Embed Size (px)
Citation preview

Different types of trial Different types of trial designdesign
and implications for reportingand implications for reportingAlison WeardenAlison Wearden

Uncontrolled trialsUncontrolled trials
• Test feasibility and acceptability of an intervention, and whether there are adverse effects
• May allow preliminary examination of mechanisms of change
• N-of-1 designs, randomized schedule, can be used to test theory (cause and effect)

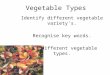
Types of BIAS Methods of bias controlSelection bias Randomized treatment assignment
Concealment of assignmentBias in studymanagement
Standardized operating proceduresTraining of research personnel
Ascertainment bias Blinding of researchers to treatment assignment
Bias introduced after randomization
Intention-to-treat analysis
Publication bias Prospective registration of trialsPublication of negative trials
From D. Wang & A Bakhai (Eds) Clinical Trials. A Practical Guide to Design, Analysis and Reporting. 2006, Remedica: London, pp 57

The hegemony of pharmacological The hegemony of pharmacological trialstrials
• Blinded randomised controlled trials considered gold standard for testing drugs
• Heavily influenced guidelines for RCTs• Are drug-RCT issues always appropriate
for complex behavioural interventions?• Can attempts to eliminate bias distort
implementation and assessment of intervention?

EfficacyExplanatory
Types of CONTROLLED TRIALS
What factors do you need to take into account choosing a trial type and design?
What is your research question?
Are there ethical constraints?
Where might you want to publish your trial?
Parallel arms/factorial?
EquivalenceNon-inferiority
EffectivenessPragmatic
Patientpreference

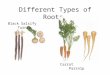
ExplanatoryExplanatory vsvs pragmatic pragmaticEfficacyEfficacy vsvs effectiveness effectiveness
Pragmatic, effectiveness
What would be the outcome if this intervention were implemented in usual clinical practice?
Explanatory, efficacy
Does this intervention work in people who receive it under carefully controlled conditions? How does it work?
•Tightly defined sample•Fixed protocol•Compliance measured•Process measures
•Broad, inclusive sample•More flexible implementation•Qualitative studies, e.g. to determine why people dropped out
See Zwarenstein et al., 2008, BMJ, 337, 1223-6

Intention to treat analysisIntention to treat analysis
• Preserves the benefits of randomization, ie minimizes bias. Withdrawals may be more common in one arm of trial
• Ecological validity (people do drop out)• It gives a pragmatic estimate of the
effectiveness of a treatment, rather than just a report of the efficacy of the treatment
• It requires a method for dealing with missing data

Equivalence trialsEquivalence trials
• Instead of having a “no treatment” control, equivalence trials test whether a new intervention is as good as (or not worse than) an established treatment with proven efficacy
• New intervention may have some advantage (convenience, cost) over established, but is it at least as efficacious?

Randomisation issuesRandomisation issues• Unit of randomisation (individual, group)• Simple or block design (to even up group
numbers)• Stratification or minimisation to achieve groups
balanced on key baseline characteristics• Patient preference designs
– Zelen– Wennberg
• Rucker– Comprehensive cohort

Preference designsPreference designs
• Patient preference may be an issue– refusal to participate– reduced compliance with non-preferred arm
• Consent may be taken AFTER randomization, e.g. Zelen design:
Eligiblepatients Randomized
NovelTreatment B
ConsentsReceives B
DeclinesReceives A
StandardTreatment A
(May be analysed asrandomized)

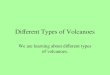
Some trial designsSome trial designs
Simple, parallel designIs A better than control?
Factorial designAre effects of A and B additive or interactive? A & B each controlled
Cross-over design(Unlikely – useful with
small samples)
EligibleRandomised to
A or control
A
control
Randomized to 1,2,3 or 4
A Controlfor A
B 1 = A+B
2 = B + control
Control for B
3 = A + control
4 = Doublecontrol
EligibleRandomised toA THEN B or
B THEN A A
B
B
A

Analysis issuesAnalysis issues
• Pre-specification of primary outcomes if there are multiple measures
• Analysis plan pre-specified and published• Intention to treat vs per protocol analysis• How are missing data dealt with?

Where do you want to publish?Where do you want to publish?
• Which audience do you want to reach?• Does impact factor matter?• Uniform requirements for “prestigious”
medical journals– Trial must be registered– Protocol must be published– CONSORT guidelines must be adhered to
• Important issue of publication bias

Special considerations for reporting Special considerations for reporting different types of trialsdifferent types of trials
• Standard CONSORT guidance is at
http://www.consort-statement.org/consort-statement/– designated primary outcomes– sequence generation– allocation concealment ….
• CONSORT guidelines have been elaborated for trials with complex interventions (cf. drug trials) and non-simple designs

Reporting of psychological trials Reporting of psychological trials should includeshould include
• Components of the intervention(s), how they were individualised (if applicable), how they were standardized
• How therapist fidelity to treatment assessed• How experimental intervention and
comparator(s) were implemented• Description of therapists (specialism,
experience etc) and setting
Boutron et al., 2008, Ann Int Med, 148, 295-309

Reporting pragmatic trialsReporting pragmatic trials
• Explanatory vs pragmatic “attitude”• Sample description and eligibility criteria –
is sample typical? Is setting typical?• CONSORT diagram should explain
reasons for non-participation if known• Particular attention to clinical interest of
findings• Description of key aspects of setting which
affected findings
Zwarenstein et al., 2008, BMJ, 337, 1223-6

Issues with equivalence, or non-Issues with equivalence, or non-inferiority, trialsinferiority, trials
• People may be carrying out equivalence trials without realising it.
• Analysis with respect to a pre-stated margin of non-inferiority (smallest clinically interesting difference)
• ITT analysis may increase risk of type 1 error
• Choice of outcomes important
Piaggio et al., 2006, JAMA,295,1152-1160

Reporting equivalence trialsReporting equivalence trials
• Need to reference established efficacy of “standard” treatment
• Hypotheses should be framed in terms of non-inferiority
• “Margins of equivalence” should be reported