Embed Size (px)
Citation preview
Differential Diagnosis
Gastrointestinal Disorders
Gastrointestinal Disorders
Can refer pain to the sternal region, shoulder, scapula, neck, mid back, low back, hip, pelvis and sacrum
Pain may mimic musculoskeletal lesions If due to GI disorder, pain is usually
accompanied by other systemic signs and symptoms
Intraabdominal diseases involving ulceration or infection of the mucosal lining most commonly refer pain to the musculoskeletal system
GI related symptoms
Abdominal pain Dysphagia Odynophagia Melena Epigastric pain with
radiation to the back Symptoms affected by
food Early satiety with weight
loss
Constipation Diarrhea Fecal incontinence Arthralgia Referred shoulder pain Psoas abscess Tenderness over
McBurney’s point
Gastrointestinal disorders
Abdominal (Visceral) pain Occurs in the midline – abdominal organs
receive sensory afferents from both sides of the spinal cord
Site of pain corresponds to the dermatome from which the diseased organ receives its innervation
Pain is not well localized Visceral pain fibers are sensitive only to
stretch or tension
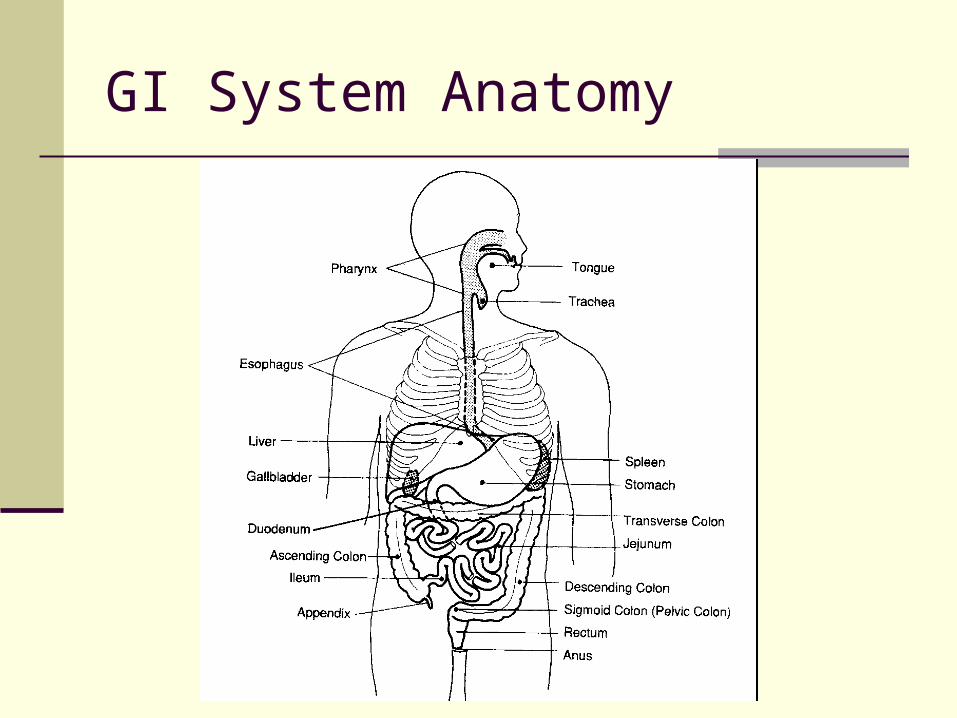
GI System Anatomy
GI disorders – Referred pain
Liver, diaphragm and pericardium (C3-C5) – refer pain to the shoulder
Gallbladder, stomach, pancreas and small intestines (T6-T9) – refer pain to the midback and scapula
Colon, appendix and pelvic viscera (T10-T11) Sigmoid colon, rectum, ureters and testes
(T11-L1, S2-S4) – refer pain to the pelvis, flank, low back or sacrum
GI disorders – Referred pain
Referred distribution area may develop: Hyperesthesia – Excessive sensibility to
sensory stimuli Hyperalgesia – Excessive sensibility to painful
stimuli Referred pain may occur alone If accompanied by visceral pain, the visceral
pain usually develops first The client usually does not connect the two
sets of symptoms
Arthralgia due to GI disorders
Asymmetric, migratory and usually only affects one or two joints at a time
Accompanied by fever, malaise, skin rash or lesions, nail bed changes, iritis or conjunctivitis
Joint pain and accompanying symptoms may not occur simultaneously. Usually accompanying symptoms occur 1-3 weeks prior to the onset of joint pain
Peripheral joints (knees > ankles > shoulders > wrists > hands and feet) are most commonly affected
Arthralgia due to GI disorders
Knee Effusion is common Muscle atrophy occurs with chronic condition Stiffness, pain, tenderness and decreased
ROM No permanent deformity persists when GI
disorder is properly treated
Arthralgia due to GI disorders
Spondylitis with sacroilitis LBP and morning stiffness Improves with activity Radiographic findings consistent with
ankylosing spondylitis with bilateral SI joint involvement
“Bamboo spine” will result if untreated
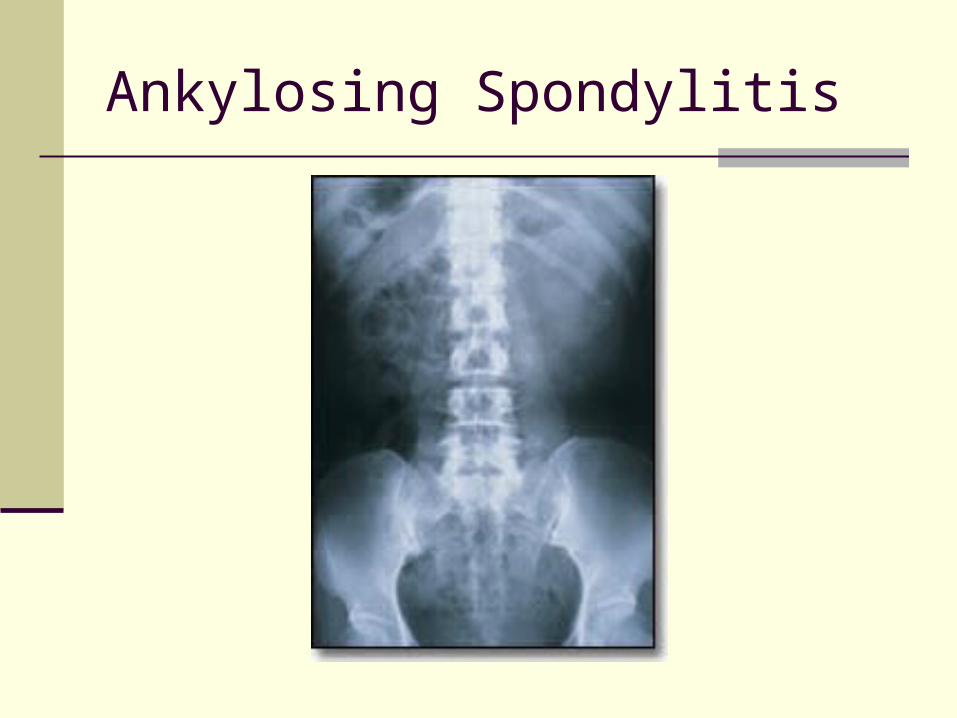
Ankylosing Spondylitis
Arthralgia due to GI disorders
Enthesitis (Inflammation involving the bony insertion of tendons and ligaments) Heel pain - Swelling and tenderness at the
Achilles tendon insertion or the calcaneal attachment of the plantar fascia
Can also occur at the knee, ischial tuberosities, greater trochanter, costovertebral and manubriosternal joints
Kehr’s sign
Pain in the left shoulder due to free air or blood in the abdominal cavity
May occur after a ruptured spleen Patient may or may not recall precipitating
trauma such as a sharp blow during an athletic event, a fall or MVA
Patient may not connect the traumatic event to complaints of shoulder pain
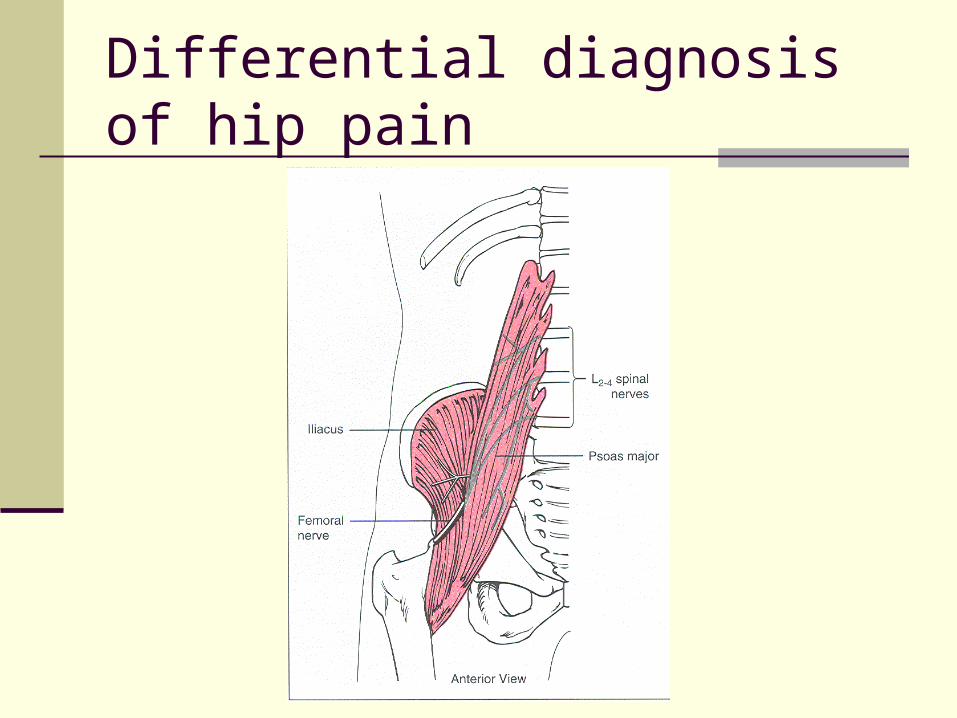
Psoas Abscess
Usually due to spread of inflammation or infection from an adjacent structure
Osteomyelitis of the ilium or septic arthritis of the SI joint can penetrate the muscle sheath of the iliacus or the psoas muscle producing an abscess
Symptoms include fever, night sweats, lower abdominal or back pain, referred pain to the hip, medial thigh, groin or knee
May develop antalgic gait pattern
Differential diagnosis of hip pain
Heel tap Gently tap the heel of the involved leg or have
the patient hop on the involved leg If the patient has peritoneal inflammation, they
will have a painful expression and complaint of right lower quadrant pain with testing, or they will be unable to tolerate or complete the test due to pain
If pain is musculoskeletal in origin, tapping the heel will not reproduce pain
Differential diagnosis of hip pain
Iliopsoas muscle test Perforated appendix or inflammed peritoneum can
press on and irritate the iliopsoas muscle Have the patient perform an active SLR in supine
position. Therapist applies resistance at the distal thigh.
Alternatively, have the patient lie on the unaffected side. Passively extend the affected leg at the hip.
If either of the above tests produces increased right abdominal, flank or pelvic pain it is suggestive of an inflamed appendix or peritoneum
Pain and/or tenderness in the left lower abdomen may be caused by bowel perforation associated with diverticulitis.
Differential diagnosis of hip pain
Differential diagnosis of hip pain
Palpate the iliopsoas muscle In supine, fully support the patient’s legs in
90/90. Locate and palpate the iliopsoas muscle one third of the distance between the ASIS and the umbilicus
If the patient c/o LBP with palpation, this is indicative of a tight or contracted iliopsoas
If palpation refers pain into the right lower quadrant, this is indicative of peritoneal inflammation or iliopsoas abscess
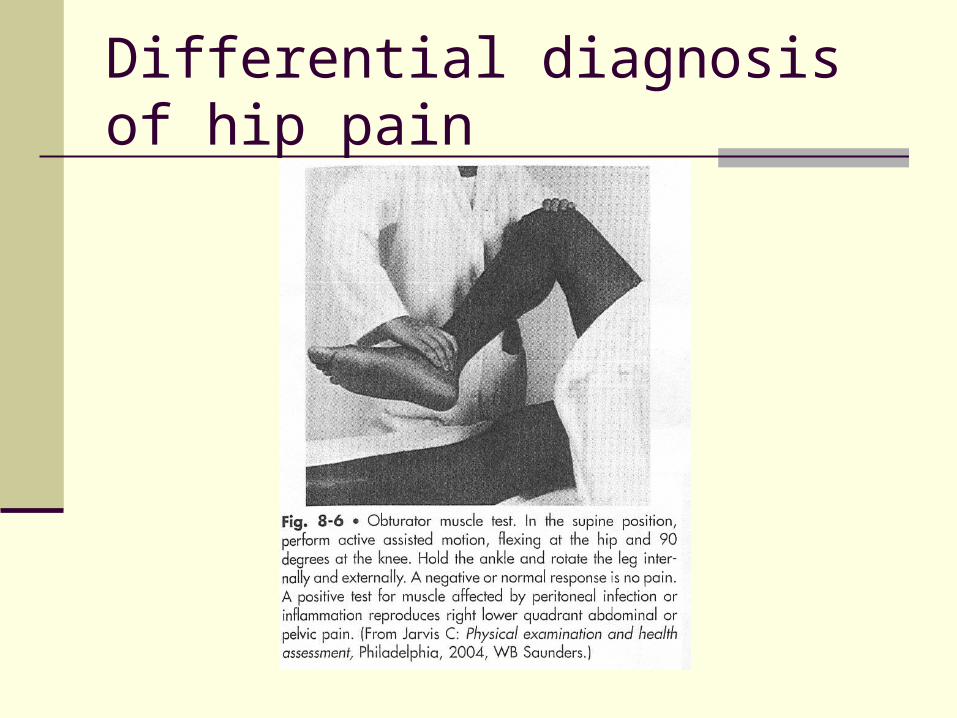
Differential diagnosis of hip pain
Obturator muscle test In supine position have the patient active
assistively flex the hip and knee to 90/90 The therapist them performs passive hip
internal and external rotation If normal, this motion should not be painful If pain is reproduced in the right lower
abdomen or the pelvic region, it is indicative of peritoneal infection or inflammation
Differential diagnosis of hip pain
Ulcers
Pain is described as burning, gnawing, cramping or aching
Pain comes in waves that last several minutes (not hours)
Pain may radiate below the costal margins into the back, and rarely into the shoulder
Pain pattern is directly related to the secretion of digestive enzymes and the presence or absence of food
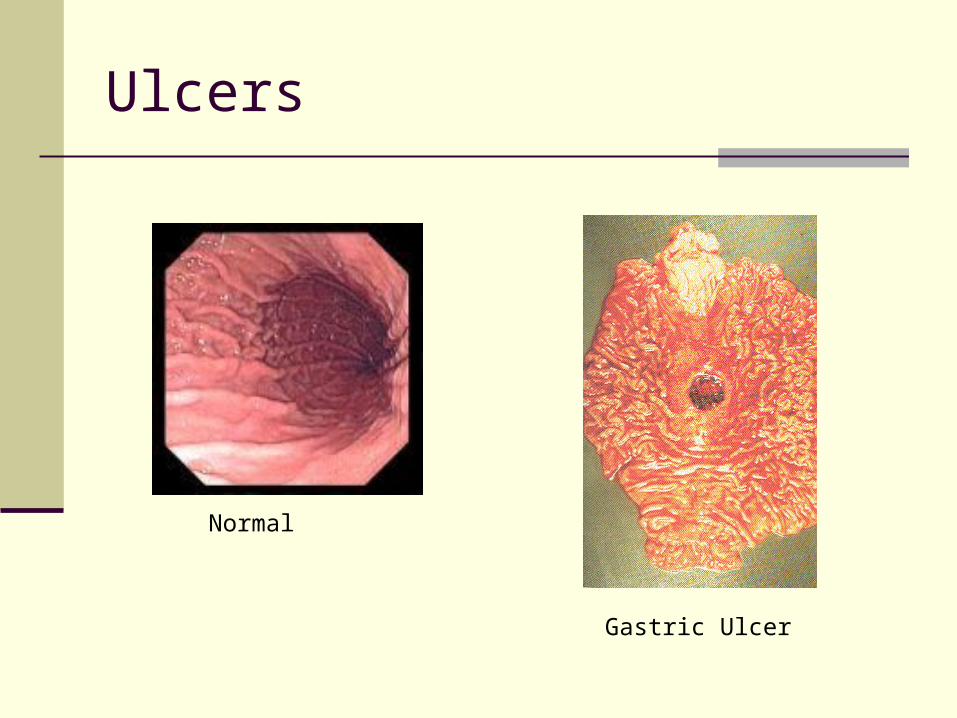
Ulcers
Normal
Gastric Ulcer
Diverticulitis
Symptom of left lower abdominal pain or tenderness
Screen for with iliopsoas and obturator tests Confirmed by accompanying fever, bloody
stools, and elevated WBC count
Appendicitis
Classic symptoms of right lower abdominal pain, nausea and vomiting
May be accompanied by high fever, coated tongue and bad breath
Pain may be referred to the thigh or right testicle
Pain comes in waves and is aggravated by movement
Patients often assume a flexed posture to relieve abdominal muscle tension
Appendicitis
Important to check for in the elderly population with c/o hip or thigh pain
May not present with classic sign of peritonitis due to lack of abdominal muscle tone
Specific tests should include iliopsoas, obturator abscess and McBurney’s point
McBurney’s point
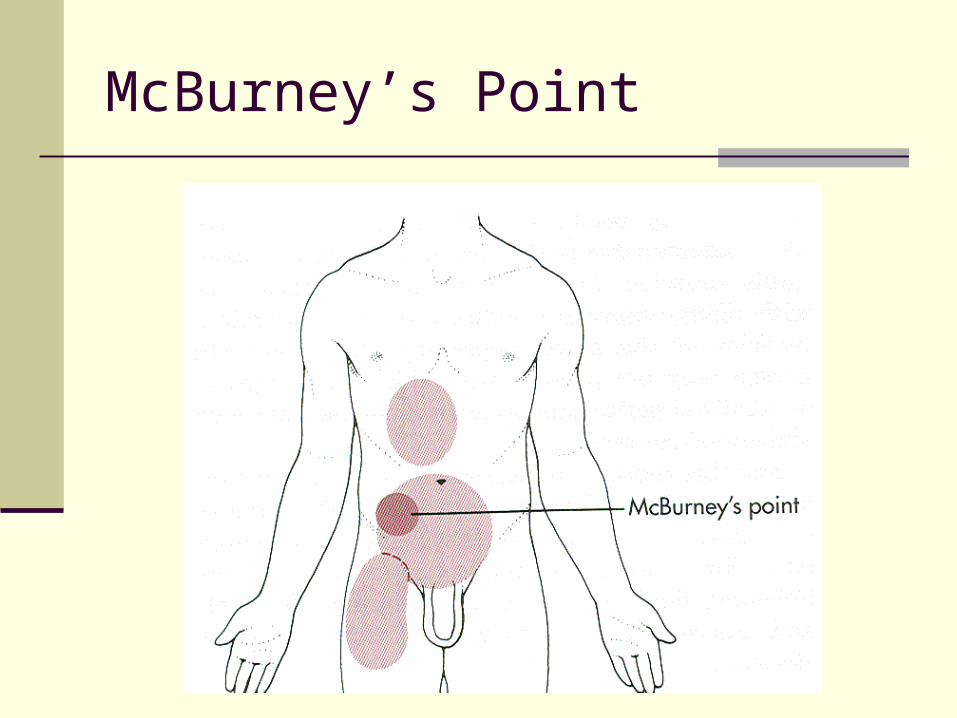
Location of parietal pain caused by inflammation of the peritoneum in acute appendicitis or peritonitis
Locate by palpation with patient in supine McBurney’s point is located half way between
the ASIS and the umbilicus Reproduction of pain with palpation is
indicative of appendicitis
McBurney’s Point
Rebound tenderness
Used to test for hip, pelvic or flank pain from peritonitis
While palpating McBurney’s point, press the fingers in firmly and slowly
Then quickly withdraw the fingers Pain induced or increased by quick
withdrawal indicates inflamed peritoneum
Acute Pancreatitis
Inflammation of the pancreas that may result in autodigestion of the pancreas by its own enzymes
Symptoms of abrupt abdominal pain in midepigastrium
Pain is described as penetrating and may radiate into the back
Pain increases in intensity over several hours and can last several days
Acute Pancreatitis
Pain is worse with walking or lying supine Pain is relieved with sitting or leaning forward Associated symptoms include nausea,
vomiting, fever, sweating, tachycardia, malaise, weakness and jaundice
Patients with chronic pancreatitis may have epigastric and left upper quadrant pain with referred pain into the upper left lumbar region
Pancreatic Cancer
Initial symptoms are usually vague and nonspecific
Most common symptoms are anorexia and weight loss, upper abdominal pain with radiation into the back, and jaundice
May have constipation, nausea, vomiting and weakness
LBP is a common symptom and may be the first or only symptom
Sitting up and leaning forward may provide some relief – indicates the tumor has spread beyond the pancreas and is inoperable
GI Complications with NSAIDs
Voltaren Lodine Indocin Relafen Anaprox Naprosyn Toradol
Aspirin Excedrin Bufferin Advil Motrin Ibuprofen Aleve
Common Nonsteroidal Anti-inflammatory Drugs
GI Complications with NSAIDs
NSAIDs have become increasingly popular because of their analgesic, antiinflammatory, antipyretic and antithrombotic actions
They have deleterious effects on the entire GI tract
Most obvious clinical effect is on the gastroduodenal mucosa
NSAID induced GI bleeding is a major cause of morbidity and mortality among the elderly
GI Complications with NSAIDs
GI complications include ulcerations, hemorrhage, perforation, stricture formation, and exacerbation of inflammatory bowel disease
Other complications Suppression of cartilage repair and synthesis Fluid retention Kidney damage Liver damage Skin reactions Nervous system impairments (headaches, depression,
confusion, memory loss, mood changes, and ringing in the ears)
References “Ankylosing Spondylitis”. Retrieved 6/22/08 from the World Wide
Web. http://www.spondylitis.org/about/as.aspx Goodman CC, Snyder TE. 2007. Screening for Gastointestinal
Disease. In: Differential Diagnosis for Physical Therapists Screening for Referral. 4th edition. St. Louis, MO: Saunders Elsevier. p366-408.
Koopmeiners MB. 1995. Screening for Gastrointestinal System Disease. In: Boissonnault editor: Examination in Physical Therapy Practice Screening for Medical Disease. 2nd edition. Philadelphia, PA: Churchill Livingstone, p102.
Reese NB. 2005. Muscle and Sensory Testing. 2nd edition. St. Louis, MO. Saunders Elsevier.p253.
Rubin E, Farber JL. 1999. Pathology. 3rd edition. Philadelphia, PA: Lippincott Williams & Wilkins p693. In: Porth editor: Pathophysiology Concepts of Altered Health States, 6th edition. Philadelphia, PA: Lippincott Williams & Wilkins, p839.