Embed Size (px)
Citation preview

InspyredThe alternative EAO voice
Volume 5, Issue 2 / Winter 2017
Different approaches for root coverage
Minimally invasive extraction with the
Benex system
Highlights from Madrid 2017
Let's rethinkdental ergonomics
Wiki-implants:Defusing an
'infl ammatory bomb'

27th
annualscientificmeetingof theeuropeanassociationfor osseointegration
EAO-congress.com
VIENNAFrom October 11th
To October 13th, 2018Invited region:Russia and BaLtic countries
Dreams & Realityin implant dentistry
in cooperation with:
C
M
J
CM
MJ
CJ
CMJ
N
18EAO_adv210x297-HD.pdf 1 16/11/2017 16:01

03 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
W elcome to the latest issue of Inspyred. We are pleased to report that our winter 2017 edition is at full capacity, and packed with
more clinical cases and innovative techniques than previous issues. To make room for all of this content in the printed version we have abridged a number of articles. So in order to get the most out of this issue, make sure you visit the Inspyred web-page to access the full versions of each article and the complete sets of fi gures and references.
Th e clinical articles in this edition cover a range of topics and describe cutting-edge technologies and techniques. In the fi rst, Julia Hehn looks at diff erent approaches for root coverage and treats gingival recessions using an interesting split-mouth design. Th e second article, by Benjamin Cortasse, looks at immediate dentoalveolar restoration and off ers a compelling new perspective for immediate placement.
On page 27 you'll fi nd a challenging clinical case submitted by Sophie Dacquin which was treated with an implant-supported part-arch bridge. Th is is followed by a case report from Katarzyna Gurzawska involving a patient at risk of medication-related osteonecrosis of the jaw (MRONJ), and minimally invasive extraction. Th e fi nal clinical article is by Peter Lindkvist and involves the use of customised allogeneic bone-blocks.
Don't miss our latest wiki-implant case on page 6, where Victor Palarie and Husein Isawi
describe an 'infl ammatory bomb' caused by implants which had been placed in infected sites. Wiki-implant articles describe the cases which don’t go to plan, so you can read about complications which have been encountered in real-life situations and how they were managed.
Also not to be missed in this issue is David Blanc's fascinating article on dental ergonomics. Find it on page 4 to get invaluable advice for setting up a workstation that works for you, and how to avoid musculoskeletal disorders.
We are also delighted to include an exclusive interview with Dr Tidu Mankoo, respected international lecturer and clinician. We asked Dr Mankoo about what is involved in treating complex cases, and you can hear his tips for optimising your daily practice and staying abreast of current literature on page 32.
Th is issue also includes highlights from this year's annual scientifi c meeting which took place in Madrid in October. See pictures, catch up on the latest association news, and fi nd out about the social and scientifi c highlights from the EAO's 26th annual meeting.
As ever, we look forward to hearing your feedback and suggestions for this and future editions. Please do not hesitate to get in touch by emailing us at [email protected].
Isabella Rocchietta and David Nisand
Editors welcomeThis winter, Inspyred unwraps new techniques and technologies
Share your clinical case and get published!Visit eao.org/inspyred for more information
To get the most out of Inspyred, visit our website, where you can view all articles in full, along with additional content.
www.eao.org/inspyred
Editorial CommitteeDavid Nisand, France (Editor)Isabella Rocchietta, UK (Editor)Martin Brient, FranceStefan Fickl, GermanyJaime Jiménez Garcia, SpainAilsa Nicol, UKIrena Sailer, SwitzerlandAlberto Sicilia, SpainTommie Van de Velde, Belgium

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 04
Let’s rethink dental ergonomicsHow to set up a workstation that works for you
S cientific literature shows that musculoskeletal disorders (MSD) are a major problem for dental health workers. A systematic review of MSD among dental
professionals by Hayes et al. in 2009 suggested that the prevalence of general musculoskeletal pain ranges between 64% and 93%. Pain is reported mainly in the back, neck and shoulder.
These statistics are much higher than for many other healthcare professionals. Rambabu et al. showed in 2014 that musculoskeletal pain was most prevalent among dentists (61%), followed by surgeons (37%) and physicians (20%).
We must therefore look at our workstations with new eyes and new tools. A variety of techniques are available to assess the health of skeletal muscles, and combined with a sound knowledge of anatomy and biomechanics are essential tools to help us enter into evidence-based ergonomics. Blanc et al. in 2013 showed that there is a high degree of variability depending on the workstation, and that clinicians can adapt their position accordingly to drastically reduce physical strain.
The origin of this line of research can be traced back to the work carried out by Dr Daryl Beach in the 1950s. He determined a new concept in ergonomics for dental care workers – his theory of proprioception. This theory can now be explained and expanded upon by biomechanics.
The problem is finding a position which works for the practitioner as well as the patient. Because our position is mainly or fully determined by the patient’s position. The patient’s position, which affects the dentist’s spine, should be considered separately from how we handle instruments, which affects our shoulders.
The patient’s position
We usually ask the patient to sit in our dental chair, and tilt the backrest until they tell us to stop. However, it is becoming increasingly standard practice to set the patient in a fully lying position to
allow for ergonomic access to their oral cavity. This position is commonly used by physiotherapists and massage therapists, and is also used for sleeping. So why is it so difficult to achieve in a dental chair? Based on human biomechanics, we can identify three reasons:
1. The backrest is often not aligned with the seat. This creates a painful lumbar lordosis and spine curvature.
2. Knees are bent. While this makes the chair more comfortable in a seated position, it also increases lumbar lordosis in a lying position (Figure 1).
3. When the chair is tilted backwards, there is no indication of when it will stop. This can be especially uncomfortable for elderly patients, who have a lower threshold for proprioception.
There are a few measures we can take to help with this. When your backrest is set horizontally, ensure the entire surface, from headrest to footrest completely flat. You can then ask your patient to lie down on the unit and put their head on the headrest. Don’t worry about whether they will miss the headrest; when someone lies on their bed, they don’t miss the pillow. Once the patient is lying down, you can place a cylindrical cushion under their knees to reduce lumbar lordosis (Figure 2).
Furthermore, if the unit is flat it will fit any patient size, and you won’t be dependent on the shape of the dental seat. The patient’s mouth is the reference point (Figure 3). When a patient is sitting in a dental chair, their ischial point is always at the same place, but their mouth is not. This requires continuous adjustment and adaptation. Surgery has been performed on a flat operating table for many years; there is no reason why oral surgery cannot be performed in a similar manner.
In fact, there may be an argument for replacing our dental chairs with operating tables. The dental unit was originally created based on the design of a
David Blanc, DDS, PT, DO, graduated in 1999 with a degree in physical therapy. In 2001 he received a degree in ergonomics and in 2009 he received a degree in osteopathy. After practising physical therapy for ten years, he returned to medical school and graduated from the University of Toulouse.
Since 2013 he has worked in private practice. He provides consultation and lectures on dental ergonomics; he also researches and has published several articles in the field. His areas of interest include implant dentistry, orthodontics, and aesthetics.
w: www.ergonomie-dentaire.com/en
Figure 1: When knees are bent in a fully lying position, the rectus femoris muscle is stretched. This increases lumbar lordosis and may lead to discomfort.
Figure 2: A cylindrical pillow placed under the knees will fit the patient’s anatomy perfectly and reduce lumbar lordosis.
Rectus femoris stretched

05 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
barber’s chair. It is clear, however, that today many dental procedures are much more akin to operations than haircuts.
Location of instruments
Th e use of instruments is governed by upper-limb movement. When referring to instruments, we should not only distinguish between the ‘chair-side cart’ and the ‘over the patient tray’. We should categorise them based on their location in relation to our articular physiology, and how easy it is to reach them. Th is is where an understanding of basic anatomy and the average range of motion is essential.
Extreme movements and high muscular strain due to the lever eff ect cause MSD. So it’s important to recognise these movements and avoid them.
Th e full range of a joint can be divided into three areas: internal, intermediate and external (Figure 4). Th e intermediate range is the only one which can be maintained comfortably, especially for postures which are adopted for long periods of time. Average human articular ranges are listed since decades, so it’s very easy to isolate the intermediate range for each movement, and establish which posture is suitable for each individual.
For instance, in the shoulder the maximum range of the scapulohumeral joint is 50° extension and 90° fl exion (Kapandji. 2007). Th e intermediate range is 5° extension and 45° fl exion. Th is indicates the area where our hand is able to reach comfortably, and therefore where our instruments should be. As a rule in ergonomics, the machine should be adapted to the user, not the other way round. Having instruments out of reach is not an option.
If we consider the position of the instrument tray which comes over the patient, it is clear that it brings the hand much too high in respect to the shoulder. Th e tray may seem useful, but if it causes shoulder pain it is not an ideal solution. Instead, we could consider using a side tray, and asking the assistant to hand us more instruments.
Th ere are two ranges of movement in the elbow: fl exion/extension, and pronation/supination. Biomechanically, however, elbow movements are oft en a combination of these two. Th ere are two physiological associations: the ‘strength elbow’, which combines fl exion supination and extension pronation when we need power, and the ‘fi nesse elbow’ which combines fl exion pronation and extension supination when precision is required (Werner et al. 1994; Galloway et al. 2002). An example of the latter is taking a pencil from a chest pocket and handing it to someone.
‘Finesse elbow’ (fl exion pronation) is most oft en required in our line of work. So when we need to place instruments back on the tray, it should be done with this physiological movement. Th e rotary instrument
Figure 4: Articular range of motion in the elbow. The intermediate range is within the comfort range.
Figure 3: When a patient is set on a fl at support, their head is always in the same place, whatever their size.
holder should be in an appropriate position to facilitate this, where our hand goes naturally. We shouldn’t bring our hand to the instrument; the instrument should come to our hand.
Five steps to make sure your workstation is ergonomically optimal:
sit comfortably on your stool without a patient bring your hands to your minimum fi eld of view ensure the dental chair is fully horizontal ask your patient to lie down and lift the chair to this height practise the ‘fi nesse elbow’ movement to see where your hand goes naturally, and bring the tray to this position
Now, you are ready to work! Once your dental chair has been adjusted correctly, you will never have to change its settings; they are suitable for all patients, whatever their size. Th eir head will always be at the same location on the headrest. Th e centre of your workstation is their mouth, so this should be the point around which everything revolves.
Th ese rules can be applied to all of our joints and all parts of our body, to obtain a fully comfortable, MSD free, pain-free, and more effi cient daily practice.
References
Blanc D, Farre P, Hamel O. Variability of musculoskeletal strain on dentists: an electromyographic and goniometric study. Int J Occup Saf Ergon. 2014;20(2):295–307.
Galloway JC, Koshland GF. General coordination of shoulder elbow and wrist dynamics during multijoint arm movements. Exp Brain Res. 2002 Jan;142(2):163–80. Epub 2001 Dec 6.
Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009 Aug;7(3):159–65. doi: 10.1111/j.1601–5037.2009.00395.x.
Kapandji IA. Articular Physiology. Tome 3. Spine, Maloine, Paris, 2007. pp114.
Rambabu T, Suneetha K. Prevalence of work related musculoskeletal disorders among physicians, surgeons and dentists: a comparative study. Ann Med Health Sci Res. 2014 Jul;4(4):578–82. doi: 10.4103/2141-9248.139327.
Werner FW, An KN. Biomechanics of the elbow and forearm. Hand Clin. 1994,10(3):357–373.
Internal range
Intermediate range
External range
Ischial point
Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 06
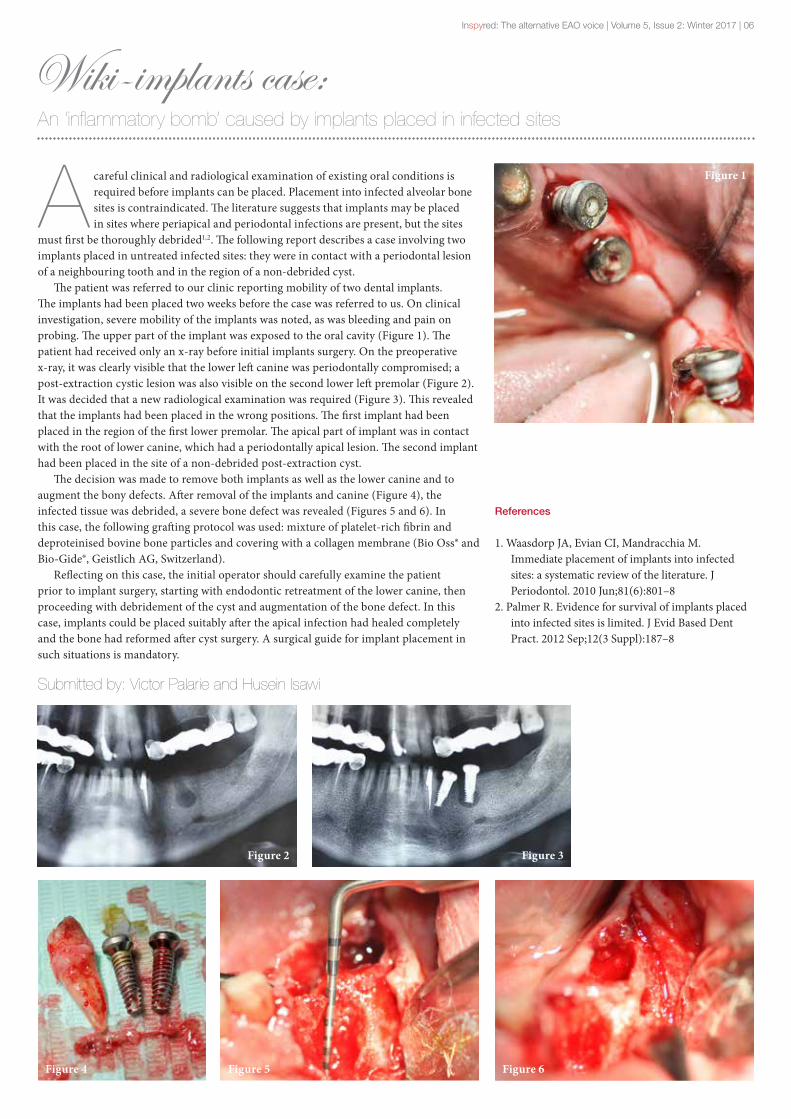
Wiki-implants case:An ‘inflammatory bomb’ caused by implants placed in infected sites
A careful clinical and radiological examination of existing oral conditions is required before implants can be placed. Placement into infected alveolar bone sites is contraindicated. The literature suggests that implants may be placed in sites where periapical and periodontal infections are present, but the sites
must first be thoroughly debrided1,2. The following report describes a case involving two implants placed in untreated infected sites: they were in contact with a periodontal lesion of a neighbouring tooth and in the region of a non-debrided cyst.
The patient was referred to our clinic reporting mobility of two dental implants. The implants had been placed two weeks before the case was referred to us. On clinical investigation, severe mobility of the implants was noted, as was bleeding and pain on probing. The upper part of the implant was exposed to the oral cavity (Figure 1). The patient had received only an x-ray before initial implants surgery. On the preoperative x-ray, it was clearly visible that the lower left canine was periodontally compromised; a post-extraction cystic lesion was also visible on the second lower left premolar (Figure 2). It was decided that a new radiological examination was required (Figure 3). This revealed that the implants had been placed in the wrong positions. The first implant had been placed in the region of the first lower premolar. The apical part of implant was in contact with the root of lower canine, which had a periodontally apical lesion. The second implant had been placed in the site of a non-debrided post-extraction cyst.
The decision was made to remove both implants as well as the lower canine and to augment the bony defects. After removal of the implants and canine (Figure 4), the infected tissue was debrided, a severe bone defect was revealed (Figures 5 and 6). In this case, the following grafting protocol was used: mixture of platelet-rich fibrin and deproteinised bovine bone particles and covering with a collagen membrane (Bio Oss® and Bio-Gide®, Geistlich AG, Switzerland).
Reflecting on this case, the initial operator should carefully examine the patient prior to implant surgery, starting with endodontic retreatment of the lower canine, then proceeding with debridement of the cyst and augmentation of the bone defect. In this case, implants could be placed suitably after the apical infection had healed completely and the bone had reformed after cyst surgery. A surgical guide for implant placement in such situations is mandatory.
Submitted by: Victor Palarie and Husein Isawi
References
1. Waasdorp JA, Evian CI, Mandracchia M. Immediate placement of implants into infected sites: a systematic review of the literature. J Periodontol. 2010 Jun;81(6):801–8
2. Palmer R. Evidence for survival of implants placed into infected sites is limited. J Evid Based Dent Pract. 2012 Sep;12(3 Suppl):187–8
Figure 1
Figure 4 Figure 5 Figure 6
Figure 2 Figure 3
07 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
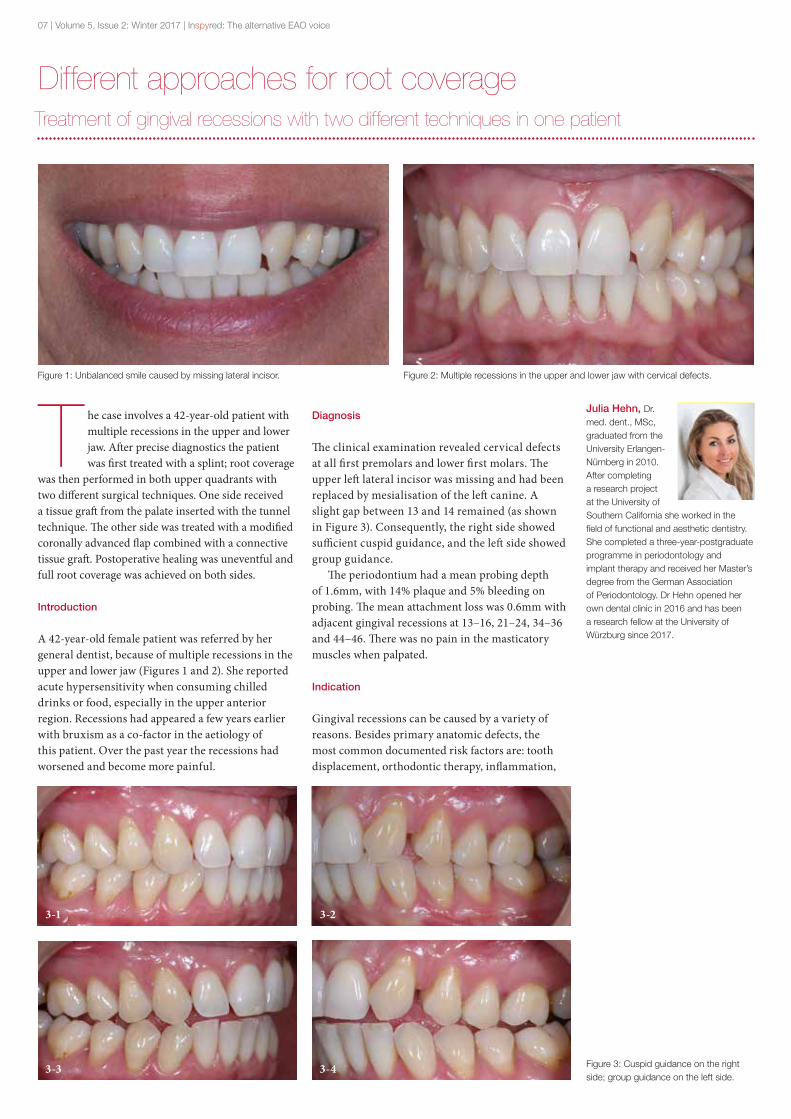
Different approaches for root coverageTreatment of gingival recessions with two different techniques in one patient
T he case involves a 42-year-old patient with multiple recessions in the upper and lower jaw. After precise diagnostics the patient was first treated with a splint; root coverage
was then performed in both upper quadrants with two different surgical techniques. One side received a tissue graft from the palate inserted with the tunnel technique. The other side was treated with a modified coronally advanced flap combined with a connective tissue graft. Postoperative healing was uneventful and full root coverage was achieved on both sides.
Introduction
A 42-year-old female patient was referred by her general dentist, because of multiple recessions in the upper and lower jaw (Figures 1 and 2). She reported acute hypersensitivity when consuming chilled drinks or food, especially in the upper anterior region. Recessions had appeared a few years earlier with bruxism as a co-factor in the aetiology of this patient. Over the past year the recessions had worsened and become more painful.
Diagnosis
The clinical examination revealed cervical defects at all first premolars and lower first molars. The upper left lateral incisor was missing and had been replaced by mesialisation of the left canine. A slight gap between 13 and 14 remained (as shown in Figure 3). Consequently, the right side showed sufficient cuspid guidance, and the left side showed group guidance.
The periodontium had a mean probing depth of 1.6mm, with 14% plaque and 5% bleeding on probing. The mean attachment loss was 0.6mm with adjacent gingival recessions at 13–16, 21–24, 34–36 and 44–46. There was no pain in the masticatory muscles when palpated.
Indication
Gingival recessions can be caused by a variety of reasons. Besides primary anatomic defects, the most common documented risk factors are: tooth displacement, orthodontic therapy, inflammation,
Julia Hehn, Dr. med. dent., MSc, graduated from the University Erlangen-Nürnberg in 2010. After completing a research project at the University of Southern California she worked in the field of functional and aesthetic dentistry. She completed a three-year-postgraduate programme in periodontology and implant therapy and received her Master’s degree from the German Association of Periodontology. Dr Hehn opened her own dental clinic in 2016 and has been a research fellow at the University of Würzburg since 2017.
Figure 1: Unbalanced smile caused by missing lateral incisor. Figure 2: Multiple recessions in the upper and lower jaw with cervical defects.
Figure 3: Cuspid guidance on the right side; group guidance on the left side.
3-23-1
3-3 3-4
Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 08
and excessive occlusal load1. A secondary loss of soft tissue can be caused by excessive brushing or poor oral hygiene.
Several techniques for treating single and multiple recessions have been published with stable long-term results2. The coronal flap is the best documented one, achieving long-term success rates of up to 90%3. However, the vertical releasing incisions involved in this procedure may decrease the blood supply to the flap and cause visible scarring4. Different flap designs without vertical incisions – like the tunnel technique or the modified coronally advanced flap technique – have therefore gained popularity5. The use of tissue grafts and substitute materials like collagen matrices or acellular dermal matrices in conjunction with this technique has been widely tested. The connective tissue graft still represents the gold standard for treating recession-type defects6, 7.
Another alternative approach is the application of enamel matrix protein derivatives. Though various publications have reported promising long-term results in periodontal regeneration therapy, its applications for treating gingival recessions remain controversial8, 9.
Planning
Before surgery, a functional analysis was carried out using a jaw measurement system (Zebris®, Mani-Schütz Dental). The patient also received splint therapy. According to the Miller classification10, all recessions were type I defects: the recessions did not reach the mucogingival junction and there was no loss of interproximal tissue. Because the patient was a non-smoker and she had good oral hygiene, the prognosis for surgical treatment was good. To avoid visible scarring and ensure a good aesthetic outcome in the upper front, techniques without vertical incisions were preferred.
Procedure
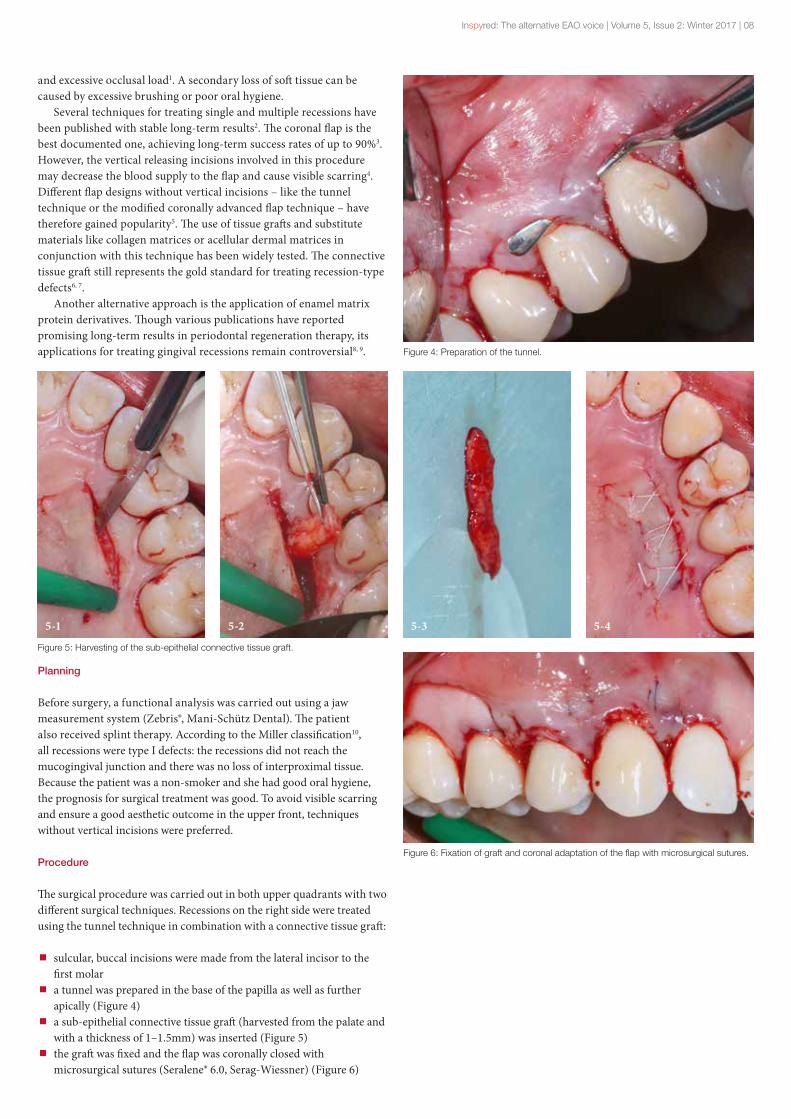
The surgical procedure was carried out in both upper quadrants with two different surgical techniques. Recessions on the right side were treated using the tunnel technique in combination with a connective tissue graft:
sulcular, buccal incisions were made from the lateral incisor to the first molar
a tunnel was prepared in the base of the papilla as well as further apically (Figure 4)
a sub-epithelial connective tissue graft (harvested from the palate and with a thickness of 1–1.5mm) was inserted (Figure 5)
the graft was fixed and the flap was coronally closed with microsurgical sutures (Seralene® 6.0, Serag-Wiessner) (Figure 6)
Figure 6: Fixation of graft and coronal adaptation of the flap with microsurgical sutures.
Figure 4: Preparation of the tunnel.
Figure 5: Harvesting of the sub-epithelial connective tissue graft.
5-45-35-1 5-2
09 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
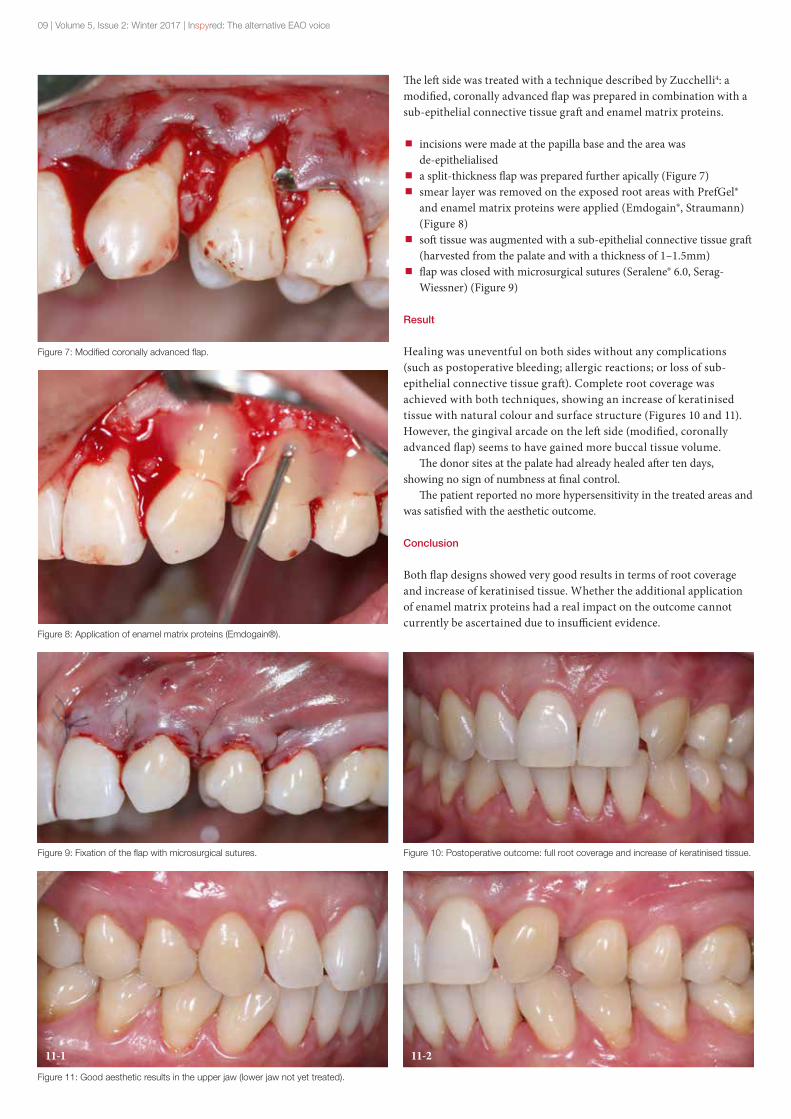
The left side was treated with a technique described by Zucchelli4: a modified, coronally advanced flap was prepared in combination with a sub-epithelial connective tissue graft and enamel matrix proteins.
incisions were made at the papilla base and the area was de-epithelialised
a split-thickness flap was prepared further apically (Figure 7) smear layer was removed on the exposed root areas with PrefGel® and enamel matrix proteins were applied (Emdogain®, Straumann) (Figure 8)
soft tissue was augmented with a sub-epithelial connective tissue graft (harvested from the palate and with a thickness of 1–1.5mm)
flap was closed with microsurgical sutures (Seralene® 6.0, Serag-Wiessner) (Figure 9)
Result
Healing was uneventful on both sides without any complications (such as postoperative bleeding; allergic reactions; or loss of sub-epithelial connective tissue graft). Complete root coverage was achieved with both techniques, showing an increase of keratinised tissue with natural colour and surface structure (Figures 10 and 11). However, the gingival arcade on the left side (modified, coronally advanced flap) seems to have gained more buccal tissue volume.
The donor sites at the palate had already healed after ten days, showing no sign of numbness at final control.
The patient reported no more hypersensitivity in the treated areas and was satisfied with the aesthetic outcome.
Conclusion
Both flap designs showed very good results in terms of root coverage and increase of keratinised tissue. Whether the additional application of enamel matrix proteins had a real impact on the outcome cannot currently be ascertained due to insufficient evidence.
Figure 11: Good aesthetic results in the upper jaw (lower jaw not yet treated).
Figure 7: Modified coronally advanced flap.
Figure 8: Application of enamel matrix proteins (Emdogain®).
Figure 9: Fixation of the flap with microsurgical sutures. Figure 10: Postoperative outcome: full root coverage and increase of keratinised tissue.
11-1 11-2

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 10
References
1. Loe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalende, severity, extent of gingival recessions. J Periodontal 1992, 63: 489–495
2. Cairo, F. (2017). "Periodontal plastic surgery of gingival recessions at single and multiple teeth." Periodontol 2000 75(1): 296–316.
3. Pini Prato, G. P., et al. (2005). "Coronally advanced flap: the post-surgical position of the gingival margin is an important factor for achieving complete root coverage." J Periodontol 76(5): 713–722.
4. Zucchelli, G., et al. (2009). "Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival recessions: a comparative controlled randomized clinical trial." J Periodontol 80(7): 1083–1094.
5. Rebele, S. F., et al. (2014). "Tunnel technique with connective tissue graft versus coronally advanced flap with enamel matrix derivative for root coverage: a RCT using 3D digital measuring methods. Part II. Volumetric studies on healing dynamics and gingival dimensions." J Clin Periodontol 41(6): 593–603.
7. Chambrone L, Chambrone D, Pustiglioni FE, Chambrone LA, Lima LA. Can subepithelial connective tissue grafts be considered the gold standard procedure in the treatment of Miller Class I and II recession-type defects? J Dent. 2008;36(9):659–671.
8. de Sanctis, M., et al. (2011). "Coronally advanced flap associated with a connective tissue graft for the treatment of multiple recession defects in mandibular posterior teeth." Int J Periodontics Restorative Dent 31(6): 623–630.
9. Zucchelli, G., et al. (2014). "The connective tissue graft wall technique and enamel matrix derivative to improve root coverage and clinical attachment levels in Miller Class IV gingival recession." Int J Periodontics Restorative Dent 34(5): 601–609.
10. Sato, S., et al. (2006). "Treatment of Miller Class III recessions with enamel matrix derivative (Emdogain) in combination with subepithelial connective tissue grafting." Int J Periodontics Restorative Dent 26(1): 71–77.
11. Miller PD., Jr A classification of marginal tissue recession. Int J Periodontics Restorative Dent. 1985;5:8–13.

11 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Immediate dentoalveolar restorationA new perspective for immediate implant placement in compromised sockets
T he purpose of this article is to present a step-by-step protocol for immediate dentoalveolar restoration (IDR). This technique (first put forward by Dr
Martins Da Rosa3, 4) offers a new approach for immediate implant placement and immediate provisionalisation following the extraction of a maxillary incisor in a compromised socket with severe damage to the buccal plate.
IDR aims to restore the bone defect while maintaining the gingival architecture and allowing implant placement and immediate loading in a single surgical procedure using a hybrid connective tissue and bone graft from the maxillary tuberosity. This article will also explore how IDR may benefit from the implementation of new technologies.
Introduction
Immediate implant placement in a fresh extraction socket has been well described. The protocol has shown very high success rates (similar to those placed in healed sites2) and is now considered highly predictable. However, the procedure can be extremely challenging in many clinical situations and is often rated either advanced or complex5, 6.
The purpose of contemporary aesthetic dentistry is to achieve an inconspicuous reconstruction or replacement of missing teeth in a biomimetic fashion. The architecture of the reconstructed hard and soft tissues should therefore mimic nature as far as possible. Nevertheless, the reasons for tooth extraction and immediate implant placement – such as endodontic failure, advanced periodontal disease, trauma and root fracture – are frequently associated with severe alveolar bone resorption and soft tissue loss4. In cases involving extensive bone loss, immediate provisionalisation is contra-indicated because of the high aesthetic risk7.
Several procedures have been proposed to re-establish the compromised gingival and alveolar bone architecture, such as forced orthodontic eruption8, 9, guided bone regeneration (GBR)10, 11, and bone-block grafts with or without sub-epithelial connective tissue grafts12, 13. All of these treatments can be used to treat bone defects before, during, or after tooth extraction, and in two or three surgical stages. Conversely, the possibility of reconstruction using grafting procedures and immediate restoration in a single operation has not been supported by several clinical studies14.
The IDR technique was developed to address extreme cases like those described above in a single surgery including: extraction of a failing tooth; implant placement; and provisionalisation using a bone reconstruction of the missing buccal plate without having to raise a flap. This technique
introduced the use of a cortico-cancellous bone graft harvested from the maxillary tuberosity to restore buccal bone defects at the time of implant placement. Several treatments of cases involving minimal-to-severe bone loss in post-extraction sites have been reported14. In what follows, we will describe two clinical cases which we treated with IDR.
Case 1
The first case involves a 49-year-old woman who was complaining about her central right maxillary incisor. The clinical examination showed a failing tooth 11. The tooth exhibited degree III mobility; localised periodontitis; pocket probing depth from 8 to 11mm; bleeding on probing; and suppuration (Figure 1). A CBCT cross-section revealed total loss of the buccal plate combined with a moderate defect in the palatal side (Figure 2).
Unfortunately, the extraction had to be performed, and it was decided that, five days prior to surgery, a prophylactic regimen of antibiotics (amoxicillin 1g twice a day) be prescribed as infection/abscess was present (as described in the original protocol).
Local anaesthesia (primacaine, adrenalin 1/100,000) was first administered. Then an intra-sulcular incision around the tooth being extracted was made using the Viper Microblade® (MJK instruments, Marseille, France) (Figure 3). The tooth was extracted without any structural damage, and the integrity of the remaining bone wall was preserved. A micro-curette was then used to remove
Benjamin
Cortasse, obtained his DDS from the University of Montpellier in 2002. He received a degree in biomaterials from Marseille University and a degree in periodontology from Montpellier University in 2004. He completed a postgraduate course in implantology and biomaterials at the University of Bordeaux.
Dr Cortasse currently works in his clinic near Avignon (France) and teaches implantology and soft tissue management at a number of companies, institutions and universities. He has authored several articles and lectured at national and international courses and conferences. He invented the Viper, a microsurgical blade.
Figure 2
Figure 1 Figure 1: Initial situation.Figure 2: Pre-operative CBCT.

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 12
the granulation tissue and the remaining periodontal connective tissue from the extracted socket.
The socket walls were probed in the apicocoronal and mesiodistal directions to assess the degree of bone damage and to confirm the anatomical shape of the defect (Figure 4). The implant was then placed in a suitable 3D position with a flapless procedure (Figure 5). The implant platform was placed 3mm apical to the cemento-enamel junction (CEJ) of the contralateral tooth. The implant was anchored to the palatal wall to provide enough space for buccal hard and soft tissue reconstruction (Figure 6). Implant position is a primary factor for achieving hard and soft tissue stability in IDR (as in any other technique). Regardless of which tooth is replaced, a gap of approximately 3mm between the buccal implant surface and the outer buccal bone wall is required.
At this stage, a provisional crown was made. In this case we chose to use the extracted tooth, by removing the root and creating a 3mm (approx.) hole through its crown. The temporary abutment, made out of titanium, was tried to ensure it could be well seated on the implant connection without occlusal interference. A composite opaque resin (Ivoclar Vivadent) was then used to offset the shade of the metal beneath (Figure 7). The appearance of the temporary crown was optimised with light-polymerising composite resin (Tetric EvoCeram, Ivoclar Vivadent).
The ideal emergence profile was worked out to obtain a concave contour for the trans-gingival part of the provisional crown (Figure 8). This provided space for better accommodation of the soft tissue and promoted a thicker and more stable gingival margin. Then, in order to harvest a connective tissue graft, the donor site was injected with anaesthetic from the base of the vestibule to the palatal portion of the maxillary tuberosity.
Figure 9
Figure 3
Figure 4c
Figure 7 Figure 8
Figure 5 Figure 6
Figure 4a Figure 4b
Figure 4a, b, c: Probe assessment of bone defect.Figure 5: Implant placement.Figure 6: Palatal implant positioning with vestibular gap.Figure 7: Provisional and temporary abutment adjustment.Figure 8: Provisional crown.Figure 9: Insertion of the bone graft harvested from tuberosity.

13 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Figure 17 Figure 18
Figure 10 Figure 12
Figure 13 Figure 14 Figure 15
Figure 11
Figure 16a Figure 16b
An initial mucoperiosteal incision was made at the maxillary tuberosity following the distal contour of the last molar. The flap was then divided starting at the buccal line angle, and directing the blade to the most posterior portion (Figure 10). Next, the bone was cut with a straight chisel (Schwert IDR Kit) along the relaxing incisions to define the bone fracture line (Figure 11). First, the chisel was placed perpendicular to the bone structure on the incision line; second, its angulation was adjusted to reach an axis parallel to the outer surface. It was gradually moved deeper, as far as the distal limit of the relaxing incisions, to obtain a uniform bone graft (Figure 12). Finally, the bone was fractured, taking care to maintain an epithelial pedicle to ensure better nutrition for the flap that would cover the donor site (Figure 13).
The bone graft was modelled to the anatomy of the defect as quickly as possible; the finer the adaptation the better (Figure 14). The bone portion of the graft must coincide with the implant platform. Its stability
Figure 10: Tuberosity access (courtesy M. Fadanelli).Figure 11: Special chisels.Figure 12: Using chisels for bone harvest from tuberosity (courtesy M. Fadanelli).Figure 13: Bone harvesting (courtesy M. Fadanelli).Figure 14: Post-operative situation: day 0.Figure 15: Post-operative healing at three weeks.Figure 16a, b: Comparative CBCT before and after treatment.Figure 17: Provisional situation six months post-operation.Figure 18: Occlusal view of transmucosal healing.
Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 14
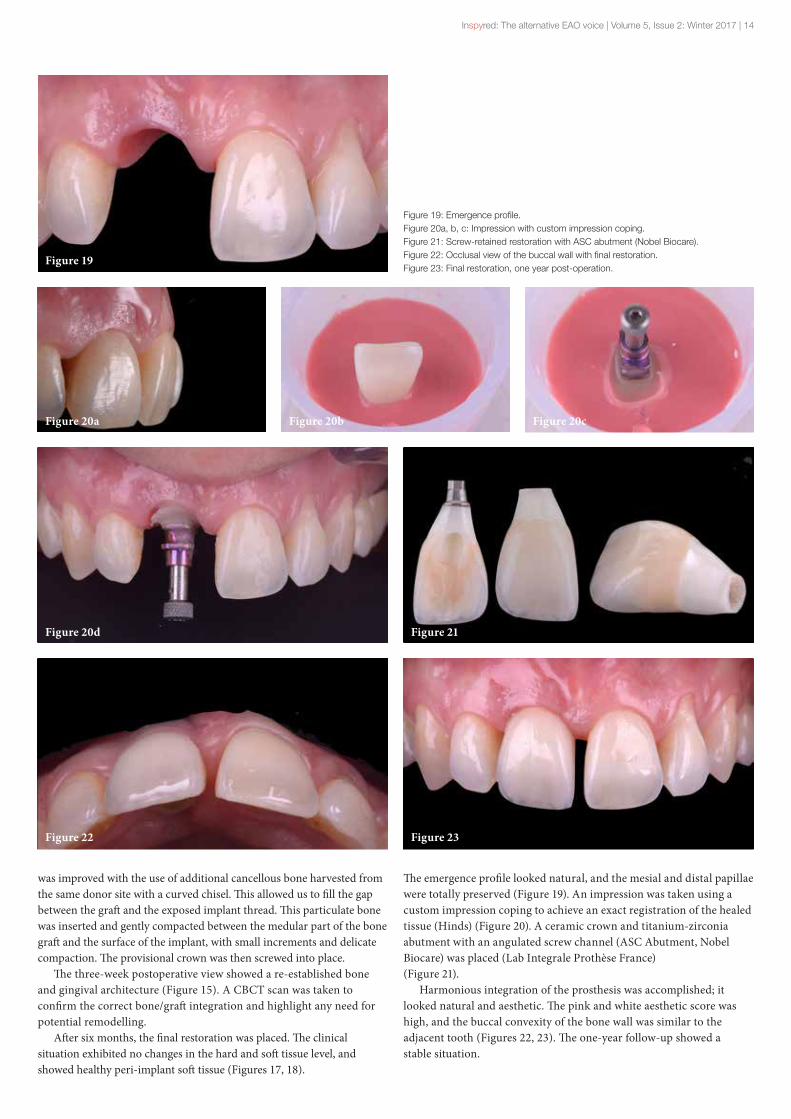
was improved with the use of additional cancellous bone harvested from the same donor site with a curved chisel. This allowed us to fill the gap between the graft and the exposed implant thread. This particulate bone was inserted and gently compacted between the medular part of the bone graft and the surface of the implant, with small increments and delicate compaction. The provisional crown was then screwed into place.
The three-week postoperative view showed a re-established bone and gingival architecture (Figure 15). A CBCT scan was taken to confirm the correct bone/graft integration and highlight any need for potential remodelling.
After six months, the final restoration was placed. The clinical situation exhibited no changes in the hard and soft tissue level, and showed healthy peri-implant soft tissue (Figures 17, 18).
The emergence profile looked natural, and the mesial and distal papillae were totally preserved (Figure 19). An impression was taken using a custom impression coping to achieve an exact registration of the healed tissue (Hinds) (Figure 20). A ceramic crown and titanium-zirconia abutment with an angulated screw channel (ASC Abutment, Nobel Biocare) was placed (Lab Integrale Prothèse France) (Figure 21).
Harmonious integration of the prosthesis was accomplished; it looked natural and aesthetic. The pink and white aesthetic score was high, and the buccal convexity of the bone wall was similar to the adjacent tooth (Figures 22, 23). The one-year follow-up showed a stable situation.
Figure 23
Figure 20b Figure 20c
Figure 22
Figure 19
Figure 20d
Figure 20a
Figure 21
Figure 19: Emergence profile.Figure 20a, b, c: Impression with custom impression coping.Figure 21: Screw-retained restoration with ASC abutment (Nobel Biocare).Figure 22: Occlusal view of the buccal wall with final restoration.Figure 23: Final restoration, one year post-operation.

15 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Case 2
The second case involves a 46-year-old patient with a root fracture on tooth 22. Initial examination showed discrete inflammation but no suppuration. A thick biotype was identified (Figure 24). From the CBCT examination, a buccal bone defect measuring around 7mm was discovered. Fortunately, this case was rated class 1 according to the root classification described by J. Kan. It was therefore decided to perform immediate dentoalveolar restoration (Figure 25).
Even if we practise classic techniques with success for many years, the inherent lack of accuracy, repeatability and simplicity naturally leads us to guided surgery. Indeed, many studies have shown the advantages of guided surgery, provided that certain criteria are met. In this case, our aim was to use a quicker, safer and more accurate alternative to free-hand positioning17, 18. A 3D printed guide (MGUIDE, MIS implant) was used.
The 3D implant position was guided by the desired prosthetic outcome. The guide was then generated (Figure 26). This type of guide has a very large number of supports to ensure an optimal stability while being very open. The guide was printed and tags were positioned on occlusal, vestibular and palatal areas. Hence it felt securely fixed when placed in the mouth. This allowed the surgeon to keep the sensation of a routine surgery and ensure greater comfort (Figure 27).
The final implant position as well as the provisional crown and the definitive zirconia abutment (Figure 28) were decided and designed. According to the literature, the best way for maximum attachment and biocompatibility to be achieved is to place the final abutment on the day of surgery, without removing it19, 20 (Figure 29). The lab (MLAB, MIS) delivered a Ti-Base with a bonded zirconia abutment and milled
provisional crown (Figure 30), with an ideal concave emergence profile (Figure 29).
After anaesthesia, an intra-sulcular incision around the tooth being extracted was made, using the Viper Microblade® (MJK instruments) (Figure 31). To perform an atraumatic extraction of the root, the Benex system (Dexter instruments) was used. It looks like a corkscrew. This instrument allowed us to extract the tooth without damaging soft and hard tissues (Figure 32).
After the extraction, the defect was probed to evaluate its anatomy. In this case it reached a depth of around 6mm and width of 4mm (Figure 33). The guide was used with a 2mm pilot drill, and at the time of placement it confirmed correct positioning (Figure 34). We decided to use the IDR technique21. The technique was performed as described in Case 1 (Figure 35).
Figure 25
Figure 28
Figure 30 Figure 31
Figure 29a Figure 29b
Figure 26 Figure 27
Figure 24
Figure 24: Case 2: initial situation.Figure 25: CBCT.Figure 26: Implant planning.Figure 27: Printed guide (Mguide, MIS).Figure 28: STL files and digital prosthetic project (Mlab, MIS).Figure 29: Ti-Base, zirconia abutment and provisional crown.Figure 30: Natural emergence profileFigure 31: Viper blade in intra-sulcular position before extraction.

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 16
Following implant placement and graft stabilisation, the final zirconia abutment was screwed on (Figure 36). A minor adjustment of the emergence profile of the temporary crown was made to enhance its compatibility with the site. A micro-concavity was created, and a sequence of polishing burrs was applied. A hole was created through the crown to facilitate removal of excess cement (Figure 37). An ideal emergence profile, similar to the natural tooth, was achieved (Figure 38).
Immediate and ten-day postoperative assessments showed how effective this less traumatic approach could be, compared to conventional immediate implant placement combined with bone and soft tissue grafts (Figure 39). Two months later, the situation has remained stable, so it is possible to move on to the next step of the treatment plan: to treat the natural teeth to rebuild a natural smile (Figure 40).
Discussion
The protocol for immediate loading of implants following tooth extraction – in cases without any damage to the tissue – is well established in the literature22, 23. Maintenance of the bone and gingival
Figure 32
Figure 38
Figure 36a Figure 36b Figure 37
Figure 34a
Figure 35b
Figure 34b
Figure 35c
Figure 33
Figure 35a
Figure 32: Root extraction with Benex system.Figure 33: Probe assessment of bone defect.Figure 34a, b: Drill sequence and implant placement through the guide.Figure 35a, b, c: Modelling and insertion of the bone harvested from tuberosity.Figure 36a, b: Final zirconia abutment.Figure 37: Enhancement of the emergence profile.Figure 38: Natural emergence profile.

17 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Figure 39a
Figure 40
Figure 39b
Figure 39a: Soft tissue position, day 0.Figure 39b: Soft tissue position, day 10.Figure 40: Three months post-operation.
architecture; aesthetic restoration; and reduction of the treatment duration are key factors which have been identified in the technique24, 25.
However, extensive damage to the buccal bone may jeopardise the outcome of immediate implant placement and immediate provisionalisation. Treatment alternatives in cases involving alveolar defects are widely documented10, 26, 27. Bone-block grafts or GBR represent viable solutions before or after delayed implant placement. But in cases of tooth loss along with the loss of support structures, there is a higher risk of unsatisfactory aesthetic outcomes. Moreover, such treatments include multiple surgeries and extended healing periods.
The IDR technique can offer significant improvements to the expected aesthetic result and treatment duration. The goal of this technique is to perform a number of procedures during a single surgical stage: the extraction of a failing tooth; implant placement; alveolar reconstruction; and provisionalisation. Furthermore, no flap needs to be raised to preserve the gingival architecture. Some studies5, 28 have shown that papilla-sparing incisions could minimise interproximal bone loss. A buccal bone wall of sufficient dimensions is a prerequisite for aesthetic soft tissue contours on the facial aspect5, 28.
A recent study found the IDR technique to be a viable option for treating a compromised extraction socket in the aesthetic zone during an immediate single implant placement29. However, the maxillary tuberosity also presents disadvantages, two of which are limited quantity and access.
Conclusion
This technique may be considered a viable and predictable option for placing implants in the aesthetic zone. Immediate loading of the implant in damaged fresh sockets, in conjunction with a bone graft from the tuberosity may be performed in a single procedure, enabling patients to avoid multiple surgical procedures. Surgical time can be further reduced if new technologies are used, such as: guided surgery protocols; printed models; and CAD/CAM restorations made before the day of surgery.
References
1. Lazzara RJ. Immediate implant placement into extraction sites: surgical and restorative advantages. Int J Periodontics Restorative Dent. 1989;9(5):332–43.
2. Del Fabbro M, Ceresoli V, Taschieri S, Ceci C, Testori T. Immediate loading of postextraction implants in the esthetic area: systematic review of the literature [published online April 22, 2013]. Clin Implant Dent Relat Res.
3. Martins Da Rosa JC, Immediate Dentoalveolar Restoration. Quintessence Editora Brasil
4. Martins Da Rosa JC, Rosa AC, da Rosa DM, Zardo CM Immediate Dentoalveolar Restoration of compromised sockets: a novel technique. Eur J Esthet Dent. 2013 Autumn;8(3):432–43.
5. Buser D, Chappuis V, Bornstein MM, Wittneben JG, Frei M, Belser UC. Long-term stability of contour augmentation with early implant placement following single tooth extraction in the esthetic zone a prospective, cross-sectional study in 41 patients with a 5- to 9-year follow- up. J Periodontol 2013;84:1517–1527.
6. Cosyn J, Eghbali A, De Bruyn H, Collys K, Cleymaet R, De Rouck T. Immediate single-tooth implants in the anterior maxilla: 3-year results of a case series on hard and soft tissue response and aesthetics. J Clin Periodontol 2011;38:746–753
7. Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. Int J Oral Maxillofac Implants 2004;19: 43–61.
8. Chambrone L, Chambrone LA. Forced orthodontic eruption of fractured teeth before implant placement: case report. J of the Canadian Dental Assoc 2005;71:257–261.
9. Salama H, Salama M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: a systematic approach to the management of the extraction site defects. Int J Periodontics Rest Dent 1993;13:312–333.

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 18
10. Jung RE, Kokovic V, Juri- sic M, Yaman D, Subramani K, Weber FE. Guided bone regeneration with a synthetic biodegradable membrane: a comparative study in dogs. Clin Oral Implants Res 2011;22:802–807.
11. Van Steenberghe D, Callens A, Geers L, Jacobs R. The clinical use of deproteinized bovine bone mineral on bone regeneration in conjunction with immediate implant installation. Clin Oral Implants Res 2000;11:210–216.
12. Schneider D, Grunder U, Ender A, Hämmerle C H, Jung RE. Volume gain and stability of peri-implant tissue following bone and soft tissue augmentation: 1-year results from a prospective cohort study. Clin Oral Implants Res 2011;22:28–37.
13. Rebaudi A, Massei G, Trisi P, Calvari F. A new technique for bone augmentation and papilla reconstruction with autogenous free gingival bone grafts. Int J Periodontics Rest Dent 2007;27: 429–439.
14. Rosa JC, Rosa AC, Francis- Esthetic outcomes and tissue stability of implant placement in compromised sockets following immediate dentoalveolar restoration: results of a prospective case series at 58 months follow-up. Int J Periodontics Restorative Dent 2014;34:199–208.
15. Hinds KF Custom impression coping for an exact registration of the healed tissue in the esthetic implant restoration. Int J Periodontics Restorative Dent. 1997 Dec;17(6):584–91
16. Kan JY1, Roe P, Rungcharassaeng K, Patel RD, Waki T, Lozada JL, Zimmerman G.Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. Int J Oral Maxillofac Implants. 2011 Jul–Aug;26(4):873–6.
17. Farley NE, Kennedy K, McGlumphy EA, Clelland NL. Split-mouth comparison of the accuracy of computer-generated and conventional surgical guides. Int J Oral Maxillofac Implants. 2013 Mar–Apr;28(2):563–72. doi: 10.11607/jomi.3025.
18. Hämmerle CH1, Cordaro L, van Assche N, Benic GI, Bornstein M, Gamper F, Gotfredsen K, Harris D, Hürzeler M, Jacobs R, Kapos T, Kohal RJ, Patzelt SB, Sailer I, Tahmaseb A, Vercruyssen M, Wismeijer D.Digital technologies to support planning, treatment, and fabrication processes and outcome assessments in implant dentistry. Summary and consensus statements. The 4th EAO consensus conference 2015. Clin Oral Implants Res. 2015 Sep;26 Suppl 11:97–101. doi: 10.1111/clr.12648.
19. Rompen EThe impact of the type and configuration of abutments and their (repeated) removal on the attachment level and marginal bone. Eur J Oral Implantol. 2012;5 Suppl:S83–90.
20. Jepsen S, Berglundh T, Genco R, Aass AM, Demirel K, Derks J, Figuero E, Giovannoli JL, Goldstein M, Lambert F, Ortiz-Vigon A, Polyzois I, Salvi GE, Schwarz F, Serino G, Tomasi C, Zitzmann NU. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol. 2015 Apr;42 Suppl 16:S152–7. doi: 10.1111/jcpe.12369.
21. da Rosa JC, Rosa AC, Fadanelli MA, Sotto-Maior Placement, reconstruction of compromised sockets, and repair of gingival recession with a triple graft from the maxillary tuberosity: a variation of the immediate dentoalveolar restoration technique. J Prosthet Dent 2014;112:717–722.
22. Belser UC, Med P, Bruno D, Higginbot- tom DM, Buser D, Dent PM. Outcome analysis of implant restorations located in the anterior maxilla: A review of the recent literature. Int J Oral Maxillofac Implants 2004;19(suppl):30–42.
23. Buser D, Martin W, Belser UC. Optimiz- ing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int J Oral Maxillofac Implants 2004;19(suppl):43–61.
24. Wöhrle PS. Single-tooth replacement in the aesthetic zone with immediate provisionalization: fourteen consecutive case reports. Pract Periodontics Aesthet Dent 1998;10:1107–1114.
25. Touati B, Guez G. Immediate implantation with provisionalization: from literature to clinical implications. Pract Proced Aesthet Dent 2002;14:699–707.
26. Berglungh T, Lindhe J. Healing arround implants placed in bone defects treated with Bio-Oss: an experimental study in the dog. Clin Oral Implants Res 1997;8: 117–124.
27. Van Steenberghe D, Callens A, Geers L, Jacobs R. The clinical use of deproteinized bovine bone mineral on bone regeneration in conjunc- tion with immediate implant installation. Clin Oral Implants Res 2000;11:210–216.
28. Cosyn J, Sabzevar MM, De Bruyn H. Predictors of inter-proximal and midfacial recession following single implant treatment in the anterior maxilla: A multivariate analysis. J Clin Periodontol 2012;39: 895–903.
29. Rosa JC, Rosa AC, Francischone CE, Sotto-Maior BS Esthetic outcomes and tissue stability of implant placement in compromised sockets following immediate dentoalveolar restoration: results of a prospective case series at 58 months follow-up. Int J Periodontics Restorative Dent. 2014 Mar–Apr;34(2):199–208. doi: 10.11607/prd.1858.

19 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Highlights from Madrid 2017Report from the EAO’s 26th annual scientific meeting
The EAO celebrated a landmark event in Madrid this October: its 26th annual scientific meeting and first ever joint congress. In
collaboration with one of Spain’s most influential associations, SEPES, and with the inclusion of a symposium organised by SEPA, the EAO delivered its prestigious annual meeting in style. A staggering 5,400 professionals came from all over the world to exchange knowledge and discover cutting-edge research.
This year's congress theme was ‘Twenty-five years of implant dentistry. What have we learned?’ More than 80 world-class experts set out to answer this question and share their expertise. Topics ranged from the evolution of surgical protocols to restorative treatments for partially edentulous patients. A number of new session formats were added to the scientific programme with a focus on take-home messages and accessible tips for attendees. And science met technology as manufacturers demonstrated their state-of-the-art equipment to help patients eat, talk and smile.
EAO online congress: A digital debut
This year, the EAO pulled out all the stops. For the first time, three sessions were broadcast live online. People who had liked the EAO on Facebook could tune in from around the world and watch these sessions free of charge. Before and after each session, viewers could access exclusive online content including: an introduction from clinical experts; debrief after the session; and a special online question and answer session.
The online congress made the annual meeting more accessible than ever. Viewers could share and comment on the livestream, and could even direct the discussion by submitting their own questions. Moderators passed online questions to the speakers to discuss live. More than 5,300 people tuned in for these special sessions, making the digital debut of the EAO congress a resounding success.

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 20
Honorary Membership
Honorary membership of the EAO was awarded to Dr Franck Renouard during the opening ceremony (pictured above). Honorary membership is awarded to individuals who have made outstanding contributions to the field. Franck was president of the EAO from 2004–2006, and has been an active and dedicated member of the EAO Council for a number of years.
Faculty and Members' dinner
This year's Faculty and Members' dinner took place at the enchanting Casino de Madrid. The Casino was founded in 1836, and now houses an exquisite collection of paintings and sculptures. EAO guests enjoyed a champagne reception before being escorted to the stunning dining rooms. A recognised site of Artistic and National Heritage, the Casino provided a beautiful setting for the dinner, where guests were treated to an exquisite five course meal.

21 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
EAO Certificate for Implant-based Therapy
During the awards ceremony on Saturday, Alberto Sicilia announced this year's recipients of the EAO's prestigious Certificate for Implant-based Therapy (pictured right, left to right): Teppei Tsukiyama, Masami Arai, Oswaldo Villa and Lucio Ruffato. Certification demonstrates to patients and regulatory authorities a clinician's competence to perform basic implant therapies.
Scientific prizes
During the awards ceremony, the winners of the EAO’s seven European Prizes for Research in Implant Dentistry were also announced. The winners received a trophy and a €2,000 award. This year's winners of each category (pictured left, left to right) were as follows:
European Prize for Clinical Research in Implant Dentistry: Surgery. Pietro Felice
European Prize for Clinical Research in Implant Dentistry: Prosthetics. Manrique Fonseca and Carina Boven
European Prize for Research in Implant Dentistry: Poster Presentation. Nicole Passia
European Prize for Basic Research in Implant Dentistry. Omar Omar
European Prize for Clinical Research in Implant Dentistry: Clinical Video on Implant Dentistry. Lukas Fürhauser
European Prize for Research in Implant Dentistry: Clinical Innovations. Giovanni Salvi
(Not pictured) European Prize for Clinical Research in Implant Dentistry: Peri-implant Biology. Stijn Vervaeke

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 22
Customised allogeneic bone-blocksClinical case involving major maxillofacial trauma
O ne of the biggest challenges associated with treating trauma to the maxilla and mandible is very often the lack of bone and teeth. When rehabilitating these
patients, bone augmentation procedures are widely performed prior to implant placement. A number of materials can be used: autologous bone, allogeneic bone, or xenogenous bone-blocks or bone granulates. Bone augmentation is required to ensure sufficient bone height and width for implant placement, and can help achieve functional and aesthetic results.
Different augmentation procedures have been described extensively. Although autografts are still considered the ‘gold standard’, there is increased interest in, and use of, allografts and xenografts.
The use of on-lay bone-blocks is often indicated for horizontal and vertical bone augmentation in cases involving large maxillary and mandibular bone defects. Autogenous bone-blocks can ensure dimensional enlargement of size and density, in contrast to the particulated form which generally require prolonged treatment time and additional materials to secure volume enhancement such as barrier membranes, with or without reinforcement, and fixation pins.
In practice, however, the amount and size of intraoral bone available at the donor site (either from the rami or the chin area) and the morbidity associated with graft procedures often limits the treatment recommendations and patient’s acceptance. Complications associated with intraoral bone-blocks are relatively common, including: pain; swelling; wound dehiscence; infection; and, more rarely, nerve injury with altered sensation in the mandibular or lingual nerve. Procedures using harvested extraoral bone from the tibia or iliac crest are often limited to cases involving severe trauma.
The treatment protocol for bone augmentation with autogenous bone is well described in the literature. Although the procedure is considered the ‘gold standard’, some published data1, 2 shows a substantial volume reduction of the augmented autogenous bone (up to 30%). The use of non-autogenous bone to achieve osseointegration is the subject of a great deal of research. A number of studies have suggested that allogeneic bone may provide a viable alternative3–6, but there is insufficient evidence available to support a definitive decision for autogenous or allogeneic bone grafts.
The use of allogeneic bone enables the selection of bone-blocks with a predefined configuration and size. In turn, this allows us to overcome the most common limitations of harvesting procedures, such as availability and morbidity. By using CBCT to create a virtual bone-defect model, it is possible to design a bone-block customised to the individual patient (CAD – computer-aided design), which is then manufactured in accordance with the design (CAM
– computer-aided manufacturing). In this way a bone-block with an optimal fit can be created. Thereby less surgical time is needed, which is linked with lower morbidity and reduced risk of infection. This factor increases patient acceptance and satisfaction. In turn, this allows the surgeon to concentrate on achieving tension-free primary wound closure, which is one of the most important factors in bone augmentation procedures. The combined CBCT and 3D CAD/CAM method has not been fully explored in the literature7–10 but studies indicate good bone formation, clinical appearance, and patient satisfaction rates.
The long-term stability of the augmented area is yet to be determined, although some studies indicate that dimensional changes in the allograft may occur, as with autogenous bone. Although more studies are required, lateral and vertical ridge augmentation using allogeneic bone-blocks can be considered to be successful both clinically and histologically. The newly formed vital bone develops a structure suitable for implant placement after 4–6 months of healing11–13. A definitive conclusion regarding the long-term success of the augmented allogeneic bone and the survival of the inserted implants cannot be reached at this time. Future studies with long-term follow-ups are required to further illuminate this issue14.
Patient case
The following case describes the treatment of a 34-year-old female who had been hit by a car and suffered multiple injuries to the body as well as major trauma to the maxillofacial bone. The patient was referred after a period of hospitalisation, and clinical examination revealed that the incisors in the upper jaw (teeth 12, 11 and 21, 22) had been lost, along with the adjacent bone.
Peter Lindkvist DDS graduated from the Royal Dentist College in Copenhagen in 1984. He is partner in Colosseumklinikken in the center of Copenhagen, and focuses on aesthetic periodontal microsurgery and implant dentistry. He has received postgraduate education in aesthetic soft tissue management, implant dentistry and surgery. He lectures nationally in implant dentistry and aesthetic periodontal microsurgery, with both theoretical and hands-on sessions. He has been a board member and president of the Danish Society for Oral Implantology, and is an active member of the EAO.
Figure 1: Traumatised anterior region 12, 11 and 21, 22.Figure 2: Noticeable lack of buccal soft tissue.
Figure 2
Figure 1
23 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
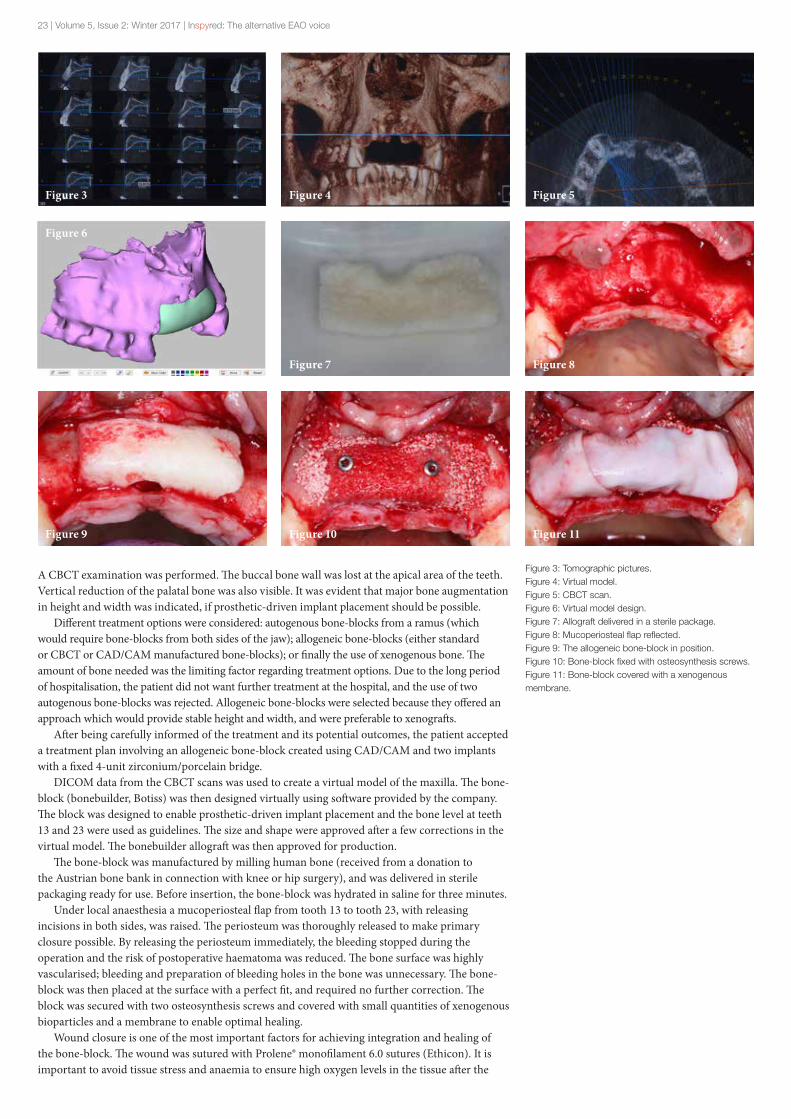
Figure 3: Tomographic pictures.Figure 4: Virtual model.Figure 5: CBCT scan.Figure 6: Virtual model design.Figure 7: Allograft delivered in a sterile package.Figure 8: Mucoperiosteal flap reflected.Figure 9: The allogeneic bone-block in position.Figure 10: Bone-block fixed with osteosynthesis screws.Figure 11: Bone-block covered with a xenogenous membrane.
A CBCT examination was performed. The buccal bone wall was lost at the apical area of the teeth. Vertical reduction of the palatal bone was also visible. It was evident that major bone augmentation in height and width was indicated, if prosthetic-driven implant placement should be possible.
Different treatment options were considered: autogenous bone-blocks from a ramus (which would require bone-blocks from both sides of the jaw); allogeneic bone-blocks (either standard or CBCT or CAD/CAM manufactured bone-blocks); or finally the use of xenogenous bone. The amount of bone needed was the limiting factor regarding treatment options. Due to the long period of hospitalisation, the patient did not want further treatment at the hospital, and the use of two autogenous bone-blocks was rejected. Allogeneic bone-blocks were selected because they offered an approach which would provide stable height and width, and were preferable to xenografts.
After being carefully informed of the treatment and its potential outcomes, the patient accepted a treatment plan involving an allogeneic bone-block created using CAD/CAM and two implants with a fixed 4-unit zirconium/porcelain bridge.
DICOM data from the CBCT scans was used to create a virtual model of the maxilla. The bone-block (bonebuilder, Botiss) was then designed virtually using software provided by the company. The block was designed to enable prosthetic-driven implant placement and the bone level at teeth 13 and 23 were used as guidelines. The size and shape were approved after a few corrections in the virtual model. The bonebuilder allograft was then approved for production.
The bone-block was manufactured by milling human bone (received from a donation to the Austrian bone bank in connection with knee or hip surgery), and was delivered in sterile packaging ready for use. Before insertion, the bone-block was hydrated in saline for three minutes.
Under local anaesthesia a mucoperiosteal flap from tooth 13 to tooth 23, with releasing incisions in both sides, was raised. The periosteum was thoroughly released to make primary closure possible. By releasing the periosteum immediately, the bleeding stopped during the operation and the risk of postoperative haematoma was reduced. The bone surface was highly vascularised; bleeding and preparation of bleeding holes in the bone was unnecessary. The bone-block was then placed at the surface with a perfect fit, and required no further correction. The block was secured with two osteosynthesis screws and covered with small quantities of xenogenous bioparticles and a membrane to enable optimal healing.
Wound closure is one of the most important factors for achieving integration and healing of the bone-block. The wound was sutured with Prolene® monofilament 6.0 sutures (Ethicon). It is important to avoid tissue stress and anaemia to ensure high oxygen levels in the tissue after the
Figure 3
Figure 8
Figure 4
Figure 9
Figure 5
Figure 10 Figure 11
Figure 6
Figure 7

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 24
surgical procedure. The healing was uneventful with only minor swelling, pain and discomfort.
Deciding how long a healing period should last (4–6 months) has often been discussed in the literature, but no decisive conclusions have been drawn. Based on the patient’s x-ray, as well as a clinical picture, we decided on a healing period of 6 months. During this period, the patient had a removable prosthesis and the healing was uneventful.
During the surgical implant installation a mucoperiosteal flap was raised and the fixation screws were removed. There were no signs of resorption of the bone-block and the head of the osteosynthesis screws were at the same level of the bone-block, as they had been at the time of the augmentation procedure (Figure 16). Two Astra EV implants (4.2mm wide and 11mm long) were inserted at region 12 and 22. The bone quality was excellent and primary stability was good. After three months of healing, the implants were exposed and a provisional bridge was inserted to ensure the best possible mucogingival architecture.
The final restoration – a cemented zirconium/porcelain 4-unit bridge on two titanium gold-hue abutments – was delivered two months after insertion of the temporary bridge and five months after implant placement. Function and aesthetics were checked, and the bridge was cemented temporarily for one month. Levels of patient satisfaction were excellent and no changes were necessary. The bridge was then permanently cemented with resin cement.
The patient had suffered the initial trauma in the summer of 2012; bone augmentation was performed in February 2013; and the bridge was cemented in August 2013 (Figure 20). Yearly follow-ups have shown no
visible signs of resorption of the integrated bone around the implants. As a consequence of the bone stability, the soft tissue shows no signs of recession (Figure 21, showing x-rays September 2017).
Conclusion
This case involving a CAD/CAM allogeneic bone-block shows excellent integration of the graft. However, the allogeneic and autogenous bone are exposed to changes during maturation, and it is not possible to precisely predict alterations of the augmented bone in the years to come. The patient’s discomfort during the treatment – both surgical and prosthetic – was minimal, and she has been extremely satisfied with the result.
More research is needed before allogeneic bone-blocks can be considered a conclusive treatment option. But for this patient, who had suffered major trauma, the use of a CAD/CAM allogeneic bone-block has been straightforward and promising.
References
1. Van der Meij AJ, Bart JA, prahl-Andersen B, Valk J, Kostense PJ, Tuinzing DB. Computer tomography in evaluation of early secondary bone grafting, Int J Oral Maxillofac Surg 1994; 23(3):132–136
2. Reinert S, König S, Bremerich A, Eufinger H, Krimmel M. Stability of bone grafting and placement of implants in the severly atrophic maxilla. Br J Oral Maxillofacial Surg 2003; 41(4):249–255.
Figure 16-1 Figure 16-2
Figure 12: Immediately after the operation.Figure 13: 10 days post-operation.Figure 14: After six-month healing period, frontal view.Figure 15: After six-month healing period, occlusal view. Noticeably increased width.Figure 16: Osteosynthesis screws level with the augmented bone after healing period.
Figure 12
Figure 14
Figure 13
Figure 15

25 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
20-1
19-1
21-1
19-3
20-2
19-2
21-2
20-3
Figure 17: Implants inserted at 12 and 22.Figure 18: After three-month healing period; provisional bridge in place.Figure 19: X-rays of the implants after three months.Figure 20: Final bridge cemented, August 2013, frontal view and x-rays.Figure 21: Follow-up x-rays, September 2017.
3. Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most succesful in furnishing bony support for implant placement? Int J Oral Maxillofacial Implants 2007, 22 (suppl):49–70
4. Peleg M, Sawatari Y, Marx RN, Santorio J, Cohen J, Bejarano P, Malinin T. Use of corticocancellous allogenic bone-blocks for augmentation of alveolar bone defects. Int J Oral Maxillofac implants 2010, 25; 153–162.
5. Lyford RH, Mills MP, Knapp Cl, Scheyer ET, Mellonig JT. Clinical evaluation of freeze dried block allografts for alveolar rigde augmentation. A case series. Int J Periodontics Restorative Dent 2003, 23;417–425.
6. Waasdorp J, Reynolds MA. Allogentic bone onlay grafts for alveolar rigde augementatioin a systematic rewiew. Int J Oral Maxillofac Implants 2010, 25;525–531.
7. Schlee M, Rothamel D. Ridge augmentation using costomized allogenic bone-blocks: Proof of concept and histological findings. Implant Dent. 2013 Jun;22(3);212–218
8. Spin-Neto R. Stavropoulos A, Coletti FL, Pereira LA, Marcantonio E jr., Wenzel A. Remodelling of cortical and corticocancellous fresh-frozen allogeneic block bone grafts – a radigraphic and histomorphometric comparison to autologous bone grafts. Clin Oral Impl Res. 2015 Jul;26(7)747–752.
9. Ahmadi RS, Sayar F, Rakhshan V, Iranpour B, Jahanbani J, Toumai A, Akhoondi N. Clinical and histomorphometric assesment of lateral alveolar rigde augmentation using a corticocancellous freeze-dried allograft bone-block. J Clin Oral Impl Res. 2017 Jun 43; (3): 202–210.
10. Jacotti M, Wang HL, Fu JH, Zamboni G, Bernardello F. Ridge augmentation with miniralized block allografts; Clinical and histological evaluation of 8 cases treated with the 3-dimensional block technique. Impl. Dent. 2012 Dec; 21(6);444–448.
Figure 17 Figure 18

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 26
11. Silva ER, Ferraz EP, Neto EC, Chaushu G, Chaushu L, Xavier SP. Volumetric stability of fresh frozen bone-blocks in atrophic posterior mandible augmentation. J oral Impl. 2017 Febr; 43(1)25–32.
12. Deluiz D, Santos Oliveira L, Ramoa Pines F, Reiner T, Amanda L, Nunes MA, Muniz Baretto Tinoco E. Incorporation and remodelling of bone-block allografts in the maxillary reconstruction: A randomized clinical trial. Clin. Impl. Dent relat. Res. 2017 Febr;19(1):180–194.
13. Jun CM, Yun JH. Three-dimensional bone regeneration of alveolar rigde defects using corticocancellous allogeneic block grafts: Histologic and immunohistochemical analysis. Int J Periodontics restorative Dent. 2016 Jan–Febr 26(1):75–81.
14. Motamedian SR, Khojasteh M, Khojasteh A. Succes rate of implants placed in autogenous bone-blocks versus allogenic bone-blocks: A systematic literature review. Ann Maxillofac surg. 2016 Jan–Jun; 6(1): 78–90.

27 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Implant-supported part-arch bridgeClinical case with two-year follow-up
A 63-year-old patient presented with the chief complaint of an unaesthetic, mobile anterior maxillary tooth due to periodontitis. He requested a permanent
fixed solution. As the patient had previously undergone periodontal therapy, we decided to maintain as many teeth as possible. Four teeth were planned for extraction (13/12/11/21) and another four were maintained (23/24/25/27).
Treatment plan
right sinus augmentation extraction of teeth 13/12/11/21 and simultaneous implant placement in 16/14/13/21/22
removable provisional prosthesis with delayed loading
definitive implant-supported part-arch bridge (two years of follow-up)
Introduction
Thanks to advances in the field of implant dentistry, we can offer our patients ambitious treatments including fixed prosthodontic restorations with reliable long-term prognoses. However, periodontal cases involving implants are often challenging. It can be difficult to know which treatment options to consider for partially edentulous periodontal patients.
This two-year follow-up clinical case shows an interesting compromise which allowed us both to maintain several natural teeth and restore the smile with a fixed implant-supported prosthesis.
Initial situation and diagnosis
A 63-year-old non-smoking patient presented for consultation. His chief complaint was an unaesthetic, mobile anterior maxillary tooth (Figures 1.1, 1.2 and 1.3). He had a removable partial denture in the maxilla, and requested a fixed alternative.
Although the patient was in good health, he had previously been diagnosed with chronic periodontitis, and his former dentist had carried out non-surgical periodontal therapy. His periodontal
status had been stable for six years, and he was receiving supportive therapy with a recall period of two visits per year.
The intraoral examination revealed a reduced but healthy periodontium. No probing pocket depth was present and there was no bleeding on probing. Overall, his plaque control was good. Teeth 13/12/11/21 showed an unfavourable prognosis with grade II mobility (Figure 2); tooth 27 showed no loss of attachment and no mobility. There was no posterior occlusion: teeth 14–17/22/26/34/35–37/44/46 were absent. Different options for maxillary rehabilitation were considered:
1. An implant-supported full-arch bridge from tooth 16 to tooth 26; immediate placement and loading
2. An implant-supported full-arch bridge from tooth 16 to tooth 26; delayed loading
3. An implant-supported part-arch bridge from tooth 16 to tooth 23; immediate placement and loading
4. An implant supported part-arch bridge from tooth 16 to tooth 23; delayed loading
One of the patient’s requests had been to proceed with the most conservative option. Because of this, and due to financial restrictions, he chose option 3: a part-arch bridge with delayed loading.
In the maxillary jaw, the mobile anterior teeth were planned for extraction (13/12/11/21); four others were maintained (23/24/25/27). The posterior occlusion was rehabilitated in the lower jaw by means of implants in sites 34/36 and 44.
Treatment plan
1. Right sinus lift2. Extraction of teeth 13/12/11/21; simultaneous
implant placement at 16/14/13/21/22; and implant placement in the lower jaw at 34/36/44
3. Removable provisional prosthesis with delayed loading in the maxilla
4. Definitive implant-supported part-arch bridge in the maxilla
5. Bridge from 34/35/36 and crown at 44 in the lower jaw
Sophie Dacquin, DDS, graduated from University of Reims Champagne-Ardenne in 2008. She obtained a masters degree in the field of Cells-Matrix Interactions from the University of Reims (2009) and has a certificate in periodontology from the faculty of dentistry at Université de Rennes (2011).
In 2014, Dr Dacquin received a degree in implantology from the University of Corsica, Corte. In 2014 she also opened a private practice in periodontology and implant dentistry.
Figure 1.1 Figure 1.2 Figure 1.3

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 28
Procedure
A CBCT scan allowed us to prepare for the surgery (Figure 3.1). The right posterior maxilla showed a lack of height; a right sinus lift was therefore performed with a lateral approach under local anaesthesia. The sinus was filled with Bio-Oss (Geistlich) and the bony window was covered with a Bio-Guide membrane (Geistlich). The flap was sutured with monocryl 5.0 (Ethicon).
The patient did not report any discomfort or post-operative problems. A radiographic control was performed after the surgery (Figure 3.2). Five months later, another CBCT scan allowed us to assess the quality of the sinus lift and plan the position of the maxillary implants (Figures 4.1–4.5).
After a further month, the surgical procedure was performed under local anaesthesia. Teeth 13/12/11/21 were extracted. A flap was raised from tooth 23 to 17, and five implants were placed at 16/14/13/21/22 according to the treatment plan (OsseoSpeed, Dentsply Implants). The flap was closed
Figure 2
Figure 3.1
Figure 4.3
Figure 3.2
Figure 4.2
Figure 4.1

29 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
with resorbable monocryl 5.0 sutures (Ethicon). A maxillary provisional removable prosthesis was provided at the same time.
Three implants were placed in the lower jaw, at sites: 34/36 and 44 (OsseoSpeed, Dentsply Implants). Oral hygiene and soft food dietary instructions were given to the patient (Figure 5). A clinical control was carried out ten days after the procedure. It showed healing around the abutments with inflammation (Figure 6).
Three months later, the mucosa around the abutments had healed uneventfully and an acceptable level of keratinised tissue was present (Figure 7.1). An impression of the implants was taken using a conventional pick-up technique. We were able to validate the impression by using copings mounted on a gypsum verification jig (Figures 7.2–7.3). This let us verify the accuracy of the impression and the passivity of the fixed prosthesis. The maxillomandibular relationship was recorded (Figure 7.4), and the tooth configuration was tried-in (Figure 7.5). A definitive part-arch bridge on an Atlantis Isus hybrid suprastructure was screwed on the implants in the maxilla (Figures 8.1–8.3).
In the mandible, a screw-retained crown on implant 44 and a cemented bridge on implants 34/36 with custom-designed Atlantis abutments were delivered. A final radiographic control was made (Figure 9).
Result
The patient was satisfied with the final aesthetic result (Figure 10). His main goal of increased function and preserving natural dentition had been achieved. At the two-year follow-up, bone and soft tissue were stable (Figure 11). Since receiving this treatment, the patient has returned twice a year for his supportive periodontal care and has continued to maintain effective plaque control (Figure 12).
Discussion
This clinical case presented a series of technical challenges which are worth discussing. In retrospect, the outcome of the sinus augmentation was far from ideal. The access point for the bony window was too far (distally) from tooth 13. The Schneiderian membrane was not raised enough on the medial wall of the sinus, which led to insufficient biomaterial filling the compartment. Additionally, the implants in the lower jaw were not placed in the planned position: the implant at 36 was not placed at bone level, and so its angulation could not allow accommodate a screw-retained prosthesis. This led to two major local risk factors for peri-implantitis: the lack of bone around the implant and the cemented bridge on the implant at 36.
Figure 6
Figure 7.1 Figure 7.2
Figure 5
Figure 4.4 Figure 4.5

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 30
Figure 7.3 Figure 7.4
Figure 7.5
Figure 8.1
Figure 8.2
Figure 8.3
On reflection, our approach for this case today would be different. Our experience and training would lead us to place a tissue-level implant with a screw-retained prosthesis. This would be especially effective in periodontally compromised patients.
The treatment options which were presented to the patient are also worthy of discussion. Each option had its advantages and disadvantages which must be taken into consideration in order to meet the patient’s expectations. Due to his periodontal status, the patient was at a higher risk of developing peri-implantitis, especially if implants were placed adjacent to natural teeth. A more aggressive approach to this case would have consisted of a full-mouth extraction, and placement of six dental implants for a full-arch implant-supported fixed prosthesis.
Nevertheless, the patient remains highly motivated and committed to effective plaque control, and comes for supportive periodontal care twice a year. For this reason, a more conservative approach for this demanding case was considered viable.

31 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Conclusion
In daily practice, clinicians are often faced with complex decisions. This is especially the case when treating patients who have a periodontal history. There is no single protocol or procedure which can improve the long-term prognosis of the intraoral situation of a partially edentulous periodontal patient. Nevertheless, supportive therapy can be a key factor for keeping these patients in good oral health.
Figure 10
Figure 12
Figure 9
Figure 11

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 32
How to create an inter-disciplinary practiceInterview with Tidu Mankoo, international lecturer and clinician
I n October, Inspyred caught up with Dr Tidu Mankoo, respected international lecturer and active clinician. Dr Mankoo recently sold his private practice in Windsor, so we asked him
about his practice; how he manages his world-class multidisciplinary team; and what is involved in treating complex cases.
What were your original goals for your practice
when you founded it?
I wanted to build a high-end, private practice outside of London. The idea was to focus on aesthetic and restorative dentistry, and from the beginning I knew I wanted to offer the best possible treatments. I have always believed in the value of quality, and I built this belief into my practice.
When I founded the practice it was a very exciting time. I had been on a few training courses about how to build a dental practice back in the 1980s. At that time, implant dentistry was not yet mainstream – it was new to a lot of people. But I wanted my practice to offer something different, so I started attending the Brånemark and a number of other courses in the 1980s and 90s. That was when people started seeing that we could treat many patients with more treatment alternatives which were simply not possible before. I have been placing and restoring implants for nearly 30 years now.
How has the practice evolved since then?
The practice has gone from strength to strength. Over the years our team has been able to collectively develop its skillset and gain expertise in a range of specialities, evolving into a very high-end inter-disciplinary practice.
One of the most obvious changes has been the kinds of cases we treat. We deal with a lot of aesthetic and restorative cases, and we tend to see patients with quite challenging dilemmas, which many dentists wouldn’t know how to treat. And because we have built our experience over such a long period, we can offer patients much more optimal and predictable solutions.
What have you learnt since founding the practice?
Where do I begin? I have learnt so much. But one thing comes to mind: always do what’s in the patient’s best interest in the long-term. Looking for short-term solutions or a ‘quick fix’ is never the answer. I have always believed this, so it isn’t really something which I have learnt – but it’s something I am reminded of every day.
Another thing which is hugely important is having a passion for excellence. When you start out
– whether you’re building your practice or getting started in the field – you must always be prepared to learn and develop. You can never think you know it all. And that’s good advice for life in general, I think.
What would you say is your practice’s core value?
One of our core values is to offer inter-disciplinary treatment approaches. To achieve this, I have spent years learning a range of skillsets. I personally carry out restorative, prosthodontic, periodontal and implant treatments. Many of the cases we treat need multiple therapies involving implant dentistry, periodontal therapy, restorative therapy and orthodontics.
But even though I had this broad skillset, I recognised very early on that I needed a team behind me to master all the disciplines. And I still know that I need help with other areas – particularly with orthodontics and endodontics.
We have a great team in place, and we work together with a team approach. This gives us a really wide range of experience and insights into many different styles of practising, which have been invaluable for developing the practice as a whole.
Some practices operate with one practitioner
who performs all procedures, whereas others
have multiple specialists under one roof handling
different areas. Which model do you think
works best?
In the UK it’s quite common for dentists to be general practitioners. There’s a tendency to have one dentist who does everything, as they are keen to keep the patient under their roof. This model can work well from a continuity of care perspective, but it also has its drawbacks. It is important to recognise when you can’t give your patient the optimum treatment – you’ve got to be able to admit when there’s someone else who might be able to do something more for the patient.
I don’t have a particularly strong opinion about which model works best. But I think at our practice we have a happy medium. Although we each have a broad skillset, we are specialised in different areas, and can refer patients among ourselves. This works well for us, and we get the best of both worlds.
In Europe, there are many practices which are
limited to only periodontics and implant dentistry.
Why do you think this isn’t very common in the UK?
As I mentioned, in the UK there’s a culture of general dentistry. There’s less of a focus on specialising than in Europe or even in the United States. I think this is because of the National Health

33 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Service (NHS) – there are more general practitioners than specialists, so people have a tendency to do everything rather than specialising in one thing, such as periodontics or implants.
But there certainly are a number of specialised practices limited to only perio or implant dentistry in the UK. So these kinds of practices can and do survive here – there are just fewer of them.
How do you approach complex cases? Is there any advice you could
give to clinicians?
That’s not something you can give a simple answer to. Of course, there’s a lot of advice already out there for how to approach complex cases. But what it really comes down to is: experience and proper treatment planning.
For me, the key is to have the skills and knowledge to recognise how to manage complex cases. The best approach is obviously to correctly diagnose the situation and plan your treatment accordingly. But being able to find that diagnosis in the first place relies on your experience as a clinician and how you have honed your skills. This is where it’s a huge help to have a multidisciplinary team behind you, because they will help you formulate an inter-disciplinary approach.
It is also very difficult to start treating complex cases unless your practice is specifically equipped to handle them. Treatment can take months – if not years – and there are often long interim periods between individual phases of treatment. So you have to be able to accommodate and manage the patients’ care in the long-term. And your practice must have the equipment and infrastructure to cater to patients’ specific needs.
One bit of advice I would give is to be ready to refer patients. It would be unwise for someone to take on a complex case before they are ready. So if you are in any doubt, you should refer the patient to someone with more experience. And that can be a learning experience in itself, even if you do not get to carry out the treatment. Just being in contact with these cases gives you something to think about and learn from.
In your experience, what would you say has had the biggest impact
on how you operate your practice?
For me, it was when I was learning from the masters. I attended many training courses early in my career, when implant dentistry was still gaining momentum.
And working with my peers in this way encouraged me to work at a higher level. It had a really profound impact on the way I work today: my colleagues and I would always be trying to push each other to step up our game and offer better treatment outcomes for patients. And that’s the way I work today – in the practice, our core aim is to offer the best treatment we can. So being involved in a lot of training courses and educational associations really shaped how I operate my practice now.
Do you have any take-home advice for
clinicians on how to optimise their daily
practises?
Be hungry to learn. Go on courses, expand your knowledge, build your experience, and learn from the best.
I know it can be difficult to find the time to read journals and stay up-to-date with clinical research. And being a lecturer as well as a practising clinician, I have to read even more than average to stay abreast of the current literature. But what works well for me is to quickly evaluate articles. I subscribe to a lot of journals, but do I read every one? No. What I do is read through the abstracts and be on the look-out for whatever piques my interest. Then I follow up on that – I’ll find the full article and read it in much more detail.
I would also encourage clinicians to use digital tools to their advantage. I read a lot online, using programmes like Papers for Mac which let me look up similar topics. There are also so many online databases and resources available – use them to dive in and find out what catches your interest, and delve further.
That’s why the annual EAO congresses are so good. They summarise key advances in the field in really informative lectures given by some of the biggest names in implant dentistry. You can absorb a huge amount of information and then follow it up with more reading of your own.
It’s my understanding that you just sold your practice. Was that a
difficult decision to make?
Yes, it was difficult to make that decision. But once I did, and once I had found the right buyer who I knew would continue with what I created, it has been very positive.
It also helps that I won’t be stopping here – I will still be involved with the practice and I’ll continue to be active as a clinician leading the clinical team. I’ll do what I can to help the practice develop and grow.
What are your next steps? Do you have any ambitions you still hope
to achieve?
I am also involved in teaching, so I’m looking forward to continuing with this. At the moment I do anything between two and five days a month. I’ll stay involved with that, and keep attending conferences regularly to stay abreast of the current literature and new developments. I’m looking forward to being able to devote even more of my time to this, and to improving my skills.

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 34
Minimally invasive extraction with the Benex systemCase report involving a patient at risk of medication-related osteonecrosis of the jaw
T his case involves minimally invasive extraction procedures in a patient who was receiving anti-vascular endothelial growth factor (anti-VEGF) targeted therapy
as part of his cancer treatment. Tooth extraction in patients receiving this kind of therapy puts them at risk of medication-related osteonecrosis of the jaw (MRONJ). Extraction may result in exposed bone caused by reduced blood supply. The Benex extraction system was used to preserve bone and soft tissue and minimise postoperative complications.
Case presentation
A 69-year-old man was referred to the Oral Surgery Department of the Birmingham Dental Hospital and School (UK) for the extraction of retained roots in the maxilla. He had a history of pain and infection related to the retained roots. He was using a removable denture, with which he was satisfied. He was anxious about extraction due to his medical condition. He had been diagnosed with adenocarcinoma of the rectosigmoid with liver and lung metastases 10 years ago; he was receiving palliative chemotherapy which included anti-vascular endothelial growth factor, an anti-angiogenic agent.
An extraoral examination of the patient did not show any abnormalities or pathology. Intraoral examination revealed erythema (redness) of soft tissues around the roots of 13, 14, 23 and 24, suggesting inflammation. Radiological examination showed retained roots with periapical radiolucency and no sign of root fillings (Figure 1).
Diagnosis
The retained roots of 13, 14, 23 and 24 were unrestorable and hopeless, showing chronic apical periodontitis, and required extraction. Due to his medication, the patient was at risk of MRONJ, and he consented to a treatment plan involving extraction under local anaesthesia over two visits.
Planning
1. Consultation with oncologist regarding a ‘drug holiday’
2. Blood test including full blood count and clotting screen, no more than five days before extraction
3. Five-day course of antibiotics starting two days before surgery
The oncologist advised that the patient continued anti-angiogenic medication and commenced treatment four weeks after his last course of chemotherapy. Blood test results were normal, and treatment was performed with conventional extraction on the right side and extraction with the Benex system (Figure 2) on the left side.
Follow-up appointments were scheduled every four weeks to assess soft mucosal coverage, which is the measure of a successful outcome of this procedure.
Aim
Our aim was to clinically evaluate healing times of the extraction socket with conventional extraction and the Benex system.
Procedure
Extraction was performed using a minimally invasive approach. The Benex system was used to provide a less painful extraction procedure and preserve bone and soft tissue. Root extraction forceps and luxators can put pressure on the socket wall; Benex instruments do not come into contact with the extraction socket, as the root is removed along the axis with the instrument.
The first round of extractions (retained roots 13 and 14) was performed using a conventional technique. The second round (retained roots 23 and 24) was performed with Benex 12 weeks after the first procedure (after observation of mucosal coverage of extraction socket). Figures 3, 4 and 5 present clinical views before and after extraction.
Conventional procedure Benex system
Local anaesthetic Local anaesthetic
� immobilisation with luxator � preparation of roots 23 and 24 with drill
� insertion of screw according to the size of the root
� impression with alginate
Extraction with forceps Extraction with Benex system
Spontaneous haemostasis Spontaneous haemostasis
15 min 25 min
Results
In our practice the soft mucosal coverage of extraction sockets in patients at risk of MRONJ is the measure of a successful outcome.
In this case, the healing process for the conventional extraction was observed after 12 weeks; with the Benex system, healing was observed after 8 weeks. The four-week clinical evaluation revealed the presence of exposed bone where the conventional method had been used, whereas the extraction socket was almost healed where the Benex system had been used (Figure 6).
Right, Figure 1: Periapical radiograph of 23 and 24 retained roots.
Katarzyna
Gurzawska, DDS, PhD, graduated from the Medical University of Lodz (MUL), Poland in 2006. She has a PhD in implant nanotechnology (University of Copenhagen, 2013) and a PhD in 3D modelling and biomechanics (MUL, 2014). In 2014 she received the Marie Sklodowska-Curie Fellowship at Charite University, Berlin. Member of the EAO Junior Committee, and Academic Clinical Lecturer at the University of Birmingham, UK (4-year Oral Surgery Registrar Training Post).
Harlene Kaur, BDS, MSc, graduated from the School of Dentistry, University of Birmingham (UK) in 2007 and completed her Masters in Oral Surgery at the University of Central Lancashire (UK) in 2015. In 2016, Harlene commenced a 3-year Oral Surgery Registrar Training Post as an Academic Clinical Fellow at the University of Birmingham.

35 | Volume 5, Issue 2: Winter 2017 | Inspyred: The alternative EAO voice
Discussion
Over the past several years, anti-VEGF targeted therapies have been incorporated into advanced cancer treatment paradigms (Pal, Figlin et al. 2010). Th ese medications inhibit blood vessel formation within tumours, thereby reducing metastasis. However, anti-angiogenic agents may also hinder bone healing aft er tooth extraction and are considered risk factors for MRONJ.
MRONJ, according to guidelines from a position paper published by the American Association of Oral and Maxillofacial Surgeons (AAOMS) in 2014 (Ruggiero, Dodson et al. 2014), may occur in patients with:
1. Current or previous treatment with anti-resorptive or anti-angiogenic agents
2. Exposed bone or bone which can be probed through an intraoral or extraoral sinus tract in the maxillofacial region which has persisted for more than 8 weeks
3. No history of radiation therapy to the jaws or obvious metastatic disease of the jaws
Th e AAOMS propose management strategies for preventing MRONJ, and suggest that procedures which involve direct osseous injury should be avoided (Ruggiero, Dodson et al. 2014).
Patients at risk of MRONJ and diabetes (for whom bone loss must be minimised, due to the risk of complications arising during healing) are suitable candidates for the Benex system. Teeth with a lack of apical pathology and minimal structure for restoration could also be considered suitable for extrusion using the Benex system.
Conclusion
Th e Benex extraction system has the potential to off er reduced healing times and could be consider as a viable treatment option to reduce risk factors for MRONJ. However, in our experience the method has a longer procedure time compared with conventional tooth extraction. A randomised controlled trial including clinical and radiological parameters describing soft and hard tissue healing is necessary to determine healing times for extractions using the Benex system as a method for MRONJ prevention.
References
Pal, S. K., et al. (2010). "Deciphering the anticancer mechanisms of sunitinib." Cancer Biology & Th erapy 10(7): 712–714.
Ruggiero, S. L., et al. (2014). "American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw–2014 update." J Oral Maxillofac Surg 72(10): 1938–1956.
Figure 2: Benex system. Figure 3: Clinical view before extraction.
Figure 4: Extraction socket.
Figure 5: Root of 23 after extraction.
Figure 6: Extraction socket after four weeks.

Inspyred: The alternative EAO voice | Volume 5, Issue 2: Winter 2017 | 36
EAO Consensus Conference7–10 February 2018, Pfäffikon, Switzerland
5th EAO Consensus Conference
7–10 February 2018 Pfäffikon, Switzerland
www.eao.org
S ince 2006, the EAO has held a Consensus Conference every three years. These conferences bring together a
faculty of 30–60 specialists to discuss and review a range of topics in implant dentistry. The aim of the conferences is to identify what problems are currently facing practitioners, and to shed a light on the solutions. They are exclusively financed by the EAO without support from industry.
Results will be published with open access in a supplement of Clinical Oral Implants Research, which will also be distributed to delegates during the EAO's annual meeting in Vienna in October 2018.
Cc
EAO CONSENSUSCONFERENCE 2015
EAO CONSENSUSCONFERENCE 2012
EAO CONSENSUSCONFERENCE 2009
EAO CONSENSUSCONFERENCE 2006
Published by:European Association for Osseointegration,38 rue Croix des Petits Champs,75001 Paris, FranceEmail: [email protected]: www.eao.org/inspyred
European Association for Osseointegration
europeanassociationforosseointegration
eao_association
The views expressed in the articles published in this magazine are those of the author(s) and do not necessarily represent EAO’s position on these issues. EAO cannot be held liable for any statements expressed therein.
Inspyred is designed and produced by www.publishingbureau.co.uk