each dementia can aid
the clinician in arriving at the specific diagnosis
• Making the specific diagnosis early is critical for
the patient and caregiver