Embed Size (px)
Citation preview

Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Didactic: Pushing the Surgical Envelope II: The Methods to Our Madness
PROGRAM CHAIR
Ted T.M. Lee, MD
Danny C.Y. Chou, MBBS, MRCOG, FRANZCOGRicardo Pereira, MD, FACOG Linda C. Yang, MD, MS

Professional Education Information Target Audience This educational activity is developed to meet the needs of surgical gynecologists in practice and in training, as well as other healthcare professionals in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 3 Troubleshooting Approaches for Challenging, Peritoneal Access and Optimizing Exposure in Gynecologic Laparoscopy L.C. Yang ....................................................................................................................................................... 4 Ureter – Techniques in Identification, Dissection and Uretolysis D.C.Y. Chou ................................................................................................................................................... 8 Maintaining and Reclaiming Hemostasis – An Untaught But Absolutely Imperative Aspect of Laparoscopic Dissection T.T.M. Lee .................................................................................................................................................... 13 Methodical Approach to the Obliterated Anterior Cul de Sac – Aftermath of Prior Cesarean Section L.C. Yang ..................................................................................................................................................... 16 Location Is Everything – The Challenges of Broad Ligament and Cervical Fibroid D.C.Y. Chou ................................................................................................................................................. 20 Unfreeze the Frozen Pelvis – Hysterectomy for Severe Endometriosis with Obliteration of Cul de Sac R. Pereira .................................................................................................................................................... 25 Laparoscopic Management of Bowel Endometriosis and Associated Repairs R. Pereira .................................................................................................................................................... 34 Laparoscopic Management of Urinary Endometriosis and Associated Repairs T.T.M. Lee ................................................................................................................................................... 41 Cultural and Linguistics Competency ......................................................................................................... 46

PUSH-707: Didactic: Pushing the Surgical Envelope II: The Methods to Our Madness
Ted T.M. Lee, Chair
Faculty: Danny C.Y. Chou, Ricardo Pereira, Linda C. Yang
As gynecologic surgeons mature in experience and skill, few will leave their comfort zone and push the
surgical envelope to tackle challenges that they most fear and avoid. Those who do push the surgical
envelope with sheer bravado alone risk failure and infamy. Surgeons who succeed are those who adopt
a methodical and systematic approach. Anatomy and exposure are frequently cited as the foundations
of pelvic surgery. Faithful practice of the principles of surgical dissection is paramount for the surgeon to
venture to the next level. True mastery occurs in those who develop the ability to quickly formulate
various strategic plans when confronted with anticipated as well as unexpected surgical difficulties.
There is certainly no shortage of challenging pathologies to push our surgical envelope in laparoscopic
surgery. The obliterated anterior cul-de-sac from previous cesarean deliveries, and a frozen pelvis as a
result of advanced endometriosis, can both present very perplexing clinical quandaries. Likewise, broad
ligament or cervical fibroids and ovarian remnants can present different sets of challenges. Refining the
skills to repair visceral injuries, control hemorrhage, and maintain hemostasis laparoscopically will help
surgeons to minimize morbidities and decrease conversions to laparotomy.
This course will explore all of these skills and more, through the use of surgical video to illustrate the
strategies and techniques necessary to overcome the difficulties associated with various anatomy
distorting pathologies. Participants will develop a greater understanding of safe and effective
approaches to the challenging surgical scenarios through lectures that are both evidence- and
experience-based.
Learning Objectives: At the conclusion of this course, the clinician will be able to: 1) Articulate
techniques to achieve peritoneal access in patients with extensive anterior abdominal wall adhesions, as
well as techniques necessary to overcome difficulties associated with laparoscopy in obese patients; 2)
formulate anatomy-based strategies when confronting various challenging surgical scenarios such as
frozen pelvis, cervical fibroid and dense uterine adhesions; 3) apply the principle behind the techniques
in the identification, dissection of ureter, and difficult uretolysis; 4) integrate various techniques to
optimize exposure during complex pelvic surgeries; 5) incorporate the techniques of detection and
repair of visceral injuries in laparoscopy; and 6) articulate the principles in the surgical treatment of GI
and GU endometriosis.
Course Outline
12:30 Welcome, Introductions and Course Overview T.T.M. Lee
12:35 Troubleshooting Approaches for Challenging, Peritoneal Access and
Optimizing Exposure in Gynecologic Laparoscopy L.C. Yang
12:55 Ureter – Techniques in Identification, Dissection and Uretolysis D.C.Y. Chou
1

1:15 Maintaining and Reclaiming Hemostasis – An Untaught But Absolutely
Imperative Aspect of Laparoscopic Dissection T.T.M. Lee
1:35 Interactive Case Video Presentation 1 Presenters: D.C.Y. Chou, L.C. Yang
Moderators: T.T.M. Lee, R. Pereira
1:55 Break
2:15 Methodical Approach to the Obliterated Anterior Cul de Sac – Aftermath of
Prior Cesarean Section L.C. Yang
2:35 Location Is Everything – The Challenges of Broad Ligament and
Cervical Fibroid D.C.Y. Chou
2:55 Unfreeze the Frozen Pelvis – Hysterectomy for Severe Endometriosis
with Obliteration of Cul de Sac R. Pereira
3:15 Laparoscopic Management of Bowel Endometriosis and Associated Repairs R. Pereira
3:35 Laparoscopic Management of Urinary Endometriosis and Associated Repairs T.T.M. Lee
3:55 Interactive Case Presentation 2 Presenters: T.T.M. Lee, R. Pereira
Moderators: D.C.Y. Chou, L.C. Yang
4:20 Questions & Answers All Faculty
4:30 Adjourn
2

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop (listed in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* R. Edward Betcher* Amber Bradshaw Speakers Bureau: Myriad Genetics Lab Other: Proctor: Intuitive Surgical Sarah L. Cohen Consultant: Olympus Erica Dun* Joseph (Jay) L. Hudgens Contracted Research: Gynesonics Ted T.M. Lee Consultant: Ethicon Endo-Surgery Frank D. Loffer, Medical Director, AAGL* Suketu Mansuria Speakers Bureau: Covidien Linda Michels, Executive Director, AAGL* Karen C. Wang* Johnny Yi* SCIENTIFIC PROGRAM COMMITTEE Sawsan As-Sanie Consultant: Myriad Genetics Lab Jubilee Brown* Aarathi Cholkeri-Singh Consultant: Smith & Nephew Endoscopy Speakers Bureau: Bayer Healthcare Corp., DySIS Medical, Hologic Other: Advisory Board: Bayer Healthcare Corp., Hologic Jon I. Einarsson* Suketu Mansuria Speakers Bureau: Covidien Andrew I. Sokol* Kevin J.E. Stepp Consultant: CONMED Corporation, Teleflex Stock Ownership: Titan Medical Karen C. Wang* FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Danny C.Y. Chou* Ted T.M. Lee Consultant: Ethicon Endo-Surgery Ricardo Pereira* Linda C. Yang* Content Reviewer has no relationships. Asterisk (*) denotes no financial relationships to disclose.
3

Troubleshooting Approaches for Challenging Peritoneal Access and
Optimizing Exposure in Gynecologic Laparoscopy
Linda C. Yang, MD MSDivision of Minimally Invasive Gynecologic Surgery
Loyola University Medical CenterStritch School of Medicine
Disclosure
I have no financial relationships to disclose.
Objectives
● Identify risks of primary peritoneal access
● Discuss strategies for safe peritoneal access
● Review intraoperative techniques for achieving maximal laparoscopic exposure
Abdominal Access Complications
• Primary peritoneal access injury occurs in <1 % of patients
• Trocars = most common device cited in malpractice claims associated with laparoscopic procedures
• >50% of laparoscopic complications occur during initial peritoneal access2-6
Abdominal Access Complications
• Bowel and retroperitoneal vascular injuries comprise ~3/4 of injuries during primary trocar placement
• 50% of bowel injuries have a delay in diagnosis (>24 hrs)7
Independent predictors of fatality:
Delayed recognition
Major vessel injury
Age >59 years
Who is at risk?
• Prior abdominal/pelvic surgery
• Extremes of BMI - morbidly obese and very thin patients
• Pregnancy
• Large abdominal or pelvic mass
• Hernia repair with mesh
4

Risk of Adhesions with Prior Surgery• Rate of umbilical adhesions8
• Group I: No prior surgery 0.68%
• Group II: Prior LSC 1.6%
• Group III: Prior laparotomy/horizontal suprapubic incision 19.8%
• Group IV: Prior laparotomy/midline 51.7%
• Rate of severe adhesions with potential for bowel injury
• Group I: 0.42%
• Group II: 0.8%
• Group III: 6.87%
• Group IV: 31.46%
Choosing Your Entry Approach
“There is insufficient evidence to recommend one laparoscopic entry technique over another” (Cochrane Database 2015)
But entry-associated complications diminish with experience
Open Hasson
Closed Veress
Direct Optical
No difference for vascular or visceral injuryClosed entry with greater risk of failed entry
closed No difference for visceral injury compared to open and
closed
Closed Veress Entry
• In obese women, the umbilicus is shifted caudally from the aortic bifurcation9
Hurd WW et al., Obstet Gynecol 1992
Hurd WW et al., Obstet Gynecol 1992
Closed Veress Entry
• In thin women, the distance from the anterior abdominal wall to aorta may be as little as 2 cm9
Hurd WW et al., Obstet Gynecol 1992
Open Hasson Entry• Choose your incision wisely: infraumbilical
vs intraumbilical • Intraumbilical incision affords entry at the
thinnest aspect of the umbilicus• Elevate the abdominal wall and provide
adequate traction• Avoid pushing the fascia away – it’s closer
than you think!• Tag fascial edges
Ensuring Safety After Entry • 360 degree survey • Maintain supine position until survey completed• Delay Trendelenburg
5

Accessory Trocar Placement• Know your abdominal wall
landmarks• Direct visualization for all
accessory trocar placement• Stay perpendicular• Drain the bladder for
suprapubic trocar placement
Overcoming the Obesity Challenge• Patient positioning pad/system
• Avoid slippage• Neural protection• Consider securing upper torso
with strap/tape
• Arm boards offer extra width • Surgeon ergonomics less
compromised than with toboggans
• Be generous with padding• Consider bariatric bed
Overcoming the Obesity Challenge
• Umbilicus = thinnest entry point, however, distortion of umbilical location due to panniculus
• Use caution with Veress (umbilical) entry given risk of failed entry
• Consider LUQ entry • Bariatric trocars may be
necessary
Trocar Placement in Obese Patients
Normal BMI Obese
Overcoming the Adhesion Challenge LUQ Entry – Palmer’s Point• 1974 Dr. Raoul Palmer• 3 cm below the left costal margin in the
mid-clavicular line
• Place orogastric/nasogastric tube• Contraindications:
• H/o gastric bypass• H/o splenectomy• Splenomegaly
6

LUQ Entry – Palmer’s Point
Costal margin
Mid-clavicular Line
Point ofentry
Adhesiolysis• Find and create windows of opportunity
• Blunt dissection – open and spread technique
• Employ cold-cutting techniques at serosal interfaces• Use energy wisely• Apply appropriate tissue tension• Do not hesitate to place an additional port (above level
of most cephalad adhesion)
Optimizing Laparoscopic Exposure (Videos)• Use of angled laparoscope • Cephalad trocar placement • Suturing of rectosigmoid• Exposure of ovarian fossa/pelvic sidewall• Vaginal cuff closure
References1. Cochrane Database of Systematic Reviews 2015, Issue 8. Art. No.: CD006583
2. Kirchoff P, et al., JMIG 2005:12(4)
3. Hurd WW, et al., Am J Obstet Gynecol 1994;171:642-6
4. Magrina JF, Clin Obstet Gynecol 2002;45(2):469
5. Makai G, Isaacson K, Clin Obstet Gynecol 2009;52(3):401-11
6. Pickett SD, et al., Obstet Gynecol Clin N Am 2010;37:387-97
7. Chandler JG, et al., J Am Coll Surg 2001; 192(4):478
8. Audebert AJM, Gomel V, Fertil Steril 2000;73(3):631
9. Hurd WW, et al., Obstet Gynecol 1992; 80(1)
Thank You!
Questions?
7

Dr Danny ChouSydney Women’s Endosurgery Centre
8

Direct VisualisationVermiculationStentDissection
9

10

11

1. De Cicco. C et al. Laparoscopic management of ureteral lesions in gynecology. Fertil Steril 2009
2. Camanni M et al. Laparoscopic conservative management of ureteral endometriosis. Current
Opinion in Obstetrics and Gynecology 2010
3. Teeluckharry B et al. Urinary Tract Injury at Benign Gynecologic Surgery and the Role of
Cystoscopy. A systematic Review and Meta-Analysis. Obstet Gynecol Dec 2015
4. Teeluckharry B et al. Urinary Tract Injury at Benign Gynecologic Surgery and the Role of
Cystoscopy. A systematic Review and Meta-Analysis. Obstetrics and Gynecology Dec 2015
5. Dowling RA et al. Iatrogenic ureteral injury. J Urol 1986
6. Ibeanu OA et al. Urinary tract injury during hysterectomy based on universal cystoscopy. Obstet
Gynecol 2009
7. Aronson MP et al. Low risk of ureteral obstruction with “deep” uterosacral ligament suture. Am J
Obstet Gynecol 2005
8. Chou MT, et al. Prophylactic ureteral catheterisation in gynecological surgery: a 12 year
randomised trial in a community hospital. Int Urogynecol J Pelvic Floor Dysfunct 2009
12

Ted Lee, M.D.
Director of Minimally Invasive Gynecologic Surgery
Magee Womens Hospital
University of Pittsburgh Medical
Disclosure
Consultant: Ethicon Endosurgery
Objectives
Describe the techniques and strategies necessary to maintain and reclaim hemostasis during laparoscopic dissection in normal as well as distorted anatomy using videos and diagrams.
Top Reasons for Hemostasis in Laparoscopic Surgery
1. If you cannot see, you cannot operate.
2. Optimize detection of tissue planes.
3. Blood suck up all of the light in the operative field.
4. Poor hemostasis diminish exposure of relevant structures which leads more visceral injury and further bleeding.
Maintaining Hemostasis
Prudent use of thermal energy for sharp dissection
Dissect in the right tissue plane and space. (Look for the bubbles)
Take care of bleeder as you see it. (Quick burst of bipolar or monopolar)
Art of blunt dissection
Sequential applications of blunt dissection and sharp dissection with energy
Minimizing Thermal Spread /Injury when Performing Sharp Dissection
with Energized Instrument
Speed: keep moving
Tissue tension
Create space
13

Sharp Dissection with Energy Dissecting in the Right tissue Plane/ Space
Timely Control of Small BleedersBlunt Dissection:
:
Tool of interrogation.
Identifying the right tissue plane for further sharp and/or blunt dissection.
Create space for safer deployment of energy
Art of Blunt DissectionSequential applications of blunt dissection and sharp
dissection with energy
14

Facilitating Dissection with Application of Differential Tissue Tension
When separating two different tissues, the dissection is facilitated when there is a difference in tissue tension between the tissues being separated.
The reason behind distending the vagina with colpotomizer cup. (Facilitate vesicovaginal dissection and rectovaginal dissection.
Reclaiming Hemostasis
While maintaining hemostasis during dissection is very important, ability to reclaim hemostasis allow the case to be done safely and laparoscopically
Reclaiming Hemostasis
Take a deep breath and stay calm.
What are the important structures around the bleeders?
Is it small bleeder slowly staining the tissue or big bleeder that demands your attention right away?
Suction and irrigation
Apply pressure with sponge.
Reclaiming Hemostasis: Tools of the Trade
Suction irrigator.
Sponge
Bipolar instruments
Clips
Suture
Reclaiming Hemostasis: Compilation Summary
Hemostatic dissection is the foundation of good surgery.
The ability to reclaim hemostasis provides the necessary confidence to push your surgical envelope.
15

Methodical Approach to the Obliterated Anterior Cul-de-Sac:
Aftermath of Prior Cesarean Section
Linda C. Yang, MD MSDivision of Minimally Invasive Gynecologic Surgery
Loyola University Medical CenterStritch School of Medicine
Disclosure
I have no financial relationships to disclose.
Objectives
● Identify the anatomic and technical challenges related to anterior cul-de-sac obliteration
●Describe surgical techniques for hysterectomy complicated by anterior cul-de-sac adhesions
●Review strategies and tools for bladder flap dissection
Facing the Challenge
●Anticipate the unexpected●Prepare for the worst case
scenario●Goals:
● Restore anatomy● Minimize bleeding● Minimize injury
Risk of Cystotomy
• Women with ≥2 CD are at greater risk of incidental cystotomies (OR: 8.55, 95% CI: 3.98-18.36)1
Anatomic Challenges
●Limits placement of suprapubic port●Uterine manipulator may be difficult to place ●Loss of tactile and visual landmarks due to obscuring of
colpotomizer cup ●Bladder margins cannot be distinguished
16

Trocar Placement Alternatives to Uterine Manipulator
Breisky-Navratil retractor
Lucite vaginal stent
Techniques of Delineating Bladder Anatomy
●Backfilling bladder● Fluid insufflation (NaCl with or without methylene blue)
● Three-way Foley catheter method● Cystoscope method● Suction-irrigator method
● CO2 insufflation
●Rigid Foley catheter guide2
Backfilling Bladder (Video)
Rigid Foley Catheter Guide Use of Rigid Foley Catheter Guide (Video)
17

Key Clinical Pearls
●Devascularize as best as possible before tackling dense adhesions● Upper pedicles (IP or utero-ovarian)● Uterine pedicles
●Restore anatomy to uncover anatomic landmarks●Find correct tissue planes
● Keep adipose tissue with bladder● Err on the side of the uterus
Approach to Vascular Pedicles
●Secure and divide upper pedicles first●Divide round ligaments●Skeletonize uterine artery pedicle ●Ligate and transect uterine artery from a posterior
approach ●Alternatively, may ligate the uterine artery at its origin
Benefits of the Posterior Approach
●Efficient control of uterine vasculature●Posterior landmarks are preserved – colpotomizer cup,
uterosacral ligaments●Does not require full development of bladder flap
Posterior Approach to Uterine Vasculature (Video)
Lateral Approach to Vesicovaginal Space
●Traditional midline approach for creation of bladder flap can predispose to injury● Common mistake: peritoneum is pushed away from bladder but
bladder remains adherent to cervix
●Lateral approach enables surgeon to identify key landmarks (uterine vasculature, colpotomizer cup, cervix)
●Development of a surgical window ●Unlikely that c-section scar extends to lateral aspect
Lateral Approach to Vesicovaginal Space (Video)
18

Adhesions likely to occur at and superior to lower uterine segment
Develop the space below the adhesion site – find the window of opportunity
Recognition of Urinary Tract Injury
●Use of sodium fluorescein during cystoscopy● 0.25 mL to 1 mL of 10% sodium fluorescein IV ● Average time until colored ureteral jets were visualized = 4.3
minutes3
References1. Duong TH, Patterson TM, Int Urogynecol J 2014; 25(8):1037-40
1. Lee TM, Hur HC, J Pelvic Med & Surgery 2006;12(5):277-279
1. Ostrosky, et al., Obstet Gynecol 2016;127:47S Thank You!
Questions?
19

20

Interventions to reduce haemorrhage during myomectomyfor fibroids (Review)
Kongnyuy EJ, WiysongeCS
Authors’ conclusions
At present thereismoderate-qualityevidencethat misoprostol or vasopressin mayreducebleedingduringmyomectomy,and low-qualityevidence that bupivacaine plus epinephrine, tranexamic acid, gelatin-thrombin matrix, ascorbic acid, dinoprostone, loop ligation, afibrin sealant patch, a peri-cervical tourniquet or a tourniquet tied round both cervix and infundibulopelvic ligament may reducebleeding during myomectomy. There isno evidence that oxytocin, morcellation and temporary clipping of theuterineartery reduceblood loss. Further well designed studiesarerequired toestablish theeffectiveness, safetyand costsof different interventionsfor reducing
Thisisareprint of aCochranereview, prepared and maintained byTheCochraneCollaboration and published in TheCochraneLibrary2014, Issue8
htt // th h lib
21

22

23

24

Unfreeze the Frozen Pelvis -Hysterectomy for Severe Endometriosis
with Obliteration of Cul de SacRicardo M A Pereira, MD
DirectorCenter for Endometriosis and Minimally Invasive Gynecological Surgery
Hospital e Maternidade Santa Joana - São Paulo
Disclosure
• I have no financial relationships to disclose.
Objectives
• Discuss the complexity of pelvic anatomy.
• Identify the anatomic location and degree of each endometriotic lesion.
• Recognize the principal landmarks related to endometriosis surgery in the posterior compartment of the pelvis.
• Demonstrate the specific dissection techniques for each anatomic region affected during hysterectomy for severe endometriosis with blockage of the cul de sac (Douglas Pouch).
• Demonstrate different techniques for hysterectomies with frozen pelvis.
Introduction
Female pelvic anatomy is one of the most complex in thehuman body. Endometriosis infiltrates the tissues and cancompletely modify this anatomy. Because of this,endometriosis surgery can be one of the most challengingto occur in gynecological surgery.
Introduction
5
Thomas S Cullen, 1868-1953
Cullen TS. Adenomyoma of the rectovaginal septum. JAMA 1916; 67:401–6.
"The removal of extensive adenomyoma of therectovaginal septum is infinitely more difficultthan a (Wertheim) hysterectomy for carcinomaof the cervix."
Introduction
"In the presence of total obliteration of the uterus beneath a roof ofextensive thick pelvic adhesions to the bladder and bowel, accessto the uterus trans-abdominally or laparoscopically is the mostdangerous and time-consuming phase of the procedure."
Pelosi and Pelosi, Journal of Laparoendoscopic & Advanced Surgical Techniques, 1997
25

Surgical Technique
en bloc resection
Laparoscopic en bloc resection for treatment of the obliterated cul-de-sac in endometriosis.
Redwine, D. J. Reprod Med 1992
Frozen Pelvis: Definition
This is the loss of mobility of the uterus and the adnexal caused by adheringlesions, due to inflammation, infection, neoplasia or surgery, with are frequentlyassociated with endometriosis, anatomic pelvic distortion and causes theobliteration of the posterior compartment, and less frequently, the anteriorcompartment.
Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Nerves and Plexus
• Vessels
• Muscular Pelvic Basin
• Anatomic Spaces
Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Vessels
• Nerves and Plexus
• Muscular Pelvic Basin
• Anatomical Spaces
Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Vessels
• Nerves and Plexus
• Muscular Pelvic Basin
• Anatomical Spaces
Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Vessels
• Nerves and Plexus
• Muscular Pelvic Basin
• Anatomical Spaces
26

Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Vessels
• Nerves and Plexus
• Muscular Pelvic Basin
• Anatomical Spaces
Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Vessels
• Nerves and Plexus
• Muscular Pelvic Basin
• Anatomical Spaces
Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Vessels
• Nerves and Plexus
• Muscular Pelvic Basin
• Anatomical Spaces
Frozen Pelvis: Anatomical Landmarks
• Viscera
• Parietal Peritoneum
• Connective Tissue
• Vessels
• Nerves and Plexus
• Muscular Pelvic Basin
• Anatomical Spaces
Central Lesion:Hysterectomy: Severe Endometriosis
• Posterior Wall (Subserosal/Myometrium)
• Retrocervical/Cervical
• Cul de Sac
• Rectovaginal Septum
• Rectossigmoid
• Posterior Vaginal Fornice (Central)
Central Lesion: Subserosal/MyometriumHysterectomy: Severe Endometriosis
27

Central Lesion: CervicalHysterectomy: Severe Endometriosis
Central Lesion: CervicalHysterectomy: Severe Endometriosis
Central Lesion: RetrocervicalHysterectomy: Severe Endometriosis
Central Lesion: RetrocervicalHysterectomy: Severe Endometriosis
Central Lesion: Cul de SacHysterectomy: Severe Endometriosis
Central Lesion: Posterior Vaginal Fornice/ Rectovaginal SeptumHysterectomy: Severe Endometriosis
28

Rectovaginal Septum AnatomyHysterectomy: Severe Endometriosis
Central Lesion: Posterior Vaginal Fornice/ Rectovaginal SeptumHysterectomy: Severe Endometriosis
Lateral Lesions:
• Adnexal
• Parametrium
• Paracervix
• Paracolpium
• Paraproctium
• Ureter
• Vessels
• Inferior Hypogastric Plexus
• Obturator Nerve
• Sacral Roots
• Sciatic Nerve
• Pelvic Floor
• Sacrospinal Ligament
Hysterectomy: Severe Endometriosis
Parametrium AnatomyHysterectomy: Severe Endometriosis
Lateral Lesions: Lateral ParametriumHysterectomy: Severe Endometriosis
Lateral Lesions: Lateral ParametriumHysterectomy: Severe Endometriosis
29

Lateral Lesions: UreterHysterectomy: Severe Endometriosis
Frozen Pelvis: Surgical Technique for Ureter
Video
Lateral Lesions: Obturator NerveHysterectomy: Severe Endometriosis
Lateral Lesions: Sacral RootsHysterectomy: Severe Endometriosis
Lateral Lesions: Obturator NerveHysterectomy: Severe Endometriosis
Pelvic Connective Tissue: AnatomyHysterectomy: Severe Endometriosis
• Parietal Pelvic Fascia
• Visceral Pelvic Fascia
• Ligament or Band
• Loose Areolar Tissue
30

Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Location:
The presacral fascia is the pelvic continuation of the visceralabdominal fascia. It traces a curve covering the pelvic wallslaterally and the sacrum dorsally and fuses ventrally with theparametrium and paracervix, laterally and dorsally with therectovaginal septum, paracolpium and paraproctium (Lat.Ligament of the Rectum), and caudally with the rectosacralfascia.
Presacral Fascia(Fascia presacralis)
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Presacral Fascia
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Presacral Fascia
Ercoli, Ceccaroni, Fanfani, and Scambia 2006
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Presacral Fascia
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Presacral Fascia
Visceral Nervous System:
13
8
2
4
5
6
7
9
1. Sup. Hypog. Plexus
2. Hypog. Nerves
3. Sacral Root
4. Pelvic Splanc. Nerve
5. Sciatic Nerve
6. Inf. Hypog. Plexus
7. Uterine Nerve
8. Intestinal Nerve
9. Vesical Nerve
31

Autonomic Nervous System (Motor)
•Hypogastric Nerves
•Inferior Hypogastric Plexus (Pelvic Plexus)
•Pelvic Splanchnic Nerves (Erigent Nerve)
•Efferent Branches Medial Bundle (Intestinal)
Cranial Bundle (Uterine)
Anterior Bundle (Vesical and Vaginal)
•Pudendal Nerves
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Deep Uterine Vein (DUV)
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Inferior Hypogastric Plexus
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Inferior Hypogastric Plexus
Endometriosis: Anatomical LandmarksHysterectomy: Severe Endometriosis
Inferior Hypogastric Plexus
Frozen Pelvis: Neural Surgical Technique
Video
32

Frozen Pelvis: Hysterectomy Technique
• Mobilization of left colon
• Dissection of lateral pelvic wall, ovary and left broad ligament
• Dissection of lateral pelvic wall, ovary and right broad ligament
• Dissection of central structures
• Detachment of intestinal lesion
• Hysterectomy
Frozen Pelvis: Hysterectomy Technique
Video
Frozen Pelvis: Vascular Surgical Technique
Video
Frozen Pelvis: Vascular Surgical Technique
Video
Conclusions
• Frozen pelvis due to endometriosis requires a deep knowledge of retroperitoneal pelvic anatomy
• Site specific surgical techniques
• Time consuming surgeries require a highly committed and trained team
References
Ercoli A, Delmas V, Fanfani F, Gadonneix P, Ceccaroni M, Fagotti A, Mancuso S, Scambia G (2005) Terminologia Anatomicaversus unofficial descriptions and nomenclature of the fasciae and ligaments of the female pelvis: a dissection-basedcomparative study. Am J Obstet Gynecol 193:1565–1573
Cullen TS. Adenomyoma of the rectovaginal septum. JAMA 1916;67: 401–6.
Pelosi A, Pelosi M III, Vaginal Hysterectomy for Benign Uterine Disease in Laparoscopically Confirmed Frozen Pelvis. Journal ofLaparoendoscopic & Advanced Surgical Techniques: Vol 7m, 6, December 1997.
Pereira RMA, Zanatta A, Reich H, et al. Use of circular stapler for laparoscopic excision of rectosigmoid anterior wallendometriosis. Surg Technol Int. 2008;17:181–186.
Pereira RM, Zanatta A, Preti CD, et al. Should the gynecologist perform laparoscopic bowel resection to treat endometriosis?Results over 7 years in 168 patients. J Minim Invasive Gynecol 2009; 16:472–479.
Pereira RM, Zanatta A, de Mello Bianchi PH, et al. Transvaginal ultrasound after bowel preparation to assist surgical planning for bowel endometriosis resection. Int J Gynaecol Obstet 2009; 104:161.
33

Laparoscopic Management of Bowel Endometriosis and Associated
RepairsRicardo M A Pereira, MD
DirectorCenter for Endometriosis and Minimally Invasive Gynecological Surgery
Hospital e Maternidade Santa Joana - São Paulo
Disclosure
• I have no financial relationships to disclose
Objectives
• Describe anatomic based strategies and techniques to remove intestinal endometriosis
• Discuss specific surgical techniques for each location
• Discuss anatomic strategies for preserving autonomous nerves and minimizing intestinal evacuation and micturition problems
• Demonstrate the use of the vaginal route as an important aid in minimally invasive surgical treatment of intestinal endometriosis
Introduction
• Rectum
• Sigmoid
• Cecum
• Appendix
• Terminal-Ileum
Pereira RM, Zanatta A, Preti CD, et al. Should the gynecologist perform laparoscopic bowel resection to treat endometriosis? Results over 7 years in168 patients. J Minim Invasive Gynecol 2009; 16:472–479.
5
LOWER R.
SIGMOID
UPPER R.
MIDDLE R.
}
}}
}24%
18%
23%
11.5%
Introduction
6
Introduction
Redwine DB, Sharpe DR. Laparoscopic segmental resection of the sigmoidcolon for endometriosis. J Laparoendosc Surg 1991; 1:217–220.
Nezhat C, Nezhat F, Pennington E. Laparoscopic treatment of infiltrativerectosigmoid colon and rectovaginal septum endometriosis by the techniqueof videolaparoscopy and the CO2 laser. Br J Obstet Gynaecol 1992;99:664–667.
34

7
Pre-operative Strategy
• Detailed anamnesis and physical examination
• It is possible to map almost all intestinal lesions using TVUS or MRI
• It is possible to plan probable site specific surgical techniques
• Prior discussion with the patient and medical team regarding surgical strategy, results and associated risks
9
Intra-operative Strategy
• Map all intestinal lesions on the rectosigmoid, ileum, cecum and appendix
• Evaluate how pre-operative mapping corresponds with clinical evaluation, TVUS and/or MRI
• Select a strategy for each lesion and the sequence for the surgery
10
Appendix Endometriosis: Lesions
• One of the most common locations for intestinal endometriosis
• Can cause local inflammatory symptoms and dyspepsia
• Frequently the lesions are located on the tip followed by the middle and base of the appendix. Occasionally lesions can be found on the mesoappendix
• The appearance of the lesions can be typical or atypical with different sizes and shapes
11
Appendix Appearance: Typical
Typical
12
Appendix Appearance: Atypical
35

13
Laparoscopic appendectomy (LscAp): Surgical Technique
• Laparoscopically assisted trans-umbilical appendectomy
• Laparoscopically assisted trans-vaginal appendectomy
• Laparoscopic appendectomy
14
Appendix Endometriosis: Surgical Technique
Video
15
Cecum Endometriosis: Lesions
• Can be isolated or infiltrated into the base of the appendix
• In rare cases it can infiltrate the ileocecal valve
• In extremely rare cases it can cause intussusception of the appendix
16
Cecum Endometriosis: Lesions
17
Laparoscopic cecectomy (LscC): Surgical Technique
• Laparoscopically assisted mini-laparotomic cecectomy
• Laparoscopically assisted trans-vaginal cecectomy
• Laparoscopic cecectomy
18
Terminal-Ileum Endometriosis: Lesions
Small Multifocal
Stenosis
36

19
Laparoscopic terminal ileal resection (LscIR): Surgical Technique
• Laparoscopic terminal ileal resection
• Laparoscopically assisted trans-umbilical ileal resection
• Laparoscopically assisted mini-laparotomic resection
20
Terminal-Ileum Endometriosis: Surgical Technique
Video
21
Sigmoid Endometriosis: Lesions
22
Cecum Endometriosis: Surgical Technique
Video
23
Rectosigmoid Endometriosis: Lesions
• Size
• Isolated form
• Multifocal
• Joint
24
Rectosigmoid Endometriosis: Size
37

25
Rectosigmoid Endometriosis: Multifocal
26
Rectosigmoid Endometriosis: Fused
27
Rectosigmoid Endometriosis: Fused
28
Rectosigmoid Endometriosis: Surgical Technique
• Sigmoid lesions are generally larger and deeper than those of the lower and middle rectum. They frequently require segmental resection
• Lower rectal lesions are technically more difficult as they involve the intraperitoneal rectum, pericervical ring and are adjacent to the inferior hypogastric plexus. This requires a high level use of nerve sparing techniques.
• Isolated lower rectum lesions can frequently be removed through a discoid resection. Rare cases require ultra-low segment resection.
29
Rectosigmoid Endometriosis: Surgical Technique
• Shaving (mucosal skinning)
• Discoid Resection
• Segmental Resection
30
Rectal Endometriosis: Shaving Technique
38

31
Rectal Endometriosis: Discoid Technique
Video32
Rectosimoid Endometriosis: Segmental Resection Surgical Technique
Video
33
Bowel Endometriosis Surgery: G.I. Injury
Video34
Bowel Endometriosis Surgery: G.U. Injury
Video
35
Bowel Endometriosis Surgery: Protecting the Anastomosis
Video
Laparoscopic Bowel Resection (LscBR) for Endometriosis performed by gynecologists
39

Conclusions
• Intestinal endometriosis surgery involves multiple surgical techniques in different locations.
• Minimize the risk of unexpected endometriosis with a thorough patient history, physical exam and a TVUS or MRI performed by a professional highly trained in mapping endometriosis
• Highly trained team in pelvic, intestinal, genitourinary and neurodisfunction surgery is necessary and can be a single gynecologist team or multi-professional.
• MIGS, using the combination of laparoscopic and vaginal route can be very valuable in intestinal endometriosis surgery.
References
3-Redwine DB, Sharpe DR. Laparoscopic segmental resection of the sigmoid colon for endometriosis. J Laparoendosc Surg 1991; 1:217–220.
2-Nezhat C, Nezhat F, Pennington E. Laparoscopic treatment of infiltrative rectosigmoid colon and rectovaginal septumendometriosis by the technique of videolaparoscopy and the CO2 laser. Br J Obstet Gynaecol 1992; 99:664–667.
1-Pereira RM, Zanatta A, de Mello Bianchi PH, et al. Transvaginal ultrasound after bowel preparation to assist surgical planningfor bowel endometriosis resection. Int J Gynaecol Obstet 2009; 104:161.
4-Pereira RM, Zanatta A, Preti CD, et al. Should the gynecologist perform laparoscopic bowel resection to treat endometriosis?Results over 7 years in 168 patients. J Minim Invasive Gynecol 2009; 16:472–479.
5-Chamié LP, Pereira RM, Zanatta A, Serafini PC. Transvaginal US after bowel preparation for deeply infiltrating
endometriosis: protocol, imaging appearances, and laparoscopic correlation. Radiographics. 2010;30(5): 1235-49.
6-Pereira RM, Zanatta A, Serafini PC, Redwine D. The feasibility of laparoscopic bowel resection performed by a gynaecologist
to treat endometriosis. Curr Opin Obstet Gynecol. 2010;22(4):344-53.
40

Laparoscopic Management of Urinary Endometriosis and
Associated Repairs
Ted Lee, M.D.Director, Minimally Invasive Gynecologic SurgeryMagee Womens HospitalUnversity of Pittsburgh Medical Center
Disclosure
Consultant: Ethicon Endosurgery
• Discuss pathophysiology bladder and ureteral endometriosis
• Review clinical presentations of bladder and ureteral endometriosis.
• Diagnosis of bladder and ureteral endometriosis.
• Explain surgical and medical management of bladder and ureteral endometriosis.
Objectives
• Relatively rare when compared to bowel endometriosis.
• Best estimate 1-2 % of all symptomatic endometriosis.
Prevalence
• Bladder-85%
• Ureter-10%
• Kidney-3%
• Urethra-2%
Locations of GU Tract Endometriosis
Definition: endometriosis infiltrating detrusor muscle
Bladder Endometriosis
41

• Similar to other deep infiltrating endometriosis.
• It can be iatrogenic from previous c-sec.
Pathogenesis
• Irritative urinary symptoms: frequency, urgency, dysuria, typically worse during menses.
• Hematuria is rare. If present, it is usually cyclic.
• Some patients maybe asymptomatic.
• Most patients have endometriosis elsewhere. Most patients will have typical symptoms of dysmenorrhea, dyspareunia and dyschezia.
Clinical Presentations
Workup for Bladder Endometriosis
• High index of clinical suspicion.
• Ultrasound or MRI.
• Cystourethroscopy.
• Be vigilant of endometriosis elsewhere in the pelvis.
42

Role of Cystoscopy
• Provide histopathologic diagnosis. Rule out other intravesical pathology.
• Assess the proximity of endometriotic nodule to the ureteral orifice.
• Same as treatment for other endometriosis.
• Limited data on efficacy.
• Preop GnRH agonist should be strongly considered if nodule is large to reduce the size of partial cystectomy. ( not evidenced based)
Medical Treatment
• Simple partial cystectomy with two layer closure for bladder dome nodule.
• Ureteral stents are recommended especially for lower nodules.
• Need to develop vesicovaginal space for nodule closer to the vesicouterine junction. Partial resection of myometrium maybe necessary for vesicouterine nodule
• For large defect, retropubic space should be developed for tension free closure.
Surgical Treatment
• If nodule is close to ureteral orifice, intravesicalportion of ureter may be involved. Ureteroneocystostomy may be necessary especially in patients with known hydronephrosis.
• Bladder is backfilled to ensure watertight closure.
• Foley catheter is left in place for 7-10 days. Followed by VCUG.
Surgical Treatment
Laparoscopic Treatment of Bladder Endometriosis
Prognosis after Partial Cystectomy for Deep Bladder Endometriosis
• Dome lesions: symptom recurrence 7%, objective recurrence 0% in 3 years.
• Bladder base lesions: symptom recurrence 37%, objective recurrence 26%.
Fedele et al., Fertil Steril June 2005;83: 1729-1733
43

Symptoms of Ureteral Endometriosis
• Some present with symptoms of acute obstruction. Flank pain in 25%
• Hematuria in 15%
• Asymptomatic in 50%
• Most with symptoms typical for endometriosis in general.
• Secondary hydronephrosis resulted from extrinsic as well as intrinsic obstruction.
• Secondary hydronephrosis resulted from extrinsic as well as intrinsic obstruction.
• Extrinsic lesion 70-80%
• Intrinsic lesion 20-30%.
• Bilateral involvement 12%
• Unilateral involvement 88%.
• Left 83% . Right 5%
Distribution of Ureteral Endometriosis
Diagnosis of Ureteral Endometriosis
• Screening renal ultrasound for patients with suspected endometriosis.
• IVP
• Ureteroscopy
• Endoluminal ultrasound
• Laparoscopy
• Largely ineffective as fibrosis does not respond to hormonal suppression.
Medical Treatment of Ureteral Endometriosis
Surgical Treatment of Ureteral Endometriosis
• Uretolysis followed by double J stent
• Segmental ureteral resection with end to end anastomosis or ureteroneocystotomy with or without psoas hitch.
Outcome of Laparoscopic Uretolysis
• 33 patients underwent uretolysis for mod to severe hydronephrosis with median 16 month follow-up.
• Bilateral involvement 12%
• Unilateral involvement 88% with the left ureter involvement in 83%
• Ureteral obstruction recurrence rate 12 %.
Ghezzi et al, Fertil Steril 2006 ;86:418-422
44

Laparoscopic Treatment for Ureteral Endometriosis. Laparoscopic Ureteral Reimplantation
• Regardless of types of surgical treatments ( uretolysis, segmental resection anastomosis, ureteroneocystomy), endometriosis should be excised in addition to the treatment of hydronephrosis to ensure pain/symptom relief as well as to minimize the risk of recurrent hydronephrosis.
Surgical Treatment of Ureteral Endometriosis
• Urinary endometriosis is relatively rare.
• Non specific urinary symptoms maybe present. Most patients have endometriosis elsewhere in the pelvis and presents with typical symptoms of endometriosis.
• High index of suspicion is often required to ensure proper preoperative workup, which is useful for proper inform and consent.
• Initial medical treatment for bladder endometriosis is reasonable after confirmation of diagnosis.
• Most patients responds well to partial cystectomy especially if the nodule is located at the bladder dome.
Summary and Recommendations
• Endometriosis nodule near triagone may require ureteroneocystotomy.
• Screening renal ultrasound in patients with suspected endometriosis is useful to prevent silent loss of renal function.
• Medical treatment of ureteral endometriosis associated with persistent hydronephrosis is largely ineffective.
• The majority of ureteral endometriosis is extrinsic in nature. Uretolysis can be attempted in most patients with hydronephrosis but reparative ureteral surgeries may be required in some.
Summary and Recommendations
45

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
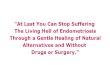
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
46