Embed Size (px)
Citation preview

Reinhard Busse, Prof. Dr. med. MPH FFPH FG Management im Gesundheitswesen, Technische Universität Berlin
(WHO Collaborating Centre for Health Systems Research and Management) &
European Observatory on Health Systems and Policies
Die GKV, der Binnenmarkt und
grenzüberschreitende
Patientenversorgung
Management im Gesundheitswesen Krankenversicherung und Leistungsanbieter
Informationen zur Klausur
• Dauer: 90 Minuten
• Umfang: Alle Themen der Vorlesung
• Termin: Do. 12.2.2015, Raum EB107, 12 Uhr c.t.
• Klausurnote geht zu 50 % in die Modulnote ein
• Musterklausur im Downloadbereich verfügbar
• Klausur muss nicht bestanden werden um das Modul zu
bestehen (Kompensationsregelung)
• Klausurwiederholung: 05./11.02. (Fragen vorbereiten)
Direkte
Ergebnisse:
Qualität,
Zufrieden-
heit Strukturen
Patienten
Prozesse
Gesundheit
der
Bevölkerung
Gesund-
heits-
“Outcome“
Andere Politikbereiche
Ernährung/ Landwirtschaft
Umwelt
Gesundheitssystem Finanzielle
Ressourcen
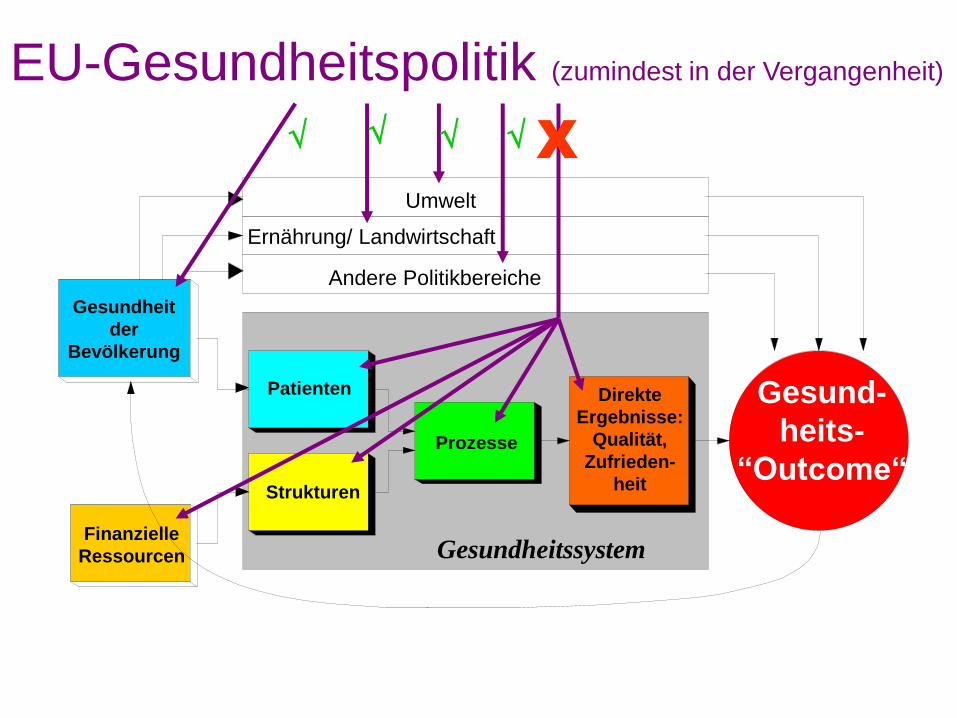
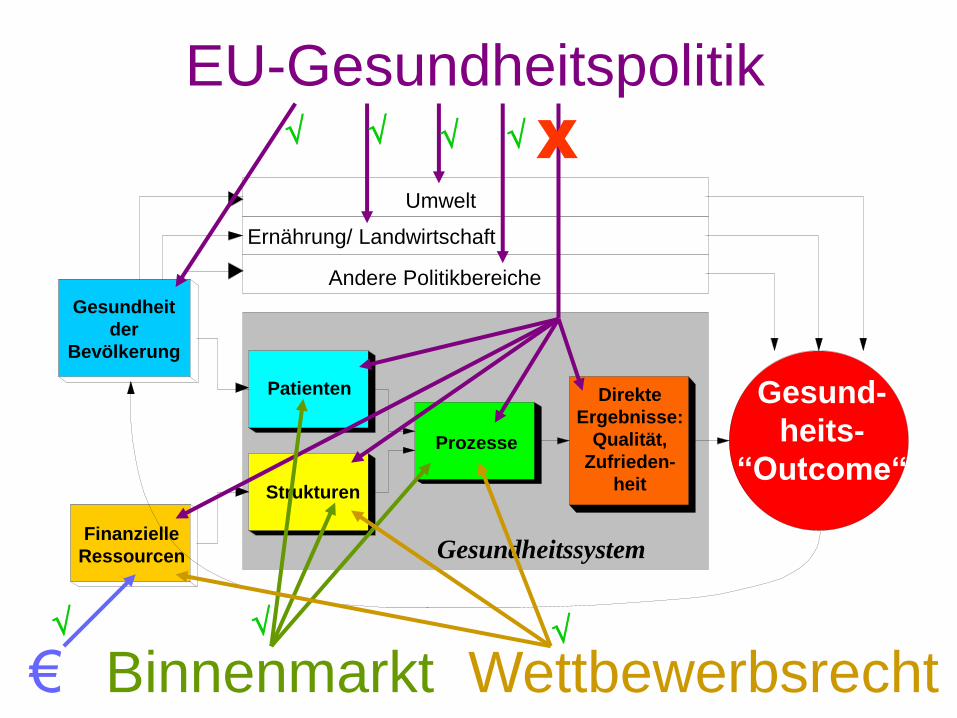
EU-Gesundheitspolitik (zumindest in der Vergangenheit)
X
ABER: • Artikel 152(5) bezog sich nur auf Public Health-
Maßnahmen
• EU-Eingriffe in Gesundheitssysteme erfolgen
aber sehr wohl durch u.a.
- Arbeitsrecht (Arbeitszeiten im Krankenhaus!)
- Wettbewerbsrecht
- Binnenmarktsrecht mit 4 Freiheiten für
Personen, Waren, Dienstleistungen und Kapital
ABER: • Artikel 152(5) bezog sich nur auf Public Health-
Maßnahmen
• EU-Eingriffe in Gesundheitssysteme erfolgen
aber sehr wohl durch u.a.
- Arbeitsrecht (Arbeitszeiten im Krankenhaus!)
- Wettbewerbsrecht
- Binnenmarktsrecht mit 4 Freiheiten für
Personen, Waren, Dienstleistungen und Kapital
= direkter Einfluss
innerhalb des Landes
= direkter Einfluss nur auf
grenzüberschreitende Personen-
und Dienstleistungsströme
Das Kernproblem bei
Grenzüberschreitung – egal ob von
Gesundheitspersonal, Patienten, Waren
• Gilt das Recht des Herkunftslandes?
• Gilt das Recht des Landes, in dem gearbeitet
wird bzw. die Leistung erbracht wird?
• Soll/ muss es ein einheitliches EU-Recht
geben?
Das Kernproblem bei
Grenzüberschreitung – egal ob von
Gesundheitspersonal, Patienten, Waren
Konkret:
• Welche Anforderungen an die Qualifikation gelten für eine polnische Krankenschwester, die in Deutschland arbeiten will?
• Welches Recht wird angewandt, wenn ein GKV-Versicherter einen Arzt in Slubice kontaktiert?
• Und wenn dieser einen Hausbesuch in Frankfurt/ Oder macht?
Die EU kennt keine einheitliche Regelung
• Sog. sektorale Richtlinien für Ärzte (einschl. 52 Fach-
arztdisziplinen), Pflegekräfte, Zahnärzte, Hebammen ...
regeln gegenseitige Anerkennung auf Grundlage von
Minimalstandards (z.B. Medizinstudium mind. 5 J. und
5500 Stunden)
• Aber: Instrument ist relativ starr, da Veränderungen im
Curriculum und neue Sub-Spezialisierungen in
Richtlinie eingearbeitet werden müssen
• Sog. allgemeine Richtlinien (für alle anderen Berufe)
sehen die Möglichkeit der Anerkennungsperiode, den
Erwerb von Zusatzausbildungen oder eine Prüfung vor
Die EU kennt keine einheitliche Regelung
harmonisiert in Richtlinie 2005/36 über die
Anerkennung von Berufsqualifikationen
(besondere Bestimmungen für Ärzte,
Krankenpfleger etc. in Anhängen geregelt)
Lösung: EU Verordnung 1408/71 (seit 2010 ersetzt durch 883/2004)
- die aber zunehmend als
ungenügend betrachtet wurde,
wie die Fälle vor dem
Europäischen Gerichtshof
(EuGH) und der
Konsultationsprozess zeigten
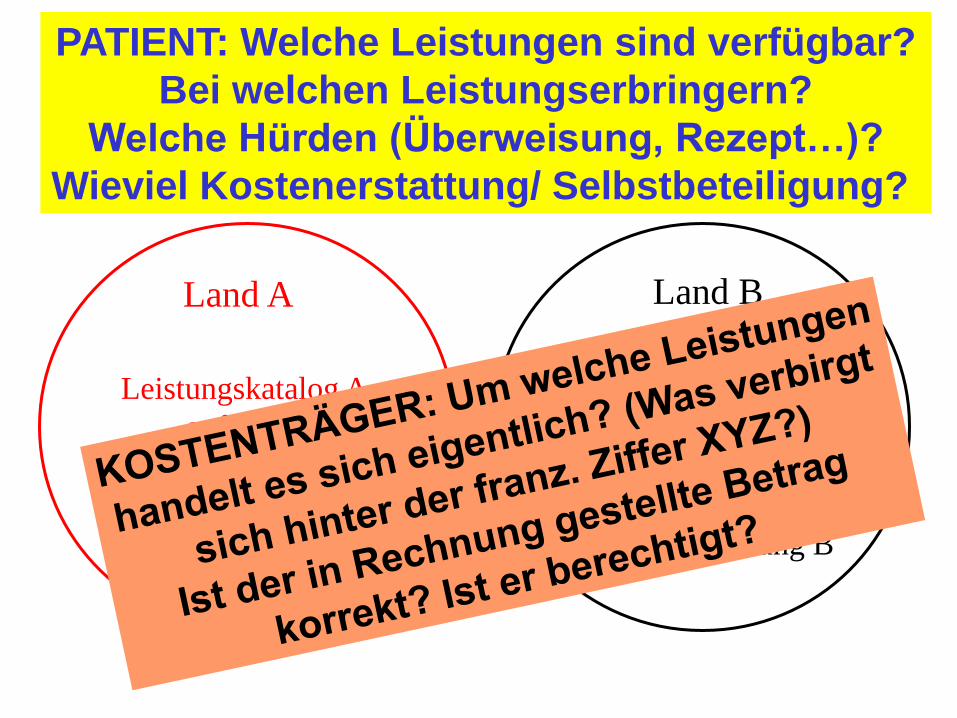
Land A Land B
Leistungskatalog A
aufgrund
Taxonomie A
und
Gebührenordnung A
Leistungskatalog B
aufgrund
Taxonomie B
und
Gebührenordnung B
PATIENT: Welche Leistungen sind verfügbar?
Bei welchen Leistungserbringern?
Welche Hürden (Überweisung, Rezept…)?
Wieviel Kostenerstattung/ Selbstbeteiligung?
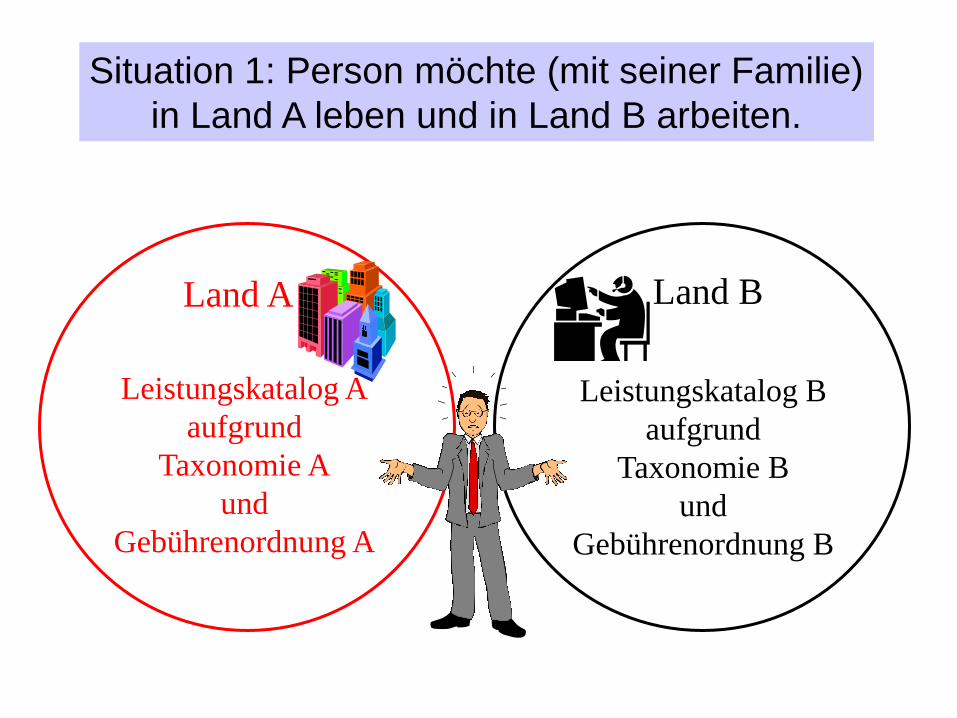
Land A Land B
Leistungskatalog A
aufgrund
Taxonomie A
und
Gebührenordnung A
Leistungskatalog B
aufgrund
Taxonomie B
und
Gebührenordnung B
Situation 1: Person möchte (mit seiner Familie)
in Land A leben und in Land B arbeiten.
Lösung: Schein E106
• Versicherung im Land des Arbeitsverhältnisses (Land B)
• Ermöglicht Grenzarbeitnehmern und ihren Angehörigen, Gesundheitsversorgung nach ihrer Wahl in beiden Ländern zu den dortigen Konditionen in Anspruch zu nehmen
• Patient präsentiert E106 dem Leistungserbringer im Land A (und die Versicherungskarte im Land B)
• Sozialversicherungsträger in B vergütet die Leistungserbringer in A anhand der dort geltenden Gebührenordnung
Land A Land B
Leistungskatalog A
aufgrund
Taxonomie A
und
Gebührenordnung A
Leistungskatalog B
aufgrund
Taxonomie B
und
Gebührenordnung B
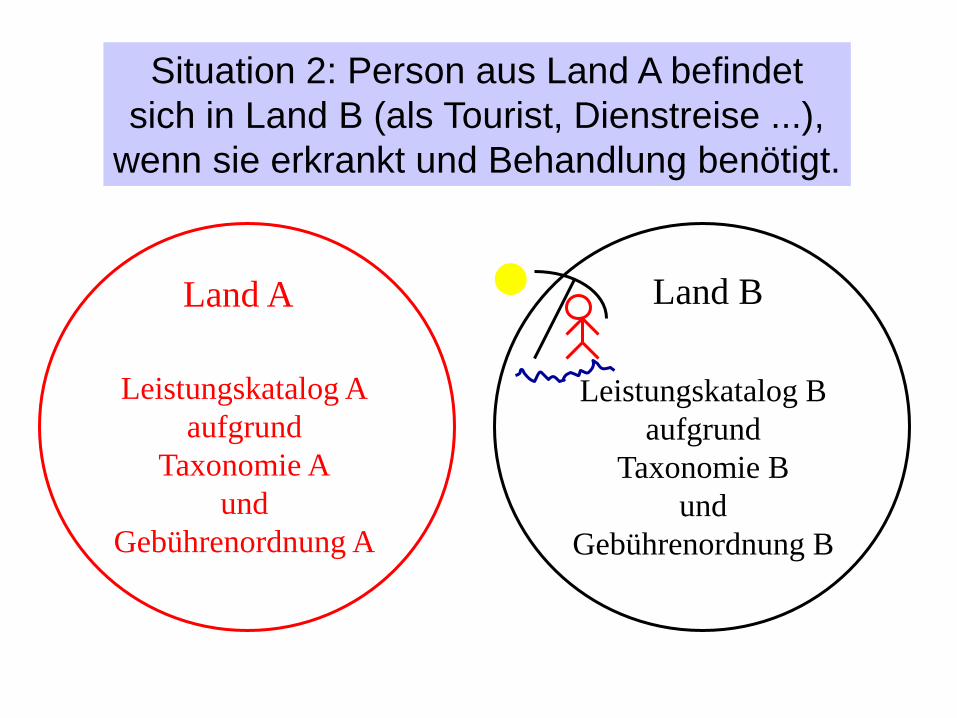
Situation 2: Person aus Land A befindet
sich in Land B (als Tourist, Dienstreise ...),
wenn sie erkrankt und Behandlung benötigt.
Lösung: Schein E111
• Patient nimmt E111 von seinem Sozialversicher im Land
A und gibt ihm dem Leistungserbringer im Land B
• E111 berechtigt zu Leistungen im Land B, die dort im
Leistungskatalog sind und die unmittelbar notwendig
sind (zu Zuzahlungen etc. wie im Land B)
• Sozialversicherer in A vergütet das Land B (via die
nationalen Verbindungsbüros) – sofern man nicht
gegenseitig darauf verzichtet („waiver agreement“)
• CAVE: Land B muss sicher stellen, dass das Geld auch
die Leistungserbringer erreicht
Land A Land B
Leistungskatalog A
aufgrund
Taxonomie A
und
Gebührenordnung A
Leistungskatalog B
aufgrund
Taxonomie B
und
Gebührenordnung B
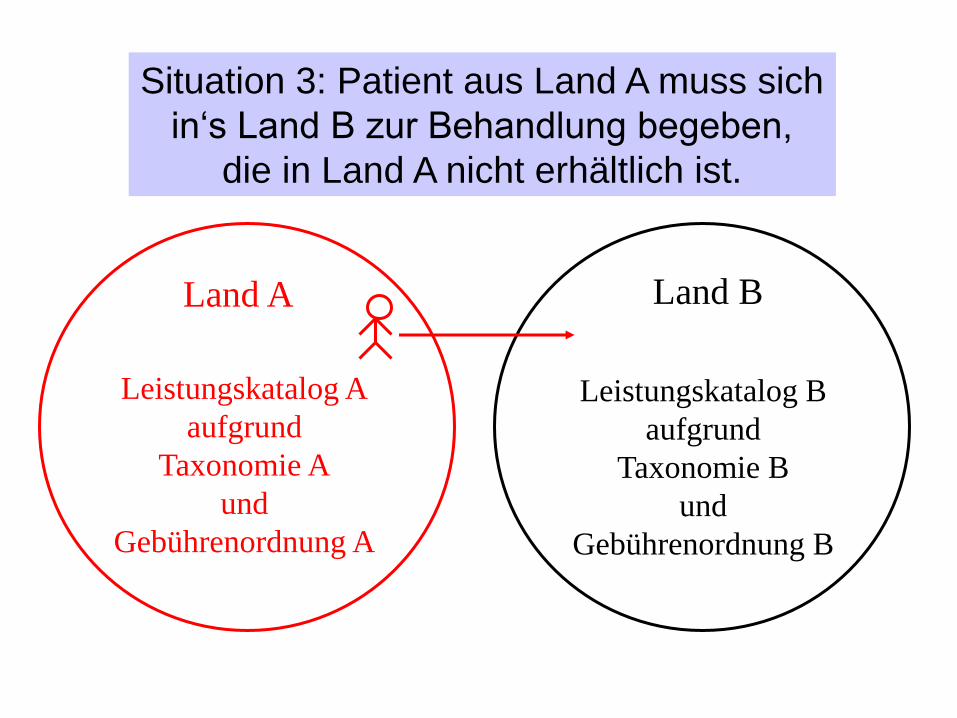
Situation 3: Patient aus Land A muss sich
in‘s Land B zur Behandlung begeben,
die in Land A nicht erhältlich ist.
Lösung: Schein E112
• Patient beantragt bei seinem
Sozialversicherungsträger im Land A, sich in
Land B zur Behandlung zu begeben
• E112 berechtigt den Patienten zu spezifischen
Leistungen im Land B (zu Konditionen wie in
Land A)
• Sozialversicherer in A vergütet den
Leistungserbringer im Land B aufgrund der
dortigen Gebührenordnung
Land A Land B
Leistungskatalog A
aufgrund
Taxonomie A
und
Gebührenordnung A
Leistungskatalog B
aufgrund
Taxonomie B
und
Gebührenordnung B
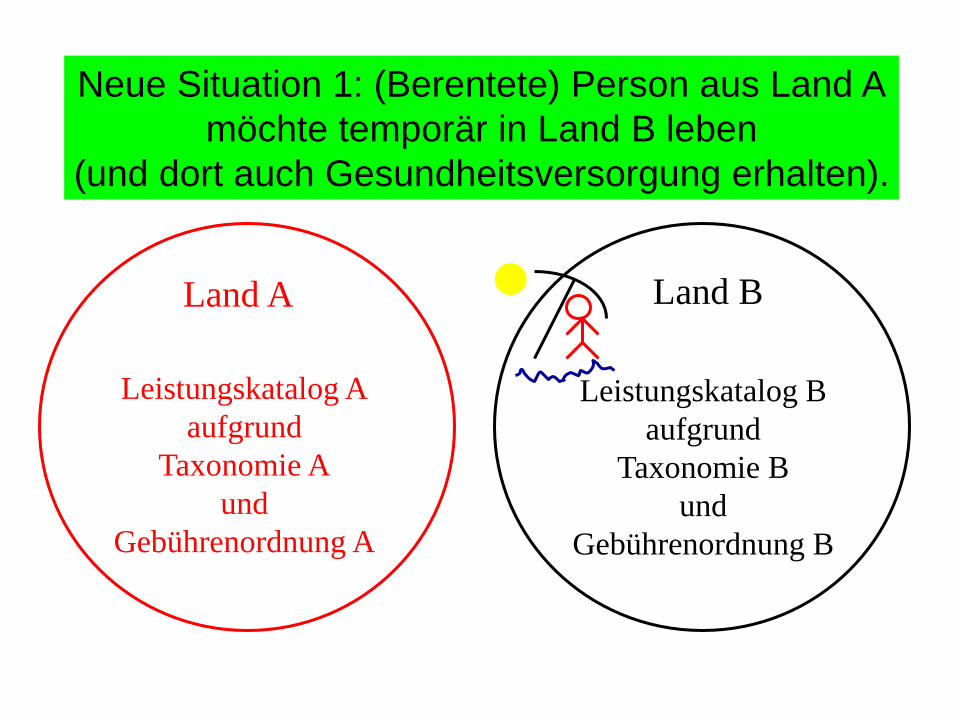
Neue Situation 1: (Berentete) Person aus Land A
möchte temporär in Land B leben
(und dort auch Gesundheitsversorgung erhalten).
Lösung: Erweiterung von E111
• (Berentete) Person erhält alle medizinisch notwendigen
Leistungen, die sich im Leistungskatalog von B befinden
(und nicht nur die unmittelbar notwendigen; unter
Verordnung 883/2004 auf alle Personen ausgeweitet)
• Sozialversicherer in A vergütet das Land B (via die
nationalen Verbindungsbüros) – sofern man nicht
gegenseitig darauf verzichtet („waiver agreement“)
• CAVE: Land B kann u.U. großzügiger als Land A sein
(z.B. keine Zuzahlungen für Ältere in Spanien)
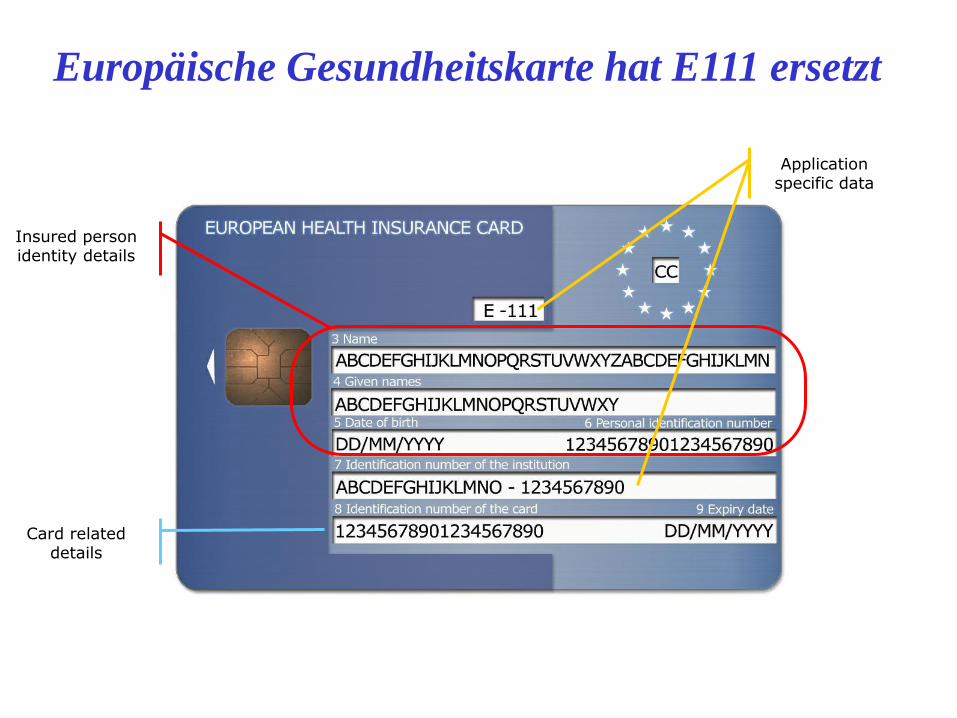
Insured person identity details
Application specific data Application
specific data
Card related details
Europäische Gesundheitskarte hat E111 ersetzt
Land A Land B
Leistungskatalog A
aufgrund
Taxonomie A
und
Gebührenordnung A
Leistungskatalog B
aufgrund
Taxonomie B
und
Gebührenordnung B
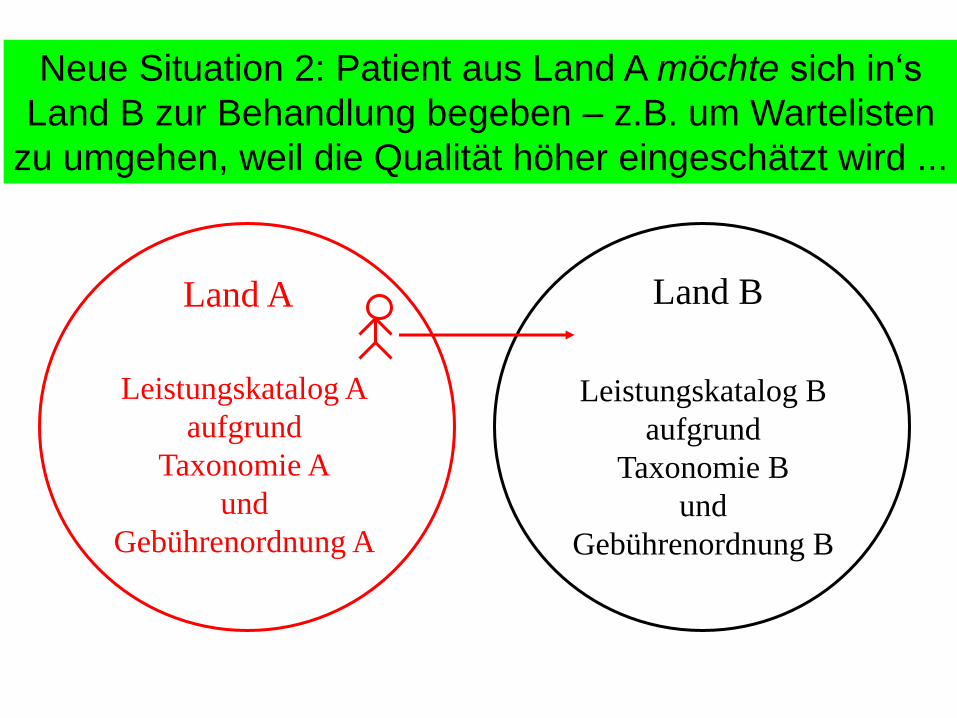
Neue Situation 2: Patient aus Land A möchte sich in‘s
Land B zur Behandlung begeben – z.B. um Wartelisten
zu umgehen, weil die Qualität höher eingeschätzt wird ...
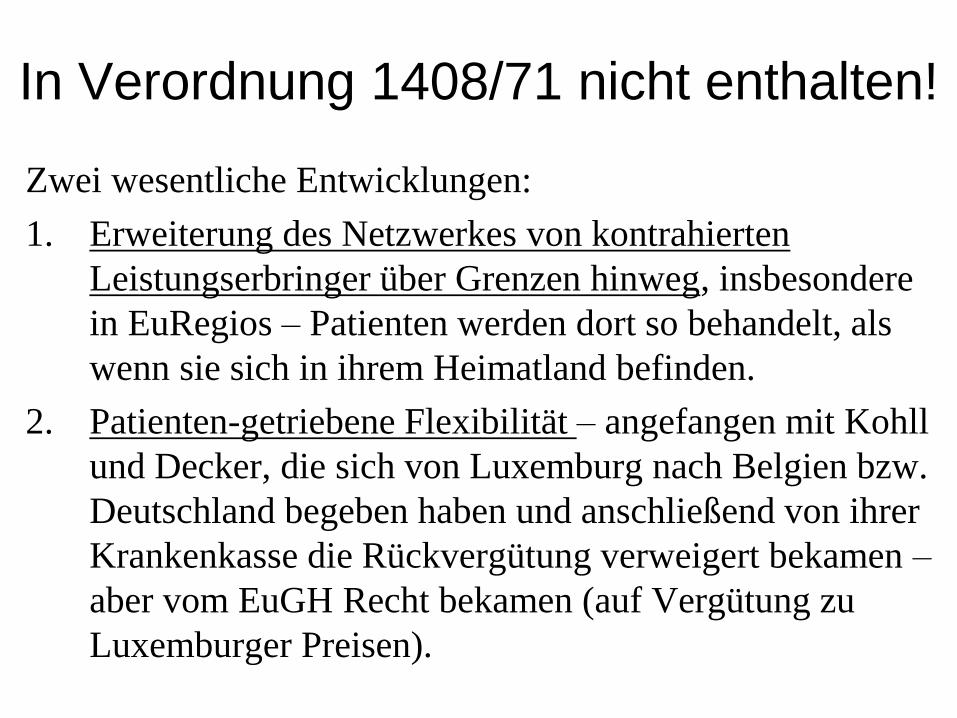
In Verordnung 1408/71 nicht enthalten!
Zwei wesentliche Entwicklungen:
1. Erweiterung des Netzwerkes von kontrahierten
Leistungserbringer über Grenzen hinweg, insbesondere
in EuRegios – Patienten werden dort so behandelt, als
wenn sie sich in ihrem Heimatland befinden.
2. Patienten-getriebene Flexibilität – angefangen mit Kohll
und Decker, die sich von Luxemburg nach Belgien bzw.
Deutschland begeben haben und anschließend von ihrer
Krankenkasse die Rückvergütung verweigert bekamen –
aber vom EuGH Recht bekamen (auf Vergütung zu
Luxemburger Preisen).
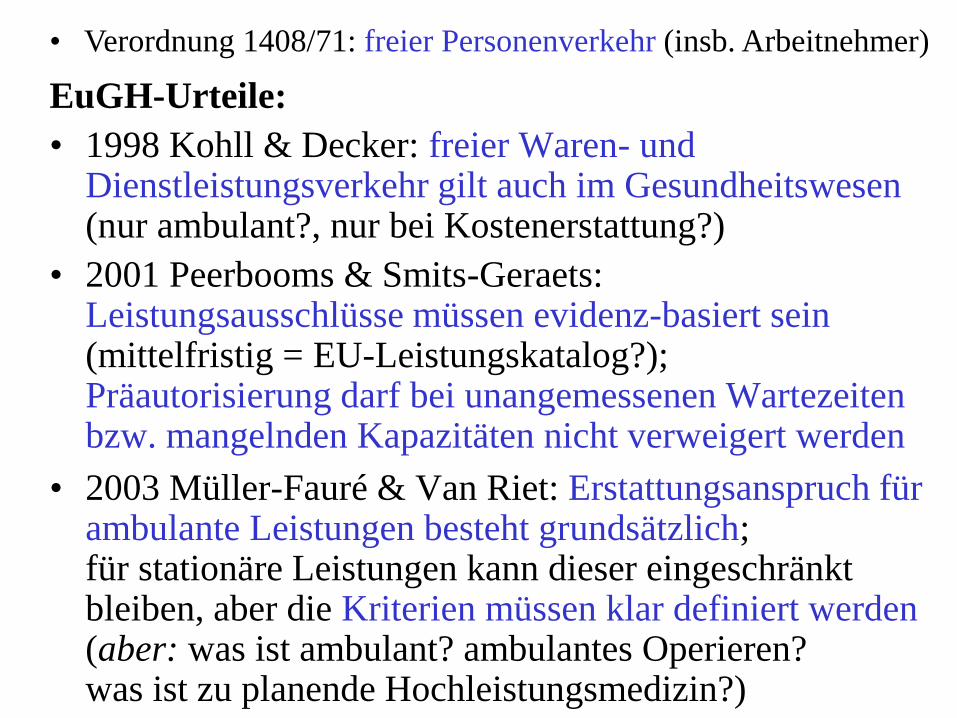
EuGH-Urteile:
• 1998 Kohll & Decker: freier Waren- und Dienstleistungsverkehr gilt auch im Gesundheitswesen (nur ambulant?, nur bei Kostenerstattung?)
• Verordnung 1408/71: freier Personenverkehr (insb. Arbeitnehmer)
EuGH-Urteile:
• 1998 Kohll & Decker: freier Waren- und Dienstleistungsverkehr gilt auch im Gesundheitswesen (nur ambulant?, nur bei Kostenerstattung?)
• 2001 Peerbooms & Smits-Geraets: Leistungsausschlüsse müssen evidenz-basiert sein (mittelfristig = EU-Leistungskatalog?); Präautorisierung darf bei unangemessenen Wartezeiten bzw. mangelnden Kapazitäten nicht verweigert werden
• Verordnung 1408/71: freier Personenverkehr (insb. Arbeitnehmer)
• 2003 Müller-Fauré & Van Riet: Erstattungsanspruch für ambulante Leistungen besteht grundsätzlich; für stationäre Leistungen kann dieser eingeschränkt bleiben, aber die Kriterien müssen klar definiert werden (aber: was ist ambulant? ambulantes Operieren? was ist zu planende Hochleistungsmedizin?)
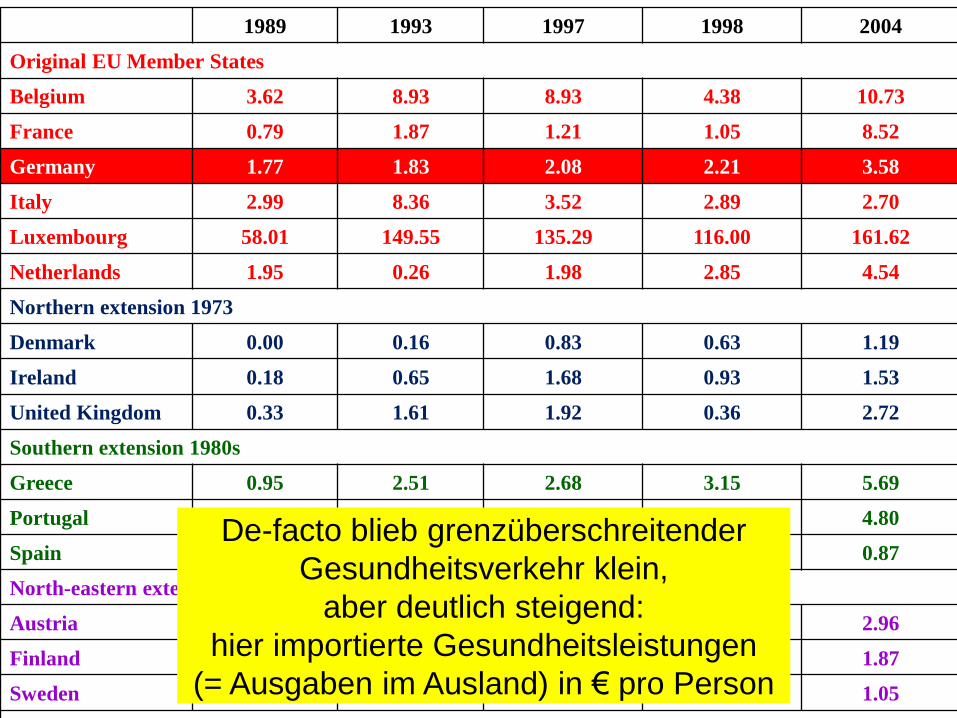
1989 1993 1997 1998 2004
Original EU Member States
Belgium 3.62 8.93 8.93 4.38 10.73
France 0.79 1.87 1.21 1.05 8.52
Germany 1.77 1.83 2.08 2.21 3.58
Italy 2.99 8.36 3.52 2.89 2.70
Luxembourg 58.01 149.55 135.29 116.00 161.62
Netherlands 1.95 0.26 1.98 2.85 4.54
Northern extension 1973
Denmark 0.00 0.16 0.83 0.63 1.19
Ireland 0.18 0.65 1.68 0.93 1.53
United Kingdom 0.33 1.61 1.92 0.36 2.72
Southern extension 1980s
Greece 0.95 2.51 2.68 3.15 5.69
Portugal 0.82 3.76 6.81 7.00 4.80
Spain 0.33 1.48 1.03 1.11 0.87
North-eastern extension 1995
Austria - - 0.48 1.87 2.96
Finland - - 0.49 0.52 1.87
Sweden - - 0.65 0.96 1.05
Eastern extension 2004
Cyprus - - - - 0.00
Czech Republic - - - - 0.02
Estonia - - - - <0.01
Hungary - - - - <0.01
Latvia - - - - <0.01
Lithuania - - - - <0.01
Malta - - - - 0.00
Poland - - - - <0.01
Slovakia - - - - 0.01
Slovenia - - - - 0.14
AVERAGE 1.31 2.95 2.37 1.99 2.59
De-facto blieb grenzüberschreitender
Gesundheitsverkehr klein,
aber deutlich steigend:
hier importierte Gesundheitsleistungen
(= Ausgaben im Ausland) in € pro Person
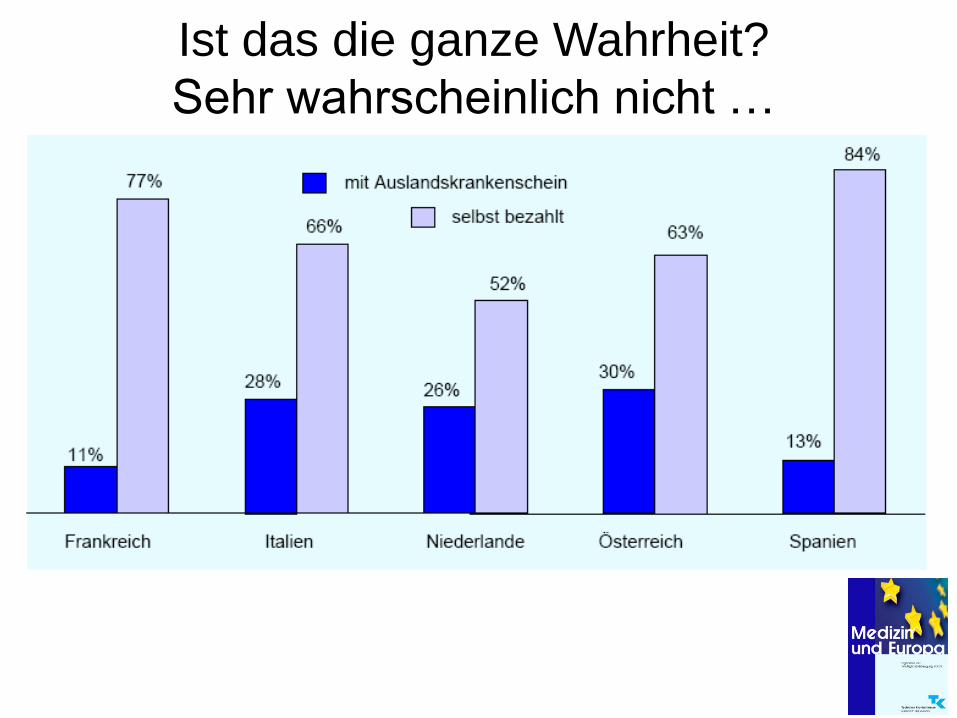
Ist das die ganze Wahrheit?
Sehr wahrscheinlich nicht …
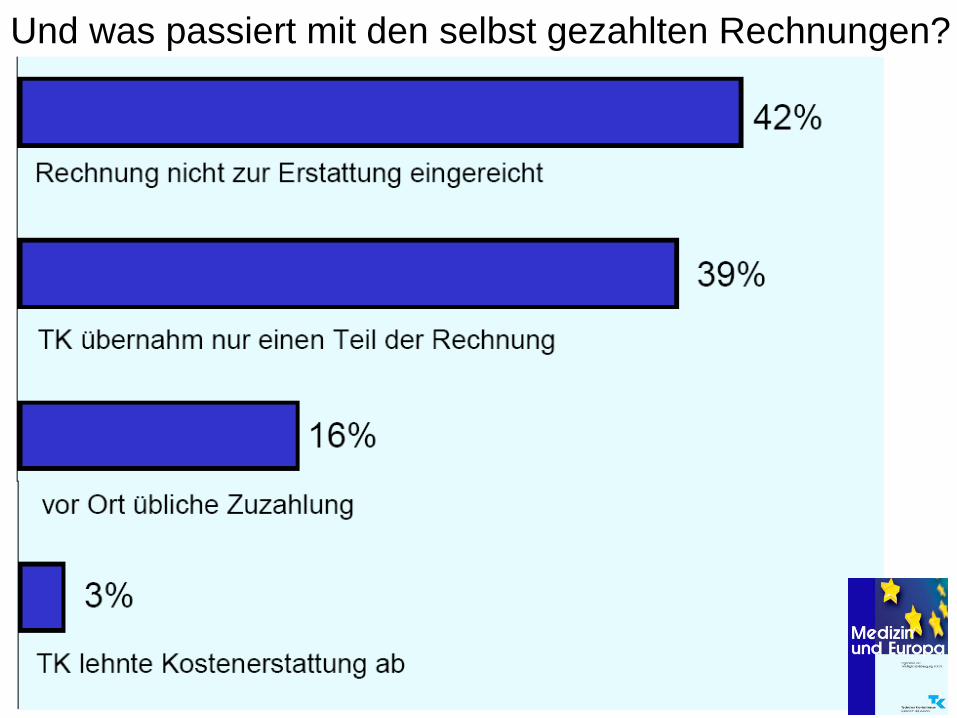
Und was passiert mit den selbst gezahlten Rechnungen?
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50
0.55
0.60
0.65
0.70
0.75
0.80
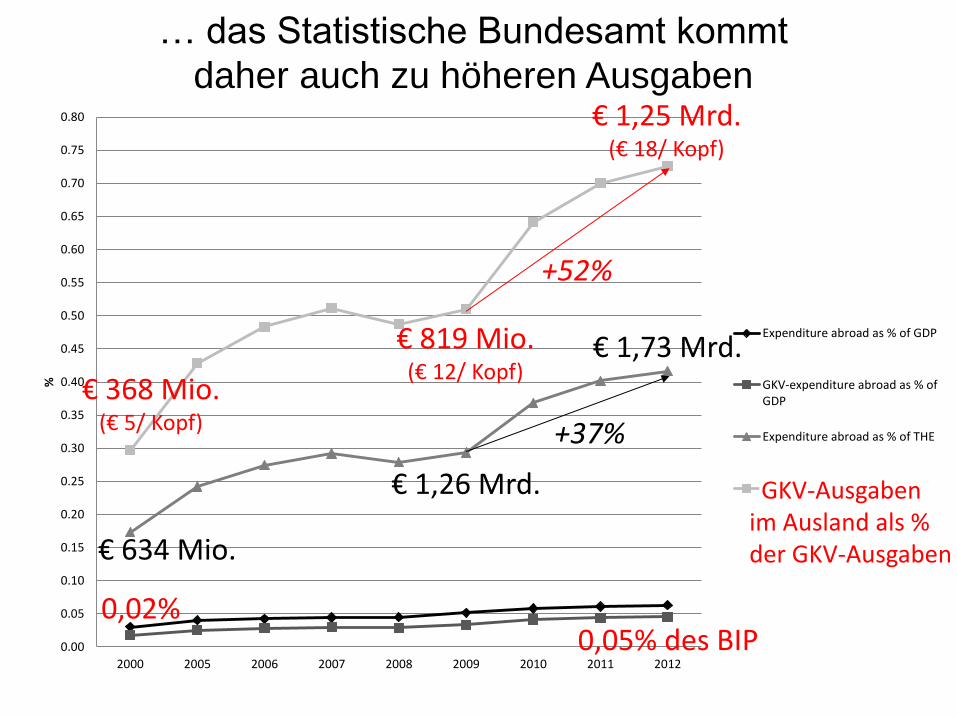
2000 2005 2006 2007 2008 2009 2010 2011 2012
%
Expenditure abroad as % of GDP
GKV-expenditure abroad as % ofGDP
Expenditure abroad as % of THE
GKV expenditure abroad as % ofGKV-expenditure
€ 634 Mio.
€ 368 Mio. (€ 5/ Kopf)
€ 1,73 Mrd.
€ 1,25 Mrd. (€ 18/ Kopf)
€ 1,26 Mrd.
€ 819 Mio. (€ 12/ Kopf)
0,05% des BIP 0,02%
GKV-Ausgaben im Ausland als % der GKV-Ausgaben
Entwicklung der Ausgaben im Ausland
+52%
+37%
… das Statistische Bundesamt kommt
daher auch zu höheren Ausgaben
Direkte
Ergebnisse:
Qualität,
Zufrieden-
heit Strukturen
Patienten
Prozesse
Gesundheit
der
Bevölkerung
Gesund-
heits-
“Outcome“
Andere Politikbereiche
Ernährung/ Landwirtschaft
Umwelt
Gesundheitssystem Finanzielle
Ressourcen
EU-Gesundheitspolitik X
Wettbewerbsrecht Binnenmarkt €
“At European level, health
services have to adapt to
market rules, while at
national level, health
services are seen as part of
a social model.
To overcome this situation
and to ensure the social
status of health services,
we need – possibly
paradoxically – to develop
a European health policy.“
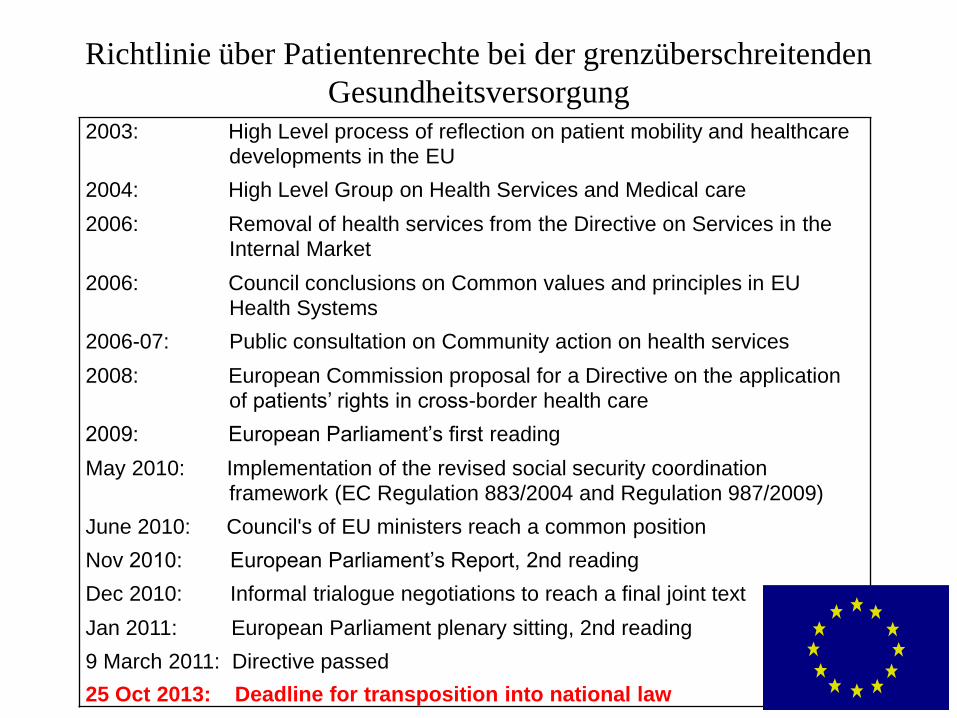
Richtlinie über Patientenrechte bei der grenzüberschreitenden
Gesundheitsversorgung 2003: High Level process of reflection on patient mobility and healthcare
developments in the EU
2004: High Level Group on Health Services and Medical care
2006: Removal of health services from the Directive on Services in the
Internal Market
2006: Council conclusions on Common values and principles in EU
Health Systems
2006-07: Public consultation on Community action on health services
2008: European Commission proposal for a Directive on the application
of patients’ rights in cross-border health care
2009: European Parliament’s first reading
May 2010: Implementation of the revised social security coordination
framework (EC Regulation 883/2004 and Regulation 987/2009)
June 2010: Council's of EU ministers reach a common position
Nov 2010: European Parliament’s Report, 2nd reading
Dec 2010: Informal trialogue negotiations to reach a final joint text
Jan 2011: European Parliament plenary sitting, 2nd reading
9 March 2011: Directive passed
25 Oct 2013: Deadline for transposition into national law
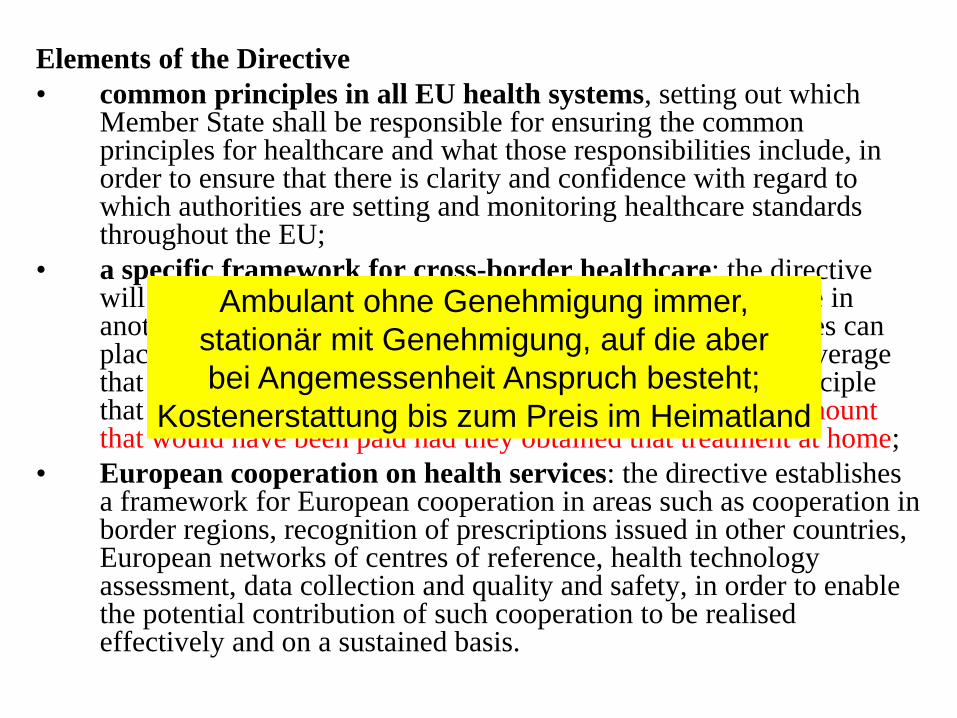
Elements of the Directive
• common principles in all EU health systems, setting out which Member State shall be responsible for ensuring the common principles for healthcare and what those responsibilities include, in order to ensure that there is clarity and confidence with regard to which authorities are setting and monitoring healthcare standards throughout the EU;
• a specific framework for cross-border healthcare: the directive will make clear the entitlements of patients to have healthcare in another Member State, including the limits that Member States can place on such healthcare abroad, and the level of financial coverage that is provided for cross-border healthcare, based on the principle that patients are entitled to obtain reimbursement up to the amount that would have been paid had they obtained that treatment at home;
• European cooperation on health services: the directive establishes a framework for European cooperation in areas such as cooperation in border regions, recognition of prescriptions issued in other countries, European networks of centres of reference, health technology assessment, data collection and quality and safety, in order to enable the potential contribution of such cooperation to be realised effectively and on a sustained basis.
Ambulant ohne Genehmigung immer,
stationär mit Genehmigung, auf die aber
bei Angemessenheit Anspruch besteht;
Kostenerstattung bis zum Preis im Heimatland
Deutsche
Verbindungsstelle
Ausland beim GKV-
Spitzenverband hat
diese Aufgabe
übernommen – aber
welche
Informationen kann
sie bieten?
Direkte
Ergebnisse:
Qualität,
Zufrieden-
heit Strukturen
Patienten
Prozesse
Gesundheit
der
Bevölkerung
Gesund-
heits-
“Outcome“
Andere Politikbereiche
Ernährung/ Landwirtschaft
Umwelt
Gesundheitssystem Finanzielle
Ressourcen
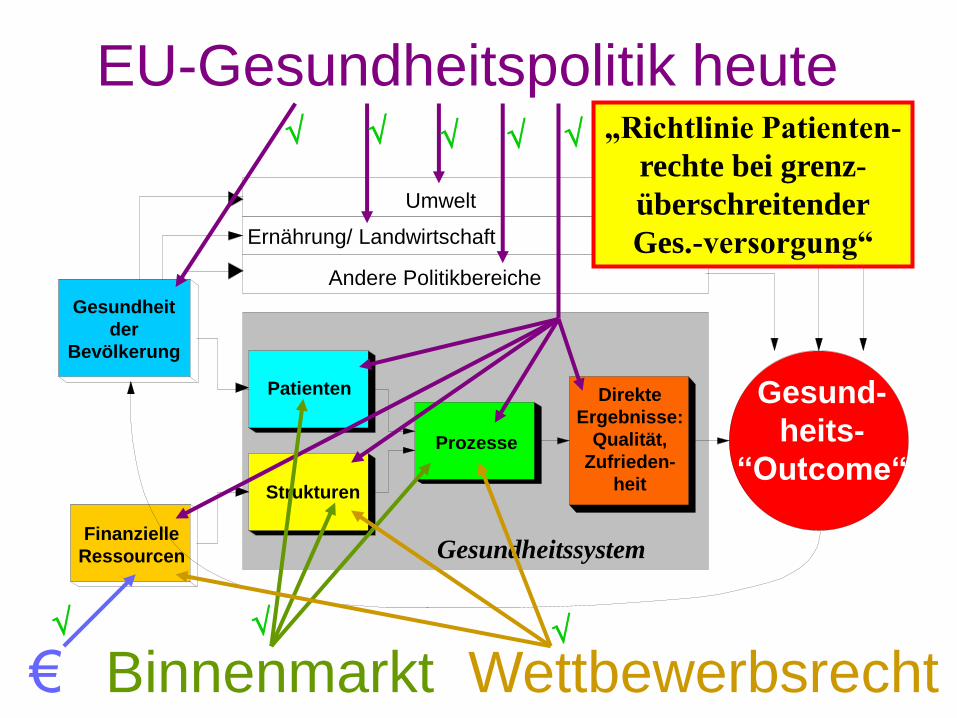
EU-Gesundheitspolitik heute
Wettbewerbsrecht Binnenmarkt €
„Richtlinie Patienten-
rechte bei grenz-
überschreitender
Ges.-versorgung“
Direkte
Ergebnisse:
Qualität,
Zufrieden-
heit Strukturen
Patienten
Prozesse
Gesundheit
der
Bevölkerung
Gesund-
heits-
“Outcome“
Andere Politikbereiche
Ernährung/ Landwirtschaft
Umwelt
Gesundheitssystem Finanzielle
Ressourcen
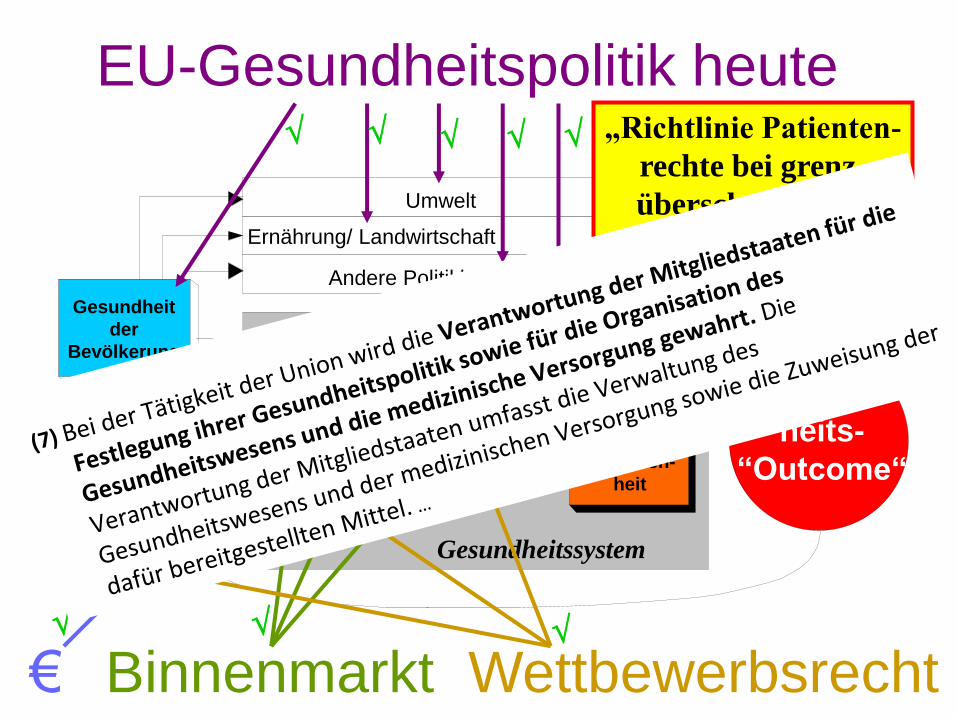
EU-Gesundheitspolitik heute
Wettbewerbsrecht Binnenmarkt €
„Richtlinie Patienten-
rechte bei grenz-
überschreitender
Ges.-versorgung“
• Direkte Wirkung 1: Klarstellung, wer verantwortlich ist
pot. Steigerung grenzüberschreitender Gesundheitsversorgung
• Direkte Wirkung 2: Kooperation bzgl. Health Technology
Assessment, europäische Referenzzentren …
• Hauptwirkung (indirekt): verstärkter Druck auf Ländern,
Qualität transparent zu machen
• (wird verstärkt durch)
– direkten Einfluss der Troika auf Gesundheitssysteme der
Länder mit Rettungspaket,
– die Einbeziehung der Gesundheitssysteme auch in die
Überprüfungen zum Stabilitäts- und Wachstumspaktes durch
die Kommission (“europäisches Semester“)
Wirkungen der Richtlinie „Patientenrechte bei grenzüberschreitender Gesundheitsversorgung“
- Public Health Expenditure at 6% of GDP
- €2 bn savings in pharmaceuticals between
2010 and 2012 (through pricing
mechanisms and prescribing monitoring)
- 25% decrease in expenditure for purchase
of medical services and goods (by end 2011)
- Introduction of single Health Insurance
Fund (EOPYY), with 50% reduction in
admin staff and 25% reduction in contracted doctors
- 10% + 5% reduction in hospital costs in 2011 and 2012
- 10% + 15% reduction in compensation costs (doctors wages and fees)
in 2011 and 2012
- Introduction of hospital computerisation and monitoring systems
Das wissen/ erwarten (?) wir: Memorandum mit Griechenland

Europäisches Semester – Landes-spezifische Empfehlungen zu
Reformen im Gesundheitssystem (plus Langzeitpflege), 2011-2014
2011:
4 Länder
2012:
6 Länder (NL zu Lang-zeitpflege)
2013:
11 Länder
2014:
16 Länder
Das wissen die meisten von uns (noch) nicht
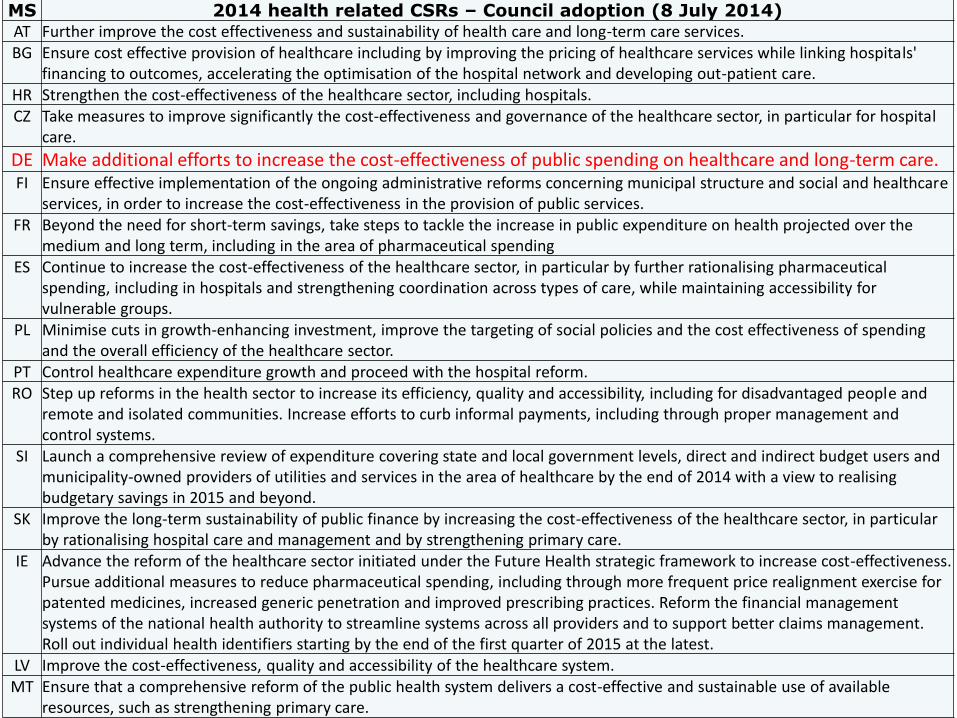
MS 2014 health related CSRs – Council adoption (8 July 2014) AT Further improve the cost effectiveness and sustainability of health care and long-term care services. BG Ensure cost effective provision of healthcare including by improving the pricing of healthcare services while linking hospitals'
financing to outcomes, accelerating the optimisation of the hospital network and developing out-patient care. HR Strengthen the cost-effectiveness of the healthcare sector, including hospitals. CZ Take measures to improve significantly the cost-effectiveness and governance of the healthcare sector, in particular for hospital
care.
DE Make additional efforts to increase the cost-effectiveness of public spending on healthcare and long-term care. FI Ensure effective implementation of the ongoing administrative reforms concerning municipal structure and social and healthcare
services, in order to increase the cost-effectiveness in the provision of public services. FR Beyond the need for short-term savings, take steps to tackle the increase in public expenditure on health projected over the
medium and long term, including in the area of pharmaceutical spending ES Continue to increase the cost-effectiveness of the healthcare sector, in particular by further rationalising pharmaceutical
spending, including in hospitals and strengthening coordination across types of care, while maintaining accessibility for vulnerable groups.
PL Minimise cuts in growth-enhancing investment, improve the targeting of social policies and the cost effectiveness of spending and the overall efficiency of the healthcare sector.
PT Control healthcare expenditure growth and proceed with the hospital reform. RO Step up reforms in the health sector to increase its efficiency, quality and accessibility, including for disadvantaged people and
remote and isolated communities. Increase efforts to curb informal payments, including through proper management and control systems.
SI Launch a comprehensive review of expenditure covering state and local government levels, direct and indirect budget users and municipality-owned providers of utilities and services in the area of healthcare by the end of 2014 with a view to realising budgetary savings in 2015 and beyond.
SK Improve the long-term sustainability of public finance by increasing the cost-effectiveness of the healthcare sector, in particular by rationalising hospital care and management and by strengthening primary care.
IE Advance the reform of the healthcare sector initiated under the Future Health strategic framework to increase cost-effectiveness. Pursue additional measures to reduce pharmaceutical spending, including through more frequent price realignment exercise for patented medicines, increased generic penetration and improved prescribing practices. Reform the financial management systems of the national health authority to streamline systems across all providers and to support better claims management. Roll out individual health identifiers starting by the end of the first quarter of 2015 at the latest.
LV Improve the cost-effectiveness, quality and accessibility of the healthcare system. MT Ensure that a comprehensive reform of the public health system delivers a cost-effective and sustainable use of available
resources, such as strengthening primary care.





























